2006 cortona, congresso tosco umbro. ablazione ne i trattamento ablativo della fibrillazione...
45
S. Nardi, MD Lab. Elettrofisiologia – Div. di Cardiologia Azienda Ospedale S. Maria - TERNI I congresso TOSCO-UMBRO “La Cardiologia che vorremmo” 22-23 Novembre, 2006 – Cortona azione nella rillazione Atriale: cazioni e strategie farmacologiche
-
Upload
centro-diagnostico-nardi -
Category
Health & Medicine
-
view
74 -
download
0
Transcript of 2006 cortona, congresso tosco umbro. ablazione ne i trattamento ablativo della fibrillazione...

S. Nardi, MDLab. Elettrofisiologia – Div. di
Cardiologia
Azienda Ospedale S. Maria - TERNI
I congresso TOSCO-UMBRO“La Cardiologia che vorremmo”22-23 Novembre, 2006 – Cortona
Ablazione nella Fibrillazione Atriale:indicazioni e strategie farmacologiche

AF
CURE Clinical Control
AFib rate controlSR restore
Clinical Control
paroxistic permanentpersistent
Therapeutic OptionsINTRODUTION

Considerations• All AFib affected patients have an increased
Morbidity• The overall increased Mortality is between 1,6-
2,6% (Manitoba and Framingham Studies) • 5% year ischemic stroke (non-rheumatic AF) 2-
7 times without AF • 1/6 Cerebro-Vascular Accident (CVA) occurs in
AFib • Framingham Study
- RHD 17 X rate of CVA (age-matched CTR)- Attributable risk 5 X > non-RHD- Risk of Stroke increased with age
(1,5% at 50-59 yrs vs 23,5% at 80-89 yrs)

AADs SUCCESS %
propafenone (e.v.)propafenone (os)flecainide (e.v.)flecainide (os)amiodarone (e.v.)ibutilide (ev)dofetilide (e.v.)dofetilide (os)
29-9172
57-5978
34-9234-47
3132
Acute efficacy
Antiarrhythmic drugs (AADs)

Quinidine 1 yr 3fold increase mortalityDrug Efficacy F.U. Drawbacks
50% SR
AuthorCoplen, ‘90
Dysopiramide 1 yr Many side effects, 11% drop out
As quinidine Karlson ‘88
Flecainide 1 yr Not indicated in CAD49% SR Van Gelder, ‘89
Propafenone 6 mo Not indicated in CAD60% SR Stroobandt, ‘97
Amiodarone 1 yr Side effects61% SR Gosselink, ‘92
Pooled (meta-analysis) data

AFFIRM
STAFSTAF
PIAPIAFF
HOT CAFÉHOT CAFÉ
PAF-PAF-22
RACRACEE
Randomized TRIALS
• Paroxysmal Atrial Fibirllation 2 (PAF2) Eur Heart J ’02
• Pharmacological Intervention in AF (PIAF) Lancet ’00.
• Comparison of rate control and rhythm control in pts with AF (AFFIRM) NEJM ‘02.
• Randomized trial of rate-control versus rhythm CTR in PeAF: the Strategies of Treatment of AF (STAF) study. JACC ‘03.
• Effect of rate or rhythm control on QoL in PeAF: results from the Rate Control Versus Electrical Cardioversion (RACE) Study. JACC ‘ 04.
• How to treat C-AF (HOT-CAFÉ`) New New DehliDehli

- Strategies based to maintaining SR at 1 yrs FU without AADs is <30% (recurrence between 50-70%) ....
Pooled (meta-analysis) data from PAF2, PIAF, STAF, AFFIRM e RACE
- … however in most cases AADs based strategies are not able to prevent RECURRENCE of A Fib.
• Global efficacy 40 - 50% (Reduce in long term FU)
25% interruption of treatment !
• SIDE EFFECTS– Until 20% of cases (3-5% TdP)

• Arrhythmia-free survival after ECV in pts with PeAF
Lower Curve Outcome after a single shock when no prophylactic AADs was givenUpper curve Outcome with repeated ECV in conjunction with AADs prophylaxis
Pooled (meta-analysis) data from PAF2, PIAF, STAF, AFFIRM e RACE

INIZIATORI(TRIGGER)
PERPETUATORI(multiple wavelet reentry)
SUBSTRATE(regione antrale)
• Attività extrasistolica
• Attività ripetitiva (FOCALE e NON FOCALE)
ELECTROPHYSIOLOGICMECHANISMS

