Anatomia Talamo y Gangliobasal (1)

of 19
-
Upload
gowtam-nara -
Category
Documents
-
view
218 -
download
0
Transcript of Anatomia Talamo y Gangliobasal (1)
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
1/19
Received: 3 January 2002Published online: 26 July 2002 Springer-Verlag 2002
ticofugal projection provides posi-tive feedback to the correct input,while at the same time suppressing
irrelevant information. Topographi-cal organisation of the thalamic af-ferents and efferents is contralateral,and the lateralisation of the thalamicfunctions affects both sensory andmotoric aspects. Symptoms of le-sions located in the thalamus areclosely related to the function of theareas involved. An infarction orhaemorrhage thalamic lesion can de-velop somatosensory disturbancesand/or central pain in the oppositehemibody, analgesic or purely algesic
thalamic syndrome characterised bycontralateral anaesthesia (or hypaes-thesia), contralateral weakness, atax-ia and, often, persistent spontaneouspain. Basal ganglia: Basal gangliaform a major centre in the complexextrapyramidal motor system, as op-posed to the pyramidal motor system(corticobulbar and corticospinalpathways). Basal ganglia are in-volved in many neuronal pathwayshaving emotional, motivational, as-sociative and cognitive functions as
well. The striatum (caudate nucleus,putamen and nucleus accumbens) re-ceive inputs from all cortical areasand, throughout the thalamus, pro-
ject principally to frontal lobe areas(prefrontal, premotor and supple-mentary motor areas) which are con-cerned with motor planning. Thesecircuits: (i) have an important regu-latory influence on cortex, providing
information for both automatic andvoluntary motor responses to the py-ramidal system; (ii) play a role in
predicting future events, reinforcingwanted behaviour and suppressingunwanted behaviour, and (iii) are in-volved in shifting attentional setsand in both high-order processes of movement initiation and spatialworking memory. Basal ganglia-thal-amo-cortical circuits maintain so-matotopic organisation of move-ment-related neurons throughout thecircuit. These circuits reveal func-tional subdivisions of the oculomo-tor, prefrontal and cingulate circuits,
which play an important role in at-tention, learning and potentiating be-haviour-guiding rules. Involvementof the basal ganglia is related to in-voluntary and stereotyped move-ments or paucity of movementswithout involvement of voluntarymotor functions, as in Parkinsonsdisease, Wilsons disease, progres-sive supranuclear palsy or Hunting-tons disease. The symptoms differwith the location of the lesion. Thecommonest disturbances in basal
ganglia lesions are abulia (apathywith loss of initiative and of sponta-neous thought and emotional re-sponses) and dystonia, which be-come manifest as behavioural andmotor disturbances, respectively.
Keywords Thalamus Basal ganglia Anatomy Behavioural disorders Motor disorders
Childs Nerv Syst (2002) 18:386404DOI 10.1007/s00381-002-0604-1 F O C U S S E S S I O N
Mara-Trinidad HerreroCarlos BarciaJuana Mari Navarro
Functional anatomy of thalamusand basal ganglia
M.-T. Herrero ( ) C. BarciaJ.M. NavarroExperimental Neurologyand Neurosurgery Group,Department of Morphological Sciencesand Psychobiology,School of Medicine, University of Murcia,Campus Espinardo, 30071 Murcia, Spaine-mail: [email protected].: +34-968-364683/3953Fax: +34-968-363955/4150
Abstract Thalamus: The humanthalamus is a nuclear complex locat-
ed in the diencephalon and compris-ing of four parts (the hypothalamus,the epythalamus, the ventral thala-mus, and the dorsal thalamus). Thethalamus is a relay centre subservingboth sensory and motor mechanisms.Thalamic nuclei (5060 nuclei) pro-
ject to one or a few well-defined cor-tical areas. Multiple cortical areas re-ceive afferents from a single thalam-ic nucleus and send back informationto different thalamic nuclei. The cor-
The pathologies that damage the humanbrain are rarely restricted to single ana-tomical structures. Stroke, trauma and par-ticularly degenerative diseases do not re-
spect functional anatomical boundaries. But there is much to be learned from obser-vation of what occurs in humans whosebrains are damaged by such insults. [12].
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
2/19
387
The thalamus
The thalamus is a nuclear complex situated in the dien-cephalon. The diencephalon forms the central core of thebrain and is surrounded by the hemisphere, so that onlythe basal surface is exposed to external view in a dia-mond-shaped area containing hypothalamic structures.The diencephalon is located at the dorsal end of the brain
stem surrounded by the internal capsule laterally and thelateral ventricles and corpus callosum superiorly. It is di-vided into symmetrical halves separated by the narrowthird ventricle but connected by the massa intermedia(Fig. 1). The rostrocaudal dimension of the human thala-mus is about 30 mm, its height about 20 mm and itswidth about 20 mm. It has been estimated that there areabout 10 million thalamic neurons in each hemisphere.The human thalamus is divided into 5060 nuclei (Fig. 1,Table 1). The names of most of these nuclei are derivedfrom their geographical locations within the thalamus.The thalamus is made up of four parts: the hypothalamus,the epithalamus, the ventral thalamus, and the dorsal thal-
amus. The traditional partition of the diencephalon intolarge ontogenic-embryologic subdivisions corresponds toHerrickss columnar model. The new neuromeric modelplaces the hypothalamus in a different neuromere [159].The epithalamus belongs to the same prosomere as thedorsal thalamus, but we can consider it separately; itcomprises the paraventricular complex, the habenularcomplex and the pretectal group. Moreover, the perithala-mus (ventral thalamus) originates from a different proso-mere and corresponds to the reticular nucleus, the zona
incerta and the pregeniculate nucleus. The dorsal thala-mus is in fact the main part of the thalamus.
The dorsal thalamus has two regions: 1 the allothalam-ic region and the isothalamic region.
The allothalamic region can be divided into:
1. The paraventricular region or midline nuclei (includ-ing the massa intermedia) (receiving afferents fromthe amygdala)
2. The centre-median-parafascicular complex (isolatedby a continuous capsule), which appears to be a majorelement in the basal ganglia system [51, 153]
3. The intralaminar region, which includes the nucleiwithin the lamina medialis
The isothalamic region constitutes the bulk of the thala-mus. It has bushy neurons and microneurons, andmost of its connections are directed to the cortical areasreceiving an important mass of corticothalamic axons (inprimates, much more important than the thalamocortical
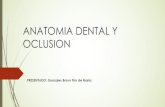
Fig. 1 Diagrammatic view of the internal structure of the dor-sal thalamus. The figure repre-sents a posterior view of rightand left sectioned thalamus.Note the regio centralis of theallothalamus and their organi-zation. The internal medullarylamina separates the regio su-perior, regio lateralis and regiomedialis. Nucleus perithalam-icus covers the thalamus ( A re-gio superior, Cme nucleus cen-tralis medius, CPf nucleus cen-tralis parafascicularis, GL nu-cleus geniculatus lateralis,GM nucleus geniculatus media-lis, dotted areas internal med-ullary lamina, LCL nucleusventralis caudalis lateralis,
LCM nucleus ventralis caudalismedialis, L regio lateralis,
M regio medialis, mi massa in-termedia, P regio posterior,PTh nucleus perithalamicus)
1Traditionally, (i) a thalamic region is defined as a gross topo-graphical division corresponding to the former nuclei; (ii) a terri-
tory such as the cerebral space filled by afferent endings from onesource; (iii) the thalamic space where neurons project to a givencortical target constitutes a source space; and (iv) a thalamic nu-cleus is defined as the intersection of a thalamocortical space withone territory. The principal terms in the nomenclature are the an-teroposterior, mediolateral and dorsoventral subdivisions, butthere are three classes of thalamic nuclei in relation to its function:specific, nonspecific and association nuclei (even if the classicconcept of nonspecific thalamus has important intranuclear varia-tions [154])
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
3/19
388
Table 1 Diencephalic elements in hierarchical order (from [154] with permission of the authors). Situs are topographic locations. Theymay or may not correspond to cytoarchitectonic subdivisions
I. Diencephalic nonthalamic elementsI.A. Perithalamus PTh (ventral thalamus, thalamus ventralis)Nucleus perithalamicus PTh
Situs perithalamicus PTh (= N. reticularis R)Situs incertus PTh ZI (= Zona incerta Zi)
Situs pregeniculatus PTh Pr (= N. pregeniculatus orprepeduncularis)
I.B. Epithalamus Hb = habenulaNucleus habenulae lateralis HbL (Hlmc)Nucleus habenulae medialis HbM (Hlpc)
II. Thalamus T (dorsal thalamus)
II.A. Allothalamus (neuronal types different from those of the isothalamus)i. Regio paraventricularis E or paramediana = Midline nuclei
+ adhesio interthalamica(massa intermedia)
ii. Regio centralis C = Centre medianparafascicularcomplex (basal ganglia)
Nucleus centralis parafascicularis CPf Nucleus centralis medius Cme pallidal thalamusNucleus centralis paralateralis CpL
iii. Regio intralaminaris Il = Intralaminar nuclei(in true sense of term)
Nucleus intralaminaris oralis IlO = paracentralis PCnNucleus intralaminaris caudalis IlC = centralis lateralis CLNucleus intralaminaris posterior IlP = I.La Postiv. Nucleus limitans Li
II.B. Isothalamus (made up of bushy thalamocortical projection neurons + microneurons)II.B.1. Regio superior SNucleus anterior A Nucleus anterior principalis
AV + AMNucleus anterodorsalis AD Nucleus anterior accessorius
Nucleus superficialis S Nucleus lateralis dorsalisII.B.2. Superregio medioposteriori. Regio medialis M Main part of the dorsomedial
nucleusNucleus medialis (man) MNucleus medialis medialis MM (amygdalar afferences)Nucleus medialis lateralis MLii. Regio posterior P Main part of the pulvinar
Nucleus posterior P4Situs medialis PuMSitus lateralis PuLSitus oralis PuOSitus oralis dorsalis PuOD (nucleus lateralis posterior)
II.B.3. Superregio basalis
i. Regio basalis BNucleus suprageniculatus Spinothalamic thalamusii. Regio intergeniculata Ig
Nucleus intergeniculatus Tectal thalamus
II.B.4. Superregio inferolateralis (sensory and motor thalamus)i. Regio geniculata G
Nucleus geniculatus GM auditory thalamusmedialisNucleus geniculatus GL visual thalamuslateralis
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
4/19
389
projection [154]). The internal and superior laminae di-vide the isothalamus into several subregions. The inter-nal medullary lamina divides the principal thalamic nu-clei into two major parts: a medial group on one side anda ventrolateral group on the other side of the internalmedullary lamina (Fig. 1). The anterior part of the inter-nal medullary lamina splits into two lamellae, which sur-round the anterior group o-nuclei. The cell groups withinthe internal medullary lamina in the caudal part are thenamed intralaminar nuclei (allothalamic region) [87].
