2007, terni, workshop interattivo, caso clinico 2
18
• A 65-year-old man presented to the Emergency Department (ED), and he had a 2 ½ hrs history of chest pain radiating to left arms and mandible. Clinical Case (1) • Anamnestic evaluation reveal that the patient’s past medical history was of familiarity, obesity, hypertension, for several years and for this he was taking beta-blocker and losartan, and dyslipidemia, for which he was taking nothing (no statin) . No ASA. • He had a 30 pack-year previous smoking history. • The onset of chest pain occurred when pt was relieved by rest. • Associated symptoms included shortness of breath, nausea and lipotimia.
-
Upload
centro-diagnostico-nardi -
Category
Health & Medicine
-
view
34 -
download
1
Transcript of 2007, terni, workshop interattivo, caso clinico 2

• A 65-year-old man presented to the Emergency Department (ED), and he had a 2 ½ hrs history of chest pain radiating to left arms and mandible.
Clinical Case(1)
• Anamnestic evaluation reveal that the patient’s past medical history was of familiarity, obesity, hypertension, for several years and for this he was taking beta-blocker and losartan, and dyslipidemia, for which he was taking nothing (no statin) . No ASA.
• He had a 30 pack-year previous smoking history.
• The onset of chest pain occurred when pt was relieved by rest.
• Associated symptoms included shortness of breath, nausea and lipotimia.

Clinical Case(1)
• Personal history reveal a previous AMI in ’91, treated (HSR) with PCA on LAD artery and Posterior Inter-ventricular right (PIV) artery whereas a pathologic Obtuse Marginal Artery (OMA) was not treated because complicated (no documentation).
• Pt reveal a subsequent coronary angiography evalutation in ’98 that confirm the patologic stenosis of OMA (no documentation) with subsequent further indication to stress-test evalutation.
• Moreover, according with his cardiologist, no further stress test evaluation was performed until now (9 yrs ago).

Clinical Case(1) EKG (Emergency Departement)

Clinical Case(1)
- R wave ≥0.04s in V1 or V2
- ST segment depr. V1 V3
- R/S ratio ≥1 in V1 and V2.
EKG (Emergency Departement)
R
R
R
S
S
• BP was 150/80 mmHg, and HR was 85/min, whereas the rest of the exam was unremarkable.

Clinical Case(1)
• First Line Therapy- Oxigen- Nitrate (iv)- ASA 500 mg (iv)- Eparin (bolus + cont. infusion iv)
• No changes in symptom
• An ECHO evaluation reveal Total Ackinesia of apex and posterior LV wall
R
R
R
S
S
Intensive CCU

• Turn ECG upside down and look at it from the back.
• Changes in V1 and V2 which might be over-looked at first glance, will be seen as abnormal Q waves, ST elevation and increased T wave inversion(2).
• R>0.04s and R≥S V1, showed a high specificity (>99%) and a high positive predictive value (91%).
• R≥0.04s and R≥S V2, showed 95% of specificity, and 73% positive predictive value.
Clinical Case(1) Intensive CCU

• Turn ECG upside down and look at it from the back.
• Changes in V1 and V2 which might be over-looked at first glance, will be seen as abnormal Q waves, ST elevation and increased T wave inversion(2).
• R>0.04s and R≥S V1, showed a high specificity (>99%) and a high positive predictive value (91%).
• R≥0.04s and R≥S V2, showed 95% of specificity, and 73% positive predictive value.
Clinical Case(1) Intensive CCU

Clinical Case(1)

