Mandible Final Ppt.
105
Dr Honey Arora Post Graduate Student Department of Prosthodontics and Implantology MANDIBLE 1
-
Upload
honey-arora -
Category
Documents
-
view
3.503 -
download
71
Transcript of Mandible Final Ppt.

1
Dr Honey Arora
Post Graduate Student
Department of Prosthodontics and Implantology
MANDIBLE

2
INTRODUCTIONOSTEOLOGYMUSCLE ATTACHMENT OF THE
MANDIBLEGROWTH AND DEVELOPMENTMANDIBLE IN COMPLETE DENTURE
CONTENTS

3
The mandible is derived from Latin word mandibula, "jawbone“.
Also referred as inferior maxillary bone Is the largest and strongest bone of the
face, serves for the reception of the lower teeth. It consists of a curved, horizontal portion, the body, and two perpendicular portions, the rami.
INTRODUCTION

4
OSTEOLOGY OF MANDIBLE

5
BODY OF MANDIBLE
corpus mandibulae The body is curved somewhat like a
horseshoe and has two surfaces and two borders.
- 2 surfaces – External Internal- 2 borders – Superior or Alveolar Inferior

6
MENTAL FORAMEN- It lies below the interval between the
premolar teeth, on the either side, midway between the upper and lower borders of the body.
It is the passage of the mental vessels and nerve. descends slightly in edentulous individualsAbsence of mental foramen and accessory mental
foramina has also been reported.[1][2]shape of the MF was oval inmost of the cases.[3] [4]Central African Journal of Medicine
STRUCTURES ON THE EXTERNAL SURFACE

7
MENTAL PROTUBERANCE- It is a median triangular projecting
area in the lower part of the midline. - The inferolateral angles of the protuberance
from the mental tubercules.

8
EXTERNAL OBLIQUE LINE It is a faint ridge running backward
and upward from each mental foramen and is continuous with the anterior border of the ramus.

9
INCISIVE FOSSA It is a depression that lies just
below the incisor teeth on the either side of the symphysis.
(no. 11 is incisive fossa)

10
MENTAL SPINES (GENIAL TUBERCULE / GENIAL APOPHYSIS)
There are 2 pairs of spines .1. Superior pair of spine –. It gives origin to the
Genioglossi and 2. Inferior pair of spines – lies immediately below the first
pair, gives origin of the Geniohyoid. SPECIAL CASES
- May be fused to form a single eminence. - A median foramen and furrow are sometimes seen above the mental spines( spinous Foramen)[6]
STRUCTURES ON THE INTERNAL SURFACE

11
ATTACHMENT OF ANTERIOR BELLY OF DIGASTRIC
It is an oval depression on the either side of the mid line jus below the mental spines for the attachment of anterior belly of digastric .

12
MYLOHYOID LINE It extends upward and backward on either
side from the lower part of the symphysis .(figure b)- It gives origin to the mylohyoid.- posterior part of this line - gives attachment to a
small part of the superior constrictor and to the pterygomandibular raphe.
-Above the anterior part of this line - is a smoothtriangular area against which the sublingual gland rests.- below the hinder part, an oval fossa for the submaxillary gland.

13

14
SUPERIOR OR ALVEOLAR BORDER –- wider behind than in front- is hollowed into cavities, for the reception of
the teeth; these cavities are sixteen in number.
- outer lip of the superior border - on either side, the buccinator is attached as far
forward as the first molar tooth.
STRUCTURES PRESENT AT THE BORDERS

15
INFERIOR BORDER - rounded, longer than the superior, and
thicker in front than behind.- point where it joins the lower border of the
ramus - A shallow groove; for the FACIAL ARTERY , may be present.

16
ramus mandibulæ; perpendicular portion The ramus is quadrilateral in
shape, and has two surfaces, four borders, and two processes
RAMUS OF MANDIBLE

17
LATERAL SURFACE
- Lateral surface is flat and marked by oblique ridges at its lower part.
- It gives attachment nearly the whole of its extent to the masseter.

