Mandible Final
139
-
Upload
shriya-marya -
Category
Documents
-
view
97 -
download
0
Transcript of Mandible Final


MANDIBLE AND ITS SIGNIFICANCE IN PROSTHODONTICS
Dr. Shriya MaryaDepartment of Prosthodontics

CONTENTS• INTRODUCTION• DEVELOPMENT OF MANDIBLE• OSTEOLOGY• ORAL ANATOMIC CONSIDERATIONS IN PROSTHODONTICS
• ANATOMIC LANDMARKS• MUSCLE ATTACHMENTS• ANATOMIC CONSIDERATIONS FOR IMPLANTS
• INNERVATION OF THE MANDIBLE• BLOOD SUPPLY OF THE MANDIBLE• AGE CHANGES• CONCLUSION• REFERENCES

INTRODUCTION
• The mandible forms the lower jaw and holds the lower teeth in place
• It is the largest, strongest and lowest bone in the face
• It has a horizontally curved body that is convex forward and two broad rami that ascend posteriorly
• It articulates with the glenoid fossa in the temporal bone in the base of the skull

DEVELOPMENT OF THE MANDIBLE
• Stomodaeum (future mouth) is a depression bound by• Cranially by the bulging process of the brain • Caudally by the pericardium
• Formation of neck:• Elongation of the region between the stomodaeum and
the pericardium• A series of mesodermal thickenings appear in the wall of
the cranial most part of the fore gut
Known as Pharyngeal or Branchial arches

• Each arch has a skeletal element, a striated muscle, and an arterial arch. Also each arch is supplied by a particular nerve
• The first arch is called the mandibular arch.• As the mandibular arches grow towards each
other, they give off a bud from its dorsal end which leads to the formation of the maxillary arch
• The cartilage of the first arch is known as Meckel’s cartilage

Ossification Of Mandible
• The cranial ends of the Meckel’s cartilage are connected with the ear capsules, and their distal extremities are joined to one another at the symphysis by mesodermal tissue.
• From the cranial end of each cartilage the malleus and incus are developed
• The next succeeding portion, as far as the lingula is replaced by fibrous tissue, which persists to form the sphenomandibular ligament
• The cartilage is surrounded by thick fibrocellular tissue membrane in which intra membranous ossification occurs

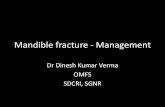
Mandible of human embryo (24mm long) outer aspect

• 6TH WEEK – Ossification takes place in the membrane covering the outer surface of the ventral end of Meckel’s cartilage. Each half of the bone is formed from a single center which appears near the mental foramen. This intramembranous ossification forms the body and ramus of the mandible.
• 10TH WEEK – The portion of Meckel’s cartilage which lies below and behind the incisor teeth is surrounded and invaded by the membrane bone. The rest of the meckel’s cartilage disappears, except for the spheno-mandibular ligament


• Somewhat later, accessory nuclei of cartilage make their appearance• Wedge-shaped nucleus in the condyloid process and
extending downward through the ramus• Small strip along the anterior border of the coronoid
process• Smaller nuclei in the front part of both alveolar walls and
along the front of the lower border of the bone

• The condylar secondary cartilage appears during the 10th week of IUL. Cartilage cells differentiate from its center and the cartilagenous condylar head increases in size by interstitial and appositional growth.
• 14th week - First evidence of endochondral bone in the condyle region
• Much of the cartilage is replaced with bone by the middle of the fetal life; but its upper end persists into adulthood , acting as both growth centre and articular cartilage.
• At birth the mandible consists of two parts, united by a fibrous symphysis, in which ossification takes place during the first year

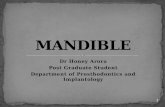
Mandible of human embryo (95mm long) outer aspect

OSTEOLOGY
• Consists of a •Horse-shoe shaped body•Pair of rami•Coronoid process•Condylar process

The Body
• Two borders• SUPERIOR BORDER It contains the alveolar process with the sockets for the teeth
• INFERIOR BORDER Extends postero-laterally from the symphysis to join with the ramus at the angle of the mandible. It consists of a concavity on either side of the symphysis, after that it is rounded and smooth

• OUTER SURFACE• Symphysis menti – line at which two halves of the mandibular process join
•Mental protuberance – median triangular projection

•Mental foramen – lies between the roots of the pre molars The mental nerves and vessels exit from here
• External oblique ridge – continuation of the sharp anterior border of the ramus which runs downward and forward
• Incisive fossa – depression just beneath the incisors

• INNER SURFACE
• Mylohyoid line – Ridge that runs downwards and forwards. The mylohyoid muscle attaches here It is sharp and distinct near the molars and fades anteriorly

• Submandibular fossa – Hepression beneath the mylohyoid line. It lodges the submandibular gland
• Sublingual fossa – Hollow above the mylohyoid line that lodges the sublingual gland
• Genial tubercles – Four small elevations on posterior surface of symphysis menti The upper ones give attachment to the genioglossus and the lower to geniohyoid