Clinical Case(1)
• No absolute or relative CI were present to fibrinolitic therapy, and then was administrated with immediately disappeared of symptom
Intensive CCU
R
R
R
S
S
• 10 hrs after fibrinolisis, pt develop cerebral symptom with evidence at TC scan of parenchimal hemorragic expansion
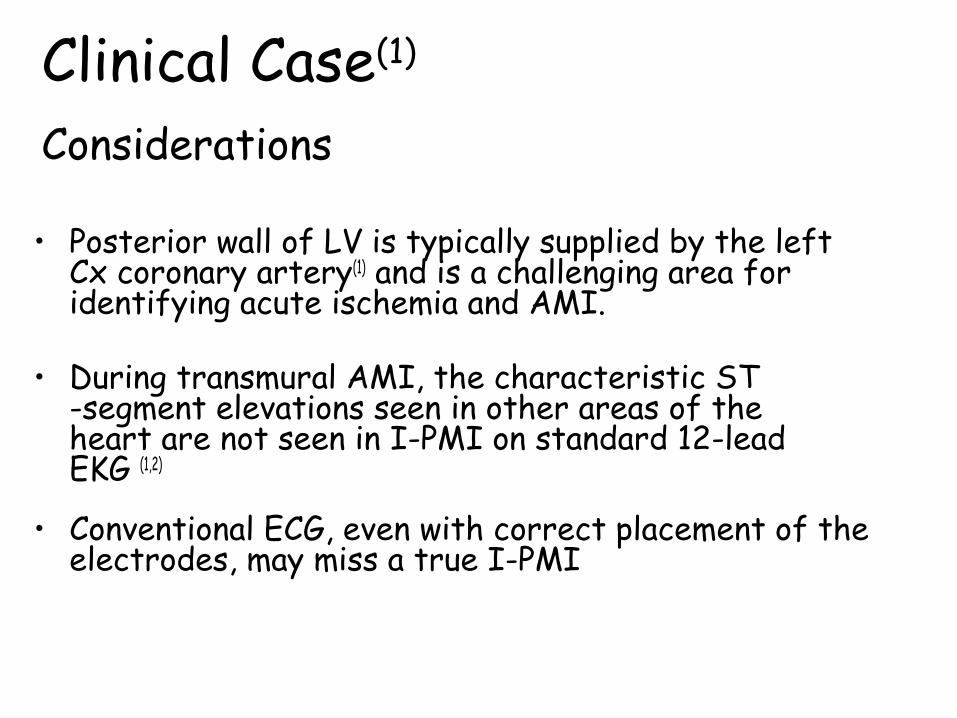
Clinical Case(1) Considerations
• Posterior wall of LV is typically supplied by the left Cx coronary artery(1) and is a challenging area for identifying acute ischemia and AMI.
• During transmural AMI, the characteristic ST -segment elevations seen in other areas of the heart are not seen in I-PMI on standard 12-lead EKG (1,2)
• Conventional ECG, even with correct placement of the electrodes, may miss a true I-PMI
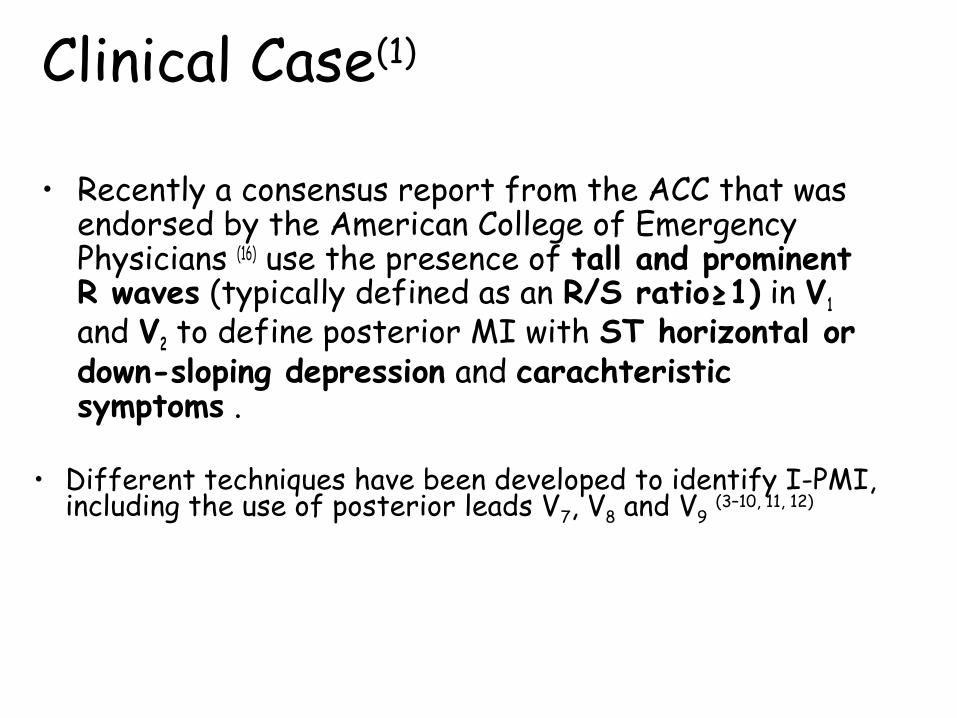
• Recently a consensus report from the ACC that was endorsed by the American College of Emergency Physicians (16) use the presence of tall and prominent R waves (typically defined as an R/S ratio≥1) in V1 and V2 to define posterior MI with ST horizontal or down-sloping depression and carachteristic symptoms .
• Different techniques have been developed to identify I-PMI, including the use of posterior leads V7, V8 and V9 (3–10, 11, 12)
Clinical Case(1)

