2006 terni, workshop interattivo. la terapia ablativa percutanea della fibrillazione atriale
47
La terapia ablativa percutanea La terapia ablativa percutanea della della FIBRILLAZIONE ATRIALE FIBRILLAZIONE ATRIALE Stefano Nardi MD, PhD “ “ SANTA MARIA” GENERAL HOSPITAL - TERNI SANTA MARIA” GENERAL HOSPITAL - TERNI THORACIC SURGERY AND THORACIC SURGERY AND CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOG CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOG CENTER AND CARDIAC PACING UNIT CENTER AND CARDIAC PACING UNIT I II II III III VI VI Map Map PV1-2 PV1-2 PV10-1 PV10-1 CS CS 13 December 2006, Terni 13 December 2006, Terni
-
Upload
centro-diagnostico-nardi -
Category
Health & Medicine
-
view
40 -
download
2
Transcript of 2006 terni, workshop interattivo. la terapia ablativa percutanea della fibrillazione atriale

La terapia ablativa percutanea La terapia ablativa percutanea della della FIBRILLAZIONE ATRIALEFIBRILLAZIONE ATRIALE
Stefano Nardi MD, PhD
“ “SANTA MARIA” GENERAL HOSPITAL - TERNISANTA MARIA” GENERAL HOSPITAL - TERNI THORACIC SURGERY AND THORACIC SURGERY AND
CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOGIC CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOGIC CENTER AND CARDIAC PACING UNIT CENTER AND CARDIAC PACING UNIT
IIIIIIIIIIIIVIVI
MapMap
PV1-2PV1-2
PV10-1PV10-1
CSCS
13 December 2006, Terni 13 December 2006, Terni

Considerations• All AFib affected patients have an increased Morbidity
• The overall increased Mortality is between 1,6-2,6% (Manitoba and Framingham Studies)
• 5% year ischemic stroke (non-rheumatic AF) 2-7 times without AF
• 1/6 Cerebro-Vascular Accident (CVA) occurs in AFib • Framingham Study
- RHD 17 X rate of CVA (age-matched CTR)- Attributable risk 5 X > non-RHD- Risk of Stroke increased with age (1,5% at 50-59 yrs vs 23,5% at 80-89 yrs)

DIAGNOSI DI PSDIAGNOSI DI PS %%Sindrome Coronarica Acuta 24.4
Dolore neuro-radicolare 17.1
Malattia Polmonare 15
ARITMIA CARDIACA ARITMIA CARDIACA 1616Vasovagale 6.5
Scompenso cardiaco congestizio 5
Iperventilazione 3.3
Crisi ipertensiva 2.2
Sindrome della parete toracica 1.8
Malattie gastrointestinali 1.2
Pneumotorace 0.6
Embolia polmonare 0.4
Dissezione Aortica 0.3
Pleurite 0.2
Pericardite 0.1
DIAGNOSI NON CHIARA DIAGNOSI NON CHIARA 5.95.9
Von Kodolitsch Y, et Al. Arch Intern Med. ‘00
PREVALENCE

1. Pharmacologic therapy (AADs)
STRATEGIES
3. Radiofrequency Catheter Ablation – AV node modulation– Ablate & Pace– Primary Ablation (CURATIVE)
2. Anti-tachycardia Pacing (ATP)
How we can approach AFib ?How we can approach AFib ?

Quinidine 1 yr 3fold increase mortalityDrug Efficacy F.U. Drawbacks
50% SR
AuthorCoplen, ‘90
Dysopiramide 1 yr Many side effects, 11% drop out
As quinidine Karlson ‘88
Flecainide 1 yr Not indicated in CAD49% SR Van Gelder, ‘89
Propafenone 6 mo Not indicated in CAD60% SR Stroobandt, ‘97
Amiodarone 1 yr Side effects61% SR Gosselink, ‘92
Overall long term efficacy (meta-analysis)
AADs is still a good option ?

