Lapjag IGD 01-03-2015
23
MORNING REPORT MARCH 1 ST 2015 EMERGENCY DEPT GP on duty : dr. Jimmy, dr Husnah Coass on duty : Kussetya, Rio
-
Upload
ghina-ninditasari -
Category
Documents
-
view
219 -
download
0
description
moderate asthma acute on mild perssten asthma
Transcript of Lapjag IGD 01-03-2015
MORNING REPORTMARCH 1ST 2015
EMERGENCY DEPT
GP on duty : dr. Jimmy, dr Husnah
Coass on duty : Kussetya, Rio
PATIENT RECAPITULATION1. Mr P, 70 yo. Vomitus observation
2. Mr AS 51 yo. Nstemi+HHD+CVD
3. Mrs K, 66 yo. Posttrauma with prolong febris
4. Mr S, 57 yo. GEA
5. Mrs SJ, 50 yo. Anemia ec breast cancer
6. Mrs KT, 52 yo. BE infectouys.
7. Mrs EN, 72 yo. Asthma acute medium
PATIENT’S IDENTITY• Name : Mrs E• Sex : female• Age : 72 years old• Religion : Moeslem• Marital Status : Married• Address : dago villa H 3/19• MR : 801885
ANAMNESIS
Autoanamnesis on 02/03/15 at 02.00 AM
• Chief Complaint : shortness of breath since 1 days before admission
• Additional complaint: productive cough
HISTORY OF PRESENT ILLNESS
- Patient come to ER with shortness of breath
since 1 day before admission
- Shortness of breath were continously. She also
complained about productive cough since 3 days
before admission but the mucus was very difficult
to take it out
- Patient has a history of asthma since she
was children. Asthma attack are not certain,
2 times a month. The relapsing factor is
dust
- She has a problem with sleep since 1 day
ago. Headache (-), nausea (-), vomitting (-),
fever (-)
• She also has a history of tumor
mediastinum and already metastase to
hepar.
• 40 years ago, she had a struma tiroid and
had been get an operation procedure for it.
PAST ILLNESS• Struma multiple nodosa post op
• There is no history
FAMILY ILLNESS
PHYSICAL EXAMINATION
VITAL SIGNS• General State : Mild Sickness• Consciousness : Compos Mentis• Blood Pressure : 100/60 mmHg• Pulse : 112x/minute, regular• Respiratory Rate : 28 x/minute, regular• Temperature : 37.2oC• Body Weight : 55 kg• Body Height : 170 cm• BMI : (normoweight)
PHYSICAL EXAMINATION
General Examination• Head : Normocephal
• Eye : anemic conjunctiva (-/-), icteric sclera (-/-)