Since the beginning of the twentieth century, the hu-
man thalamus has been divided into subnuclei and insome functional aspects on the basis of anatomical crite-ria and clinicopathological observations [38, 39, 76, 81,86]. However, the functional parcellation of the thala-mus has suffered from historical and technical draw-backs because of an archaic, rigid conception of thethalamic nucleus; overexploitation of cytoarchitecturetechnique, comparative anatomy and cortical connec-tions; underexploitation of subcortical afferent territo-ries, and opposition between ventral (relay) and dorsal
(associative) nuclei [154]. The thalamus is a relay cen-tre in subserving both sensory and motor mechanismsand then, awareness [179], attention [20] and other neu-rocognitive processes such as memory and language[47, 85]. Thalamic relay neurons receive excitatory glu-tamatergic input from peripheral sensory pathways [15].After neuroanatomical tracing studies in primates usingstereotactic atlases [140, 198] we know that most of thethalamic nuclei project to one or few well-defined corti-cal areas, with the exceptions of the reticular nucleusand the intralaminar nuclei, which project diffusely to
many areas of the cortex and have been defined as non-specific thalamic nuclei (Fig. 2) [81, 86, 87, 154]. Thecentromedian and parafascicular nuclei (nucleus centra-lis medius and nucleus centralis parafascicularis, respec-tively) also project back to the striatum [153]. More-over, thalamocortical interconnections may not be sim-ple one-to-one connections between single thalamic nu-clei and single cortical areas [81, 154]: multiple corticalareas receive afferents from a single thalamic nuclei andsend information back to different thalamic nuclei [63].
ii. Regio lateralis L (lateral mass plusparalaminar partsof the dorsomedialnucleus with ventralafferences)
a. Subregio arcuata LArc gustatory thalamusNucleus lateralis arcuatus LAcSensorimotor thalamus
b1. Subregio caudalis LC lemniscal thalamusNucleus ventralis caudalis LCL
lateralisNucleus ventralis caudalis LCM
medialisb2. Motor thalamus
I. Subregio intermedia LI cerebellar thalamusNucleus lateralis LIL
intermedius lateralisNucleus lateralis LIM (VIM + DI)intermedius mediodorsalisSitus ventralis medialis LIMmSitus dorsalis LlMdSitus postremus LlMps
Situs paralaminaris plIintermediusII. Subregio oralis LO pallidal thalamus
Nucleus lateralis oralis LO (VOL + DO)Situs principalis LO1 (VOL = Voe = Vlo)Situs dorsalis LOd (DO = Doe = dorsolateral VA)Situs ventralis Lov (VOV = VLm, lat)
III. Subregio dorsalis LR nigral thalamusNucleus lateralis rostralis LR ( VOM + LPo)Situs polaris LrpoSitus perifascicularis LRmcSitus ventralis medialis LRvmSitus paralaminaris rostralis PlONucleus lateralis rostralis LRM nigral + amygdalar
pars medialis
Table 1 (continued)
I
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
5/19
390
In addition to this, the corticofugal projection providespositive feedback to the correct input, while at thesame time suppressing irrelevant information: a giventhalamic neuron receives excitation from a small corti-cal area that shares the same stimulus selectivity (ego-centric selection) [203]. The corticothalamocorticalloops amplify the cortical oscillations (fast synchronousrhythms) [115], but thalamocortical neurons control theslow oscillations [116]. Within the thalamus exist pow-erful mechanisms that lead the promotion of synchro-nous and phasic 3 Hz neuronal activity that appears toarise from a perturbation of a physiological higher fre-quency spindle oscillation [80]. In normal circumstanc-es inhibitory synaptic responses, including those fromthe reticular nucleus, are required for network syn-chronisation. Cortical oscillations (fast synchronousrhythms) [115] are differentially affected by lesions of the corticothalamocortical loops and/or by lesions of thedifferent areas involved. Both fast [180] and slow oscil-lations [116] are synchronised not only in intracortical
but also in intrathalamic and thalamocortical networks.Moreover, the role of thalamus in cortico-cortical com-munication addresses the implications on higher corticalfunctions when thalamic or corticothalamocortical path-ways are involved [63].
The topographical organisation of the afferents at thelevel of the thalamic nuclei is contralateral. The laterali-sation of the thalamic functions affects motoric aspectsof different patterns such as speech production and non-verbal memory [85]; however, some nuclei have bothcontralateral and ipsilateral connections [144]. Instead of this, deafferentation results in reorganisation of the so-matosensory map but with different patterns and degrees
of somatotopic organisation, all of which may be associ-ated with pain syndromes [88, 92]. The plasticity and re-organisation are mediated by corticofugal loops [49], andit has been suggested that thalamic maps are constantlyadjusted by sensory experience [200]. However, the in-trathalamic connections [32] are still essential to under-stand, for instance, how thalamic syndrome produces al-terations to visual orientation when somatosensory fieldsare involved [7].
Each anatomically defined thalamic nucleus has itsown characteristic afferent and efferent connections [154]:this defines its function. Two distinct types of thalamicnucleus are proposed on the basis of their afferent fibres
from ascending pathways and/or from the cerebral cortex:1. First-order nuclei, with a modulatory function, receive
primary afferent fibres from ascending pathways andreceive corticothalamic afferents from cortical layer 6,which sends branches to the reticular nucleus
2. Higher order nuclei receive primary afferents from py-ramidal neurons of the cortical layer 5 lacking a branchto the reticular nucleus; its function is concerned withtransmitting information about the output of one corti-
Fig. 2 Distribution of the reciprocal right thalamocortical path-way. Above : lateral ( left ) and medial ( right ) surfaces of the hemi-sphere show the main thalamocortical projections. Correspondenc-es with thalamic nuclei are shown with the same pattern ( below ).[ I Regio superior (nucleus anterior), II regio medialis (nucleus me-dialis), III regio posterior (nucleus posterior), IV regio lateralis:
A subregio oralis + subregio dorsalis (pallidal + nigral thalamus), B subregio intermedia (cerebellar thalamus), C subregio arcuata +subregio caudalis (gustatory + lemniscal thalamus), GL nucleusgeniculatus lateralis, GM nucleus geniculatus medialis]
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
6/19
2. Elevation of the intracranial pressure and intracranialherniations produced by the oedema and the tumourmass
Tumours located deep in the brain, (involving the centralregion of thalamus and/or basal ganglia and spreadingbilaterally) can produce internal hydrocephalus, cortico-spinal signs, extrapyramidal symptoms, dementia, andeven neuroendocrine dysfunction. The symptoms of le-sions located in different parts of the thalamus are close-ly related to the function of the areas involved (nucleiare named as in Table 1).
Nucleus perithalamicus
The reticular nucleus, which surrounds much of the thal-amus like an eggshell, especially on its lateral side, wasdescribed by Klliker [94] as the Gitterkern or latticenucleus, as the fibrous latticework is a characteristic fea-
ture of this area. It contains inhibitory GABAergic neu-rons, which exert weak or strong inhibitory connectionswith significantly different responses on thalamic neu-rons [31]. A thalamic nucleus that does not project to thecortex, however, receives collaterals from thalamocorti-cal and corticothalamic axons. It is in an excellent posi-tion to monitor the activity in the corticothalamic andthalamocortical channels and to transmit informationback to the thalamus and the midbrain. Then the reticularnucleus controls the activity of thalamocortical channels,which is of fundamental importance for the two-waythalamocortical and corticothalamic connections [1, 14].The reticular nucleus can be divided into sectors that are
connected to more than one thalamic nucleus and tomore than one cortical area: and each sector has topo-graphically mapped connections with the thalamus andthe cortex, and each has a different function (sight, hear-ing, touch, movement or limbic functions) [64].
Allothalamus
The intralaminar nuclei have been included in the non-specific ascending reticular activating system projectingto extensive areas of the cerebral cortex the inputs re-ceived from the brain stem reticular formation [151].
These nuclei have been functionally associated with at-tention, arousal and consciousness. The nuclei are divid-ed into a rostral group and a central-caudal group. Aunique combination of calcium-binding protein stainingclearly delineates the intralaminar nuclei. The regio in-tralaminaris (nucleus intralaminaris oralis or paracentra-lis, nucleus intralaminaris caudalis or centralis lateralis)showed intense staining for both calretinin and calbin-din-D28 k [129]. The central-caudal group (regio centra-lis: nucleus centralis parafascicularis and nucleus centra-
391
cal area to another cortical area (playing a part in cor-tico-cortical connections on higher cortical functions)[63]; but again, intrathalamic interactions among dorsalthalamic nuclei can also be important [32]
Few neurological diseases have been correlated withchanges in a particular thalamic nucleus. The most fre-quent pathologies are vascular lesions and tumours.Haemorrhagic stroke frequently involves multiple struc-tures in basal ganglia-thalamocortical circuits and, sur-prisingly, those permit enhanced recovery comparedwith stroke restricted to the putamen or thalamus [124].Lesions confined to the thalamus have been associatedwith asterixis [103], and lesions of the thalamus plusbasal ganglia seem to be related to dystonia [104]. Focallesions of the thalamus and/or of the subthalamic regionlead to the development of dyskinesia and bilateralblepharospasm (associated with right posterior thalamiclesions). A classic thalamic syndrome is characterised bycontralateral anaesthesia (or hypaesthesia), contralateral
weakness, ataxia and, often, persistent spontaneous painthat can be treated by stereotactic thalamotomy [139].The vascularisation of the thalamus is of a great impor-tance when tumor pathology or infarction is affectingthese structures [150]; there is even a correspondence be-tween specific arteries and thalamic areas, which deter-mines the semeiology of thalamic syndromes [18, 47,133, 188]. A thalamic lesion caused by infarction orhaemorrhage can quickly lead to the development of so-matosensory disturbances and/or central pain in the op-posite hemibody, analgesic thalamic syndrome or a purealgesic syndrome [44]. CT scanning has shown that aparamedian or an anterolateral thalamic lesion (infarc-
tion) causes central pain, but a posterolateral ischaemicthalamic lesion will not be accompanied by central pain[194]. The posterior cerebral artery stroke syndrome in-volving the lateral thalamus (superregio inferolateralis)includes visual field deficits and, frequently, sensory,slight motor, neuropsychological and unilateral head-aches or migraine [18]. When the haemorrhages are re-stricted to the ventral posterior lateral territories of thethalamus (regio lateralis) this leads to a cheiro-oral syn-drome [175] or choreiform and dystonic movements as-sociated with rhythmic, alternating movements of low-frequency (myorhythmia) [108]. When tumours involvethe inferolateral nucleus of the thalamus one symptom
can be mutism, which is defined as a state in which thepatient is conscious but unwilling or unable to speak,even if this is usually a transient condition [34]. On theother hand, if a tumor grows slowly and infiltrates tissuerather than destroying it, symptoms will evolve slowlyand may be overlooked for a long time. The two basicmechanisms by which tumours produce symptoms are:
1. Focal disturbances resulting from compression, irrita-tion or destruction of adjacent tissue
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
7/19
Superregio medioposterior
Regio medialis . The nucleus medialis receives a largeprojection from the rhinal and dorsolateral prefrontalcortices [149], amygdala, ventral globus pallidus and ni-gral projections [27, 164, 169]. It projects to the orbital,medial and dorsal prefrontal cortex [141, 163] and showsstrong degeneration after frontal leucotomy [142]. Thenucleus shows an intensive pattern of cannabinoid recep-tors, as many of the regions are associated with higherfunctions [60]. It has been implicated in cognition [9],recognition memory [136] and habituation, in olfaction[157], in the wakesleep cycle, in respiration [3] and inother vegetative and endocrine circadian activities [10].In the case of infarcts involving the anterior or medialregion of the thalamus (both regio superiorregio media-lis), a loss of memory processes and cognition disordershave been described in the acute phase of insult [89].Moreover, it may be important to look at the conse-quences of thalamic infarctions, the damage to the nucle-
us medialis and nuclei of the allothalamus, or a com-bined lesion of these structures for deficits of executivefunctioning [188]. After a bithalamic infarction involv-ing the nucleus medialis a syndrome of lost physicalself-activation is common; this includes apathy, indiffer-ence and poor motivation [48].
