Fibrillazione Atriale Non Valvolare Ischemia o Emorragia ... · Gianluca Botto, MD, FESC, UO...
46
Gianluca Botto, MD, FESC, UO Elettrofisiologia, Dip Medicina Fibrillazione Atriale Non Valvolare Ischemia o Emorragia le Due Utopie Rivali nella Scelta dei NAO
Transcript of Fibrillazione Atriale Non Valvolare Ischemia o Emorragia ... · Gianluca Botto, MD, FESC, UO...

Gianluca Botto, MD, FESC,UO Elettrofisiologia, Dip Medicina
Fibrillazione Atriale Non
Valvolare Ischemia o Emorragia le
Due Utopie Rivali nella Scelta dei
NAO
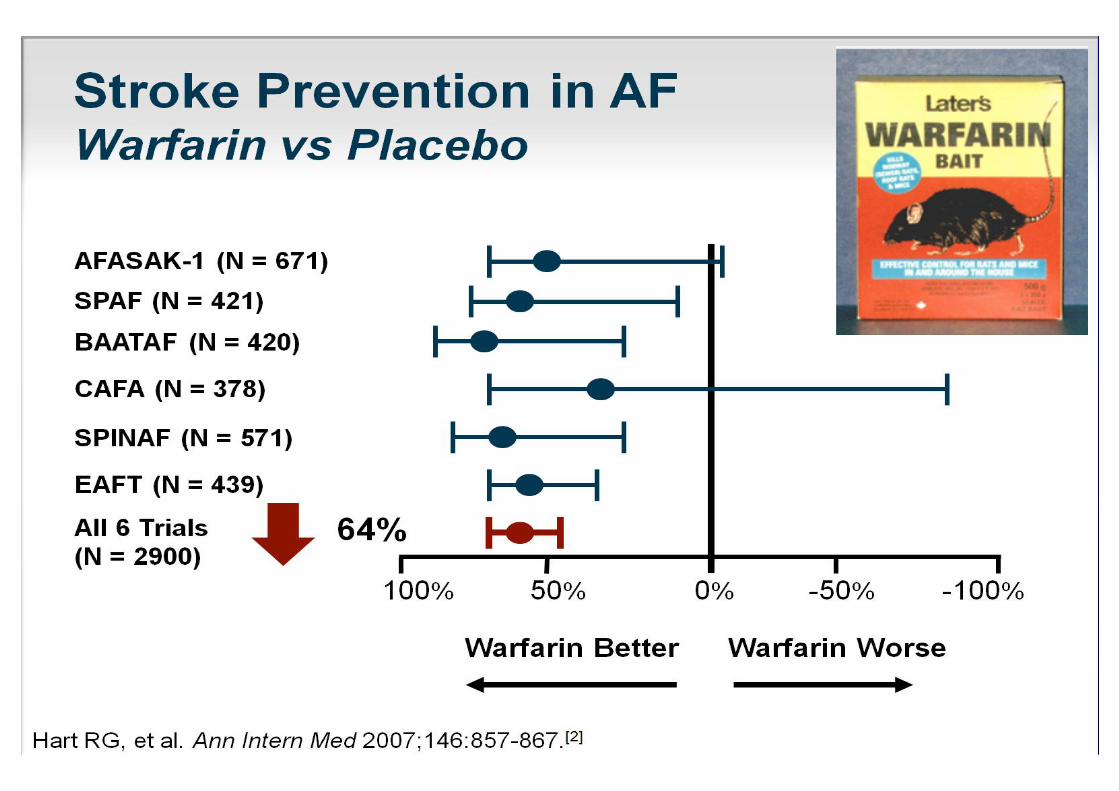
Limitations of VKA TherapyLimitations of VKA Therapy
Routine coagulationmonitoring
Slow onset/offset of action
Warfarin resistance
Numerous drug–druginteractions
Numerous food–druginteractions
Narrow therapeuticwindow (INR range 2.0–3.0)
Ansell J. Chest 2008; 133; 160S-198S.
Umer Ushman MH. J Interv Card Electrophysiol 2008; 22: 129-137.
Nutescu EA. Cardiol Clin 2008; 26: 169-187.
VKA therapy has several limitations that make it difficult to use
in practice
Frequent doseadjustments
Unpredictableresponse
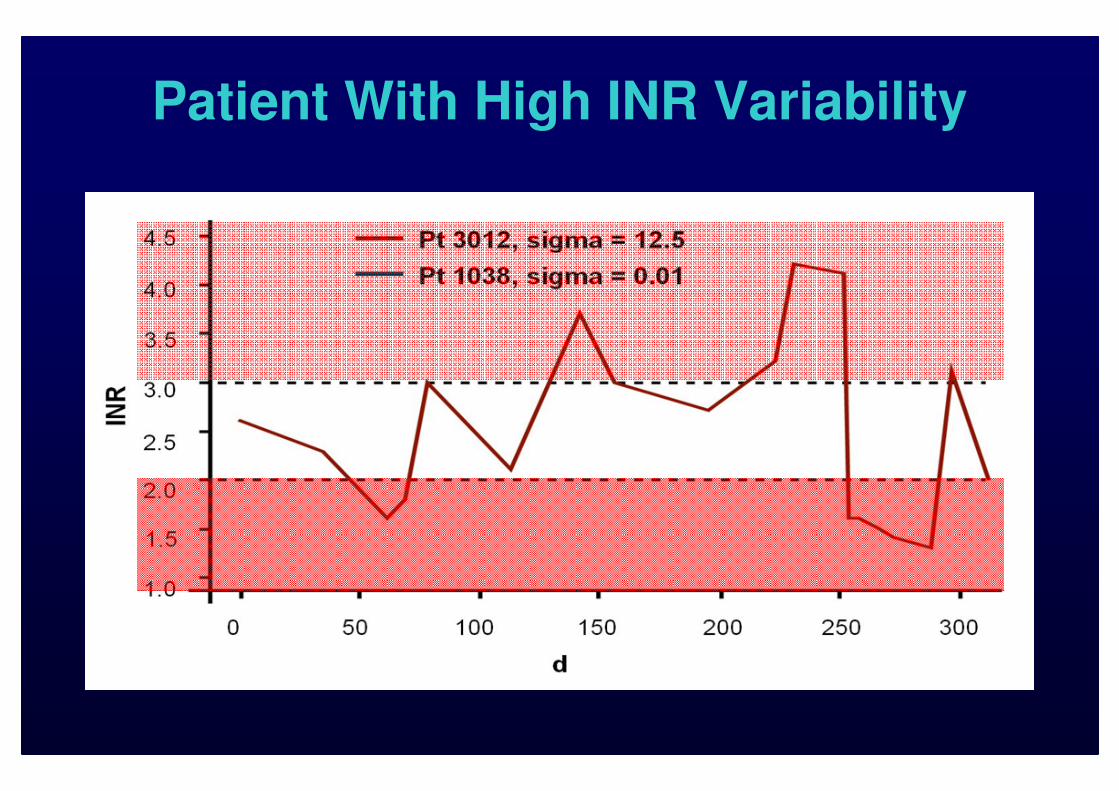
Patient With High INR Variability
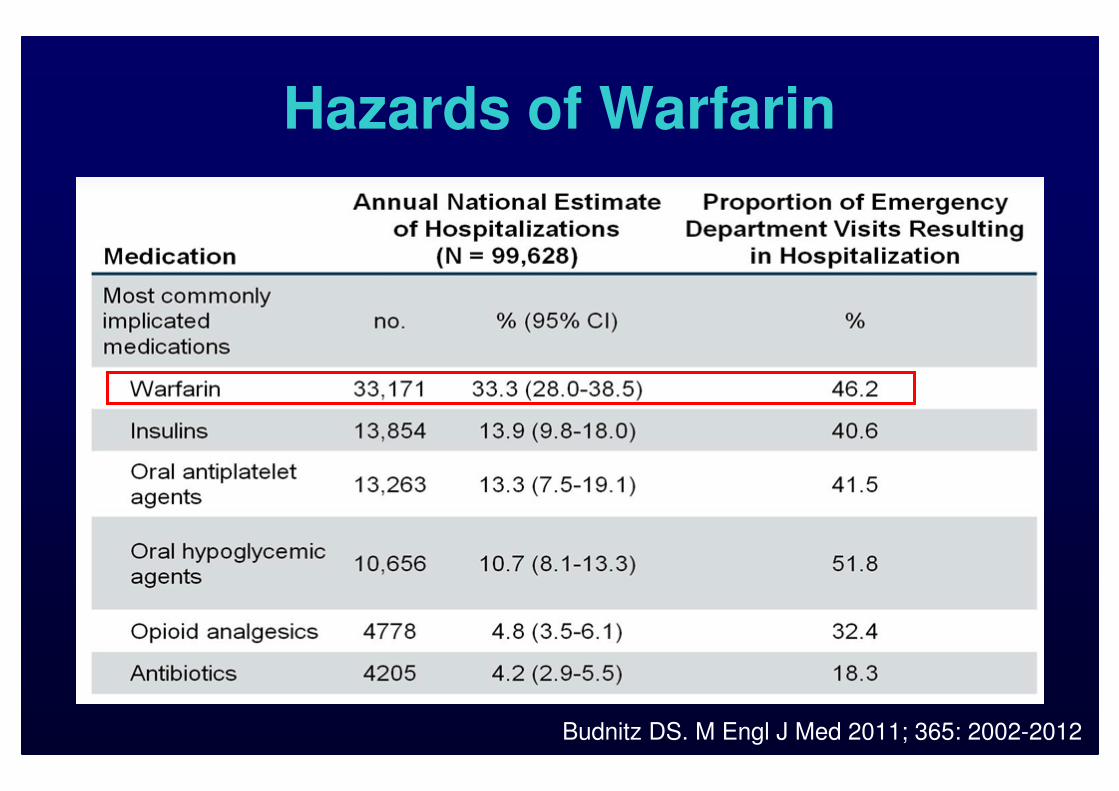
Hazards of Warfarin
Budnitz DS. M Engl J Med 2011; 365: 2002-2012
Rationale of a Replacement for
Warfarin in NV-AF
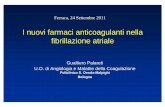
■ W is an effective agent for stroke prevention in NV-AF, however:
■ Pts find frequent INR monitoring difficult
■ Phisicians are reluctant to use W due to the increased risk for bleeds
■ The potential for improvement in bleeding and possibly stroke prevention was seen with more targeted NOAC therapy
Selecting the most appropriate
antithrombotic therapy for
a pt is one of the most important
management decisions in AFIB
The net clinical benefit associated
with a given therapeutic choice
should guide this decision.
The net clinical benefit
associated with a given therapeutic choice
should guide this decision.
