Targeted Therapy News May 2013
36
Targeted Feature Researchers Identify How Nongenetic Mechanisms of Cancer Cell Diversity Can Affect Treatment Response By Anna Azvolinsky, PhD A new study suggests that even tumor cells with a common genetic back- ground can display functional heterogeneity. The results point to nonge- netic mechanisms, such as microenvironment and epigenetic differences, that contribute to tumor growth as well as tolerance to therapy. The research, led by Antonija Kreso, PhD, Catherine O’Brien, MD, and John Dick, PhD, of the Princess Margaret Cancer Centre and the University of Toronto, Canada, was published in the February 2013 issue of Science. “Genetic mutations are thought to account for tumor formation and growth, but our results indicate intra-clonal diversity with respect to functional properties also plays a role,” said Kreso. The predominant theory of solid tumor heterogeneity states that tumor cell di- versity is a result of progressive mutational changes that form distinct tumor cell clones, with each type of subclone thought to be genetically similar. But how non- genetic factors contribute to tumor heterogeneity along with genetic diversity is not clear. Kreso and colleagues addressed whether these genetic clones are functionally equivalent and respond in the same manner to chemotherapy treatment by track- ing individually labeled human colorectal cancer (CRC) cells in mice. They found that individual tumor cells within the same lineage had a spectrum of survival (continued on page 17) (continued on page 17) BRCA Patenting Case Reaches the Supreme Court By Ben Leach T he question of the validity of gene patents has reached the Supreme Court, and the im- pending decision could transform the current research landscape. The company on the defensive end of the case is Utah-based Myriad Genetics, a molecular diagnos- tic company responsible for the development of the BRACAnalysis test. In 1994, it was discovered that the BRCA1 and BRCA2 genes were linked to an in- creased risk of breast cancer and ovarian cancer. As the patent holder, Myriad requires that all testing for the genes be done with the company’s test only. (see page 24) Personalized Medicine For the Practicing Oncology Professional Vol. 2 No. 3 An Interview with Douglas Yee, MD, Scientific Program Chair ASCO 2013: Key Targeted Trials Peter Meldrum I n September 2012, the FDA ap- proved regorafenib (Stivarga) as a salvage treatment for metastatic colorectal cancer (mCRC) previously treated with chemotherapy, an anti- vascular endothelial growth factor (VEGF) therapy, or an anti-epidermal growth factor receptor (EGFR) therapy. Regorafenib had received a fast-track FDA review status and was approved after only a three-month review pro- cess. The drug is the first targeted oral therapy to receive an FDA approval for treatment of advanced CRC, and the second drug to be approved for mCRC in 2012. Although progress has been made in treating colorectal cancer, in- cluding the development of biologic agents that target EGFR and angiogen- esis, the median survival in mCRC re- mains about two years. The five-year survival rate for a patient with stage II Feature New Developments in Oral Targeted Agents for Advanced Colorectal Cancer By Anna Azvolinsky, PhD (continued on page 18) Targeted Therapy News ™ In this issue... Prostate Cancer • Biomarkers Still Needed Ovarian Cancer • Possible Mechanism of Platinum Resistance in Ovarian Cancer Identified Genetic Research • Metabolic Gene Expression Altered in Cancer, Providing Potential Drug Targets Hematologic Malignancies • Numerous Drug Classes Studied for Use in Follicular and Other Lymphomas • Seeking a Standard in the Treat- ment of Elderly Patients With CLL AACR Meeting • Spotlight on Novel Agents in Early Development Breast Cancer • Trials Examine Use of T-DM1 as Combination Therapy for HER2 Breast Cancer • FDA Grants Breakthrough Therapy Designation for Palbociclib in Breast Cancer Lung Cancer • HER2-Targeted Agents May Benefit Patients With Non-Small Cell Lung Cancer Axel Grothey, MD
-
Upload
intellisphere-llc -
Category
Documents
-
view
217 -
download
5
description
Targeted Therapy News is aimed at helping oncologists meet these challenges by providing the information and analyses they need to best use targeted therapies in clinical practice.
Transcript of Targeted Therapy News May 2013

Targeted TherapyNews™
Feature
Researchers Identify How Nongenetic Mechanisms of Cancer Cell Diversity Can Affect Treatment ResponseBy Anna Azvolinsky, PhD
A new study suggests that even tumor cells with a common genetic back-ground can display functional heterogeneity. The results point to nonge-netic mechanisms, such as microenvironment and epigenetic differences,
that contribute to tumor growth as well as tolerance to therapy. The research, led by Antonija Kreso, PhD, Catherine O’Brien, MD, and John Dick, PhD, of the Princess Margaret Cancer Centre and the University of Toronto, Canada, was published in the February 2013 issue of Science.
“Genetic mutations are thought to account for tumor formation and growth, but our results indicate intra-clonal diversity with respect to functional properties also plays a role,” said Kreso.
The predominant theory of solid tumor heterogeneity states that tumor cell di-versity is a result of progressive mutational changes that form distinct tumor cell clones, with each type of subclone thought to be genetically similar. But how non-genetic factors contribute to tumor heterogeneity along with genetic diversity is not clear.
Kreso and colleagues addressed whether these genetic clones are functionally equivalent and respond in the same manner to chemotherapy treatment by track-ing individually labeled human colorectal cancer (CRC) cells in mice. They found that individual tumor cells within the same lineage had a spectrum of survival
(continued on page 17)
(continued on page 17)
BRCA Patenting Case Reaches the Supreme Court
By Ben Leach
The question of the validity of gene patents has reached the Supreme Court, and the im-pending decision could transform the current
research landscape.The company on the defensive end of the case is
Utah-based Myriad Genetics, a molecular diagnos-tic company responsible for the development of the BRACAnalysis test. In 1994, it was discovered that the BRCA1 and BRCA2 genes were linked to an in-creased risk of breast cancer and ovarian cancer. As the patent holder, Myriad requires that all testing for the genes be done with the company’s test only.
(see page 24)
Personalized Medicine For the Practicing Oncology Professional
Vol. 2 No. 3
An Interview with Douglas Yee, MD, Scientific Program Chair
ASCO 2013: Key Targeted Trials
Peter Meldrum
In September 2012, the FDA ap-proved regorafenib (Stivarga) as a salvage treatment for metastatic
colorectal cancer (mCRC) previously treated with chemotherapy, an anti-
vascular endothelial growth factor (VEGF) therapy, or an anti-epidermal growth factor receptor (EGFR) therapy. Regorafenib had received a fast-track FDA review status and was approved after only a three-month review pro-cess. The drug is the first targeted oral therapy to receive an FDA approval for treatment of advanced CRC, and the second drug to be approved for mCRC in 2012.
Although progress has been made in treating colorectal cancer, in-cluding the development of biologic agents that target EGFR and angiogen-esis, the median survival in mCRC re-mains about two years. The five-year survival rate for a patient with stage II
Feature
New Developments in Oral Targeted Agents for Advanced Colorectal CancerBy Anna Azvolinsky, PhD
(continued on page 18)
Targeted TherapyNews™
In this issue...
Prostate Cancer
• �Biomarkers Still Needed
Ovarian Cancer
• �Possible Mechanism of Platinum Resistance in Ovarian Cancer Identified
Genetic Research
• �Metabolic Gene Expression Altered in Cancer, Providing Potential Drug Targets
Hematologic Malignancies
• �Numerous Drug Classes Studied for Use in Follicular and Other Lymphomas
• �Seeking a Standard in the Treat- ment of Elderly Patients With CLL
AACR Meeting
• �Spotlight on Novel Agents in Early Development
Breast Cancer
• �Trials Examine Use of T-DM1 as Combination Therapy for HER2 Breast Cancer
• �FDA Grants Breakthrough Therapy Designation for Palbociclib in Breast Cancer
Lung Cancer
• �HER2-Targeted Agents May Benefit Patients With Non-Small Cell Lung Cancer
Axel Grothey, MD

HALAVEN® (eribulin mesylate) Injection BRIEF SUMMARY – See package insert for full prescribing information.2.2 Dose Modification Assess for peripheral neuropathy and obtain complete blood cell counts prior to each dose.Recommended dose delays• Do not administer HALAVEN on Day 1 or Day 8 for any of the following:
– ANC <1,000/mm3
– Platelets <75,000/mm3
– Grade 3 or 4 non-hematological toxicities.• The Day 8 dose may be delayed for a maximum of 1 week.
– If toxicities do not resolve or improve to ≤ Grade 2 severity by Day 15, omit the dose. – If toxicities resolve or improve to ≤ Grade 2 severity by Day 15, administer HALAVEN at a reduced dose and initiate
the next cycle no sooner than 2 weeks later.Recommended dose reductions• If a dose has been delayed for toxicity and toxicities have recovered to Grade 2 severity or less, resume HALAVEN at a
reduced dose as set out in Table 1.• Do not re-escalate HALAVEN dose after it has been reduced.Table 1 Recommended Dose Reductions
Event Description Recommended HALAVEN Dose
Permanently reduce the 1.4 mg/m2 HALAVEN dose for any of the following:
1.1 mg/m2
ANC <500/mm3 for >7 days ANC <1,000 /mm3 with fever or infectionPlatelets <25,000/mm3
Platelets <50,000/mm3 requiring transfusionNon-hematologic Grade 3 or 4 toxicities Omission or delay of Day 8 HALAVEN dose in previous cycle for toxicityOccurrence of any event requiring permanent dose reduction while receiving 1.1 mg/m2 0.7 mg/m2
Occurrence of any event requiring permanent dose reduction while receiving 0.7 mg/m2 Discontinue HALAVEN ANC = absolute neutrophil count. Toxicities graded in accordance with National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) version 3.0. 5 WARNINGS AND PRECAUTIONS5.1 Neutropenia Severe neutropenia (ANC <500/mm3) lasting more than one week occurred in 12% (62/503) of patients in Study 1, leading to discontinuation in <1% of patients. Patients with alanine aminotransferase or aspartate aminotransferase >3 × ULN (upper limit of normal) experienced a higher incidence of Grade 4 neutropenia and febrile neutropenia than patients with normal aminotransferase levels. Patients with bilirubin >1.5 × ULN also had a higher incidence of Grade 4 neutropenia and febrile neutropenia.Monitor complete blood counts prior to each dose; increase the frequency of monitoring in patients who develop Grade 3 or 4 cytopenias. Delay administration of HALAVEN and reduce subsequent doses in patients who experience febrile neutropenia or Grade 4 neutropenia lasting longer than 7 days. Clinical studies of HALAVEN did not include patients with baseline neutrophil counts below 1,500/mm3.5.2 Peripheral Neuropathy Grade 3 peripheral neuropathy occurred in 8% (40/503) of patients, and Grade 4 in 0.4% (2/503) of patients in Study 1. Peripheral neuropathy was the most common toxicity leading to discontinuation of HALAVEN (5% of patients; 24/503). Neuropathy lasting more than one year occurred in 5% (26/503) of patients. Twenty-two percent (109/503) of patients developed a new or worsening neuropathy that had not recovered within a median follow-up duration of 269 days (range 25-662 days). Monitor patients closely for signs of peripheral motor and sensory neuropathy. Withhold HALAVEN in patients who experience Grade 3 or 4 peripheral neuropathy until resolution to Grade 2 or less.5.3 Embryo-Fetal ToxicityThere are no adequate and well-controlled studies of HALAVEN in pregnant women. HALAVEN is a microtubule inhibitor; therefore, it is expected to cause fetal harm when administered to a pregnant woman. Embryo-fetal toxicity and teratogenicity occurred in rats that received eribulin mesylate at approximately half of the recommended human dose based on body surface area. If this drug is used during pregnancy, or if a patient becomes pregnant while taking this drug, she should be apprised of the potential hazard to the fetus.5.4 QT ProlongationIn an uncontrolled open-label ECG study in 26 patients, QT prolongation was observed on Day 8, independent of eribulin concentration, with no QT prolongation observed on Day 1. ECG monitoring is recommended if therapy is initiated in patients with congestive heart failure, bradyarrhythmias, drugs known to prolong the QT interval, including Class Ia and III antiarrhythmics, and electrolyte abnormalities. Correct hypokalemia or hypomagnesemia prior to initiating HALAVEN and monitor these electrolytes periodically during therapy. Avoid HALAVEN in patients with congenital long QT syndrome. 6 ADVERSE REACTIONSThe following adverse reactions are discussed in detail in other sections of the labeling:•Neutropenia•Peripheralneuropathy•QTintervalprolongationThe most common adverse reactions (≥25%) reported in patients receiving HALAVEN were neutropenia, anemia, asthenia/fatigue, alopecia, peripheral neuropathy, nausea, and constipation. The most common serious adverse reactions reported in patients receiving HALAVEN were febrile neutropenia (4%) and neutropenia (2%). The most common adverse reaction resulting in discontinuation of HALAVEN was peripheral neuropathy (5%). Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in other clinical trials and may not reflect the rates observed in clinical practice. In clinical trials, HALAVEN has been administered to 1,222 patients with multiple tumor types, including 240 patients exposed to HALAVEN for 6 months or longer. The majority of the 1,222 patients were women (82%) with a median age of 58 years (range: 26 to 91 years). The racial and ethnic distribution was Caucasian (83%), Black (5%), Asian (2%), and other (5%).The adverse reactions described in Table 2 were identified in 750 patients treated in Study 1. In Study 1, patients were randomized (2:1) to receive either HALAVEN (1.4 mg/m2 on Days 1 and 8 of a 21-day cycle) or single agent treatment chosen by their physician (control group). A total of 503 patients received HALAVEN, and 247 patients in the control group received therapy consisting of chemotherapy [total 97% (anthracyclines 10%, capecitabine 18%, gemcitabine 19%, taxanes 15%, vinorelbine 25%, other chemotherapies 10%)] or hormonal therapy (3%). The median duration of exposure was 118 days for patients receiving HALAVEN and 63 days for patients receiving control therapy. Table 2 reports the most common adverse reactions occurring in at least 10% of patients in either group.Table 2 Adverse Reactions with a Per-Patient Incidence of at Least 10% in Study 1
MedDRA ver 10.0 HALAVEN (n=503) Control Group (n=247)All Grades ≥ Grade 3 All Grades ≥ Grade 3
Blood and Lymphatic System Disordersa Neutropenia 82% 57% 53% 23%Anemia 58% 2% 55% 4%Nervous system disordersPeripheral neuropathyb 35% 8% 16% 2%Headache 19% <1% 12% <1%General disorders and administrative site conditionsAsthenia/Fatigue 54% 10% 40% 11%Mucosal inflammation 9% 1% 10% 2%Pyrexia 21% <1% 13% <1%Gastrointestinal disordersConstipation 25% 1% 21% 1%Diarrhea 18% 0 18% 0Nausea 35% 1% 28% 3%Vomiting 18% 1% 18% 1%Musculoskeletal and connective tissue disordersArthralgia/Myalgia 22% <1% 12% 1%Back pain 16% 1% 7% 2%Bone pain 12% 2% 9% 2%Pain in extremity 11% 1% 10% 1%InvestigationsWeight decreased 21% 1% 14% <1%Metabolism and nutrition disordersAnorexia 20% 1% 13% 1%Respiratory, thoracic, and mediastinal disordersCough 14% 0 9% 0Dyspnea 16% 4% 13% 4%Skin and subcutaneous tissue disordersAlopecia 45% NAc 10% NAc
Table 2 (cont'd)MedDRA ver 10.0 HALAVEN (n=503) Control Group (n=247)
All Grades ≥ Grade 3 All Grades ≥ Grade 3Infections and InfestationsUrinary Tract Infection 10% 1% 5% 0
aBased upon laboratory data.b Includes neuropathy peripheral, neuropathy, peripheral motor neuropathy, polyneuropathy, peripheral sensory neuropathy, and paraesthesia.cNot applicable; (grading system does not specify > Grade 2 for alopecia).Cytopenias: Grade 3 neutropenia occurred in 28% (143/503) of patients who received HALAVEN in Study 1, and 29% (144/503) of patients experienced Grade 4 neutropenia. Febrile neutropenia occurred in 5% (23/503) of patients; two patients (0.4%) died from complications of febrile neutropenia. Dose reduction due to neutropenia was required in 12% (62/503) of patients and discontinuation was required in <1% of patients. The mean time to nadir was 13 days and the mean time to recovery from severe neutropenia (<500/mm3) was 8 days. Grade 3 or greater thrombocytopenia occurred in 1% (7/503) of patients. G-CSF (granulocyte colony-stimulating factor) or GM-CSF (granulocyte–macrophage colony-stimulating factor) was used in 19% of patients who received HALAVEN. Peripheral Neuropathy: In Study 1, 17% of enrolled patients had Grade 1 peripheral neuropathy and 3% of patients had Grade 2 peripheral neuropathy at baseline. Dose reduction due to peripheral neuropathy was required by 3% (14/503) of patients who received HALAVEN. Four percent (20/503) of patients experienced peripheral motor neuropathy of any grade and 2% (8/503) of patients developed Grade 3 peripheral motor neuropathy.Liver Function Test Abnormalities: Among patients with Grade 0 or 1 ALT levels at baseline, 18% of HALAVEN-treated patients experienced Grade 2 or greater ALT elevation. One HALAVEN-treated patient without documented liver metastases had concomitant Grade 2 elevations in bilirubin and ALT; these abnormalities resolved and did not recur with re-exposure to HALAVEN.Less Common Adverse Reactions: The following additional adverse reactions were reported in ≥5% to <10% of the HALAVEN- treated group: • Eye Disorders: increased lacrimation• Gastrointestinal Disorders: dyspepsia, abdominal pain, stomatitis, dry mouth• General Disorders and Administration Site Conditions: peripheral edema• Infections and Infestations: upper respiratory tract infection• Metabolism and Nutrition Disorders: hypokalemia• Musculoskeletal and Connective Tissue Disorders: muscle spasms, muscular weakness• Nervous System Disorders: dysgeusia, dizziness• Psychiatric Disorders: insomnia, depression• Skin and Subcutaneous Tissue Disorders: rash8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy Category DThere are no adequate and well-controlled studies with HALAVEN in pregnant women. HALAVEN is a microtubule inhibitor; therefore, it is expected to cause fetal harm when administered to a pregnant woman. Embryo-fetal toxicity and teratogenicity occurred in rats that received eribulin mesylate at approximately half of the recommended human dose based on body surface area. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. In a developmental toxicity study, pregnant rats received intravenous infusion of eribulin mesylate during organogenesis (Gestation Days 8, 10, and 12) at doses approximately 0.04, 0.13, 0.43 and 0.64 times the recommended human dose, based on body surface area (mg/m2). Increased abortion and severe external or soft tissue malformations were observed in offspring at doses 0.64 times the recommended human dose based on body surface area (mg/m2), including the absence of a lower jaw, tongue, stomach and spleen. Increased embryo-fetal death/resorption, reduced fetal weights, and minor skeletal anomalies consistent with developmental delay were also reported at or above doses of 0.43 times the recommended human dose. Maternal toxicity of eribulin mesylate was reported in rats at or above doses of 0.43 times the recommended human dose (mg/m²), and included enlarged spleen, reduced maternal weight gain and decreased food consumption.8.3 Nursing MothersIt is not known whether HALAVEN is excreted into human milk. No studies in humans or animals were conducted to determine if HALAVEN is excreted into milk. Because many drugs are excreted into human milk and because of the potential for serious adverse reactions in human milk fed infants from HALAVEN, a decision should be made whether to discontinue nursing or to discontinue HALAVEN taking into account the importance of the drug to the mother. 8.4 Pediatric UseThe safety and effectiveness of HALAVEN in pediatric patients below the age of 18 years have not been established.8.6 Hepatic ImpairmentAdministration of HALAVEN at a dose of 1.1 mg/m2 to patients with mild hepatic impairment and 0.7 mg/m2 to patients with moderate hepatic impairment resulted in similar exposure to eribulin as a dose of 1.4 mg/m2 to patients with normal hepatic function. Therefore, a lower starting dose of 1.1 mg/m2 is recommended for patients with mild hepatic impairment (Child-Pugh A) and of 0.7 mg/m2 is recommended for patients with moderate hepatic impairment (Child-Pugh B). HALAVEN was not studied in patients with severe hepatic impairment (Child-Pugh C). 8.7 Renal ImpairmentFor patients with moderate renal impairment (CrCl 30-50 mL/min), the geometric mean dose-normalized systemic exposure increased 2-fold compared to patients with normal renal function. A lower starting dose of 1.1 mg/m2 is recommended for patients with moderate renal impairment. The safety of HALAVEN was not studied in patients with severe renal impairment (CrCl <30 mL/min). 10 OVERDOSAGE Overdosage of HALAVEN has been reported at approximately 4 times the recommended dose, which resulted in Grade 3 neutropenia lasting seven days and a Grade 3 hypersensitivity reaction lasting one day. There is no known antidote for HALAVEN overdose.12 CLINICAL PHARMACOLOGY12.3 PharmacokineticsSpecific PopulationsHepatic ImpairmentA study evaluated the PK of eribulin in patients with mild (Child-Pugh A; n=7) and moderate (Child-Pugh B; n=5) hepatic impairment. Compared to patients with normal hepatic function (n=6), eribulin exposure increased 1.8-fold and 2.5-fold in patients with mild and moderate hepatic impairment, respectively. Administration of HALAVEN at a dose of 1.1 mg/m2 to patients with mild hepatic impairment and 0.7 mg/m2 to patients with moderate hepatic impairment resulted in similar exposure to eribulin as a dose of 1.4 mg/m2 to patients with normal hepatic function. Renal ImpairmentNo formal PK trials were conducted with HALAVEN in patients with renal impairment. Available data suggests that geometric mean dose-normalized systemic exposure is similar for patients with mild renal impairment (CrCl 50-80 mL/min) relative to patients with normal renal function. However, for patients with moderate renal impairment (CrCl 30-50 mL/min), the geometric mean dose-normalized systemic exposure increased 2-fold compared to patients with normal renal function. 12.6 Cardiac ElectrophysiologyThe effect of HALAVEN on the QTc interval was assessed in an open-label, uncontrolled, multicenter, single-arm dedicated QT trial. A total of 26 patients with solid tumors received 1.4 mg/m2 of HALAVEN on Days 1 and 8 of a 21-day cycle. A delayed QTc prolongation was observed on Day 8, with no prolongation observed on Day 1. The maximum mean QTcF change from baseline (95% upper confidence interval) was 11.4 (19.5) ms.13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, mutagenesis, impairment of fertilityCarcinogenicity studies have not been conducted with eribulin mesylate. Eribulin mesylate was not mutagenic in in vitro bacterial reverse mutation assays (Ames test). Eribulin mesylate was positive in mouse lymphoma mutagenesis assays, and was clastogenic in an in vivo rat bone marrow micronucleus assay. The effects of HALAVEN on human fertility are unknown. Fertility studies have not been conducted with eribulin mesylate in humans or animals. However, nonclinical findings in repeated-dose dog and rat toxicology studies suggest that male fertility may be compromised by treatment with eribulin mesylate. Rats exhibited testicular toxicity (hypocellularity of seminiferous epithelium with hypospermia/aspermia) following dosing with eribulin mesylate at or above 0.43 times the recommended human dose (mg/m2) given once weekly for 3 weeks, or at or above 0.21 times the recommended human dose (mg/m2) given once weekly for 3 out of 5 weeks, repeated for 6 cycles. Testicular toxicity was also observed in dogs given 0.64 times the recommended human dose (mg/m2) weekly for 3 out of 5 weeks, repeated for 6 cycles. 17 PATIENT COUNSELING INFORMATIONSee FDA-Approved Patient Labeling• Advise patients to contact their health care provider for a fever of 100.5°F or greater or other signs or symptoms of infection
such as chills, cough, or burning or pain on urination.• Advise women of childbearing potential to avoid pregnancy and to use effective contraception during treatment with HALAVEN.––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
HALAVEN® is a registered trademark used by Eisai Inc. under license from Eisai R&D Management Co., Ltd.© 2012 Eisai Inc. All rights reserved. Printed in USA / March 2012 ERI 346
ERIBPUS-4306_M04_A_SIZE_Brief_Summary.indd 1 3/28/12 3:08 PM
HALAVEN: The FIRST and ONLY single-agent therapy proven to signifi cantly extend OVERALL SURVIVAL after 2 prior lines of MBC therapy1-9
To learn more about Halaven, visit www.halaven.com
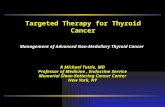
Results from an updated, unplanned survival analysis of the Phase III, randomized, open-label, multicenter, multinational EMBRACE† trial of Halaven versus TPC in patients with metastatic breast cancer (MBC) (N=762), conducted when 77% of events (deaths) had been observed. The primary endpoint was OS. Patients were randomized (2:1) to receive either Halaven 1.4 mg/m2 IV for 2 to 5 minutes on Days 1 and 8 of a 21-day cycle, or any single-agent therapy, selected prior to randomization. At baseline, all patients had received ≥2 prior chemotherapeutic regimens for metastatic disease and demonstrated disease progression within 6 months of their last chemotherapeutic regimen. All patients received prior anthracycline- and taxane-based chemotherapy, unless contraindicated. Therapies in the TPC arm consisted of 97% chemotherapy (26% vinorelbine, 18% gemcitabine, 18% capecitabine, 16% taxanes [included paclitaxel, docetaxel, nab-paclitaxel, and ixabepilone], 9% anthracyclines, 10% other chemotherapy), and 3% hormonal therapy.
The updated OS analysis was consistent with the primary analysis1
The primary analysis, conducted when ~50% of events (deaths) had been observed, demonstrated a median OS for Halaven vs TPC of 13.1 months (95% CI: 11.8, 14.3) vs 10.6 months (95% CI: 9.3, 12.5), HR*=0.81 (95% CI: 0.66, 0.99) (P=0.041)1,10
DISCOVER OVERALL SURVIVAL
After 2 prior lines of MBC chemotherapy,
IndicationHalaven is indicated for the treatment of patients with metastatic breast cancer who have previously received at least two chemotherapeutic regimens for the treatment of metastatic disease. Prior therapy should have included an anthracycline and a taxane in either the adjuvant or metastatic setting.
Important Safety InformationNeutropenia• Monitor complete blood counts prior to each dose, and increase the frequency of
monitoring in patients who develop Grade 3 or 4 cytopenias. Delay administration and reduce subsequent doses in patients who experience febrile neutropenia or Grade 4 neutropenia lasting longer than 7 days
• Severe neutropenia (ANC <500/mm3) lasting more than 1 week occurred in 12% (62/503) of patients. Patients with elevated liver enzymes >3 × ULN and bilirubin >1.5 × ULN experienced a higher incidence of Grade 4 neutropenia and febrile neutropenia than patients with normal levels
• Grade 3 and Grade 4 neutropenia occurred in 28% and 29%, respectively, of patients who received Halaven. Febrile neutropenia occurred in 5% of patients and two patients (0.4%) died from complications
Peripheral Neuropathy • Patients should be monitored closely for signs of peripheral motor and sensory
neuropathy• Grade 3 peripheral neuropathy occurred in 8% of patients, and Grade 4 in 0.4% of
patients who received Halaven. Delay administration of Halaven until resolution to Grade 2 or less
• Neuropathy lasting more than 1 year occurred in 5% of patients. Twenty-two percent of patients developed a new or worsening neuropathy that had not recovered within a median follow-up duration of 269 days (range 25-662 days)
• Peripheral neuropathy (5%) was the most common adverse reaction resulting in discontinuation
Pregnancy Category D • Halaven is expected to cause fetal harm when administered to a pregnant
woman and patients should be advised of these risks
QT Prolongation• In an uncontrolled ECG study in 26 patients, QT prolongation was observed on Day 8,
independent of eribulin concentration, with no prolongation on Day 1. ECG monitoring is recommended for patients with congestive heart failure; bradyarrhythmias; concomitant use of drugs that prolong QT interval, including Class Ia and III antiarrhythmics; and electrolyte abnormalities
• Correct hypokalemia or hypomagnesemia prior to initiating Halaven and monitor electrolytes periodically during therapy. Avoid in patients with congenital long QT syndrome
Hepatic and Renal Impairment • For patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic and/or moderate
(CrCl 30-50 mL/min) renal impairment, a reduction in starting dose is recommended
Most Common Adverse Reactions• Most common adverse reactions (≥25%) reported in patients receiving Halaven were
neutropenia (82%), anemia (58%), asthenia/fatigue (54%), alopecia (45%), peripheral neuropathy (35%), nausea (35%), and constipation (25%)
• The most common serious adverse reactions reported in patients receiving Halaven were febrile neutropenia (4%) and neutropenia (2%)
References: 1. Halaven [package insert]. Woodcliff Lake, NJ: Eisai Inc; 2012. 2. Saad ED et al. J Clin Oncol. 2010;28(11):1958-1962. 3. Slamon DJ et al. N Engl J Med. 2001;344(11):783-792. 4. Geyer CE et al. N Engl J Med. 2006;355(26):2733-2743. 5. von Minckwitz G et al. J Clin Oncol. 2009;27(12):1999-2006. 6. Miller K et al. N Engl J Med. 2007;357(26):2666-2676. 7. Robert NJ et al. J Clin Oncol. 2011;29(10):1252-1260. 8. Sparano JA et al. J Clin Oncol. 2010;28(20):3256-3263. 9. Jones SE et al. J Clin Oncol. 2005;23(24):5542-5551. 10. Cortes J et al. Lancet. 2011;377(9769):914-923.
*HR=hazard ratio. † EMBRACE=Eisai Metastatic Breast Cancer Study Assessing Physician’s Choice versus E7389 (Eribulin).
Please see accompanying brief summary of Halaven full Prescribing Information.
HALAVEN® is a registered trademark used by Eisai Inc. under license from Eisai R&D Management Co., Ltd.© 2012 Eisai Inc. All rights reserved. Printed in USA/August 2012 HALA0042 R1
CI=con� dence interval; Treatment of Physician’s Choice (Control arm)=TPC.aConducted in the intent-to-treat (ITT) population.
UPDATED OVERALL SURVIVAL (OS) ANALYSIS (UNPLANNED): MEDIAN OS, MONTHS (95% CI)1,10,a
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
TIME (MONTHS)
PR
OP
OR
TIO
N O
F P
AT
IEN
TS
AL
IVE
0 6 12 18 24 30 36
508 406 274 142 54 11 0254 178 106 61 26 5 0
HalavenTPC
Number ofpatients at risk
Treatment of Physician’s Choice (n=254)
10.6(9.2, 12.0)Deaths=203
Halaven (n=508) 25%(2.6 month)
INCREASE IN MEDIAN OS
13.2(12.1, 14.4)Deaths=386
ERIBPUS-4563_M01_Comp3_King_Single.indd 1 1/30/13 12:01 PM