Regio posterior . The pulvinar-lateral posterior complex,which has reciprocal connections with the associated pa-rieto-occipito-temporal cortical areas, is involved in vi-sual and language functions. The pulvinar has a role inselective visual attention. It has four areas (medial, cen-tral, lateral and lateral shell) demarcated by acetylcholin-
esterase and cytochrome oxidase [28]. Even if its lesionsare apparently silent they can affect superior functionsinvolving visual and language modalities and are relatedto hallucination experiences in patients.
Superregio basalis
Regio basalis . The nucleus suprageniculatus is locatedposteromedial to the nucleus ventralis caudalis lateralis(lemniscal thalamus), ventral to the regio posterior (pul-vinar) and the regio ventralis (allothalamus), lateral tothe nucleus centralis parafascicularis and dorsal to the
nucleus geniculatus medialis. The nucleus is the relay forpain and temperature sensation [33], including visceralinformation [24, 54]. Pain is a message that is protectivein nature. There are two pain systems, one signalling thediscriminative aspects of pain (location and intensity)and the other, the affective aspects of pain. Our responseto a noxious stimulus reflects the actions of both systems[196]. The spinothalamic tract arises from cells in laminaI and lamina V of the dorsal horn and projects to the nu-cleus suprageniculatus of the thalamus [161] establishing
392
lis medius) showed a complementary pattern of staining:the nucleus parafascicularis shows immunoreactivity forboth calbindin-D28 k and calretinin, while the nucleuscentralis medius shows immunoreactivity only for parv-albumin. As the nuclei from the regio centralis have im-portant connections with the basal ganglia [153], it hasbeen suggested that calcium-binding protein may play animportant role in the interactions between cerebral cortexand the basal ganglia [129]. By way of nonselective in-puts, mainly from the cholinergic brain stem nuclei aspedunculopontine nucleus and laterodorsal nucleus, thecentral-caudal group could modify the activity of thebasal ganglia-thalamocortical loops [62]. In fact, there isa loss of neurons in the caudal intralaminar nuclei in Par-kinsons disease and in progressive supranuclear palsy[69]. This central group is prominent in primates: themotor functional importance in the basal ganglia circuit-ry is related to the nucleus centralis medius, whereas thenucleus centralis parafascicularis is related mainly tocognitive, oculomotor and limbic functions [168]. The
functional role of these nuclei remains uncertain. Theyhave been proposed as an appropriate target for the treat-ment of intractable deep pain of central origin or follow-ing stroke or due to cancer, as they receive nondiscrimi-native or affective sensory information [11]. However,even if the nuclei are projecting diffusely to much widercortical areas (to one or few well-defined cortical fields)as a part of the diffuse or nonspecific ascending acti-vating system its nonspecificity has been questioned [62,117].
Isothalamus
Regio superior
The nucleus anterior receives projections from the mam-millary body (mammillothalamic tract) and projects tothe cingulate cortex belonging to the Papez circuit, theneural circuit for emotion [75, 143]. Lesions involvingthe nucleus anterior resulted in neuropsychological dys-function (aphasia and memory impairments) [133, 136]and in anomia for proper names [125]. Then, cognition,memory and emotion affect each other reciprocally, andatrophy or dysfunction of the midline groups has beenassociated with anterograde amnesia [148, 192]. Tu-
mours involving part of the Papez circuit, such as the an-terior nucleus of the thalamus, the hypothalamus andeven the anterior part of basal ganglia, disclosed memorydisturbances (but not emotional impairment), and aftersurgery of the tumour an improvement in memory func-tion has been reported even though radiation therapy candecrease the intellectual ability [136].
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
8/19
simple axodendritic synapses [162]. The calbindin-im-mnunoreactive fibres belong to the lamina I spinotha-lamic tract fibres and to the vagal-solitary-parabrachialafferents, representing different aspects of enteroceptiveinformation and regarding the physiological status of thetissues and organs of the body [16]. In humans, vascularinfarcts in this region cause analgesia and thermoanaes-thesia and can lead to the paradoxical development of central pain. It has even been suggested that activation of thermal pathways may contribute to modulation of noci-ceptive information [46]. The thalamic pain syndromehas been studied and located by anatomical (magneticresonance imaging) and metabolic correlation in thesame area [44]. The nucleus evokes painful and nonpain-ful paraesthetic cutaneous sensations when stimulated.The pain is described as like having a baby, and thestimulation of a ventrocaudal region to the ventrocaudalnucleus evokes visceral pain and even triggers painmemories [36, 37]. Moreover, the dorsal aspect of thisnucleus has a significant tonic, graded response to cool
stimuli and to innocuous mechanical stimuli [106].
Superregio inferolateralis
Regio geniculata . The GM (nucleus geniculatus media-lis) is situated lateral to the midbrain tegmentum in thecaudal region of the diencephalon rostral to the pulvinar.It has three parts:
1. A medial part with magnocellular neurons which re-ceive somatosensory, vestibular and auditory affer-ents.
2. A dorsal part, a small nucleus, receiving visual andauditory inputs.3. A ventral part with parvocellular neurons which re-
ceive only auditory signals.
The brachium from the inferior colliculus enters the nu-cleus in its posteromedial aspect. The acoustic radiationbegins in the anterolateral border of the nucleus andcurve in an anterior direction through the white matterwithin the transverse temporal gyrus to reach the primaryauditory cortex. Clinically, it has been reported that asmall haemorrhagic infarction located in the nucleus hascaused auditory illusions, such as hyperacousia and pa-
linacousia [57], dichotic listening and complete extinc-tion of the contralateral ear input [53]. Lesions, such asbilateral putaminal haemorrhage, involving the acousticradiation cause auditory agnosia for all sounds or for en-vironmental sounds only [185].
The GL (nucleus geniculatus lateralis) resembles ahat in shape and is positioned inferior to the pulvinar andlateral to the nucleus geniculatus medialis . In sagittalMR images the nucleus lies anterior and superior to thehippocampal formation and in coronal MR images the
nucleus is situated between the pulvinar and the cerebralcrus (the corticospinal fibres in the anterior part of themidbrain). Microscopically, it is made up of six layersseparated by thin white layers. The retinotopy is easilystudied by functional magnetic resonance imaging [26].The optic radiation begins in the posterior half of the lat-eral side of the nucleus and curves over the temporalhorn of the lateral ventricle to reach the primary visualcortex [25]. Both the nucleus and the optic radiation canbe analysed by MRI for the interpretation of the brain le-sions [21]. Lesions involving the nucleus or the optic ra-diation may result in homonymous quadrantanopia andhomonymous hemianopia. The syndrome of posteriorchoroidal artery territory infarction includes homony-mous quadrantanopsia, neuropsychological dysfunction(aphasia and memory disturbances) with or withouthemisensory loss, and the damage involves the nucleusgeniculatus lateralis, the posterior thalamus, the nucleusanterior and other regions, such as the hippocampus orthe parahippocampal gyrus [133].
Regio lateralis. Subregio arcuata . The gustatory thala-mus , just rostral to the lemniscal thalamus, is the relayfor gustatory sensation receiving the inputs from the ros-tral part of the lemniscus medialis (trigeminal pathway).The posterior border of the ventral posterolateral nucleus(nucleus ventralis caudalis lateralis) leading to the pulvi-nar is indicated by a triangular area (Wernickes triangu-lar area), and patients with lesions of this region demar-cated by the posterior limb of the internal capsule, havean absence of sensitivity.
The nucleus of the subregio caudalis lemniscal thala-mus is found lateral to the internal medullary lamina,
caudal to the ventral intermediate nucleus (subregio in-termedia) and rostral to the pulvinar. Laterally it is sur-rounded by the nucleus reticularis (nucleus perithalam-icus) and the external medullary lamina, and dorsally bythe nucleus posterior. The lemniscus medialis enters thisthalamic nucleus on its inferomedial aspect at its borderwith the pulvinar. The nucleus has a role as a somatosen-sory information modulator [127]. A three-link neuronalchain forms the lemniscus medialis system, connectingthe mechanosensory and propioceptive receptors neuronsof the extremities, trunk, neck and back of the head withthe primary somatosensory cortex throughout the thala-mus using glutamate as a transmitter [40]. However, a
visceral nociceptive input to this nucleus has also beendescribed [4]. It has been reported that single ischaemiclesions in the nucleus lead to development of the sensorythalamic syndrome [175] whose basic symptom is chron-ic pain [199]. Moreover, as sensory inputs have a signifi-cant role in dystonia, a reorganisation in the cutaneousreceptive fields at the level of the lemniscal thalamus hasbeen described in dystonia [105].
The motor thalamus can be identified as the nucleithat transfer information from the substantia nigra (sub-
393
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
9/19
regio dorsalis), the globus pallidus (subregio oralis) andthe cerebellum (subregio intermedia) to the prefrontal,supplementary, premotor, motor and somatosensory ar-eas of the cerebral cortex [78, 118, 154]. Notwithstand-ing these segregated pathways, there are overlappingprojections to the pre-supplementary motor area, wherethere are interdigitating foci of pallidal and cerebellarterritories [170]. All the thalamic motor neurons becomeactive before the onset of movement [193]. In the nucle-us a voluntary unit has been described, a cluster of neurons that are linked to rhythmic activity [160]. Theseneurons are activated only by voluntary movements of the contralateral limb and not by passive movements[160]. The motor thalamus receives projections from thenucleus perithalamicus in a specific diffuse manner,which can also contribute to the transfer of motor infor-mation [82]. One report described how a lesion in thebasal territory of the thalamus (ventral anterior and ven-tral lateral nuclei: subregio dorsalis and subregio oralis)either severely disrupted or completely prevented the re-
learning of a motor task [23]. Focal lesions involving theposterolateral quadrant of the thalamus are associatedwith abnormal movements [175]. The cerebellar thala-mus connections with motor cortex are an essential com-ponent in the pathophysiology of tremor [120]. The nu-cleus lateralis oralis (LO/VOL) has received much atten-tion in stereotactic treatment of Parkinsons disease andother involuntary motor disorders [135, 184], and thala-motomy of the motor thalamus is effective for dystoniatreatment even if the concrete target is not well defined[113]. Thalamotomy of the nucleus lateralis oralis ame-liorates rigidity but not tremor [137], but the thalamoto-my of the subregio intermedia (LIM/Vim), the cerebellar
thalamus, results in a permanent abolition of the tremorwithout affecting the general somatic sensation [68,138]. Multiple sclerosis patients with disabling tremorhave also benefited from thalamotomy [111]. Moreover,thalamotomy is also recommended for the treatment of dystonia [113], as thalamic activity of this nucleus con-tributes to dystonic movements [107].