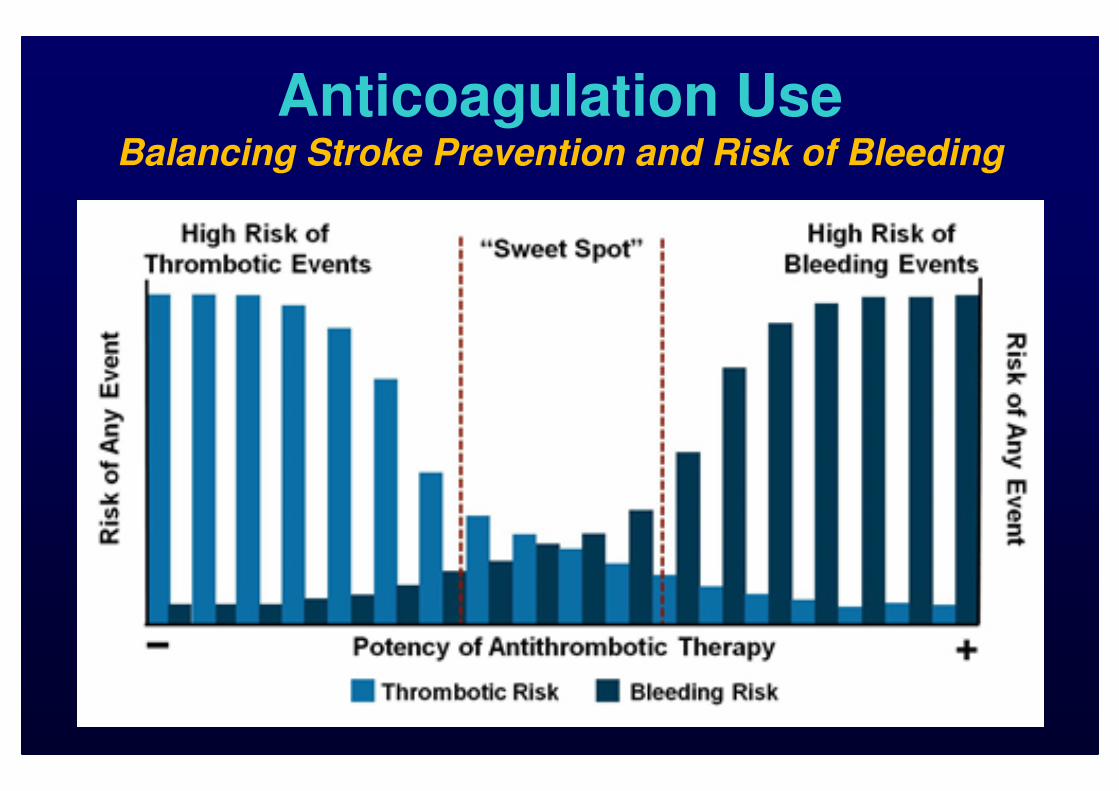
Anticoagulation UseBalancing Stroke Prevention and Risk of Bleeding
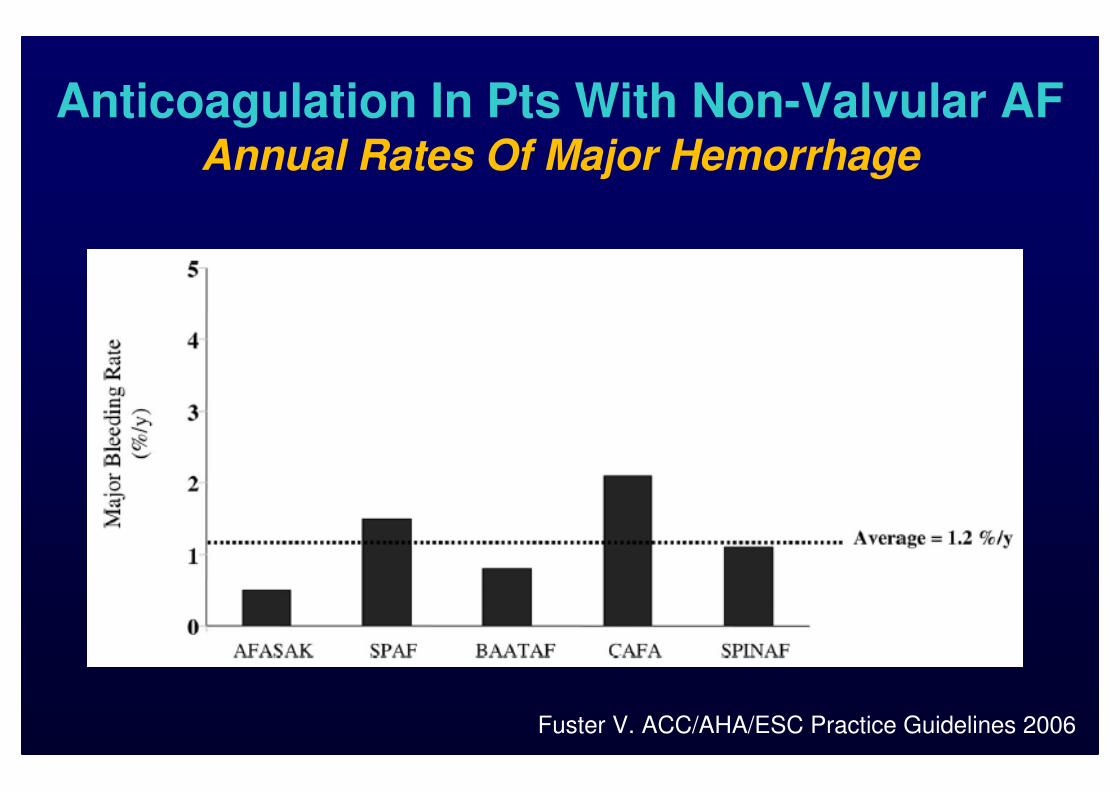
Anticoagulation In Pts With Non-Valvular AFAnnual Rates Of Major Hemorrhage
Fuster V. ACC/AHA/ESC Practice Guidelines 2006
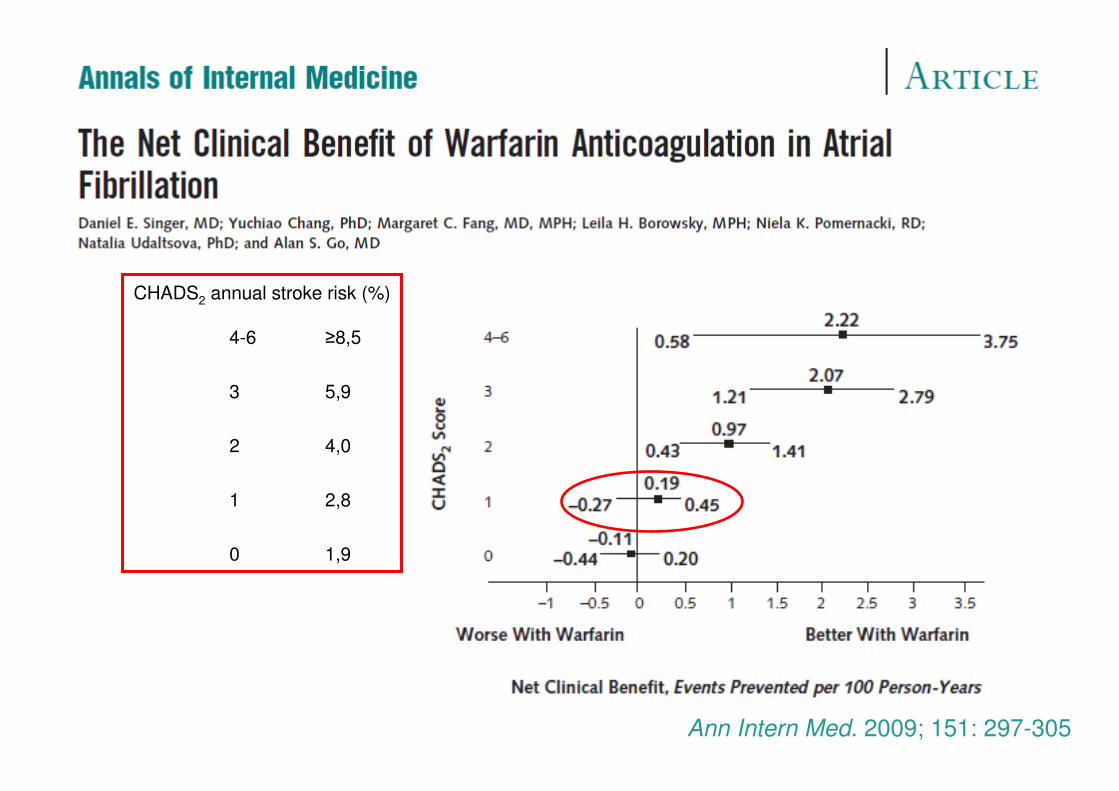
Ann Intern Med. 2009; 151: 297-305.
CHADS2 annual stroke risk (%)
4-6 ≥8,5
3 5,9
2 4,0
1 2,8
0 1,9

AVERROESPrimary Efficacy and Safety Outcome
AVERROESPrimary Efficacy and Safety Outcome
Connolly SJ. N Engl J Med 2011; 364: 806-17
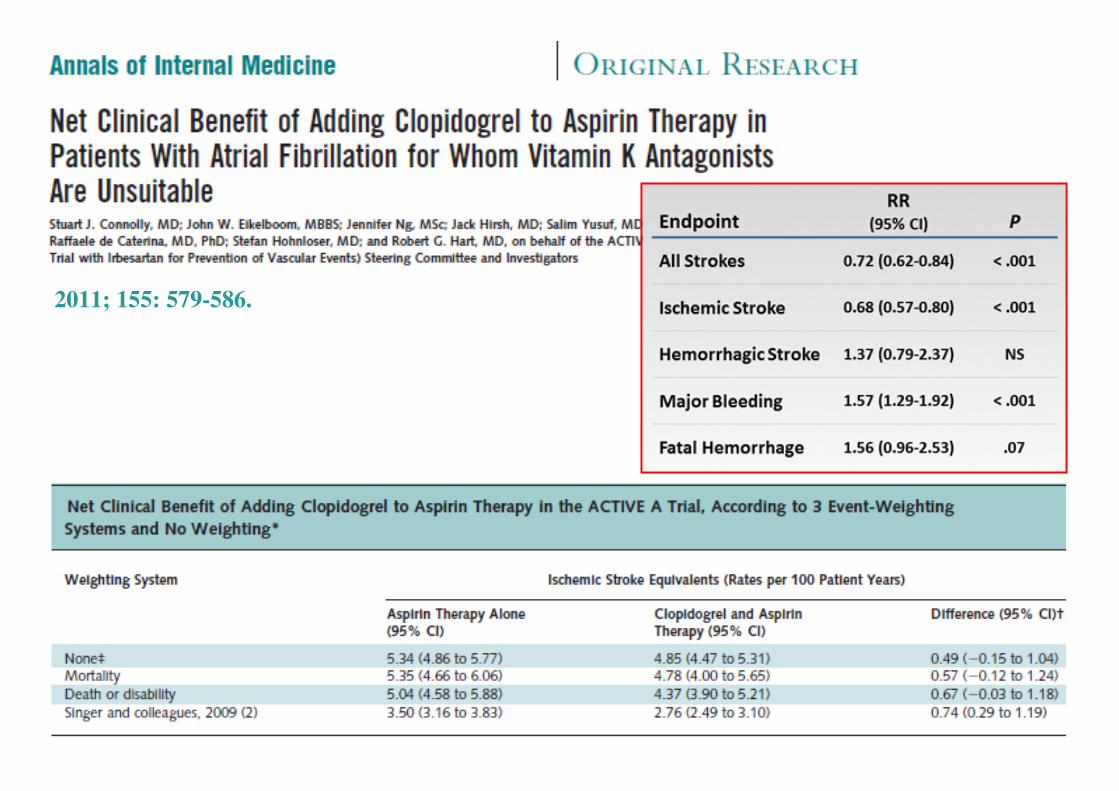
2011; 155: 579-586.