The Ramus• Quadrilateral in shape• Two surfaces:• LATERAL SURFACE – flat with a number of longitudinal
ridges. It bears attachment to the masseter muscle• MEDIAL SURFACE – • Mandibular foramen lies a little above the middle of the
ramus at occlusal level of the teeth. The inferior alveolar nerves and vessels enter the mandibular canal through this
• Lingula – sharp tongue shaped projection forming anterior border of the mandibular foramen
• Mylohyoid groove – begins just below the mandibular foramen

• Four borders:• Upper – thin and forms a notch called the mandibular
notch
• Lower – it’s the backward continuation of the inferior border of the body of the ramus
• Anterior – thin and continuous with the anterior border of the coronoid process
• Posterior – it is thick and continues as the neck of the condyle



CORONOID PROCESS
• It projects upward and slightly forward as a triangular plate of bone
• Its posterior border bounds the mandibular notch and the anterior border is continuous with the ramus
• The temporal crest is a ridge that runs on its medial side from the tip of the process till its base
• The temporalis muscle is attached here

CONDYLAR PROCESS
• Strong upward projection from the postero-superior part of the ramus
• The upper end expands to form the head, while the constriction below the head forms the neck
• When viewed from above the head is ovoid in shape, with the antero-posterior diameter half of the medio-lateral diameter• 3/4th inch (19mm) wide• Less than ½ inch (12.5mm) long anteropsteriorly

• The neck of the condyle is constricted to about half of the size of the head
• The anterior surface of the neck contains the pterygoid fovea, where the lateral pterygoid muscle attaches

TEMPOROMANDIBULAR JOINT• The condylar process of the mandible articulates
with the glenoid fossa of the temporal bone to form the temporomandibular joint
• It allows for hinge as well as gliding movement hence it is a called a “Ginglymo-arthroidial joint”

• It consists of:• Bony components: • Condylar process of mandible• Mandibular or glenoid fossa of temporal bone
• Articular disc• Its is a biconcave dense fibrous tissue disc that divides
the TMJ into the upper (meniscotemporal) compartment and the lower (meniscomandibular) compartment
• Ligaments• Fibrous capsule• Lateral/temporomandibular ligament• Sphenomandibular ligament• Stylomandibular ligament

Glenoid fossaArticular discArticular eminenceCondylar process

ANATOMIC CONSIDERATIONS IN THE
MANDIBLE

ANATOMICAL LANDMARKS• A prosthesis must function in harmony with the
tissues that support them and those that surround them
• Hence the dentist must understand the macroscopic as well as microscopic anatomy of the supporting and limiting structures of the denture
• This knowledge aids in determining• The selective placement of forces by the denture bases
upon the supporting tissues• The form of the denture borders that will be harmonious
with the normal function of the limiting structures that surround them

Pterygomandibular raphe
Lingual flange
Labial vestibule
Labial frenum
Lingual frenum
Retromylohyoid fossa
Premylohyoid eminence
Buccal frenum
Buccal vestibule
Buccal shelf
Retromolar pad
Tongue
Residual alveolar ridge

1.SUPPORTING STRUCTURES2.RELIEF AREAS
3.LIMITING STRUCTURES

SUPPORTING STRUCTURES• Denture support is ‘the resistance to vertical forces of
mastication, occlusal forces and other forces applied in a direction towards the denture-bearing area’
• The supporting structures are ‘those areas of maxillary and mandibular edentulous ridges that are considered best suited to carry the forces of mastication when dentures are in function’
• Support for the lower denture is provided by the mandible and the soft tissues overlying it
• Some parts of the mandible are more favorable for this function than others and pressure must be selectively applied only in these areas that can resist the stresses of occlusion

• The areas of support are divided into 1. Primary • Usually at right angles to the occlusal forces• Do not resorb easily• Buccal shelf area
2. Secondary• Either at an angle greater than 90˚ to the occlusal
forces, or parallel to them• Tend to resorb at a higher rate• Slopes of the ridge

Residual Alveolar Ridge• It is defined as “the portion of the alveolar ridge
and its soft tissue covering which remains following the removal of teeth.”
• It forms the main supporting area in edentulous maxillae and mandibles
• It can be classified as:• Inverted ‘U’• Inverted ‘V’• Knife edged
• The surface of the ridge can be • Smooth-even• Rough-uneven

• The ideal ridge:• high ridge with a Flat crest and parallel sides. • It will give maximum amount of support and stability.
• As age advances• the ridge resorbs and either become flatter, V shaped or Knife edged.• Knife edged ridges with multiple bony spicules offer the poorest prognosis.• Incapable of withstanding occlusal force. • Can easily become sore.