AFFIRM
STAFSTAF
PIAFPIAF
HOT CAFÉHOT CAFÉ
PAF-2PAF-2
RACERACE
Randomized TRIALS
• Paroxysmal Atrial Fibirllation 2 (PAF2) Eur Heart J ’02
• Pharmacological Intervention in AF (PIAF) Lancet ’00.
• Comparison of rate control and rhythm control in pts with AF (AFFIRM) NEJM ‘02.
• Randomized trial of rate-control versus rhythm CTR in PeAF: the Strategies of Treatment of AF (STAF) study. JACC ‘03.
• Effect of rate or rhythm control on QoL in PeAF: results from the Rate Control Versus Electrical Cardioversion (RACE) Study. JACC ‘ 04.
• How to treat C-AF (HOT-CAFÉ`) New DehliNew Dehli

The original AFFIRM STUDY

- Strategies based to maintaining SR at 1 yrs FU without AADs is <30% (recurrence between 50-70%) ....
Pooled (meta-analysis) data from PAF2, PIAF, STAF, AFFIRM e RACE
- … however in most cases AADs based strategies are not able to prevent RECURRENCE of A Fib.
• Global efficacy 40 - 50% (Reduce in long term FU)
25% interruption of treatment !
• SIDE EFFECTS– Until 20% of cases (3-5% TdP)
CHALLANGE of AADsCHALLANGE of AADs

• Arrhythmia-free survival after ECV in pts with PeAF
Lower Curve Outcome after a single shock when no prophylactic AADs was given
Upper curve Outcome with repeated ECV in conjunction with AADs prophylaxis
CHALLANGE of AADs + ECVCHALLANGE of AADs + ECV
Carlsson J, JACC ‘01

Ozcan C, NEJM ’01 and ‘04
• Controversial issue in the long-term FU (detrimental effects of RVA pacing)
• Continue to have loss of LA contraction
Pooled (meta-analysis) data from PAF2, PIAF, STAF, AFFIRM e RACE
CHALLANGE of Ablate & PaceCHALLANGE of Ablate & Pace
Reduction of symptoms w/o eliminating AF Still have CVA risk and necessity of ACT. (Wood MA, Circulation ’00; Brignole M, EHJ ’02, Europace ‘01)
Limit: Palliative Rx Need of PM !

One year later…
AFFIRM revisited…AFFIRM revisited…
AFFIRM revisited…AFFIRM revisited…
AFFIRM revisited…AFFIRM revisited…
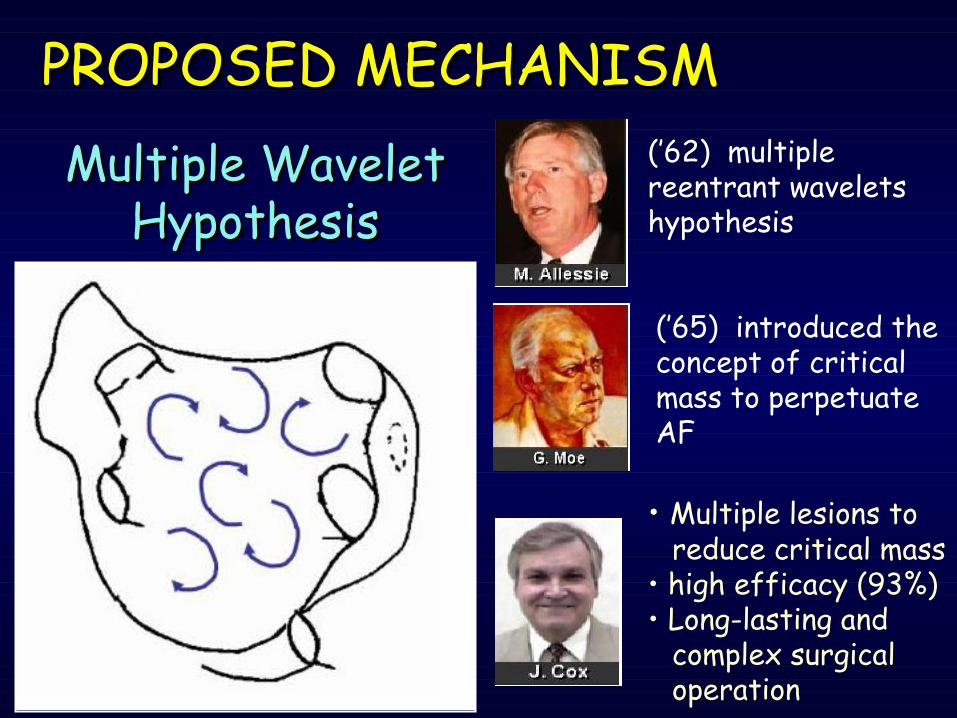
PROPOSED MECHANISM PROPOSED MECHANISM Multiple Wavelet Multiple Wavelet
HypothesisHypothesis(’62) multiple reentrant wavelets hypothesis
(’65) introduced the concept of critical mass to perpetuate AF
• Multiple lesions to reduce critical mass
• high efficacy (93%)• Long-lasting and
complex surgical operation

