Slide 1 Maintenance Therapy Genentech Targeted Agents...
12
Slide 1 Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Targeted Agents as Maintenance Therapy ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 2 Disclosures • Genentech – Advisory Board ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 3 Maintenance Therapy Drug Therapy Defined Treatment Non-Progressing Patients Until progression Continuation or Switch Molecularly Targeted Agents Are Ideal Candidates • Majority have an oral route of administration • Modest to low toxicity profile with potential for long term administration ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________
Transcript of Slide 1 Maintenance Therapy Genentech Targeted Agents...
Slide 1
Karen Kelly, MDProfessor of Medicine
UC Davis Cancer Center
Targeted Agents as Maintenance Therapy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 2
Disclosures
• Genentech – Advisory Board
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 3 Maintenance Therapy
Drug TherapyDefined TreatmentNon-Progressing
PatientsUntil progression
Continuation
or
Switch
Molecularly Targeted Agents Are Ideal Candidates
• Majority have an oral route of administration
• Modest to low toxicity profile with potential for long term administration
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
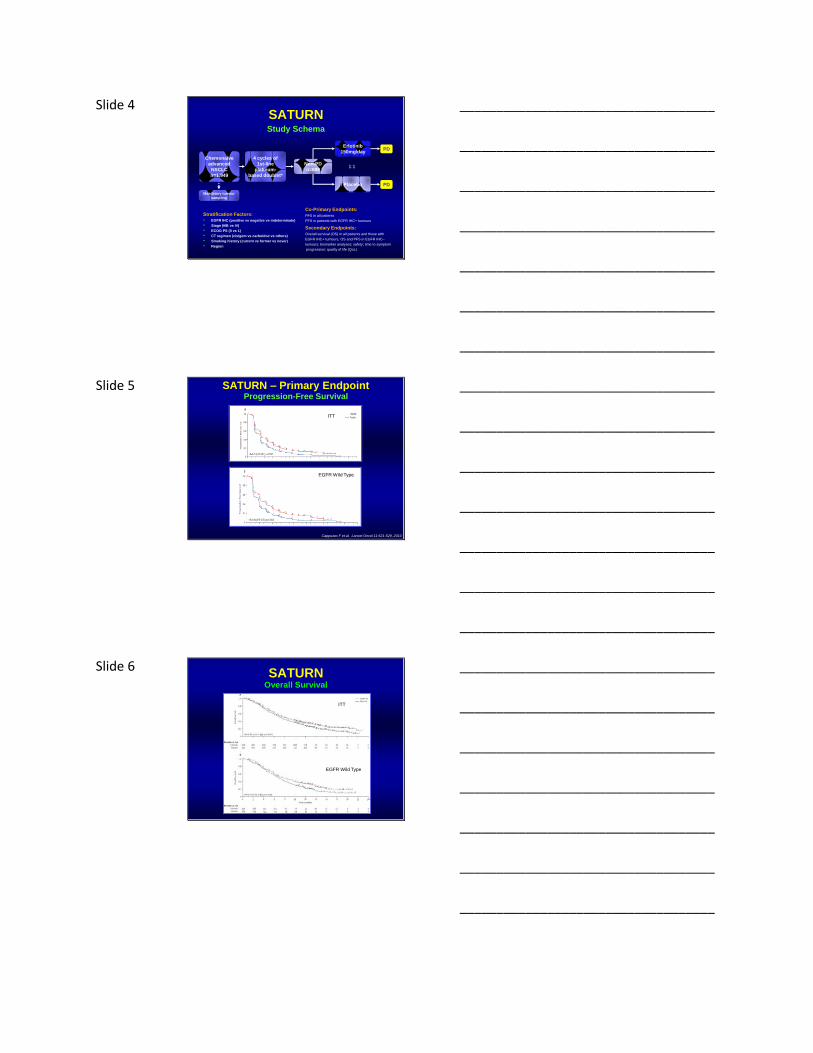
Slide 4
Stratification Factors:
• EGFR IHC (positive vs negative vs indeterminate)
• Stage (IIIB vs IV)
• ECOG PS (0 vs 1)
• CT regimen (cis/gem vs carbo/doc vs others)
• Smoking history (current vs former vs never)
• Region
1:1
Chemonaïve
advanced
NSCLC
n=1,949
Non-PD
n=889
4 cycles of
1st-line
platinum-
based doublet*
Placebo PD
Erlotinib
150mg/dayPD
Mandatory tumour
sampling
Co-Primary Endpoints:
PFS in all patients
PFS in patients with EGFR IHC+ tumours
Secondary Endpoints:
Overall survival (OS) in all patients and those with
EGFR IHC+ tumours, OS and PFS in EGFR IHC–
tumours; biomarker analyses; safety; time to symptom
progression; quality of life (QoL)
SATURNStudy Schema
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 5
ITT
EGFR Wild Type
Cappuzzo F et al. Lancet Oncol 11:521-529, 2010
SATURN – Primary EndpointProgression-Free Survival
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 6 SATURN
Overall Survival
ITT
EGFR Wild Type
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
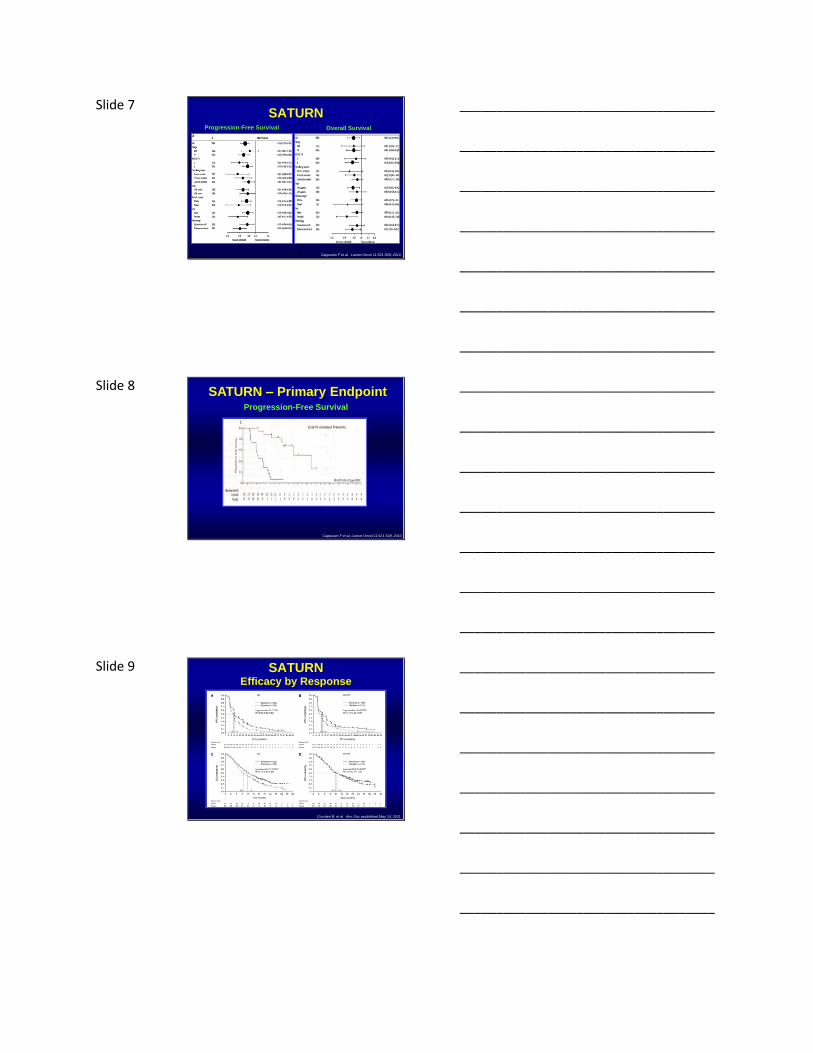
Slide 7 SATURN
Progression-Free Survival
Cappuzzo F et al. Lancet Oncol 11:521-529, 2010
Overall Survival
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 8 SATURN – Primary Endpoint
Cappuzzo F et al. Lancet Oncol 11:521-529, 2010
EGFR mutated Patients
Progression-Free Survival
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 9 SATURNEfficacy by Response
Courdert B, et al. Ann Onc epublished May 24, 2011
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 10 SATURN Efficacy in Patients with Stable Disease
Overall Survival
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 11 SATURNEfficacy in Patients with Stable Disease
Courdert B, et al. Ann Onc epublished May 24, 2011
EGFR Wild Type
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12 INFORM: Study Design
Gefitinib(250 mg/day)
Placebo(once daily)
1:1 randomization
Patients
Age ≥18 years
Completed 4 cycles of first-line platinum-based chemotherapy without PD or unacceptable toxicity
Life expectancy≥12 weeks
WHO PS 0-2
Measurable Stage IIIB/IV disease
Endpoints
Primary
Progression-free survival (PFS)
Secondary
Objective response rate (ORR)
Disease control rate (DCR)
Overall survival (OS)
Quality of life
Safety and tolerability
Exploratory
Biomarkers
EGFR mutation
Zhang L, et al. J Clin Oncol 29:478s, 2011