RFFiriing or spontaneous diastolic depolarisation
Haissaguerre ’96 Chen ’97
Triggers

• Origin from a velry limited area
• Localized in the media of PVs prevalently or in other areas (SVC, IVC, atrial myocardial wall)
• Abolished with small lesion size (~ 150 mm³)
FOCAL ACTIVITYFOCAL ACTIVITY
It’s enought to explain the evolution from PaAF to
PeAF ?
ELECTROPHYSIOLOGICMECHANISMS
Haissaguerre ’96 Chen ’97
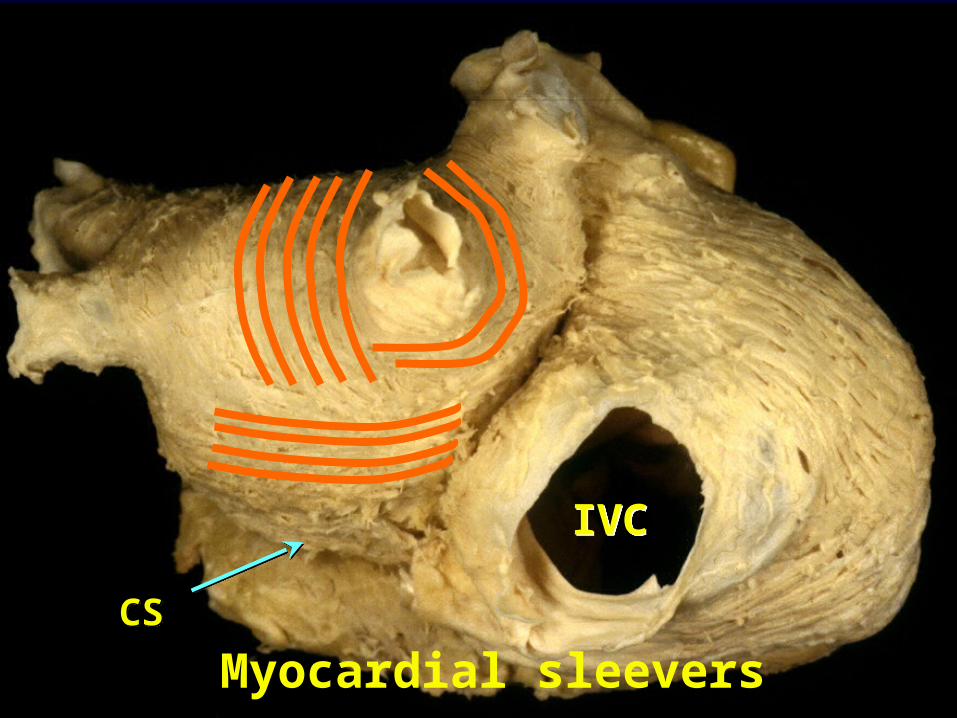
IVCIVC
CSCS
Myocardial sleevers

• In 1907 the presence of muscular sleeves around the PVs was documented for the first time
• Now they are considered important triggers of AFib