• CREST• It is covered in a healthy mouth by keratinized stratified squamous epithelium • The mucosa is firmly attached by its sub mucosa to the periosteum of the mandible• The extent of its attachment to the bone varies greatly

• It might be loosely attached to the bone over the entire crest, rendering the mucosa movable•Movable soft tissue must be registered carefully in its resting position • In relatively few patients the mucosa is firmly attached which is capable of providing soft-tissue support for lower denture

•Mostly the underlying bone in this region is cancellous and hence prone to resorption due to the lack of a cortical bony covering• Even though the fibrous tissue closely attached to the bone is favorable for resisting the occlusal load, if the underlying bone is cancellous, this advantage is lost• Therefore in such scenarios the area should be relieved while making the impression

Buccal Shelf Area
• It is the PRIMARY support of the mandibular denture
• Also known as Buccal flange area• Boundaries:• Anteriorly by the buccal frenum• Distally by the retro molar pad• Medially by the crest of the residual alveolar ridge• Laterally by the external oblique ridge

RETROMOLAR PAD
BUCCAL SHELF
TONGUE
RESIDUAL ALVEOLAR RIDGE

• It is usually quite wide (4-6mm wide on an average mandible, 2-3 mm in a narrow mandible)
• Factors making buccal shelf ideal for stress bearing:• Perpendicular to the direction of occlusal forces
• The mucous membrane here is less keratinized and more loosely attached than ideal, but the bone has a layer of compact bone containing haversian systems
• The fibers of the buccinator run horizontally in the sub mucosa and are attached here. The contraction of these muscle fibers directed antero-posteriorly tend to stabilize the denture instead of displacing it. This allows the denture to rest on this part of the muscle without damage to the muscle as well

• SLOPE OF THE RESIDUAL ALVEOLAR RIDGE• It serves as the secondary stress bearing area in the mandible• The sub mucosa here is firmly attached to the periosteum • The epithelium is keratinized

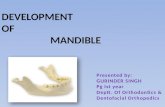
A – Crest of residual alveolar ridgeB – Buccal shelf (cortical bone)C – Mental foramenD – Genial tubercles E – Coronoid process

Retro molar pad• Sicher has described the retromolar pad as a soft
elevation of the mucosa that lies distal to the third molar
• It is covered by smoother, less keratinized epithelium than the crest
• Contents :Glandular tissueTemporalis tendon – posteriorly Buccinator – enters buccally Medially - pterygomandibular raphe and superior
constrictor

• The term ‘Pear-shaped pad’ was coined by Craddock
• It forms the distal termination of the ridge• The mandibular denture should terminate over
the distal edge of this pad• Importance:• It is an area that rarely resorbs – the temporalis muscle
exerts tensile stimulus onto the bone, which responds by growth and apposition• It ensures the peripheral seal of the denture is maintained• It can be used as a landmark for placement of occlusal
plane

• Teeth should not be placed on the retromolar pad. Reason:• Bone is situated in a inclined plane and hence forces exerted on teeth in this area will not be directed perpendicular to the bone• This would lead to dislodgement of the denture• It would lead to soreness of tissue

Mucosa• The mucosa covering the residual alveolar ridge
has been classified by HOUSE as:
• Class 1: healthy• Class 2: irritated• Class 3: pathologic

LIMITING STRUCTURES• The denture should be extended as far as possible
within the limits of health and function of tissues and structures that support and surround them
1. Labial frenum2. Labial vestibule3. Buccal frenum4. Buccal vestibule5. Lingual frenum6. Alveololingual sulcus7. Retromolar pad8. Pterygomandibular raphe

Labial frenum• Usually a single narrow band, but may consist of 2
or more bands• It is shorter and wider than the maxillary frenum• It contains a band of fibrous connective tissue that
helps to attach the orbicularis oris

• It is an active frenum and hence quite sensitive
• The activity of this frenum is mostly in a vertical direction, hence a narrow notch should be made in the denture to accommodate the frenum and maintain the peripheral seal without causing soreness
• The incisivus (depressor labi inferioris) may also alter the extent of the denture in this region

Labial vestibule • It is the region between the labial frenum and the
buccal frenum• The major muscle in this region is orbicularis oris• The muscle fibers in this region are mainly
horizontal hence care must be taken not to over extend the impression in this area
• The mentalis muscle originates from the mental tubercles and inserts into the lower lip. It is a vertical muscle and may be very active in some patients
• Hence careful border moulding in this area is essential

• Excessive muscle activity here may leads to a very short denture flange which may affect the seal of the denture
• But the drape of the lip and cheeks usually creates a “facial seal” which compensates
• In a ridge with a good vertical height, the labial denture border should be thin (1-2mm) since a thicker border might distort the lip
• But if the ridge is flat, a thicker border is needed for lips and cheek support and to provide a better seal