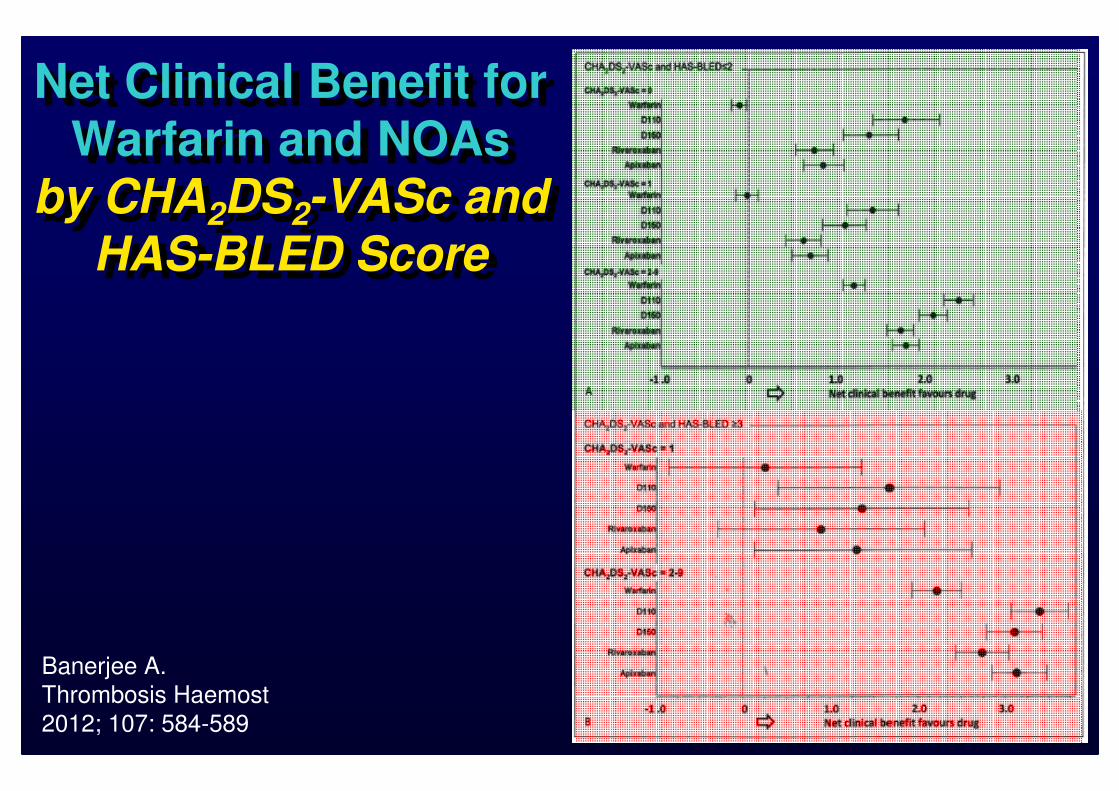
Net Clinical Benefit for
Warfarin and NOAs by CHA2DS2-VASc and
HAS-BLED Score
Net Clinical Benefit for
Warfarin and NOAs
by CHA2DS2-VASc and HAS-BLED Score
Banerjee A.
Thrombosis Haemost
2012; 107: 584-589
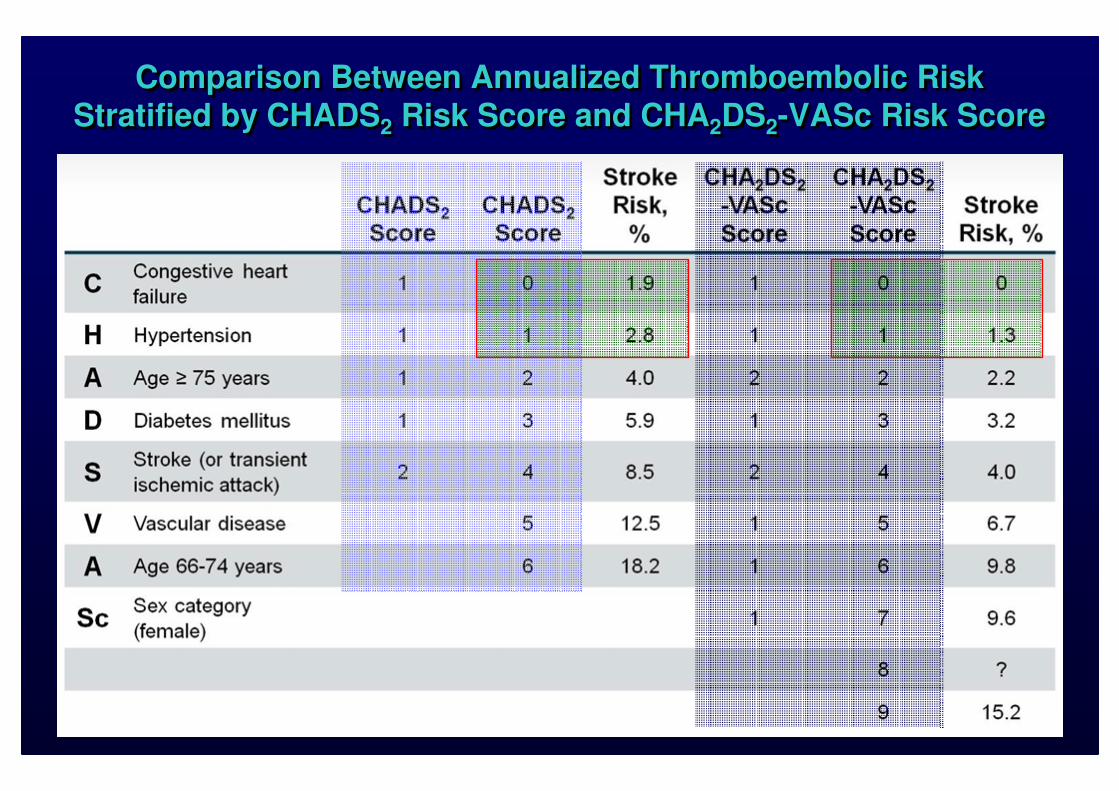
Comparison Between Annualized Thromboembolic Risk Stratified by CHADS2 Risk Score and CHA2DS2-VASc Risk Score
Comparison Between Annualized Thromboembolic Risk Stratified by CHADS2 Risk Score and CHA2DS2-VASc Risk Score
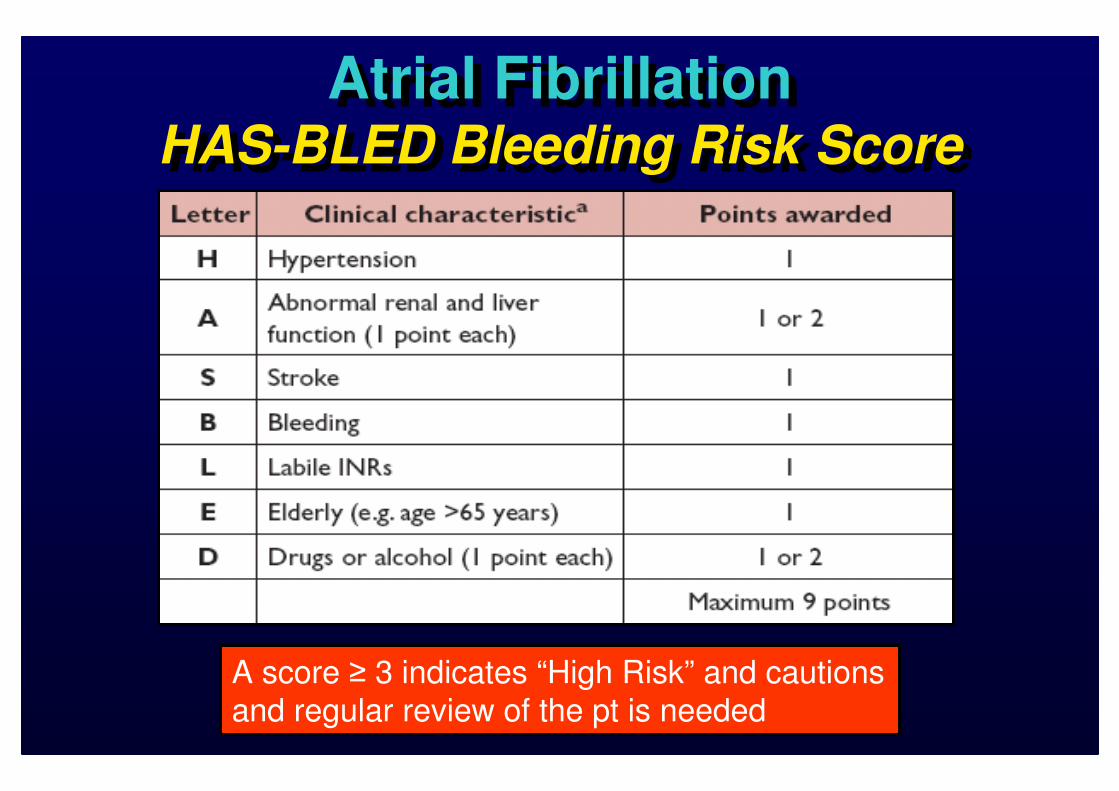
Atrial FibrillationHAS-BLED Bleeding Risk Score
Atrial FibrillationHAS-BLED Bleeding Risk Score
A score ≥ 3 indicates “High Risk” and cautions and regular review of the pt is needed
Although Stroke Is Generally
More Feared By Patients, There Is A Strong Bias
Among Physician Not To Cause Harm
Although Stroke Is Generally
More Feared By Patients, There Is A Strong Bias