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
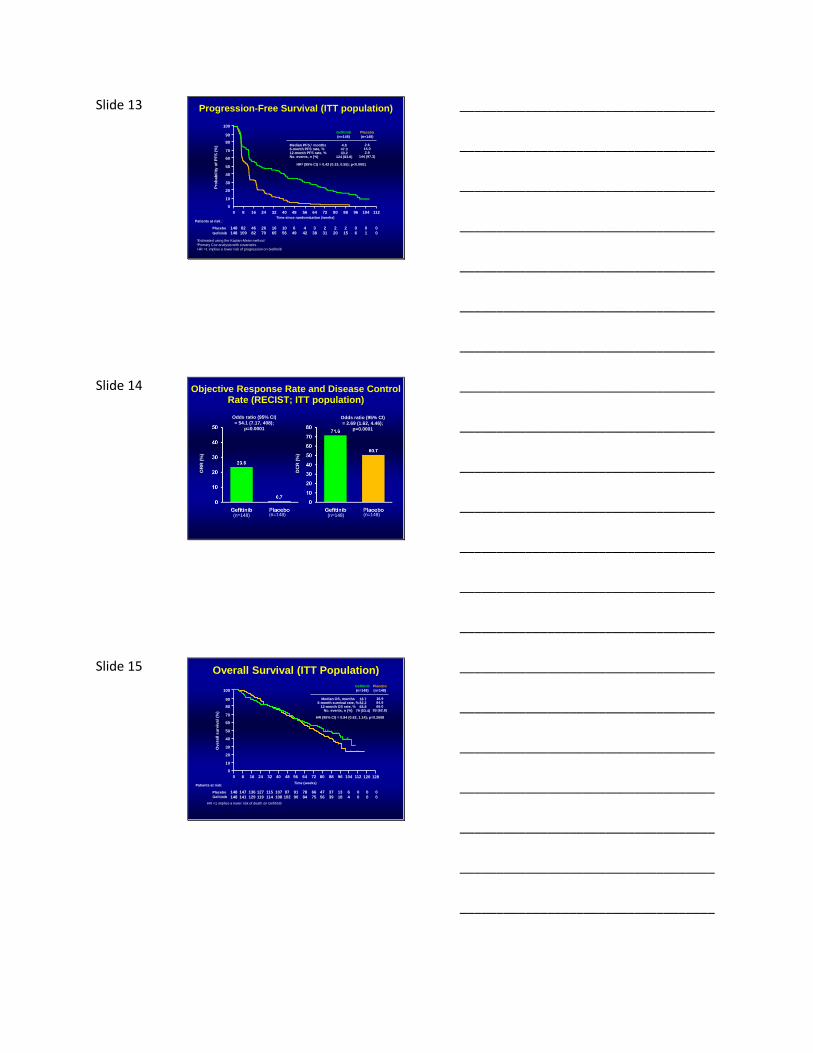
Slide 13 Progression-Free Survival (ITT population)
HR‡ (95% CI) = 0.42 (0.33, 0.55); p<0.0001
Gefitinib
(n=148)
Placebo
(n=148)
Median PFS,† months6-month PFS rate, %12-month PFS rate, %No. events, n (%)
4.847.333.2
124 (83.8)
2.615.02.9
144 (97.3)
0 16 40 56 72 96 112
0
10
40
60
80
100
Pro
bab
ilit
y o
f P
FS
(%
)
20
30
50
70
90
8 24 32 48 64 80 88 104
Time since randomization (weeks)
†Estimated using the Kaplan-Meier method‡Primary Cox analysis with covariates
HR <1 implies a lower risk of progression on Gefitinib
Gefitinib
Placebo
Patients at risk :
148 46 10 4 2 0 082 26 16 6 3 2 2 0
148 82 56 42 31 6 0109 70 65 49 38 20 15 1
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
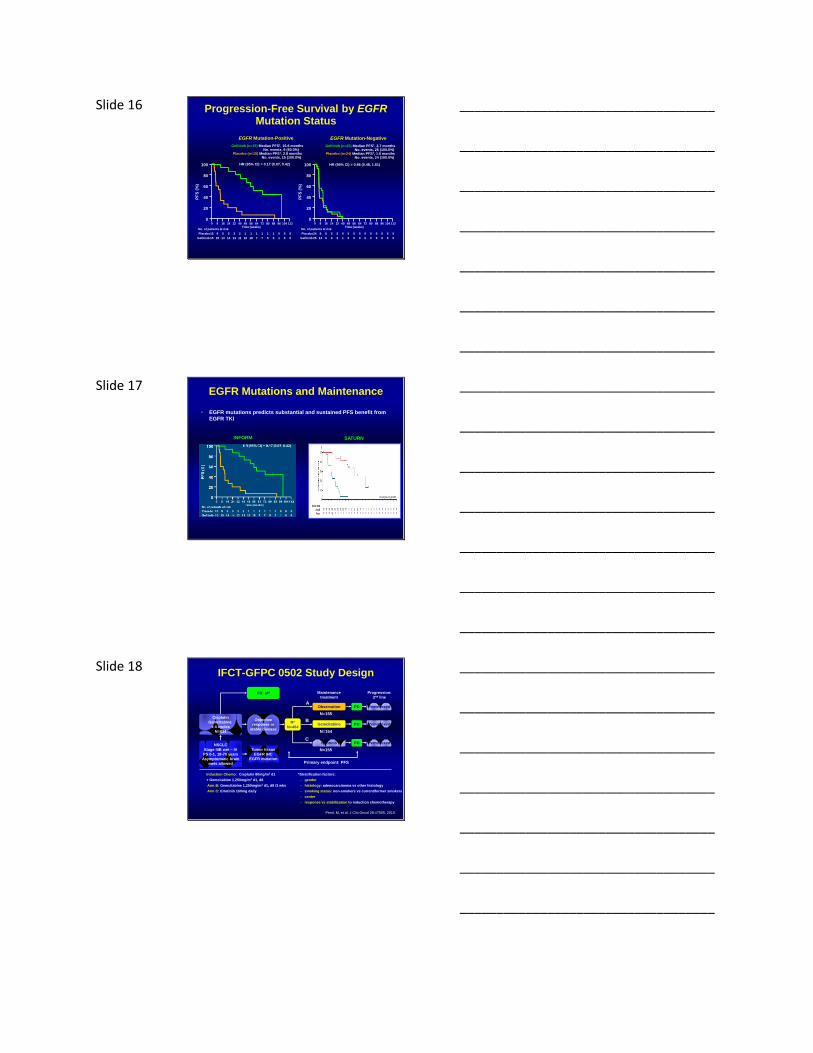
Slide 14 Objective Response Rate and Disease Control Rate (RECIST; ITT population)
OR
R (
%)
(n=148) (n=148)
Odds ratio (95% CI)
= 54.1 (7.17, 408);
p=0.0001
(n=148) (n=148)
DC
R (
%)
Odds ratio (95% CI)
= 2.69 (1.62, 4.46);
p=0.0001
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
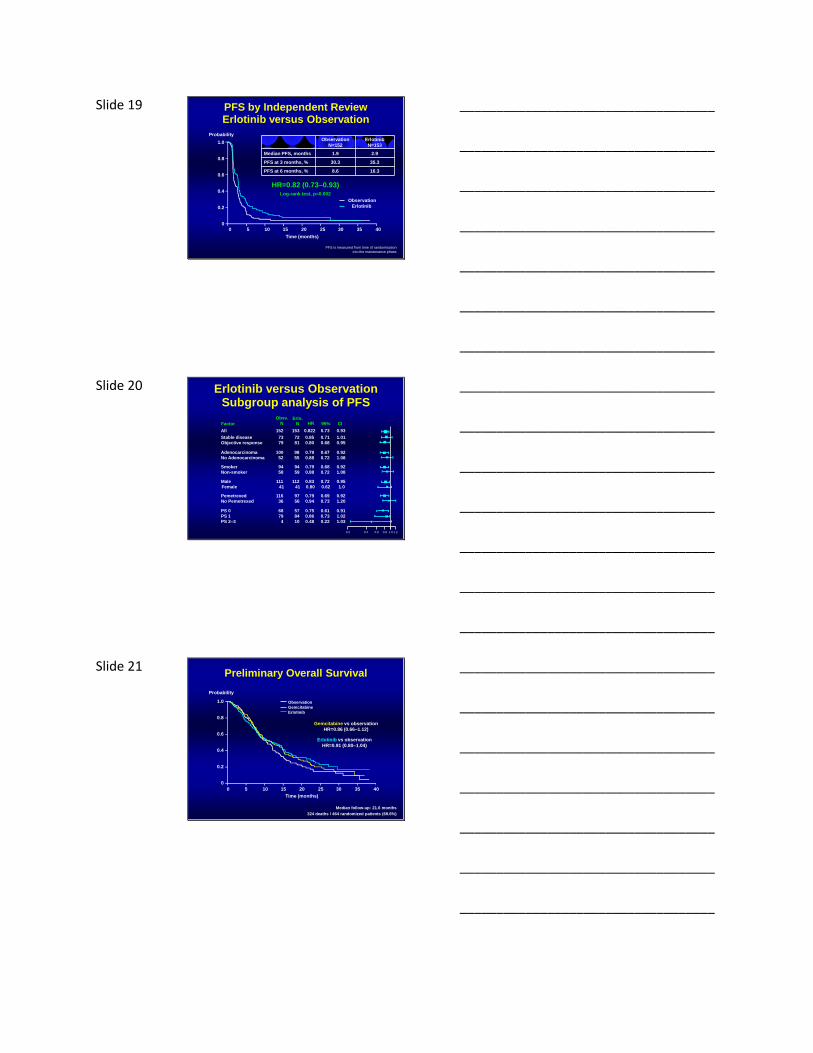
Slide 15 Overall Survival (ITT Population)
0 16 40 56 72 96 112
0
10
40
60
80
100
Overa
ll s
urv
ival
(%)
20
30
50
70
90
8 24 32 48 64 80 88 104 120 128
Time (weeks)
Placebo
Patients at risk:
148 136 97 78 37 0 0147 115 107 91 66 13 6 0
148 129 102 84 39 0 0141 114 108 90 75 18 4 0
47
56
127
119Gefitinib
HR (95% CI) = 0.84 (0.62, 1.14); p=0.2608
Gefitinib
(n=148)
Placebo
(n=148)
Median OS, months6-month survival rate, %
12-month OS rate, %No. events, n (%)
18.782.268.8
79 (53.4)
16.984.966.0
93 (62.8)
HR <1 implies a lower risk of death on Gefitinib
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
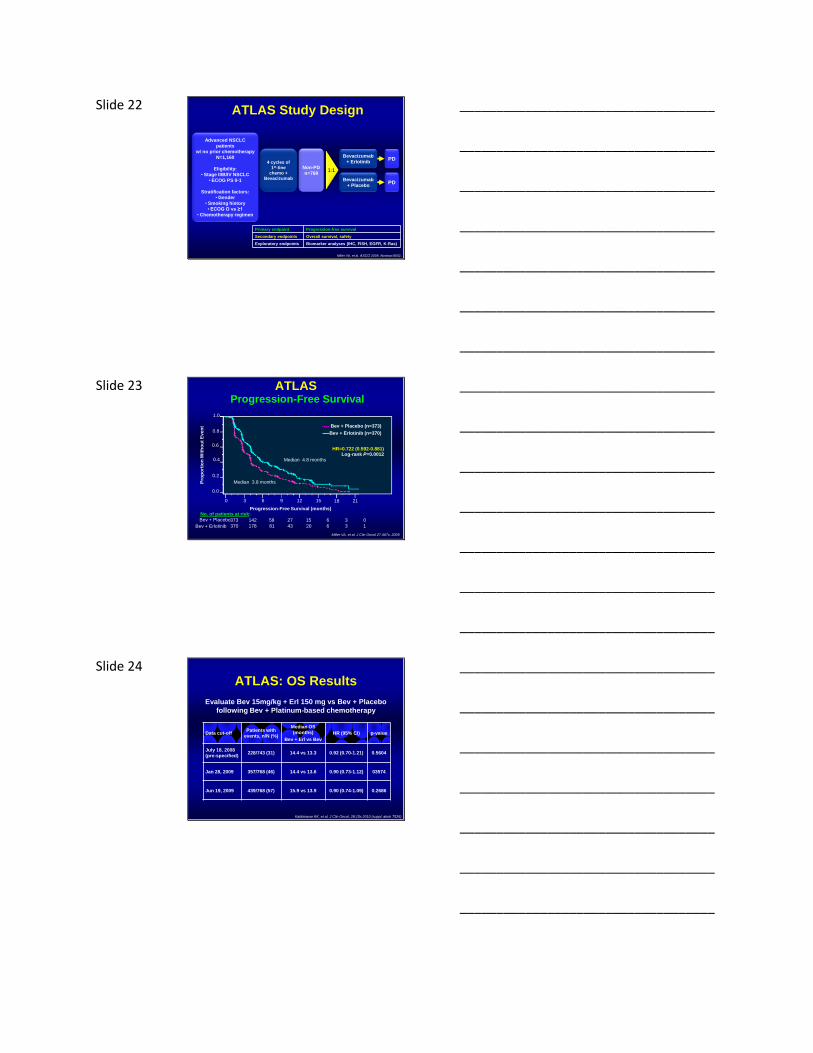
Slide 16
HR (95% CI) = 0.17 (0.07, 0.42)
