Targeted Therapies For Blood Cancers 2015 · Colorado Blood Cancer Institute . Targeted Therapy...
53
Immune and Targeted Therapies, Including CAR T Cells, for Blood Cancers Michael B. Maris, MD Director of Research Colorado Blood Cancer Institute
Transcript of Targeted Therapies For Blood Cancers 2015 · Colorado Blood Cancer Institute . Targeted Therapy...

Immune and Targeted Therapies Including CAR T Cells for Blood
Cancers
Michael B Maris MD Director of Research
Colorado Blood Cancer Institute
Targeted Therapy
bull Therapy that takes advantage of molecular and genetic information to cause tumor cell kill by blocking key malignant cell function or by enhancing immunologic function
bull Specific (against tumor cell)
bull Reduces global toxicity to patient
bull More tolerable
bull More effective
bull More expensive
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull ABL ndash Imatinib dasatinib nilotinib
bull FLT-3 ndash Sorafinib Midostaurin
bull BTK ndash Ibrutinib
bull PI3K ndash Idelsilib IPI-145
ndash Small Molecules
bull BCL-2 inhibitor - ABT 199
bull Inhibition of transcription ndash BET inhibitor
Targeted Therapy
2 ImmunologicImmunotoxins Therapies
- Antibody
- CD 20 ndash rituxamab obinotuzamab
- CD 30 ndash brentuximab
- CD 33 ndash SGN CD33a
- Bifunctional
bull CD 19CD3 ndash Blinotumamab
Targeted Therapy
2 Cellular Therapies
- Chimeric Antigen Receptor (CAR) T Cells
- CD 19 ndash KiteJunoNovartis
- CD 20 ndash
- CD 33 ndash
- CD 138
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
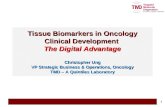
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
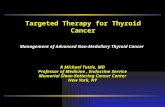
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy
bull Therapy that takes advantage of molecular and genetic information to cause tumor cell kill by blocking key malignant cell function or by enhancing immunologic function
bull Specific (against tumor cell)
bull Reduces global toxicity to patient
bull More tolerable
bull More effective
bull More expensive
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull ABL ndash Imatinib dasatinib nilotinib
bull FLT-3 ndash Sorafinib Midostaurin
bull BTK ndash Ibrutinib
bull PI3K ndash Idelsilib IPI-145
ndash Small Molecules
bull BCL-2 inhibitor - ABT 199
bull Inhibition of transcription ndash BET inhibitor
Targeted Therapy
2 ImmunologicImmunotoxins Therapies
- Antibody
- CD 20 ndash rituxamab obinotuzamab
- CD 30 ndash brentuximab
- CD 33 ndash SGN CD33a
- Bifunctional
bull CD 19CD3 ndash Blinotumamab
Targeted Therapy
2 Cellular Therapies
- Chimeric Antigen Receptor (CAR) T Cells
- CD 19 ndash KiteJunoNovartis
- CD 20 ndash
- CD 33 ndash
- CD 138
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull ABL ndash Imatinib dasatinib nilotinib
bull FLT-3 ndash Sorafinib Midostaurin
bull BTK ndash Ibrutinib
bull PI3K ndash Idelsilib IPI-145
ndash Small Molecules
bull BCL-2 inhibitor - ABT 199
bull Inhibition of transcription ndash BET inhibitor
Targeted Therapy
2 ImmunologicImmunotoxins Therapies
- Antibody
- CD 20 ndash rituxamab obinotuzamab
- CD 30 ndash brentuximab
- CD 33 ndash SGN CD33a
- Bifunctional
bull CD 19CD3 ndash Blinotumamab
Targeted Therapy
2 Cellular Therapies
- Chimeric Antigen Receptor (CAR) T Cells
- CD 19 ndash KiteJunoNovartis
- CD 20 ndash
- CD 33 ndash
- CD 138
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy
2 ImmunologicImmunotoxins Therapies
- Antibody
- CD 20 ndash rituxamab obinotuzamab
- CD 30 ndash brentuximab
- CD 33 ndash SGN CD33a
- Bifunctional
bull CD 19CD3 ndash Blinotumamab
Targeted Therapy
2 Cellular Therapies
- Chimeric Antigen Receptor (CAR) T Cells
- CD 19 ndash KiteJunoNovartis
- CD 20 ndash
- CD 33 ndash
- CD 138
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy
2 Cellular Therapies
- Chimeric Antigen Receptor (CAR) T Cells
- CD 19 ndash KiteJunoNovartis
- CD 20 ndash
- CD 33 ndash
- CD 138
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Phase I Study ABT-199 in CLL
Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Phase I Study ABT-199 in CLL
Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy
1 Drug therapy
ndash Tyrosine Kinase Inhibitors
bull PI3K ndashIPI-145
25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

25
Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Lymph Node Reduction in iNHL Patients with CT Scans
26
Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Progression-Free Survival (PFS)
27
Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Overall Survival (OS)
28
bull Median OS not reached
ndash 89 survival at 24 months (25 mg BID)
AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