Buccal frenum• It connects as a continuous band through the
modiolus at the corner of the mouth and on up to the buccal frenum of the maxilla
• This usually exists in the area of the pre-molars• It is mostly made of multiple bands• Muscles:• Buccinator• Depressor anguli oris

• The muscular activity in this region is more in a horizontal direction rather than in a vertical direction ( such as while puckering, grinning)
• The fibrous and muscular tissues pull across the denture borders, hence the extent of the denture in this region is less. Hence proper functional trimming of the denture is essential here

• The frenum attachment level has been classified by House:
• Class 1: low in the mandible with respect to crest of the ridge• Class 2: medium• Class 3: freni encroach on the crest of the ridge and may interfere with the denture seal

Buccal vestibule• It extends from the buccal frenum up to the retro-
molar pad• Its width and length are mainly dependent on the
buccal shelf area and the buccinator muscle• The length of the buccal flange usually extends up
to the lateral end of the buccal shelf or the external oblique ridge. Palpation of the external oblique ridge is a valuable aid in helping to determine the amount of resistance or the lack of resistance offered by the border tissues in these areas
• This length is not very critical for the peripheral seal because the drape of the cheek provides facial seal

• The thickness of the borders in this region should always be smooth and round so as not to irritate the cheek
• Their thickness should be about 2mm• The buccinator in this region does not displace the
denture as the direction of muscle fibers and their action is parallel to the borders of the denture
• The resistance offered to the denture in this region decreases within a few weeks of wearing the denture as the tissues are stretched

• Muscular attachment level (by House):
• Class 1: attachment is low in the mandible with respect to crest of the ridge (0.5 inches or more between level of attachment and crest of the ridge)• Class 2: attachment height in relation to the crest of the
ridge is between 0.25 – 0.50 inches• Class 3: attachment height is less than 0.25 inches from
the ridge crest

• Masseter muscle region• The distobuccal corner of the mandibular denture must
converge rapidly to avoid displacement because of contracting pressure of the masseter muscle whose anterior fibers pass outside the buccinator muscle in this region• Contraction of the muscle alters the shape and size of the
distobuccal end of the lower vestibule as it pushes inward• If the ramus has a perpendicular surface and the origin of
the muscle on the zygomatic arch is medial-ward the muscle pulls more directly across the denture border

• Registration of this pull can be done by:• Softening of the compound in the distobuccal region• Insert in patient’s mouth • Apply downward pressure by placing the index finger in
the second molar region • Asking patient to exert closing force

Effect of masseter muscle on distobuccal border
• Pic frm levin page 42
• Moderate Activity – Straight Line• Active Muscle – Concave • Inactive Muscle - Convex
STRAIGHT CONCAVE CONVEX

• Distal extension of the mandibular impression is limited by • The ascending border of the ramus• By the buccinator as it crosses the mandible from buccal
to lingual to join the pterygomandibular raphe and the superior constrictor muscle• By the sharpness of the lateral bony boundaries of the
retromolar fossa (formed by continuation of the external and internal oblique ridges as they ascend the ramus)
• The desirable extent is slightly lingual to these bony prominences and including the retro molar pad under the denture – forms an excellent soft-tissue seal

Lingual Frenum• It is a fold of mucous membrane extending from the
floor of the mouth to the ventral surface of the tongue
• The height and the width of the lingual frenum varies considerably.
• High frenum attachment is called a TONGUE TIE.• It should be corrected as it affects the denture
stability.

Alveolo lingual sulcus• It is the space between the tongue and the
residual alveolar ridge• It extends from the lingual frenum to the
retromylohyoid curatin
• It can be divided into three parts:• Anterior vestibule (sublingual crescent area)• Middle vestibule (mylohyoid area)• Distolingual vestibule (lateral throat form)

ANTERIOR LINGUAL SULCUS• Also known as sublingual crescent area or anterior
sublingual fold• Extent: from the lingual frenum
point where the mylohyoid ridge curves down below the level of the sulcus
• Roberts has written that the anterior vestibule should have a border that is as thick as possible, similar to a “dam”, in order to ensure a better seal

• On palpation – a depression known as premylohyoid fossa can be felt
• Due to the mandible joining the convexity of the mylohyoid ridge
• Influenced by:• Genioglossus • Lingual frenum• Sublingual gland (to some extent)

• Lingual frenum is superimposed over the genioglossus which raises the tongue
• If the mandibular ridge is highly resorbed the attachment of the genioglossus lies almost at the level of the crest of the alveolar ridge.
• Surgical sulcus deepening may be required in such scenarios

• The width of the border of the denture in this region is usually about 2mm. But the width depends on the tonicity of the genioglossus
• The genioglossus and the lingual frenum are recorded by asking the patient to moderately protrude the tongue as these tissues do not tolerate impingement

MIDDLE VESTIBULE• Also known as mylohyoid vestibule• Forms the largest part of the alveololingual sulcus• Influenced by:• Mylohyoid muscle• Sublingual glands