18
MEDIAL SURFACE
MANDIBULAR FORAMEN It provides entrance for the inferior
alveolar nerve and vessels.

19
LINGULA OR LINGULAE MANDIBULAE it is a sharp spine present in front
of mandibular foramen opening .- It gives attachment to the spenomandibular
ligament

20
MYLOHYOID GROOVE From the lower and back part of the
lingulae mandibulae is a notch from which the mylohyoid groove runs obliquely downward and forward.
- It lodges the mylohyoid vessels and nerve.

21
MANDIBULAR CANAL The mandibular canal is a canal
within the mandible that contains the inferior alveolar nerve ,inferior alveolar artery, and inferior alveolar veins.
runs obliquely downward and forward in the ramus
then horizontally forward in the body
communicates with alveoli by small openings

22
Types of mandibular canal [5]1. TYPE III - the canal is located close to the
lower border of the mandible is the most common,
2. TYPE II -the canal is noted between the apices of the first and second molars and the lower border of the mandible
3. TYPE I -the canal is in close contact with the apices of the first and the second molars
Hell Period 1990

23
LOWER BORDER – Is marked by oblique ridges on each
side, for the attachment of the Masseter laterally, and the pterygoideus internus medially; the sphenomandibular ligament is attached to the angle between these muscles.

24
ANTERIOR BORDER – Is thin above, thicker below, and
continuous with the oblique line.POSTERIOR BORDER – Is thick, smooth, rounded, and covered
by the parotid gland.

25
UPPER BORDER – Is thin, and is surmounted by 2 processes - the coronoid in front the condyloid behind, separated by a deep concavity, the
mandibular notch.

26
processus condyloideus Is thicker than the coronoid, and
consists of two portions: the condyle, and the constricted portion which supports it, the neck.
It forms the articular surface for articulation with articular disk of tempromandibular joint.
CONDYLOID PROCESS

27
THE CONDYLE - It presents an articular
surface for articulation with the articular disk of the temporomandibular joint
- At the lateral extremity of the condyle is a small tubercle for the attachment of the temporomandibular ligament.

28
THE NECK – The neck is flattened from backward, and
strengthened by ridges which descend from the forepart and sides of the condyle.
- Its posterior surface is convex- its anterior surface presents a depression for
the attachment of the Pterygoideus externus.

29
processus coronoideus Is a thin, triangular eminence,
which is flattened from side to side and varies in shape and size.
The Coronoid process (from Greek korone, "like a crown")
CORONOID PROCESS

30
BORDERS
anterior border - is convex and is continuous below with the anterior border of the ramus.
posterior border- is concave and forms the anterior
boundary of the mandibular notch.

31
SURFACESLateral Surface - affords insertion to the
Temporalis and Masseter.Medial Surface -provides insertion to the
Temporalis and presents a ridge from apex till last molar
Between This Ridge And The Anterior Border - is a grooved triangular area, the upper part of which gives attachment to the Temporalis, the lower part to some fibers of the buccinator.

32
It is the faint ridge on the median line of the external surface of the mandible.
This ridge divides below and encloses a triangular
eminence, the mental protuberance,
the base of which is depressed in the center but raised on either side to form the mental
tubercule.It serves as the origin for the Geniohyoid and the Genioglossus
SYMPHYSIS MENTI

33
It is the junction of the lower border of the ramus of the mandible with the posterior border of body of mandible
Provides attachment - Masseter laterally - the Pterygoideus internus medially - the stylomandibular ligament is attached to the angle between these muscles.
ANGLE OF MANDIBLE

34
Sub-mandibular: run along the underside of the jaw on either side, drains the structures in the floor of the mouth also drain mandibular teeth except the central incisors.
Sub-mental: These nodes are just below the chin. They drain the central incisors and midline of lower lip and tip of the tongue.
LYMPHATICS

35
mainy by the 3rd division of trigeminal nerve -> mandibular nerve
INFERIOR ALVEOLAR NERVE, branch of the mandibular division -> enters mandibular foramen and runs forward in the mandibular canal, supplying sensation to the teeth->at mental foramen the nerve divides into two terminal branches: incisive and mental nerves-> The incisive nerve runs forward in the mandible and supplies the anterior teeth. The mental nerve exits the mental foramen and supplies sensation to the lower lip.
NERVE SUPPLY