• LA-PVs junction could be functionally considered a “BROAD BAND” • Possible arrhythmogenic nature due to Automatism (EMBRIONAL NATURE) or micro-reentry (anisotropic carachteristic of LA-PVs junction)
JUNCTIONJUNCTION
Hocini M, Card. Res ’02 Hocini M, Circulation ’02Arora, Circulation 03
Haissaguerre, NEJM ‘96
Pato-physiology and Electrogenesis
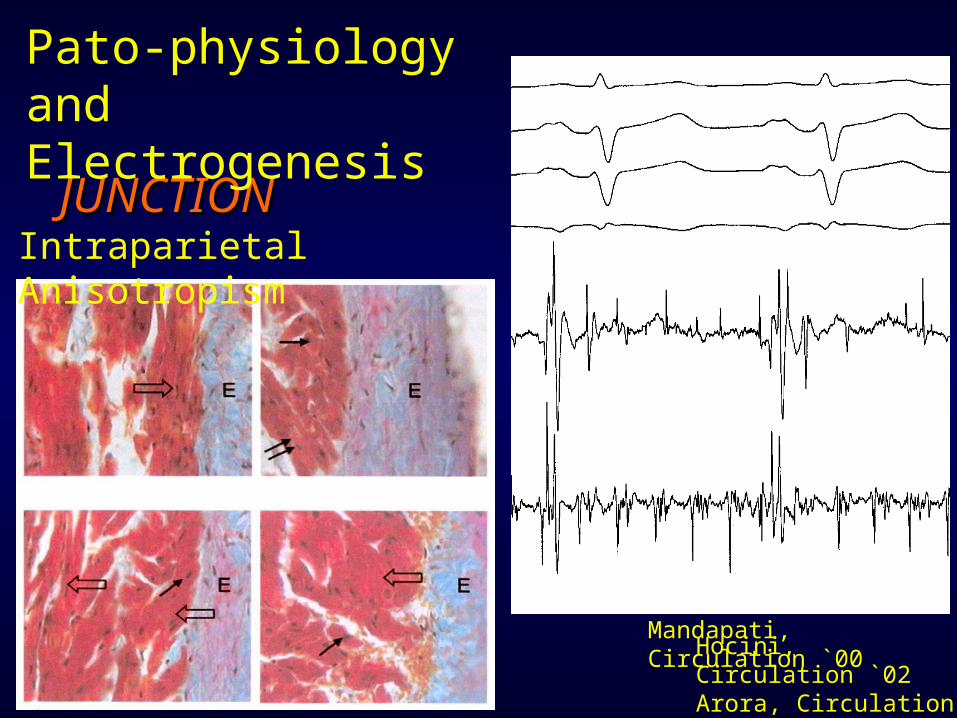
Hocini, Circulation `02Arora, Circulation `03
Mandapati, Circulation `00
Intraparietal Anisotropism
JUNCTIONJUNCTION
Pato-physiology and Electrogenesis

Spragg DD, Circulation ’03
Regional Alterations of Protein Expression in AFib dogs
ELECTROPHYSIOLOGICMECHANISMS

Sueda Sueda Ann Thorac Surg 1997Ann Thorac Surg 1997
Micro-reentry Micro-reentry circuitscircuits
HaissaguerreHaissaguerreNEJM 1998NEJM 1998 Focal Focal
activity activity from PVfrom PV
L di ML di M
HwangHwangCirculation 2000Circulation 2000
ELECTROPHYSIOLOGICMECHANISMS

• singole appl.RFsingole appl.RF • LassoLasso• SpiralSpiral• BasketBasket
• XrayXray
• CARTOCARTO• LocaLisaLocaLisa• NavXNavX• RPMRPM
• ICEICE
• ConvenzionaleConvenzionale
• 8 mm tip8 mm tip• Irrigated tipIrrigated tip• InvestigationalInvestigational(balloon, cryo)(balloon, cryo)
- Framework per l’ablazioneFramework per l’ablazione
- Guidare il mappaggioGuidare il mappaggio
- Localizzazione Localizzazione AnatomicaAnatomica
- Tag sui siti di ablazione- Tag sui siti di ablazione
- Valutazione del Valutazione del contatto del contatto del catetere catetere
-Miglioramento Miglioramento dell’efficienza dell’efficienza dell’erogazione dell’erogazione di energia di energia
MAPPAGGIO MAPPAGGIO TRACKINGTRACKING ABLAZIONE ABLAZIONE

• 251 Patients• 54±12 min di RF applicata attorno alle VP
Pappone et al. Circulation 2000 e 2001Pappone et al. Circulation 2000 e 2001
Assenza di eventi TROMBO-EMBOLICI e di STENOSI VP durante la degenza
End Point: (75%)• PVP < 0.1 mV• Delay > 30 ms (LAT)
% di successo in assenza di AA: 148/179 FA parossisitica (83%)40/72 FA persistente (55%)
Circumferencial Left AtrialApproach (CLAA)

Ernst et al. JACC `03Ernst et al. JACC `03
Lesioni Lesioni completecompleteA – 5% A – 5%
B – 21% B – 21%
C – 28 % C – 28 %
D - 61-66%D - 61-66%
RISULTATIRISULTATI
• Quando le lesioni Quando le lesioni erano complete, erano complete, 74% asintomatici 74% asintomatici senza AA senza AA
• Se lesioni Se lesioni incomplete quasi incomplete quasi tutti recidiva tutti recidiva dell’aritmia dell’aritmia
Circumferencial Left AtrialApproach (CLAA)