Mylohyoid muscle and ridge• The mylohyoid ridge is close to the crest of the
ridge in the molar region and close to the lower border of the mandible in the anterior region

• It is important to determine the prominence of the ridge because:• It may interfere with the development of a correct lingual
flange • A sharp ridge may cause pain
• The extension of the denture can go beyond the mylohyoid muscle line as the mucolingual fold is not in that area. Also as the fibres are directed in a forward and downward direction they allow for denture extension beyond the level of muscle attachment
Ensures soft-tissue peripheral seal

• Impression may depart from stress bearing area of lingual surface of ridge, hence the flange will be suspended under the tongue in soft tissues in a direction parallel to the direction of the mylohyoid muscle
• Advantage of this:• Lack of direct pressure on this sharp edge of bone will
reduce chances of soreness• Completion of border seal• Even during muscle contraction of mylohyoid muscle the
denture will not be displace

• During rest when the mylohyoid lies low, there will be a space between the mylohyoid muscle and the denture border
• But during muscle contraction this gap will close
• The final length and breadth of the flange can only be determined by skillful border moulding and impression procedure
• On an average the denture border lies usually 4-6mm below the mylohyoid line, but it varies from patient to patient

Sublingual gland• They are located above the mylohyoid muscle• Their size usually varies from small to big enough
to lie at a level higher than the residual ridge

• Usually very soft and displaceable
• The sublingual gland cannot be visualised and need to be palpated
• Unless they are firm, they do not influence the impression much

DISTOLINGUAL VESTIBULE• Also known as lateral throat form or
retromylohyoid fossa• Bound • Anteriorly – Mylohyoid Muscle• Laterally – Pear Shaped Pad• Postero-laterally – Superior Constrictor Muscle• Postero-medially – Palatoglossus• Medially – Tongue

• The superior constrictor muscle originates from the pterygomandibualr raphe
• This raphe arises from the hamular process of the medial pterygoid plate and gets attached to the mylohyoid ridge. This raphe also gives origin to the buccinator along with the superior constrictor
• The posterior extent of the mandibular denture is determined by the palatoglossus muscle and some what by the weaker superior constrictor muscle, which is easily displaceable
• This area is known as the retromylohyoid curatin

• The retromylohyoid curtain:• Overlies the superior constrictor muscle in the postero-
lateral portion• Covers the palatoglossus and the lateral surface of the
tongue in the postero-medial portion• The medial pterygoid muscle lies just posterior to it
• Contraction of medial pterygoid can cause a bulge in the wall of Retromylohyoid curtain


• The ‘S’ curve of the mandibular denture, results from the stronger intrinsic and extrinsic tongue muscles, which usually places the retromylohyoid borders more laterally and toward the retromolar fossa than in the mylohyoid area

• Neil classified the Lateral Throat Form:
• CLASS I• The anatomic structure will accommodate a fairly long
and wide flange• Thickness can vary from 2-3mm upto 4-5mm for better
seal if the border is flat• The retromylohyoid curtain area should be thinner (2-
3mm) and very rounded and smooth so as not to interfere with the palatoglossus muscle

• CLASS III• It has minimum length• Border usually ends 2-3mm below the mylohyoid ridge, or sometimes, at the mylohyoid ridge• Thickness should be no more than 2mm, or even knife edged if it has to end at the mylohyoid ridge

• CLASS II:• Half as long and wide as Class I• Twice as long as Class III•Most common

1. Mylohyoid muscle2. Palatoglossus muscle3. Superior constrictor muscle4. Pterygomandibuilar raphe5. Buccinator muscle

• The proper extension of the mandibular denture into the lingual sulcus, within their anatomical and functional limits, ensure a proper peripheral seal
• Also, these flanges present favorable inclined planes to the tongue resulting in vectors of forces that help maintain the mandibular denture in place

RELIEF AREAS
• These are the areas that cannot bear the forces of occlusion
• These areas in the mandibular arch are:• Mylohyoid ridge• Mental foramen• Genial tubercles• Mandibular tori

• Soft tissues often hide the sharpness of the mylohyoid ridge which can be found by palpation.
• Mucous membrane over a sharp or irregular mylohyoid ridge will be easily traumatized by denture base, unless relief is provided in the denture base.
Mylohyoid ridge

Mental foramen
• As resorption takes place, the mental foramen will come to lie closer to the crest of ridge.
• In these circumstances, the mental nerve and blood vessels may be compressed by denture base unless relief is provided.
• Pressure on mental nerve can cause numbness of lower lip.

Severely resorbed mandible with the mental foramen placed close to crest of the ridge

Genial tubercles
• Like the mental foramina, the genial tubercles usually lie well away from the crest of the ridge.
• With resorption they becomes prominent and closer to crest
• In severly resorbed cases they may rerquire surgical correction

Torus Mandibularis
• Torus mandibularis is a bony prominence.• Usually found bilaterally and lingually
near the first and second premolars.