Gefitinib (n=15) Median PFS†, 16.6 monthsNo. events, 9 (60.0%)
Placebo (n=15) Median PFS†, 2.8 monthsNo. events, 15 (100.0%)
EGFR Mutation-Positive
HR (95% CI) = 0.86 (0.48, 1.51)
Gefitinib (n=25) Median PFS†, 2.7 monthsNo. events, 25 (100.0%)
Placebo (n=24) Median PFS†, 1.5 monthsNo. events, 24 (100.0%)
EGFR Mutation-Negative
0
20
40
60
80
100
0 8 16 24 32 40 48 56 64 72 80 88 96 104 112
PF
S (
%)
Time (weeks)
15 9 5 3 3 2 1 1 1 1 1 1 0 0 0
15 15 14 14 13 11 10 18 7 7 5 3 1 0 0
Placebo
Gefitinib
No. of patients at risk
0
20
40
60
80
100
0 8 16 24 32 40 48 56 64 72 80 88 96 104 112
PF
S (
%)
Time (weeks)
24 9 5 3 2 0 0 0 0 0 0 0 0 0 0
25 14 6 3 3 1 0 0 0 0 0 0 0 0 0
Placebo
Gefitinib
No. of patients at risk
Progression-Free Survival by EGFRMutation Status
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 17 EGFR Mutations and Maintenance
• EGFR mutations predicts substantial and sustained PFS benefit from
EGFR TKI
INFORM SATURN
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 18 IFCT-GFPC 0502 Study Design
Observation
Progression:
2nd line
Primary endpoint: PFS
A
C
Maintenance
treatment
PD
N=155
N=154
N=155
PD: off
Objective
response or
stable disease
Cisplatin
Gemcitabine
x 4 cycles
N=834
NSCLC
Stage IIIB wet – IV
PS 0-1, 18-70 years
Asymptomatic brain
mets allowed
Tumor tissue
EGFR IHC
EGFR mutation
R*
N=464
BGemcitabine
Erlotinib
PD
PD
Pemetrexed
Pemetrexed
Pemetrexed
*Stratification factors:
– gender
– histology: adenocarcinoma vs other histology
– smoking status: non-smokers vs current/former smokers
– center
– response vs stabilization to induction chemotherapy
Induction Chemo: Cisplatin 80mg/m2 d1
+ Gemcitabine 1,250mg/m2 d1, d8
Arm B: Gemcitabine 1,250mg/m2 d1, d8 /3 wks
Arm C: Erlotinib 150mg daily
Perol, M, et al. J Clin Oncol 28:#7505, 2010
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 19
PFS is measured from time of randomisation