Conclusion
The thalamus has been of great interest as a target organin stereotactic surgery for pain relief and in treatment of
movement disorders [83, 181, 202]. In fact, even as earlyas the second part of the nineteenth century, the livinghuman thalamus was studied directly by a stereotacticapproach and some atlases constructed using the inter-commissural line (connecting the anterior and posteriorcommissures in relation to the third ventricle) [67]. Re-cently, some changes have been brought about by stan-dardisation procedures correcting the antero-posteriorco-ordinates in relation to different intercommissural dis-tances, to interindividual nuclear variations [126] or
based on intraoperative neurophysiological data and in-traoperative X-ray films [201], or in detailed studies pre-serving post-mortem anatomical structures [98]. Howev-er, it is still far from easy to achieve the desired localisa-tion in functional surgery of the thalamus, because manyof the nuclei remain unstudied enigmas [186].
The basal ganglia
The term basal ganglia has not been precisely delimitedand there is no generally accepted definition. Classicanatomists described the deep large grey masses col-lectively as the basal ganglia of the telencephalon, whichare embedded in the white matter of each cerebral hemi-sphere. Initially basal ganglia was a descriptive termfor use in onto-phylogenetic or topographic classifica-tions (even the thalamus was regarded as a part of thebasal ganglia until the work of Vicq dAzyr in 1786).The basal ganglia include the caudate nucleus, the lenti-
form nucleus (the distinction between the putamen andthe pallidum was not made until the beginning of thetwentieth century), the subthalamic nucleus and the sub-stantia nigra (Fig. 3). The largest of these structures isthe corpus striatum. The corpus striatum (neostriatum),which is especially well developed in man, comprisesthe caudate nucleus and the putamen. The caudate nucle-us assumes the shape of a comet curving along the lateralwall of the lateral ventricle. It consists in a large head atthe front, a narrow dorsal body and a thin tail which fol-lows a course passing ventrally along the temporal hornof the ventricle and ending at the amygdaloid body. Theinferior part of the head is connected with the putamen at
the ventral part, at the level of the nucleus accumbens.The demarcation of the caudate nucleus at the level of the body and tail is easy, as is surrounded medially bythe lateral ventricle and laterally by the internal capsule.The head of the caudate nucleus and the putamen areconnected by thin bridges of grey matter (pontes griseicaudatolenticularis). The putamen is a shell-shapedstructure situated medial to the cortex of the insula andsurrounded laterally by the external capsule, medially bythe lateral medullary lamina of the globus pallidus, andsuperiorly by the white matter of the corona radiata. inT1-weighted MR images putamen is demarcated by thewhite matter and the globus pallidus, which are less sig-
nal intense. The globus pallidus (paleostriatum) has twoparts, medial and lateral. Both lie medial to the putamen,and together with it, constitute the lentiform nucleus.The lateral medullary lamina separates the lateral globuspallidus from the putamen, and the medial medullarylamina separates the medial from the lateral globus pall-idus. Medially it is limited by the posterior limb of theinternal capsule, while inferiorly it lies close to the sub-stantia innominata and the anterior commissure in therostral part. The subthalamic nucleus is a small lentiform
394
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
10/19
395
nucleus located at the border between the midbrain andthe diencephalon. It is bordered medially by the posteriorlimb of the internal capsule, dorsally by the lenticularfasciculus and ventrally by the zona incerta. As the sub-thalamic nucleus is surrounded by white fibres, it is easi-ly demarcated in T1- and T2-weighted MR images. Thesubstantia nigra lies in the ventral tegmentum of the mid-brain. The pars compacta is the largest part; it is dorsal
and caudal to the pars reticulata. In post-mortem tissuethe pars compacta is defined by the black staining by ne-uromelanin (included in dopaminergic neurons).
The anatomical and functional organisation of the bas-al ganglia help us to understand how motor and cognitivefunctions operate in normal and in diseased brain. Thebasal ganglia make up a major centre in the complex ex-trapyramidal motor system, as opposed to the pyramidalmotor system (corticobulbar and corticospinal pathways).The basal ganglia have been considered a motor centre
since the end of the nineteenth century: the corpus stria-tum contained the centres of automatic or sub-voluntary
integration of the various motor centres where habitual orautomatic movements become organised 52]. Its motoractions are mediated through the pyramidal system [187],as the basal ganglia do not make direct output connec-tions to the spinal cord [152] even if parallel projectionsfrom the substantia nigra pars reticulata to the tectum andthe reticular formation can descend to the spinal cord(through the tectospinal and reticulospinal pathways).The basal ganglia participate in many neuronal pathways,and their functions are not restricted to the motor behav-iour: they also have emotional, motivational, associativeand cognitive functions [6, 19, 93, 130, 167, 171, 172].Moreover, the basal ganglia have a role in error correc-
tion mechanisms [102], in which striatum is a central se-lection device [165]. New concepts have been establishedby basic research in human and in nonhuman primates[29, 166] and by a practical ex vivo method of learningfunctional thalamic and basal ganglia anatomy [195].
It was not until the 1960s that the importance of thestriato-pallido-nigral network (the Nauta-Mehler loop)was recognised [132]. The main transmission circuit of the basal ganglia originates in the whole of the neocortex[66, 174] (Fig. 4, left). The caudate and putamen receive
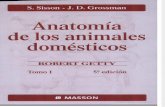
Fig. 3 Anatomical localisation of thalamus and basal ganglia,viewed from the left. Thalamus and basal ganglia are located closetogether. Lesions do not usually involve one nucleus only, but af-fect multiple structures in basal ganglia-thalamocortical circuits.Note the massa intermedia connecting right and left thalamus ( dis-continuous trace )
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
11/19
396
inputs from associative areas of the neocortex and thesensorimotor cortex (dorsal basal ganglia circuit), andthe nucleus accumbens receives input from the orbito-frontal cortex and other limbic cortical areas as well asfrom the hippocampus and the amygdala (ventral basalganglia circuit) [58, 131]. Dorsal and ventral basal gan-glia circuits are anatomochemically segregated in rela-
tion to the relative abundance of parvalbumin striatal in-terneurons [58, 173] and to the nitric oxide synthasemRNA expression [134]. Both circuits start in the cere-bral cortex (and/or subcortical telencephalic structures)throughout the neostriatum, paleostriatum and the ven-tral thalamic nuclei and reach not only the motor andpremotor areas of the frontal lobe concerned with themotor planning but also the associative and limbic corti-cal areas of the frontal lobe [182]. The funnel system of information flow has been discarded in favour of the five
parallel and largely segregated loops pertaining to motor,oculomotor, cognitive, associative and limbic functionsrelated to the major cortical areas of origin, which main-tain apparently segregated parallel pathways through thestriatum, both segments of the globus pallidus, the sub-thalamic nucleus and the substantia nigra pars reticulatawith a strict somatotopic organisation [5, 6, 19]. Howev-
er, these five parallel loops are not completely indepen-dent; there is a convergence of information:
1. At the level of the globus pallidus and substantia ni-gra pars reticulata [55, 95, 153]
2. At the level of the thalamus [176]3. By axonal collateralisation within the different nuclei
[147]
It is likely that the parallel but convergent and integra-tive mechanisms is the reason for the varied symptoma-tology seen in basal ganglia disease [131].
The efferent neurons of the striatum are the medium
spiny neurons which have a common morphology interms of dendritic organisation, local axon collateralsand size. All of them are GABAergic neurons. However,there is some segregation of projections. The efferencesfrom the striatum are divided into a dual projection of striatal outputs, some neurons projecting to the internalglobus pallidus and the substantia nigra pars reticulata(the striatal direct output pathway) and others to the ex-ternal globus pallidus (the striatal indirect output path-way) (Fig. 4, left) [146]. The direct pathway is provided
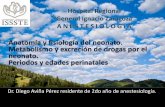
Fig. 4 Cortico-basal ganglia-cortical circuitry (through thalamicnuclei) in control brain ( left ) and in one affected by parkinsoniansyndrome ( right ). In the latter, imbalance in both direct and indi-rect pathways is seen by the size of the arrows . Note hyperactivityof output nucleus of basal ganglia circuit (substantia nigra pars re-ticulata and internal globus pallidus) and subthalamic nucleus inparkinsonian syndrome. Only a subset of basal ganglia pathwaysis shown ( D1 dopamine receptor type 1, D2 dopamine receptortype 2, SP substance P, Met-Enk met-enkephalin, DA dopamine,Gpe external globus pallidus, Gpi internal globus pallidus, SNpcsubstantia nigra pars compacta, SNpr substantia nigra pars reticul-ata, STN subthalamic nucleus; SO subregio oralis, SI subregio in-termedia
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
12/19
by D1-dopamine receptors, substance-P and dynorphin-containing neurons. The indirect pathway is provided byD2-dopamine receptors and enkephalin-containing neu-rons. Output neurons of the external globus pallidus areGABAergic and exert an inhibitory effect on the subtha-lamic glutamatergic neurons, which in turn send excita-tory projections to both output nuclei of the basal ganglia(namely the internal globus pallidus and the substantianigra pars reticulata, whose neurons are GABAergic asare those of the external globus pallidus). Both pathwaysthen provide antagonistic effects to the output of the bas-al ganglia: the direct pathway sends an inhibitory inputto both nuclei, whereas the indirect pathway results inexcitatory input (Fig. 4, left). The dual projection fromthe output nuclei of the basal ganglia to the different nu-clei of the thalamus (regio lateralis, regio centralis andregio dorsalis; see above) is organised in parallel and so-matotopically [5, 55] while, again, thalamic neuronssend convergent inputs to the same cortical areas but dif-ferent laminae [77]. The function of basal ganglia is
modulated by both striatal and extrastriatal dopaminergicinnervation [30, 177]. However, dopamine in striatalspiny neurons gives rise to synapses at dendritic spinesthat are also modulated by excitatory inputs from thecortex [178]. In these circumstances, striatal spiny neu-rons are trained by a dopamine-mediated reinforcementsignal to recognise and register salient contexts and/orstates that are likely to be useful in guiding behaviour[79].
