UNIVERSIDADE ESTADUAL DE CAMPINAS DORA ZULEMA … · Biologia Buco-Dental, na área de Anatomia....
43
UNIVERSIDADE ESTADUAL DE CAMPINAS FACULDADE DE ODONTOLOGIA DE PIRACICABA DORA ZULEMA ROMERO DIAZ ESTUDO ULTRASSONOGRÁFICO DE ESTRUTURAS ANATÔMICAS DA ARTICULAÇÃO TEMPOROMANDIBULAR EM INDIVÍDUOS COM E SEM DISFUNÇÃO TEMPOROMANDIBULAR ULTRASONOGRAPHIC STUDY OF ANATOMICAL STRUCTURES OF TEMPOROMANDIBULAR JOINT IN INDIVIDUALS WITH AND WITHOUT TEMPOROMANDIBULAR DISORDERS Piracicaba 2017
Transcript of UNIVERSIDADE ESTADUAL DE CAMPINAS DORA ZULEMA … · Biologia Buco-Dental, na área de Anatomia....

UNIVERSIDADE ESTADUAL DE CAMPINAS
FACULDADE DE ODONTOLOGIA DE PIRACICABA
DORA ZULEMA ROMERO DIAZ
ESTUDO ULTRASSONOGRÁFICO DE ESTRUTURAS ANATÔMICAS DA
ARTICULAÇÃO TEMPOROMANDIBULAR EM INDIVÍDUOS COM E SEM
DISFUNÇÃO TEMPOROMANDIBULAR
ULTRASONOGRAPHIC STUDY OF ANATOMICAL STRUCTURES OF
TEMPOROMANDIBULAR JOINT IN INDIVIDUALS WITH AND WITHOUT
TEMPOROMANDIBULAR DISORDERS
Piracicaba
2017

DORA ZULEMA ROMERO DIAZ
ESTUDO ULTRASSONOGRÁFICO DE ESTRUTURAS ANATÔMICAS DA
ARTICULAÇÃO TEMPOROMANDIBULAR EM INDIVÍDUOS COM E SEM
DISFUNÇÃO TEMPOROMANDIBULAR
ULTRASONOGRAPHIC STUDY OF ANATOMICAL STRUCTURES OF
TEMPOROMANDIBULAR JOINT IN INDIVIDUALS WITH AND WITHOUT
TEMPOROMANDIBULAR DISORDERS
Piracicaba
2017
Dissertação apresentada à Faculdade de Odontologia de
Piracicaba da Universidade Estadual de Campinas, como parte
dos requisitos exigidos para a obtenção do titulo de Mestra em
Biologia Buco-Dental, na área de Anatomia.
Dissertation presented to the Piracicaba Dental School of the
University of Campinas in partial fulfillment of the requirements
for the degree of Master in Oral Biology, in Anatomy area.
Orientadora: Profa. Dra. Maria Beatriz Duarte Gavião
Este exemplar corresponde à versão final da dissertação
defendida pela aluna Dora Zulema Romero Diaz e
orientada pela Profa. Dra. Maria Beatriz Duarte Gavião.

Agência(s) de fomento e nº(s) de processo(s): CAPES
Ficha catalográfica
Universidade Estadual de Campinas Biblioteca da
Faculdade de Odontologia de Piracicaba Marilene
Girello - CRB 8/6159
Diaz, Dora Zulema Romero, 1987-
D543e Estudo ultrassonográfico de estruturas anatômicas da articulação
temporomandibular em indivíduos com e sem disfunção temporomandibular / Dora
Zulema Romero Diaz. – Piracicaba, SP : [s.n.], 2017.
Orientador: Maria Beatriz Duarte Gavião.
Dissertação (mestrado) – Universidade Estadual de Campinas, Faculdade de
Odontologia de Piracicaba.
1. Ultrassonografia. 2. Articulação temporomandibular. 3. Anatomia. I.
Gavião, Maria Beatriz Duarte,1955-. II. Universidade Estadual de Campinas.
Faculdade de Odontologia de Piracicaba. III. Título.
Informações para Biblioteca Digital
Título em outro idioma: Ultrasonographyc study of anatomical structures of
temporomandibular joint in individuals with and without temporomandibular disorders
Palavras-chave em inglês:
Ultrasonography
Temporomandibular joint
Anatomy
Área de concentração: Anatomia
Titulação: Mestra em Biologia Buco-Dental
Banca examinadora:
Maria Beatriz Duarte Gavião [Orientador]
Polliane Morais de Carvalho
Ana Cláudia Rossi
Data de defesa: 04-08-2017
Programa de Pós-Graduação: Biologia Buco-Dental

UNIVERSIDADE ESTADUAL DE CAMPINAS
Faculdade de Odontologia de Piracicaba
A Comissão Julgadora dos trabalhos de Defesa de Dissertação de Mestrado, em sessão
pública realizada em 04 de Agosto de 2017, considerou a candidata DORA ZULEMA
ROMERO DIAZ aprovada.
PROFa. DR
a. MARIA BEATRIZ DUARTE GAVIÃO
PROFa. DR
a. POLLIANE MORAIS DE CARVALHO
PROFa. DR
a. ANA CLÁUDIA ROSSI
A Ata de defesa com as respectivas assinaturas dos membros encontra-se no processo
de vida acadêmica do aluno.

DEDICATÓRIA
Dedico este trabalho a:
DEUS, meu Pai, que foi minha fortaleza nos momentos mais difíceis, por
NUNCA ter me deixado mesmo nas horas de angústia e solidão. Por ter me abençoado
com a dádiva da vida, a coragem de aproveitar as oportunidades que ele me apresentou
e pela felicidade de realizar todos os meus sonhos.
María Zulema Díaz, minha mãe, que mesmo não compreendendo a natureza
do meu trabalho, sempre me apoiou de forma INCONDICIONAL e me moldou no que
hoje sou.
A eles sou imensamente grata!

AGRADECIMENTOS
Agradeço acima de tudo a DEUS, pela vida e pela benção concedida de
terminar o meu mestrado.
À Universidade Estadual de Campinas, na pessoa do Magnifico Reitor Prof.
Dr. Marcelo Knobel.
À Faculdade de Odontologia de Piracicaba, na pessoa do senhor Diretor,
Prof. Dr. Guilherme Elias Pessanha Henriques.
À Coordenadoria de Pós-graduação, na pessoa da Senhora Coordenadora
Profa. Dra. Cinthia Pereira Machado Tabchoury.
Ao Programa de Pós-graduação em Biologia Buco-Dental, na pessoa da
Coordenadora Profa. Dra. Maria Beatriz Duarte Gavião.
A minha orientadora Profa. Dra. Maria Beatriz Duarte Gavião, por ter me
ajudado e apoiado em todos os momentos, mesmo diante de toda dificuldade, agradeço
imensamente pela participação ativa e direta neste passo gigantesco a caminho da
construção de minha carreira profissional, muito obrigada!
À Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – CAPES
pela da bolsa de estudos concedida.
Ao Prof. Dr. Luciano José Pereira, pelo treinamento com o ultrassom.
Ao Prof. Dr. Yuri Martins Costa, por ter compartilhado o seu conhecimento
durante o treinamento para o preenchimento do índice DC/TMD.
Ao Prof. Paulo Henrique Caria, pelos seus ensinamentos, conselhos e
criticas nos seminários, que me modelaram na minha formação acadêmica.