into the maintenance phase
Observation
Erlotinib
HR=0.82 (0.73–0.93)Log-rank test, p=0.002
Observation
N=152
Erlotinib
N=153
Median PFS, months 1.9 2.9
PFS at 3 months, % 30.3 35.3
PFS at 6 months, % 8.6 16.3
1.0
0.8
0.6
0.4
0.2
00 5 10 15 20 25 30 35 40
Time (months)
Probability
PFS by Independent ReviewErlotinib versus Observation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 20
0.2 0.4 0.6 0.8 1.0 1.2
Factor
Obsv.
NErlo.
N HR 95% CI
Stable disease 73 72 0.85 0.71 1.01
Objective response 79 81 0.80 0.68 0.95
Adenocarcinoma 100 98 0.79 0.67 0.92
No Adenocarcinoma 52 55 0.88 0.72 1.08
Smoker 94 94 0.79 0.68 0.92
Non-smoker 58 59 0.88 0.72 1.08
Male 111 112 0.83 0.72 0.95
Female 41 41 0.80 0.62 1.0
Pemetrexed 116 97 0.79 0.69 0.92
No Pemetrexed 36 56 0.94 0.73 1.20
PS 0 68 57 0.75 0.61 0.91
PS 1 79 84 0.86 0.73 1.02
PS 2–3 4 10 0.48 0.22 1.03
All 152 153 0.822 0.73 0.93
Erlotinib versus ObservationSubgroup analysis of PFS
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21 Preliminary Overall Survival
Observation
Gemcitabine
Erlotinib
Gemcitabine vs observation
HR=0.86 (0.66–1.12)
Erlotinib vs observation
HR=0.91 (0.80–1.04)
Median follow-up: 21.6 months
324 deaths / 464 randomized patients (69.6%)
1.0
0.8
0.6
0.4
0.2
0
0 5 10 15 20 25 30 35 40
Time (months)
Probability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 22
Bevacizumab
+ Erlotinib
Bevacizumab
+ Placebo
PD
PD
Advanced NSCLC
patients
w/ no prior chemotherapy
N=1,160
Eligibility:
• Stage IIIB/IV NSCLC
• ECOG PS 0-1
Stratification factors:
• Gender
• Smoking history
• ECOG O vs ≥1
• Chemotherapy regimen
Primary endpoint Progression-free survival
Secondary endpoints Overall survival, safety
Exploratory endpoints Biomarker analyses (IHC, FISH, EGFR, K-Ras)
1:1
4 cycles of
1st-line
chemo +
Bevacizumab
Non-PD
n=768
Miller VA, et al. ASCO 2009. Abstract 8002.