36
MUSCLE ATTACHMENT TO THE MANDIBLE
INTERNAL SURFACE

37
EXTERNAL SURFACE

38
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE
SUPPLY
ACTION & CLINICAL
SIGNIFICANCE
MASSETERmusculus masseter( Greek word chewing , associated with anger )
ORIGIN –Zygomatic arch
Blood supply Masseteric Artery Nerve supply: Masseteric Nerve
Elevation and retraction of the mandibleAntagonist muscle – platysma
INSERTION –Coronoid process and ramus of mandible
TEMPORALISmusculus temporalis
ORIGIN – Temporal line on the parietal bone of the skull
Blood supply : Deep temporal artery Nerve supply: Mandibular nerve
Elevation and retraction of the mandibleAntagonist muscle - platysmaINSERTION –
Coronoid process of mandible

39
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE
SUPPLY
ACTION
MEDIAL PTERYGOIDmusculus pterygoideus internus
ORIGIN –Medial surface of lateral pterygoid plate of sphenoid, palatine bone , pterygoid fossa
Blood supply:Medial pterygoid arteryNerve supply: Medial pterygoid Nerve
Elevates mandible, closes jaw, helps lateral pterygoids in moving the jaw from side to side
INSERTION –Inner surface of ramus ,Angle of the mandible
LATERAL PTERYGOID m. pterygoideus externus
ORIGIN – • Superior head: lateral surface of the greater wing of the sphenoid• Inferior head: lateral surface of the lateral pterygoid plate
Blood supply:Lateral pterygoid arteryNerve supply: lateral pterygoid Nerve
Depresses mandible, Protrude mandible, side to side movement of mandible
INSERTION –neck of the mandibular condyle , articular disk of the TMJ

40
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE
SUPPLY
ACTION
DEPRESSORANGULI ORIS (musculus depressor anguli oris)
ORIGIN –• along the oblique line of mandible • lateral aspect of mental tubercle of the mandible
Blood supply:Facial arteryNerve supply: Mandibular branch of facial Nerve
Depresses the mouth as in frowning
INSERTION –modiolus
DEPRESSOR LABII INFERIORISmusculus depressor labii inferioris
ORIGIN – Oblique line of mandible, between symphysis and mental foramen
Blood supply:Facial arteryNerve supply: Mandibular branch of facial Nerve
Draws the lip downward and laterally
INSERTION –Skin of the lower lip

41
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE
SUPPLY
ACTION
BUCCINATORmusculus buccinator
ORIGIN –Posterior alveolar process of maxilla and mandible
Blood supply :Buccal arteryNerve supply: buccal branch of facial nerve
The buccinator compresses the cheeks against the teeth and is used in acts such as blowing. It is an assistant muscle of mastication(chewing).
INSERTION –modiolus
ORBICULARISORIS
ORIGIN – Near midline on anterior surface of maxilla and mandible and modiolus at angle of mouth
Blood supply :Facial arteryNerve supply: buccal branch of facial nerve
Narrows orifice of mouth, purses lips and puckers lip edges
INSERTION –Mucous membrane of margin of lips and raphe with buccinator at modiolus

42
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE
SUPPLY
ACTION
MENTALIS(so named because it is associated with thinking or concentration and use to express doubt)
ORIGIN –Symphysis of mandible
Blood supply :Buccal arteryNerve supply: mandibular branch of facial nerve
elevates and wrinkles skin of chin, protrudes lower lip
INSERTION –Skin of chin
PLATYSMA ORIGIN – subcutaneous tissue of infraclavicular and supraclavicular regions
Blood supply :branches of the Submental artery and Suprascapular arteryNerve supply: cervical branch of the facial nerve
Draws the corners of the mouth inferiorly and widens it (as in expressions of sadness and fright). Also draws the skin of the neck superiorly when teeth are clenched
INSERTION –base of mandible; skin of cheek and lower lip; angle of mouth; orbicularis oris