À Profa. Dra. Ana Claudia Rossi, pelos ensinamentos durante o programa
de estágio docente os quais me permitiram desenvolver uma das minhas paixões,
ensinar.
A Florence Cuadra, pela amizade que me motiva ser uma pessoa melhor,
que me inspira ser boa profissional. Sou grata pela ajuda incondicional: você foi o anjo
que Deus colocou na minha vida.
A todos os voluntários que dispuseram do seu tempo, história e
sintomatologia para o desenvolvimento científico deste trabalho.
A Cristina Emöke Erika Müller, pela amizade, ajuda fundamental e peça
imprescindível para a realização desta obra.
A Mariana Fernandes dos Santos, pela sua amizade e pelo carinho que me
deu desde que nós conhecemos, pelas nossas conversas e pelos conselhos.
A Sra. Leni Aparecida Garcia de Brito e ao Sr. Valdir Francisco de Brito,
meus pais em Piracicaba, muito obrigada pela sua ajuda e apoio, os senhores foram uma
benção na minha vida.
Agradeço a Deus por ter colocado aos meus amigos “estrangeiros” na minha
vida, sou muito grata por todos os momentos que passamos juntos sempre estarão
guardados comigo, mesmo que o tempo passe e a distância seja grande; vocês fizeram
minha estadia mais leve e me apoiaram quando necessitei!

RESUMO
O objetivo desse estudo foi descrever estruturas anatômicas da articulação
temporomandibular (ATM) pela ultrassonografia. O estudo caracterizou-se como
observacional-descritivo de tipo transversal e comparativo. Participaram 32 indivíduos
(17 do sexo feminino e 15 do sexo masculino) na faixa etária de 19 a 39 anos.
Aplicaram-se os critérios diagnósticos para disfunção temporomandibular (DC/TMD),
dividindo os voluntários em grupo DTM com 20 voluntários e grupo assintomático com
12 voluntários. Portanto, foram avaliadas 64 articulações temporomandibulares pela
ultrassonografia de alta resolução do lado direito e esquerdo na posição de boca-fechada
(BF) e boca-aberta (BA), por um único examinador treinado e calibrado (Kappa=0,7).
As estruturas avaliadas foram a cabeça da mandíbula, o disco articular, o espaço supra e
infradiscal e a cápsula articular. Além disso, mensurou-se a distância entre o ponto mais
lateral da cápsula articular e o ponto mais lateral da cabeça da mandíbula (distância
lateral cápsula-cabeça da mandíbula) nas posições de BF e BA. As respectivas medidas
foram comparadas entre os grupos, aplicando-se os testes t de Student pareado e não
pareado (α=0,05). As imagens ultrassonográficas possibilitaram visualizar o polo lateral
da cabeça da mandíbula como uma imagem hiperecóica; o disco articular como uma
imagem hiperecogênica central rodeada por uma imagem linear superior e inferior
hipoecoica, o espaço supra e infradiscal respectivamente; a borda superior da cápsula
articular como uma imagem linear hiperecóica. As médias da distância lateral cápsula-
cabeça da mandíbula no lado direito no grupo DTM foram 0,69±0,19 mm em BF e
0,61±0,15 mm em BA e no grupo assintomático 0,71±0,16 mm e 0,63±0,16 mm,
respectivamente. No lado esquerdo, as medidas em BF para o grupo DTM foi 0,68±0,15
mm e no grupo assintomático 0,70±0,14 e em BA 0,64±0,15 mm para o grupo DTM e
no grupo assintomático 0,66±0,15. Perante os resultados encontrados, pode-se
considerar a Ultrassonografia como uma ferramenta promissora e viável para avaliação
da ATM. As mensurações da distancia cápsula-cabeça da mandíbula não diferiu entre o
grupo TMD e o grupo assintomático.
Palavras-chaves: Ultrassonografia, Articulação temporomandibular, Anatomia.

ABSTRACT
The purpose of this study was to describe anatomic structures of the
temporomandibular joint (TMJ) by high-resolution ultrasonography. The study was
characterized as observational-descriptive, cross-sectional and comparative. Participants
were 32 volunteers (17 females and 15 males) in the age of 19 to 39 years. Diagnostic
criteria for temporomandibular dysfunction (CD/TMD) were applied, and the volunteers
were divided in two groups, TMD group of 20 volunteers and an asymptomatic group of
12 volunteers. Therefore, 64 temporomandibular joints were evaluated by high-
resolution ultrasonography on the right and left side in the closed- mouth (CM) and
open-mouth (OM) positions, by a single trained and calibrated examiner (Kappa = 0.7).
The evaluated structures were the mandibular condyle, the articular disc, the supra and
infradiscal spaces and the upper edge of the articular capsule. In addition, the distances
between the most lateral point of the articular capsule and the most lateral point of the
mandibular condyle (lateral capsule-condyle distance) at the CM and OM positions
were measured. The respective measurements were compared between the groups,
applying paired and unpaired Student t tests (α = 0.05). Ultrasound imaging made it
possible to visualize the articular surface of the mandibular condyle as a hyperechoic
image; the articular disc as a central hyperechogenic image surrounded by a hypoechoic
linear image; the upper border of the articular capsule as a linear hyperechoic image.
The averages of lateral capsule-mandibular condyle distance on the right side in the
TMD group were 0.69±0.19 mm in CM and 0.61±0.15 mm in OM and in the
asymptomatic group 0.71±0.16 mm and 0.63±0.16 mm, respectively. On the left side,
the CM measurements for the TMD group were 0.68±0.15 mm and in the asymptomatic
group 0.70±0.14 and in the OM 0.64±0.15 mm for the TMD group and in the
asymptomatic group 0.66±0.15. Given the results found, Ultrasonography can be
considered as a promising and feasible tool for the assessment of TMJ. The distance
from the most lateral point of the articular capsule to the most lateral point of the
mandibular condyle (lateral capsule-condyle distance), measured on the
ultrasonographic scans, did not differ between TMD group and asymptomatic group.
Keywords: ultrasonography, temporomandibular joint, anatomy.

LISTA DE ILUSTRAÇÕES
Figura 1 - Transducer positioned against the patient’s face, perpendicular
to the Frankfort horizontal plane and parallel to the mandibular
ramus
Figura 2 - Flow chart
Figura 3 - Ultrasonography scan of the left temporomandibular joint in
closed- mouth position in transversal/axial slice of a volunteer
of the TMD group
Figura 4 - Ultrasonography scan of the right temporomandibular joint in
open-mouth position in transversal/axial slice of a volunteer of
the TMD group
Figura 5 - Measurement of the distance between the most lateral point of
the articular capsule and the most lateral point of the
mandibular condyle (lateral capsule-condyle distance) in
ultrasonographic scan of the right temporomandibular joint in
closed-mouth of a volunteer of the TMD group
Figura 6 - Measurement of the distance between the most lateral point of
the articular capsule and the most lateral point of the
mandibular condyle (lateral capsule-condyle distance) in
ultrasonographic scan of the right temporomandibular joint in
open-mouth of a volunteer of the TMD group

LISTA DE TABELAS
Tabela 1 – Sample distribution according to sex and DC/TMD
Tabela 2 – Measurement of the distance between the most lateral point of the
articular capsule and the most lateral point of the mandibular
condyle (lateral capsule-condyle distance) in the
Temporomandibular disorders group and asymptomatic group
(mm)
Tabela 3 – Measurement of the distance between the most lateral point of the
articular capsule and the most lateral point of the mandibular
condyle (lateral capsule-condyle distance) in the volunteers with
intra-articular disorders and asymptomatic group (mm)