Among Physician Not To Cause Harm
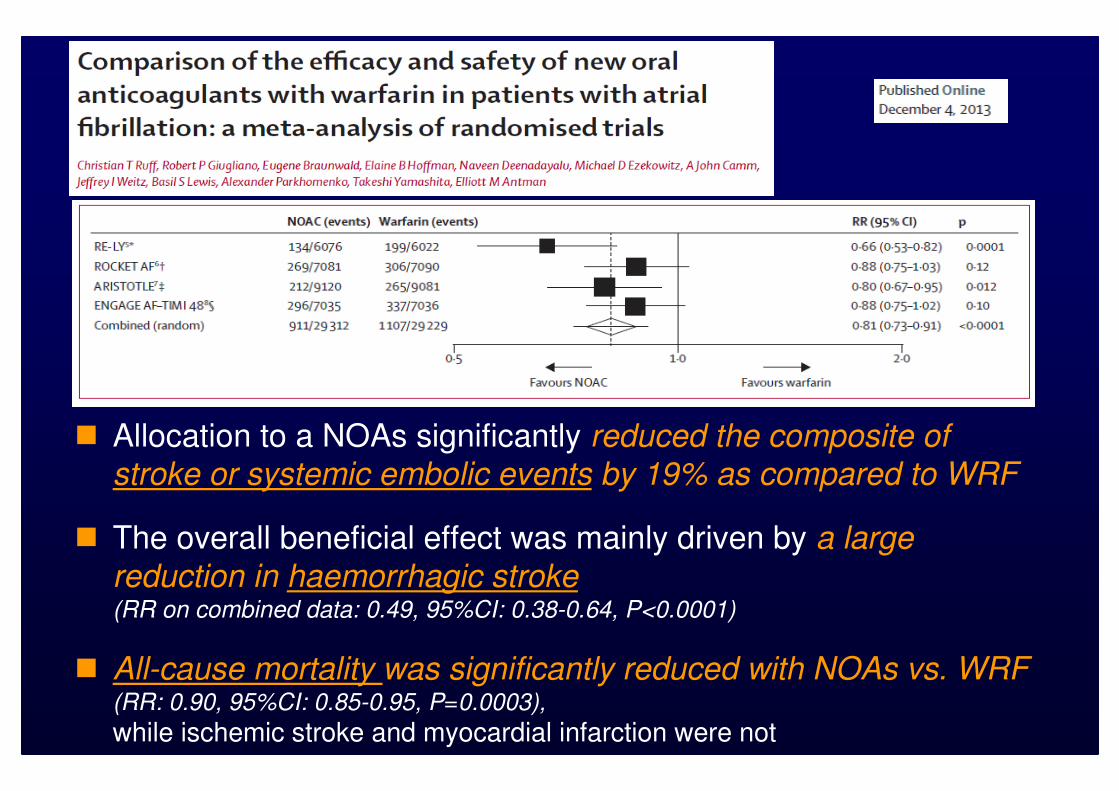
� Allocation to a NOAs significantly reduced the composite of stroke or systemic embolic events by 19% as compared to WRF
� The overall beneficial effect was mainly driven by a large
reduction in haemorrhagic stroke(RR on combined data: 0.49, 95%CI: 0.38-0.64, P<0.0001)
� All-cause mortality was significantly reduced with NOAs vs. WRF (RR: 0.90, 95%CI: 0.85-0.95, P=0.0003),
while ischemic stroke and myocardial infarction were not
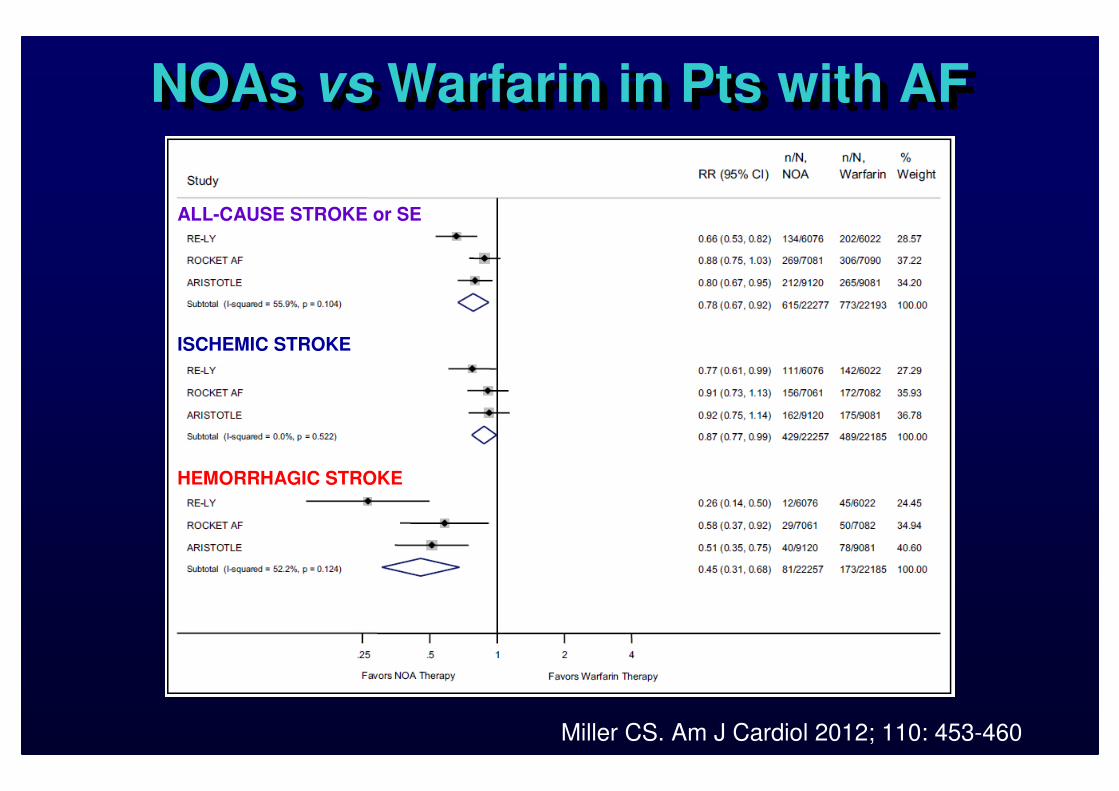
NOAs vs Warfarin in Pts with AFNOAs vs Warfarin in Pts with AF
Miller CS. Am J Cardiol 2012; 110: 453-460
ALL-CAUSE STROKE or SE
ISCHEMIC STROKE
HEMORRHAGIC STROKE
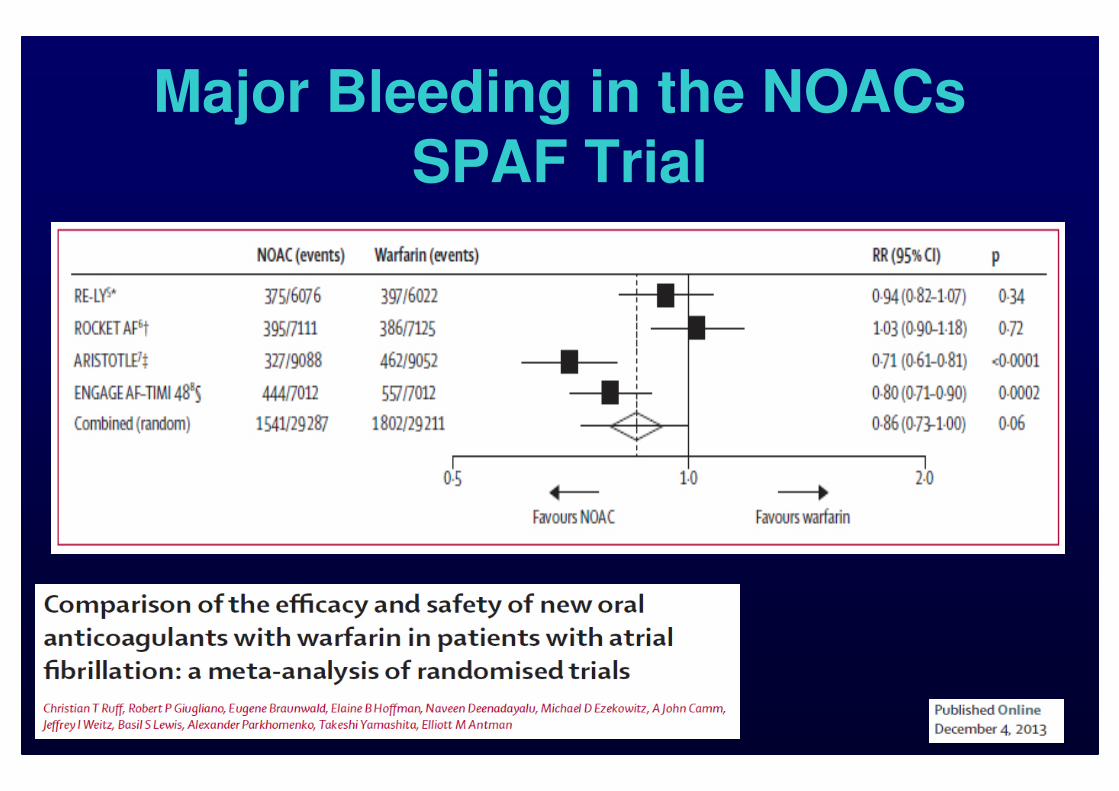
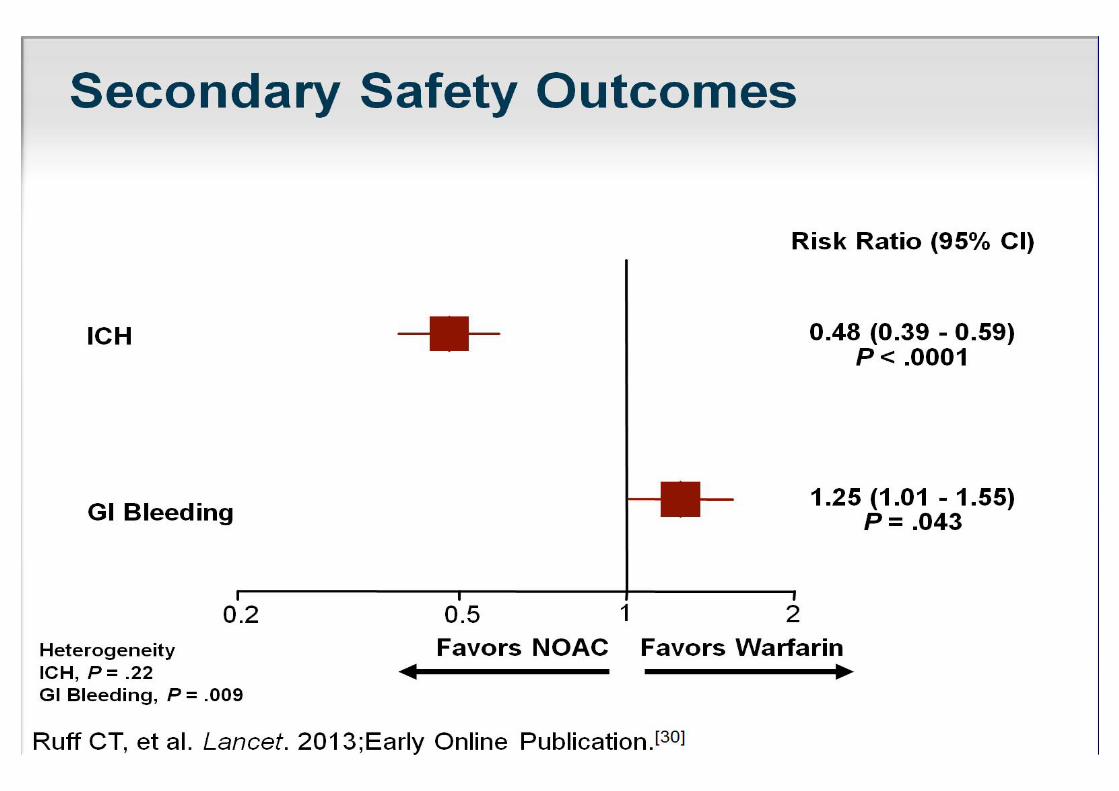
Major Bleeding in the NOACs SPAF Trial
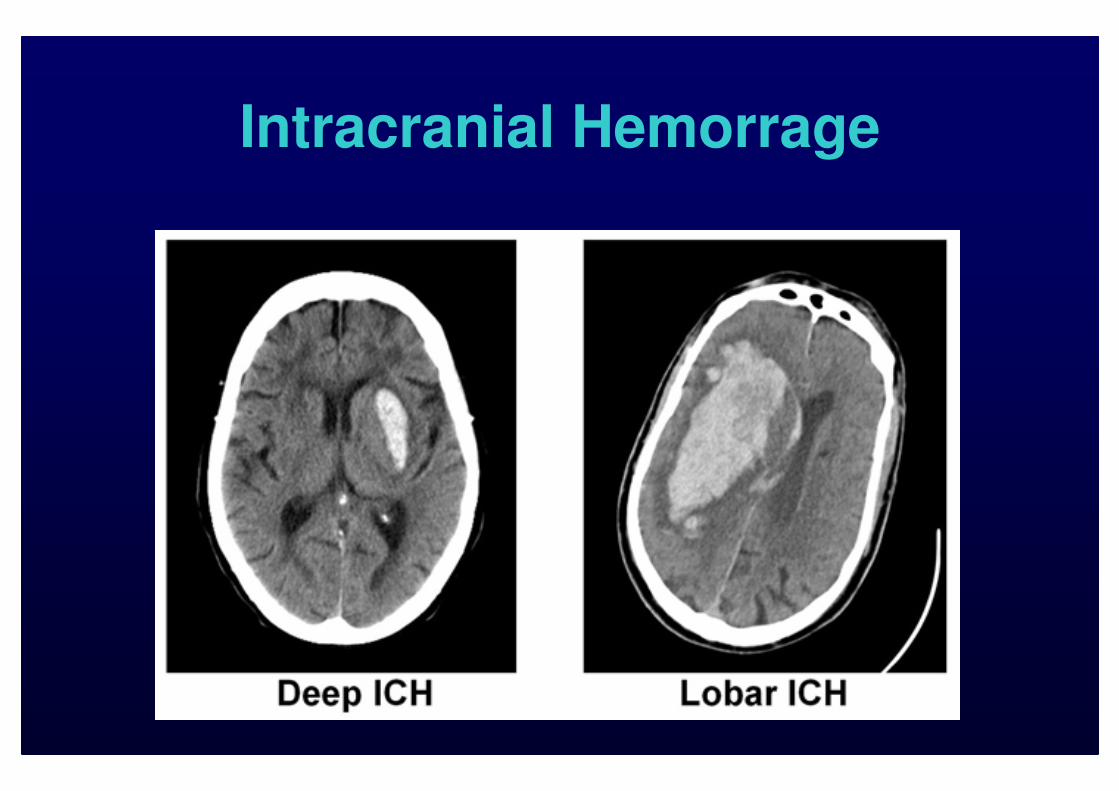
Intracranial Hemorrage