• Superior border of the torus may be flush with crest of the residual ridge in severe resorption
• The torus mandibularis is covered by an extremely thin layer mucous membrane
• It can be difficult to provide relief within the denture without breaking the border seal
• It often needs surgical removal

MUSCLE ATTACGHMENTS TO THE MANDIBLE
• Buccal or Facial attachments• Mentalis muscle• Buccinator
muscle• Masseter muscle• Platysma• Depressor anguli
oris• Depressor labi
inferioris

• Lingual or Medial attachments• Mylohyoid muscle• Genioglossus muscle• Medial pterygoid
muscle• Lateral pterygoid
muscle• Temporalis muscle

• Muscles of mastication have their origin from the bone of the skull and is attached to the mandible.
• These muscles are involved not only in the masticatory movements of the mandible, but also in the nonmasticatory movements.
MUSCLES OF MASTICATION

MASSETER
• It is a quadrilateral muscle that covers the lateral surface of the ramus of the mandible
• It has three layers:• Superficial• Middle • Deep

• Origin:• Zygomatic arch
• Insertion• Superficial: Lower part of lateral
surface of ramus• Middle: Middle part of ramus• Deep: Upper part of ramus
• Action• Elevates the mandible to bite
• Influence in prosthodontics:• Distobuccal flange on lower
denture

TEMPORALIS• It is a fan shaped muscle• It fills the temporal fossa
• Origin:• Temporal fossa• Temporal fascia
• Insertion:• Margins and deep surface of coronoid process• Anterior border of ramus

• Action:• Elevates the mandible• Postrerior fibers retract the protruded mandible• Helps in side to side grinding movement

• Significance of temporalis in prosthodontics:• It may affect the mandibular posterior denture border• Elevator muscle -- co ordinates the closing movements, brings teeth in contact• Significant positioning muscle of the mandible.

MEDIAL PTERYGOID• It is a quadrilateral muscle • It has two heads• Superficial• Deep
• Action:• Elevation• Protrusion • Unilateral contraction brings about movement of the
mandible to the opposite site

• Origin:• Superficial head – tuberosity of maxilla and adjoining bone• Deep head – medial surface of the lateral pterygoid and
adjoining process of palatine plate
• Insertion• Roughened area on the medial surface of angle and
adjoining ramus of the mandible
Medial pterygoid m.

LATERAL PTERYGOID
• It is a short conical muscle• It has two heads• Upper head (smaller)• Lower head (larger)
• Origin:• Upper head – infratemporal surface and greater
wing of sphenoid• Lower head – lateral surface of lateral pterygoid
plate

• Insertion • Pterygoid fovea on the anterior surface of the neck of the condyle• Anterior margin of articular disc and capsule of temporomandibular joint
lateral pterygoid m.

• Actions:• Bilateral contraction • brings about protrusion by pulling condyle down the
eminence (acts with depressors)• Unilateral contraction • creates a mediotrusive movement of that condyle• causes a lateral movement of the mandible to the same
side
• Inactive during jaw opening, becomes active only in conjunction with the elevators.
• Especially active during power stroke & when teeth are held together.

BUCCINATOR
• Buccinator is a broad band of the muscle, forming the entire side wall of the cheek.
• It passes along the outer surface of the maxilla and mandible until it reaches the ramus, where it passes to the lingual surface to join the superior constrictor at the pterygomandibular raphe.

It originates in three sets of fibres with separate innervations –
• Upper fibres• Middle fibres• Lower fibres
• The middle fibres constitute the most active muscle, whose function is primarily to control the food bolus during mastication.
• They also cross the modiolus and called orbicularis oris muscle.
Buccinator muscle

• The upper and lower fibres are relatively flaccid, especially at the area of origin.
• The insertion of the buccinator muscle into and
through the modiolus, permits this muscle to move the angle of the mouth:
• backward, with the middle fibres.• upwards with the upper fibres.• downwards with the lower fibres.

GENIOGLOSSUS• A fan shaped muscle which forms the main bulk of
the tongue• Origin - Genial tubercles
• Insertion• Upper fibers – into the tip• Middle fibers – dorsum of the tongue• Lower fibers – hyoid bone
• Action• Upper fibers – retract tip• Middle fibers – depress tongue• Lower fibers – protrude tongue

MYLOHYOID• Flat, triangular muscle• Origin – mylohyoid line on mandible
• Insertion • posterior fibers – body of hyoid bone• Middle and anterior fibers – median raphe between
mandible and hyoid bone
• Action• Elevates floor of the mouth• Depression of mandible• Elevate the hyoid