LISTA DE ABREVIATURAS E SIGLAS
DTM - Disfunção Temporomandibular
US - Ultrassonografia / Ultrasonography
DC/TMD - Diagnostic Criteria for Temporomandibular Disorders
TMD - Temporomandibular Disorders
ATM - Articulação temporomandibular
ATMs - Articulações temporomandibulares
TMJ - Temporomandibular joint
MHz - Megahertz
mm - Milímetros

SUMÁRIO
1 INTRODUÇÃO ................................................................................................. 14
2 ARTIGO Ultrasonography of anatomical structures of
temporomandibular joint in individual with and without
temporomandibular disorders ……………………………...
17
3 CONCLUSÃO .................................................................................................. 35
REFERÊNCIAS
APÊNDICES
Apêndice 1 Ficha de avaliação
Apêndice 2 Ficha de avaliação dos dados ultrassonográficos
ANEXOS
Anexo 1 Certificado do Comitê de Ética em Pesquisa com seres
humanos da FOP - UNICAMP
Anexo 2 DC/TMD

14
1 INTRODUÇÃO
A Articulação temporomandibular (ATM) é uma das articulações sinoviais mais
complexas do corpo humano e apresenta como componentes ósseos a fossa mandibular na
porção petrosa do osso temporal e a cabeça da mandíbula. Possui um disco articular de
fibrocartilagem localizado entre ambas as estruturas ósseas permitindo melhor adaptação
entre elas, fixando-se nos polo medial e lateral da cabeça da mandíbula para acompanha-la
durante os movimentos; divide o espaço articular em dois compartimentos: o espaço
supradiscal e infradiscal. A cápsula articular estende-se dos limites da superfície articular
craniana em direção inferior para o colo da mandíbula, circundando assim toda a ATM.
Também apresenta ligamentos extracapsulares que restringem os movimentos mandibulares
para evitar possíveis danos nas estruturas (Alomar et al., 2007).
Quando a cavidade bucal se encontra fechada, a cabeça da mandíbula deve estar
situada na região central da fossa mandibular; a posição do disco articular é considerada
normal quando a porção posterior e se localiza entre 12 e 13 horas na superfície articular, a
porção central do disco posiciona-se na face anterior superior da superfície articular da cabeça
da mandíbula (Mello-Júnior et al., 2011).
Hábitos parafuncionais como ranger e/ou apertar os dentes podem alterar as relações
de normalidade das estruturas anatômicas e, consequentemente, gerar disfunções na
articulação temporomandibular (DTM) com o passar do tempo.
A DTM refere-se a um conjunto complexo de condições que podem se manifestar com
dor na região das articulações e limitações nos movimentos normais de abertura e fechamento
da boca. De acordo com Schiffmanet et al. (2014), os principais sintomas incluem clique,
crepitação, redução ou dificuldade na capacidade de fazer os movimentos mandibulares, dor
na área da articulação e nos músculos da mastigação. Além disso, pode ocorrer posição
anormal do disco articular em relação à cabeça da mandíbula e da fossa mandibular gerando
deslocamento anormal durante os movimentos mandibulares (Emshoff et al., 2002,
Melchiorre et al., 2010, Mello-Júnior et al., 2011).
A abordagem dos pacientes que sofrem de DTM começa com o diagnóstico completo,
incluindo um minucioso exame clínico. O Diagnostic Criteria for Temporomandibular

15
Disorders (DC/TMD) é um dos protocolos mais indicado para o diagnóstico da DTM, pois é
um método de avaliação com critérios claramente definidos, simples de aplicar e de fácil
pontuação (Schiffman et al., 2014). As imagens das ATMs podem ser indicadas para
completar o diagnóstico da disfunção (Kundu et al., 2013). A finalidade das imagens da ATM
consiste em avaliar a integridade e a relação dos tecidos duros e moles, e observar o progresso
da alteração (Byahatti et al., 2010).
Os métodos mais usados para a obtenção das imagens da ATM incluem a ressonância
magnética, a tomografia computadorizada, a artrografia, a radiografia panorâmica e
ultrassonografia (US). O padrão ouro para a avaliação da articulação é a ressonância
magnética, porém a sua disponibilidade é relativamente baixa devido a seu elevado custo, uso
restrito em indivíduos com marcapassos, próteses e claustrofóbicos. Nas ultimas duas década,
autores como Hayashi et al. (2001), Emshoff et al. (2002), Pereira et al. (2007), Byahatti et al.
(2010) e Assaft et al. (2013), mostraram que a US pode ser uma ferramenta promissora e
viável na avaliação das estruturas anatômicas da ATM.
A imagem ultrassonográfica se forma quando um grupo de elementos piezoelétricos
localizados dentro do transdutor (emissor/receptor.), ao receber energia elétrica, vibram,
produzindo um pulso que gera milhares de ecos, os quais atingem os tecidos corporais, parte
deste eco é refletida de volta para os elementos piezoelétricos, os quais o transformam em
sinais que serão visualizados na tela do equipamento de ultrassom em diversas escalas de
cinza de acordo com a ecogenicidade do tecido. Parte das ondas remanescentes continuam seu
caminho, gerando ecos adicionais, até que a energia inicial seja totalmente dissipada. A
ecogenicidade do tecido depende das características estruturais como espessura, largura,
comprimento, quantidade de gordura e água presente; assim, os tecidos que geram ecos de
onda de alta freqüência aparecerão mais brilhantes – hiperecóicos (branco) - no monitor.
Aqueles que produzem poucos ecos de onda de baixa freqüência aparecerão hipoecóicos
(cinza). Os pulsos de frequência mais baixa podem caminhar mais facilmente e gerar ecos que
retornam mais facilmente ao transdutor gerando mais sinal do tecido, porém os detalhes da
imagem podem ser de baixa resolução. A idéia é usar a onda com frequência mais alta
possível que permite alcançar a área de interesse com sinal suficiente para visualizar maiores
detalhes do tecido, isto é, com alta resolução. A US permite visualizar o movimento das
estruturas por que os ecos gerados são rápidos, aproximadamente a 1540 m/seg nos tecidos
moles, o que permite visualizar a imagem 30 vezes por segundo (van Holsbeeck et al., 2001).

16
Sendo assim, a US como método de diagnóstico por imagem uma técnica não invasiva usada
no âmbito clinico por ser de rápida execução e de baixo custo, com a vantagem de permitir
avaliar as estruturas em “tempo real”.
Com o decorrer dos anos e o avanço da tecnologia, surgiram novos equipamentos de
ultrassonografia com transdutores de maior resolução, capazes de transmitir sinais mais claros
que possibilitam melhor visualização das estruturas anatômicas do corpo para prover ao
paciente um diagnóstico preciso. Para o aproveitamento dessas novas tecnologias se faz
necessário estudos que mostrem a sua utilidade na pratica clinica. Nesse sentido, o objetivo
desta pesquisa foi descrever estruturas anatômicas que compõem a articulação
temporomandibular, como a cabeça da mandíbula, o disco articular, o espaço supra e
infradiscal, e a cápsula articular, além disso, a mensuração da distância entre o ponto mais
lateral da cápsula articular e o ponto mais lateral da cabeça da mandíbula (distância lateral da
cápsula-cabeça da mandíbula) nas posições de boca fechada e boca aberta, pela
ultrassonografia de alta resolução em voluntários com sinais e sintomas de disfunção
temporomandibular, comparando-os com voluntários assintomáticos.