43
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE
SUPPLY
ACTION
GENIOGLOSSUSmusculus genioglossus
ORIGIN –Superior part of mental spine of mandible
Blood supply:Lingual arteryNerve supply: Hypoglossal nerve
Inferior fibers protrude the tongue, middle fibers depress the tongue, and its superior fibers draw the tip back and down
INSERTION –Dorsum of tongue and body of hyoid
GENIOHYOID musculus geniohyoideus
ORIGIN – Inferior mental spine on the inner surface of the symphi
Blood supply :Lingual arteryNerve supply: C1 and Hypoglossal nerve
Elevates the tongue, depress the mandible , helps in deglutition
INSERTION –Body of hyoid bone

44
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE SUPPLY
ACTION
ANTERIOR BELLY OF DIGASTRIC musculus digastricus
ORIGIN –digastric fossa (mandible)
Blood supply:anterior belly - Submental branch of facial artery;Nerve supply: mandibular division (V3) of the trigeminal (CN V) via the mylohyoid nerve
Opens the jaw when the masseter and the temporalis are relaxed.
INSERTION –Intermediate tendon (hyoid bone)
MYLOHYOIDmusculus mylohyoideus
ORIGIN – inner surface of mandible off the mylohyoid line
Blood supply :mylohyoid branch of inferior alveolar arteryNerve supply: mylohyoid nerve
Raises oral cavity floor, elevates hyoid, elevates tongue, depresses mandibleINSERTION –
body of hyoid bone and median raphe

45
MUSCLE ORIGIN AND INSERTION
BLOOD & NERVE SUPPLY
ACTION
SUPERIOR CONSTRICTOR
ORIGIN –pterygoid hamulus, pterygomandibular raphe, posterior end of the mylohyoid line of the mandible, and side of tongue.
Blood supply:Ascending pharyngeal artery and tonsillar branch of facial arteryNerve supply: pharyngeal plexus of nerves(IX , X and cervical sympathetic ganglion )
deglutition
INSERTION –median raphe of pharynx and pharyngeal tubercle.

46
LIGAMENT ORIGIN AND INSERTION
DESCRIPTION
STYLOMANDIBULAR LIGAMENT
ORIGIN –Apex of styloid process of the temporal bone
Paired , it is the thickening of parotid fascia,from its deep surface some fibers of the Styloglossus take origin.
INSERTION –to the angle and posterior border of the angle of mandible
SPHENOMANDIBULAR LIGAMENT
ORIGIN – the ligament that attaches to the spine of the sphenoid bone superiorly
• paired; pterygoid fascia thickening and is a remnant of the Meckel's cartilage• limit distension of the mandible in an inferior direction.• its related to lateral pterygoid (laterally ) and medial pterygoid (medially)
INSERTION –the lingula of the mandible inferiorly

47
PTERYGOMANDIBULAR RAPHE (LIGAMENT) Tendinous band of buccopharyngeal fascia
passes between the tip of the hamulus of the pterygoid bone and the internal surface of the mandible at a point just posterosuperior to the posterior limit of the mylohyoid ridge
medial surface - covered by the mucous membrane. lateral surface - is separated from the ramus of the mandible by a quantity of adipose tissue. posterior border- gives attachment to the superior pharyngeal constrictor muscle. anterior border attaches to the posterior edge of the buccinator

48
GROWTH AND DEVELOPMENT

49
Prenatal Week 6 - Intramembranous ossification center develops lateral to
Meckel's cartilage. Week 7 - Coronoid process begins differentiating. Week 8 - Coronoid process fuses with main mandibular mass. Week 10 (approx) - Both condylar and coronoid processes are
recognizable and anterior portion of Meckel's cartilage begins to ossify.
Weeks 12-14 - Secondary cartilages for the condyle, coronoid, and symphysis appear.
Weeks 14-16 - Deciduous tooth germs start to form.
Birth At birth mandible still has separate right and left halves.
Postnatal Year 1 - Fusion of right and left halves of mandible at the
symphysis. Infancy and childhood - Increase in both size and shape of the
mandible; eruption and replacement of teeth. Year 12-14 - All permanent teeth emerged except third molars.