Clinical Case(1)
• It has been suggested that tall R waves in anterior leads (V1, V2 and V3) are simply the electrical equivalent of Q waves in the posterior leads (V7, V8 and V9)(1,2)
• If acute I-PMI was suspected in the ED, these pt should be considered for thrombolytic therapy or – if possible – to immediate interventional Cath. Lab. (3–6)

• This pt presented with suggestive symptom, previous AMI and PCA procedure, several risk factor and EKG analisis of tall R waves in V1,V2,V3 an down-sloping ST depression in V1 V4 and a R/S ratio≥1 in V1 and V2
Clinical Case(1)
• No EKG signs reveal a previous MI • ECHO analysis reveal ackinesia of apex and posterior
LV wall• No Absolute or Relative CI were present for
fibrinolitic therapy
• Symptoms immediately disappeared after rTPA

• The true incidence of I-PMI is unknown but has been reported between 0-12% (6,7,9,18) of AMI when posterior leads V7 through V9 were obtained.
• If this were the case, these two findings would always occur simultaneously on a 15-lead ECG (a 12-lead ECG + posterior leads).
Clinical Case(1)


References(1)
1. Topol EJ, Van De Werf FJ. Acute myocardial infarction: Earlydiagnosis and management. In: EJ Topol, ed. Textbook ofCardiovascular Medicine. Philadelphia: Lippincott Williams andWilkins, 2002: 385-419.
2. Alexander RW, Pratt CM, Ryan TJ, Roberts R. ST-segmentelevation myocardial infarction: clinical presentation, diagnosticevaluation, and medical management. In: Fuster V, AlexanderRW, ORourke RA, eds. Hursts The Heart. New York: McGrawHill, 2004: 1277-349.
3. Oraii S, Maleki M, Tavakolian AA, et al. Prevalence and outcomeof ST-segment elevation in posterior electrocardiographic leadsduring acute myocardial infarction. J Electrocardiol 1999; 32:275-8.
4. Schamroth L. Posterior wall myocardial infarction. In: The 12-leadElectrocardiogram, Book 1 (of 2). Boston: Blackwell, 1989:176-80.

References(1)
5. Bough EW, Boden WE, Korr KS, Gandsman EJ. Left ventricularasynergy in electrocardiographic “posterior” myocardial infarction.J Am Coll Cardiol 1984; 4:209-15.
6. Agarwal JB, Khaw K, Aurignac F, LoCurto A. Importance ofposterior chest leads in patients with suspected myocardialinfarction, but nondiagnostic, routine 12-lead electrocardiogram.Am J Cardiol 1999; 83:323-6.
7. Huey BL, Beller GA, Kaiser DL, Gibson RS. A comprehensiveanalysis of myocardial infarction due to left circum.ex arteryocclusion: comparison with infarction due to right coronary arteryand left anterior descending artery occlusion. J Am Coll Cardiol1988; 12:1156-66.
8. Chaitman BR. Posterior myocardial infarction revisited. J AmColl Cardiol 1988; 12:167-8.

References(1)
9. Wang SF, Drew BJ. New electrocardiographic criteria for posteriorwall acute myocardial ischemia validated by a PTCA model of AMI. Am J Cardiol 2001; 87:970-4.
10. Madird WL, Sanmarco ME, Gaarder TG, Selvester RH. Circum.exocclusion and posterior MI, diagnostic criteria and automated ECG analysis programs. In: Bailey JJ, ed. Computerized Interpretation of the ECG. XI. Proceedings of the Engineering Foundation Conferences. New York: Engineering Foundation, 1986: 37-44.
11. Casas RE, Marriott HJL, Glancy DL. Value of leads V7-V9 indiagnosing posterior wall AMI and other causes of tall R waves in V1-V2. Am J Cardiol 1997; 80:508-9.
12. OKeefe JH, Sayed-Taha K, Gibson W, et al. Do patients withleft circum.ex coronary artery-related AMI without ST-segment elevation bene.t from reperfusion therapy?Am J Card. 1995; 75:718-20.