• Swartz (‘96) demonstrated its percutaneous feasibility
• 29 pts treated (C-AF) successfully (79%), but… high procedural time and unacceptable rate of major complications (22% - stroke, tamponade, PV stenosis)
EARLY PERCUTANEOUS APPROACHES EARLY PERCUTANEOUS APPROACHES

Right Atrium procedure showed success-rate w/o AADs between 6 and 25%, whereas the percentage increased if line extended to Left Atrium, even if no reproducible
Haissaguerre ’96 40%Pappone ’99 58% Ernst ‘00 0%
Pericardial Effusion/ tamponade (11%)SNA dysfunction (8%)Cerebral infarction (>8%)PVs stenosis ( ? )
LINEAR APPROACHLINEAR APPROACH
Gaita F, Circulation; ’98, Garg A, J CV El ’99, Natale A, P Cl El, ’00; Calò L, It Heart J, ’01

Pulmonary Vein triggers
Haissaguerre, NEJM ‘’98
Firing from PVs
RF

RF
Atrial Fibrillation MechanismsAtrial Fibrillation Mechanisms
• PVs as TRIGGER and PERPETUATORS
• SUBSTRATE with CRITICAL MASS
• GANGLIONIC PLEXI affecting vagal innervation
• ROTOR sites critical to the maintenance of reentry
How does it work?

• In 1907 the presence of muscular sleeves around the PVs was documented for the first time
• Now they are considered important triggers of AFib

• LA-PVs junction could be functionally considered a “BROAD BAND”
• Possible arrhythmogenic nature due to Automatism (EMBRIONAL NATURE) or micro-reentry (anisotropic carachteristic of LA-PVs junction)
JUNCTIONJUNCTION
Hocini M, Card. Res ’02 Hocini M, Circulation ’02Arora, Circulation 03
Haissaguerre, NEJM ‘96
Pato-physiology and Electrogenesis

Hocini, Circulation `02Arora, Circulation `03
Mandapati, Circulation `00
Intraparietal Anisotropism JUNCTIONJUNCTION
Pato-physiology and Electrogenesis

Spragg DD, Circulation ’03
Regional Alterations of Protein Expression in AFib dogs
ELECTROPHYSIOLOGICMECHANISMS

How can we Ablate AFib ?How can we Ablate AFib ?

How can we Ablate AFib ?How can we Ablate AFib ?