50
The mandible makes its structure in the sixth week of foetal life.
It is ossified in the fibrous membrane covering the outer surfaces of Meckel's cartilages, derrivative of first brachial arch
These cartilages form the cartilaginous bar of the mandibular arch and are two in number, a right and a left.
BODY OF MANDIBLE

51
Their proximal or cranial ends are connected with the ear capsules, and their distal extremities are joined to one another at the symphysis by mesodermal tissue.
INCUS 51
MALLEUS

52
Meckel’s cartilage has a close, relationship to the mandibular nerve, at the junction between posterior and middle thirds, where the mandibular nerve divides into the lingual and inferior alveolar nerve.

53
The lingual nerve passes forward, on the medial side of the cartilage, while the inferior Alveolar lies lateral to its upper margins & runs forward parallel to it and terminates by dividing into the mental and incisive branches.

54
LINGULA is replaced by fibrous tissue, which persists to form the sphenomandibular ligament & the perichondrium of the cartilage persist as sphenomallular ligament.
Between the lingula and the canine tooth the cartilage disappears, while the portion of it below and behind the incisor teeth becomes ossified and incorporated with this part of the mandible.

55
Greater part of Meckel’s cartilage disappears without contributing to the formation of mandible.
Small part of cartilage near the midline is the site of endochondral ossification. Here it calcifies and is destroyed by chondroblasts and are replaced by connective tissue and then by bone.
Small irregular bones known as mental ossicles develop in it and by the end of first year fuse with the mandibular body.
At the same time two halves of mandible unite by ossification of the symphyseal fibrocartilage.
REMANATS OF MECKEL CARTILAGE

The ramus of the mandible develops by a rapid spread of ossification backwards into the mesenchyme of the first branchial arch diverging away from Meckel’s cartilage. This point of divergence is marked by the mandibular foramen.
56
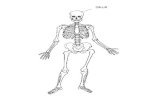
Mandible of human embryo 95 mm. long. Outer aspect. Nuclei of cartilage stippled.

57
Somewhat later, accessory nuclei of cartilage make their appearance:
a wedge-shaped nucleus in the condyloid process and extending downward through the ramus.
a small strip along the anterior border of the coronoid process.
.
Mandible of human embryo 95 mm. long. Outer aspect. Nuclei of cartilage stippled.

58
The condylar cartilage:Carrot shaped cartilage appears in the region of the
condyle and occupies most of the developing ramus. It is rapidly converted to bone by endochondral ossification (14th. WIU) it gives rise to -> Condyle head and neck of the mandible.
• The posterior half of the ramus to the level of inferior dental foramen

59
The coronoid cartilage:It is relatively transient growth cartilage center ( 4th. -
6th. MIU). it gives rise to -> Coronoid process.
• The anterior half of the ramus to the level of inferior dental foramen

60
GROWTH OF MANDIBLE

61
Growth of the mandible
I. Growth by secondary cartilage
II. Development of the alveolar process
III. Subperiosteal bone appositionand bone resorption

62
I. Growth by secondary cartilage ( mainly condylar cartilage )
Increase in height of the mandibular ramus
Increase in the over all lengthof the mandible
Increase of the inter condylar distance

63
II DEVELOPMENT OF ALVEOLAR PROCESS
bone apposition occurs at the crest of the alveolar process and the fundus of the alveolus contributing to the growth of mandible in height.

Bone deposition
Bone resorption
Result in
External surface of the
mandible
Inner surface of the
mandible
Increase the transeverse dimension
Posterior border of the
ramus
Anterior border of the
ramus
Adjust the thickness of the ramus
Anterior border of the
coronoid process
Posterior border of the
coronoid process
Displacement of the
coronoid process
Chin region ــــــــــــــــــــــــ Modeling of the lower face
64
III. Subperiosteal bone apposition and bone resorption:

65
COMPLETE DENTURES

66
The available area of support from an edentulous mandible is
14 cm2 while the same for the edentulous maxilla is 24cm2 .
The landmarks can be broadly grouped into:
Limiting structures:Labial frenum Labial vestibuleBuccal frenumBuccal vestibuleLingual frenumAlveololingual sulcusRetromolar padsPterygomandibular raphe.
ANATOMICAL LANDMARK

67
Supporting structures:Buccal shelf areaResidual alveolar ridge
Relief areas:Crest of the residual alveolar ridgeMental foramenGenial tuberclesTorus mandibularis.