• Lesioni lineari complete sono Lesioni lineari complete sono teoricamente identiche alle incisioni teoricamente identiche alle incisioni chirurgichechirurgiche
VPIL
Pacing dal CS
Mitrale
Thomas, JACC 2000Thomas, JACC 2000Ernst, Circulation 1999Ernst, Circulation 1999
• Sono difficili da ottenere (con Sono difficili da ottenere (con aumentato rischio procedurale)aumentato rischio procedurale)
• La creazione di linee incomplete La creazione di linee incomplete è pro-aritmica è pro-aritmica
Pooled (meta-analysis) Circumferencial Left AtrialApproach (CLAA)

Bazaz & SchwartzmanBazaz & Schwartzman
VP settaliVP settali VP lateraliVP laterali
Potenziali PITFALL

Kato et al
Potenziali PITFALL
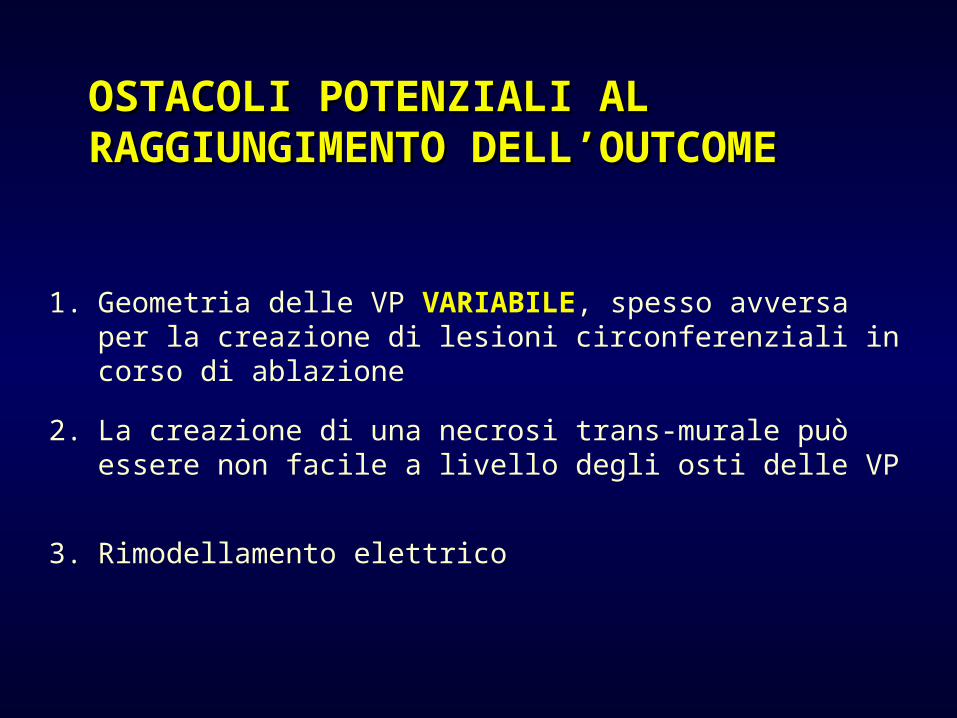
1. Geometria delle VP VARIABILE, spesso avversa per la creazione di lesioni circonferenziali in corso di ablazione
2. La creazione di una necrosi trans-murale può essere non facile a livello degli osti delle VP
3. Rimodellamento elettrico
OSTACOLI POTENZIALI AL OSTACOLI POTENZIALI AL RAGGIUNGIMENTO DELL’OUTCOMERAGGIUNGIMENTO DELL’OUTCOME

Pulmonary Vein Isolations (PVI)

Oral et al. Circulation 2003Oral et al. Circulation 2003
80 pts FAP
42±14 min di RFRedo: 0%“encircling + lesioni lineari 1 flutter AS
67%67%
88%88%
p=0.02p=0.02
20% flutter AS 20% flutter AS (meeting Boston (meeting Boston ed AF ed AF symposium symposium di Roma) di Roma)
18±9 min di RFRedo: 18%IVP

TERNI REGISTRYTERNI REGISTRY

• 422 pts with symptomatic PaAF and PeAF referred to us between July ‘04 and September ‘06
• RFCA performed in 145/422 pts (34%).
MATERIALSTERNI REGISTRYTERNI REGISTRY
• At least one MONTHLY episode of Persistent symptomatic AF
• At least ONE WEEKLY episode of PaAF or PeAF
• At least Two or More AADs unable to control symptoms