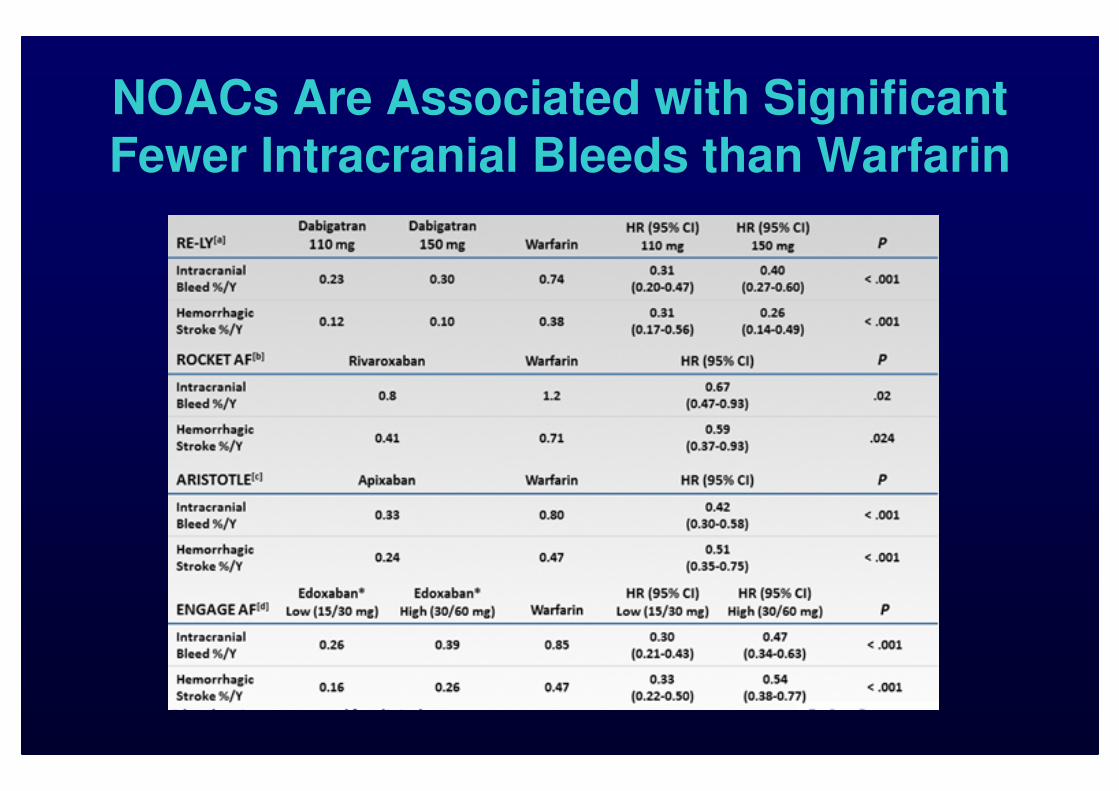
NOACs Are Associated with Significant
Fewer Intracranial Bleeds than Warfarin
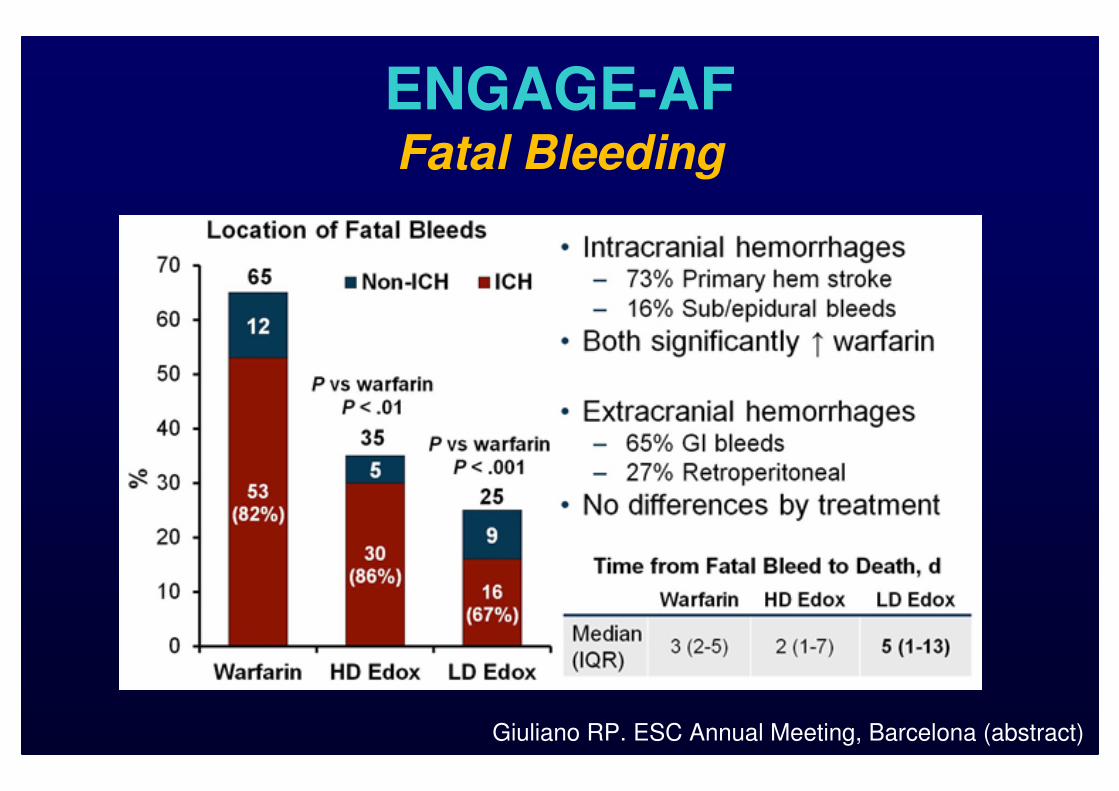
ENGAGE-AFFatal Bleeding
Giuliano RP. ESC Annual Meeting, Barcelona (abstract)
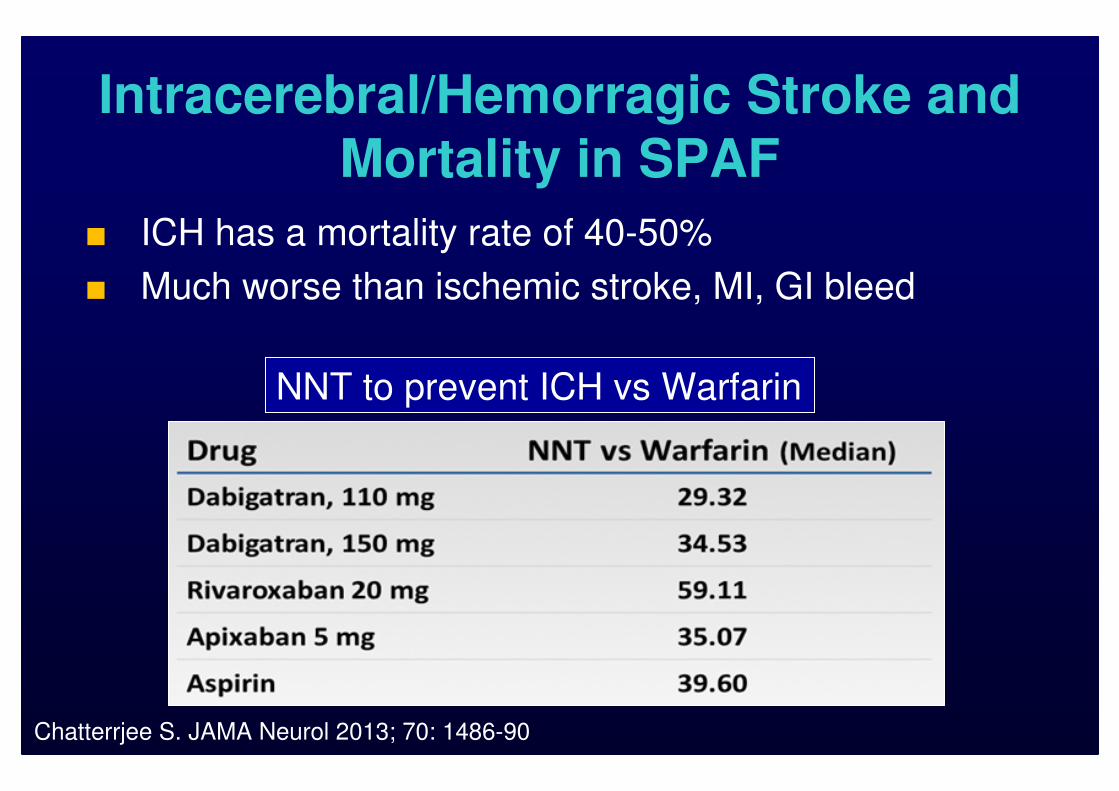
Intracerebral/Hemorragic Stroke and
Mortality in SPAF
■ ICH has a mortality rate of 40-50%
■ Much worse than ischemic stroke, MI, GI bleed
Chatterrjee S. JAMA Neurol 2013; 70: 1486-90
NNT to prevent ICH vs Warfarin
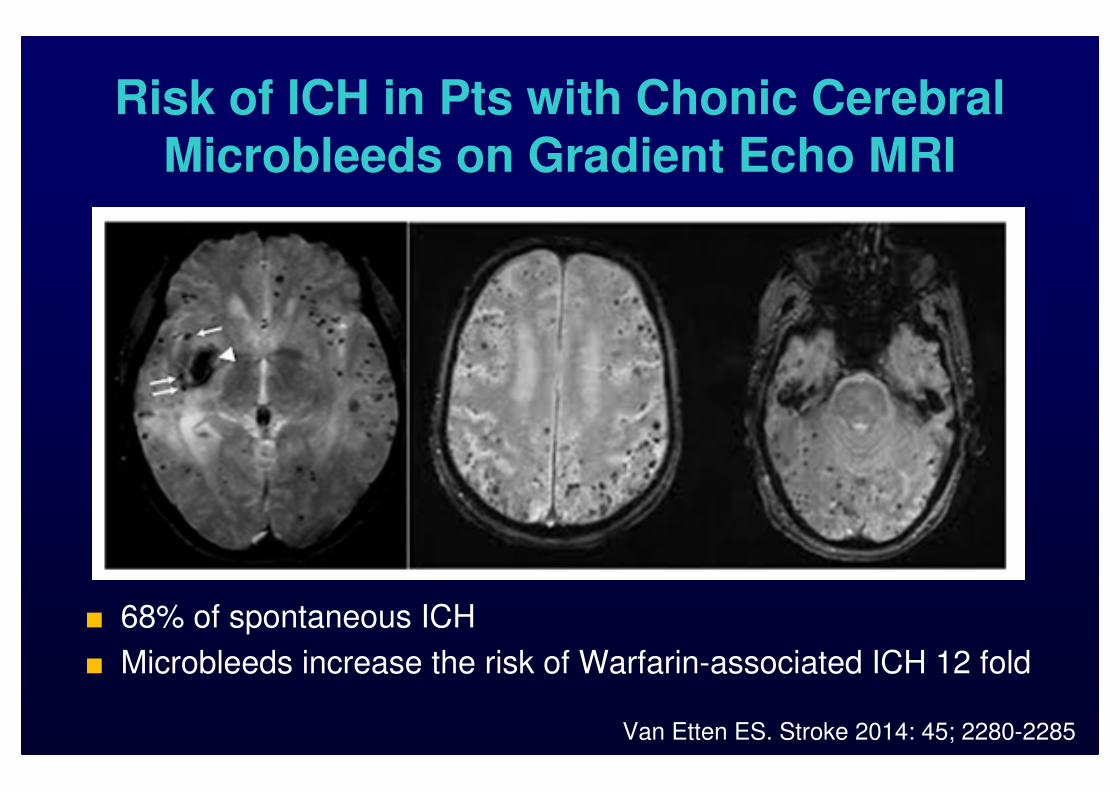
Risk of ICH in Pts with Chonic Cerebral
Microbleeds on Gradient Echo MRI
■ 68% of spontaneous ICH
■ Microbleeds increase the risk of Warfarin-associated ICH 12 fold
Van Etten ES. Stroke 2014: 45; 2280-2285
Reducing the Risk for ICH in SPAF
Pts Receiving Anticoagulation Rx
■ Assesses risk factors
■ Aggressive risk factor reduction
■ Do not add AP to anticoagulant unless pts has recently had a coronary stent deployed