• Ears : normotia, discharge (-)• Nose : septum deviation (-), discharge (-)• Mouth : Pharynx hyperemis (-)
• Neck : nodes enlargement(+), followed with gerakan menelan
• Thorax : symmetric, intercostal retraction (-)
• Cor : ictus cordis -, thrill -, heave -, regular 1st and 2nd heart sound, murmur (-), gallop (-)
• Pulmo : vesicular (+/+). rales (-/-), wheeze(+/+)
• Abdomen : flat, not distended, epigastric
tenderness (-), timpani, no
enlargement of liver & lien, N bowel
sound
• Extremities: warm, edema (-/-), cyanosis (-),
CRT < 2 seconds
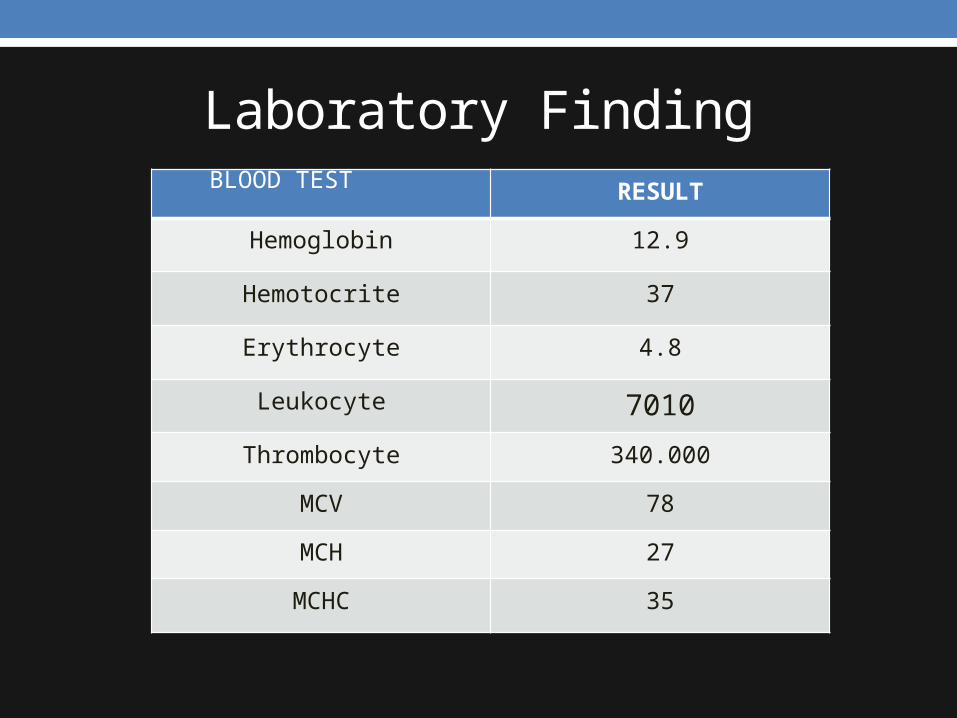
Laboratory FindingRESULT
Hemoglobin 12.9
Hemotocrite 37
Erythrocyte 4.8
Leukocyte 7010
Thrombocyte 340.000
MCV 78
MCH 27
MCHC 35
BLOOD TEST
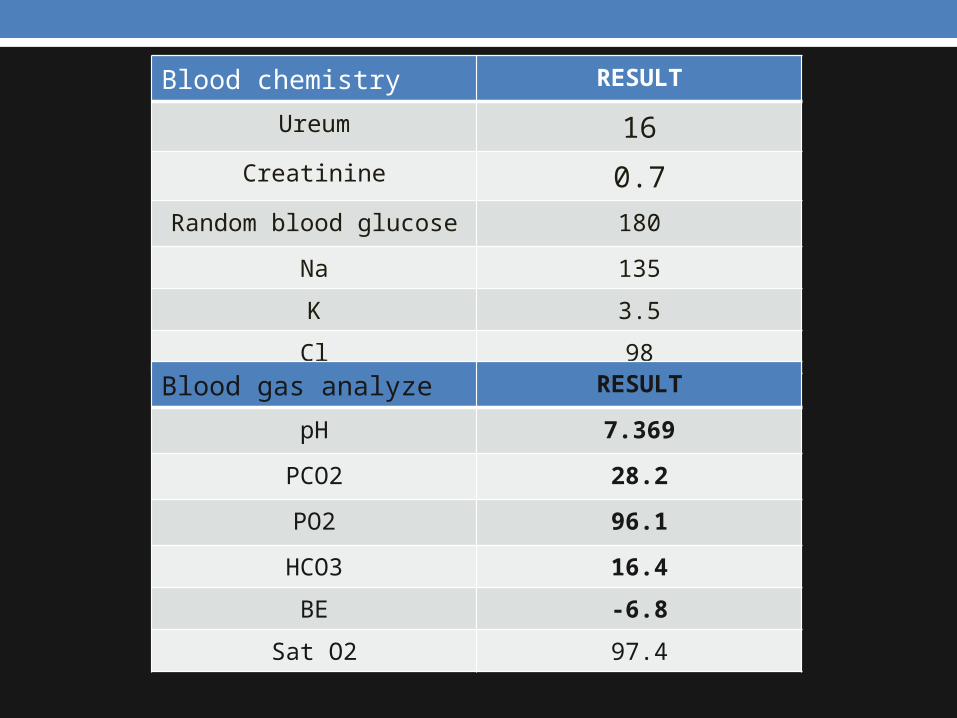
Blood chemistry RESULT
Ureum 16
Creatinine 0.7
Random blood glucose 180
Na 135
K 3.5
Cl 98
Blood gas analyze RESULT
pH 7.369
PCO2 28.2
PO2 96.1
HCO3 16.4
BE -6.8
Sat O2 97.4
RESUME
Female 70 years old came with shortness of breath since1
days before admission. She had history of asthma since
she was child. She complained about her productive cough
which are difficult to take out the mucus. She had a history
of struma nodosa and tumor mediastinum that have been
metastase to hepar..
• PE : HR: 112bpm, RR: 28x/min
neck: nodul enlargement (+)
pulmo : wheezing +/+•Lab finding: asidosis respiratorik
PROBLEMS LIST
• Moderate asthma acute on mild persisten asthma
ASSESSMENT
Moderate asthma acute on mild persisten asthma
Anamnesis:
• Shortness of breath 1 day ago, it happen continously.
Productive cough (+). Its difficult to take the mucuse out.
Had history of asthma. He only talk kata per kata
• PE: takipneu, takikardia. Px pulmo: wheezing (+)
• Lab: asidosis respiratorik
• Plan of diagnosis:• Rontgen Thorax • APE• Spirometri if patient in a stable condition
• Plan of therapy• O2 nasal canule 3 L/min• Ventolin + budesonide nebulizer• Dexamethason inj 1 amp• Aminofilin bolus inj ½ amp + 1 ½ amp drip
PROGNOSIS• Qua ad vitam : Dubia ad bonam• Qua ad functionam : Dubia ad bonam• Qua ad sanationam : Dubia ad bonam
THANK YOU
Comments