AE 25 mg BID
n=19 All Doses
N=36
ALTAST increase 2 (11) 4 (11)
Pneumonia
(combined)
1 (5) 2 (6)
Rash (combined) 1 (5) 2 (6)
Febrile
neutropenia
0 1 (3)
Neutropenia 0 1 (3)
Diarrhea 1 (5) 1 (3)
Stomatitis 1 (5) 1 (3)
Herpes zoster
(disseminated)
0 1 (3)
SAE 25 mg BID
n=19 All Doses
N=36
Pneumonia
(combined)
4 (21) 9 (25)
Pyrexia 1 (5) 5 (14)
Febrile
neutropenia
1 (5) 3 (8)
Diarrhea 1 (5) 3 (8)
Nausea 1 (5) 2 (6)
Influenza 1 (5) 2 (6)
29
IPI 145 Toxicity
Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy (AML)
1 Immunconjugate
ndash SGN CD33a
Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy (ALL)
1 Bifunctional Immunconjugate
ndash Blinatumamab
Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Blinatumamab Engages Malignant Cells with Endogenous T cells
copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

copy2014 by American Society of Clinical Oncology
Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Targeted Therapy (ALL and NHL)
1 CAR T cells
ndash anti CD19
Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Why Consider CAR T Cell therapy
bull Remarkable responses demonstrated in refractory B
cell malignances
bull Potential ability to target other malignancies with
suitable antigenic targets
bull Specialized activity need for cell processing and BMT
like capabilities to perform this therapy
bull Could replace the use of BMT for some indications
bull Patients will seek heme malignancy programs that can
offer this therapy
RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

RIC Principle
Shift burden of tumor cell kill
from cytotoxic
Chemoradiotherapy
to
Donor T cells
Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Graft vs Tumor Effect
Thomas et al N Engl J Med 1981
copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

copy2014 by American Society of Hematology
CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

CAR T cells
bull Key element is production of T cells transfected with a
fusion protein with two main components
ndash Antigen recognition domain eg CD19
ndash T cell activation domaincostimulatory domains eg
CD28 costimulatory domain and T-cell receptor (TCR)
ndash T cell activation domains
bull Achieved through transduction into autologous T cells of
vectors with coding DNA
copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

copy2011 by American Society of Hematology
Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Kochenderfer JN et JCO AUGUST 2014
15 patients with advanced B-cell malignancies
9 diffuse large B-cell lymphoma (DLBCL)
2 indolent lymphomas
4 chronic lymphocytic leukemia
bull Patients received cyclophosphamide and fludarabine followed by a single
infusion of anti-CD19 CAR T cells
RESULTS
bull eight achieved complete remissions (CRs)
bull four achieved partial remissions one had stable lymphoma and
bull two were not evaluable for response
bull CRs were obtained by four of seven evaluable patients with
chemotherapy-refractory DLBCL
three of these four CRs with durations ranging from 9 to 22 months
Acute toxicities
bull fever hypotension delirium and other neurologic toxicities toxicities resolved
within 3 weeks after cell infusion
bull One patient died suddenly as a result of an unknown cause 16 days after cell
infusion
CAR T cells in NHL
9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

9 months
Kochenderfer et al J Clin Oncol 2014 Aug 25
CAR T in NHL
James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

James N Kochenderfer et al JCO 201533540-549
Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Results in ALL
Maude et al N Engl J Med 2014 3711507-1517October 16 2014
bull Autologous T cells transduced with a CD19-directed chimeric antigen
receptor (CTL019) lentiviral vector in patients with relapsed or refractory
ALL
bull Doses of 076times106 to 206times106 CTL019 cells per kilogram
Results
bull 30 children and adults received CTL019
bull Complete remission in 27 patients (90) 15 after prior stem-cell
transplantation
bull CTL019 cells proliferated in vivo and were detectable in the blood bone
marrow and cerebrospinal fluid
bull 6-month event-free survival rate of 67 and overall survival rate of 78
bull At 6 months the probability of persistence of CTL019 was 68 (95 CI
50 to 92)
bull Probability of relapse-free B-cell aplasia was 73 (95 CI 57 to 94)
RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

RESULTS IN ALL
Cytokine-release syndrome
N Engl J Med 2014 3711507-1517October 16 2014
bull All the patients had the cytokine-release syndrome
bull Severe cytokine-release syndrome which developed in 27
of the patients
- was associated with a higher disease burden before infusion
bull Effectively treated with the antindashinterleukin-6 receptor
antibody tocilizumab
bull 30 treated in ICU
bull Not directly correlated with neurological toxicity
Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Toxicities of CAR T therapy bull Fever
bull Hypotension
bull Pulmonary leak
bull Coagulopathy
bull Cytopenias
bull Renal changes
bull Neurological
bull B cell aplasia with hypogammablobulinemia
bull Tumor lysis syndrome
Cytokine Release Syndrome
Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive

Conclusion
bull Targeted therapy takes advantage of molecular and genetic information to cause tumor cell kill
bull There is an explosion of novel therapies that may help change the natural history of many aggressive blood cancers
bull Therapies include
1 Small molecules (TKI anti BCL2 BCR inhibitorshellip)
2 Immunconjugates bifunctional agent
3 CAR T cells
bull Agents have unique toxicities
bull Are likely to be very expensive