HALAVEN® (eribulin mesylate) Injection BRIEF SUMMARY – See package insert for full prescribing information.2.2 Dose Modification Assess for peripheral neuropathy and obtain complete blood cell counts prior to each dose.Recommended dose delays• Do not administer HALAVEN on Day 1 or Day 8 for any of the following:
– ANC <1,000/mm3
– Platelets <75,000/mm3
– Grade 3 or 4 non-hematological toxicities.• The Day 8 dose may be delayed for a maximum of 1 week.
– If toxicities do not resolve or improve to ≤ Grade 2 severity by Day 15, omit the dose. – If toxicities resolve or improve to ≤ Grade 2 severity by Day 15, administer HALAVEN at a reduced dose and initiate
the next cycle no sooner than 2 weeks later.Recommended dose reductions• If a dose has been delayed for toxicity and toxicities have recovered to Grade 2 severity or less, resume HALAVEN at a
reduced dose as set out in Table 1.• Do not re-escalate HALAVEN dose after it has been reduced.Table 1 Recommended Dose Reductions
Event Description Recommended HALAVEN Dose
Permanently reduce the 1.4 mg/m2 HALAVEN dose for any of the following:
1.1 mg/m2
ANC <500/mm3 for >7 days ANC <1,000 /mm3 with fever or infectionPlatelets <25,000/mm3
Platelets <50,000/mm3 requiring transfusionNon-hematologic Grade 3 or 4 toxicities Omission or delay of Day 8 HALAVEN dose in previous cycle for toxicityOccurrence of any event requiring permanent dose reduction while receiving 1.1 mg/m2 0.7 mg/m2
Occurrence of any event requiring permanent dose reduction while receiving 0.7 mg/m2 Discontinue HALAVEN ANC = absolute neutrophil count. Toxicities graded in accordance with National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) version 3.0. 5 WARNINGS AND PRECAUTIONS5.1 Neutropenia Severe neutropenia (ANC <500/mm3) lasting more than one week occurred in 12% (62/503) of patients in Study 1, leading to discontinuation in <1% of patients. Patients with alanine aminotransferase or aspartate aminotransferase >3 × ULN (upper limit of normal) experienced a higher incidence of Grade 4 neutropenia and febrile neutropenia than patients with normal aminotransferase levels. Patients with bilirubin >1.5 × ULN also had a higher incidence of Grade 4 neutropenia and febrile neutropenia.Monitor complete blood counts prior to each dose; increase the frequency of monitoring in patients who develop Grade 3 or 4 cytopenias. Delay administration of HALAVEN and reduce subsequent doses in patients who experience febrile neutropenia or Grade 4 neutropenia lasting longer than 7 days. Clinical studies of HALAVEN did not include patients with baseline neutrophil counts below 1,500/mm3.5.2 Peripheral Neuropathy Grade 3 peripheral neuropathy occurred in 8% (40/503) of patients, and Grade 4 in 0.4% (2/503) of patients in Study 1. Peripheral neuropathy was the most common toxicity leading to discontinuation of HALAVEN (5% of patients; 24/503). Neuropathy lasting more than one year occurred in 5% (26/503) of patients. Twenty-two percent (109/503) of patients developed a new or worsening neuropathy that had not recovered within a median follow-up duration of 269 days (range 25-662 days). Monitor patients closely for signs of peripheral motor and sensory neuropathy. Withhold HALAVEN in patients who experience Grade 3 or 4 peripheral neuropathy until resolution to Grade 2 or less.5.3 Embryo-Fetal ToxicityThere are no adequate and well-controlled studies of HALAVEN in pregnant women. HALAVEN is a microtubule inhibitor; therefore, it is expected to cause fetal harm when administered to a pregnant woman. Embryo-fetal toxicity and teratogenicity occurred in rats that received eribulin mesylate at approximately half of the recommended human dose based on body surface area. If this drug is used during pregnancy, or if a patient becomes pregnant while taking this drug, she should be apprised of the potential hazard to the fetus.5.4 QT ProlongationIn an uncontrolled open-label ECG study in 26 patients, QT prolongation was observed on Day 8, independent of eribulin concentration, with no QT prolongation observed on Day 1. ECG monitoring is recommended if therapy is initiated in patients with congestive heart failure, bradyarrhythmias, drugs known to prolong the QT interval, including Class Ia and III antiarrhythmics, and electrolyte abnormalities. Correct hypokalemia or hypomagnesemia prior to initiating HALAVEN and monitor these electrolytes periodically during therapy. Avoid HALAVEN in patients with congenital long QT syndrome. 6 ADVERSE REACTIONSThe following adverse reactions are discussed in detail in other sections of the labeling:•Neutropenia•Peripheralneuropathy•QTintervalprolongationThe most common adverse reactions (≥25%) reported in patients receiving HALAVEN were neutropenia, anemia, asthenia/fatigue, alopecia, peripheral neuropathy, nausea, and constipation. The most common serious adverse reactions reported in patients receiving HALAVEN were febrile neutropenia (4%) and neutropenia (2%). The most common adverse reaction resulting in discontinuation of HALAVEN was peripheral neuropathy (5%). Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in other clinical trials and may not reflect the rates observed in clinical practice. In clinical trials, HALAVEN has been administered to 1,222 patients with multiple tumor types, including 240 patients exposed to HALAVEN for 6 months or longer. The majority of the 1,222 patients were women (82%) with a median age of 58 years (range: 26 to 91 years). The racial and ethnic distribution was Caucasian (83%), Black (5%), Asian (2%), and other (5%).The adverse reactions described in Table 2 were identified in 750 patients treated in Study 1. In Study 1, patients were randomized (2:1) to receive either HALAVEN (1.4 mg/m2 on Days 1 and 8 of a 21-day cycle) or single agent treatment chosen by their physician (control group). A total of 503 patients received HALAVEN, and 247 patients in the control group received therapy consisting of chemotherapy [total 97% (anthracyclines 10%, capecitabine 18%, gemcitabine 19%, taxanes 15%, vinorelbine 25%, other chemotherapies 10%)] or hormonal therapy (3%). The median duration of exposure was 118 days for patients receiving HALAVEN and 63 days for patients receiving control therapy. Table 2 reports the most common adverse reactions occurring in at least 10% of patients in either group.Table 2 Adverse Reactions with a Per-Patient Incidence of at Least 10% in Study 1
MedDRA ver 10.0 HALAVEN (n=503) Control Group (n=247)All Grades ≥ Grade 3 All Grades ≥ Grade 3
Blood and Lymphatic System Disordersa Neutropenia 82% 57% 53% 23%Anemia 58% 2% 55% 4%Nervous system disordersPeripheral neuropathyb 35% 8% 16% 2%Headache 19% <1% 12% <1%General disorders and administrative site conditionsAsthenia/Fatigue 54% 10% 40% 11%Mucosal inflammation 9% 1% 10% 2%Pyrexia 21% <1% 13% <1%Gastrointestinal disordersConstipation 25% 1% 21% 1%Diarrhea 18% 0 18% 0Nausea 35% 1% 28% 3%Vomiting 18% 1% 18% 1%Musculoskeletal and connective tissue disordersArthralgia/Myalgia 22% <1% 12% 1%Back pain 16% 1% 7% 2%Bone pain 12% 2% 9% 2%Pain in extremity 11% 1% 10% 1%InvestigationsWeight decreased 21% 1% 14% <1%Metabolism and nutrition disordersAnorexia 20% 1% 13% 1%Respiratory, thoracic, and mediastinal disordersCough 14% 0 9% 0Dyspnea 16% 4% 13% 4%Skin and subcutaneous tissue disordersAlopecia 45% NAc 10% NAc
Table 2 (cont'd)MedDRA ver 10.0 HALAVEN (n=503) Control Group (n=247)
All Grades ≥ Grade 3 All Grades ≥ Grade 3Infections and InfestationsUrinary Tract Infection 10% 1% 5% 0
aBased upon laboratory data.b Includes neuropathy peripheral, neuropathy, peripheral motor neuropathy, polyneuropathy, peripheral sensory neuropathy, and paraesthesia.cNot applicable; (grading system does not specify > Grade 2 for alopecia).Cytopenias: Grade 3 neutropenia occurred in 28% (143/503) of patients who received HALAVEN in Study 1, and 29% (144/503) of patients experienced Grade 4 neutropenia. Febrile neutropenia occurred in 5% (23/503) of patients; two patients (0.4%) died from complications of febrile neutropenia. Dose reduction due to neutropenia was required in 12% (62/503) of patients and discontinuation was required in <1% of patients. The mean time to nadir was 13 days and the mean time to recovery from severe neutropenia (<500/mm3) was 8 days. Grade 3 or greater thrombocytopenia occurred in 1% (7/503) of patients. G-CSF (granulocyte colony-stimulating factor) or GM-CSF (granulocyte–macrophage colony-stimulating factor) was used in 19% of patients who received HALAVEN. Peripheral Neuropathy: In Study 1, 17% of enrolled patients had Grade 1 peripheral neuropathy and 3% of patients had Grade 2 peripheral neuropathy at baseline. Dose reduction due to peripheral neuropathy was required by 3% (14/503) of patients who received HALAVEN. Four percent (20/503) of patients experienced peripheral motor neuropathy of any grade and 2% (8/503) of patients developed Grade 3 peripheral motor neuropathy.Liver Function Test Abnormalities: Among patients with Grade 0 or 1 ALT levels at baseline, 18% of HALAVEN-treated patients experienced Grade 2 or greater ALT elevation. One HALAVEN-treated patient without documented liver metastases had concomitant Grade 2 elevations in bilirubin and ALT; these abnormalities resolved and did not recur with re-exposure to HALAVEN.Less Common Adverse Reactions: The following additional adverse reactions were reported in ≥5% to <10% of the HALAVEN- treated group: • Eye Disorders: increased lacrimation• Gastrointestinal Disorders: dyspepsia, abdominal pain, stomatitis, dry mouth• General Disorders and Administration Site Conditions: peripheral edema• Infections and Infestations: upper respiratory tract infection• Metabolism and Nutrition Disorders: hypokalemia• Musculoskeletal and Connective Tissue Disorders: muscle spasms, muscular weakness• Nervous System Disorders: dysgeusia, dizziness• Psychiatric Disorders: insomnia, depression• Skin and Subcutaneous Tissue Disorders: rash8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy Category DThere are no adequate and well-controlled studies with HALAVEN in pregnant women. HALAVEN is a microtubule inhibitor; therefore, it is expected to cause fetal harm when administered to a pregnant woman. Embryo-fetal toxicity and teratogenicity occurred in rats that received eribulin mesylate at approximately half of the recommended human dose based on body surface area. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. In a developmental toxicity study, pregnant rats received intravenous infusion of eribulin mesylate during organogenesis (Gestation Days 8, 10, and 12) at doses approximately 0.04, 0.13, 0.43 and 0.64 times the recommended human dose, based on body surface area (mg/m2). Increased abortion and severe external or soft tissue malformations were observed in offspring at doses 0.64 times the recommended human dose based on body surface area (mg/m2), including the absence of a lower jaw, tongue, stomach and spleen. Increased embryo-fetal death/resorption, reduced fetal weights, and minor skeletal anomalies consistent with developmental delay were also reported at or above doses of 0.43 times the recommended human dose. Maternal toxicity of eribulin mesylate was reported in rats at or above doses of 0.43 times the recommended human dose (mg/m²), and included enlarged spleen, reduced maternal weight gain and decreased food consumption.8.3 Nursing MothersIt is not known whether HALAVEN is excreted into human milk. No studies in humans or animals were conducted to determine if HALAVEN is excreted into milk. Because many drugs are excreted into human milk and because of the potential for serious adverse reactions in human milk fed infants from HALAVEN, a decision should be made whether to discontinue nursing or to discontinue HALAVEN taking into account the importance of the drug to the mother. 8.4 Pediatric UseThe safety and effectiveness of HALAVEN in pediatric patients below the age of 18 years have not been established.8.6 Hepatic ImpairmentAdministration of HALAVEN at a dose of 1.1 mg/m2 to patients with mild hepatic impairment and 0.7 mg/m2 to patients with moderate hepatic impairment resulted in similar exposure to eribulin as a dose of 1.4 mg/m2 to patients with normal hepatic function. Therefore, a lower starting dose of 1.1 mg/m2 is recommended for patients with mild hepatic impairment (Child-Pugh A) and of 0.7 mg/m2 is recommended for patients with moderate hepatic impairment (Child-Pugh B). HALAVEN was not studied in patients with severe hepatic impairment (Child-Pugh C). 8.7 Renal ImpairmentFor patients with moderate renal impairment (CrCl 30-50 mL/min), the geometric mean dose-normalized systemic exposure increased 2-fold compared to patients with normal renal function. A lower starting dose of 1.1 mg/m2 is recommended for patients with moderate renal impairment. The safety of HALAVEN was not studied in patients with severe renal impairment (CrCl <30 mL/min). 10 OVERDOSAGE Overdosage of HALAVEN has been reported at approximately 4 times the recommended dose, which resulted in Grade 3 neutropenia lasting seven days and a Grade 3 hypersensitivity reaction lasting one day. There is no known antidote for HALAVEN overdose.12 CLINICAL PHARMACOLOGY12.3 PharmacokineticsSpecific PopulationsHepatic ImpairmentA study evaluated the PK of eribulin in patients with mild (Child-Pugh A; n=7) and moderate (Child-Pugh B; n=5) hepatic impairment. Compared to patients with normal hepatic function (n=6), eribulin exposure increased 1.8-fold and 2.5-fold in patients with mild and moderate hepatic impairment, respectively. Administration of HALAVEN at a dose of 1.1 mg/m2 to patients with mild hepatic impairment and 0.7 mg/m2 to patients with moderate hepatic impairment resulted in similar exposure to eribulin as a dose of 1.4 mg/m2 to patients with normal hepatic function. Renal ImpairmentNo formal PK trials were conducted with HALAVEN in patients with renal impairment. Available data suggests that geometric mean dose-normalized systemic exposure is similar for patients with mild renal impairment (CrCl 50-80 mL/min) relative to patients with normal renal function. However, for patients with moderate renal impairment (CrCl 30-50 mL/min), the geometric mean dose-normalized systemic exposure increased 2-fold compared to patients with normal renal function. 12.6 Cardiac ElectrophysiologyThe effect of HALAVEN on the QTc interval was assessed in an open-label, uncontrolled, multicenter, single-arm dedicated QT trial. A total of 26 patients with solid tumors received 1.4 mg/m2 of HALAVEN on Days 1 and 8 of a 21-day cycle. A delayed QTc prolongation was observed on Day 8, with no prolongation observed on Day 1. The maximum mean QTcF change from baseline (95% upper confidence interval) was 11.4 (19.5) ms.13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, mutagenesis, impairment of fertilityCarcinogenicity studies have not been conducted with eribulin mesylate. Eribulin mesylate was not mutagenic in in vitro bacterial reverse mutation assays (Ames test). Eribulin mesylate was positive in mouse lymphoma mutagenesis assays, and was clastogenic in an in vivo rat bone marrow micronucleus assay. The effects of HALAVEN on human fertility are unknown. Fertility studies have not been conducted with eribulin mesylate in humans or animals. However, nonclinical findings in repeated-dose dog and rat toxicology studies suggest that male fertility may be compromised by treatment with eribulin mesylate. Rats exhibited testicular toxicity (hypocellularity of seminiferous epithelium with hypospermia/aspermia) following dosing with eribulin mesylate at or above 0.43 times the recommended human dose (mg/m2) given once weekly for 3 weeks, or at or above 0.21 times the recommended human dose (mg/m2) given once weekly for 3 out of 5 weeks, repeated for 6 cycles. Testicular toxicity was also observed in dogs given 0.64 times the recommended human dose (mg/m2) weekly for 3 out of 5 weeks, repeated for 6 cycles. 17 PATIENT COUNSELING INFORMATIONSee FDA-Approved Patient Labeling• Advise patients to contact their health care provider for a fever of 100.5°F or greater or other signs or symptoms of infection
such as chills, cough, or burning or pain on urination.• Advise women of childbearing potential to avoid pregnancy and to use effective contraception during treatment with HALAVEN.––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
HALAVEN® is a registered trademark used by Eisai Inc. under license from Eisai R&D Management Co., Ltd.© 2012 Eisai Inc. All rights reserved. Printed in USA / March 2012 ERI 346
ERIBPUS-4306_M04_A_SIZE_Brief_Summary.indd 1 3/28/12 3:08 PM