ATLAS Study Design
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 23
No. of patients at risk:
373 142 58 27 15 6 3 0Bev + Placebo
370 178 81 43 20 6 3 1Bev + Erlotinib
ATLASProgression-Free Survival
0 3 6 9 12 15 18 21
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n W
ith
ou
t E
ven
t
HR=0.722 (0.592-0.881)Log-rank P=0.0012
Progression-Free Survival (months)
Bev + Placebo (n=373)
Bev + Erlotinib (n=370)
Miller VA, et al. J Clin Oncol 27:407s, 2009
Median 4.8 months
Median 3.8 months
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 24 ATLAS: OS Results
Data cut-offPatients with
events, n/N (%)
Median OS
(months)
Bev + Erl vs Bev
HR (95% CI) p-value
July 18, 2008
(pre-specified)228/743 (31) 14.4 vs 13.3 0.92 (0.70-1.21) 0.5604
Jan 28, 2009 357/768 (46) 14.4 vs 13.6 0.90 (0.73-1.12) 03574
Jun 19, 2009 439/768 (57) 15.9 vs 13.9 0.90 (0.74-1.09) 0.2686
Evaluate Bev 15mg/kg + Erl 150 mg vs Bev + Placebo
following Bev + Platinum-based chemotherapy
Kabbinavar KK, et al, J Clin Oncol, 28:15s 2010 (suppl; abstr 7526)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 25 Erlotinib Maintenance
4 cycles of
Platinum-based
Chemotherapy
(EGFR wild type)
R
A
N
D
O
M
I
Z
E
R
E
G
I
S
T
E
R
Erlotinib
ErlotinibPlacebo
NPD
NPD
Primary endpoint: OS
N = 610
Starting 11/11
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 26 The Role of Maintenance Therapy SWOG 0023
CDDP 50 mg/2
d 1,8,29,36
VP-16 50 mg/m2
d1-5, 29-33
XRT 1.8- 2 Gy/d
61 Gy