Different Approach
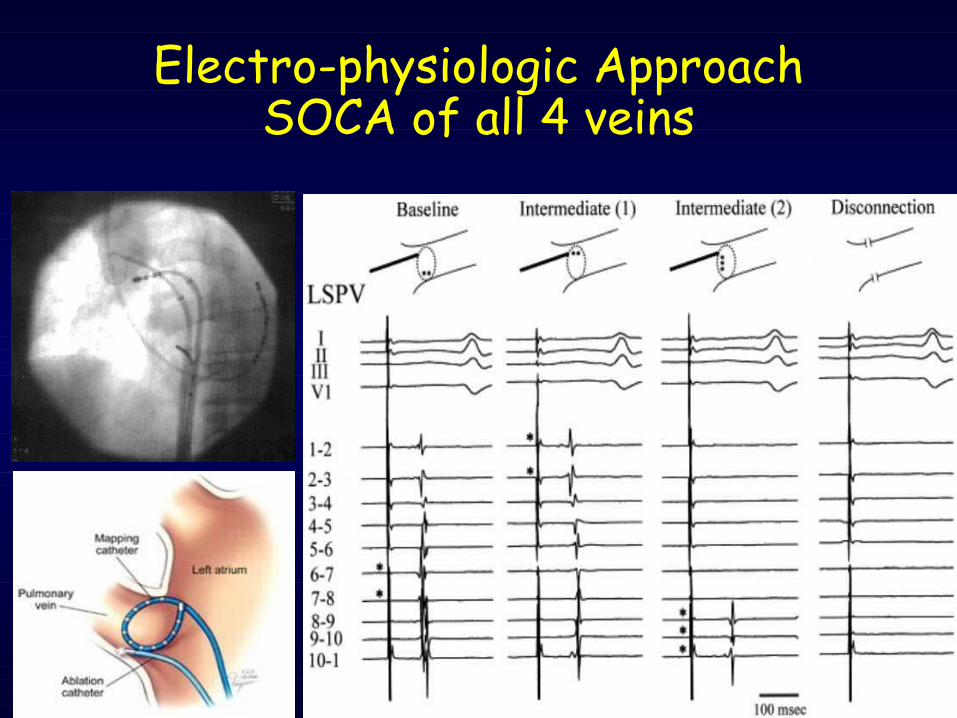
Electro-physiologic ApproachSOCA of all 4 veins

AuthorsAuthors % success-rate % success-rate
HaissaguerreHaissaguerre Circulation 2000Circulation 2000 73%73% FAPFAPChen SAChen SA Circulation 2001Circulation 2001 81%81% FAPFAPErnstErnst PACE 2003PACE 2003 69%69% FAPFAPArentzArentz Circulation 2003Circulation 2003 62%62% FAPFAPCappatoCappato Circulation 2003Circulation 2003 8888%% FAPFAPMarroucheMarrouche JACC 2002JACC 2002 90%90% FAP FAP OralOral Circulation 2002Circulation 2002 85% 85% FAP FAP
22%22% FACFAC
Electro-physiologic ApproachSOCA of all 4 veins

Pulmonary vein anatomy the first
challenge
Left common trunk 3 right lower veins
Normal

Evolution over the time3D mapping system in AFib3D mapping system in AFib

Anatomical Approach Anatomical Approach CLAACLAA
• 251 Patients• 54±12 min of RF
End Point: (75%)• PVP < 0.1 mV• Delay > 30 ms
Success off AADs:• 148/179 PaAF (83%)• 40/72 PeAF (55%)
Pappone, Circulation ‘01Pappone, Circulation ‘01

AuthorsAuthors Success rate w/o AADsSuccess rate w/o AADs
PapponePappone 83% FAP/75%FAC83% FAP/75%FACJACC 2003JACC 2003
StabileStabile 38% FAP/FAC38% FAP/FACCirculation Circulation 20032003HociniHocini 60% FAP*60% FAP*AbstractAbstract
OralOral 88% FAP (+ line)*88% FAP (+ line)*Circulation 2003Circulation 2003
* 8-20% incidence of LA flutter* 8-20% incidence of LA flutter
Anatomical Approach Anatomical Approach CLAACLAA