In This Issue...2
Targeted Therapy News • 5.13
17 Researchers Identify How Nongenetic Mechanisms of Cancer Cell Diversity Can Affect Treatment Response
ByAnnaAzvolinsky,PhD A new study suggests that even
tumor cells with a common genetic background can display functional heterogeneity. This may mean that nongenetic mechanisms, such as microenvironment and epigenetic differences, may contribute to tumor growth and therapy resistance.
17 BRCA Gene Patenting Case Reaches the Supreme Court
ByBenLeach An impending court decision could
change the research landscape.
18 New Developments in Oral Targeted Agents for Advanced Colorectal Cancer
ByAnnaAzvolinsky,PhD Although progress has been
made in treating colorectal cancer, the median survival re-mains about two years. New, targeted oral agents are in development.
20 Integrating Novel Agents into the Treatment of Prostate Cancer Case-Based Discussion
ByBethFandIncollingo In the wake of the approval of several
novel treatments for prostate can-cer—including antiandrogens enzalu-tamide and abiraterone and immuno-therapy sipuleucel-T, physicans must now focus on how to best integrate new therapies into prostate cancer treatment.
24 A Guide to ASCO 2013: Key Targeted Trials
ByAnnaAzvolinsky,PhD An Interview with Douglas
Yee, MD, Scientific Program Chair
28 Research Profile: Notch Holds Promise, but Presents Obstacles as Cancer Target
EvIDEnCE-BASED OnCOlOgY29 Bundled Payment: Practice Savior or Killer? By Kurt Ullman
Features News
Departments
PrOSTATE CAnCEr7 Biomarkers Still Needed
By Devera Pine
OvArIAn CAnCEr7 Possible Mechanism of Platinum
Resistance in Ovarian Cancer IdentifiedBy Ben Leach
gEnETIC rESEArCh8 Metabolic Gene Expression Altered
in Cancer, Providing Potential Drug TargetsBy Andrew J. Roth
hEMATOlOgIC MAlIgnAnCIES9 Numerous Drug Classes Studied for Use in
Follicular and Other LymphomasBy Beth Fand Incollingo
13 Seeking a Standard in the Treatment of Elderly Patients With CLLBy Beth Fand Incollingo
AACr AnnuAl MEETIng14 Spotlight on Novel Agents in Early
Development By Anna Azvolinsky, PhD
BrEAST CAnCEr15 Trials Examine Use of T-DM1 as
Combination Therapy for HER2 Breast CancerBy Ben Leach
15 FDA Grants Breakthrough Therapy Designation for Palbociclib in Breast CancerBy Ben Leach
lung CAnCEr16 HER2-Targeted Agents May Benefit
Patients With Non-Small Cell Lung CancerBy Ben Leach
OfficeCenteratPrincetonMeadows,Bldg.300Plainsboro,NJ08536•(609)716-7777
The content contained in this publication is for general information purposes only. The reader is encouraged to confirm the information presented with other sources. Targeted Therapy News makes no representations or warranties of any kind about the complete-ness, accuracy, timeliness, reliability, or suitability of any of the information, including content or advertisements, contained in this publication and expressly disclaims liability for any errors and omissions that may be presented in this publication. Targeted Therapy News reserves the right to alter or correct any error or omission in the information it provides in this publication, without any obligations. Targeted Therapy News further disclaims any and all liability for any direct, indirect, consequential, special, exemplary, or other damages arising from the use or misuse of any material or information presented in this publication. The views expressed in this publication are those of the authors and do not necessarily reflect the opinion or policy of Targeted Therapy News.
HealthcareCommunications
Targeted
Chairman/Chief Executive OfficerMike Hennessy
Chief Operating OfficerTighe Blazier
Chief Financial OfficerNeil Glasser, CPA / CFE
Executive vice President, Executive Director of EducationJudy V. Lum, MPA
vice President, Executive Creative DirectorJeff Brown
Corporate
Director of OperationsThomas J. Kanzler
Director of CirculationJohn [email protected]
ControllerJonathan Fisher, CPA
Assistant ControllerLeah Babitz, CPA
Operations & Finance
vice President, Digital MediaJung Kim
Digital Media
Executive vice President Rob [email protected]
vice President, Sales & MarketingLisa [email protected]
Director of SalesScott [email protected]
national Accounts representativeNicole [email protected]
Sales & Marketing
EditorDevera [email protected]
vice President, Oncology and Managed MarketsLyn [email protected]
Senior EditorsAnita T. ShafferJason M. BroderickBeth Fand Incollingo
Associate EditorsLauren M. GreenBen Leach
Web Editor, Social Strategy ManagerSilas Inman
Assistant Web EditorAndrew J. Roth
Design DirectorJennifer Rittmann
Editorial & Production
PresidentPeter [email protected]
Leonard Gomella, MD
Douglas Yee, MD
In the newly metastatic CRPC patient who is asymptomatic or minimally symptomatic
INDICATION: PROVENGE® (sipuleucel-T) is an autologous cellular immunotherapy indicated for the treatment of asymptomatic or minimally symptomatic metastatic castrate resistant (hormone refractory) prostate cancer. IMPORTANT SAFETY INFORMATION: PROVENGE is intended solely for autologous use and is not routinely tested for transmissible infectious diseases. In controlled clinical trials, serious adverse events reported in the PROVENGE group included acute infusion reactions (occurring within 1 day of infusion) and cerebrovascular events. Severe (Grade 3) acute infusion reactions were reported in 3.5% of patients in the PROVENGE group. Reactions included chills, fever, fatigue, asthenia, dyspnea, hypoxia, bronchospasm, dizziness, headache, hypertension, muscle ache, nausea, and vomiting. No Grade 4 or 5 acute infusion reactions were reported in patients in the PROVENGE group. The most common adverse events (incidence ≥15%) reported in the PROVENGE group were chills, fatigue, fever, back pain, nausea, joint ache, and headache. For more information on PROVENGE, please see Brief Summary of Prescribing Information on adjacent pages.
*A sustained immune response was seen out to 26 weeks in the pivotal study (the last time point measured).1
AND HELPS HIS IMMUNE SYSTEMSUSTAIN* IT1
STARTS THE FIGHT
• Targets and attacks prostate cancer cells
• Statistically signifi cant overall survival advantage1,2
• Sustained* immune response
www.PROVENGEHCP.com
PROF35855_ProvengeAd_TarTherNews_DR2.indd 1 3/8/13 11:13 AM
Daniel P. Petrylak, MD
Dennis Vitkup, PhD
Bruce D Cheson, MD
Mark Pegram, MD
Richard Finn, MD
Benjamin W. Purow, MD

In the newly metastatic CRPC patient who is asymptomatic or minimally symptomatic
INDICATION: PROVENGE® (sipuleucel-T) is an autologous cellular immunotherapy indicated for the treatment of asymptomatic or minimally symptomatic metastatic castrate resistant (hormone refractory) prostate cancer. IMPORTANT SAFETY INFORMATION: PROVENGE is intended solely for autologous use and is not routinely tested for transmissible infectious diseases. In controlled clinical trials, serious adverse events reported in the PROVENGE group included acute infusion reactions (occurring within 1 day of infusion) and cerebrovascular events. Severe (Grade 3) acute infusion reactions were reported in 3.5% of patients in the PROVENGE group. Reactions included chills, fever, fatigue, asthenia, dyspnea, hypoxia, bronchospasm, dizziness, headache, hypertension, muscle ache, nausea, and vomiting. No Grade 4 or 5 acute infusion reactions were reported in patients in the PROVENGE group. The most common adverse events (incidence ≥15%) reported in the PROVENGE group were chills, fatigue, fever, back pain, nausea, joint ache, and headache. For more information on PROVENGE, please see Brief Summary of Prescribing Information on adjacent pages.
*A sustained immune response was seen out to 26 weeks in the pivotal study (the last time point measured).1
AND HELPS HIS IMMUNE SYSTEMSUSTAIN* IT1
STARTS THE FIGHT
• Targets and attacks prostate cancer cells
• Statistically signifi cant overall survival advantage1,2
• Sustained* immune response
www.PROVENGEHCP.com
PROF35855_ProvengeAd_TarTherNews_DR2.indd 1 3/8/13 11:13 AM

PROVENGE® (sipuleucel-T)Suspension for Intravenous Infusion Rx Only
BRIEF SUMMARY — See full Prescribing Information for complete product information
INDICATIONS AND USAGE: PROVENGE® (sipuleucel-T) is an autologous cellular immunotherapy indicated for the treatment of asymptomatic or minimally symptomatic metastatic castrate resistant (hormone refractory) prostate cancer.
DOSAGE AND ADMINISTRATION •For Autologous Use Only. •TherecommendedcourseoftherapyforPROVENGEis3completedoses,givenat
approximately 2-week intervals. •Premedicatepatientswithoralacetaminophenandanantihistaminesuchas
diphenhydramine. •Beforeinfusion,confirmthatthepatient’sidentitymatchesthepatientidentifierson
the infusion bag. •Do Not Initiate Infusion of Expired Product. •InfusePROVENGEintravenouslyoveraperiodofapproximately60minutes.
Do Not Use a Cell Filter. •Interruptorslowinfusionasnecessaryforacuteinfusionreactions,dependingon
the severity of the reaction.
(See Dosage and Administration [2] of full Prescribing Information.)
CONTRAINDICATIONS: None.
WARNINGS AND PRECAUTIONS
•PROVENGE is intended solely for autologous use.
•Acute infusion reactions (reported within 1 day of infusion) included, but were not limited to, fever, chills, respiratory events (dyspnea, hypoxia, and bronchospasm), nausea, vomiting, fatigue, hypertension, and tachycardia. In controlled clinical trials, 71.2% of patients in the PROVENGE group developed an acute infusion reaction.
In controlled clinical trials, severe (Grade 3) acute infusion reactions were reported in 3.5% of patients in the PROVENGE group. Reactions included chills, fever, fatigue, asthenia, dyspnea, hypoxia, bronchospasm, dizziness, headache, hypertension, muscle ache, nausea, and vomiting. The incidence of severe events was greater following the secondinfusion(2.1%vs0.8%followingthefirstinfusion),anddecreasedto1.3%following the third infusion. Some (1.2%) patients in the PROVENGE group were hospitalized within 1 day of infusion for management of acute infusion reactions. No Grade 4 or 5 acute infusion reactions were reported in patients in the PROVENGE group.
Closely monitor patients with cardiac or pulmonary conditions. In the event of an acute infusion reaction, the infusion rate may be decreased, or the infusion stopped, depending on the severity of the reaction. Appropriate medical therapy should be administered as needed.
•Handling Precautions for Control of Infectious Disease. PROVENGE is not routinely tested for transmissible infectious diseases. Therefore, patient leukapheresis material and PROVENGE may carry the risk of transmitting infectious diseases to health care professionals handling the product. Universal precautions should be followed.
•Concomitant Chemotherapy or Immunosuppressive Therapy. Use of either chemotherapy or immunosuppressive agents (such as systemic corticosteroids) given concurrently with the leukapheresis procedure or PROVENGE has not been studied. PROVENGE is designed to stimulate the immune system, and concurrent useofimmunosuppressiveagentsmayaltertheefficacyand/orsafetyofPROVENGE.Therefore, patients should be carefully evaluated to determine whether it is medically appropriate to reduce or discontinue immunosuppressive agents prior to treatment with PROVENGE.
•Product Safety Testing. PROVENGE is released for infusion based on the microbial and sterility results from several tests: microbial contamination determination by Gram stain, endotoxin content, and in-process sterility with a 2-day incubation to determineabsenceofmicrobialgrowth.Thefinal(7-dayincubation)sterilitytestresults are not available at the time of infusion. If the sterility results become positive for microbial contamination after PROVENGE has been approved for infusion, Dendreon will notify the treating physician. Dendreon will attempt to identify the microorganism, perform antibiotic sensitivity testing on recovered microorganisms, and communicate the results to the treating physician. Dendreon may request additional information from the physician in order to determine the source of contamination.
(See Warnings and Precautions [5] of full Prescribing Information.)
ADVERSE REACTIONSBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
ThesafetyevaluationofPROVENGEisbasedon601prostatecancerpatientsinthePROVENGE group who underwent at least 1 leukapheresis procedure in four randomized, controlled clinical trials. The control was non-activated autologous peripheral blood mononuclear cells.
The most common adverse events, reported in patients in the PROVENGE group at a rate ≥15%, were chills, fatigue, fever, back pain, nausea, joint ache, and headache. Severe (Grade3)andlife-threatening(Grade4)adverseeventswerereportedin23.6%and4.0%of patients in the PROVENGE group compared with 25.1% and 3.3% of patients in the control group. Fatal (Grade 5) adverse events were reported in 3.3% of patients in the PROVENGE group compared with 3.6% of patients in the control group.
Seriousadverseeventswerereportedin24.0%ofpatientsinthePROVENGEgroupand25.1% of patients in the control group. Serious adverse events in the PROVENGE group included acute infusion reactions (see Warnings and Precautions), cerebrovascular events, and single case reports of eosinophilia, rhabdomyolysis, myasthenia gravis, myositis, and tumor flare.
PROVENGE was discontinued in 1.5% of patients in Study 1 (PROVENGE group n=341; Control group n=171) due to adverse events. Some patients who required central venous catheters for treatment with PROVENGE developed infections, including sepsis. A small number of these patients discontinued treatment as a result. Monitoring for infectious sequelae in patients with central venous catheters is recommended.
Each dose of PROVENGE requires a standard leukapheresis procedure approximately 3 days prior to the infusion. Adverse events that were reported ≤1 day following a leukapheresis procedure in ≥5% of patients in controlled clinical trials included citrate toxicity (14.2%), oralparesthesia(12.6%),paresthesia(11.4%),andfatigue(8.3%).
Table 1 provides the frequency and severity of adverse events reported in ≥5% of patients in the PROVENGE group of randomized, controlled trials of men with prostate cancer. Thepopulationincluded485patientswithmetastaticcastrateresistantprostatecancerand 116 patients with non-metastatic androgen dependent prostate cancer who were scheduled to receive 3 infusions of PROVENGE at approximately 2-week intervals. The populationwasage40to91years(median70years),and90.6%ofpatients were Caucasian.
Table 1 Incidence of Adverse Events Occurring in ≥5% of Patients Randomized to PROVENGE
Any Adverse EventChillsFatigueFeverBack painNauseaJoint acheHeadacheCitrate toxicityParesthesiaVomitingAnemiaConstipationPainParesthesia oralPain in extremityDizzinessMuscle acheAstheniaDiarrheaInfluenza-like illnessMusculoskeletal painDyspneaEdema peripheralHot flushHematuriaMuscle spasms
591 (98.3)319(53.1)247 (41.1)188(31.3)178(29.6)129(21.5)118(19.6)109(18.1)89(14.8)85(14.1)80(13.3)75 (12.5)74 (12.3)74 (12.3)74 (12.3)73 (12.1)71(11.8)71(11.8)65(10.8)60(10.0)58(9.7)54(9.0)52(8.7)50(8.3)49(8.2)46 (7.7)46 (7.7)
186 (30.9)13 (2.2)6(1.0)6(1.0)18(3.0)3(0.5)11(1.8)4(0.7)0(0.0)1(0.2)2(0.3)11(1.8)1(0.2)7 (1.2)0(0.0)5(0.8)2(0.3)3(0.5)6(1.0)1(0.2)0(0.0)3(0.5)11(1.8)1(0.2)2(0.3)6(1.0)2(0.3)
291 (96.0)33(10.9)105(34.7)29(9.6)87(28.7)45(14.9)62(20.5)20(6.6)
43 (14.2)43 (14.2)
23 (7.6)34 (11.2)40(13.2)20(6.6)
43 (14.2)40(13.2)34 (11.2)
17 (5.6)20(6.6)
34 (11.2)11 (3.6)31(10.2)
14 (4.6)31(10.2)29(9.6)18(5.9)17 (5.6)
97 (32.0)0(0.0)4 (1.3)3(1.0)9(3.0)0(0.0)5 (1.7)0(0.0)0(0.0)0(0.0)0(0.0)7 (2.3)3(1.0)3(1.0)0(0.0)1(0.3)0(0.0)0(0.0)2(0.7)3(1.0)0(0.0)3(1.0)3(1.0)1(0.3)1(0.3)3(1.0)0(0.0)
All Gradesn (%)
All Gradesn (%)
Grade 3-5n (%)
Grade 3-5n (%)
PROVENGE (N = 601) Control* (N = 303)
(Table 1 continued on next page.)
PROF35855_ProvengeAd_TarTherNews_DR2.indd 2 3/8/13 11:13 AM

Targeted Therapy News • 5.13
This year’s annual meeting of the American Society of Clinical Oncology (ASCO) will feature the presentation of new data that advances our understanding and targeted treatment of cancer. In this issue of Targeted Therapy News, we speak
with Douglas Yee, MD, chair of ASCO’s Scientific Program Committee, about key presen-tations and new features at this year’s meeting. This issue also offers an in-depth look at some of the intriguing research results that came out of the American Association for Cancer Research (AACR) annual meeting held in April.
For breaking news from ASCO, check TargetedHC.com daily, follow TargetedHC on Twitter, or find us on Facebook. Expert perspectives and reports on ASCO findings will be featured in our next issue, in July, as well as in the June issue of our sister publication, The International Journal of Targeted Therapies in Cancer.
Thank you for reading.
Peter Ciszewski
Key Targeted Therapy Trials From ASCO 2013
Follow us!
The content contained in this publication is for general information purposes only. The reader is encouraged to confirm the information presented with other sources. Targeted Therapy News makes no representations or warranties of any kind about the completeness, ac-curacy, timeliness, reliability, or suitability of any of the information, including content or advertisements, contained in this publication and expressly disclaims liability for any errors and omissions that may be presented in this publication. Targeted Therapy News reserves the right to alter or correct any error or omission in the information it provides in this publication, without any obligations. Targeted Therapy News further disclaims any and all liability for any direct, indirect, consequential, special, exemplary, or other damages arising from the use or misuse of any material or information presented in this publication. The views expressed in this publication are those of the authors and do not necessarily reflect the opinion or policy of Targeted Therapy News.
From the Publisher 5
©2013DendreonCorporation. Allrightsreserved.January2013. Printed in the U.S.A. Dendreon, the Dendreon logo, and PROVENGE are registered trademarks of Dendreon Corporation.P-A-01.13-002.00
Cerebrovascular Events. In controlled clinical trials, cerebrovascular events, including hemorrhagic and ischemic strokes, were reported in 3.5% of patients in the PROVENGE group compared with 2.6% of patients in the control group.
(See Adverse Reactions [6] of full Prescribing Information.)
To report SUSPECTED ADVERSE REACTIONS, contact Dendreon Corporation at 1-877-336-3736 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Table 1 Incidence of Adverse Events Occurring in ≥5% of Patients Randomized to PROVENGE
HypertensionAnorexiaBone painUpper respiratory tract infectionInsomniaMusculoskeletal chest painCoughNeck painWeight decreasedUrinary tract infectionRashSweatingTremor
45 (7.5)39(6.5)38(6.3)38(6.3)
37 (6.2)36(6.0)
35(5.8)34 (5.7)34 (5.7)33 (5.5)31 (5.2)30(5.0)30(5.0)
3(0.5)1(0.2)4(0.7)0(0.0)
0(0.0)2(0.3)
0(0.0)3(0.5)2(0.3)1(0.2)0(0.0)1(0.2)0(0.0)
14 (4.6)33(10.9)
22 (7.3)18(5.9)
22 (7.3)23 (7.6)
17 (5.6)14 (4.6)24(7.9)18(5.9)10(3.3)3(1.0)9(3.0)
0(0.0)3(1.0)3(1.0)0(0.0)
1(0.3)2(0.7)
0(0.0)2(0.7)1(0.3)2(0.7)0(0.0)0(0.0)0(0.0)
All Gradesn (%)
All Gradesn (%)
Grade 3-5n (%)
Grade 3-5n (%)
PROVENGE (N = 601) Control* (N = 303)
*Control was non-activated autologous peripheral blood mononuclear cells.
Dendreon Corporation Seattle, Washington 98101
REFERENCES: 1. PROVENGE[packageinsert].DendreonCorporation;June2011. 2. Kantoff PW, Higano CS, Shore ND, et al; for the IMPACT Study Investigators. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med.2010;363:411-422.
PROF35855_ProvengeAd_TarTherNews_DR2.indd 3 3/8/13 11:13 AM