17
2 ARTIGO
ULTRASONOGRAPHIC STUDY OF ANATOMICAL STRUCTURES OF
TEMPOROMANDIBULAR JOINT IN INDIVIDUALS WITH AND WITHOUT
TEMPOROMANDIBULAR DISORDERS
Dora Zulema Romero Diaz1, Cristina Emöke Erika Müller
1, Maria Beatriz Duarte Gaviao*
2.
1Department of Morphology, Piracicaba Dental School, University of Campinas
2Department of Pediatric dentistry, Piracicaba Dental School, University of Campinas
*Correspondence to:
Prof. Maria Beatriz Duarte Gavião
Faculdade de Odontologia de Piracicaba, Universidade Estadual de Campinas
Address: Av. Limeira 901, Bairro Areião, CEP 13414-903, Piracicaba, SP, Brasil
E-mail: [email protected]
Artigo submetido ao periódico Dentomaxillofacial Radiology

18
Abstract
The purpose of this study was to describe anatomic structures of the
temporomandibular joint (TMJ) by high-resolution ultrasonography. The study was
characterized as observational-descriptive, cross-sectional and comparative. Participants were
32 volunteers (17 females and 15 males) in the age of 19 to 39 years. Diagnostic criteria for
temporomandibular dysfunction (DC/TMD) were applied, and the volunteers were divided in
two group, TMD group of 20 volunteers and asymptomatic group of 12 volunteers. Therefore,
64 temporomandibular joints were evaluated by high-resolution ultrasonography on the right
and left side in the closed-mouth (CM) and open-mouth (OM) positions, by a single trained
and calibrated examiner (Kappa = 0.7). The evaluated structures were the mandibular
condyle, the articular disc, the supra and infradiscal spaces and the articular capsule. In
addition, the distances between the most lateral point of the articular capsule and the most
lateral point of the mandibular condyle (lateral capsule-condyle distance) at the CM and OM
positions were measured. The respective measurements were compared between the groups,
applying paired and unpaired Student t tests (α = 0.05). Ultrasound imaging made it possible
to visualize the articular surface of the mandibular condyle as a hyperechoic image; the
articular disc as a central hyperechogenic image surrounded by a hypoechoic linear image; the
upper border of the articular capsule as a linear hyperechoic image. The averages of lateral
capsule-mandibular condyle distance on the right side in the TMD group were 0.69±0.19 mm
in CM and 0.61±0.15 mm in OM and in the asymptomatic group 0.71±0.16 mm and
0.63±0.16 mm, respectively. On the left side, the CM measurements for the TMD group were
0.68±0.15 mm and in the asymptomatic group 0.70±0.14 and in the OM 0.64±0.15 mm for
the TMD group and in the asymptomatic group 0.66±0.15. Given the results found,
Ultrasonography can be considered as a promising and feasible tool for the assessment of
TMJ, and the distance from the most lateral point of the articular capsule to the most lateral
point of the mandibular condyle (lateral capsule-condyle distance), measured on the
ultrasonographic scans, did not differ between TMD group and asymptomatic group.
Keywords: Ultrasonography, temporomandibular joint, anatomy.

19
INTRODUCTION
One of the most important synovial joints in the human body is the
temporomandibular joint (TMJ), which acts with the muscles and teeth during mandibular
movements. The anatomical elements that form it are the mandibular fossa located in the
petrous portion of the temporal bone and the mandibular condyle. Between those bones there
is the articular disc, a fibrocartilage, which improves their adaptation and is attached to the
medial and lateral pole of the mandibular condyle to accompanying it during the mandibular
movements. The articular disc divides the joint space into two compartments: the supradiscal
and infradiscal space. The TMJ is surrounded by the articular capsule, and the extracapsular
ligaments restrict the mandibular movements avoiding possible damages in the structures
(Alomar et al., 2007). The proper position of the mandibular condyle relative to the
mandibular fossa; the position of the articular disc is considered normal when its posterior
portion is located between 12 and 13 o´clock on the articular surface and its central portion on
the upper anterior face of the articular surface of the mandibular condyle (Mello-Júnior et al.,
2011).
Adverse conditions affecting the masticatory musculature and TMJ can compromise
the relationship between the TMJ structures, and consequently to determine a negative effect
on functions, causing pain, noise and movement limitation. This condition is called
temporomandibular disorder (TMD).
The approach of individual suffering of TMD begins with a complete diagnosis,
follows by a detailed clinical examination. The Diagnostic Criteria for Temporomandibular
Disorders (DC/TMD) is an evaluation method with defined criteria, simple to apply and easy
to punctuate to obtain the diagnosis of dysfunction (Schiffman et al., 2014). Moreover, TMJ
images can be necessary to confirm the suspicion of the disorder (Kundu et al., 2013),
assessing the relationship of anatomical structures, and observing the progress of an alteration
(Byahatti et al., 2010).
The most common imaging methods are panoramic radiography, arthroscopy,
computed tomography scan, ultrasonography, and magnetic resonance imaging (MRI). The
MRI is considered the gold standard for the evaluation of the anatomic structures of the TMJ,
but its availability is relatively low due to high cost and restriction in some cases, such as
pacemaker use or claustrophobic individuals. Recently, ultrasound (US) has been considered a

20
promising and viable tool for the evaluation of the anatomical structures of the TMJ, and their
relationships during mandibular movements (Emshoff et al. (2002), Pereira et al. (2007),
Byahatti et al. (2010) and Assaft et al. (2013). US is a non-invasive technique that can be used
clinically because it is inexpensive and allow evaluating the structures in "real time".
In this context, the purpose of this study was to describe anatomical structures of TMJ
by high-resolution US, such as the mandibular condyle, the articular disc, the supra and
infradiscal space, and the articular capsule in individuals with and without TMD.
Furthermore, the measurement of the distance from the lateral point of the articular capsule to
the lateral point of the mandibular condyle was carried out to verify possible differences
between participants with articular disorders and the asymptomatic ones.
MATERIAL AND METHODS
Sample
The study was approved by the Ethics Committee in Research of Piracicaba Dental
School, University of Campinas (FOP-UNICAMP), with register number 051/2015 (Annex
1). It was cross-sectional observational study.
Young adults aged from 18-40 years, with or without clinical signs and symptoms of
TMD, were invited to participate. From August 2016 to February 2017, 37 individuals were
assessed for eligibility. The final sample was composed of 17 female and 15 male, in the age
range of 19 and 39 years (26.24 ± 4.63 years), who presented at the Ultrasound laboratory of
the FOP-UNICAMP. They were distributed in two groups accordingly the following inclusion
criterial:
TMD group (N=20): presence of clinical signs and symptoms of TMD during the last
six months or more, without treatment.
Asymptomatic group (N=12): absence of signs and symptoms suggestive of TMD.
The exclusion criteria for both groups were unable individuals to sign informed
consent, developmental disorders that directly or indirectly could affect the structures of head
and neck, radiotherapy and chemotherapy of head and neck, surgery of TMJ, use of
medication for pain, such as narcotics.