68
These are the sites that will guide us in having an optimum extension of the denture so as to engage maximum surface area without encroaching upon the muscle actions
Encroaching upon these structures will lead to dislodgement
of thedenture and/or soreness
of thearea while failure to
cover the areas upto the
limiting structurewill imply
decreased retention stability
and support.
LIMITING STRUCTURES

Masticatory forces produce quite a pressure on the underlying structures and not everyplace beneath the denture can take such stress hence we need to know the areas which can bear the stresses well.
These can be divided into-1.Primary stress bearing area2.Secondary stress bearing area
SUPPORTING/ STRESS BEARING AREA
69

70
PRIMARY STRESS BEARING AREA
These are the areas that are most capable to take
the masticatory load providing a proper support
to the denture.- Are at right angle and usually do not resorb
easily ( buccal shelf area )
Properties :-
1.Tightly adherent sufficient fibrous connective
tissue with an overlying keratinized mucosa
2.Presence of cortical bone cover
3.Should be at right angles to the vertical occlusal forces.
4.No underlying structures should be present that will get harmed due to stress.

71
SECONDARY STRESS BEARING AREA
Area of edentulous ridge that are greater than or at right angle to occlusal forces but tend to resorb under load.
Mandibular:- ridge slopes Secondary stress bearing area
Secondary stress bearing area

72
These are the areas which either resorb under constant load or have fragile structures within or are covered by thin mucosa which can be easily traumatized
& hence should be relieved.
RELIEF AREAS

73
Fibrous band extending fromthe labial aspect of the residualalveolar ridge to the lip.Give attachment to orbicularis oris and incisivus.Active and sensitive frenumThe activity of this area tends to be vertical so the
labial notch on the denture should be narrow.
LABIAL FRENUM

74
Extends from the labial frenum to the buccal frenum on each side.
Potiential space bounded by - mucolabial fold - orbicularis oris - labial aspect of residual alveolar ridgeMentalis – quite active in this region.
LABIAL VESTIBULE

75
CLINICAL SIGNIFICANCEExtent of denture is limited because of
muscle inserted close to the ridge .Muscles of lip actively pull across the
denture.(on opening mouth wide orbicularis muscle is stretched-> narrowing the sulcus -> displacing denture )
Impression are narrower in this region.Tone of the skin of lip and orbicularis
depends on the thickness & position of the flange.
HISTOLOGY -Epithelium is thin and non-keratinized - Submucosa – formed by loosely
arranged connective tissue fibre mixed with elastic and muscle fibre.

76
It overlies the depressor anguli oris muscle
Clinical significance - Clearance must be achieved in the denture to
avoid dislodgement of the denture
BUCCAL FRENUM

77
LINGUAL FRENUMAccomodated within
sublingual cresent area .
Vary in width and height.
Overlies the genioglossus muscle which takes origin from mental spine
Fold of mucous membrane from tongue to the residual ridge is sublingual fold.

78
It extends posteriorly form buccal frenum to the retromolar pad .
Houses the buccal flangeClinical significance - Impression is wide in this region- It is nearly 90 degree to the biting forces ,
providing denture with greates surface for the resistance to the vertical occlusal forces.
BUCCAL VESTIBULE

79
Buccinator muscle in buccal vestibule The extent of the buccal flange is
highly influenced by the buccinator muscle, which extends from
- Modiolus (anteriorly) - Pterygomandibular raphe ( posteriorly )Clinical significance:-- Denture should completely cover the vestibule and buccal shelf- Action of buccinator muscle moulds the buccal flange.

80
External oblique ridge It is a ridge of dense bone
extending from jus above the mental foramen and distally , becoming continous with anterior border of the ramus
- Gives attachment to buccinator muscled fibres.
Clinical significance:-- Can be used as guide for extent of denture
laterally

81
It accomodates the masseter muscle in the distobuccal area of the denture
Magnitude of its force is exerting the molar region.
Clinical significance :-- Overextension – soreness of the tissue &
dislodgement of the denture
Masseter notch

82
It is recorded by masseter muscle contraction, its fibres runs ouside and behind the buccinator -> contraction of masseter ->pushes inward against the buccinator muscle -> producing bulge.
Movements – - downward pressure in 2nd premolar region
by dentist and forces exerted by the closing of the mouth.