Editorial Board6
Targeted Therapy News • 5.13
Jame Abraham, MDSection of Hematology/OncologyMary Babb Randolph Cancer CenterWest Virginia UniversityMorgantown, WV
ross Abrams, MDDepartment of Radiation OncologyRush University Medical CenterChicago, IL
Alex A. Adjei, MD, PhDDepartment of MedicineRoswell Park Cancer InstituteBuffalo, NY
lawrence Afrin, MDDivision of Hematology/OncologyMedical University of South CarolinaCharleston, SC
Sanjiv S. Agarwala, MDDivision of Oncology/HematologySt. Luke’s Hospital & Health NetworkBethlehem, PA
nita Ahuja, MDSurgery & OncologyThe Johns Hopkins HospitalBaltimore, MD
lowell Anthony, MDSection of Hematology & OncologyLouisiana State UniversityNew Orleans, LA
David Artz, MD, MBAInformation Systems Memorial Sloan-Kettering Cancer CenterNew York, NY
J. robert Beck, MDFox Chase Cancer CenterPhiladelphia, PA
Tomasz Beer, MDProstate Cancer ProgramOregon Health & Science University Cancer InstitutePortland, OR
E. roy Berger, MDNorth Shore Hematology AssociatesEast Setauket, NY
ralph v. Boccia, MDCenter for Cancer and Blood DisordersBethesda, MD
Jeffrey Bumpous, MDDivision of Otolaryngology-HNS University of LouisvilleLouisville, KY
Barbara A. Burtness, MDHead and Neck Medical OncologyFox Chase Cancer CenterPhiladelphia, PA
John Caton Jr, MDMedical OncologyWillamette Valley Cancer CenterEugene, OR
Emily Chan, MD, PhDVanderbilt UniversityNashville, TN
helen Chan, MDGI Surgical OncologyLakeland Regional Cancer CenterLakeland, FL
Tarek Chidiac, MDMid-Ohio Oncology/Hematology Inc, dbaThe Mark H. Zangmeister CenterColumbus, OH
Patrick Wayne Cobb, MDHematology-Oncology Centers of the Northern RockiesBillings, MT
Ezra E. W. Cohen, MDSection of Hematology/OncologyUniversity of ChicagoChicago, IL
richard Cohen, MDCohen Hufford Koltzova MedicalSan Francisco, CA
Allan Cohn, MDRocky Mountain Cancer CenterDenver, CO
Sandra Cuellar, PharmD, BCOPDepartment of Pharmacy PracticeUniversity of Illinois at ChicagoChicago, IL
Mary Daly, MD, PhDPopulation ScienceFox Chase Cancer CenterPhiladelphia, PA
Don Dizon, MDProgram in Women’s OncologyWomen & Infants HospitalProvidence, RI
habib Doss, MDTennessee Oncology, PLLCNashville, TN
Anthony Elias, MDBreast Cancer & Sarcoma ProgramsUniversity of Colorado Cancer CenterAurora, CO
Fadi Estephan, MDMedical OncologyHutchinson ClinicHutchinson, KS
Evelyn Fleming, MDGynecologic OncologyDartmouth-Hitchcock Medical CenterLebanon, NH
Michele Fox, MDPathologyMyeloma Institute for Research & TherapyUniversity of Arkansas for Medical SciencesLittle Rock, AR
Sharon l. Francz, BhA, BS, ONational Coalition of Oncology Nurse NavigatorsRockville, MD
David r. gandara, MDDivision of Hematology and OncologyUC Davis Cancer CenterSacramento, CA
leonard g. gomella, MDDepartment of UrologyThomas Jefferson UniversityPhiladelphia, PA
Andre goy, MD, MSJohn Theurer Cancer Center Hackensack University Medical CenterHackensack, NJ
David graham, MDClinical Trials Carle Clinic AssociationUrbana, IL
gregory griffin, MDDivision of Hematology/OncologyAlfred I. duPont Hospital for ChildrenWilmington, DE
reuben guerrero, MDDivision of Oncology/HematologyStraub Clinic & HospitalHonolulu, HI
Mahendra gupta, MDMedical OncologyInnovis HealthFargo, ND
Daniel hamstra, MD, PhDPediatric Radiation OncologyGenitourinary Radiation OncologyUniversity of MichiganAnn Arbor, MI
robin hanson, MD, PhDCardinal Kids Cancer CenterSt. John’s Mercy Medical CenterCreve Coeur, MO
roy S. herbst, MD, PhDDivision of Medical OncologyYale School of MedicineNew Haven, CT
William hocking, MDHematology/OncologyMarshfield ClinicMarshfield, WI
Clifford A. hudis, MDBreast Cancer Medicine ServicesMemorial Sloan-Kettering Cancer CenterNew York, NY
Dennie Jones, Jr, MDNew Mexico Cancer Care AllianceUniversity of New MexicoAlbuquerque, NM
Emad Kandil, MDDepartment of SurgerySection of Endocrine & Oncological SurgeryTulane Cancer CenterNew Orleans, LA
Song Kang, MDVirginia Oncology AssociatesSentara Careplex HospitalHampton, VA
gary lyman, MD, MPh, FrCP(Edin)Duke University Medical CenterDurham, NC
David g. Maloney, MD, PhDClinical Research DivisionFred Hutchinson Cancer Research CenterSeattle, WA
Maurie Markman, MDClinical Affairs & Medical Oncology Cancer Treatment Centers of AmericaPhiladelphia, PA
robert Meister, MDArlington-Fairfax HematologyArlington, VA
Wilson Mertens, MDCancer ServicesBaystate HealthSpringfield, MA
Joseph Mikhael, MDDivision of Hematology/OncologyDepartment of Internal MedicineMayo ClinicScottsdale, AZ
Mohamed Mitwally, MDDepartment of Obstetrics & Gynecology University of MinnesotaMinneapolis, MN
Janaki Moni, MDMichiana Hematology OncologySouth Bend, IN
hyman Muss, MDUniversity of Vermont and Vermont Cancer CenterHematology Oncology UnitBurlington, VT
leigh neumayer, MDIntegrated Breast ProgramHuntsman Cancer InstituteSalt Lake City, UT
Anthony nguyen, MDMedical OncologyComprehensive Cancer Centers of Nevada-SienaHenderson, NV
Joyce A. O’Shaughnessy, MDDivision of Breast Cancer ResearchTexas Oncology/US OncologyDallas, TX
Daniel A. Osman, MDBreast Cancer SurgeonMiami, FL
Andrew l. Pecora, MDJohn Theurer Cancer Center Hackensack University Medical CenterHackensack, NJ
Edith A. Perez, MDDepartment of Hematology/OncologyMayo ClinicJacksonville, FL
roman Perez-Soler, MDDivision of OncologyAlbert Einstein College of MedicineBronx, NY
Daniel P. Petrylak, MDGenitourinary Oncology SectionColumbia University Medical CenterNew York, NY
Aarati rao, MDDivision of Pediatric Hematology/OncologyUniversity of South AlabamaMobile, AL
Douglas reding, MD, MPhMarshfield CenterMarshfield, WI
John rhee, MDMedical Oncology & Hematology, PCYale-New Haven HospitalNew Haven, CT
Adam I. riker, MDCancer ServicesOchsner Cancer InstituteNew Orleans, LA
Steven rosen, MDRobert H. Lurie Comprehensive Cancer CenterNorthwestern UniversityChicago, IL
richard J. rosenbluth, MD John Theurer Cancer CenterHackensack University Medical CenterHackensack, NJ
Oliver Sartor, MDDepartment of UrologyTulane Cancer CenterNew Orleans, LA
lee Schwartzberg, MDThe West ClinicMemphis, TN
Maureen Sheehan, MDKansas City Cancer CenterKansas City, MO
Edibaldo Silva, MD, PhDDivision of Surgical OncologyEppley Cancer Center University of Nebraska Medical Center Omaha, NE
David Spigel, MD Lung Cancer ProgramThe Sarah Cannon Research InstituteNashville, TN Kellie Sprague, MDBone Marrow TransplantationTufts Medical CenterBoston, MA
richard Tenglin, MDOncology AssociatesRapid City Regional HospitalRapid City, SD
J. Tate Thigpen, MDDivision of Medical OncologyUniversity of MississippiJackson, MS
Katherine Tkaczuk, MDMedicine & Oncology University of Maryland Cancer CenterBaltimore, MD
Debu Tripathy, MDWomen’s Cancer ProgramUniversity of Southern CaliforniaLos Angeles, CA
Philip villiotte, MDSpectrum Medical GroupScarborough, ME
roland Walter, MD, PhDClinical Research DivisionFred Hutchinson Cancer Research Center Seattle, WA
ronald Walters, MD, MBA, MhAMedical Operations & InformaticsBreast Medical OncologyMD Anderson Cancer CenterHouston, TX
richard Wein, MDDepartment of Otolaryngology-Head & Neck SurgeryTufts Medical CenterBoston, MA
h. Jack West, MDThoracic Oncology ProgramSwedish Cancer InstituteSeattle, WA
James Wheeler, MDRadiation Oncology ProgramGoshen Center for Cancer CareGoshen, IN
Andrew D. Zelenetz, MD, PhDDepartment of MedicineMemorial Sloan-Kettering Cancer CenterNew York, NY
Paul Zeltzer, MDNeurosurgeryDavid Geffen School of MedicineUniversity of California, Los AngelesLos Angeles, CA
Jeffrey Zonder, MDHematology/OncologyKarmanos Cancer CenterDetroit, MI
HealthcareTargeted

News
Targeted Therapy News • 5.13
7
Biomarkers Still NeededBy Devera Pine
Targeted Therapies: Ovarian Cancer
Although a variety of biomarkers have been shown to correlate with survival in men with pros-
tate cancer, the use of biomarkers in the management of these patients may be dependent upon the clinical state and the class of drug evaluated. Speaking at the 6th Annual Interdisciplinary Pros-tate Cancer Congress, held in New York City on March 16, Daniel P. Petrylak, MD, director of the Genitourinary Oncology Program at Yale Cancer Center in New Haven, Connecticut, re-viewed the evidence for biomarkers to date. “There is nothing at this point that has fallen out as absolutely prognostic or predictive in an in-dividual situation,” he said.
One area of interest is the prognostic value of promoter methylation of genes associated with various parameters of prostate cancer progres-sion.1,2 Henrique et al evaluated methylation of APC, CCND2, GSTP1, RARB2, and RASSF1A as biomarkers for prognosis.2 High-level methylation of APC was the only epigenetic event significantly associated with a worse disease-free or disease-specific sur-vival. There was a trend toward worse outcome in patients treated with andro-gen-deprivation therapy (ADT) who had APC hypermethylation (P=.079). APC
hypermethylation was associated with a shorter time to biochemical relapse (disease-free survival) in patients treat-ed with prostatectomy (P=.043), but not in patients treated with external-beam radiation therapy or ADT.
Okegawa et al assessed whether cir-culating tumor cells (CTCs) with tumor-related methylated DNA could be used to predict survival in patients with hor-mone-refractory prostate cancer.3 The researchers analyzed blood samples
from 76 patients; CTC evaluations occurred 3.5 to 78.5 months after the initial diagnosis. Serum DNA methylation status was assessed for APC, GSTP1, RASSF1A, MDR1, and PTGS2.
A total of 47 patients (62%) had 5 or more CTCs and a median overall survival (OS) of 12 months compared with 26 months for pa-tients with fewer than 5 CTCs (P<.001). The pres-ence of 5 or more CTCs was significantly cor-
related with the detection of 1 or more methylated loci (P <.001). The median OS for patients with methylated DNA was 12 months versus 48 months or more for patients without methylated DNA (P <.001).
Posttreatment CTC levels were shown to predict OS in a study of 231 patients with progressive CRPC4; data from the
study led to FDA approval of the Cell-Search assay. However, in his talk, Pet-rylak said that although CTCs are use-ful for predicting treatment response or survival with cytotoxic and hormonal therapies, about half of patients do not have detectable CTC levels by current detection methods. More-sensitive CTC detection techniques are needed, he said.
The TMPRSS2-ERG gene fusion, which is present in approximately half of new-ly diagnosed prostate cancer cases, has also been investigated as a biomarker, though the clinicopathologic impact of the fusion is not clear, Petrylak said. Dif-ferent subtypes of TMPRSS2-ERG have been detected, and the Edel subtype may represent a more lethal genotype, susceptible to higher recurrence, more likely to evolve to CRPC and to progress to metastasis.5 A role has been postu-lated for TMPRSS2-ERG as a predictive biomarker for sensitivity to abiraterone acetate; however, a phase II trial found that the fusion has a limited role in this area.6
In summary, Petrylak said, although a variety of biomarkers correlate with survival, none are “ready for prime time.” However, he said, research on biomarkers should be an element in all subsequent phase III trials. TTN
1. Roupret M, Hupertan V, Catto JW, et al. Pro-
moter hypermethylation in circulating blood cells
identifies prostate cancer progression. Int J Can-cer. 2008;122(4):952-956.
2. Henrique R, Ribeiro FR, Fonseca D, et al. High
promoter methylation levels of APC predict poor
prognosis in sextant biopsies from prostate can-
cer patients. Clin Cancer Res. 2007;13(20):6122-
6129.
3. Okegawa T, Nutahara K, Higashihara E. Associ-
ation of circulating tumor cells with tumor-related
methylated DNA in patients with hormone-refrac-
tory prostate cancer. Int J Urol. 2010;17(5):466-
475.
4. de Bono JS, Scher HI, Montgomery RB, et al. Cir-
culating tumor cells predict survival benefit from
treatment in metastatic castration-resistant pros-
tate cancer. Clin Cancer Res. 2008;14(19):6302-
6309.
5. Mehra R, Tomlins SA, Yu J, et al. Character-
ization of TMPRSS2-ETS gene aberrations in an-
drogen-independent metastatic prostate cancer. Cancer Res. 2008;68(10):3584-3590.
6. Danila DC, Anand A, Sung CC, et al. TMPRSS2-
ERG status in circulating tumor cells as a predic-
tive biomarker of sensitivity in castration-resistant
prostate cancer patients treated with abiraterone
acetate. Eur Urol. 2011;60(5):897-904.
Daniel P. Petrylak, MD
Key Points:
• Use of biomarkers in the management of prostate cancer may be dependent upon the clinical state and the class of drug evaluated
• Approximately half of patients do not have detectable CTC levels by current detection methods
• Research on biomarkers should be an element in phase III trials
Possible Mechanism of Platinum Resistance in Ovarian Cancer IdentifiedBy Ben Leach
Researchers have determined that the P-type ATPase membrane pro-tein ATP11B may play a role in cis-
platin resistance in ovarian cancer and propose that inhibition of ATP11B expres-sion could help overcome cisplatin resis-tance. The research was published online by The Journal of Clinical Investigation.
Although platinum-based chemo-therapy is a standard of care across many tumor types, eventually, patients develop primary or acquired resistance to these drugs. This can be caused by reduced platinum uptake and increased platinum export, which in turn limit the extent of the DNA damage that the
chemotherapy causes. Patients with platinum-resistant ovarian cancer have a poor prognosis and few treatment op-tions, with only about 10% to 15% of patients responding to treatment with therapies such as paclitaxel, pegylated liposomal doxorubicin (PLD), and topo-tecan.
In searching for candidate genes that could cause cisplatin resistance, researchers found that expression of ATP11B was markedly increased in cis-platin-resistant cells. After examining 111 ovarian cancer specimens and 10 normal ovarian surface epithelial cell specimens, the researchers determined
Targeted Therapies: Prostate Cancer

that there was a significant relation-ship between higher tumor stage and ATP11B expression (P = .04). High ATP11B expression was also associated with worse overall survival compared with low ATP11B expression, with a median overall survival of 2.75 years in those with high expression compared with 9.25 years in those with low expression (P < .001).
To determine whether any effect was observed if ATP11B expression was lowered, the researchers examined the effect of ATP11B silencing in vitro and
found that it restored the sensitivity of ovarian cancer cells to cisplatin. When this was tested in mice, the mice with ATP11B-silenced RNA showed signifi-cant decreases in cell proliferation and higher apoptotic rates. The researchers also determined that ATP11B enhances the export of cisplatin from cells, sug-gesting that the protein contributes to the secretory vesicular transport of cis-platin from Golgi to the plasma mem-brane.
“Collectively, our data demonstrate that overexpression of ATP11B confers
cisplatin resistance in ovarian cancer cells by enhancing the efflux of cisplatin via the vesicular secretory pathway,” the authors wrote. “On the basis of these findings, ATP11B appears to be an im-portant target for overcoming cisplatin resistance.” TTN
Moreno-Smith M, Halder JB, Meltzer PS, et al.
ATP11B mediates platinum resistance in ovarian
cancer [published online ahead of print April 15,
2013]. J Clin Invest. doi:10.1172/JCI65425.
Targeted Therapies: Ovarian Cancer
Targeted Therapies: Genetic Research
An analysis of metabolic gene ex-pression patterns in 22 human tumors types identified multiple
metabolic expression changes associ-ated with cancer, as well as hundreds of potential drug targets for disrupting the fuel supply of tumors or interrupting the synthesis of essential building blocks. The study, conducted at Columbia Uni-versity Medical Center (CUMC), was pub-lished online in Nature Biotechnology.
“The importance of this new study is its scope,” said Dennis Vitkup, PhD,
associate professor of Biomedical In-formatics at CUMC and the study’s lead investigator, in a state-ment. “So far, people have focused mainly on a few genes involved in major metabolic pro-cesses. Our study pro-vides a comprehensive, global view of diverse metabolic alterations at the level of gene expression.”
A fundamental change in me-tabolism is one of the emerg-ing hallmarks of cancer. How-ever, researchers do not yet know how the expres-sion of metabolic genes differs in cancerous versus normal cells, or whether meta-bolic changes are the same across tumor types. The CUMC team aimed to identify metabolic pro-gramming differ-ences.
The analysis found multiple meta-bolic expression changes in tumors.
Some of the changes, in-cluding upregulation of nucleotide biosynthesis and glycolysis, were fre-quently found across tu-mor types. Others, such as expression changes in oxidative phosphory-lation, were heteroge-neous.
“Our study clearly demonstrates that there are no single and uni-versal changes in cancer metabolism,” said Mat-thew Vander Heiden, MD, PhD, assistant pro-
fessor at the Massachusetts Institute of Technology and a coauthor, in a state-ment.
In some cases, the researchers found that gene expression changes worked with cancer mutations, driving tumor formation. For instance, in several cancer types, including acute myeloid leukemia, mutations in the isocitrate dehydrogenase enzyme produces 2-hy-droxyglutarate, a metabolite that pro-motes tumor growth. The researchers found that in tumors with recurrent mutations, isocitrate dehydrogenase expression was significantly increased, leading to overproduction of 2-hydroxy- glutarate.
The analysis also identified hun-dreds of metabolic isoenzymes with significant and tumor-specific expres-sion changes that could potentially be targeted for anticancer therapy. For
example, in kidney and liver cancers, a quick-acting aldolase isoenzyme was more prevalent than the slow-moving version found in normal kidney and liver tissue. This quick-acting version is suitable for fast cell proliferation and tumor growth. Prior to the study, a few isoenzyme expression discrepancies were known, but this research identi-fied hundreds more.
“Inhibiting specific isoenzymes in tumors may be a way to selectively hit cancer cells without affecting normal cells, which could get by with other isoenzymes,” said Jie Hu, PhD, a post-doctoral researcher at CUMC and co-author, in a statement. TTN
Hu J, Locasale JW, Bielas JH, et al. Heterogene-
ity of tumor-induced gene expression changes in
the human metabolic network [published online
ahead of print. April 21, 2013]. Nature Biotech-nol. doi:10.1038/nbt.2530.
Metabolic Gene Expression Altered in Cancer, Providing Potential Drug TargetsBy Andrew J. Roth
Key Points:
• An analysis of metabolic gene expression patterns in 22 human tumors types identified multiple metabolic expression changes associated with cancer
• There were no single and universal changes in cancer metabolism
• The analysis also identified hundreds of metabolic isoenzymes with significant and tumor-specific expression changes that could potentially be targeted for anticancer therapy
Key Points:
• P-type ATPase membrane protein ATP11B may play a role in cisplatin resistance in ovarian cancer
• Silencing ATP11B in vitro restored the sensitivity of ovarian cancer cells to cisplatin
• Inhibition of ATP11B expression could help overcome cisplatin resistance
Dennis Vitkup, PhD
News8
Targeted Therapy News • 5.13
Imag
e pr
ovid
ed b
y D
r. V
itkup
Global mapping of cancer gene expression changes to the human metabolic network; increased enzymatic expression in red; decreased in blue.

News
Targeted Therapy News • 5.13
9
Imag
e pr
ovid
ed b
y D
r. V
itkup
Follicular lymphoma (FL) is char-acterized by repeated treatment responses and then relapses, and
until more effective frontline therapies become available, researchers will need to generate a growing list of drug choic-es to keep pace with patients’ needs, according to Bruce D. Cheson, MD, of the Lombardi Comprehensive Cancer Center at Georgetown University, Wash-ington, DC, and chair of the Lymphoma Committee of the Alliance for Clinical Trials in Oncology/Cancer and Leuke-mia Group B (CALGB).
Cheson, who spoke at the 17th An-nual International Con-gress on Hematologic Malignancies, held in February in New York City, noted that although there are no new che-motherapy drugs in de-velopment for FL, work is being done to bring other classes of agents into the treatment ar-mamentarium—partic-ularly monoclonal anti-bodies, signaling path-way-targeting agents, a p o p t o s i s - i n d u c i n g compounds, and immunomodulatory drugs.
Rituximab, a monoclonal antibody approved to treat FL, will soon go off patent, but other anti-CD20 antibod-ies are in development, Cheson said. However, to have value, he noted, such drugs will need to be more effective than rituximab or work in rituximab-resistant disease.
Ofatumumab, a novel humanized monoclonal anti-CD20 antibody that is approved for use in chronic lympho-cytic leukemia (CLL), has shown some promise as a single agent in patients with rituximab-resistant FL. In a multi-center study of patients with rituximab-refractory FL (N=116), ofatumumab was well tolerated and modestly active.1 In the study, 27 patients had an over-all response rate (ORR) of 22% to the antibody. For all participants, median progression-free survival (PFS) was 5.8 months. PFS jumped to 9.1 months in the 46% of patients who demonstrated tumor reduction 3 months after the start of therapy.
Cheson said “the jury is still out” on
antibody GA101, which was tested in patients with relapsed FL, and gener-ated response rates and PFS results similar to those associated with ritux-imab.2,3 “Whether that will go anywhere remains to be demonstrated by the on-going trial of [alkylating agent] benda-mustine with or without GA101 in ritux-imab-refractory patients,4” he said.
Meanwhile, two antibody drug con-jugates that showed promise in phase I trials—DCDT2980S, an anti-CD22 agent, and DCDS4501A, an anti-CD79b agent—are being tested in a randomized phase II study.5 Investigators are combining
either of the drugs with rituximab in patients with FL and diffuse large B-cell lymphoma, and are allowing crossover at progression to check for non–cross-resistance between the two mol-ecules, Cheson said.
Also on tap is a phase II study of ibrutinib, a specific and irrevers-ible inhibitor of Bruton’s tyrosine kinase that demonstrated an ORR of about 40% in patients
with FL in an earlier study, Cheson said. The pill-a-day regimen has been suc-cessful for as long as 2 years in patients with relapsed or refractory FL, he said, and the trial will shed more light on the drug’s toxicity and response rate and duration.6
Another promising development is idelalisib (GS-1101), a delta isoform-specific PI3 kinase inhibitor, Cheson said. In a single-agent, phase I trial, 59% of heavily pretreated patients with in-dolent non-Hodgkin lymphoma (iNHL) subtypes responded to a dosage of 100 mg or more of the drug twice a day.7 The drug’s tolerability was “ex-ceptional,” Cheson said. Grade 3-4 ad-verse events occurring in 5% or more of patients and due to any cause were neutropenia (9%), lymphopenia (5%), and thrombocytopenia (5%) with uncer-tain relationship to the study drug. No pattern of drug-related symptomatic adverse events was seen.
A separate phase I trial combined ide-lalisib with rituximab, bendamustine, or a combination of the two in previously treated patients with iNHL.8 All com-
binations resulted in “profound reduc-tions” in lymphadenopathy. The ORR in the intent-to-treat group was 77% to 85% with any regimen, and the PFS at 1 year was 78% to 90% with any regimen. There were no overlapping toxicities with the drugs. The results indicate that “maybe you don’t need the chemother-apy after all,” Cheson said.
Due to some data indicating that si-multaneously inhibiting two pathways may lead to better results, agents in-cluding PI3K/mTOR inhibitors and del-ta/gamma inhibitors are being investi-gated, Cheson said.
In the arena of apoptosis-inducing drugs, Cheson mentioned six agents in development, including ABT-199, which induces cancer cell death by targeting BCL-2. In an early study, 4 of 5 patients with FL had a partial response to the drug, but the agent may work better if combined with another treatment, Che-son pointed out.9
Cheson was part of the CALGB team that conducted study 50401 of the im-munomodulatory drug lenalidomide, with or without rituximab, in patients whose FL had relapsed after one or more rituximab-based regimens.10 The ORR was 72.7% in the experimental arm versus 51.1% in the control arm. The complete response rate was 36.4% for the experimental arm versus 13.3% for the control arm; the partial response rate was 36.4% versus 37.8%, respective-ly; and the 2-year event-free survival was 44% versus 27%, respectively.
While there was “no real difference in overall survival,” Cheson noted that some “astounding” results came out of a phase II study of lenalidomide and rituximab in untreated indolent lym-phoma, conducted by Fowler et al.11 In 46 patients with FL, the ORR was 98%, with 87% of those responses complete. PFS was 89% at 36 months, and the tox-icity profile was mild, with manageable hematologic side effects.
“This has the potential to totally change the way we approach follicular lymphoma,” Cheson said.
Those results led to the randomized, phase III RELEVANCE trial,12 which is testing rituximab and lenalidomide against rituximab and any of several chemotherapy regimens, Cheson said. The study is scheduled to continue through 2024.
Pending CALGB trials include a study testing rituximab and lenalidomide plus ibrutinib in untreated follicular NHL, and another testing rituximab and lenalidomide plus idelalisib in relapsed or refractory follicular NHL after at least one anti-CD20-based regimen.
Looking ahead, challenges will in-volve determining how to develop ratio-nal combinations of new drugs, choos-ing appropriate endpoints for clinical trials, and figuring out who will pay for studies, Cheson said.
“We need to recognize the heteroge-neity of lymphomas and do correlative studies to figure out which drugs and combinations will most likely benefit each individual patient,” he said, add-ing that it is important to enroll eligible patients in trials to support research efforts. TTN
1. Czuczman MS, Fayad L, Delwail V, et al. Ofatu-
mumab monotherapy in rituximab-refractory follic-
ular lymphoma: results from a multicenter study.
Blood. 2012;119(16):3698-3704.
2. Salles GA, Morschhauser F, Thieblemont C, et
al. Efficacy and safety of obinutuzumab (GA101)
monotherapy in relapsed/refractory indolent non-
Hodgkin’s lymphoma: results from a phase I/II
study (BO20999). Presented at the 53rd Annual
Meeting and Exposition of the American Society of
Hematology; December 10-13, 2011; San Diego,
CA. Blood. 2011;118(suppl; abstr 268).
3. Sehn LH, Goy A, Offner FC, et al. Random-
ized phase II trial comparing GA101 (obinutu-
zumab) with rituximab in patients with relapsed
CD20+ indolent B-cell non-Hodgkin lymphoma:
preliminary analysis of the GAUSS study. Blood. 2011;118(suppl; abstr 269).
4. Clinical Trials Identifier NCT01059630. www.
clinicaltrials.gov.
Numerous Drug Classes Studied for Use in Follicular and Other LymphomasBy Beth Fand Incollingo
Targeted Therapies: Hematologic Malignancies
Key Points:
• Ofatumumab, a novel humanized monoclonal anti-CD20 antibody, has shown promise as a single agent therapy for rituximab-resistant FL
• In NHL, pending trials include a study of rituximab and lenalidomide plus ibrutinib in untreated follicular NHL, and another testing rituximab and lenalidomide plus idelalisib in relapsed or refractory follicular NHL
Bruce D. Cheson, MD