21
The examiner was trained by experts in the DC/TMD (Annex 2). Previously, the
participants were informed about the objectives and methodology to be used in a clear and
easily understandable way. Their written authorization was required, by sign the consent from
for participation in the survey. After that, the volunteers provide personnel information filling
a specific from (Appendix 1).
Diagnostic Criteria for Temporomandibular Disorders (DC/TMD)
The axis I of the DC/TMD (Gonzales et al. 2014), which corresponds to the clinical
evaluation, was applied. The volunteer remained sit down, with his back resting on the
backrest of a chair, head in natural position and feet on the floor. Moreover, they were asked
about TMD symptoms using a questionnaire. The exams were performed by a single
examiner (D.Z.R.D.).
The DC/TMD evaluate the following parameters: location of the pain and headache;
incisal relationships: horizontal and vertical incisal (mm); opening pattern: straight, corrected
or uncorrected deviation (mm); opening movements: pain free on opening, on maximum
unassisted and assisted opening (mm); lateral and protrusive movements (mm); TMJ noises
during open, closing, and lateral and protrusive movements; muscle (temporalis and masseter
muscle) and TMJ pain on palpation.
The DC/TMD diagnosis was obtained from the diagnostic decision tree, which has
three large branches, the first one is related to the pain diagnosis [Pain-Related TMD and
Headache] and two latter are to obtain the diagnosis of jaw joint disorders [Intra-articular
Joint Disorders e Degenerative Joint Disorders]. After that, the participants were located in
TMD and asymptomatic group.
Ultrasonography
Imaging Acquisition
Sonography was performed with a high-resolution linear array transducer of 38 mm
and 7-18 MHz [SSA-780A – APLIO MX (Toshiba Medical Systems Corporation, Japan)],
belonging of the Department of Pediatric Dentistry of the Piracicaba Dental School,
University of Campinas. The images were obtained by a single examiner (D.Z.R.D.), properly
trained. The 14 MHz was the best resolution achieved. After that, a pilot study was developed
with a sample of 10 healthy volunteers and the DC/TMD was applied twice with an interval

22
of seven days, at least. The intraexaminer agreement was determined using Cohen’s kappa
coefficient, obtained a value of 0.7.
In total, 64 joints of the 32 participants were evaluated accordingly with the following
parameters: visualization of the articular disc during mouth closing and opening, articular
surface of the mandibular condyle, upper edge of joint capsule and mensuration of the
distance capsule-mandibular condyle.
Ultrasound was performed in a room poor lighting, the participants remained sitting
with the back resting on the backrest of the chair, head in natural position and feet on the
floor; the transducer was placed over the TMJ, perpendicular and inferior to the zygomatic
arch and parallel to the mandible ramus for a axil view, as shown in figure 1.
Figure 1 – Transducer positioned against the patient’s face, perpendicular to the Frankfort horizontal plane
and parallel to the mandibular ramus
A static image of the right and left TMJ was obtained with the mandible in rest
position (without dental occlusion and slightly closed lips), and the transducer was tilted out
until an optimal view of the joint was obtained according to the participant´s face for axial
plan.
The disc was assessed during the static and dynamic examinations. Moreover, the
distance from the upper border of the joint capsule to the upper contour of the mandibular
condyle was measured in millimeters with the tools of the ultrasound equipment, in closed-
and open-mouth (Appendix 2).

23
The participants diagnosed with TMD were referred to specialized center for
treatment.
Statistical analysis
Descriptive statistics were applied consisting of means and standard deviations. The
values of the distance capsule-mandibular condyle were submitted to paired Student t test for
inter-groups comparisons and for intra-group comparisons referent to the right and left sides.
Bioestat 5.4 software package was used, adopting the significant level of 0.05.
RESULTS
Thirty-two young adults, mean age of 26.24 years ± 4.63 were examined clinically
using DC/TMD and ultrasonography. The volunteers included in this study was distributed in
two groups: TMD group n= 20 and Asymptomatic group n=12, as demonstrated in flow chart
(Figure 2).
Assessed for eligibility (n=37)
Convenience sample
Evaluated (n=32)
Consent form
Evaluation sheet
Ultrasonography
Excluded (n=5)
Did not attend the scheduled date
DTM Group
♀ (n=12)
♂ (n=8)
Asymptomatic Group
♀ (n=5)
♂ (n=7)
n=12 n=20
Fin
al g
rou
p
All
oca
tio
n
En
roll
men
t
Figure 2 – Flow chart

24
The sample distribution related to TMD according to DC/TMD is showed in Table 1.
Table 1 – Sample distribution according to sex and DC/TMD
Characteristic Female (%) Male (%)
Group
TMD group 12(37.5%) 8 (25%)
Asymptomatic group 5 (15.63%) 7 (21.87%)
TMD group
Only pain related TMD 3 (25%) 0
Myalgia 2 (16.66%) 0
Local myalgia 1 (8.34%) 0
Only intra-articular joint disorders 2 (16.66%) 7 (87.5%)
Disc displacement with reduction 1 (8.33%) 6 (75%)
Disc displacement without reduction, with limited opening 1 (8.33%) 0
Degenerative joint disease 0 1 (12.5%)
Pain related TMD + intra-articular joint disorders 7(58.33%) 1(12.5%)
Myalgia + Arthralgia+ DJD 0 1 (12.5%)
Headache attributed to TMD + DDR 4 (33.33%) 0
Myalgia + Arthralgia + DDR 2 (16.66%) 0
Myalgia + Arthralgia+ Headache attributed to TMD + DDR 1 (8.34%) 0
Total 12(100%) 8 (100%)
DJD: degenerative joint disease; DDR: disc displacement with reduction.
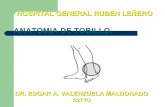
Along the US images of TMJ, the superior convexity of the mandibular condyle and
the articular disc were visualized as a hyperechoic. Moreover, the articular disc presented a
superior and inferior hypoechoic halo, corresponding to the supradiscal and infardiscal space,
respectively. The upper border of the joint capsule consisted of a linear hyperechoic image as
shown in Figure 3 and 4; there details were observed for all participants.

25
Figure 3 – Ultrasonographic scan of the left temporomandibular joint in closed-mouth
position in axial slice of a volunteer of the TMD group
The white triangles follow the upper contour of the mandibular condyle. The smaller arrow marks the articular disc. The
greater arrow points to the upper border of the articular capsule (typical anatomical structures).
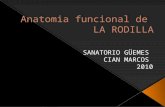
Figure 4 – Ultrasonographic scan of the right temporomandibular joint in open-mouth
position in axial slice of a volunteer of the TMD group
The white triangles point the upper contour of the mandibular condyle. The arrow points the articular disc.