DOCETAXEL
75 mg/m2
x 3 cycles
1o Endpoint: Overall Survival;
20 Endpoint: PFS, toxicity and correlative scienceMaintenance therapy could continue for a maximum of 5 years
Stratification factors: IIIA vs IIIB; Measurable vs Non-measurable disease;
squamous vs nonsquamous
PLACEBO
GEFITINIB
500 mg/day
250 mg/day
(5-1-03)
Definitive TX Consolidation Maintenance
R
A
N
D
O
M
I
Z
E
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27 SWOG 0023: Overall Survival
From Randomization
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60
Months After RANDOMIZATION
Gefitinb
Placebo
N
118
125
Events
71
54
Median
in Months
23
35
P = .01
1 YR
OS
2 YR
OS
73% 46%
59%81%
Median FU time: 27 months
Kelly, K et al. J Clin Oncol. 26:2450-2460, 2008
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
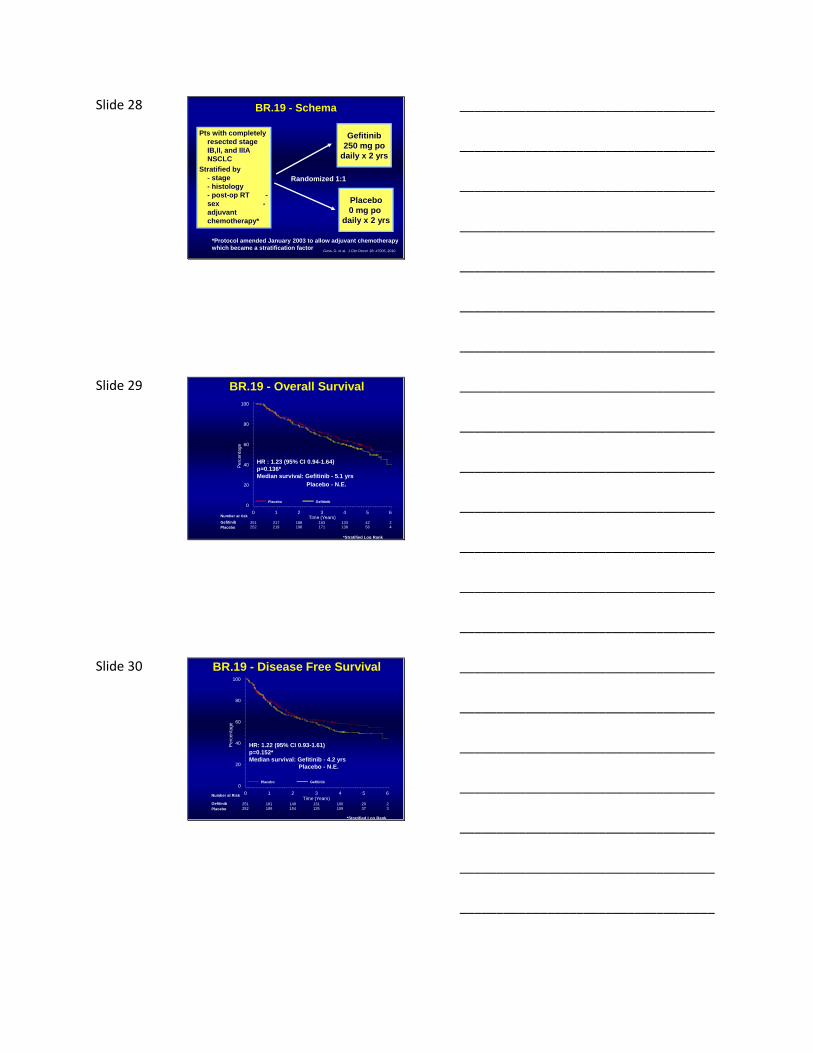
Slide 28 BR.19 - Schema
Pts with completely
resected stage
IB,II, and IIIA
NSCLC
Stratified by
- stage
- histology
- post-op RT -
sex -
adjuvant
chemotherapy*
Gefitinib
250 mg po
daily x 2 yrs
Placebo
0 mg po
daily x 2 yrs
Randomized 1:1
*Protocol amended January 2003 to allow adjuvant chemotherapy
which became a stratification factorGoss, G. et al. J Clin Oncol 28: #7005, 2010
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
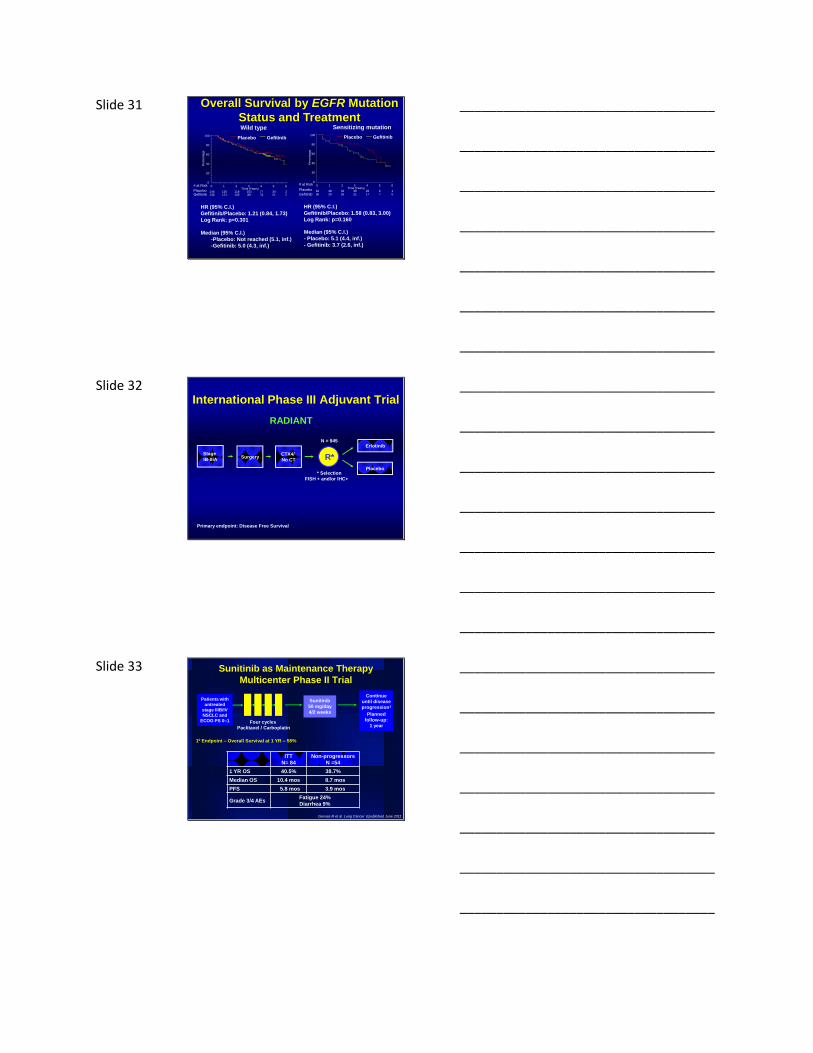
Slide 29 BR.19 - Overall Survival
Number at risk
Gefitinib
Placebo
HR : 1.23 (95% CI 0.94-1.64)
p=0.136*
Median survival: Gefitinib - 5.1 yrs
Placebo - N.E.