The pathophysiological changes that occur in disor-ders of the basal ganglia have been clarified in recentyears by experimental approaches using the MPTP(1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) model
of parkinsonism in non-human primates. MPTP is aneurotoxin that induces extensive dopaminergic degen-eration resulting in a parkinsonian syndrome [70, 90].The basal ganglia are organised in such a fashion thatnigrostriatal denervation (the hallmark of Parkinsonsdisease) leads to overactivity of the internal globus pall-idus and the substantia nigra pars reticulata (Fig. 4,right) [74, 190]. The pathological hyperactivity of boththese nuclei and the subthalamic nucleus [191] has beenseen as the result of a reduced inhibitory input from thestriatum to the direct pathway [109] and increased activ-ity of the indirect pathway [71]. However, the activityand function of other nuclei, such as the external globus
pallidus, needs to be better understood [73], and clinicalsymptoms of Parkinsons disease or other pathologies,even the symptoms observed by focal pathology, are notfully explained by the current models of basal gangliacircuitry [110, 114].
The study of 240 cases with lesions in the basal gan-glia [12] has indicated that the commonest disturbancesin basal ganglia lesions are the syndrome of abulia (apa-thy with loss of initiative and of spontaneous thoughtand emotional responses) and dystonia, which manifest
397
as behavioural and motor disturbances, respectively.The symptoms differ depending on the location of thelesion: when lesions affect the caudate nucleus evenunilateral lesion can cause abulia, or more rarely disin-hibited behaviour; and occasionally they cause motordisorders (never cause parkinsonism but sometimes cho-rea or dystonia); lesions of the lentiform nucleus com-monly cause dystonia and rarely cause chorea; lesionsinvolving the putamen are more prone to cause dystoniathan those involving the globus pallidus; infrequentlythey cause abulia or disinhibition, and in this case, theglobus pallidus is usually involved; however, bilaterallesions involving the globus pallidus do not often causeparkinsonism but it is common for them to cause behav-ioural disturbances.
Motor symptomatology
Where necrosis of the caudate nucleus and putamen has
been present for a long period there is retrograde degen-eration of the cortico-striate fibres both in the subcallo-sal fasciculus and in the external capsule [42]. As thepyramidal motor system, the basal ganglia-thalamocorti-cal circuits maintain somatotopic organisation of move-ment-related neurons throughout the circuit [5, 99],mainly through the putamen, where neurons related toactive and/or passive movements of the lower extremityare found in a long rostrocaudal extension of the dorso-lateral putamen, neurons related to orofacial movementsare located ventromedially, and neurons related tomovements of the upper extremity are located in an in-termediate position. This somatotopical distribution has
the same pattern in both segments of the globus pallidus[145]. Interruption of the extrapyramidal system appearsto be responsible for muscle spasticity and hyperactivedeep reflexes. Involvement of the basal ganglia (includ-ing ventrobasal nuclei of the thalamus) is linked with in-voluntary and stereotyped movements without involvingvoluntary motor functions. Diseases of the basal ganglia(extrapyramidal pathology) result in profound move-ment disorders, which cause changes in motor func-tions:
1. Spontaneous hyperkinetic disorders such as are seenin Huntingtons disease [61, 84] or Tourettes syn-
drome2. Diminished movement (akinesia or hypokinesia) suchas is seen in Parkinsons disease [189] and progres-sive supranuclear palsy [112]
3. Motor stereotypies [22]
Moreover, lesions of the basal ganglia result in changesin muscle tone (muscular rigidity), fine resting tremor,postural disorders and athetosis (vermicular movementsof the distal extremities). Other involuntary movement
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
13/19
398
disorders include such symptoms as hyperactivity, dys-kinesia or hemiballismus, depending of the position of the lesion in the basal ganglia. A progressive generali-sed chorea and dementia with neostriatal neuronal lossand gliosis (vascular chorea) has been described [13].The variable tremor and rigidity of Wilsons disease isassociated with degeneration of the lenticular nucleus(putamen and globus pallidus) resulting from a disorderof copper metabolism [59]. Other degenerative changesin the basal ganglia (caudate nucleus and putamen) areassociated with complex stereotypies [119], dystonia af-ter head trauma [41, 43, 105], involuntary movementsof choreiform type (jerky, rapid and purposeless move-ments involving axial and proximal musculature of theextremities), athetoid-type movements (slow, sinuousand aimless movements involving distal limb muscula-ture) [43] or ballism [45]. Indeed, the best pathologicalcorrelation is that of hemiballismus: uncontrollable sud-den, flailing gross movements of the proximal limbmusculature of one or both limbs on the contralateral
side of the lesion [91]. It is associated with lesion of thecontralateral subthalamic nucleus of Luys [121] or itsconnections, but there are even reports of hemiballis-mus without subthalamic lesion but with a lenticular la-cunar infarct, probably with internal globus pallidus in-volvement [122, 123]. Subthalamic nucleus (and inter-nal globus pallidus) are important pacemakers of thebasal ganglia [156]. The cardinal motor signs found inParkinsons disease (akinesia, rigidity and resting trem-or) are generally attributed to the loss of dopaminergicinput to the striatum that results from the degenerationof the substantia nigra pars compacta [50]. Chronictreatment with levodopa and/or dopaminergic agonists
results in unacceptable side effects, such as dyskinesiaor hyperkinesia [189]. This reversal of symptoms iscaused by the imbalance of the direct and indirect basalganglia pathways required for coordinated movements[72, 96]. In recent years, new therapeutic approacheshave included:
1. Pharmacological strategies with different dopamine-receptor agonists [114] and new surgical approachessuch as
2. Transplantation of dopaminergic neurons [56]3. Lesions or deep brain stimulation of the subthalamic
nucleus or of the internal globus pallidus [65, 97]
Behavioural disturbances
Basal ganglia and the adjacent structures play a part inpredicting future events, reinforcing wanted behaviourand suppressing unwanted behaviour [172] and are in-volved in shifting attentional sets and in high-order pro-cesses of movement initiation [17] as well as in spatialworking memory [158]. As functions of the basal gan-
glia include cognitive and emotional aspects, clinicalsymptomatology is not restricted to the motor system;some psychological, disorders of mood and thought dis-turbances are known, including depression, schizophre-nia and obsessive compulsive disorder [2, 61, 155, 173].Basal gangliathalamocortical circuits reveal functionalsubdivisions of the oculomotor, prefrontal and cingulatecircuits [5, 19, 58, 66], which have an important role inattention, learning and potentiation of behaviour-guidingrules [171, 197, 198], making them comparable to thesomatotopic channels within the motor circuit, which areinvolved in the programming and control of movement.In the Bhatia and Marsden study [12] of a total of 240patients with basal ganglia lesions, 111 had some type of behavioural disorder with aphasic and dysarthric dys-function, abulia, depression, disinhibited behaviour andacute confusional state after haemorrhage into the cau-date (even if this last is probably the consequence of awidespread brain dysfunction due to intraventricularbleeding). Aphasia has been described without haemor-
rhagic lesions when lesions are located in the caudatenucleus [8, 35, 100, 101]. Frontal lobe syndrome [183],psychic akinesia [100] and obsessive compulsive distur-bances [101] have been described when bilateral lesionsare established. The caudate nucleus contributes to mem-ory [197], learning [93, 130], cognitive [165, 171] andbehaviour [172] functions; its bilateral damage leads toapathy, decreased recent memory and reduced initiativeand spontaneity [128].
Despite the voluminous literature available on it, therole of basal ganglia in health and disease remains con-troversial. Moreover, as basal ganglia are closely locatedto the thalamus and they have intimate and highly specif-
ic afferent and efferent connections with cerebral cortexand thalamus, basal ganglia should not be viewed as nu-clei with a role independent of both structures [130,153].
Acknowledgements The authors would like to express their ac-knowledgement to their colleagues of the Experimental Neurologyand Neurosurgery Group. M.T.H. also wishes to thank ProfessorAgid, Dr. Hirsch, Dr. Obeso and Dr. Percheron for their scientificsupport and helpful advice on these topics. Drawings in the figureshave been performed by C. Barcia. This work was supported bygrants nos. FIS 99/1392 and FEDER 1FD971931.