JAK targeted to make a difference
Percent Change in Total Symptom Score (TSS) in Individual Patients From Baseline to Week 24 or Last Observation1,a,b
150
100
50
0
-50
-100
Ch
ang
e Fr
om
Bas
elin
e (%
)
IMP
RO
VE
ME
NT
WO
RS
EN
ING
50% Improvement
Upper 50th Percentile Upper 50th Percentile
Placebo (n = 145)Jaka� (n = 145)
Upper 50th Percentile Upper 50th Percentile
Placebo (n = 153)Jaka� (n = 155)
80
60
40
20
0
-20
-40
-60
-80
Ch
ang
e Fr
om
Bas
elin
e (%
)
Percent Change in Spleen Volume in Individual Patients From Baseline to Week 24 or Last Observation1,a
IMP
RO
VE
ME
NT
WO
RS
EN
ING
35% Reduction
Jaka� ® (JAK-ah-fye)—First and Only FDA-Approved Agent for MYELOFIBROSIS (MF)*
JAK2
JAK1
* Intermediate or high-risk MF.
REDUCEsplenomegaly and symptoms of MF
REGULATEJAK signalingJAK signaling
References: 1. Jaka� Prescribing Information. Incyte Corporation. June 2012. 2. Verstovsek S, Mesa RA, Gotlib J, et al. N Engl J Med. 2012;366:799-807.
Jaka� is a registered trademark of Incyte Corporation.© 2012, Incyte Corporation. All rights reserved. RUX-1160C 07/12
Indications and UsageJaka� is indicated for treatment of patients with intermediate or high-risk myelo� brosis, including primary myelo� brosis, post–polycythemia vera myelo� brosis and post–essential thrombocythemia myelo� brosis.
Important Safety Information• Treatment with Jakafi can cause hematologic adverse reactions,
including thrombocytopenia, anemia and neutropenia, which are each dose-related effects, with the most frequent being thrombocytopenia and anemia. A complete blood count must be performed before initiating therapy with Jaka� . Complete blood counts should be monitored as clinically indicated and dosing adjusted as required
Please see Brief Summary of Full Prescribing Information on the following page.
• The three most frequent non-hematologic adverse reactions were bruising, dizziness and headache
• Patients with platelet counts <200 × 109/L at the start of therapy are more likely to develop thrombocytopenia during treatment. Thrombocytopenia was generally reversible and was usually managed by reducing the dose or temporarily withholding Jaka� . If clinically indicated, platelet transfusions may be administered
• Patients developing anemia may require blood transfusions. Dose modi� cations of Jaka� for patients developing anemia may also be considered
• Neutropenia (ANC <0.5 × 109/L) was generally reversible and was managed by temporarily withholding Jaka�
• Patients should be assessed for the risk of developing serious bacterial, mycobacterial, fungal and viral infections. Active serious infections should have resolved before starting Jaka� . Physicians should carefully observe patients receiving Jakafi for signs and symptoms of infection (including herpes zoster)
and initiate appropriate treatment promptly• A dose modifi cation is recommended when administering Jakafi
with strong CYP3A4 inhibitors or in patients with renal or hepatic impairment [see Dosage and Administration]. Patients should be closely monitored and the dose titrated based on safety and ef� cacy
• There are no adequate and well-controlled studies of Jakafi in pregnant women. Use of Jaka� during pregnancy is not recommended and should only be used if the potential bene� t justi� es the potential risk to the fetus
• Women taking Jakafi should not breast-feed. Discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother
a As studied in COMFORT-I, a randomized, double-blind, placebo-controlled phase III study with 309 total patients (United States, Canada, Australia). The primary endpoint was the proportion of subjects achieving a ≥35% reduction in spleen volume from baseline to Week 24 as measured by magnetic resonance imaging (MRI) or computed tomography (CT) . A secondary endpoint was the proportion of subjects with a ≥50% reduction in TSS from baseline to Week 24 as measured by the daily patient diary, the modi� ed Myelo� brosis Symptom Assessment Form (MFSAF v2.0).1,2
b Symptom scores were captured by a daily patient diary recorded for 25 weeks. TSS encompasses debilitating symptoms of MF: abdominal discomfort, early satiety, pain under left ribs, pruritus, night sweats and bone/muscle pain. Symptom scores ranged from 0 to 10 with 0 representing symptoms “absent” and 10 representing “worst imaginable” symptoms. These scores were added to create the daily total score, which has a maximum of 60. At baseline, mean TSS was 18.0 in the Jaka� group and 16.5 in the placebo group.1,2
Jaka�
At Week 24, signi� cantly more patients receiving Jaka� vs placebo had
— A ≥35% reduction in spleen volume (41.9% vs 0.7%, respectively; P < 0.0001)1,2,a
— A ≥50% improvement in TSS (45.9% vs 5.3%, respectively; P < 0.0001)1,2,a,b
Reductions in spleen volume and improvements in TSS were seen with Jaka� in both JAK2V617F-positive patients and JAK2V617F-negative patients, relative to placebo2
Visit www.jaka� .com/explorefor more information on Jaka� and MF, plus valuable educational resources.
Jaka� demonstrated superior reductions in spleen volume andimprovements in symptom scores at Week 241,2,a,b
In these charts, each bar represents an individual patient’s response. Worsening of TSS is truncated at 150%.
74240ha_d.indd 1 7/30/12 4:42 PM

JAK targeted to make a difference
Percent Change in Total Symptom Score (TSS) in Individual Patients From Baseline to Week 24 or Last Observation1,a,b
150
100
50
0
-50
-100
Ch
ang
e Fr
om
Bas
elin
e (%
)
IMP
RO
VE
ME
NT
WO
RS
EN
ING
50% Improvement
Upper 50th Percentile Upper 50th Percentile
Placebo (n = 145)Jaka� (n = 145)
Upper 50th Percentile Upper 50th Percentile
Placebo (n = 153)Jaka� (n = 155)
80
60
40
20
0
-20
-40
-60
-80
Ch
ang
e Fr
om
Bas
elin
e (%
)
Percent Change in Spleen Volume in Individual Patients From Baseline to Week 24 or Last Observation1,a
IMP
RO
VE
ME
NT
WO
RS
EN
ING
35% Reduction
Jaka� ® (JAK-ah-fye)—First and Only FDA-Approved Agent for MYELOFIBROSIS (MF)*
JAK2
JAK1
* Intermediate or high-risk MF.
REDUCEsplenomegaly and symptoms of MF
REGULATEJAK signalingJAK signaling
References: 1. Jaka� Prescribing Information. Incyte Corporation. June 2012. 2. Verstovsek S, Mesa RA, Gotlib J, et al. N Engl J Med. 2012;366:799-807.
Jaka� is a registered trademark of Incyte Corporation.© 2012, Incyte Corporation. All rights reserved. RUX-1160C 07/12
Indications and UsageJaka� is indicated for treatment of patients with intermediate or high-risk myelo� brosis, including primary myelo� brosis, post–polycythemia vera myelo� brosis and post–essential thrombocythemia myelo� brosis.
Important Safety Information• Treatment with Jakafi can cause hematologic adverse reactions,
including thrombocytopenia, anemia and neutropenia, which are each dose-related effects, with the most frequent being thrombocytopenia and anemia. A complete blood count must be performed before initiating therapy with Jaka� . Complete blood counts should be monitored as clinically indicated and dosing adjusted as required
Please see Brief Summary of Full Prescribing Information on the following page.
• The three most frequent non-hematologic adverse reactions were bruising, dizziness and headache
• Patients with platelet counts <200 × 109/L at the start of therapy are more likely to develop thrombocytopenia during treatment. Thrombocytopenia was generally reversible and was usually managed by reducing the dose or temporarily withholding Jaka� . If clinically indicated, platelet transfusions may be administered
• Patients developing anemia may require blood transfusions. Dose modi� cations of Jaka� for patients developing anemia may also be considered
• Neutropenia (ANC <0.5 × 109/L) was generally reversible and was managed by temporarily withholding Jaka�
• Patients should be assessed for the risk of developing serious bacterial, mycobacterial, fungal and viral infections. Active serious infections should have resolved before starting Jaka� . Physicians should carefully observe patients receiving Jakafi for signs and symptoms of infection (including herpes zoster)
and initiate appropriate treatment promptly• A dose modifi cation is recommended when administering Jakafi
with strong CYP3A4 inhibitors or in patients with renal or hepatic impairment [see Dosage and Administration]. Patients should be closely monitored and the dose titrated based on safety and ef� cacy
• There are no adequate and well-controlled studies of Jakafi in pregnant women. Use of Jaka� during pregnancy is not recommended and should only be used if the potential bene� t justi� es the potential risk to the fetus
• Women taking Jakafi should not breast-feed. Discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother
a As studied in COMFORT-I, a randomized, double-blind, placebo-controlled phase III study with 309 total patients (United States, Canada, Australia). The primary endpoint was the proportion of subjects achieving a ≥35% reduction in spleen volume from baseline to Week 24 as measured by magnetic resonance imaging (MRI) or computed tomography (CT) . A secondary endpoint was the proportion of subjects with a ≥50% reduction in TSS from baseline to Week 24 as measured by the daily patient diary, the modi� ed Myelo� brosis Symptom Assessment Form (MFSAF v2.0).1,2
b Symptom scores were captured by a daily patient diary recorded for 25 weeks. TSS encompasses debilitating symptoms of MF: abdominal discomfort, early satiety, pain under left ribs, pruritus, night sweats and bone/muscle pain. Symptom scores ranged from 0 to 10 with 0 representing symptoms “absent” and 10 representing “worst imaginable” symptoms. These scores were added to create the daily total score, which has a maximum of 60. At baseline, mean TSS was 18.0 in the Jaka� group and 16.5 in the placebo group.1,2
Jaka�
At Week 24, signi� cantly more patients receiving Jaka� vs placebo had
— A ≥35% reduction in spleen volume (41.9% vs 0.7%, respectively; P < 0.0001)1,2,a
— A ≥50% improvement in TSS (45.9% vs 5.3%, respectively; P < 0.0001)1,2,a,b
Reductions in spleen volume and improvements in TSS were seen with Jaka� in both JAK2V617F-positive patients and JAK2V617F-negative patients, relative to placebo2
Visit www.jaka� .com/explorefor more information on Jaka� and MF, plus valuable educational resources.
Jaka� demonstrated superior reductions in spleen volume andimprovements in symptom scores at Week 241,2,a,b
In these charts, each bar represents an individual patient’s response. Worsening of TSS is truncated at 150%.
74240ha_d.indd 1 7/30/12 4:42 PM

Table 2: Worst Hematology Laboratory Abnormalities in the Placebo-controlled Studya
Jakafi Placebo (N=155) (N=151)Laboratory All All Parameter Gradesb Grade 3 Grade 4 Grades Grade 3 Grade 4 (%) (%) (%) (%) (%) (%)Thrombocytopenia 69.7 9.0 3.9 30.5 1.3 0Anemia 96.1 34.2 11.0 86.8 15.9 3.3Neutropenia 18.7 5.2 1.9 4.0 0.7 1.3
a Presented values are worst Grade values regardless of baselineb National Cancer Institute Common Terminology Criteria for Adverse Events, version 3.0Additional Data from the Placebo-controlled Study 25.2% of patients treated with Jakafi and 7.3% ofpatients treated with placebo developed newly occurring or worsening Grade 1 abnormalities in alanine trans-aminase (ALT). The incidence of greater than or equal to Grade 2 elevations was 1.9% for Jakafi with 1.3%Grade 3 and no Grade 4 ALT elevations. 17.4% of patients treated with Jakafi and 6.0% of patients treatedwith placebo developed newly occurring or worsening Grade 1 abnormalities in aspartate transaminase(AST). The incidence of Grade 2 AST elevations was 0.6% for Jakafi with no Grade 3 or 4 AST elevations.16.8% of patients treated with Jakafi and 0.7% of patients treated with placebo developed newly occurring orworsening Grade 1 elevations in cholesterol. The incidence of Grade 2 cholesterol elevations was 0.6% forJakafi with no Grade 3 or 4 cholesterol elevations.DRUG INTERACTIONS Drugs That Inhibit or Induce Cytochrome P450 Enzymes Ruxolitinibis predominantly metabolized by CYP3A4. Strong CYP3A4 inhibitors: The Cmax and AUC of ruxolitinibincreased 33% and 91%, respectively, with Jakafi administration (10 mg single dose) following ketoconazole200 mg twice daily for four days, compared to receiving Jakafi alone in healthy subjects. The half-life was alsoprolonged from 3.7 to 6.0 hours with concurrent use of ketoconazole. The change in the pharmacodynamicmarker, pSTAT3 inhibition, was consistent with the corresponding ruxolitinib AUC following concurrent admin-istration with ketoconazole. When administering Jakafi with strong CYP3A4 inhibitors a dose reduction isrecommended [see Dosage and Administration (2.4) in Full Prescribing Information]. Patients should beclosely monitored and the dose titrated based on safety and efficacy. Mild or moderate CYP3A4 inhibitors:There was an 8% and 27% increase in the Cmax and AUC of ruxolitinib, respectively, with Jakafi administration(10 mg single dose) following erythromycin, a moderate CYP3A4 inhibitor, at 500 mg twice daily for 4 days,compared to receiving Jakafi alone in healthy subjects. The change in the pharmacodynamic marker, pSTAT3inhibition was consistent with the corresponding exposure information. No dose adjustment is recommendedwhen Jakafi is coadministered with mild or moderate CYP3A4 inhibitors (eg, erythromycin). CYP3A4inducers: The Cmax and AUC of ruxolitinib decreased 32% and 61%, respectively, with Jakafi administration(50 mg single dose) following rifampin 600 mg once daily for 10 days, compared to receiving Jakafi alone inhealthy subjects. In addition, the relative exposure to ruxolitinib’s active metabolites increased approximately100%. This increase may partially explain the reported disproportionate 10% reduction in the pharmaco-dynamic marker pSTAT3 inhibition. No dose adjustment is recommended when Jakafi is coadministered witha CYP3A4 inducer. Patients should be closely monitored and the dose titrated based on safety and efficacy.USE IN SPECIFIC POPULATIONS Pregnancy Pregnancy Category C: There are no adequate and well-controlled studies of Jakafi in pregnant women. In embryofetal toxicity studies, treatment withruxolitinib resulted in an increase in late resorptions and reduced fetal weights at maternally toxic doses.Jakafi should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.Ruxolitinib was administered orally to pregnant rats or rabbits during the period of organogenesis, at dosesof 15, 30 or 60 mg/kg/day in rats and 10, 30 or 60 mg/kg/day in rabbits. There was no evidence of terato-genicity. However, decreases of approximately 9% in fetal weights were noted in rats at the highest andmaternally toxic dose of 60 mg/kg/day. This dose results in an exposure (AUC) that is approximately 2 timesthe clinical exposure at the maximum recommended dose of 25 mg twice daily. In rabbits, lower fetal weightsof approximately 8% and increased late resorptions were noted at the highest and maternally toxic dose of60 mg/kg/day. This dose is approximately 7% the clinical exposure at the maximum recommended dose. Ina pre- and post-natal development study in rats, pregnant animals were dosed with ruxolitinib from implan-tation through lactation at doses up to 30 mg/kg/day. There were no drug-related adverse findings in pups forfertility indices or for maternal or embryofetal survival, growth and development parameters at the highestdose evaluated (34% the clinical exposure at the maximum recommended dose of 25 mg twice daily).Nursing Mothers It is not known whether ruxolitinib is excreted in human milk. Ruxolitinib and/or itsmetabolites were excreted in the milk of lactating rats with a concentration that was 13-fold the maternalplasma. Because many drugs are excreted in human milk and because of the potential for serious adversereactions in nursing infants from Jakafi, a decision should be made to discontinue nursing or to discontinuethe drug, taking into account the importance of the drug to the mother. Pediatric Use The safety and effec-tiveness of Jakafi in pediatric patients have not been established. Geriatric Use Of the total number ofmyelofibrosis patients in clinical studies with Jakafi, 51.9% were 65 years of age and older. No overall differ-ences in safety or effectiveness of Jakafi were observed between these patients and younger patients. RenalImpairment The safety and pharmacokinetics of single dose Jakafi (25 mg) were evaluated in a study inhealthy subjects [CrCl 72-164 mL/min (N=8)] and in subjects with mild [CrCl 53-83 mL/min (N=8)],moderate [CrCl 38-57 mL/min (N=8)], or severe renal impairment [CrCl 15-51 mL/min (N=8)]. Eight (8)additional subjects with end stage renal disease requiring hemodialysis were also enrolled. The pharmaco-kinetics of ruxolitinib was similar in subjects with various degrees of renal impairment and in those withnormal renal function. However, plasma AUC values of ruxolitinib metabolites increased with increasingseverity of renal impairment. This was most marked in the subjects with end stage renal disease requiringhemodialysis. The change in the pharmacodynamic marker, pSTAT3 inhibition, was consistent with the corresponding increase in metabolite exposure. Ruxolitinib is not removed by dialysis; however, the removalof some active metabolites by dialysis cannot be ruled out. When administering Jakafi to patients withmoderate (CrCl 30-59 mL/min) or severe renal impairment (CrCl 15-29 mL/min) with a platelet countbetween 100 X 109/L and 150 X 109/L and patients with end stage renal disease on dialysis a dose reductionis recommended [see Dosage and Administration (2.5) in Full Prescribing Information]. HepaticImpairment The safety and pharmacokinetics of single dose Jakafi (25 mg) were evaluated in a study inhealthy subjects (N=8) and in subjects with mild [Child-Pugh A (N=8)], moderate [Child-Pugh B (N=8)], orsevere hepatic impairment [Child-Pugh C (N=8)]. The mean AUC for ruxolitinib was increased by 87%, 28%and 65%, respectively, in patients with mild, moderate and severe hepatic impairment compared to patientswith normal hepatic function. The terminal elimination half-life was prolonged in patients with hepaticimpairment compared to healthy controls (4.1-5.0 hours versus 2.8 hours). The change in the pharmaco-dynamic marker, pSTAT3 inhibition, was consistent with the corresponding increase in ruxolitinib exposureexcept in the severe (Child-Pugh C) hepatic impairment cohort where the pharmacodynamic activity wasmore prolonged in some subjects than expected based on plasma concentrations of ruxolitinib. When administering Jakafi to patients with any degree of hepatic impairment and with a platelet count between 100 X 109/L and 150 X 109/L, a dose reduction is recommended [see Dosage and Administration (2.5) inFull Prescribing Information].
BRIEF SUMMARY: For Full Prescribing Information, see package insert.INDICATIONS AND USAGE Jakafi is indicated for treatment of patients with intermediate or high-riskmyelofibrosis, including primary myelofibrosis, post-polycythemia vera myelofibrosis and post-essentialthrombocythemia myelofibrosis.CONTRAINDICATIONS None.WARNINGS AND PRECAUTIONS Thrombocytopenia, Anemia and Neutropenia Treatmentwith Jakafi can cause hematologic adverse reactions, including thrombocytopenia, anemia and neutropenia.A complete blood count must be performed before initiating therapy with Jakafi [see Dosage andAdministration (2.1) in Full Prescribing Information]. Patients with platelet counts of less than 200 X 109/Lat the start of therapy are more likely to develop thrombocytopenia during treatment. Thrombocytopenia wasgenerally reversible and was usually managed by reducing the dose or temporarily withholding Jakafi. If clinically indicated, platelet transfusions may be administered [see Dosage and Administration (2.2) in FullPrescribing Information, and Adverse Reactions]. Patients developing anemia may require blood trans-fusions. Dose modifications of Jakafi for patients developing anemia may also be considered. Neutropenia(ANC less than 0.5 X 109/L) was generally reversible and was managed by temporarily withholding Jakafi[see Adverse Reactions]. Complete blood counts should be monitored as clinically indicated and dosingadjusted as required [see Dosage and Administration (2.2) in Full Prescribing Information, and AdverseReactions]. Infections Patients should be assessed for the risk of developing serious bacterial, mycobac-terial, fungal and viral infections. Active serious infections should have resolved before starting therapy withJakafi. Physicians should carefully observe patients receiving Jakafi for signs and symptoms of infection andinitiate appropriate treatment promptly. Herpes Zoster Physicians should inform patients about early signsand symptoms of herpes zoster and advise patients to seek treatment as early as possible [see AdverseReactions].ADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted underwidely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directlycompared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. Thesafety of Jakafi was assessed in 617 patients in six clinical studies with a median duration of follow-up of 10.9months, including 301 patients with myelofibrosis in two Phase 3 studies. In these two Phase 3 studies,patients had a median duration of exposure to Jakafi of 9.5 months (range 0.5 to 17 months), with 88.7% ofpatients treated for more than 6 months and 24.6% treated for more than 12 months. One hundred andeleven (111) patients started treatment at 15 mg twice daily and 190 patients started at 20 mg twice daily. Ina double-blind, randomized, placebo-controlled study of Jakafi, 155 patients were treated with Jakafi. Themost frequent adverse drug reactions were thrombocytopenia and anemia [see Table 2]. Thrombocytopenia,anemia and neutropenia are dose related effects. The three most frequent non-hematologic adverse reactionswere bruising, dizziness and headache [see Table 1]. Discontinuation for adverse events, regardless ofcausality, was observed in 11.0% of patients treated with Jakafi and 10.6% of patients treated with placebo.Following interruption or discontinuation of Jakafi, symptoms of myelofibrosis generally return topretreatment levels over a period of approximately 1 week. There have been isolated cases of patients discon-tinuing Jakafi during acute intercurrent illnesses after which the patient’s clinical course continued to worsen;however, it has not been established whether discontinuation of therapy contributed to the clinical course inthese patients. When discontinuing therapy for reasons other than thrombocytopenia, gradual tapering of thedose of Jakafi may be considered [see Dosage and Administration (2.6) in Full Prescribing Information].Table 1 presents the most common adverse reactions occurring in patients who received Jakafi in the double-blind, placebo-controlled study during randomized treatment.Table 1: Adverse Reactions Occurring in Patients on Jakafi in the Double-blind, Placebo-controlledStudy During Randomized Treatment
Jakafi Placebo (N=155) (N=151)Adverse All All Reactions Gradesa Grade 3 Grade 4 Grades Grade 3 Grade 4 (%) (%) (%) (%) (%) (%)Bruisingb 23.2 0.6 0 14.6 0 0Dizzinessc 18.1 0.6 0 7.3 0 0Headache 14.8 0 0 5.3 0 0Urinary Tract Infectionsd 9.0 0 0 5.3 0.7 0.7Weight Gaine 7.1 0.6 0 1.3 0.7 0Flatulence 5.2 0 0 0.7 0 0Herpes Zosterf 1.9 0 0 0.7 0 0
a National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 3.0b includes contusion, ecchymosis, hematoma, injection site hematoma, periorbital hematoma, vessel puncture site
hematoma, increased tendency to bruise, petechiae, purpurac includes dizziness, postural dizziness, vertigo, balance disorder, Meniere’s Disease, labyrinthitisd includes urinary tract infection, cystitis, urosepsis, urinary tract infection bacterial, kidney infection, pyuria, bacteria
urine, bacteria urine identified, nitrite urine presente includes weight increased, abnormal weight gainf includes herpes zoster and post-herpetic neuralgiaDescription of Selected Adverse Drug Reactions Anemia In the two Phase 3 clinical studies, mediantime to onset of first CTCAE Grade 2 or higher anemia was approximately 6 weeks. One patient (0.3%)discontinued treatment because of anemia. In patients receiving Jakafi, mean decreases in hemoglobinreached a nadir of approximately 1.5 to 2.0 g/dL below baseline after 8 to 12 weeks of therapy and thengradually recovered to reach a new steady state that was approximately 1.0 g/dL below baseline. This patternwas observed in patients regardless of whether they had received transfusions during therapy. In therandomized, placebo-controlled study, 60% of patients treated with Jakafi and 38% of patients receivingplacebo received red blood cell transfusions during randomized treatment. Among transfused patients, themedian number of units transfused per month was 1.2 in patients treated with Jakafi and 1.7 in placebotreated patients. Thrombocytopenia In the two Phase 3 clinical studies, in patients who developed Grade 3or 4 thrombocytopenia, the median time to onset was approximately 8 weeks. Thrombocytopenia wasgenerally reversible with dose reduction or dose interruption. The median time to recovery of platelet countsabove 50 X 109/L was 14 days. Platelet transfusions were administered to 4.7% of patients receiving Jakafiand to 4.0% of patients receiving control regimens. Discontinuation of treatment because of thrombo-cytopenia occurred in 0.7% of patients receiving Jakafi and 0.9% of patients receiving control regimens.Patients with a platelet count of 100 X 109/L to 200 X 109/L before starting Jakafi had a higher frequency ofGrade 3 or 4 thrombocytopenia compared to patients with a platelet count greater than 200 X 109/L (16.5%versus 7.2%). Neutropenia In the two Phase 3 clinical studies, 1.0% of patients reduced or stopped Jakafibecause of neutropenia. Table 2 provides the frequency and severity of clinical hematology abnormalitiesreported for patients receiving treatment with Jakafi or placebo in the placebo-controlled study.
Jakafi is a registered trademark of Incyte Corporation. All rights reserved.U.S. Patent No. 7,598,257© 2011-2012 Incyte Corporation. All rights reserved.Issued: June 2012 RUX-1040a
74240ha_d.indd 2 7/30/12 4:42 PM