■ Switch from an AVK to a NAOC
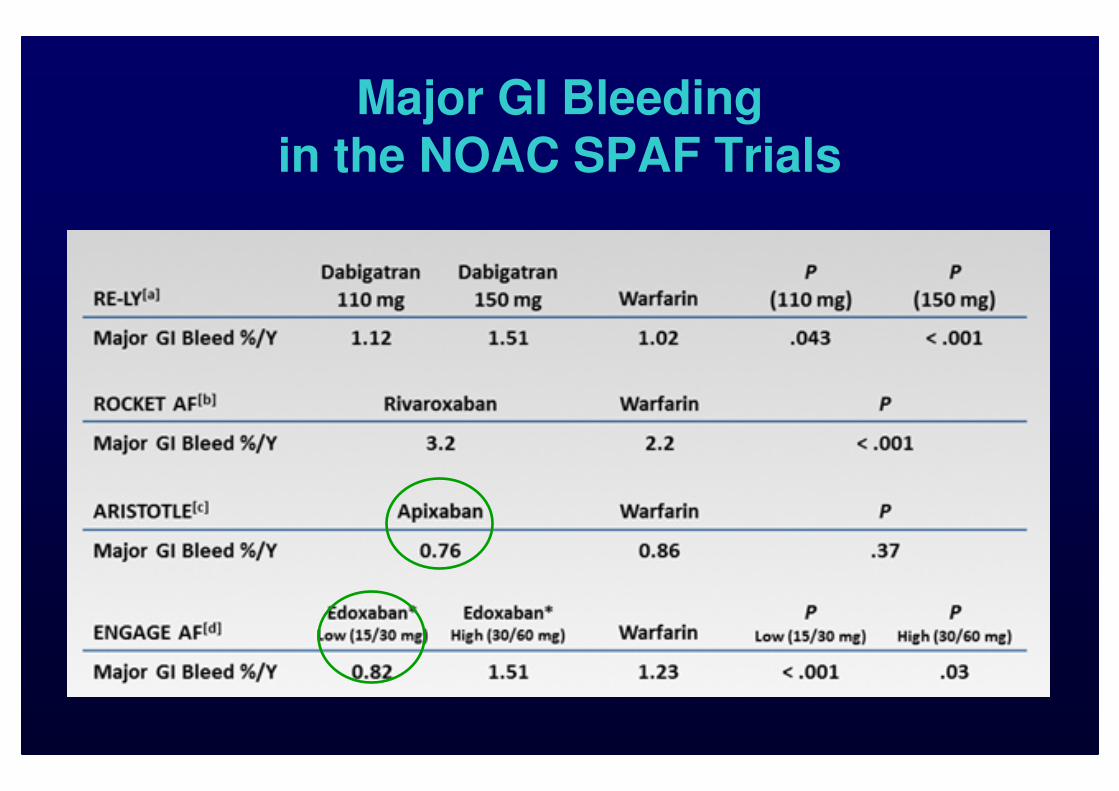
Major GI Bleeding
in the NOAC SPAF Trials
Flexible Dosing to Prevent Bleeding
■ High vs low-dose regimens- more ischemic events but less bleeding
■ Dose modification/reduction- preventing excess dose exposure in
vulnerable pts
■ Once-daly vs twice-daily dosing- different plasma concentration carries
differen bleeding risk
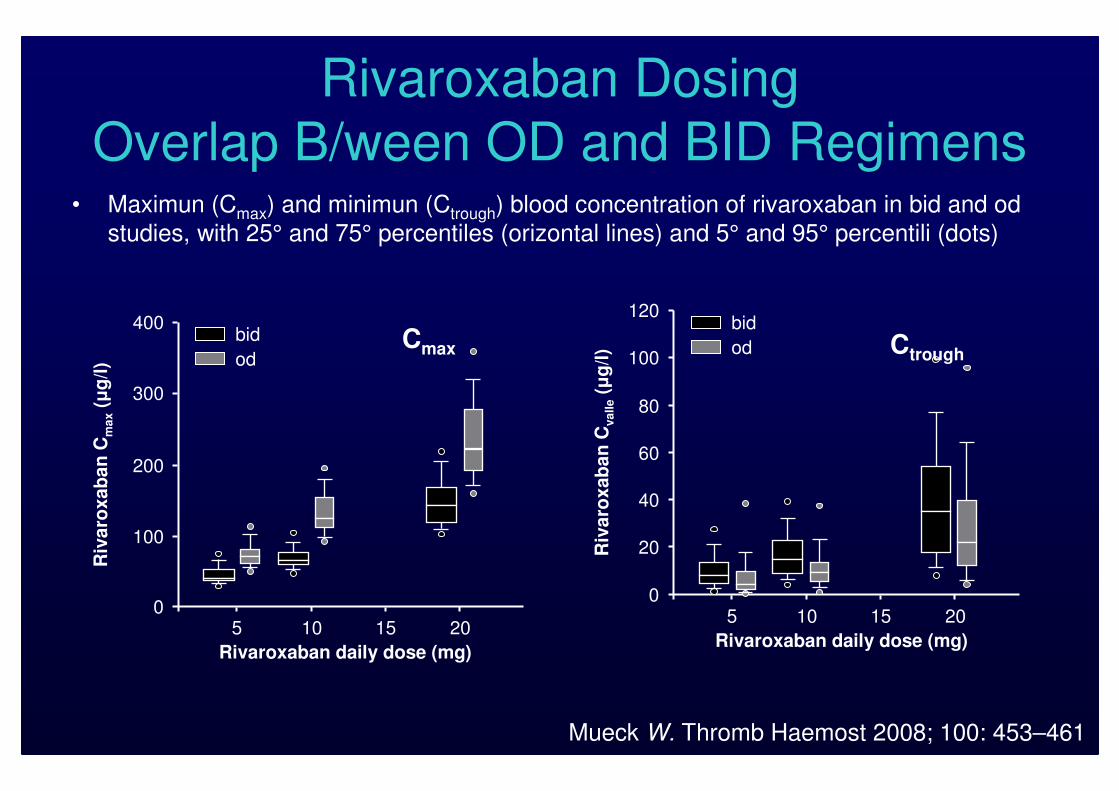
Rivaroxaban Dosing
Overlap B/ween OD and BID Regimens• Maximun (Cmax) and minimun (Ctrough) blood concentration of rivaroxaban in bid and od
studies, with 25° and 75° percentiles (orizontal lines) and 5° and 95° percentili (dots)
100
200
300
400
05 10 15 20
Rivaroxaban daily dose (mg)
Riv
aro
xab
an
Cm
ax
(µg
/l)
bid
od
5 10 15 20
120
100
80
60
40
20
0
Rivaroxaban daily dose (mg)
Riv
aro
xab
an
Cva
lle
(µg
/l)
bid
odCmax Ctrough
Mueck W. Thromb Haemost 2008; 100: 453–461