APPLIED ANATOMY FOR DENTAL IMPLANTS
• MANDIBULAR CANAL AND MENTAL FORAMEN• The canal - may be placed at high, low or intermediate
location may be divided into two or three rami• Hence it is essential to conduct proper radiographic
examination using conventional and tomographic radiography, as well as MRI
• At the distal aspect of first molar, the canal is at its lowest point. So this is the safest place for implant placement
• In the horizontal plane , the canal: -begins posteriorly at the lingual cortical plate -crosses over laterally to the buccal cortex to exit at the mental foramen --1stmolar region: midway between the two cortical plates

• An adequate safety margin of about 2 mm above the inferior alveolar canal is recommended
• In excessively resorbed ridge, the mental foramen with its neurovascular contents can be found on the crest of the ridge.
• Surgical manipulation of mucoperiosteum in this region must avoid the injury to these vital structures

• Lingual nerve• Since the nerve lies just medial to the retromolar pad,
incision in this region should remain lateral to the pad
• Nerve to mylohyoid • Motor branch of inferior alveolar nerve given off just
before the nerve enters the mandibular foramen.• Since the nerve is closely related to the ramus of
mandible, surgical interventions in this area may lead to injury of this important motor nerve.

• Long buccal nerve• Nerve courses between the two heads of lateral pterygoid
muscle, then proceeds medial to and sometimes within the medial tendon of temporalis, to gain access to the surface of buccinator muscle• Surgical manipulation in this area during insertion of a sub
periosteal implant may injure this nerve.

• Mucoperiosteal reflection• While reflecting the mucoperiosteal flap for subperiosteal
implants, lingually the mylohyoid muscle gets reflected in the second molar region• Similarly, surgical manipulation of the tissue of the floor of
the mouth may lead to edematous swelling of the sublingual space• Ecchymosis from blood accumulation may occur in
sublingual or submandibular space

• Superior genial tubercles • May be located near to the crest of mandibular edentulous
ridges.• Hence the muscle also has the chance of getting detached
when mucoperiosteal flap is reflected lingually• However, the muscle should not be completely detached
from the tubercle, as this may result in retrusion of the tongue and possible airway obstruction.
• Attachment of the temporalis muscle• Superficial tendon located laterally and deep tendon
medially.• The incisions placed on the anterior ascending ramus for
subperiosteal or blade implants should be inferior to the insertion of the two tendons of temporalis

• Mentalis muscle attachment• Complete reflection of mentalis muscles for the purpose
of extension of a subperiosteal implant or symphyseal intraoral graft may result in “witch’s chin”, probably caused by the failure of muscle reattachment.• If the muscle is completely detached to expose the
symphysis then an elastic bandage is applied externally• Hence, the inferior portion of the mental protuberance
should not be interfered with.

• Infection, in some cases, may start and spread lingually and lead to an abscess or cellulitis in the sublingual or submandibular space
• Extensive bilateral sublingual and submandibular cellulitis is a life threatening condition known commonly as – Ludwig’s Angina
• Masseter muscle• The muscle can be easily deflected during surgery to
expose the bone for the ramus extension needed for lateral support of the subperiosteal implant.• The space between the masseteric fascia and the muscle
is a potential surgical space, the masseteric space, into which the infection may spread, causing myositis and trismus

• Medial pterygoid muscle• Forms the medial boundary for pterygomandibular space• This space is entered when an inferior alveolar nerve
block is administered. This space may also be entered when surgery for unilateral subperiosteal implant is performed• Infection of this space is dangerous because of its
proximity to the parapharyngeal spaces and potential of the infection to spread into mediastinum

Available bone angulation.• Ideally it is aligned with the forces of occlusion
and is parallel to the long axis of the prosthodontic restoration.
• The alveolar bone angulation represents the root trajectory in relation to the occlusal plane.
• Rarely does this bone angulation remain constant after the loss of teeth
• Posterior mandibular region.• Submandibular fossa mandates implant placement with
increasing angulation as they progress distally.• Second premolar region – 10 degrees• First molar region – 15 degrees• Second molar region – 20-25 degrees.

INNERVATION OF THE MANDIBLE• INFERIOR ALVEOLAR NERVE• Branch of posterior division of Mandibular nerve• It appears at the inferior border of the lateral pterygoid
muscle, courses downward and enters the mandibular foramen on medial aspect of the mandible• Branches:• Nerve to mylohyoid• Mental nerve• Incisive nerve

• LINGUAL NERVE• Branch of posterior division of Mandibular nerve• It also appears at the inferior border of the lateral
pterygoid muscle anterior to the inferior alveolar nerve and enters the oral cavity above the posterior edge of the mylohyoid muscle• It is joined by the chorda tympani nerve in the infra-
temporal fossa which carries taste fibers from anterior 2/3rd of the tongue
• LONG BUCCAL NERVE• Sensory branch of the mandibular division of the
trigeminal nerve• Supply skin and mucous membrane of the cheek and the
buccal mucosa opposite the mandibular molar region

BLOOD SUPPLY OF THE MANDIBLE
• INFERIOR ALVEOLAR ARTERY• Enters mandible along with the
inferior alveolar nerve• Gives off lingual artery before
entering the mandibular canal
• Coronoid process, condylar process, angle of the mandible • Blood supply is by the arteries that
supply the muscles that attach to these sites
• Periosteal vessels

CHANGES IN BLOOD SUPPLY OF MANDIBLE WITH AGE:• Blood circulation in young adults – centrifugal• With age – direction of blood flow may reverse• Inferior alveolar artery is prone to arteriosclerotic
changes• Reduction in blood flow may be associated with
tooth extraction.