83
Relief area Microscopically - Mucous membrane ->
keratinized layer - submucosa is attached to
the periosteum.- Covered by fibrous
connective tissue.- Bone -> cancellous and
without good cortical plate covering.
Clinical significance :-- Should be relieved during
impression making.
CREST OF ALVEOLAR RIDGE

84
Primary stress bearing area Consist of horizontal shelves 0f
bone so called buccal shelf (by sheldon winkler 2nd edition )
Bounded by :- - medially -> crest of residual alveolar ridge - anteriorly -> buccal frenum - laterally -> external oblique ridge - distally -> retromolar pad
BUCCAL SHELF AREA

85
Wide and perpendicular to the vertical occlusal forces , so offers excellent resistance to such forces -> serving as primary stress bearing area.
Buccinator muscle fibres runs anteroposteriorly, paralleling the bone and denture doesnot resist the contracting forces of the muscle.

Microscopically - Mucous membrane -> loosely attached and
less keratinized than crest of residual ridge - Thicker submucosal layer - Fibres of buccinator are found running
horizontally in submucosa - Bone -> compact thus making it suitable as
primary stress bearing area - Buccinator fibres -> runs horizontally allows
denture to rest without damage to the muscle or dislodgement of denture
86

Irregular rough, bony crest extending from the 3rd molar region to the lower border of the mandible
Prominent -> 3rd molar the 2nd bicuspid.Levels of attachments of mylohyoid muscle :- - anteriorly-> close to the inferior border of mandible - posteriorly ->close to the alveolar crest
87
MYLOHYOID RIDGE

88
Clinical significance :-- Mucous membrance can be easily
traumatized by denture.- Area under ridge is undercut- Lingual flange of the mandible should
extend inferior but not lateral to the mylohoid line
Buccal
AttachmentsTo Hyoid
MylohyoidRidge

89
Irregular area of bony prominence at the distal termination of the mylohyoid line
Prominent -> acts as undercut
LINGUAL TUBEROSITY

90
It is located on the lateral surface of the mandible, between the 1st and 2nd bicuspid , halfway between the lower border and the alveolar crest.
Clinical significance :-- Extensive loss of alveolar ridge -> foramen occupies more superior position.- Should be relieved over the foramen- If not relieved -> can occlude the mental nerve and blood vessels -> causing numbness of the lip
MENTAL FORAMEN

91
Situated on the lingual aspect of the symphysis area slightly above the border.
Divided into :- - superior -> genioglossi attachment - inferior -> genohoid attachmentClinical significance:-- Extensive loss -> superior positioning of spine -> soreness -> surgical procedure indicated.
GENIAL TUBERCULE / MENTAL SPINE

92
Pear shaped pad Triangular soft pad of the tissue at the distal end
of the lower ridge.Microscopically - Composed of a thin nonkeratinized epithelium and
loose areolar tissue- Submucosa contains : > glandular tissue > fibres of buccinator and superior constrictor >pterygomandibular raphe > tendons of temporalis
RETROMOLAR PAD

93
Clinical significance :-- Usable guide on the cast for
the distal extension of denture - Action of the muscles in
retromolar pad , limits the extent of the denture -> So denture base should extend approximately ½ to 2/3rd over the retromolar pad. (zarb-bolender 12th edition )
- Should be covered by denture (sheldon winkler 2nd )
- Aids in the stability of the denture by adding another plane to resist movement of the denture.

94
Is a small pear shaped area of gingival tissue that remains fused to the scar after loss of the last molar.
This small , hard pale pear shaped tissue is situated at the base of the retromolar pad, approximately at the centre of the ridge.
RETROMOLAR PAPILLA

95
It can be divided into three areas
anterior vestibule/sublingual crescent area/
anterior sublingual fold
the middle vestibule/ mylohyoid area
the distolingual vestibule/ lateral throat form/
retromylohyoid fossa
LINGUAL VESTIBULE / ALVEOLINGUAL SULCUS

96
Anterior lingual vestibule
This extends from the lingual frenum to where
the mylohyoid ridge curves down below the level
of sulcus. Here a depression the premylohyoid
fossa can be palpated.
This is mainly influenced by the genioglossus
muscle, lingual frenum and some part by anterior
portion of sublingual glands .