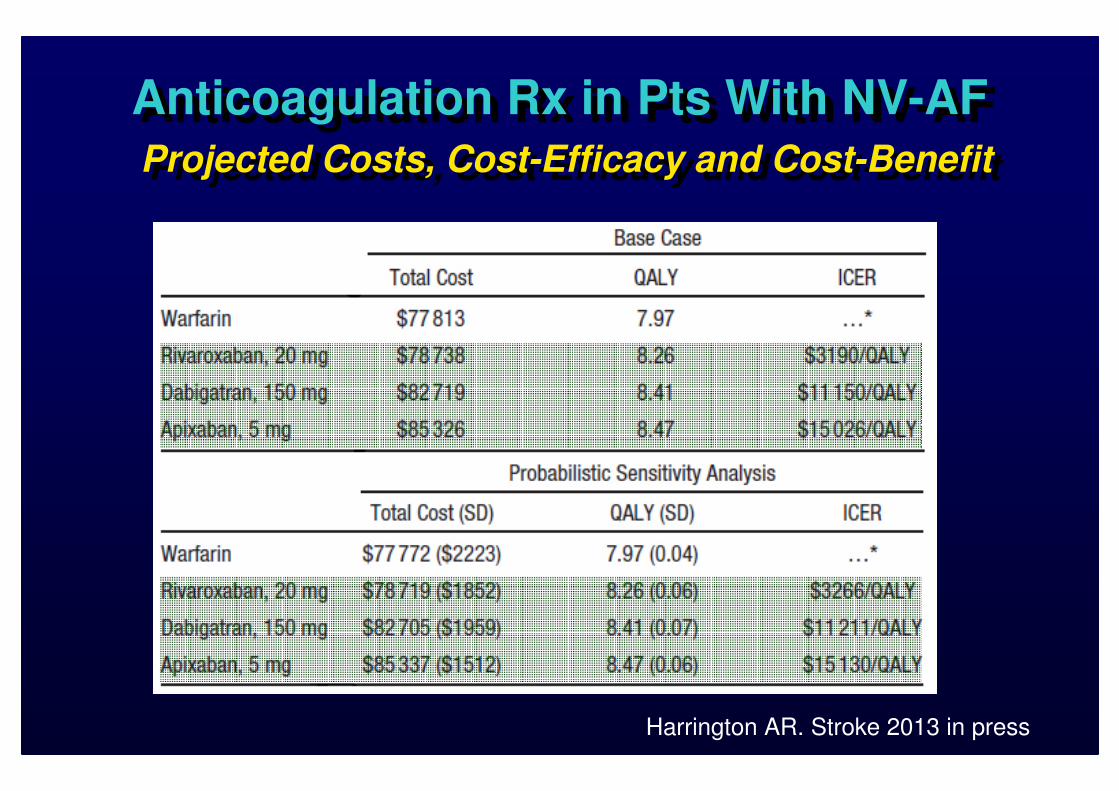
Anticoagulation Rx in Pts With NV-AF
Projected Costs, Cost-Efficacy and Cost-Benefit
Anticoagulation Rx in Pts With NV-AF
Projected Costs, Cost-Efficacy and Cost-Benefit
Harrington AR. Stroke 2013 in press
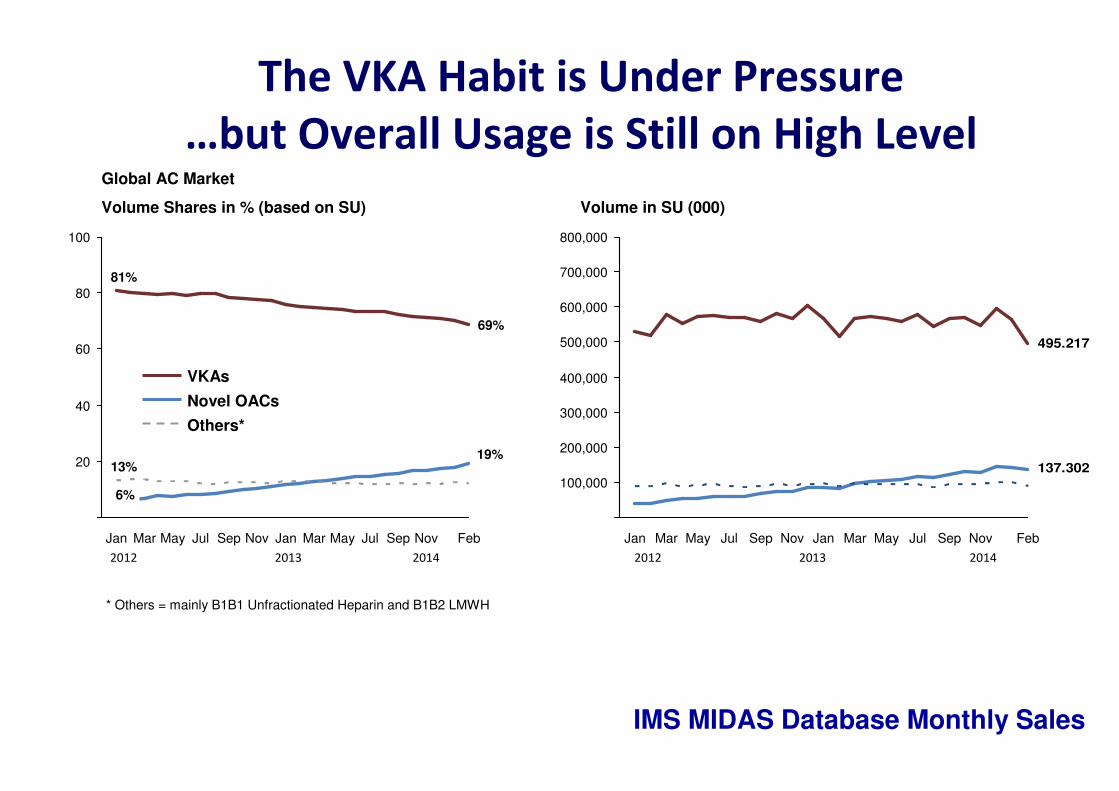
The VKA Habit is Under Pressure
…but Overall Usage is Still on High Level
100
80
60
40
20
Feb
69%
NovSepJulMayMarJanNovSepJulMayMarJan
13%
6%
81%
19%
Others*
Novel OACs
VKAs
Global AC Market
Volume Shares in % (based on SU) Volume in SU (000)
495.217
137.302
800,000
700,000
600,000
500,000
400,000
300,000
200,000
100,000
FebNovSepJulMayMarJanNovSepJulMayMarJan
2012 2013 2014 2012 2013 2014
* Others = mainly B1B1 Unfractionated Heparin and B1B2 LMWH
IMS MIDAS Database Monthly Sales
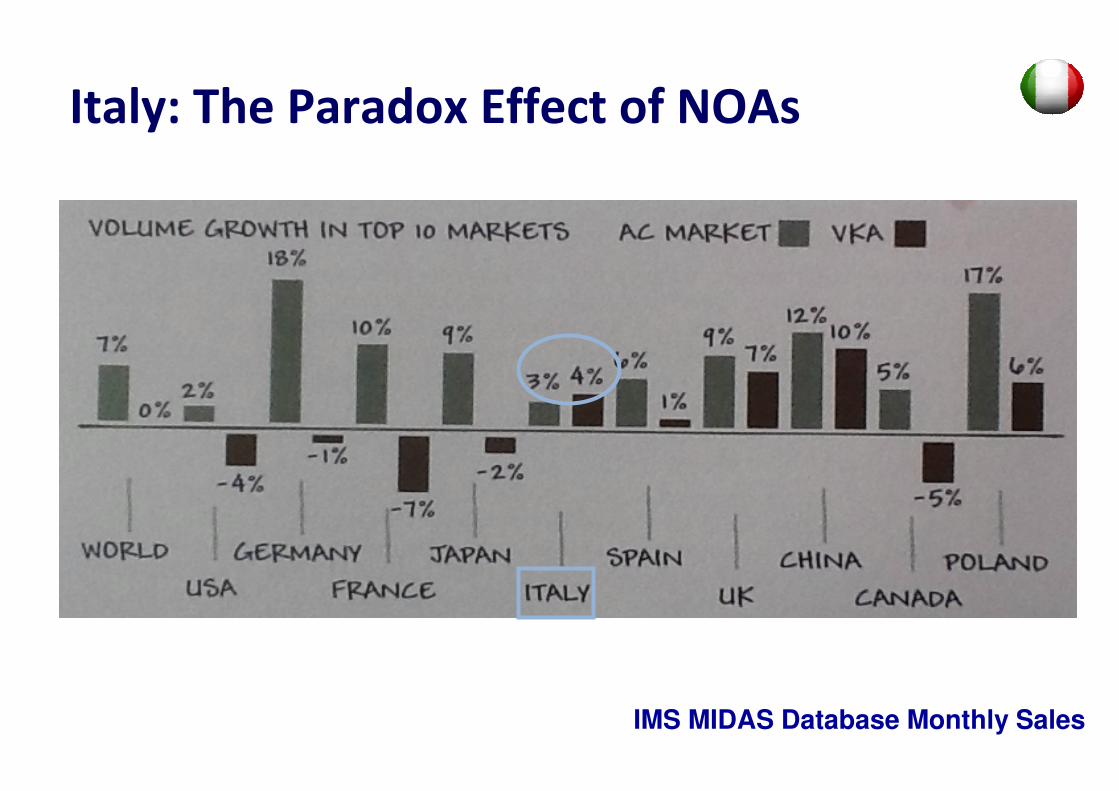
Italy: The Paradox Effect of NOAs
IMS MIDAS Database Monthly Sales
Summary