Challenge of CLAAChallenge of CLAA• Complete linear lesions are
analogous to surgical incisions
• They are challenging to achieve (with increased procedural risk)
• Incomplete linear lesions are pro-arrhythmic
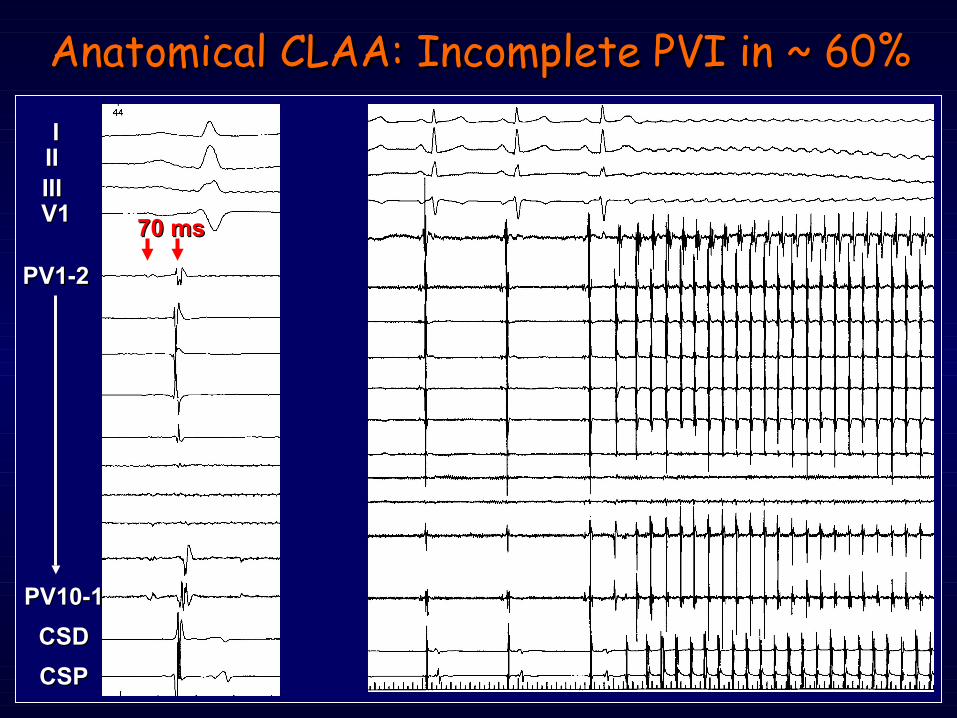
Anatomical CLAA: Incomplete PVI in ~ 60%Anatomical CLAA: Incomplete PVI in ~ 60%
70 ms70 ms
IIIIIIIIIIIIV1V1
PV1-2PV1-2
PV10-1PV10-1
CSDCSD
CSPCSP
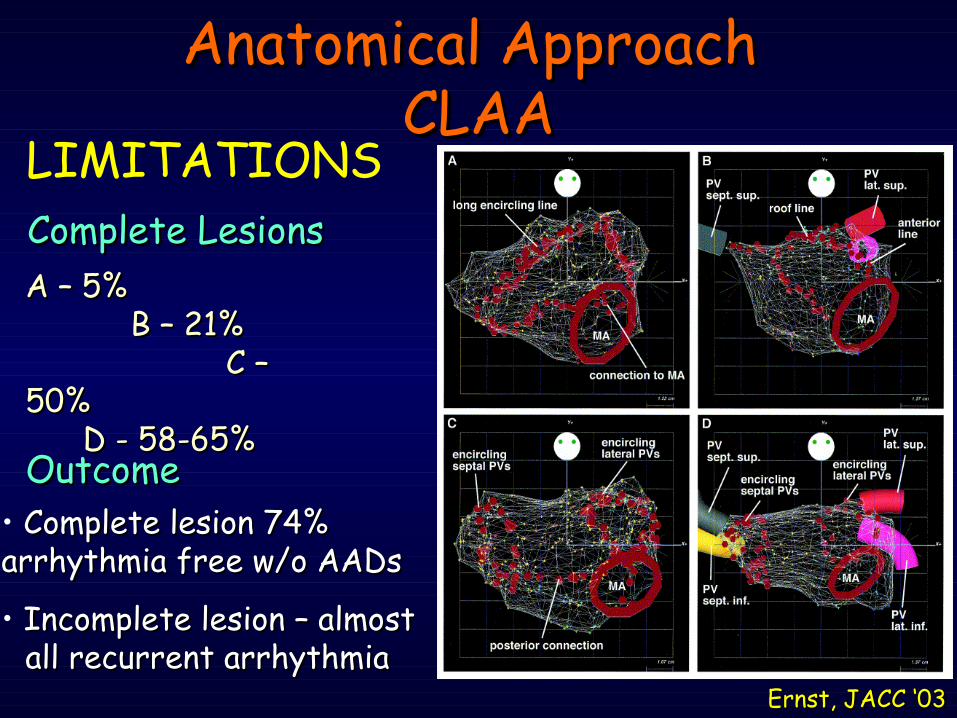
LIMITATIONS
Ernst, JACC ‘03Ernst, JACC ‘03
Complete LesionsComplete LesionsA – 5% A – 5% B – 21% B – 21% C – C – 50% 50% D - 58-65% D - 58-65%OutcomeOutcome
• Complete lesion 74% Complete lesion 74% arrhythmia free w/o AADsarrhythmia free w/o AADs
• Incomplete lesion – almost Incomplete lesion – almost all recurrent arrhythmiaall recurrent arrhythmia
Anatomical Approach Anatomical Approach CLAACLAA