• Age >75 yrs• Contraindications to ACT• Congestive HEART FAILURE• NYHA functional class III / IV• LVEF ≤35% and/or LA
diameter ≥55mm• Presence of Cardiac
Thrombus• Life expectancy <1 yr• CCH surgery <3 mo or
PROSTHETIC valves
Exclusion criteriaExclusion criteriaTERNI REGISTRYTERNI REGISTRY

AFib PAROX. PERSIST. TOTALPatients 91 54 145 Age 62±13 67±8 64±10Sex (M/F) 61/26 37/21 98/47Duration 36±12N.episodes/mo 4±6LVEF (%) 55±6 51±9 53±9,7LA diameter 44±8 47±8 46±8CAD 15 21 36
TERNI REGISTRYTERNI REGISTRY

TERNI REGISTRYTERNI REGISTRY

• Procedura (min): 14826 14424
151 29
• Fluoroscopia (min): 5917 5816
6619
• Mappaggio (min): 158 139
184
• No. erogazioni di RF: 6216 6017
6519
RISULTATIRISULTATI Globale Pz.in RS Pz. in
FA
TERNI REGISTRYTERNI REGISTRY
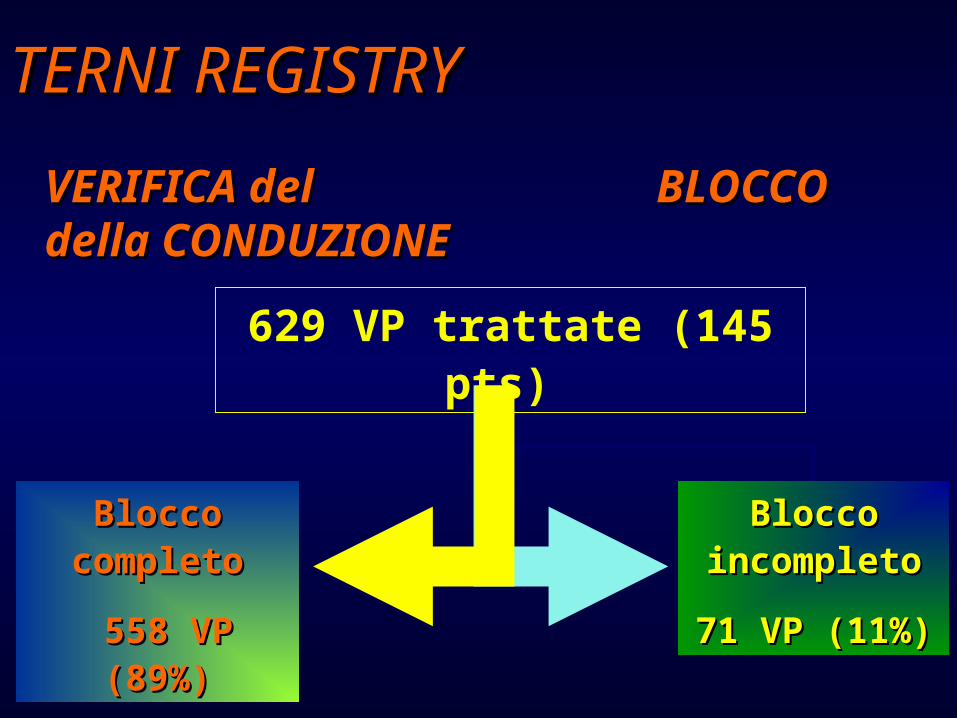
VERIFICA del VERIFICA del BLOCCO della CONDUZIONE BLOCCO della CONDUZIONE
629 VP trattate (145 pts)
Blocco Blocco completocompleto
558 VP 558 VP (89%)(89%)
Blocco Blocco incompletoincompleto
71 VP (11%)71 VP (11%)
TERNI REGISTRYTERNI REGISTRY

• After a mean FU Overall FREEDOM FROM AF (both PaAF and PeAF) was 66% (72% and 58%), w/o AADs and 79% (84% and 70%) with previous ineffective AADs.
Clinical OUTCOME
• The Kaplan-Meier statistical analysis probability of freedom from arrhythmia was maximal at 10 months
TERNI REGISTRYTERNI REGISTRY