Placebo Gefitinib
Perc
enta
ge
0
20
40
60
80
100
0
251252
1
217219
2
188198
3Time (Years)
163171
4
133138
5
4256
6
24
*Stratified Log Rank
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
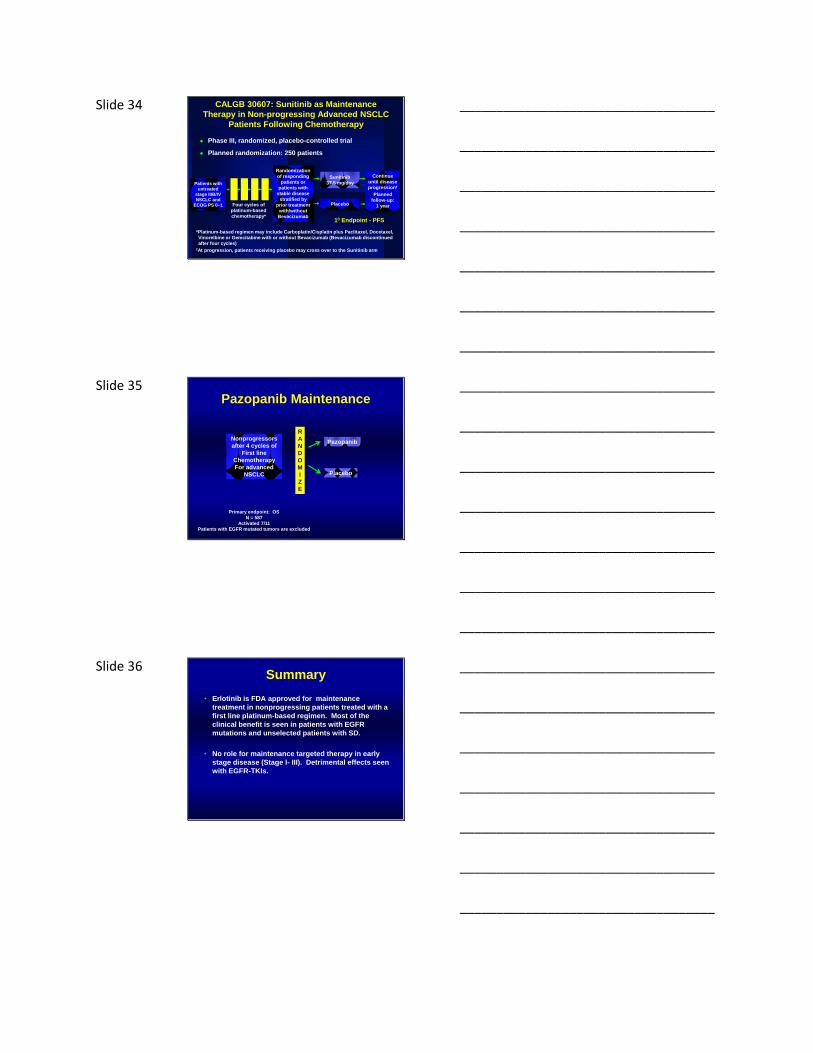
Slide 30 BR.19 - Disease Free Survival
Number at Risk
Gefitinib
Placebo
Placebo Gefitinib
Perc
enta
ge
0
20
40
60
80
100
0
251
252
1
181
189
2
149
154
3Time (Years)
131
135
4
100
109
5
29
37
6
2
3
HR: 1.22 (95% CI 0.93-1.61)
p=0.152*
Median survival: Gefitinib - 4.2 yrs
Placebo - N.E.
*Stratified Log Rank
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 31 Overall Survival by EGFR Mutation
Status and Treatment
# at Risk
PlaceboGefitinib
Wild type
Placebo Gefitinib
Perc
enta
ge
0
20
40
60
80
100
0
145136
1
126121
2
118105
3Time (Years)
10189
4
7774
5
3421
6
22
# at Risk
Placebo
Gefitinib
Sensitizing mutation
Placebo Gefitinib
Perc
enta
ge
0
20
40
60
80
100
0
4036
1
3829
2
3226
3Time (Years)
3021
4
2617
5
67
6
10
HR (95% C.I.)
Gefitinib/Placebo: 1.21 (0.84, 1.73)
Log Rank: p=0.301
Median (95% C.I.)
-Placebo: Not reached (5.1, inf.)
-Gefitinib: 5.0 (4.3, inf.)
HR (95% C.I.)
Gefitinib/Placebo: 1.58 (0.83, 3.00)
Log Rank: p=0.160
Median (95% C.I.)
- Placebo: 5.1 (4.4, inf.)
- Gefitinib: 3.7 (2.6, inf.)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 32
Stage
IB-IIIASurgery
CTX4/
No CT
Erlotinib
Placebo
R*
* Selection
FISH + and/or IHC+
RADIANT
International Phase III Adjuvant Trial
Primary endpoint: Disease Free Survival
N = 945
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 33 Sunitinib as Maintenance Therapy
Multicenter Phase II Trial
Continue
until disease
progression†
Planned
follow-up:
1 year
Sunitinib
50 mg/day
4/2 weeks
Patients with
untreated
stage IIIB/IV
NSCLC and
ECOG PS 0–1 Four cycles
Paclitaxel / Carboplatin
10 Endpoint – Overall Survival at 1 YR – 55%
ITT
N= 84
Non-progressors
N =54
1 YR OS 40.5% 38.7%
Median OS 10.4 mos 8.7 mos
PFS 5.8 mos 3.9 mos
Grade 3/4 AEsFatigue 24%
Diarrhea 9%
Gervais R et al. Lung Cancer Epublished June 2011
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 34 CALGB 30607: Sunitinib as Maintenance
Therapy in Non-progressing Advanced NSCLC
Patients Following Chemotherapy
Phase III, randomized, placebo-controlled trial
Planned randomization: 250 patients
Continue
until disease
progression†
Planned
follow-up:
1 year
Sunitinib
37.5 mg/day
Placebo
Randomization
of responding
patients or
patients with
stable disease
stratified by
prior treatment
with/without
Bevacizumab
Patients with
untreated
stage IIIB/IV
NSCLC and
ECOG PS 0–1 Four cycles of
platinum-based
chemotherapy*
*Platinum-based regimen may include Carboplatin/Cisplatin plus Paclitaxel, Docetaxel,
Vinorelbine or Gemcitabine with or without Bevacizumab (Bevacizumab discontinued
after four cycles)†At progression, patients receiving placebo may cross over to the Sunitinib arm
10 Endpoint - PFS
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 35 Pazopanib Maintenance
Nonprogressors
after 4 cycles of
First line
Chemotherapy
For advanced
NSCLC
R
A
N
D
O
M
I
Z
E
Pazopanib
Placebo
Primary endpoint: OS
N = 587
Activated 7/11
Patients with EGFR mutated tumors are excluded
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 36 Summary
• Erlotinib is FDA approved for maintenance
treatment in nonprogressing patients treated with a
first line platinum-based regimen. Most of the
clinical benefit is seen in patients with EGFR
mutations and unselected patients with SD.
• No role for maintenance targeted therapy in early
stage disease (Stage I- III). Detrimental effects seen
with EGFR-TKIs.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________