News
Targeted Therapy News • 5.13
13
Gentle yet effective therapies are called for when treating pa-tients with chronic lymphocytic
leukemia (CLL) who are age 65 years and older. While there is no standard treatment for most of those patients, several regimens are being tested in clinical trials, according to Alessandra Ferrajoli, MD, who spoke at the 17th Annual International Congress on He-matologic Malignancies, held in Febru-ary in New York City.
The treatment of elderly patients with CLL is an important area of study because 69% of patients with the dis-ease fit into that category at the time of diagnosis, making them more likely to have comorbidities that compro-mise their ability to tolerate aggressive treatments, said Ferrajoli, an associate professor in the Department of Leuke-mia at The University of Texas MD An-derson Cancer Center. In fact, she said, at age 70 years, one-third of such pa-tients have two or more comorbidities. Compared with people age 65 years and older in the general population, people in that age group who have CLL face a significantly increased mortality rate, she added.
For the healthiest elderly patients with CLL, the standard of treatment is a regimen of fludarabine, cyclophospha-mide, and rituximab (FCR), a combi-nation tested in the recent CLL8 trial,1 versus treatment with fludarabine plus cyclophosphamide.
The overall response rate was 90% in the three-drug arm versus 80% in the two-drug arm, and the complete re-sponse rate in the experimental arm was double that of the control arm, at
44% versus 22%, respectively.As a result, Ferrajoli said, the three-
drug combination is the preferred treatment for patients who boast phys-ical fitness, a lack of comorbidities, and excellent renal function, regardless of age.
Elderly patients with CLL who do not fit into that group, however, should be treated with the regimens they can withstand based on their age and health: supportive therapies for the frailest, reduced-intensity regimens for those whose health is somewhat com-promised, and more aggressive treat-ments for healthier patients, Ferrajoli said. She cited a number of clinical tri-als aimed at developing tolerable stan-dard treatments for those subgroups.
A study by Hillmen et al2 found that adding rituximab to chlorambucil pro-duced better results than chlorambu-cil alone. The investigators compared their data to that generated in an ear-lier study of single-agent chlorambucil in patients with CLL.
The overall response rate (ORR) in the intent-to-treat population was 82%, which was 16% higher than the ORR in the study of single-agent chlorambucil. The majority of responses, 68%, were partial.
“These data confirm that, in previ-ously untreated CLL patients who are unable to tolerate a more intensive chemotherapy regimen, the combina-tion of rituximab and chlorambucil is an efficacious therapy with an accept-able tolerability profile resulting in a better ORR than chlorambucil mono-therapy,” the authors wrote.
In another study that is now in press, Ferrajoli and colleagues tested whether granulocyte-macrophage colony-stim-ulating factor (GM-CSF) would increase the activity of rituximab in untreated, elderly CLL patients.
The combination sparked a response rate of 68%, better than that of ritux-imab alone, with minimal toxicity. The regimen improved symptoms includ-ing fatigue, and the combination also increased the surface expression of CD20 in CLL cells, potentially making them better targets for rituximab, Fer-rajoli said.
“At 3 years follow-up, over 80% of the patients are alive, and that means that, if needed, they can then be treated with subsequent or more aggressive approaches,” Ferrajoli said during her talk.
Another phase II study, CLL11,3 being conducted in Germany, is evaluating whether a combination of chloram-bucil and obinutuzumab (GA101), an anti-CD20 monoclonal antibody, will generate better progression-free sur-vival in elderly patients with CLL than chlorambucil plus rituximab or chlo-rambucil alone.
Finally, Ferrajoli expressed excite-ment about the promise of lenalido-mide, an immunomodulatory drug, in elderly patients with CLL. In a phase II study by Badoux et al,4 60 patients age 65 years and older with untreated CLL experienced a 65% ORR when treated with single-agent lenalidomide. In a recent update of the data, on file at MD Anderson, the patients had a 38% over-all complete response rate, 52% had remained progression-free for more than 3 years, and 37% were still taking lenalidomide. In an evaluation after 6.5 years, investigators pinpointed median progression-free survival at 52 months; overall survival had not been reached, Ferrajoli reported. She called the re-sults “very remarkable, considering the median age of these patients.”
Other promising agents that could eventually become frontline treatments include ibrutinib, GS-1101, and Tru-016.
In continuing to test new agents for the treatment of elderly patients with CLL, researchers should consider sur-vival, rather than type of response, as the ideal endpoint for studies, Ferrajoli suggested. She added that investiga-tors need to determine whether treat-ments should be continuous or inter-mittent.
Ferrajoli also cautioned that the “de-mands” associated with each therapy should be considered when treating elderly patients. “The number of trips they need to make to their oncology office, the need to arrange for trans-portation, the idea of receiving intrave-nous infusion and being in the infusion chair for hours, is very important for this population,” she said. “They have a strong preference for treatment they feel they are managing without going to the office.” TTN
1. Molica S. Clinical trial report. Progress in the
treatment of chronic lymphocytic leukemia: re-
sults of the German CLL8 trial. Expert Rev Anti-cancer Ther. 2011;11(9):1333-1340.
2. Hillmen P, Gribben JG, Follows, GA, et al.
Rituximab plus chlorambucil in patients with
CD20-positive B-cell chronic lymphocytic leu-
kemia (CLL): final response analysis of an open-
label phase II study. Presented at the American
Society of Hematology Annual Meeting; Decem-
ber 4-7, 2010; Orlando, FL. Blood. 2010;116(21).
Abstract 697.
3. Goede V, Fischer K, Busch R, et al. Chemoim-
munotherapy with GA101 plus chlorambucil in
patients with chronic lymphocytic leukemia and
comorbidity: results of the CLL11 (BO21004)
safety run-in [published online ahead of print
August 31, 2012]. Leukemia. doi: 10.1038/
leu.2012.252.
4. Badoux XC, Keating MJ, Wen S, et al. Le-
nalidomide as initial therapy of elderly patients
with chronic lymphocytic leukemia. Blood. 2011;118(13):3489-3498.
Targeted Therapies: Hematologic Malignancies
5. Clinical Trials Identifier NCT01691898. www.
clinicaltrials.gov.
6. Advani RH, Buggy JJ, Sharman JP, et al. Bruton’s
tyrosine kinase inhibitor ibrutinib (PCI-32765)
has significant activity in patients with relapsed/
refractory B-cell malignancies [published online
ahead of print October 8, 2012]. J Clin Oncol. 2013;31(1):88-94.
7. Kahl B, Byrd JC, Flinn IW, et al. Clinical safety
and activity in a phase 1 study of CAL-101, an
isoform-selective inhibitor of phosphatidylino-
sitol 3-kinase P110δ, in patients with relapsed
or refractory non-Hodgkin lymphoma. Blood. 2010;116(21)(suppl; abstr 1777).
8. Fowler NH, de Vos S, Schreeder MT, et al.
Combinations of the phosphatidylinositol 3-ki-
nase-delta (PI3Kδ) Inhibitor GS-1101 (CAL-101)
with rituximab and/or bendamustine are tolerable
and highly active in previously treated, indolent
non-Hodgkin lymphoma: results from a phase I
study. Presented at the 54th Annual Meeting of
the American Society of Hematology; December
8-11, 2012; Atlanta, GA. Blood. 2012;120(suppl;
abstr 3645).
9. Davids MS, Roberts AW, Anderson MA, et al.
The BCL-2-specific BH3-mimetic ABT-199 (GDC-
0199) is active and well-tolerated in patients with
relapsed non-Hodgkin lymphoma: interim results
of a phase I study. Presented at the 54th Annual
Meeting of the American Society of Hematol-
ogy; December 8-11, 2012; Atlanta, GA. Blood. 2012;120(suppl; abstr 304).
10. Leonard J, Jung S-H, Johnson JL. CALGB
50401: a randomized trial of lenalidomide alone
versus lenalidomide plus rituximab in patients with
recurrent follicular lymphoma: final results of a
phase II study. Presented at the Annual Meeting
of the American Society of Clinical Oncology; June
1-5, 2012; Chicago, IL. J Clin Oncol. 2012;30(sup-
pl; abstr 8000).
11. Fowler N, Hagemeister F, McLaughlin P, et al.
High response rates with lenalidomide plus ritux-
imab for untreated indolent B cell non-Hodgkins
lymphoma. Ann Oncol. 2011;22(suppl 4; abstr
137).
12. Clinical Trials Identifier NCT01476787. www.
clinicaltrials.gov.
Seeking a Standard in the Treatment of Elderly Patients With CLL
By Beth Fand Incollingo

News14
Targeted Therapy News • 5.13
The American Association for Cancer Research (AACR) is an an-nual showcase of the latest sci-
entific cancer research, with updates on phase I, often first-in-human clini-cal trials. This year’s meeting theme, “Personalizing Cancer Care Through Discovery Science,” featured many presentations of novel mechanisms of action for targeting cancer. Follow-ing is a review of several studies that delved into how specific therapies work against cancer.
Tyrosine Kinase Inhibitor Targets Bone MetastasisThe oral therapy cabozantinib has been shown to stabilize and even resolve metastatic bone lesions in patients with metastatic castration-resistant prostate cancer (mCRPC).1 Although the study was initially set to random-ize all patients to either oral cabozan-tinib or placebo, the randomization was stopped after an interim analysis showed cabozantinib was able to ef-fectively shrink bone lesions. Of the 154 patients who could be evaluated, 72% had regression of their soft tissue lesions and 68% had improvements in bone lesions, including 12% who had complete resolution.
At AACR, a poster presentation by re-searchers from the Institute of Cancer Research in London, England, revealed some of the ways in which cabozantinib is able to target prostate cancer bone lesions.2 The researchers used a mouse model of prostate cancer that produces measurable bone metastases. By in-jecting the mouse model with prostate
cancer cells labeled with a biolumines-cent marker, researchers were able to track the cancer cells as they destroyed normal bone tissue and developed into bone lesions in the mouse—lesions with the same features as bone tumors that occur in human patients.
When these bone metastases-posi-tive mice were treated with cabozan-tinib, the animals showed evidence of inhibition of tumor growth and tumor cell death, similar to what has been seen in clinical trials. Radiological scans of the bones of the mice showed a fair amount of normal bone tissue re-turning compared to mice were treated with a placebo.
Cabozantinib (Cometriq), an inhibi-tor of multiple tyrosine kinases includ-ing RET, MET, and VEGFR2, is being in-vestigated as a treatment for advanced prostate cancer in two phase III trials and is already approved by the FDA for treatment of progressive metastatic medullary thyroid cancer.
Mechanisms for the Antineoplastic Effects of Eribulin Eribulin mesylate (Halaven) is ap-proved for advanced metastatic breast cancer and is undergoing clinical test-ing for other cancers, including phase III trials in soft-tissue sarcoma and lung cancer. Eribulin is a synthetic ver-sion of a molecule derived from a ma-rine sponge that is able to arrest cell division by inhibiting cells’ ability to polymerize the protein tubulin, an es-sential component for cell replication. Although treatment with eribulin can cause tumor regression via its cell cycle arrest function, exactly how the drug works is still not clear.
Several presentations at AACR in-vestigated potential mechanisms for the antigrowth effects of eribulin. The combined results suggest eribulin may have antimetastatic effects.
Researchers demonstrated evidence supporting a previous observation that eribulin can disrupt vascular activity.3 Using a rat model of human breast xe-nograft tumors, researchers from Ei-sai Co., which manufactures eribulin, found that the drug can improve blood perfusion within the core of these xe-nograft tumors, preventing hypoxic conditions. This supports the role of er-ibulin in inhibiting hypoxia, and there-fore potentially inhibiting metastasis
of tumor cells, a process that has been shown to occur under hypoxic condi-tions. The results also support the role of eribulin in remodeling vasculature morphology.
Another study, also presented at AACR, demonstrated that eribulin is able to change the expression level of genes that may function in the epithe-lial-mesenchymal transition (EMT).4 The EMT is the process by which tumor cells acquire several characteristics, such as the ability to migrate, that are common to mesenchymal cells. This transition is thought to facilitate the process of tumor metastasis. The study measured the expression level changes of sets of genes among breast cancer cell lines treated with either eribulin or paclitaxel, a cytotoxic chemotherapy agent also known to target tubulin and cause cell-cycle arrest. Genes associ-ated with the EMT were upregulated in breast cancer cell lines that had resis-tance to eribulin. The study also iden-tified active pathways in breast cancer lines that were particularly sensitive to eribulin. Overall, the results showed that gene expression may be used to predict the sensitivity of breast cancer to eribulin, but additional studies are needed.
Ibrutinib Reduces Lymph Node Tumor Burden in Mouse ModelIbrutinib, a selective inhibitor of Bru-ton’s tyrosine kinase (Btk) is currently in phase II development for hema-tologic malignancies, including non-Hodgkin lymphoma and mantle cell lymphoma (MCL). In a presentation at AACR, researchers demonstrated that the drug is able to inhibit the adhesion and migration of malignant MCL cells using a mouse cell model, although more studies on this mechanism are needed.5
In clinical trials, patients treated with ibrutinib had an observed in-crease of MCL cells in the circulating blood that was followed by a reduction in tumor burden, suggesting that ma-lignant cells were traveling from the tumor to the peripheral blood. The re-sults presented at AACR showed that mice treated with ibrutinib had lower levels of malignant cells that traveled to and grew in lymph nodes and in the bone marrow. TTN
1. Smith DC, Smith MR, Sweeney C, et al. Cabo-
zantinib in patients with advanced prostate can-
cer: results of a phase II randomized discontinua-
tion trial. J Clin Oncol. 2013;31(4):412-419.
2. Graham TJ, Box G, Attard G, et al. Multimodal-
ity imaging investigation of response to cabozan-
tinib in a VCaP model of prostate bone metasta-
sis. Presented at American Association for Can-
cer Research Annual Meeting 2013; April 6-10,
2013; Washington, DC. Abstract 3924.
3. McCracken PJ, Ito K, Yanagimachi M, et al.
Eribulin alters vascular function in human triple-
negative (TN) breast MX-1 and MDA-MB-231
tumor xenograft models as measured by DCE-
MRI. Presented at American Association for Can-
cer Research Annual Meeting 2013; April 6-10,
2013; Washington, DC. Abstract 4502.
4. Dezso Z, Oestreicher J, Weaver A, et al. Gene
expression profiling (GEP) reveals epithelial mes-
enchymal transition (EMT) genes selectively dif-
ferentiating eribulin sensitive breast cancer cell
lines. Presented at American Association for
Cancer Research Annual Meeting 2013; April
6-10, 2013; Washington, DC. Abstract 1522.
5. Chang BY, Francesco M, Steggerda S, et al.
Ibrutinib inhibits malignant cell adhesion and mi-
gration and reduces tumor burden in lymph node
and bone marrow in a murine model of mantle
cell dissemination and progression. Presented at
American Association for Cancer Research An-
nual Meeting 2013; April 6-10, 2013; Washing-
ton, DC. Abstract 923.
Spotlight on Novel Agents in Early DevelopmentBy Anna Azvolinsky, PhD
Targeted Therapies: AACR Annual Meeting
Key Points:
• In mouse model of prostate cancer with bone metastases, cabozantinib inhibited tumor growth and tumor cell death
• Results of two preclinical studies indicate that eribulin may have antimetastatic effects
• In a mouse cell model, ibrutinib inhibited adhesion and migration of malignant MCL cells
Several presentations at AACR investigated potential mechanisms for the antigrowth effects of eribulin.