How can we do a “ good mapping “ ? Importing the CT/MRI 3D Model
Digital Image Fusion
CT/MRI Scanner
DICOM 3 Slice Data
Worstation
Segmented 3D ModelSegmentation Module
User Interface

Virtual Reality Today
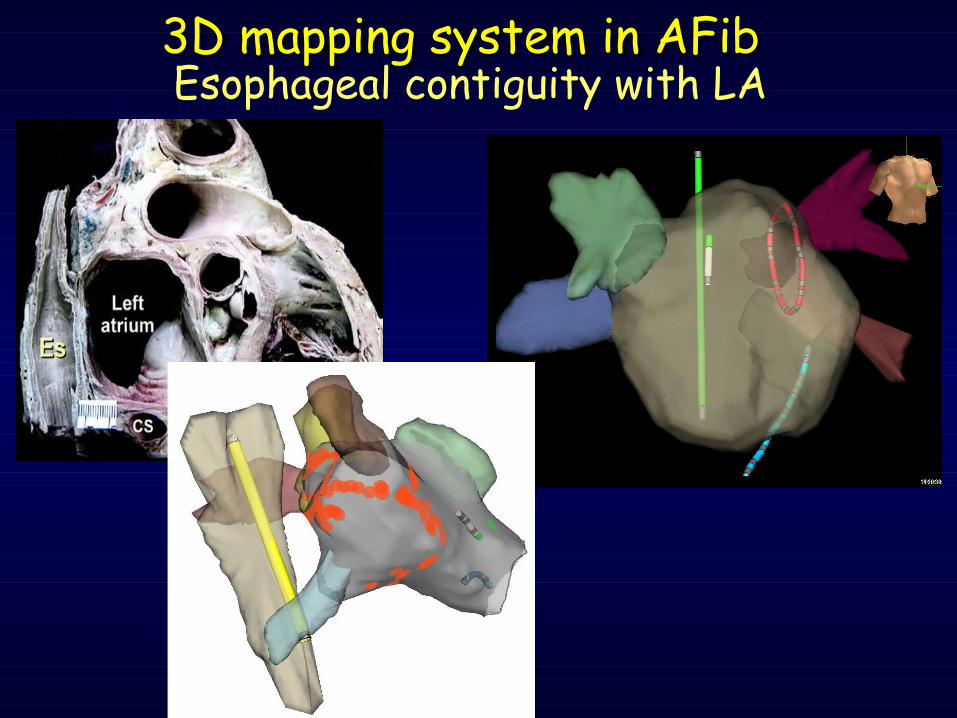
Esophageal contiguity with LA3D mapping system in AFib3D mapping system in AFib
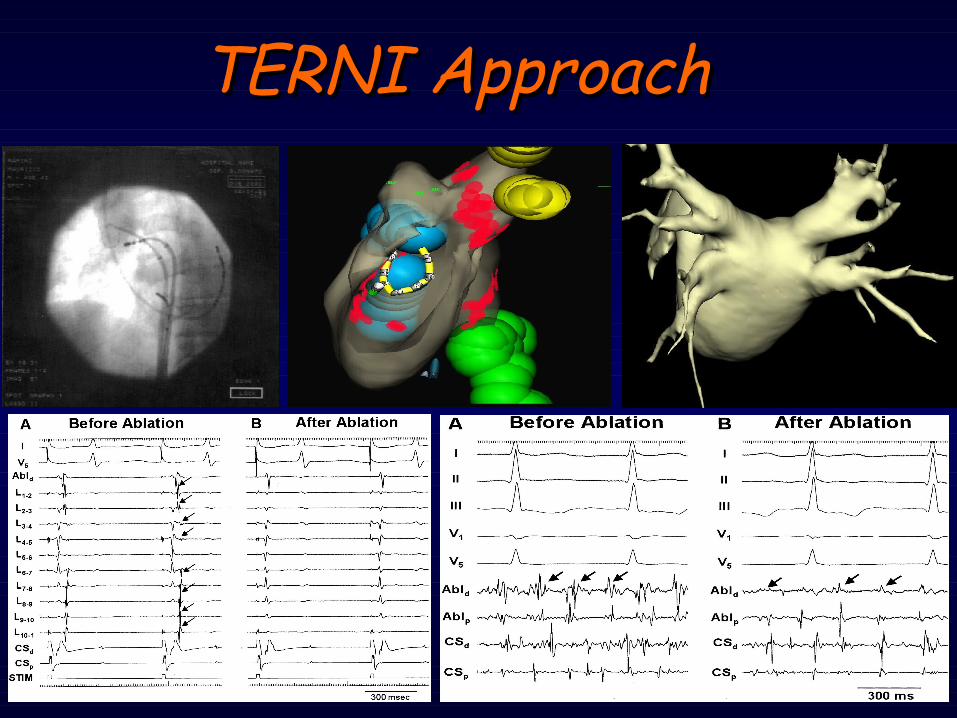
TERNI ApproachTERNI Approach