26
In Figure 5 and 6, the landmarks for measurement of the distance from articular capsule
to the upper point of the mandibular condyle were demonstrated.
Figure 5 – Measurement of the distance between the most lateral point of the articular capsule
and the most lateral point of the mandibular condyle (lateral capsule-condyle
distance) in ultrasonographic scan of the right temporomandibular joint in closed-
mouth of a volunteer of the TMD group
Figure 6 – Measurement of the distance between the most lateral point of the articular capsule
and the most lateral point of the mandibular condyle (lateral capsule-condyle
distance) in ultrasonographic scan of the right temporomandibular joint in open-
mouth of a volunteer of the TMD group

27
The measurements were performed in millimeters and the values are seen in Table 2
and Table 3, according to articular/pain and muscular disorders found in TMD Group and
mean values for Asymptomatic group. There was no difference between right and left side in
both groups (P>0.05). Moreover, the values did not differ between groups, as well as between
participants with intra-articular disorders with pain and those without pain.
Table 2 – Measurement of the distance between the most lateral point of the articular capsule and
the most lateral point of the mandibular condyle (lateral capsule-condyle distance) in
the Temporomandibular disorders group and asymptomatic group (mm)
Right US - CM Right US - OM Left US - CM Left US - OM
TMD group 0.69 ± 0.19 0.61 ±0 .15 0.68 ± 0.15 0.64 ± 0.15
Asymptomatic Group 0.71 ± 0.16 0.63 ± 0.16 0.7 ± 0.14 0.66 ± 0.15
*p>0,05 0.77 0.52 0.06 0.23
Right US - CM = Right ultrasound in a closed-mouth position / Right US - OM = Right ultrasound in open-mouth position / Left US -
CM = Left ultrasound in closed-mouth position / Left US - OM = Left ultrasound in open-mouth position

28
28
Table 3 – Measurement of the distance between the most lateral point of the articular capsule and the most lateral point of the
mandibular condyle (lateral capsule-condyle distance) in the volunteers with intra-articular disorders and
asymptomatic group (mm)
Interarticular Diagnosis Pain Diagnosis Sex Right US - CM Right US - OM Left US - CM Left US - OM
Degenerative joint disease right
Participant 1 None M 0.60 0.37 0.70 0.57
Degenerative joint disease right and left
Participant 2 Myalgia, artralgia right/ left M 0.57 0.57 0.50 0.47
Disc displacement without reduction, without limited opening
Participant 3 None F 0.95 0.77 0.90 0.93
Disc displacement with reduction left
Participant 4 None M 1.00 0.57 0.67 0.60
Participant 5 None M 0.80 0.63 0.67 0.60
Participant 6 Headache attributed to TMD F 1.23 0.87 0.83 0.97
Participant 7 Myalgia, arthralgia right/left F 0.60 0.47 0.53 0.43
Participant 8 Myalgia, arthralgia left F 0.60 0.60 0.63 0.63
Mean (SD) 0.85 (0.27) 0.63 (0.15) 0.67 (0.11) 0.65 (0.20)
Disc displacement with reduction right
Participant 9 Headache attributed to TMD F 0.83 0.87 0.83 0.70
Participant 10 None M 0.63 0.53 0.63 0.67
Participant 11 None M 0.50 0.47 0.40 0.47
Participant 12 None M 0.60 0.47 0.53 0.53
Mean (SD) 0.64 (0.14) 0.58 (0.19) 0.60 (0.18) 0.59 (0.11)
SD - Standard Deviation
28

29
29
Table 3 continued
Intra-articular Diagnosis Pain Diagnosis Sex Right US - CM Right US - OM Left US - CM Left US - OM
Disc displacement with reduction right and left
Participant 13 Headache attributed to TMD F 0.67 0.87 0.87 0.90
Participant 14 Headache attributed to TMD F 0.60 0.67 0.67 0.53
Participant 15 None F 0.70 0.70 0.80 0.60
Participant 16 None M 0.60 0.60 0.80 0.80
Participant 17 Myalgia, arthralgia right/left,
headache attributed to TMD F 0.63 0.53 0.47 0.57
Mean (SD) 0.64 (0.04) 0.67 (0.13) 0.72 (0.16) 0.68 (0.16)
Without articular disorders
Participant 18 Muscular pain on palpation 0.60 0.57 0.63 0.67
Participant 19 Muscular pain on palpation 0.43 0.40 0.60 0.53
Participant 20 Muscular pain on palpation 0.87 0.73 0.97 0.80
Mean (SD) 0.63 (0.22) 0.57 (0.17) 0.73 (0.20) 0.67 (0.13)
Intra-articular disorders and pain
(N=8) - 0.71 (0.22) 0.68 (0.16) 0.66 (0.16) 0.65 (0.19)
Intra-articular disorders no pain
(N=9)
- 0.70 (0.17) 0.56 (0.12) 0.67 (0.15) 0.64 (0.14)
TMD Group - 0.69 ± 0.19 0.61 ±0 .15 0.68 ± 0.15 0.64 ± 0.15
Asymptomatic Group - 0.71 (0.16) 0.63 (0.16) 0.70 (0.14) 0.66 (0.15)
SD - Standard Deviation
29

30
DISCUSSION
Temporomandibular disorders represent 5-12% of a chronic pain condition and are
becoming more frequent in young adults (NIDCR, 2017). In this study, 32 young adults were
evaluated, being 12 females (37.5%) and 8 males (25%) presenting signs and symptoms of
TMD as shown in Table 1. Those frequencies and sample size are similar to Mello-Júnior et
al. (2011), who evaluated by high-resolution US, 9 males and 29 females presenting intra-
capsular TMD; and Müller et al. (2009) who evaluated 16 females and 14 males with TMJ
arthritis using ultrasound (US) and MRI. All these study showed higher frequency in females
than in males.
The anatomic structures of the temporomandibular joint are visualized on
ultrasonography at different echogenicity scales. In the present study, along the closed and
open-mouth position, the articular disc was visualized as hyperechoic image with a superior
and inferior hypoechoic halo as shown in Figure 3. Similar image has been described by
Manfredini et al (2003) and Emshoff et al. (1997). Conversely, Byahatti et al. (2010) and Jank
et al. (2001) observed the articular disc as a hypo to isoechoic band.
The articular surface of the mandibular condyle showed a hyperechoic image, and the
upper border of the joint capsule was visualized as a hyperechoic image, as seen by Assaft et
al. (2013). These differences may be related to the resolution of the transducer, which has
been varied from 7.5 to 12 MHZ (Emshoff et al., 1997; Manfredini et al., 2003; Jank et al.
2001; Elias et al., 2006; Byahatti et al. 2010; Mello-Júnior et al., 2011; Assaf et al., 2013). In
the present study a transducer of 14 MHz was used that allowed images with anatomical
structures well defined. The sensitivity of US has been considered to be directly proportional
to the resolution of the transducer (Kundu et al., 2013), i.e., increasing in resolution,
increasing the sensitivity of US.
Fifteen participants of TMD Group presented disc displacement with reduction and
one without reduction, accordingly DC/TMD. Nevertheless, there was a great difficulty in
observing the disc position relative to the mandibular condyle along the US images. Thus, the
position of other anatomical structures could give signs of disk position (Landes et al., 2000;
Hayashi et al., 2001; Elias et al., 2006). In this way, the distance from the most lateral point of
the articular capsule and the most lateral point of the mandibular condyle (lateral capsule-