• The blood flow may become almost negligible. In such cases the mandibles receives blood from:• Periosteal vessels• Mandibular branch of sublingual artery• Facial artery• Muscular branches of maxillary artery• These anastomoses are critical in case of implant
dentistry as dehiscence of mucosa at the incision lines during flap reflection have been reported.

AGE CHANGES IN THE MANDIBLE
• After birth the two segments of the bone become joined at the symphysis, from below upward during the first year
• but a trace of separation may be visible in the beginning of the second year near the alveolar margin.
• Once the teeth erupt, the body becomes elongated in its whole length, but more especially behind the mental foramen, to provide space for the three additional teeth developed in this part.

• The depth of the body increases owing to increased growth of the alveolar part, to afford room for the roots of the teeth, and by thickening of the subdental portion which enables the jaw to withstand the powerful action of the masticatory muscles.
• The mandibular canal, after the second dentition, is situated just above the level of the mylohyoid line; and the mental foramen occupies the position usual to it in the adult.
• The angle becomes less obtuse, owing to the separation of the jaws by the teeth. By about the fourth year it is 140°.

• In the adult • the alveolar and subdental portions of the body
are usually of equal depth. • The mental foramen opens midway between the
upper and lower borders of the bone, and the mandibular canal runs nearly parallel with the mylohyoid line.
• The ramus is almost vertical in direction, the angle measuring from 110° to 120°.

• In old age the bone reduces in size due to the loss of the teeth the and, consequently, the chief part of the bone is below the oblique line.
• The mandibular canal, with the mental foramen opening from it, is close to the alveolar border.
• The ramus is oblique in direction, the angle measures about 140°, and the neck of the condyle is more or less bent backward.

• The bone mass is maximum at during midlife• The turnover and metabolism of the bone undergo
a change with age, and in older individuals, the resorption surpasses the formation of bone
• Residual ridge resorption may also be a manifestation of type I or post-menopausal osteoporosis

• Progressive resorption of the ridges makes the mandible wider and the maxilla narrower
The lines A and B represent the centres of the ridges. The distance between them becomes greater as the maxilla and
mandible resorb

Saliva
• Older people take a vast variety of potentially xerostomic drugs for allergies, heart problems etc
• Sjogren’s syndrome and radiation treatment also reduce salivary flow
• Even though the change in quality of saliva may not be evident on initial clinical examination, it should be suspected as a cause for denture intolerance if a patient is on multiple medications

Mucosa
• Stomatitis and other mild inflammations are the most commonly encountered in older edentulous mouths
• External carcinogens such as nicotine and alcohol become more damaging to the oral mucosa with age due to atrophy

CONCLUSION
• The knowledge of oral anatomy, microscopic as well as macroscopic better equips us as prosthodontists to • Decide how to make the impression•What material to use• How to plan the treatment
• All this will result in a successful prosthetic treatment

REFERNCES• Gray’s Anatomy : The Anatomical Basis Of Clinical
Practice, 14th edition. Elsevier ,2008• T.W.sadler : Langman’s Medical Embryology, 11th
edition. • Zarb Bolender, Biological considerations of
mandibular impressions. : Boucher’s Prosthodontic Treatment For Edentulous Patients, 9th Edition. 174-203
• Charles M.Heartwell : Syllabus Of Complete Dentures, 4th Edition.
• Gray’s anatomy, The anatomical basis of clinical practice. 455-92
• Bocage M, Lehrhaupt J. Lingual flange design in complete dentures. J Prosthet Dent. 1977 May;37(5):499-506.

• Chaurasia B.D. Osteology of head and neck. In Human anatomy dissection and Clinical Volume 3 Head, Neck and Brain 4th Edition. CBS publishing.31-4
• Chaurasia B.D. Temporal; and infratemporal fossa. In Human anatomy dissection and Clinical Volume 3 Head, Neck and Brain 4th Edition. CBS publishing. 144-151
• Levin B. Related Anatomy, Impressions for Complete Dentures. Quintessence publishing Co.,1984. 35-60
• Carl E. Misch, Contemporary Implant Dentistry 3rd edition. Elsevier
• Roberts, A.C. Full denture impression making. J. Prosthet. Dent. 1:213-228, 1951