• 422 pts with symptomatic PaAF and PeAF referred to us between July ‘04 and September ’06. CA performed in 145/422 pts (34%).
TERNI RegistryTERNI Registry
• At least one MONTHLY episode of Persistent symptomatic AF
• At least ONE WEEKLY episode of PaAF or PeAF
• At least Two or More AADs unable to control symptoms
• Age >75 yrs• Contraindications to ACT• Congestive HF• NYHA class III or IV• LVEF ≤35% • LA diameter ≥55mm• CARDIAC THROMBUS• Life expectancy <1 yr• CCH surgery <3 mo or
PROSTHETIC valves
Inclusion criteriaInclusion criteria Exclusion criteriaExclusion criteria

Procedure (min): 148±26 144±24 151± 29
Fluoroscopy (min): 59±17 58±16 66±19
Mapping (min): 15±8 13±9 18±4
Nr. Pulses of RF: 62±16
60±17 65±19
RESULTSRESULTS Global Pz.in SR Pz. in AF
TERNI RegistryTERNI Registry
629 VP treated (145 pts)
Acute Complete BlockAcute Complete Block
558 VP (89%)558 VP (89%)
Incomplete BlockIncomplete Block
71 VP (11%)71 VP (11%)

• NO major complication (including death, stroke or other thromboembolic events) observed.
• MILD pericardial effusion observed in 4 pts.
• ANGIOGRAFIC analysis of all PVs performed post- procedure in all pts (no PV stenosis).
Clinical OUTCOME
TERNI RegistryTERNI Registry

• After a mean FU Overall FREEDOM FROM AF (both PaAF and PeAF) was 60% (69% and 48%), w/o AADs and 72% (80% and 55%) with previous ineffective AADs.
Clinical OUTCOMETERNI RegistryTERNI Registry
• Among UNIVARIATE predictors, LA size and structural HD, this approach revealed that an increased LA >50mm is anindipendet predictor of AF recurrence
87% success87% success
62% success62% success
Nardi S, PACE ‘’07 in Press

181/777 181/777 Laboratori in tutto il mondo Laboratori in tutto il mondo8.7458.745 pz da 90 Laboratori pz da 90 Laboratori10.19910.199 ATC x FA (90% in ASn) ATC x FA (90% in ASn)PERIODOPERIODO:: 1995 – 2002 1995 – 2002
Cappato R et al; Circulation 2004
Worldwide AFib SurveyWorldwide AFib Survey
Ablazione Transcatetere della Ablazione Transcatetere della FIBRILLAZIONE ATRIALEFIBRILLAZIONE ATRIALE

• In a broad spectrum of EP laboratories using different techniques over a wide time frame (7 yrs)
- free of AADs 48.0%- under AADs 24.1%
SUCCESS RATES
CLINICAL SUCCESS - Free of AADs: 3,866 (47,0%) - With AADss: 7,408 (79,0%)
LATE RECURRENCE
Cappato R, Circulation ‘04
Worldwide AFib SurveyWorldwide AFib Survey