31
condyle distance) was selected in the present study, since this contour represents lateral
surface of mandibular condyle in an axial view. According to Hayashi et al. (2001) and
Mello-Júnior et al. (2011), these landmarks can be considered as indirect ultrasonographic
signs of the disc position, probably enlarged in cases of lateral disc displacement. In the
present study, the respective values in open- and closed-mouth ranged from 0.58 mm to 0.68
mm for participants with disk displacement with reduction, accordingly with DC/TMD,
values lesser than the cut-off stated by Hayashi et al. (2001) to separate joints with and
without anterolateral disc displacement. Besides, Mello-Júnior et al. (2006) found the distance
varying from 1.2 mm to 1.6 mm in TMD individuals without disc displacement. Thus, it is
possible to infer that the US images, in the present study, could not confirm the disk
displacement diagnosed clinically. A large sample with severe TMD is indicated to confirm
the findings.
Furthermore, the measurements of the distance capsule-mandibular condyle did not
differ significantly between the TMD and Asymptomatic Groups in both mouth positions.
These results were not expected, since in TMD Group 15 participants were clinically
diagnosed with disc displacement and two with degenerative joint disease. The enlargement
distance between the articular capsule and mandibular condyle could be an indicative of disc
displacement (Hayashi et al., 2001; Elias et al., 2006), as commented above. Moreover, for
Motoyoshi et al. (1998), irregularities of the soft tissues surrounding the TMJ could also point
out the disc displacement.
It was not observed also differences in images and distance the most lateral point of
the articular capsule and the most lateral point of the mandibular condyle (lateral capsule-
condyle distance) between individuals with intra-articular disorders and pain (N=8) and those
without pain (N=9). Probably, the number of individuals could have a determinant factor in
this result, as well as the pain intensity.
The different findings between this study and others, cited above can be attributed to
technique itself, and despite the methodological details have been precisely taken into
account, US images depend on the direction of the scanning and the mouth/head posture. The
position of the transducer may vary from horizontal (parallel to the zygomatic arc) to vertical
(parallel to the ramus of the mandible), thus giving a different image of the TMJ in a
transverse or a coronal / sagittal plane. In fact, the planes of the images are not truly
transverse, coronal or sagittal, but they are almost inclined, because the transducer is tilted

32
during the examination, in order to achieve a better visualization of the different components
of the TMJ (Kundu et al., 2013).
One limitation of the US is the correct visualization of the articular disc, as observed
during the rotation and translation of mandibular condyle in dynamic images as shown in
Figure 4, i.e., from the mouth-closed position to the mouth-open position; however, the
central portion of the disk was observed in all participants adjusting the position of the
transducer constantly. According to Kundu et al. (2013), only the lateral part of the TMJ can
be reached in the sonograms, while the medial part remains hidden by the structures,
consequently the medial displacements of the disc can remain overlooked.
CONCLUSION
Ultrasonography allowed visualization of the anatomical structures of the TMJ as
follows: the articular surface of the mandibular condyle was visualized as an hyperchoic
image; the articular disc as an hyperechoic image with a superior and inferior hypoechoic halo
(dividing the joint space into two compartments, superior and inferior, the supra and
infradiscal space, respectively); the upper border of the joint capsule was visualized as an
hyperchoic image.
The distance from the most lateral point of the articular capsule to the most lateral
point of the mandibular condyle (lateral capsule-condyle distance), measured on the
ultrasonographic scans, did not differ between TMD group and asymptomatic group.

33
REFERENCES
Alomar X, Medrano J, Cabratosa J, Clavero JA, Lorente M, Serra I, et al. Anatomy of The
Temporomandibular Joint. Semin ultrasound CT MR.2007;28(3):170-83.
Mello-Júnior CF, Saito Osmar C, Guimarães Filho HA. Avaliação ultrassonográfica dos
distúrbios intracapsulares temporomandibulares. Radiol Bras [internet]. 2011; [acesso
2017 Jul 27] 44(6):355-359. Disponível em:
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0100-
39842011000600005&lng=pt.
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic for
Temporomandibular disorders (DC/TMD) for Clinical and Reserarch Applications:
Recommendations of the Internacional RDC/TMD Consortium Network and Oralfacial
Pain Special Interest Group. J Oral Facial Pain Headache. 2014;28(1); 6-27.
Kundu H, Basavaraj P, Kote S, Singla A, Singh S. Assessment of TMJ Disorders Using
Ultrasonography as a Diagnostic Tool: A Review. J Clin Diagn Res. 2013
Dec;7(12):3116-20. doi: 10.7860/JCDR/2013/6678.3874.
Byahatti SM, Ramamurthy BR, Mubeen M, Agnihothri PG. Assessment of diagnostic
accuracy of high-resolution ultrasonography in determination of temporomandibular
joint internal derangement. Indian J Dent Res. 2010 Apr-Jun;21(2):189-94. doi:
10.4103/0970-9290.66634.
Emshoff R, Jank S, Bertram S, Rudisch A, Bodner G. Disk displacement of the
temporomandibular joint: sonography versus MR imaging. AJR Am J Roentgenol.
2002 Jun;178(6):1557-62.
Pereira LJ, Gavião MB, Bonjardim LR, Castelo PM. Ultrasound and tomographic evaluation
of temporomandibular joints in adolescents with and without signs and symptoms of
temporomandibular disorders: a pilot study. Dentomaxillofac Radiol. 2007
Oct;36(7):402-8.
Assaf AT, Kahl-Nieke B, Feddersen J, Habermann CR. Is high-resolution ultrasonography
suitable for the detection of temporomandibular joint involvement in children with
juvenile idiopathic arthritis? Dentomaxillofac Radiol. 2013;42(3):20110379. doi:
10.1259/dmfr.20110379.
Gonzalez Y, Chwirut J, List T, Ohrbach R. Diagnostic Criteria for Temporomandibular
Disorders Clinical Protocol and Assessment Instruments. MedEdPORTAL
Publications [internet]. 2014 Nov [acesso 2017 Jul 27];10:9946. Disponível em

34
https://www.mah.se/PageFiles/96306061/DC-
TMD%20Axis%20I%20_Axis%20II%20Protocol%20-%202013_06_08.pdf.
Nacional institute of dental and craniofacial research. Facial pain. [acesso 2017 Ago 9].
Disponível em:
https://www.nidcr.nih.gov/DataStatistics/FindDataByTopic/FacialPain/PrevalenceTMJ
D.htm.
Müller L, Kellenberger CJ, Cannizzaro E, Ettlin D, Schraner T, Bolt IB, et al. Early diagnosis
of temporomandibular joint involvement in juvenile idiopathic arthritis: a pilot study
comparing clinical examination and ultrasound to magnetic resonance imaging.
Rheumatology (Oxford). 2009 Jun;48(6):680-5. doi: 10.1093/rheumatology/kep068.
Manfredini D, Tognini F, Melchiorre D, Zampa V, Bosco M. Ultrasound assessment of
increased capsular width as a predictor of temporomandibular joint effusion.
Dentomaxillofac Radiol. 2003 Nov;32(6):359-64.
Emshoff R, Bertram S, Rudisch A, Gassner R. The diagnostic value of ultrasonography to
determine the temporomandibular joint disk position. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. 1997 Dec;84(6):688-96.
Jank S, Rudisch A, Bodner G, Brandlmaier I, Gerhard S, Emshoff R. High-resolution
ultrasonography of the TMJ: helpful diagnostic approach for patients with TMJ
disorders?. J Craniomaxillofac Surg. 2001 Dec;29(6):366-71.
Elias FM, Birman EG, Matsuda CK, Oliveira Ilka RS, Jorge WA. Ultrasonographic findings
in normal temporomandibular joints. Braz Oral Res. 2006;20(1): 25-32.
Landes C, Walendzik H, Klein C. Sonography of the temporomandibular joint from 60
examinations and comparison with MRI and axiography. J Craniomaxillofac Surg
2000;28(6):352-61.
Motoyoshi M, Kamijo K, Numata K, Namura S. Ultrasonic imaging of the
temporomandibular joint: a clinical trial for diagnosis of internal derangement. J Oral
Sci. 1998;40(2):89-94.
https://www.mah.se/PageFiles/96306061/DC-TMD%20Axis%20I%20_Axis%20II%20Protocol%20-%202013_06_08.pdf

35
3 CONCLUSÃO
A ultrassonografia possibilitou a visualização das estruturas anatômicas da articulação
temporomandibular como o polo lateral da cabeça da mandíbula em uma imagem linear
hiperecóica, o disco articular como uma imagem linear hiperecóica e como este divide o
espaço articular em dois compartimentos menores, um superior e outro inferior (espaço supra
e infradiscal, respectivamente) visualizados em uma imagem linear hipoecóica, e a borda
superior da cápsula articular como uma imagem linear hiperecóica.
A mensuração da distância entre o ponto mais lateral da cápsula articular e o ponto
mais lateral da cabeça da mandíbula (distância lateral da cápsula-cabeça da mandíbula) nas
posições de boca fechada e boca aberta não diferiu significativamente entre os participantes
com DTM e os participantes assintomáticos.