News
Targeted Therapy News • 5.13
15
Ado-trastuzumab emtansine (Kad-cyla, or T-DM1 in clinical trials) received FDA approval in Feb-
ruary, and a number of ongoing trials now seek to determine whether the antibody-drug conjugate (ADC) can be combined with other agents.
Mark Pegram, MD, director of the Breast Cancer Program at the Stanford Women’s Cancer Center in California, discussed the promise of ADCs and on-going research with T-DM1 at the An-nual Miami Breast Cancer Conference in March.
Although targeted antibodies in can-cer have been promising, with a few ex-ceptions, most have only marginal activ-ity in their targeted cancer and must be paired with a chemotherapeutic agent to maximize their efficacy. Researchers who worked on monoclonal antibod-ies during their early development had hoped that the new drugs would serve as a “magic bullet” in cancer, something that would prove to be effective in treat-ing the disease without the side effects frequently caused by chemotherapy, Pegram said.
His research in the 1990s included work on trastuzumab, a monoclonal an-tibody that targets HER2 on tumor cells, and he found the drug to be somewhat disappointing because it had to be com-bined with cytotoxic agents in order to provide patients with any substantial benefit.
However, even just a few years ago, the thought of combining trastuzumab with the cytotoxic agent emtansine
(DM1) would have been unthinkable, Pegram said. Following early research in the 1980s, emtansine sat on the shelf for many years after being developed because it was deemed too toxic to be given to patients parenterally.
“Now, we have the opportunity to recapture the promise of targeted an-tibody therapeutics because these an-tibody-drug conjugates, at least in the case of T-DM1, are very well tolerated,” Pegram said.
When emtansine is conjugated to trastu-zumab, the total amount of the cytotoxic agent is trivial when com-pared to the traditional delivery method for chemotherapy drugs, Pegram said. Addition-ally, trastuzumab has a tight binding affinity to HER2-overexpressing tumor target cells, so emtansine ends up in the tumor bed and not scattered in normal tissues, where it is prohibitively toxic.
“The therapeutic index, which is effi-cacy divided by toxicity, is exceptionally wide and really lives up to the promise of the ‘magic bullet’ finally in the case of T-DM1 because you get so much thera-peutic response with so little toxicity,” Pegram said.
The phase III EMILIA trial confirmed the efficacy of T-DM1. In that trial, 991 patients with HER2-positive advanced
breast cancer previously treated with trastuzumab and a taxane were ran-domized in a 1:1 ratio to receive T-DM1 or the combination of lapatinib and capecitabine.
In results presented at the European Society for Medical Oncology (ESMO) 2012 Congress, and concurrently pub-lished in The New England Journal of Medicine, T-DM1 was shown to reduce the mortality risk in women with HER2-
positive, unresectable, locally advanced or metastatic breast can-cer by 32% when com-pared with lapatinib and capecitabine (hazard ratio [HR] = 0.68; 95% CI, 0.55-0.85; P <.001), with a 6-month difference fa-voring T-DM1.1 Median overall survival was 30.9 months for T-DM1 ver-sus 25.1 months for lapa-tinib and capecitabine.
The survival benefit comes with an excellent
safety profile, according to Pegram. The only toxicities that have been observed in clinical trials are transient transami-nase elevation and thrombocytopenia, which Pegram said are both reversible. Pegram highlighted the fact that pa-tients did not experience common side effects, including alopecia and neutro-penia, and very little gastrointestinal toxicity was observed.
Stanford is one site for a phase I tri-al that is currently enrolling patients.
Pegram and his colleagues are studying whether T-DM1 can be given in combi-nation with paclitaxel with or without pertuzumab, another monoclonal an-tibody. Results are expected to be pre-sented at the 2013 San Antonio Breast Cancer Symposium in December.
Results from the phase III MARIANNE trial should also be presented sometime within the coming year. In that trial, pa-tients were randomized to T-DM1 plus pertuzumab, T-DM1 plus placebo, or trastuzumab plus a taxane (either pacli-taxel or docetaxel). TTN
1. Verma S, Miles D, Gianni L. Updated overall
survival results from EMILIA, a phase 3 study of
trastuzumab emtansine (T-DM1) vs capecitabine
and lapatinib in HER2-positive locally advanced
or metastatic breast cancer. Presented at: 37th
European Society for Medical Oncology Congress;
September 28-October 2, 2012; Vienna, Austria.
Abstract LBA12.
Palbociclib (formerly known as PD 0332991), a novel oral and selective inhibitor of cyclin-de-
pendent kinases (CDK) 4 and 6, has re-ceived a Breakthrough Therapy desig-nation from the FDA for the treatment of patients with breast cancer. The FDA can assign a Breakthrough Therapy designation to drugs that treat a life-threatening condition and demon-
strate a substantial improvement over existing therapies. The designation promotes an expedited review process by allowing for more meetings between the FDA and the manufacturer during development, requiring fewer patients for clinical trials, and reducing the amount of time required for trials. Pfiz-er, palbociclib’s manufacturer, is still able to seek fast-track designation, ac-
celerated approval, and priority review for the drug.
CDK 4 and 6 play an important role in regulating cell cycle progression, and preclinical models have shown that pal-bociclib has activity in patients with ER-positive breast cancer, including those with HER2-amplification.
“CDK4/6 proteins are very impor-tant in regulating cell cycle progres-
Trials Examine Use of T-DM1 as Combination Therapy for HER2 Breast CancerBy Ben Leach
Targeted Therapies: Breast Cancer
Key Points:
• T-DM1 reduced mortality risk by 32% vs lapatinib/capecitabine in HER2-positive, unresectable, locally advanced or metastatic breast cancer
• Toxicities observed in clinical trials included transient transaminase elevation and thrombocytopenia
• Trials of T-DM1 in combination therapies and in earlier-stage disease are ongoing
Key Points:
• Palbociclib has received a Breakthrough Therapy designation from the FDA for the treatment of patients with breast cancer
• A randomized, multicenter, double-blind phase III trial is now open and enrolling
FDA Grants Breakthrough Therapy Designation for Palbociclib in Breast Cancer
Mark Pegram, MD

sion,” said Richard Finn, MD, Division of Hematology/Oncology at the Jonsson Comprehensive Cancer Center, Univer-sity of California, Los Angeles, at the 2012 CTRC-AACR San Antonio Breast Cancer Symposium (SABCS). “In evalu-ating a potential role for this molecule in breast cancer, we used preclinical models and determined that there ap-peared to be a preferential activity for this molecule and this novel mecha-nism of action in models represent-ing ER-positive breast cancer as well as those representing HER2-amplified breast cancer.”
The results from a two-part phase II study of palbociclib were presented at SABCS. Postmenopausal women with
ER-positive/HER2-neg-ative advanced breast cancer were random-ized 1:1 to receive letro-zole plus palbociclib or letrozole alone. Pooled results from both parts demonstrated a me-dian progression-free survival of 26.1 months with the combination (95% CI, 12.7–26.1) com-pared with 7.5 months with letrozole alone (95% CI, 5.6–12.6). This represented a 63% im-provement in risk of progression (hazard
ratio [HR]=0.37; 95% CI, 0.21–0.63, P < .001). The most commonly report-ed adverse events were neutropenia, leukopenia, anemia, and fatigue.
Response rates in pa-tients with measurable disease were 45% for the combination arm versus 31% for letrozole alone. The clinical benefit rate, which represented com-plete and partial re-sponse rates plus stable disease, was 70% com-pared with 44%, respec-tively.
Study 1008, a randomized, multi-center, double-blind phase III trial, is now open and enrolling. The study will compare palbociclib and letrozole to letrozole alone as first-line treatment for postmenopausal patients with ER-positive, HER2-negative breast cancer with locally advanced or metastatic disease. TTN
Finn RS, Crown JP, Lang I, et al. Results of a ran-
domized phase 2 study of PD 0332991, a cyclin-
dependent kinase (CDK) 4/6 inhibitor, in combina-
tion with letrozole vs letrozole alone for first-line
treatment of ER+/HER2- advanced breast cancer
(BC). Presented at: 2012 CTRC-AACR San Antonio
Breast Cancer Symposium; December 4 – 8, 2012;
San Antonio, Texas. Abstract S1-6.
News16
Targeted Therapy News • 5.13
A large retrospective study has found that rare mutations of the human epidermal growth factor
receptor 2 (HER2) gene in patients with non-small cell lung cancer (NSCLC) po-tentially could be treated with HER2-targeted drugs. The study was pub-lished in the Journal of Clinical Oncology.
HER2 mutations are more closely as-sociated with certain types of breast cancer, but HER2 protein overexpres-sion occurs in 6% to 35% of patients with NSCLC, and HER2 gene amplifica-tion occurs in 10% to 20% of patients. Actual mutations of the HER2 gene only occur in 1% to 2% of patients with NSCLC, and are more frequently ob-served in female patients, nonsmokers, and patients with the adenocarcinoma subtype.
Because a number of HER2-targeted agents, including trastuzumab, per-tuzumab, and lapatinib, have already been approved to treat other tumor types, it may be that these agents could be used to successfully treat HER2-mu-tated NSCLC. Previous studies of HER2-targeted therapies in patients with NSCLC showed only a minimal benefit, but those studies were done in patients with HER2 overexpression, but not nec-essarily a HER2 mutation.
In this retrospective study, muta-tions of HER2 were identified in 65 out
of 3800 (1.7%) patients with NSCLC in France, Switzerland, and Spain. Pa-tients with mutated HER2 were mainly female (45 women vs 20 men), never-smokers (n=34; 52.3%), and had adeno-carcinomas, with approximately 50% of patients identified as having stage IV disease at the time of diagnosis. These characteristics matched the patient profile of HER2-mutated NSCLC sug-gested by previous studies.
A total of 33 patients with stage IV or recurrent NSCLC received conventional chemotherapy (a platinum-based dou-blet with or without bevacizumab). Of those, 16 patients also received HER2-targeted therapies. Some patients re-ceived either two (n=3) or four (n=1) different HER2-targeted drugs, so that a total of 22 individual anti-HER2 treat-ments were evaluable across the 16 patients.
Of the 16 patients, four had progres-sive disease, seven had disease stabi-lization, and 11 had partial responses, with an overall response rate of 50% and a disease control rate of 82%. The disease control rate was 93% in patients who received trastuzumab-based ther-apies (n=15) and 100% in patients who received afatinib (n=3). However, no re-sponse to other targeted therapies was observed (n=3). The median progres-sion-free survival for patients who re-
ceived HER2-targeted therapies was 5.1 months. The median survival was 89.6 months in patients with early-stage disease and 22.9 months in patients who had stage IV disease.
“Our study suggests that many pa-tients with HER2 mutations may ben-efit from anti-HER2 drugs,” said Julien Mazières, MD, PhD, professor of Pulm-onology at Larrey Hospital in Toulouse, France, and lead author of the study, in a statement. “While this benefit still needs to be confirmed in a prospective clinical trial, we hope that, based on this and other studies, HER2 status will
be taken into account when making treatment decisions.”
Mazières said that more data should be available to evaluate the efficacy of HER2-targeted agents in NSCLC within the next year or two. TTN
Mazières J, Peters S, Lepage B, et al. Lung can-
cer that harbors a HER2 mutation: epidemiologic
characteristics and therapeutic perspectives
[published online ahead of print April 22, 2013]. J Clin Oncol. doi:10.1200/JCO.2012.45.6095.
HER2-Targeted Agents May Benefit Patients With Non-Small Cell Lung CancerBy Ben Leach
Targeted Therapies: Lung Cancer
Targeted Therapies: Breast Cancer
Key Points:
• HER2 mutations in NSCLC potentially can be treated with HER2-targeted drugs, according to the results of this small preliminary study
• Prospective clinical trials are needed
Richard Finn, MD
“Our study suggests that many patients with HER2 mutations may benefit from anti-HER2 drugs.”
—Julien Mazières, MD, PhD

Nongenetic Mechanisms(continued from cover)
BRCA Patenting Case(continued from cover)
and growth patterns and responded dif-ferently to chemotherapy. The findings suggest that there are more mecha-nisms that contribute to cancer treat-ment failure than simply acquired genetic mutations of the tumor.
To understand whether the cells of a tumor that drive tumor growth are genetically the same, and whether these cells could have different func-tions, the authors both dissected the genetic sequences of the cells and per-formed functional tests on individu-ally marked cells to measure how well each cell could drive tumor growth. Fluorescently labeled CRC cells derived from 10 human colorectal tumors were transplanted into mice and allowed to grow into a new tumor with the same genomic makeup as the original, tu-mor-initiating cells. Cells from these tumors were then serially transplanted, up to five times, into other mice and al-lowed to form new tumors. Each time, the genome of the CRC tumor remained stable. The time to form a stable tumor was the same over serial transplants, and each clone retained characteristics of the original human tumor.
The authors found that genetics could not explain the different behav-iors of the tumors. The genetic clones that were selected in the mouse mod-els remained very stable, yet the tumor cells displayed markedly different types of growth behaviors. While some cells divided rapidly when transplanted into new mice, others did not reproduce well through serial transplantations. Still other cells did not grow well upon a first or second serial passage, but then regained the ability to grow well upon
subsequent passages. A total of five distinct functional behaviors were ob-served among the clones. “The distinct proliferative kinetics of the five clonal behaviors we observed underscore the functional variability of individual cells,” the authors wrote. Both deep se-quencing of mutational hotspots and copy number alteration analysis were used to assess genomic diversity.
When the transplanted tumor cells were exposed to chemotherapy, they also exhibited a range of distinct re-sponses. Mice with established CRC tumors that were marked to distin-guish single cells were treated with the chemotherapy oxaliplatin, and these chemotherapy-exposed cells were then transplanted into a new mouse. The re-sulting tumors were generated predom-inantly by previously slow-growing and dormant clones, similar to the behavior of the nonchemotherapy-exposed cells in the original experiment. This sug-gests that chemotherapy may select for the survival of those cells that are slow-growing or even dormant. These cells can then re-initiate tumor growth posttreatment, which could account for disease recurrence after initial response to chemotherapy.
“The biggest surprise was when we found that quiescent or slowly cycling cells survive chemotherapy better than their highly proliferative counterparts,” said Kreso. These chemotherapy-ex-posed cells still had very similar genetic profiles to the original, nontreated cells, suggesting a nongenetic way in which cells can outlive anticancer therapy.
The genetic variability of subclones within a tumor contributes to tumor
growth and survival. Different types of stress and exposure to anticancer thera-py can select for the growth of subclones that are able to overcome treatment, re-sulting in outgrowth of tumor cells and contributing to disease recurrence. But while researchers have presumed that genetic driver mutations—those either selected or acquired—result in therapy resistance, acquired driver mutations may not always be associated with tol-erance or resistance to a therapy, ac-cording to the new study.
Kreso and colleagues are now work-ing to understand the nongenetic fac-tors that play an important role in tu-mor cell behavior, especially response to chemotherapy. “We want to identify the epigenetic or environment factors that influence [a cell’s functional prop-erties],” Kreso explained. One approach is to compare the epigenetic marks be-tween cells with different growth kinet-ics observed in this study. “If we can gain a better understanding of the fac-tors that control cancer cell behavior, we may be able to design more specific therapies.”
The researchers are also determining both the number and the functions of genetically different clones, as well as the heterogeneity between the differ-ent clones. Kreso believes that the basic principles observed in their analysis are likely to extend to other epithelial can-cers.
These results have implications about how to identify novel anticancer targets. “We have to broaden our search and look for more than just genetic mu-tations to target tumor growth,” said Kreso. Techniques to test novel thera-
pies also need to move beyond in vitro cell line growth assays to testing the ability of tumor cells to form new tu-mors. Particularly, identification of ways to prevent metastasis remains a major hurdle in cancer treatment. “It will be interesting to see whether some tumor cells are more efficient at forming me-tastasis, whether this is linked to the cell types we have described, and which genetic or epigenetic factors contribute to this behavior,” said Kreso. TTN
Kreso A, O’Brien CA, van Galen P, et al. Variable
clonal repopulation dynamics influence chemo-
therapy response in colorectal cancer. Science. 2013;339(6119):543-548. doi: 10.1126/science.
1227670.
Key Points:
• Researchers have been able to track the growth of single human tumor cells into tumors over time in mice
• Tracking human colorectal cancer cells, the researchers were able to show that not just genes, but other biological factors can contribute to the growth and behavior of the colorectal tumor cells and contribute to failure of therapy and cancer relapse
• The results challenge the traditional notion that the properties of tumor cells, including resistance to treatment, are dictated only by the genetic makeup and spectrum of tumor mutations
Before any insurance coverage, the test costs approximately $3,340.
In 2010, the American Civil Liberties Union (ACLU) filed a lawsuit against the US Patent and Trademark Office, as well as Myriad Genetics and the University of Utah Research Foundation. The lawsuit charged that human gene patents are invalid as they are “products of nature.”
The US Patent and Trademark Office has been awarding patents on genes for about 30 years. According to a study published earlier this year in the jour-nal Genome Medicine by Jeffrey A. Rosen-feld and Christopher E. Mason, there are patents on approximately 41% of the genes that have been identified in the human genome.
This patent, which will expire in ap-proximately two years, has prevented
other companies from developing tests that identify BRCA1 and BRCA2 muta-tions. In a statement from the Associa-tion for Molecular Pathology, a plaintiff in the case, patents on genes have the potential to cause monopolies and re-strict access to databases containing genetic information acquired through these tests.
“Gene patents prevent pathologists from reading their patients’ DNA se-quences to assess their risks for dis-ease, their prognoses, or their poten-tial responsiveness to therapy,” said Iris Schrijver, MD, director of the Mo-lecular Pathology laboratory at Stan-ford University and past president of the Association of Molecular Pathol-ogy, in a statement released when the association appealed a ruling in favor
of the patent in September. “The re-sult of this lack of competition is in-creased test costs, decreased patient access, reduced innovation in the de-velopment of new test methods, and dramatically reduced knowledge dis-semination.”
However, not all physicians who use the test feel as though the patent is harmful to patients or researchers. In an interview at the 30th Annual Miami Breast Cancer Conference in March, Patrick I. Borgen, MD, chair of the de-partment of Surgery at Maimonides Breast Cancer Center at Maimonides Medical Center in Brooklyn, New York, said that in his personal experience with frequent use of the test for re-search, Myriad has not impeded his ability to get work done. Likewise, he
said that there have not been arbitrary price increases on the test.
In 2012, the US Court of Appeals for the Federal Circuit declared the isolated DNA of the BRCA1 and BRCA2 genes falls under the category of patent-eligible material.
“This case has potentially broad im-plications for the biotech, animal health and agricultural industries and the de-velopment of products and services of enormous benefit to society,” said Peter Meldrum, president and CEO of Myriad. “Countless companies and investors have risked billions of dollars to re-search and develop scientific advances under the promise of strong patent pro-tection.”
A ruling from the Supreme Court is expected this summer. TTN
Targeted Therapy News • 5.13
Feature 17

CRC is approximately 50%, but for stage IV it is only 6%, according to the Ameri-can Cancer Society. It is estimated that nearly 52,000 men and women died of colorectal cancer in the United States in 2012, according to the National Can-cer Institute.
Regorafenib was approved based on the results of the phase III CORRECT trial, which demonstrated an improved median overall survival (OS) of 1.4 months versus placebo in patients with mCRC that had progressed on previous therapy. The results were initially pre-sented at the annual American Society of Clinical Oncology (ASCO) meeting in June 2012,1 and updated survival data were subsequently presented at the annual European Society for Medical Oncology (ESMO) meeting in Septem-ber/October 2012.2 The full trial results have been published in The Lancet.3
The CORRECT trial randomized 760 patients in a 2:1 ratio to receive either 160 mg of once-daily regorafenib plus best supportive care or placebo plus best supportive care. Patients all were previously treated for mCRC with ei-ther oxaliplatin-, irinotecan-, or flu-oropyrimidine-based chemotherapy or with bevacizumab. Median OS was 6.4 months in the regorafenib arm compared with 5.0 months in the pla-cebo arm (P =.0052). The OS rate at 12 months was 24.1% in the regorafenib arm compared with 17% in the pla-cebo arm. The median progression-free survival (PFS) was 2.0 months in the experimental arm compared with 1.7 months in the placebo arm (P <.0001). Regorafenib reduced the risk of progression by 51%.
“I think many oncologists are adopt-ing the use of regorafenib,” said Randall F. Holcombe, MD, professor of Medicine, Hematology and Oncology at Mount Sinai Hospital and deputy director of the Tisch Cancer Institute in New York City. “We have many patients who have progressed on all standard therapies. [The drug is a good option], especially for those whose tumors harbor a KRAS mutation, who are not candidates for EGFR antibody therapy, but who still have a good performance status and are looking for additional treatment options.”
“Regorafenib is not a drug without toxicities,” said Holcombe. “Patients can have fatigue, fever, rash, includ-ing a hand-foot syndrome, mucositis, diarrhea, fluid retention and anorexia.” Treatment-related toxicities occurred in the vast majority, 93%, of patients on regorafenib therapy. Serious side ef-fects included hepatotoxicity, hemor-rhage, and gastrointestinal perforation.
According to Axel Grothey, MD, of
the division of Medical Oncology at the Mayo Clinic in Rochester, Minnesota, and lead author of the CORRECT trial, it is sometimes difficult to decide if the symptoms experienced on therapy are truly drug- or tumor-related. Grothey noted that side effects on regorafenib tend to occur within the first two weeks of treatment, when patients should be closely monitored.
Regorafenib is a multikinase inhibi-tor that targets various intracellular and membrane-associated kinases in-volved in angiogenic, stromal, and on-cogenic signaling. Its targets include VEGFR1 and 2, KIT, FGFR1 and 2, BRAF, and the Abl kinase.
New Targets, New Drugs in DevelopmentAs data on the genetic basis of CRC ac-cumulate, new treatment targets are emerging. For example, the BRAF kinase is mutated in 5% to 10% of mCRC. An extensive analysis of 276 colon and rec-tal tumors by The Cancer Genome At-las Network confirmed genetic targets and identified novel genes frequently mutated, as well as chromosomal rear-rangements and amplifications.4 KRAS and PIK3CA, the phosphatidylinositide 3-kinase catalytic subunit of the PI3 ki-nase, were both identified among the eight most frequently mutated genes in either colon or rectal tumors.
Such detailed analyses continue to lead to a better understanding of the important genes and pathways in-volved in CRC development and pro-gression. This knowledge is facilitat-ing not only the development of new targeted agents, but also allowing for risk stratification based on molecular subtypes and molecular predictors of response to therapies.
Oral Kinase Inhibitors in DevelopmentSeveral oral tyrosine kinase inhibitors (TKIs) are currently in development for advanced CRC. Cediranib, an oral in-hibitor of VEGF kinase, has been tested in a phase III trial in combination with chemotherapy for first-line mCRC in comparison with bevacizumab plus chemotherapy. The HORIZON III tri-al5 demonstrated that cediranib was similar to bevacizumab in terms of OS and PFS. Unfortunately, the study also found that cediranib was associated with worse patient-reported outcomes, resulting in interruption of treatment, noted Holcombe.
Trials with other TKIs are still await-ing results. Tivozanib, also an oral VEGF inhibitor, is currently in a phase II trial in combination with chemotherapy versus bevacizumab in patients with
treatment-naïve mCRC. Apatinib, an oral, selective inhibitor of the VEGF re-ceptor-2 is being tested as a monother-apy for advanced CRC.
“Any of these oral tyrosine kinase in-hibitors may have an advantage over bevacizumab, although it is not clear which if any will prove to be superior to bevacizumab yet,” said Holcombe. “The oral mode of administration is appeal-ing if the toxicity profile is not worse than that of bevacizumab.”
Regorafenib is being tested both in the first- and second-line CRC set-ting in combination with chemother-apy. Grothey sees regorafenib moving into these earlier treatment settings. Currently, bevacizumab is the most frequently used biologic agent in ad-vanced CRC.
These TKIs are promising, but not as add-on therapies to standard first-line chemotherapy FOLFOX, which is “a graveyard for many interesting agents,” Grothey said. Instead, he believes that regorafenib should be tested as a main-tenance monotherapy after first-line induction with chemotherapy.
Other Targeted AgentsSeveral oral agents that target the PI3K pathway are in phase I development for cancers that include advanced CRC. These include BKM120, a specific class I PI3K inhibitor, and DS-7423, a dual in-hibitor of PI3K and mammalian target of rapamycin (mTOR) kinase. “Combi-nations of inhibitors targeting the MAP kinase pathway, including BRAF and MEK along with PI3K inhibitors, are promising,” said Grothey.
Holcombe agrees. “I think agents tar-geting the PI3K/AKT signaling pathway are potentially especially promising,” he said. “These agents will likely need to be combined with either traditional chemotherapy or other biologics for maximal effectiveness because of re-dundancy in signaling pathways,” Hol-combe added.
Prognostic and Predictive BiomarkersMany clinical trials for CRC now in-clude biomarker analyses as part of the drug development. For example, it has been known for some time that those patients whose CRC tumor harbors a mutation in the KRAS gene do not re-spond to treatment with cetuximab, an anti-EGFR antibody. About 30% to 50% of patients with CRC have a KRAS mu-tation. The FDA has recently approved a polymerase chain reaction (PCR)-based screening test to determine the KRAS mutation status of a CRC tumor. The test recognizes seven frequent mutations in the KRAS gene.
Mutations in the BRAF gene also are a likely predictor of nonresponse to anti-EGFR therapy. Many other mo-lecular biomarkers are still in early de-velopment awaiting clinical validation testing. For antiangiogenesis therapy, there is not likely to be a single marker that can predict response to treatment, Grothey said. If any biomarkers are identified, they will likely be quantita-tive, generating a predictive value score on a continuous scale.
“Angiogenesis is a very complicated process involving signals from the tu-mor cells, but also from the stromal cells in the tumor microenvironment,” said Holcombe. “The process also in-volves the ability of endothelial cells in this tumor environment to respond to a variety of signals.” This is one reason that simple biomarkers, particularly molecular biomarkers, are not likely for antiangiogenesis therapy.
Many more studies are needed to un-derstand how molecular mutations can dictate either response or resistance to a targeted therapy. A molecular muta-tion or genotype is not always associat-ed with a particular treatment response or phenotype because of the complexi-ty of the genetics of CRC. Datasets such as that created by The Cancer Genome Atlas Network will continue to serve as tools for both the creation of new ther-apies and for predictive and prognostic biomarker approaches. Furthermore, analyses of epigenetic alterations and other layers of complexity will need to be integrated for a full understanding of what drives colorectal cancer. TTN
1. Van Cutsem E, Sobrero AF, Siena S, et al. Phase
III CORRECT trial of regorafenib in metastatic
colorectal cancer (mCRC). J Clin Oncol. 2012;30
(suppl; abstr 3502).
2. Van Cutsem EJD, Grothey A, Laeuven BE.
Phase 3 CORRECT trial of regorafenib in meta-
static colorectal cancer (mCRC): overall survival
update. Presented at: 38th European Society for
Medical Oncology (ESMO) Congress; September
28-October 2, 2012; Vienna Austria. Ann Oncol. 2012;23(suppl 9; abstr LBA18).
3. Grothey A, Van Cutsem E, Sobrero A, et al.
Regorafenib monotherapy for previously treated
metastatic colorectal cancer (CORRECT): an inter-
national, multicentre, randomised, placebo-con-
trolled, phase 3 trial. The Lancet. 2013;381(9863):
303-312.
4. The Cancer Genome Atlas Network. Compre-
hensive molecular characterization of human co-
lon and rectal cancer. Nature. 2012;487(7407):
330-337.
5. Schmoll HJ, Cunningham D, Sobrero A, et al.
Cediranib with mFOLFOX6 versus bevacizumab
with mFOLFOX6 as first-line treatment for pa-
tients with advanced colorectal cancer: a double-
blind, randomized phase III study (HORIZON III). J Clin Oncol. 2012;30(29):3588-3595.
Feature18
Targeted Therapy News • 5.13
18
Colorectal Cancer(continued from cover)
Feature