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
14/19
399
References
1. Adams NC, Lozsadi DA, Guillery RW(1997) Complexities in the thalamocor-tical and corticothalamic pathways. EurJ Neurosci 9:204209
2. Afifi AK (1994) Basal ganglia: func-tional anatomy and physiology, II.J Child Neurol 9:352361
3. Akopyan NS, Baklavadzhyan OG,Sarkisyan NV (2000) The effects of themediodorsal nucleus of the thalamuson respiratory neurons of the medullaoblongata and respiration in rats inconditions of hypoxia. Neurosci BehavPhysiol 30:449453
4. Al-Chaer ED, Lawand NB, WestlundKN, Willis WD (1996) Visceral noci-ceptive input into the ventral postero-lateral nucleus of the thalamus: a newfunction for the dorsal column path-way. J Neurophysiol 76:26612674
5. Alexander GE, Crutcher MD (1990)Functional architecture of basal gangliacircuits: neural substrates of parallelprocessing. Trends Neurosci13:266271
6. Alexander GE, DeLong MR, Strick PL(1986) Parallel organization of func-tionally segregated circuits linking bas-al ganglia and cortex. Annu Rev Neu-rosci 9:357381
7. Anastasopoulos D, Bronstein AM(1999) A case of thalamic syndrome:somatosensory influences on visualorientation. J Neurol Neurosurg Psy-chiatry 67:390394
8. Barat M, Mazaux JM, Bioulac B,Giroire JM, Vital C, Arn L (1981)Troubles du langage de type aphasiqueet lsions putamino-caudes. Observa-tion anatomo-clinique. Rev Neurol137:343356
9. Barbas H (2000) Connections underly-ing the synthesis of cognition, memory,and emotion in primate prefrontal cor-tices. Brain Res Bull 52:319330
10. Barriga F, Ruiz Dominguez JA,Velayos JL (1997) Insomnio familiar:una enfermedad prinica humana queabre las puertas a un mayor conocimi-ento del tlamo. Rev Med UnivNavarra 41:224228
11. Berendsen HW, Gronewegen HJ(1991) Restricted cortical terminalfields of the midline and intralaminarthalamic nuclei in the rat. Neurosci-ence 42:73102
12. Bhatia KP, Marsden CD (1994) Thebehavioural and motor consequences of focal lesions of the basal ganglia inman. Brain 117:859876
13. Bhatia KP, Lera G, Luthert PJ,Marsden CD (1994) Vascular chorea:case reported with pathology. Mov Dis-ord 9:447450
14. Bickle J, Bernstein M, Heatley M,Worley C, Stiehl S (1999) A functionalhypothesis for LGN-V1-TRN connec-tivities suggested by computer simula-tion. J Comput Neurosci 6:251261
15. Blomqvist A, Ericson AC, Craig AD,Broman J (1996) Evidence for gluta-mate as a neurotransmitter in spinotha-lamic tract terminals in the posteriorregion of owl monkeys. Exp Brain Res108:3344
16. Blomqvist A, Zhang ET, Craig AD(2000) Cytoarchitectonic and immuno-histochemical characterization of aspecific pain and temperature delay,the posterior portion of the ventral me-dial nucleus, in the human thalamus.Brain 123:36013619
17. Boussaoud D, Kermadi I (1997) Theprimate striatum: neuronal activity inrelation to spatial attention versus mo-tor preparation. Eur J Neurosci9:21522168
18. Brandt T, Steinke W, Thic A, PessinMS, Caplan LR (2000) Posterior cere-bral artery territory infarcts: clinicalfeatures, infarcts topography, causesand outcome. Multicenter results and areview of the literature. CerebrovascDis 10:170182
19. Brown J, Bullock D, Grossberg S(1999) How the basal ganglia use par-allel excitatory and inhibitory learningpathways to selectively respond to un-expected rewarding cues. J Neurosci19:1050210511
20. Buchel C, Josephs O, Rees G, TurnerR, Frith CD, Friston KJ (1998) Thefunctional anatomy of attention to visu-al motion. A functional MRI study.Brain 121:12811294
21. Burgel U, Schormann T, Schleicher A,Zilles K (1999) Mapping of histologi-cally identified long fiber tracts in hu-man cerebral hemispheres to the MRIvolume of a reference brain: positionand spatial variability of the optic radi-ation. Neuroimage 10:489499
22. Canales JJ, Graybiel AM (2000) Ameasure of striatal function predictsmotor stereotypy. Nat Neurosci3:377383
23. Canavan AGM, Nixon PD, PassinghamRE (1989) Motor learning in monkeys( Macaca fascicularis ) with lesions inmotor thalamus. Exp Brain Res77:113126
24. Chandler MJ, Hobbs SF, Fu QG,Kenshalo DR, Blair RW, Foreman RD(1992) Responses of neurons in ventro-posterolateral nucleus of primate thala-mus to urinary bladder distension.Brain Res 571:2634
25. Chen W, Zhu XH (2001) Correlation of activation sizes between lateral genicu-late nucleus and primary visual cortexin humans. Magn Reson Med45:202205
26. Chen W, Zhu XH, Thulborn KR,Ugurbil K (1999) Retinotopic mappingof lateral geniculate nucleus in humansusing functional magnetic resonanceimaging. Proc Natl Acad Sci USA96:24302434
27. Churchill L, Kalivas PW (1999) Theinvolvement of the mediodorsal nucle-us of the thalamus and the midbrain ex-trapyramidal area in locomotion elicit-ed from the ventral pallidum. BehavBrain Res 104:6371
28. Cola MG, Gray DN, Seltzer B, Cusick CG (1999) Human thalamus: neuro-chemical mapping of inferior pulvinarcomplex. Neuroreport 16:37333738
29. Collins P, Wilkinson LS, Everitt BJ,Robbins TW, Roberts AC (2000) Theeffect of dopamine depletion from thecaudate nucleus of the common mar-moset ( Callithrix jacchus ) on tests of prefrontal cognitive function. BehavNeurosci 114:317
30. Cossete M, Levesque M, Parent A(1999) Extrastriatal dopaminergic in-nervation of human basal ganglia. Neu-rosci Res 34:5154
31. Cox CL, Huguenard JR, Prince DA(1997) Nucleus reticularis neurons me-diate diverse inhibitory effects in thala-mus. Proc Natl Acad Sci USA94:88548859
32. Crabtree JW, Collingridge GL, Isaac JT(1998) A new intrathalamic pathwaylinking modality-related nuclei in thedorsal thalamus. Nat Neurosci1:389394
33. Craig AD, Bushnell MC, Zhang ET,Blomqvist A (1994) A thalamic nucle-us specific for pain and temperaturesensation. Nature 372:770773
34. Crutchfield JS, Sawaya R, Meyers CA,Moore BD (1994) Postoperative mut-ism in neurosurgery. Report of twocases. J Neurosurg 81:115121
35. Damasio AR, Damasio H, Rizzo M,Varney N, Gersh F (1982) Aphasiawith non-hemorrhagic lesion in thebasal ganglia and internal capsule.Arch Neurol 39:1524
36. Davis KD, Tasker RR, Kiss ZH,Hutchison WD, Dostrovsky JO (1995)Visceral pain evoked by thalamic mi-crostimulation in humans. Neuroreport26:369374
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
15/19
400
37. Davis KD, Lozano RM, Manduch M,Tasker RR, Kiss ZH, Dostrovsky JO(1999) Thalamic relay site for cold per-ception in humans. J Neurophysiol81:19701973
38. Debakan A (1953) Human thalamus.An anatomical developmental andpathological study. I. Division of thehuman adult thalamus into nuclei byuse of the cytomyeloarchitectonicmethod. J Comp Neurol 99:639667
39. Debakan A (1954) Human thalamus.An anatomical developmental andpathological study: development of thehuman thalamic nuclei. J Comp Neurol100:6397
40. De Biasi S, Amadeo A, Spreafico R,Rustioni A (1994) Enrichment of gluta-mate immunoreactivity in lemniscalterminals in the ventropostero lateralthalamic nucleus of the rat: an immu-nogold and WGA-HRP study. AnatRec 240:131140
41. Demierre B, Rondot P (1983) Dystoniacaused by putamino-capsulo-caudatevascular lesions. J Neurol NeurosurgPsychiatry 46:404409
42. Denny-Brown D (1962) The basal gan-glia and their relation to disorders of movement. Oxford University Press,London
43. Denny-Brown D (1968) Symposium ondisease of the basal ganglia. Nature of dystonia. Rev Bras Med 25:769773
44. De Salles AA, Bittar GT Jr (1994)Thalamic pain syndrome: anatomic andmetabolic correlation. Surg Neurol41:147151
45. Deste A, Muller JP, Vermersch P,Pruvo JP, Warot P (1990) Hemibal-lisme. Hemichore. Infarctus striatal.Rev Neurol 146:150152
46. Duncan GH, Kupers RC, Marchand S,Villemure JG, Gybels JM, BushnellMC (1998) Stimulation of human thal-amus for pain relief: possible modula-tory circuits revealed by positron emis-sion tomography. J Neurophysiol80:33263330
47. Engelborghs S, Marien P, Martin JJ, DeDeyn PP (1998) Functional anatomy,vascularisation and pathology of thehuman thalamus. Acta Neurol Belg98:252265
48. Engelborghs S, Marien P, Pickutt BA,Verstraeten S, De Deyn PP (2000) Lossof psychic self-activation after parame-
dian bithalamic infarction. Stroke31:1762176549. Ergenzinger ER, Glasier MM,
Hahm JO, Pons TP (1998) Corticallyinduced thalamic plasticity in the pri-mate somatosensory system. Nat Neu-rosci 1:226229
50. Fearnley JM, Lees AJ (1991) Ageing andParkinsons disease: substantia nigra re-gional selectivity. Brain 114:22832301
51. Fenelon G, Francois C, Percheron G,Yelnik J (1991) Topographic distribu-tion of the neurons of the central com-plex (centre median-parafascicularcomplex) and of other thalamic neu-rons projecting to the striatum in ma-caques. Neuroscience 45:495510
52. Ferrier D (1876) The functions of thebrain. London
53. Fischer C, Bognar L, Turjman F,Lapras C (1995) Auditory evoked po-tentials in a patient with a unilateral le-sion of the inferior colliculus and me-dial geniculate body. Electroencepha-logr Clin Neurophysiol 96:261267
54. Foreman RD (1999) Mechanism of cardiac pain. Annu Rev Physiol61:143147
55. Franois C, Yelnik J, Percheron G,Fenelon G (1994) Topographic distri-bution of the axonal endings from thesensorimotor and associative striatumin the macaque pallidum and substantianigra. Exp Brain Res 102:305318
56. Freed CR, Greene PE, Breeze RE,Tsai WY, DuMouchel W, Kao R,Dillon S, Winfield H, Culver S,Trojanowski JQ, Eidelberg D, Fahn S(2001) Transplantation of embryonicdopamine neurons for severe Parkin-sons disease. N Engl J Med34:710719
57. Fukutake T, Hattori T (1998) Auditoryillusions caused by a small lesion in theright medial geniculate body. Neurolo-gy 51:14691471
58. Gerfen CR (1984) The neostriatal mo-saic: compartmentalization of cortico-striatal input and striatonigral outputsystems. Nature 311:461464
59. Giagheddu M, Tamburini G, Piga M,Tacconi P, Giagheddu A, Serra A,Siotto P, Satta L, Demelia L,Marrosu F (2001) Comparison of MRI,EEG, EPs and ECD-SPECT inWilsons disease. Acta Neurol Scand103:7181
60. Glass M, Dragunow M, Faull RL(1997) Cannabinoid receptors in thehuman brain: a detailed anatomical andquantitative autoradiographic study inthe fetal, neonatal and adult humanbrain. Neuroscience 77:299318