REFERÊNCIAS
Alomar X, Medrano J, Cabratosa J, Clavero JA, Lorente M, Serra I, et al. Anatomy of The
Temporomandibular Joint. Semin ultrasound CT MR.2007;28(3):170-83.
Mello-Júnior CF, Saito Osmar C, Guimarães Filho HA. Avaliação ultrassonográfica dos
distúrbios intracapsulares temporomandibulares. Radiol Bras [internet]. 2011; [acesso
2017 Jul 27] 44(6):355-359. Disponível em:
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0100-
39842011000600005&lng=pt.
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic for
Temporomandibular disorders (DC/TMD) for Clinical and Reserarch Applications:
Recommendations of the Internacional RDC/TMD Consortium Network and Oralfacial
Pain Special Interest Group. J Oral Facial Pain Headache. 2014;28(1); 6-27.
Emshoff R, Jank S, Bertram S, Rudisch A, Bodner G. Disk displacement of the
temporomandibular joint: sonography versus MR imaging. AJR Am J Roentgenol.
2002 Jun;178(6):1557-62.
Melchiorre D, Falcini F, Kaloudi O, Bandinelli F, Nacci F, Matucci CM. Sonographic
evaluation of the temporomandibular joints in juvenile idiopathic arthritis. Journal of
Ultrasound. 2010; 13(1): 34–37. doi: 10.1016/j.jus.2009.09.008.
Kundu H, Basavaraj P, Kote S, Singla A, Singh S. Assessment of TMJ Disorders Using
Ultrasonography as a Diagnostic Tool: A Review. J Clin Diagn Res. 2013
Dec;7(12):3116-20. doi: 10.7860/JCDR/2013/6678.3874.
Byahatti SM, Ramamurthy BR, Mubeen M, Agnihothri PG. Assessment of diagnostic
accuracy of high-resolution ultrasonography in determination of temporomandibular
joint internal derangement. Indian J Dent Res. 2010 Apr-Jun;21(2):189-94. doi:
10.4103/0970-9290.66634.
Hayashi T, Ito J, Koyama J, Yamada K. The accuracy of sonography for evaluation of
internal derangement of the temporomandibular joint in asymptomatic elementary
school children: comparison with MR and CT. AJNR Am J Neuroradiol.
2001;22(4):728-734.
Pereira LJ, Gavião MB, Bonjardim LR, Castelo PM. Ultrasound and tomographic evaluation
of temporomandibular joints in adolescents with and without signs and symptoms of
temporomandibular disorders: a pilot study. Dentomaxillofac Radiol. 2007
Oct;36(7):402-8.

Assaf AT, Kahl-Nieke B, Feddersen J, Habermann CR. Is high-resolution ultrasonography
suitable for the detection of temporomandibular joint involvement in children with
juvenile idiopathic arthritis? Dentomaxillofac Radiol. 2013;42(3):20110379. doi:
10.1259/dmfr.20110379.
van Holsbeeck M, Introcaso JH. Ultras-sonografia Musculoesquelética. Rio de Janeiro:
Editora Guanabara Koogansa; 2001.

APÊNDICE 1/APPENDIX 1
UNIVERSIDADE ESTUADUAL DE CAMPINAS
FACULDADE DE ODONTOLOGIA DE PIRACICABA
DEPARTAMENTO DE MORFOLOGIA
ÁREA DE ANATOMIA
FICHA DE AVALIAÇÃO
Data da avaliação: _____/ ______/ ________.
Nome Completo: _________________________________________________. Sexo:
Telefone: fixo _____________________________________/
celular____________________________.
Endereço: _________________________________________ N°:______
Bairro:____________________
Cidade___________________________________ Estado:__________________________________.
Horários d isponíveis:__________________________________________________________.
Profissão: ________________________________________.
1. Anamnese:______________________________________________________________________
2. Histórico
Familiar:_________________________________________________________________
3. Critérios de Inclusão:
Idade:______ anos. Peso: ______Kg. Altura: ________ cm. IMC: ____________
1.1. História de cinco meses ou más de sintomas como:
Indicação: marque com uma X sobreo a resposta que represente o seu sentir.
Ruídos próximos dos ouvidos .................................................... Sim Não
Restrição na capacidade de abrir e fechar a boca .................... Sim Não
Dor na área da articulação ........................................................ Sim Não
Dor no mús. da mastigação ....................................................... Sim Não
1.2. Você já recebeu tratamento prévio ou atual para seus sintomas: Sim Não
1.3. Ciclo menstrual: Regular Anticoncepcional
1.4. Data do último ciclo menstrual [1° dia] ______/______/_______.
2. Critérios de Exclusão:
Indicação: marque com uma X sobreo a resposta que represente o seu sentir.
Tratamento ortodôntico atual: Sim Não (se sim, a quantos anos_________________________)
Comprometimento sistêmico como febre reumática, endócrina ou autoimune: Sim Não .
Tratamento atual ou passado de radioterapia de cabeça e pescoço: Sim Não
Cirurgia da ATM: Sim Não
Trauma na mandíbula por acidentes: Sim Não
Dificuldade para se comunicar devido à barreira da língua e / ou incompetência mental: Sim Não
Gestante: Sim Não
O uso de medicação para a dor [narcóticos, relaxantes musculares, esteroides, antidepressivos e/ou
abuso de drogas: Sim Não
Pessoas comprometidas com transtornos de desenvolvimento que afetam direta ou indiretamente a
cavidade oral [qualquer tipo de síndrome diagnosticado clinica ou geneticamente]: Sim Não
F M

APÊNDICE 2/APPENDIX 2
FICHA DE AVALIAÇÃO DOS DADOS ULTRASSONOGRAFICOS
Data da avaliação: ______/_______/______.
Nome completo:________________________________________________________________
Nome do avaliador: _____________________________________________________________
Mensuração em milímetros do espaço do disco articular da ATM Direita
[A distância entre o polo lateral do côndilo e da parte lateral da cápsula articular].
Posição do
Paciente
Postura
mandibular Ultrassom
Media
Sentado
Boca
fechada [lábios levemente
encostados sem
contato oclusal]
Boca aberta [sem forçar, nem
dor].
Mensuração em milímetros do espaço do disco articular da ATM Esquerda
Posição do
Paciente
Postura
mandibular Ultrassom
Media
Sentado
Boca
fechada [lábios levemente
encostados sem
contato oclusal]
Boca aberta [sem forçar, nem
dor].

ANEXO 1/ANNEX 1

ANEXO 2 /ANNEX