■ Appropriate AC is required to prevent TE events in pts with NV-AF while minimizing the risk for bleeding
■ NOACs provide a similar level of protection from ischemic stroke as VKAs but are associated with a significant lower rate of intracranial bleeding
■ NOACs are powerful drugs, can cause serious bleeding and should be used in strict accordance with their specific scientific evidence
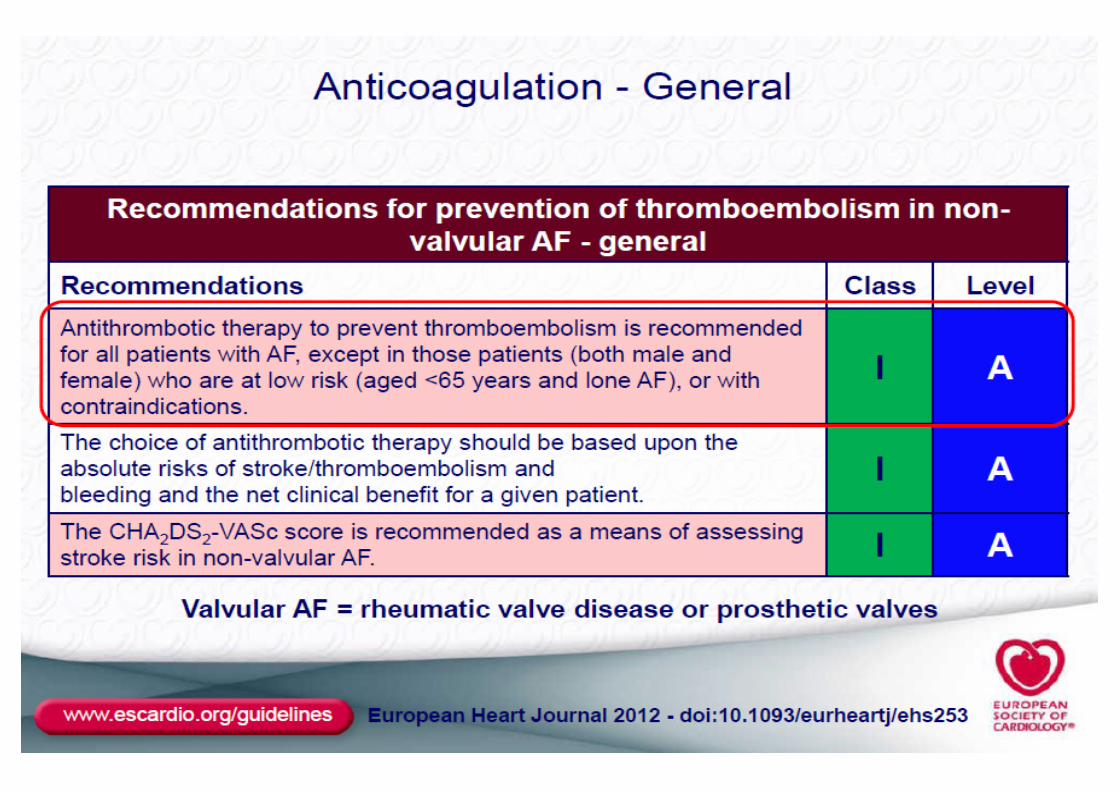
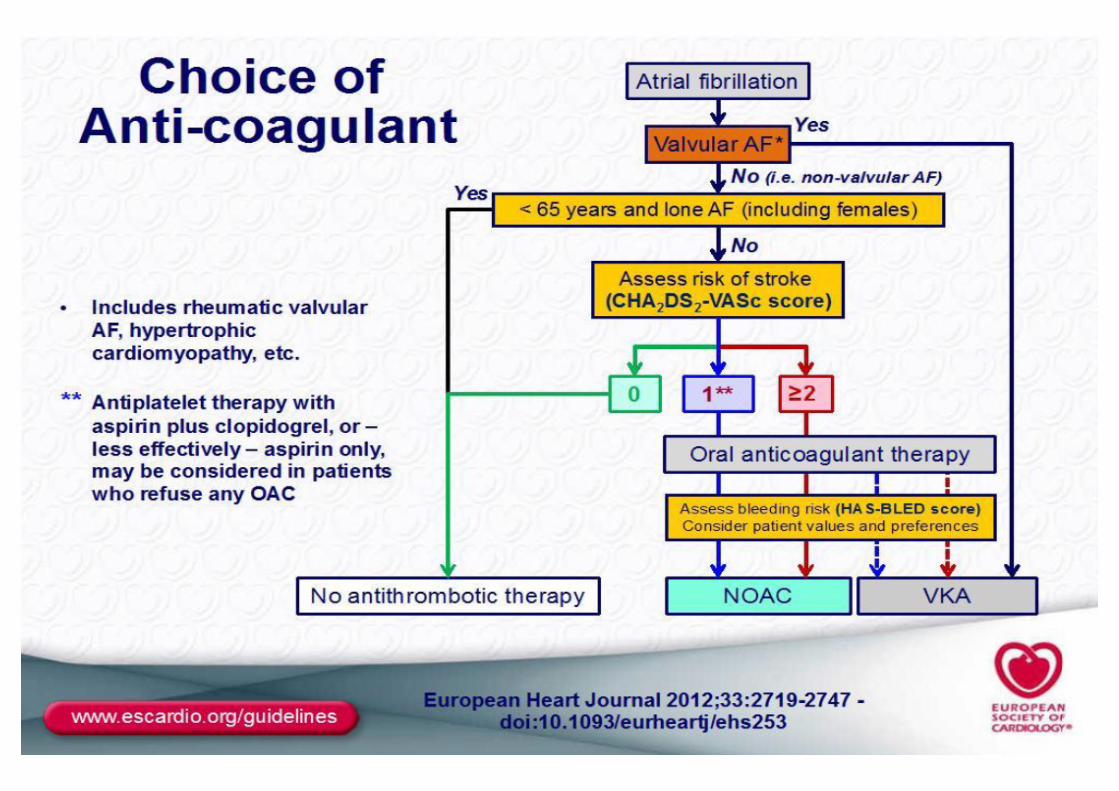
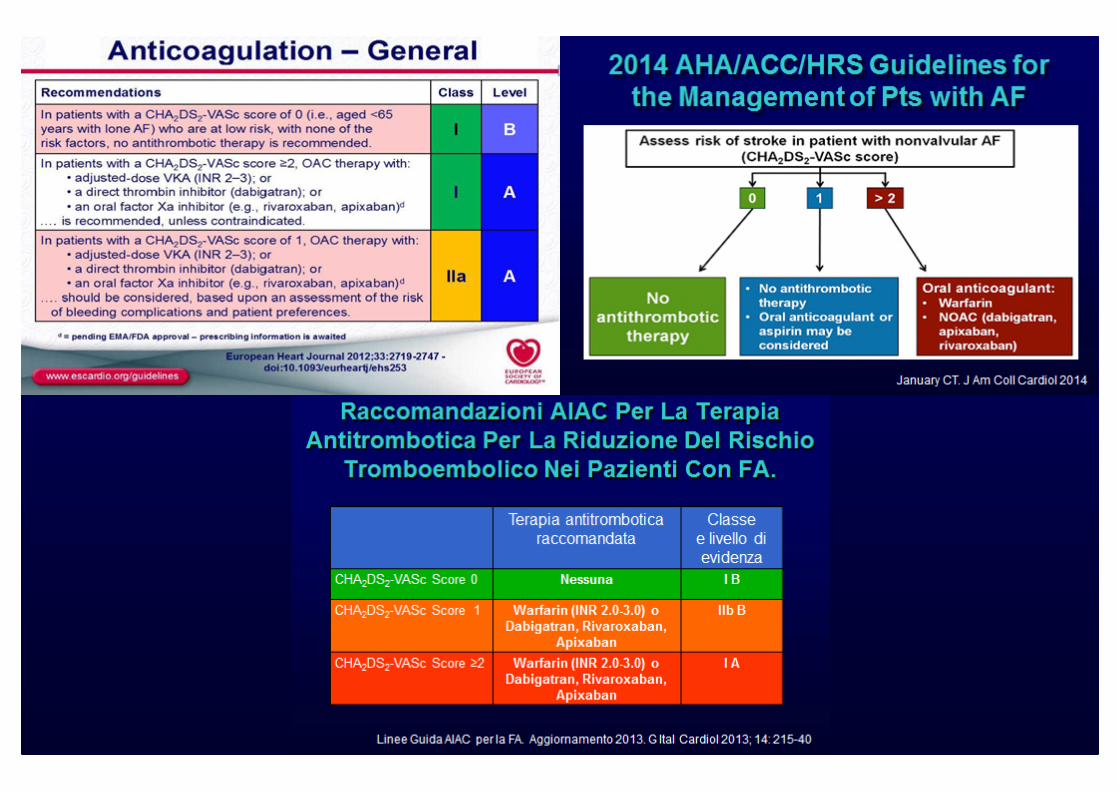
New Guidelines for Anticoagulation of Pts With AF
New Guidelines for Anticoagulation of Pts With AF
� Particular emphasis on identification of pts at low risk that don’t need any antithrombotic Rx
� ASA just for few pts for whom anticoagulation cannot be proposed
� NOAs significantly reduce the major bleedingPrimarily driven by a substantial reduction in ICH
� NOAs are poised to replace warfarin for the majority of the pts