61. Graveland GA, Williams RS, DiFiglia
M (1985) Evidence for degenerativeand regenerative changes in neostriatalspiny neurons in Huntingtons disease.Science 227:770773
62. Groenewegen HJ, Berendse HW(1994) The specificity of the nonspe-cific midline and intralaminar thalam-ic nuclei. Trends Neurosci 17:5257
63. Guillery RW (1995) Anatomical evi-dence concerning the role of the thala-mus in corticocortical communication:a brief review. J Anat 187:583592
64. Guillery RW, Feig SL, Lozsadi DA(1998) Paying attention to the thalamicreticular nucleus. Trends Neurosci21:2832
65. Guridi J, Herrero MT, Luquin MR,Guillen J, Ruberg M, Laguna J,Vila M, Javoy-Agid F, Agid Y,Hirsch EC, Obeso JA (1996) Subthala-motomy in parkinsonian monkeys. Be-havioural and biochemical analysis.Brain 119:17171727
66. Haber SN, Kunishio K, Mizobuchi M,Lynd-Balta E (1995) The orbital andmedial prefrontal circuit through theprimate basal ganglia. J Neurosci15:48514867
67. Hassler R (1982) Architectonic organi-zation of the thalamic nuclei. In:Schaltenbrand G, Walker AE (eds)Stereotaxy of the human brain ana-tomical, physiological and clinical ap-plications, 2nd edn. Thieme, Stuttgart,pp 140180
68. Hayase N, Miyashita N, Endo K,Narabayasi H (1998) Neuronal activityin GP and Vim of parkinsonian patientsand clinical changes of tremor throughsurgical interventions. Stereotact FunctNeurosurg 71:2028
69. Henderson JM, Carpenter K,Cartwright H, Halliday GM (2000)Loss of thalamic intralaminar nuclei inprogressive supranuclear palsy and Par-kinsons disease: clinical and therapeu-tic implications. Brain 123:14101421
70. Herrero MT, Hirsch EC, Kastner AM,Ruberg M, Luquin MR, Laguna J,Javoy-Agid F, Obeso JA, Agid Y(1993) Does neuromelanin contributeto the vulnerability of catecholaminer-gic neurons in monkeys intoxicatedwith MPTP? Neuroscience 56:499511
71. Herrero MT, Augood SJ, Hirsch EC,Javoy-Agid F, Agid Y, Obeso JA,Emson PC (1995) Effects of l-DOPAon preproenkephalin and preprotachy-kinin gene expression in the MPTP-treated monkeys striatum. Neurosci-ence 68:11891198
72. Herrero MT, Augood SJ, Asensi H,Hirsch EC, Agid Y, Obeso JA, EmsonPC (1996) Effects of l-DOPA-therapyon dopamine D2 receptor mRNA ex-pression in the striatum of MPTP-intoxicated parkinsonian monkeys.Mol Brain Res 42:149155
73. Herrero MT, Levy R, Ruberg M,
Javoy-Agid F, Luquin MR, Agid Y,Hirsch EC, Obeso JA (1996) Glutamicacid decarboxylase mRNA expressionin medial and lateral pallidal neuronsin the MPTP-treated monkeys and pa-tients with Parkinsons disease. AdvNeurol 69:209216
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
16/19
401
74. Herrero MT, Levy R, Ruberg M,Luquin MR, Villares J, Guillen J,Faucheux B, Javoy-Agid F, Guridi J,Agid Y, Obeso JA, Hirsch EC (1996)Consequence of nigrostriatal denerva-tion and l-DOPA therapy on the ex-pression of glutamic acid decarboxyl-ase messenger RNA in the pallidum.Neurology 47:219224
75. Hess WR (1954) Diencephalon: auto-nomic and extrapyramidal functions.Grune and Stratton, New York
76. Hirai T, Jones EG (1989) A new par-cellation of the human thalamus on thebasis of histochemical staining. BrainRes Rev 14:134
77. Holsapple JW, Preston JB, Strick PL(1991) The origin of thalamic inputs tothe hand representation in the primarymotor cortex. J Neurosci 11:26442654
78. Hoover JE, Strick PL (1993) Multipleoutput in the basal ganglia. Science259:819821
79. Houk JC, Wise SP (1995) Distributedmodular architectures linking basalganglia, cerebellum, and cerebral cor-tex: their role in planning and control-ling action. Cereb Cortex 2:95110
80. Huguenard JR (1999) Neuronal circuit-ry of thalamocortical epilepsy andmechanisms of antiabsence drug ac-tion. Adv Neurol 79:991999
81. Illinsky IA, Kultas-Illinsky K (1987)Sagittal cytoarchitectonic maps of the
Macaca mulat ta thalamus with a re-vised nomenclature of motor-relatednuclei validated by observations ontheir connectivity. J Comp Neurol262:331364
82. Illinsky IA, Ambardekar AV,Kultas-Illinsky K (1999) Organizationof projections from the anterior pole of the nucleus reticularis thalami (NRT)to subdivisions of the motor thalamus:light and electron microscopic studiesin the rhesus monkey. J Comp Neurol409:369384
83. Jeanmonod D, Magnin M, Morel A(1994) Chronic neurogenic pain andthe medial thalamotomy. SchweizRundsch Med Prax 83:702707
84. Joel D (2001) Open interconnectedmodel of basal ganglia-thalamocorticalcircuitry and its relevance to the clini-cal syndrome of Huntingtons disease.Mov Disord 16:407423
85. Johnson MD, Ojemann GA (2000) The
role of the human thalamus in languageand memory: evidence from electro-physiological studies. Brain Cogn42:218230
86. Jones EG (1985) The thalamus. Ple-num, New York
87. Jones EG (1990) Correlation and re-vised nomenclature of ventral nuclei inthe thalamus of human and monkey.Stereotact Funct Neurosurg 54/55:120
88. Jones EG (2000) Cortical and subcor-tical contributions to activity-depen-dent plasticity in primate somatosen-sory cortex. Annu Rev Neurosci23:137
89. Kalashnikova LA, Gulevskaya TS,Kashina EM (1999) Disorders of higher mental functions due to singleinfarctions in the thalamus and inthe area of the thalamofrontaltracts. Neurosci Behav Physiol29:397403
90. Kastner AM, Herrero MT, Hirsch EC,Guillen J, Luquin MR, Javoy-Agid F,Obeso JA, Agid Y (1994) Decreasedtyrosine hydroxylase content in thedopaminergic neurons of MPTP-in-toxicated monkeys: effect of levodopaand GM1 ganglioside therapy. AnnNeurol 36:206214
91. Kim JS, Suh DC (2001) Hemiballism-hemichorea and posterior communi-cating artery stenosis. Eur Neurol45:182183
92. Kiss ZH, Dostrovsky JO, Tasker RR(1994) Plasticity in human somato-sensory thalamus as a result of deaf-ferentation. Stereotact Funct Neuro-surg 62:153163
93. Knowlton BJ, Mangels JA, Squire LR(1996) A neostriatal habit learningsystem in humans. Science273:13991402
94. Klliker A (1896) Handbuch derGewebelehre des Menschen. Nerven-systeme des Menschen und derThiere, vol 2, 6th edn. Engelman,Leipzig
95. Kolomiets BP, Deniau JM, Mailly P,Mntrey A, Glowinski J, ThierryAM (2001) Segregation and conver-gence of information flow through thecortico-subthalamic pathways. J Neu-rosci 21:57645772
96. Korstzewa RM (1995) Dopamine re-ceptor sensitivity. Neurosci BiobehavRev 19:117
97. Krause M, Fogel W, Heck A,Hacke W, Bonsanto M, TrenkwalderC, Tronnier V (2001) Deep brainstimulation for the treatment of Par-kinsons disease: subthalamic nucleusversus globus pallidus internus.J Neurol Neurosurg Psychiatry70:464470
98. Kretschmann HJ, Weinrich W (1998)Neurofunctional systems. 3D recon-
structions with correlated neuro-imaging. Thieme, Stuttgart,pp 110117
99. Kunzle H (1977) Projections from theprimary somatosensory cortex to bas-al ganglia and thalamus in the mon-key. Exp Brain Res 30:481491
100. Laplane D, Baulac M, Widlocher D,Dubois B (1984) Pure psychic akine-sia with bilateral lesions of basal gan-glia. J Neurol Neurosurg Psychiatry47:377385
101. Laplane D, Levasseur M, Pillon B,Dubois B, Baulac M, Mazoyer B,Tran Dinh S, Sette G, Danze F,Baron JC (1989) Obsessive-compul-sive and other behavioural changeswith bilateral basal ganglia lesions.A neuropsychological, magnetic reso-nance imaging and positron tomogra-phy study. Brain 112:699725
102. Lawrence AD (2000) Error correctionand the basal ganglia: similar compu-tations for action, cognition and emo-tion? Trends Cogn Sci 4:365367
103. Lee MS, Marsden CD (1994) Move-ment disorders following lesions of the thalamus or subthalamic region.Mov Disord 9:493507
104. Lee MS, Rinne JO, Ceballos-Baumann A, Thompson PD,Marsden CD (1994) Dystonia afterhead trauma. Neurology44:13741378
105. Lenz FA, Byl NN (1999) Reorganiza-tion in the cutaneous core of the hu-man thalamic principal somatic senso-ry nucleus (Ventral caudal) in patientswith dystonia. J Neurophysiol82:32043212
106. Lenz FA, Dougherty PM (1998) Neu-rons in the human thalamic somato-sensory nucleus (Ventralis caudalis)respond to innocuous cool and me-chanical stimuli. J Neurophysiol79:22272230
107. Lenz FA, Jaeger CJ, Seike MS,Lin YC, Reich SG, DeLong MR,Vitek JL (1999) Thalamic single neu-ron activity in patients with dystonia:dystonia-related activity and somaticsensory reorganization. J Neuro-physiol 82:23722392
108. Lera G, Scipioni O, Garcia S,Cammarota A, Fischbein G,Gershanik O (2000) A combined pat-tern of movement disorders resultingfrom posterolateral thalamic lesionsof a vascular nature: a syndrome withclinico-radiologic correlation. MovDisord 15:120126
109. Levy R, Herrero MT, Ruberg M,Villares J, Faucheux B, Guridi J,Guillen J, Luquin MR, Javoy-Agid F,Obeso JA, Agid Y, Hirsch EC (1995)Effects of nigrostriatal denervationand l-DOPA therapy on the GABA-ergic neurons of the striatum inMPTP-treated monkeys and Parkin-
sons disease. Eur J Neurosci7:11991209110. Levy R, Hazrati LN, Herrero MT,
Vila M, Hassani OK, Mouroux M,Ruberg M, Asensi H, Agid Y, Feger J,Obeso JA, Parent A, Hirsch EC(1997) Re-evaluation of the functionalanatomy of the basal ganglia in nor-mal and parkinsonian states. Neuro-science 76:335343
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
17/19
402
111. Liu X, Aziz TZ, Miall RC, Rowe J,Alusi SH, Bain PG, Stein JF (2000)Frequency analysis of involuntarymovements during wrist tracking: away to identify MS patients withtremor who benefit from thalamoto-my. Stereotact Funct Neurosurg74:5362
112. Litvan I, Dickson DW, Buttner-Ennever JA, Delacourte A, Hutton M,Dubois B, Golbe LI, Hallet M,Schellenberg GD, Standert D,Brooks DJ, Price D, et al (2000) Re-search goals in progressive supranu-clear palsy. Mov Disord 15:446458
113. Lozano A, Linazasoro G (2000) Sur-gical treatment of dystonia. Rev Neu-rol 30:10731076
114. Lozano AM, Lang AE, HutchinsonWD, Dostrowsky JO (1998) New de-velopments in understanding the etiol-ogy of Parkinsons disease and itstreatment. Curr Opin Neurobiol8:783790
115. Lumer ED, Edelman GM, Tononi G(1997) Neural dynamics in a model of the thalamocortical system. I. Layers,loops and the emergence of fast syn-chronous rhythms. Cereb Cortex7:207227