82% success82% success
61% success61% success
La NON INDUCIBILITA’ post-IVP (67%) si associa ad una bassa ricorrenza di FA (87%) e potrebbe essere un utile ENDPOINT procedurale da perseguire per
razionalizzare le STRATEGIE
Nardi S, in Press
1st MESSAGETERNI REGISTRYTERNI REGISTRY

• I maggiori ostacoli alla stabilizzazione dei risultati ottenibili in acuto appaiono legati alla POSSIBILE TRANSITORIETA’ degli effetti termici su di un substrato complesso e delicato
OPEN QUESTIONS
• Recidiva possibile dopo un periodo variabile di FU privo di sintomi per presenza di ALTRE SORGENTI localizzate al di fuori delle VP a prevalenza rilevante
2nd MESSAGETERNI REGISTRYTERNI REGISTRY
• Among UNIVARIATE predictors, the variables of age, sex, duration and frequency of AF, LVEF, LA
size and structura HD, this approach revealed that only an increased LA SIZE >50 mm were an Indipendent Predictor of
RECURRENCE
• During FU, all pts w/o AF recurrence showed preserved or improved LA contraction (PW Doppler)
• Probably, pts with an enlarged LA may require a different strategy to achieve AF suppression.
3th MESSAGETERNI REGISTRYTERNI REGISTRY

Randomized Trials
Catheter ablation treatment in pts with AADs- refractory AFib: a prospective, multi-centre, randomized, controlled study (Catheter Ablation For The Cure Of Atrial Fibrillation Study). Stabile Eur H J ‘06
RFCA vs AADs as first-line treatment of symptomatic AFib: a randomized trial. Wazni OM, JAMA ‘05
Stabile G, Eu H J ‘06
“ Ablation therapy combined with AADs therapy is superior tu AADs alone in preventing arrhythmia recurrences in pts with PaAF or PeAF in whom AADs therapy has already failed “

Reant P, Circulation ‘05
Reverse Remodelling
• 48 pts with isolated AF • AADs ineffective• RFCA with PVI +
CT isthmus• Echo evaluation• 1 yr Follow up
78% PaAF 54% C-AF
PROSPECTIVE DOUBLE BLINDEDSTUDY

• In a broad spectrum of EP laboratories using different techniques over a wide time frame (7 yrs)
- free of AADs 48.0%- under AADs 24.1%
SUCCESS RATES
CLINICAL SUCCESS - Free of AADs: 3,866 (47,0%) - With AADss: 7,408 (79,0%)
LATE RECURRENCE
Cappato R, Circulation ‘04
Worldwide AFib SurveyWorldwide AFib Survey

But ….. back in the real world
• Data comes from 3 centres with a huge experience
Mickelson S, JICE ‘05
Cappato R, Circulation ‘05
In US EP believe 29% of pts with AF are candidates for RFCA
•Within these 3 centres there was a definite learning curve
• Lower volume centres have lower success rates and higher complication rate

• Nei soggetti con FA cronica o FA complicata (cardiopatia) è probabile che esista una maggiore complessità del disegno, con diversa combinazione dei meccanismi proposti (FOCALI e NON FOCALI) nella perpetuazione dell’ FA.
• Nei soggetti senza cardiopatia e/o con FA Parox, le VP svolgono una funzione sia di TRIGGER che di PERPETUAMENTO
… … il PRESENTE …il PRESENTE …

Who to refer ….•Symptomatic PaAF or PeAF with failed AADs
•No major cardiac structural disease •Age <70 yrs and LA size < 5,0 cm
Pts should be judged on an individual basis according to the Ablation Centre’s experience
When considered RFCA as 1When considered RFCA as 1stst line line ?? - Highly symptomatic AFib pts who refuse AADs.
- When Amiodarone represent the only AAD of choice
- In high risk pts for stroke who refuse or cannot take long term ACT
- Young pts with PaAF and SND who may not tolerate AADs w/o a permanent PM

Only large and prospective or randomized clinical studies in comparison between RFCA of PV and alternative approach (rate CTR, AADs Rx for prevent AFib , Ablate and Pace etc) for Rhythm CTR and for Ventricular rate based strategies will give us the ANSEWERs our question on best treatment for AFib
Conclusions

Grazie per la Cortese Attenzione