97
Middle vestibule:
This is the largest area and is mainly influenced by mylohyoid muscles and somewhat by sublingual glands.
The mylohyoid muscle is the largest muscle in the floor of the mouth whose principal function occurs during swallowing. Its intra oral appearance is misleading because the membranous attachment makes the muscle appear to be horizontal when contracting.

98
Nagel and sears have shown that at maximum contraction the fibers are still in a downward and forward direction so that a denture can be extended below the muscle attachment along the mylohyioid ridge.
The lingual borders in the mylohyoid areas are formed by contact with the mylohyoid muscle in functional, but not extreme, contracted or elevated positions.
The average mylohyoid border is 4-6 mm beyond the mylohyoid ridge in fair to good ridge it is about 2-3 mm . If the ridge is flat it is often advantageous to make mylohyoid border thicker (4-5mm or more).

99
Distolingual vestibule:
The lateral throat form is bounded anteriorly by mylohyoid muscle, laterally by pear shaped pad, posterolaterally by superior constrictor, posteromedially by palatoglossus and medially by tongue.
The so called “s” curve of the lingual flange of the mandibular denture results from stronger intrinsic and extrinsic tongue muscles, which usually place the retromylohyoid borders more laterally and towards the retromylohyoid fossa, as the oppose weaker superior constrictor muscle.

100
The posterior limit of the mandibular denture is determined mainly by the palatoglossus muscle and somewhat by weaker superior constrictor muscle this is area is called posterior/ retromylohyoid curtain.
Neil described this area and noted that the denture
could have three possible lengths, depending on the
tonicity, activity, and anatomic attachments of the
adjacent structures-
Class III lateral throat form has minimum length
and thickness. The border usually ends 2-3 mm below
the mylohyoid ridge or sometimes just at the ridge.
LATERAL THROAT FORM

101
Class I throat form: The horizontal border is usually 2-3 mm thick, but a thicker border of 4-5 mm should be used for better seal if the ridge is flat. The retromylohyoid curtain area should be thinner, about 2-3 mm, and very rounded and smooth.
Class II throat form is about half as long and narrow as class I and about twice as long as class III.

102
COMPARISION BETWEEN EDENTULOUS MAXILLA AND MANDIBLE
Maxilla-1.Has more
supporting areas2.Limiting structures
are less in number and have a less stronger influence over the denture border
Mandible-1.Has less
supporting area.2.Limiting
structures are more in number and have a stronger influence over the denture border

103
1. de Freitas V, Madeira MC, Toledo Filho JL, Chagas CF. Absence of the mental foramen in dry human mandibles. Acta Anat (Basel). 1979; 104(3): 353-355.
2. Dharmar S. Locating the mandibular canal in panoramic radiographs. Int J Oral Maxillofac Implants. 1997; 12: 113-117.
REFRENCES

104
3. Mbajiorgu EF, Mawera G, Asala SA, Zivanovic S. Position of the mental foramen in adult black Zimbabwean mandibles: a clinical anatomical study. Central African Journal of Medicine 1998; 44: 24-30.
4. Gershenson A, Nathan H, Luchansky E. Mental foramen and mental nerve: changes with age. Acta Anatomica 1986; 126: 21-8.5. Zografos J, Kolokoudias M, Papadakis E Dental
School, University of Athens, Greece. Hell Period Stomat Gnathopathoprosopike Cheir. 1990 Mar;5(1):17-20.

105
6. Sheller WR and wisewell OB. Lingual foramen on the mandible. Anat rac 1954; 119 387-390
7. Sheldon winkler 2nd edition OF ESSENTIALSOF COMPLETE DENTURE PROSTHESIS
8. Charles m. heartwell, Jr, urthur O. Rahn . Syllabus of complete denture 4th edition
9. Grays anatomy 39th edition10. Zarb and Bolender 12th edition .
Prosthodontic treatment of edentulous patient