116. Lytton WW, Destexhe A, SejnowskiTJ (1996) Control of slow oscillationsin the thalamocortical neuron: a com-puter model. Neuroscience70:673684
117. Macchi G, Bentivoglio M (1999) Isthe nonspecific thalamus still non-specific? Arch Ital Biol 137:201226
118. Macchi G, Jones EG (1997) Towardsan agreement on terminology of nu-clear and subnuclear divisions of themotor thalamus. J Neurosurg86:670685
119. Maraganore DM, Lees AJ, MarsdenCD (1991) Complex stereotypies afterright putaminal infarction: a case re-port. Mov Disord 6:358361
120. Marsden JF, Ashby P, Limousin-Dowsey P, Rothwell JC, Brown P(2000) Coherence between cerebellarthalamus, cortex and muscle in man:cerebellar thalamus interactions.Brain 123:14591470
121. Martin JP (1927) Hemichorea result-ing from a local lesion of the brain(the syndrome of the body of Luys).Brain 50:637651
122. Martin JP (1957) Hemichorea (hemi-ballismus) without lesions in the cor-pus Luysii. Brain 80:110
123. Mas JL, Launay M, Derouesne C(1987) Hemiballism and CT-docu-mented lacunar infarct in the lenticu-lar nucleus. J Neurol Neurosurg Psy-chiatry 50:104105
124. Miyai I, Suzuki T, Kang J, Volpe BT(2000) Improved functional outcomein patients with hemorrhagic stroke inputamen and thalamus compared withthose with stroke restricted to the put-amen or thalamus. Stroke31:13651369
125. Moreaud O, Pellat J, Charnallet A,Carbonell S, Brennen T (1995) Dfi-cit de la production et de lapprentiss-age des noms propres aprs lsion is-chemique tubero-thalamique gauche.Rev Neurol 151:9399
126. Morel A, Magnin M, Jeanmonod D(1997) Multiarchitectonic and stereo-tactic atlas of the human thalamus.J Comp Neurol 387:588630
127. Morrow TJ, Casey KL (1992) State-related modulation of thalamicsomatosensory responses in theawake monkey. J Neurophysiol67:305317
128. Mrabet A, Mrad-Ben Hammouda I,Abroug Z, Smiri W, Haddad A (1994)Infarctus bilatral des noyaux cauds.Rev Neurol 150:6769
129. Munkle MC, Waldvogel HJ, Faull RL(1999) Calcium-binding protein im-munoreactivity delineates the intra-laminar nuclei of the thalamus in thehuman brain. Neuroscience90:485491
130. Nakano K (2000) Neural circuits andtopographical organization of the bas-al ganglia and related regions. BrainDev 22:S5-S16
131. Nakano K, Kayahara T, Tsutsumi T,Ushiro H (2000) Neural circuits andfunctional organization of the stria-tum. J Neurol 247:115
132. Nauta WJH, Mehler WR (1966)Projections from the lentiformnucleus in the monkey. Brain Res1:342
133. Neau JP, Bogousslavsky J (1996) Thesyndrome of posterior choroidal ar-tery territory infarction. Ann Neurol39:779788
134. Nisbet AP, Foster OJ, Kingsbury A,Lees AJ, Marsden CD (1994) Nitricoxide synthase mRNA expression inhuman subthalamic nucleus, striatumand globus pallidus: implications forbasal ganglia function. Mol Brain Res22:329332
135. Nowinski WL (1998) Anatomical tar-geting in functional neurosurgery by
the simultaneous use of multipleSchaltenbrand-Wahren brain atlas mi-croseries. Stereotact Funct Neurosurg71:103116
136. Ogawa K, Toita T, Kakinohana Y,Tominaga D, Miyagi K, Yoshii Y,Horikawa A, Sawada S (1999) A pa-tient with improvement in short-termmemory disturbance brought about byradiation therapy for germinoma in-volving Papez circuit. Radiat Med17:317322
137. Ohye C (1986) Rle des noyaux thal-amiques dans lhypertonie et le trem-blement de la maladie de Parkinson.Rev Neurol 142:362367
138. Ohye C, Hirai T, Miyazaki M,Shibazaki T, Nakajima H (1982) Vimthalamotomy for the treatment of var-ious kinds of tremor. Appl Neuro-physiol 45:245250
139. Ohye C, Shibazaki T, Hirai T,Kawashima Y, Hirato M, MatsumuraM (1985) Plastic change of the tha-lamic organization in the cases withtremor after stroke. Appl Neuro-physiol 61:488500
140. Olszewski J (1952) The thalamus of Macaca Mulatta . An atlas for usewith the stereotaxic instruments.Karger, Basel
141. Ongur D, Price JL (2000) The organi-zation of networks within the orbitaland medial prefrontal cortex of rats,monkeys and humans. Cereb Cortex10:206219
142. Pakkenberg B (1993) Leucotomizedschizophrenics loss neurons in themediodorsal nucleus. NeuropatholAppl Neurobiol 19:373380
143. Papez JW (1937) A proposed mecha-nism of emotion. Arch Neurol Psychi-atry 38:725743
144. Pare D, Steriade M (1993) The reticu-lar thalamic nucleus projects to thecontralateral dorsal thalamus in ma-caque monkey. Neurosci Lett154:96100
145. Parent A (1990) Extrinsic connectionsof the basal ganglia. Trends Neurosci13:254258
146. Parent A, Hazrati LN (1993) Anatom-ical aspects of information processingin primate basal ganglia. Trends Neu-rosci 16:111116
147. Parent A, Sato F, Wu Y, Gauthier J,Lvesque M, Parent M (2000) Organi-zation of the basal ganglia: the impor-tance of axonal collateralization.Trends Neurosci 23:S20-S27
148. Parker A, Eacott MJ, Gaffan D (1997)The recognition memory deficitcaused by mediodorsal thalamic le-sion in non-human primates: a com-parison with rhinal cortex lesion. EurJ Neurosci 9:24232431
149. Pepin EP, Auray-Pepon L (1993) Se-lective dorsolateral frontal lobe dys-function associated with diencephalic
amnesia. Neurology 43:733741150. Percheron G (1982) Arterial supply of the thalamus. In: Schaltenbrand G,Walker AE (eds) Stereotaxy of the hu-man brain, 2nd edn. Thieme,Stuttgart, pp 218232
-
8/11/2019 Anatomia Talamo y Gangliobasal (1)
18/19
403
151. Percheron G, Francois C, Talbi B,Meder JF, Fenelon G, Yelnik J (1991)The primate motor thalamus analyzedwith reference to subcortical afferentterritories. Stereotact Funct Neurosurg93:3241
152. Percheron G, Fenelon G, Leroux-Hugon V, Feve A (1994) History of the basal ganglia system. Slow devel-opment of a major cerebral system.Rev Neurol 150:543554
153. Percheron G, Franois C, Yelnik J,Fnelon G, Talbi B (1994) The basalganglia related system of primates:definition, description and informa-tional analysis. In: Percheron G,Mckenzie JS, Feger J (eds) The basalganglia IV. Plenum, New York,pp 320
154. Percheron G, Franois C, Talbi B,Yelnik J, Fnelon G (1996) The pri-mate motor thalamus. Brain Res Rev22:93181
155. Pitman RK (1987) A cybernetic mod-el of obsessive-compulsive psychopa-thology. Comp Psychiatry28:334343
156. Plenz D, Kitai ST (1999) A basal gan-glia pacemaker formed by the subtha-lamic nucleus and external globuspallidus. Nature 400:677682
157. Poellinger A, Thomas R, Lio P,Lee A, Makris N, Rosen BR,Kwong KK (2001) Activation and ha-bituation in olfaction an fMRIstudy. Neuroimage 13:547560
158. Postle BR, Corkin S, Jonides J,Smith EE, Growdon JH (1997) Spa-tial, but not object, delayed responseis impaired in early Parkinsons dis-ease. Neuropsychology 11:171179
159. Puelles L, Rubinstein JL (1993) Ex-pression patterns of homeobox andother putative regulatory genes in theembryonic mouse forebrain suggest aneuromeric organization. Trends Neu-rosci 16:472479
160. Raeva S (1986) Localization in hu-man thalamus of units triggered dur-ing verbal commands, voluntarymovements and tremor. Electroencep-halogr Clin Neurophysiol 63:160173
161. Ralston HJ, Ralston DD (1992) Theprimate dorsal spinothalamic tract:evidence for a specific termination inthe posterior nuclei (Po/SG) of thethalamus. Pain 48:107118
162. Ralston HJ, Ralston DD (1994) Medi-al lemniscal and spinal projections tothe macaque thalamus: an electronmicroscopic study of differingGABAergic circuitry serving thalamicsomatosensory mechanisms. J Neuro-sci 14:24852502
163. Ray JP, Price JL (1993) The organiza-tion of projections from the medio-dorsal nucleus of the thalamus to or-bital and medial prefrontal cortex inmacaque monkeys. J Comp Neurol337:13
164. Ray JP, Russchen FT, Fuller TA,Price JL (1992) Sources of presump-tive glutamatergic/aspartatergic affer-ents to the mediodorsal nucleus of thethalamus in the rat. J Comp Neurol320:435456
165. Redgrave P, Prescott TJ, Gurney K(1999) The basal ganglia: a vertebratesolution to the selection problem?Neuroscience 89:10091023
166. Rogers RD, Andrews TC, GrasbyPM, Brooks DJ, Robbins TW (2000)Contrasting cortical and subcorticalactivations produced by attentional-set shifting and reversal learning inhumans. J Cogn Neurosci 12:142162
167. Rolls ET (1994) Neurophysiology andcognitive functions of the striatum.Rev Neurol 150:648660
168. Sadikot AF, Parent A, Franois C(1992) Efferent connections of thecentromedian and parafascicular tha-lamic nuclei in the squirrel monkey: aPHA-L study of subcortical projec-tions. J Comp Neurol 315:137159
169. Sakai ST, Patton K (1993) Distribu-tion of cerebellothalamic and nigro-thalamic projections in the dog: adouble anterograde tracing study.J Comp Neurol 330:183194
170. Sakai ST, Stepniewska I, Qi HX,Kaas JH (2000) Pallidal and cerebel-lar afferents to pre-supplementarymotor area thalamocortical neurons inthe owl monkey: a multiple labelingstudy. J Comp Neurol 417:164180
171. Salinas E, Opris I, Zainos A,Hernandez A, Romo R (2000) Motorand non motor roles of the corticobasal ganglia circuitry. In: Miller R,Wickens J (eds) Brain dynamics andthe striatal complex. Conceptual ad-vances in brain research, vol 1. Har-wood Academic, pp 237255
172. Schultz W, Dayan P, Montague PR(1997) A neural substrate of predictionand reward. Science 275:15931599
173. Selden N, Geula C, Hersch L,Mesulam MM (1994) Human stria-tum: chemoarchitecture of the caudatenucleus, putamen and ventral striatum
in health and Alzheimers disease.Neuroscience 60:621636174. Selemon LD, Goldman-Rakic PS
(1985) Longitudinal topography andinterdigitation of corticostriatal pro-
jections in the rhesus monkey. J Neu-rosci 5:776794
175. Shintani S, Tsuruoka S, Shiigai T(2000) Pure sensory stroke caused bya cerebral hemorrhage: clinical-radio-logic correlations in seven patients.Am J Neuroradiol 21:515520
176. Sidibe M, Bevan MD, Bolam JP,Smith Y (1997) Efferent connectionsof the internal globus pallidus in thesquirrel monkey. I. Topography andsynaptic organization of the pallido-thalamic projection. J Comp Neurol382:323347
177. Smith Y, Kieval JZ (2000) Anatomyof the dopamine system in the basalganglia. Trends Neurosci 23:S28S33
178. Smith Y, Bennett BD, Bolam JP,Parent A, Sadikot AF (1994) Synapticrelationships between dopaminergicafferents and cortical or thalamic