Reant P, Circulation ‘05
Reverse Remodelling
• 48 pts with isolated AF • AADs ineffective• RFCA with PVI +
CT isthmus• Echo evaluation• 1 yr Follow up
78% PaAF 54% C-AF PROSPECTIVE DOUBLE BLINDED
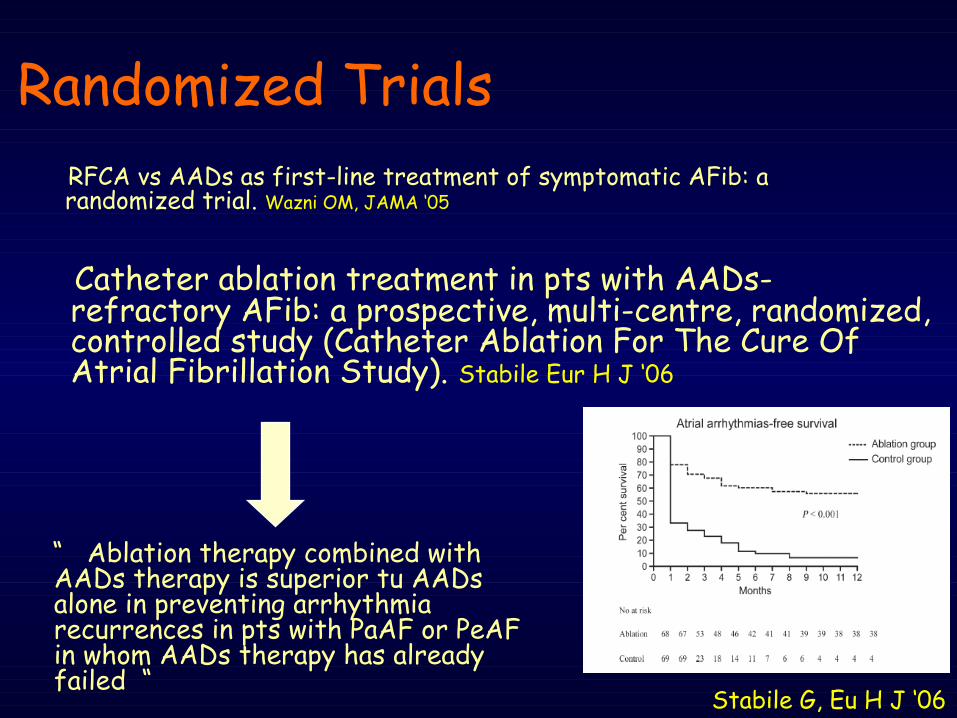
Randomized Trials
Catheter ablation treatment in pts with AADs- refractory AFib: a prospective, multi-centre, randomized, controlled study (Catheter Ablation For The Cure Of Atrial Fibrillation Study). Stabile Eur H J ‘06
RFCA vs AADs as first-line treatment of symptomatic AFib: a randomized trial. Wazni OM, JAMA ‘05
Stabile G, Eu H J ‘06
“ Ablation therapy combined with AADs therapy is superior tu AADs alone in preventing arrhythmia recurrences in pts with PaAF or PeAF in whom AADs therapy has already failed “

- Highly symptomatic AFib pts who refuse AADs.
When considered RFCA as When considered RFCA as 11stst line therapy in AFib ? line therapy in AFib ?
- When Amiodarone represent the only AAD of choice - In high risk pts for stroke who refuse or cannot take long term warfarin therapy (???) - Young pts with FAP and SND who may not tolerate AADs w/o a permanent pacemaker.

Only large and prospective or randomized clinical studies in comparison between RFCA of PV and alternative approach (rate CTR, AADs Rx for prevent AFib , Ablate and Pace etc) for Rhythm CTR and for Ventricular rate based strategies will give us the ANSEWERs our question on best treatment for AFib
Conclusions
What is success?
• Complete freedom of AF, off drug RX?
• No symptoms, but drug Rx required?
• Dramatic decrease in symptoms, but AADs still required?
• QoL
• How do we detect asymptomatic episodes?
• Anticoagulation ………………...?
QUESTIONSQUESTIONS