Primary endpoint: Progression-free survival
Key secondary endpoint: Overall survival
Buparlisib + fulvestrant Placebo + fulvestrant
Randomization
Pioneering Research of PI3K inhibitors in Malignancies
For more informationwww.clinicaltrials.gov (NCT01610284 and NCT01633060) Novartis Oncology Clinical Trials Hotline: 1-800-340-6843 (USA only) Or contact your local Novartis representative
BELLE-2 and BELLE-31
Postmenopausal women with HR+/HER2– locally advanced or metastatic breast cancer pretreated with aromatase inhibitor
Archival tumor tissue for analysis of PI3K pathway activation
No more than one prior line of chemotherapy for metastatic disease
ECOG Performance Status ≤2
BELLE-31
Evidence of progression on or after mTOR inhibitor-based treatment
Buparlisib (BKM120) is an investigational new drug. Efficacy and safety have not been established. There is no guarantee that buparlisib will become commercially available.
1Additional inclusion/exclusion criteria apply.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; HER2–, human epidermal growth factor receptor 2-negative; HR+, hormone receptor-positive; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
©Novartis 2012Novartis Pharmaceuticals CorporationEast Hanover, NJ 07936 August 2012 G-BKE-1047878
Novartis Pharma AG CH-4002, Basel, Switzerland
BELLE-2 and BELLE-3Two Phase III studies investigating the pan-PI3K inhibitor, buparlisib (BKM120), plus fulvestrant in HR+/HER2– advanced breast cancer
NOW ENROLLING TWO PHASE III STUDIES
Primary endpoint: Progression-free survival
Key secondary endpoint: Overall survival
Buparlisib + fulvestrant Placebo + fulvestrant
Randomization
Pioneering Research of PI3K inhibitors in Malignancies
For more informationwww.clinicaltrials.gov (NCT01610284 and NCT01633060) Novartis Oncology Clinical Trials Hotline: 1-800-340-6843 (USA only) Or contact your local Novartis representative
BELLE-2 and BELLE-31
Postmenopausal women with HR+/HER2– locally advanced or metastatic breast cancer pretreated with aromatase inhibitor
Archival tumor tissue for analysis of PI3K pathway activation
No more than one prior line of chemotherapy for metastatic disease
ECOG Performance Status ≤2
BELLE-31
Evidence of progression on or after mTOR inhibitor-based treatment
Buparlisib (BKM120) is an investigational new drug. Efficacy and safety have not been established. There is no guarantee that buparlisib will become commercially available.
1Additional inclusion/exclusion criteria apply.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; HER2–, human epidermal growth factor receptor 2-negative; HR+, hormone receptor-positive; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
©Novartis 2012Novartis Pharmaceuticals CorporationEast Hanover, NJ 07936 August 2012 G-BKE-1047878
Novartis Pharma AG CH-4002, Basel, Switzerland
BELLE-2 and BELLE-3Two Phase III studies investigating the pan-PI3K inhibitor, buparlisib (BKM120), plus fulvestrant in HR+/HER2– advanced breast cancer
NOW ENROLLING TWO PHASE III STUDIES
Primary endpoint: Progression-free survival
Key secondary endpoint: Overall survival
Buparlisib + fulvestrant Placebo + fulvestrant
Randomization
Pioneering Research of PI3K inhibitors in Malignancies
For more informationwww.clinicaltrials.gov (NCT01610284 and NCT01633060) Novartis Oncology Clinical Trials Hotline: 1-800-340-6843 (USA only) Or contact your local Novartis representative
BELLE-2 and BELLE-31
Postmenopausal women with HR+/HER2– locally advanced or metastatic breast cancer pretreated with aromatase inhibitor
Archival tumor tissue for analysis of PI3K pathway activation
No more than one prior line of chemotherapy for metastatic disease
ECOG Performance Status ≤2
BELLE-31
Evidence of progression on or after mTOR inhibitor-based treatment
Buparlisib (BKM120) is an investigational new drug. Efficacy and safety have not been established. There is no guarantee that buparlisib will become commercially available.
1Additional inclusion/exclusion criteria apply.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; HER2–, human epidermal growth factor receptor 2-negative; HR+, hormone receptor-positive; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
©Novartis 2012Novartis Pharmaceuticals CorporationEast Hanover, NJ 07936 August 2012 G-BKE-1047878
Novartis Pharma AG CH-4002, Basel, Switzerland
BELLE-2 and BELLE-3Two Phase III studies investigating the pan-PI3K inhibitor, buparlisib (BKM120), plus fulvestrant in HR+/HER2– advanced breast cancer
NOW ENROLLING TWO PHASE III STUDIES
Primary endpoint: Progression-free survival
Key secondary endpoint: Overall survival
Buparlisib + fulvestrant Placebo + fulvestrant
Randomization
Pioneering Research of PI3K inhibitors in Malignancies
For more informationwww.clinicaltrials.gov (NCT01610284 and NCT01633060) Novartis Oncology Clinical Trials Hotline: 1-800-340-6843 (USA only) Or contact your local Novartis representative
BELLE-2 and BELLE-31
Postmenopausal women with HR+/HER2– locally advanced or metastatic breast cancer pretreated with aromatase inhibitor
Archival tumor tissue for analysis of PI3K pathway activation
No more than one prior line of chemotherapy for metastatic disease
ECOG Performance Status ≤2
BELLE-31
Evidence of progression on or after mTOR inhibitor-based treatment
Buparlisib (BKM120) is an investigational new drug. Efficacy and safety have not been established. There is no guarantee that buparlisib will become commercially available.
1Additional inclusion/exclusion criteria apply.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; HER2–, human epidermal growth factor receptor 2-negative; HR+, hormone receptor-positive; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
©Novartis 2012Novartis Pharmaceuticals CorporationEast Hanover, NJ 07936 August 2012 G-BKE-1047878
Novartis Pharma AG CH-4002, Basel, Switzerland
BELLE-2 and BELLE-3Two Phase III studies investigating the pan-PI3K inhibitor, buparlisib (BKM120), plus fulvestrant in HR+/HER2– advanced breast cancer
NOW ENROLLING TWO PHASE III STUDIES
Primary endpoint: Progression-free survival
Key secondary endpoint: Overall survival
Buparlisib + fulvestrant Placebo + fulvestrant
Randomization
Pioneering Research of PI3K inhibitors in Malignancies
For more informationwww.clinicaltrials.gov (NCT01610284 and NCT01633060) Novartis Oncology Clinical Trials Hotline: 1-800-340-6843 (USA only) Or contact your local Novartis representative
BELLE-2 and BELLE-31
Postmenopausal women with HR+/HER2– locally advanced or metastatic breast cancer pretreated with aromatase inhibitor
Archival tumor tissue for analysis of PI3K pathway activation
No more than one prior line of chemotherapy for metastatic disease
ECOG Performance Status ≤2
BELLE-31
Evidence of progression on or after mTOR inhibitor-based treatment
Buparlisib (BKM120) is an investigational new drug. Efficacy and safety have not been established. There is no guarantee that buparlisib will become commercially available.
1Additional inclusion/exclusion criteria apply.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; HER2–, human epidermal growth factor receptor 2-negative; HR+, hormone receptor-positive; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
©Novartis 2012Novartis Pharmaceuticals CorporationEast Hanover, NJ 07936 August 2012 G-BKE-1047878
Novartis Pharma AG CH-4002, Basel, Switzerland
BELLE-2 and BELLE-3Two Phase III studies investigating the pan-PI3K inhibitor, buparlisib (BKM120), plus fulvestrant in HR+/HER2– advanced breast cancer
NOW ENROLLING TWO PHASE III STUDIES
Primary endpoint: Progression-free survival
Key secondary endpoint: Overall survival
Buparlisib + fulvestrant Placebo + fulvestrant
Randomization
Pioneering Research of PI3K inhibitors in Malignancies
For more informationwww.clinicaltrials.gov (NCT01610284 and NCT01633060) Novartis Oncology Clinical Trials Hotline: 1-800-340-6843 (USA only) Or contact your local Novartis representative
BELLE-2 and BELLE-31
Postmenopausal women with HR+/HER2– locally advanced or metastatic breast cancer pretreated with aromatase inhibitor
Archival tumor tissue for analysis of PI3K pathway activation
No more than one prior line of chemotherapy for metastatic disease
ECOG Performance Status ≤2
BELLE-31
Evidence of progression on or after mTOR inhibitor-based treatment
Buparlisib (BKM120) is an investigational new drug. Efficacy and safety have not been established. There is no guarantee that buparlisib will become commercially available.
1Additional inclusion/exclusion criteria apply.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; HER2–, human epidermal growth factor receptor 2-negative; HR+, hormone receptor-positive; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
©Novartis 2012Novartis Pharmaceuticals CorporationEast Hanover, NJ 07936 August 2012 G-BKE-1047878
Novartis Pharma AG CH-4002, Basel, Switzerland
BELLE-2 and BELLE-3Two Phase III studies investigating the pan-PI3K inhibitor, buparlisib (BKM120), plus fulvestrant in HR+/HER2– advanced breast cancer
NOW ENROLLING TWO PHASE III STUDIES
Primary endpoint: Progression-free survival
Key secondary endpoint: Overall survival
Buparlisib + fulvestrant Placebo + fulvestrant
Randomization
Pioneering Research of PI3K inhibitors in Malignancies
For more informationwww.clinicaltrials.gov (NCT01610284 and NCT01633060) Novartis Oncology Clinical Trials Hotline: 1-800-340-6843 (USA only) Or contact your local Novartis representative
BELLE-2 and BELLE-31
Postmenopausal women with HR+/HER2– locally advanced or metastatic breast cancer pretreated with aromatase inhibitor
Archival tumor tissue for analysis of PI3K pathway activation
No more than one prior line of chemotherapy for metastatic disease
ECOG Performance Status ≤2
BELLE-31
Evidence of progression on or after mTOR inhibitor-based treatment
Buparlisib (BKM120) is an investigational new drug. Efficacy and safety have not been established. There is no guarantee that buparlisib will become commercially available.
1Additional inclusion/exclusion criteria apply.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; HER2–, human epidermal growth factor receptor 2-negative; HR+, hormone receptor-positive; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
©Novartis 2012Novartis Pharmaceuticals CorporationEast Hanover, NJ 07936 August 2012 G-BKE-1047878
Novartis Pharma AG CH-4002, Basel, Switzerland
BELLE-2 and BELLE-3Two Phase III studies investigating the pan-PI3K inhibitor, buparlisib (BKM120), plus fulvestrant in HR+/HER2– advanced breast cancer
NOW ENROLLING TWO PHASE III STUDIES
A12392-full_TTN_Novartis-Belle.indd 8 10/17/12 4:14 PM

Feature
In the wake of the approval of sev-eral novel treatments for prostate cancer—including antiandrogens
enzalutamide and abiraterone and im-munotherapy sipuleucel-T, physicians must now focus on how best to integrate new therapies into the treatment of pa-tients with prostate cancer. At the 2013 Annual Interdisciplinary Prostate Can-cer Congress (IPCC), in New York City, researchers reviewed the latest strate-gies and therapeutic agents available for patients, and held a case-based dis-cussion to build consensus about best treatments. The cases were presented by IPCC Co-Chair Leonard Gomella, MD, and discussed by a panel that included Co-Chair Daniel P. Petrylak, MD; Robert Dreicer, MD, MS; E. David Crawford, MD; and Susan Slovin, MD.
Case 1Gomella: The patient is a 55-year-old white male. His father died of prostate cancer at 65 years of age, and no other family members have any history of prostate cancer. The pa-tient is worried and wants to be checked, al-though he’s done some reading and is doubt-ful about the value of the prostate-specific antigen (PSA) test. What do you tell him?Dreicer: The patient is at risk, since he had a first-degree relative who was im-pacted. Screening is reasonable for him.Petrylak: I’d tell him that PSA has its implications. If it’s elevated, he’ll need a biopsy, and then he’ll have to choose either local therapy or observation. I would do it if I were him. But he needs to know what the studies say.Slovin: I would explain the pros and cons and then leave it up to him, although I probably would give him the strong arm because his risk is at least two-fold higher than Joe Blow’s next door as a re-sult of his family history. I’d also make sure he’s had a screening colonoscopy.Crawford: One family member probably doesn’t increase risk a lot. You’ve got to have two or three to be at a higher risk.
Gomella: The patient has his PSA tested and it’s deemed normal at 1.1 His digital rectal exam is normal. Can you tell him he doesn’t have prostate cancer?Crawford: No. Based on the results of the Prostate Cancer Prevention Trial [in which 15% of men with PSAs of <4 ng/mL were found to have prostate cancer], he still faces a risk.1 I’d do a Prostate Cancer Gene 3 (PCA3) test on him.
Petrylak: He needs a repeat biopsy. I would do a saturation biopsy. Gomella: How about PCA3, if he didn’t have it before?Petrylak: It probably would be appropri-
ate, but I still think he’s going to need a biopsy.Gomella: What about free-to-total PSA? Is anyone using that anymore? We asked this question two years ago and just about everybody put their hands up, and now, as I look around, there seems to be a lot of cooled enthusiasm.
What would the audience do in this setting? The choices are: (1) perform a biopsy; (2) repeat the PSA test; (3) check free-to-total PSA; or (4) check PCA3.
Okay, 61% said biopsy, 22% repeat PSA, 7% free-to-total PSA, and 9% PCA3.Dreicer: I’d do a PCA3 first, though.Gomella: I agree, although it does scare me a little bit that his PSA had had such a rapid rise.Crawford: The PCA3 would make me feel better about doing another biopsy.
Gomella: The patient comes back three years later and his PSA is up to 8. He’s had at least three sets of 12-core biopsies, and they’ve all been negative. Now where are we?Crawford: This is a guy that I would get the MRI on, and the mapping bi-opsies. I’d also consider the fact that, every time you have one negative biopsy, your risk goes down. If the guy is tired of biopsies or his insur-ance company won’t pay for more, I’d also think about putting him on dutasteride to see what his PSA does, because I’ve seen peo-ple like this go from 8 to 1 again, or at least cut their PSA in half.
Gomella: Dave, what about transurethral (TUR) biopsy? We used to do that in the ’90s when we ran into this situation. It was sort of an anterior biopsy. Is this a dead issue now because of MRIs?
Gomella: Even though he hasn’t had a biopsy yet, you would jump the fence on the PCA3 and use it sort of off-label? The labeled indication is to see if a sec-ond biopsy is needed.Crawford: Yes.Gomella: What I tell my residents—and my pa-tients—is that we’re finding our way with PCA3, but that we have a lot of questions. Still, I’d rather have a PCA3 in the bank in case some breakthrough comes up over the next couple of years.
So, you can’t tell the pa-tient he doesn’t have pros-tate cancer. What would you do next?Slovin: I would ask him to repeat a PSA in a short period of time to get a sense of how rapidly it’s going up.
Gomella: Let’s assume he had a biopsy a year ago that was completely normal. Now he comes in and his PSA has gone up to 5. He still has a normal digital rectal exam. What would you do next?
Crawford: A lawyer told me the other day that he’s defending a urologist for that very thinking. The patient was just like this one: negative biopsy, negative biopsy, negative biopsy, PSA not even up this high, and so he didn’t do any-thing. A couple of years later he’s got metastatic disease, and they’re saying he should have had a TUR biopsy. But to me, what takes the place of the TUR biopsy are the staging and mapping bi-opsies. We’ve actually shown that if you take those biopsies and you correlate them to whole mount radical prostatec-tomy specimens, they’re just as accu-rate, if not more accurate, at predicting what’s there.Audience member: I have a question about PSA leaks in people who’ve had multiple biopsies. I’ve certainly done three or four biopsies on people, but I worry that I have created the [elevated] PSA with all the [needle] sticks.
Gomella: Dave, with all those needle sticks in the prostate, are you making a leaky pros-tate, making neovascular channels when it heals, and sending more PSA out to the bloodstream?Crawford: I don’t buy it.
Gomella: There’s some data out there now saying that the more biopsies you have, the more difficult it may be to spare nerves when you get treated definitively
with a radical prostatect- omy. What do you think about that, Dave?Crawford: Well, I’ve had a lot of experience in going in after mapping. Since the mapping is done transperineally, it’s not much more diffi-cult to do. In the people that have had a couple of what you described as saturation biop-sies, which are tran-srectal, that has been difficult.
Gomella: So what can a pa-tient like this do to prevent prostate cancer, and what should you recommend?Slovin: There are data that there is some benefit to changing the diet, limiting the amount of red meat. And while I recom-mend that for some patients who are on the heavier side, I don’t know that
Targeted Therapy News • 5.13
20
Integrating Novel Agents Into the Treatment of Prostate CancerCase-Based Discussion
By Beth Fand Incollingo
Leonard Gomella, MD
Daniel P. Petrylak, MD
“What I tell my residents—and my patients—is that we’re finding our way with PCA3, but that we have a lot of questions. Still, I’d rather have a PCA3 in the bank in case some breakthrough comes up over the next couple of years.”
—Leonard Gomella, MD

Feature
it’s something we would do for every-body. The question is, do I put him on dutasteride or finasteride? I’d be a little worried, but you can make an argument that if the prostate shrinks down a little bit more, it’s going to be easier to find a Gleason 8 or 9 cancer sitting there wait-ing for us.Gomella: It’s kind of disappointing that we don’t have this as an approved pre-vention strategy, since we have two large clinical trials that show a 20% to 25% relative risk reduction with 5 alpha-reductase inhibitors, and data from tri-als such as CombAT demonstrating no increased risk of high-grade cancer.2 Dr. Dreicer, you’ve been involved in some drug discussions at the FDA level. Do you think there’s any chance that this thing could get resurrected?
Dreicer: None.Crawford: Less than none. We’ve been through so many things on the preven-tion of prostate cancer: vitamin E, and selenium, and saw palmetto, and the 5-alpha reductase inhibitors, and Vioxx. I think the benefit of 5-alpha reductase inhibitors is real, but we also need to document the risk of high-grade can-cer, which is probably volume-related. In my opinion, chemo prevention trials in prostate cancer are dead, because it’s too risky.Gomella: You may also be familiar with the data that came out a few years ago that patients with advanced prostate cancer who went on hyper-vitamin therapy actually had a worse outcome. They progressed more rapidly. So we have to convince our patients that more is not necessarily better.Petrylak: That was demonstrated in the SELECT trial, too.3 The trial took all com-ers, and you wonder what giving these vitamins at high dosages to somebody who has a normal level is going to do to their prostate tissue. A lot of these agents are yin-yang: In low doses they may be inhibitory, in high doses they may be stimulatory. So when designing these studies in the future, you’re going
21
JOB#: 22705A CLIENT: Exelixis DESC: Journal Ad FILE NAME: EXL_XLX_Q35692A_JA_D01.indd DATE: 4-3-2013 12:16 PM ROUND: 1PG: millerk/dilenam AD: PC TC: SC AE: None CW: None Last Saved: 4-3-2013 12:16 PMTRIM: 7.5” x 10.5” BLEED: 8.25” x 11.25” SAFETY: 6.75” x 9.75” PROD: M Haight INK Spec: 4C PRINT SCALE: 100%FONTS: Futura Std (Medium Condensed, Medium, Extra Bold Condensed)
IMAGES: Exelixis_blk.eps (19.2%), COMET_3025_4C.eps (51.6%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: Macintosh HD:Users:millerk:Des...JA_D01:EXL_XLX_Q35692A_JA_D01.inddNOTES: None
EXL_XLX_Q35692A_JA_D01.indd Galley: 1
S&H PharmaGraphics
Disk Release
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
Randomization
Cabozantinib 60 mg QD
Prednisone
KEY ELIGIBILITY CRITERIA• Diagnosis of CRPC • Presence of bone metastases• Prior treatment with docetaxel• Prior treatment with abiraterone and/or MDV3100 (enzalutamide)• No limit to the number of prior therapies
COMET-1
PRIMARY ENDPOINT Confirmed Pain Response
COMET-2
PRIMARY ENDPOINTOverall Survival
Randomized, double-blind, controlled trial Randomized, double-blind, controlled trial
Visit www.Cometclinicaltrials.com or call 1-855-85-COMET to learn more about these trials.
Randomization
Cabozantinib 60 mg QD
Mitoxantrone +
Prednisone
Cabozantinib phase 3 trials in castration-resistant prostate cancer (CRPC) for patients with bone metastases
© 2013 Exelixis, Inc. 210 East Grand Avenue, So. San Francisco, CA 94080 04/13 [MA0015v01]
CRPC (N=960)
• Prior docetaxel treatment
• Prior abiraterone and/or MDV3100 treatment
• No limit to number of prior therapies
CRPC(N=246)
• Prior docetaxel treatment
• Prior abiraterone and/or MDV3100 treatment
• No limit to number of prior therapies
• Pain related to bone metastases
INVESTIGATIONAL PHASE 3 TRIALS CURRENTLY ACCRUING
2ej1 Q1 Q2Cosmos Communications 718.482.1800
24587a 04.03.13 133C M Y K
S:6.75”
S:9.75”
T:7.5”
T:10.5”
B:8.25”
B:11.25”
“In my opinion, chemo prevention trials in prostate cancer are dead, because it’s too risky.”
—E. David Crawford
to have to look at levels and see wheth-er you’re supplementing something that doesn’t need to be supplemented.Gomella: And despite this data, we still find all our patients taking vitamin E
and selenium to prevent prostate can-cer, which is really sad.
Case 2Gomella: The patient is a 62-year-old who de-
velops urinary frequency. His primary care doctor detects a nodule on rectal exam and a PSA of 82. A urologist does a biopsy and finds Gleason 7 cancer. A bone scan shows four lesions in the lumbar sacral spine, and

Feature
Targeted Therapy News • 5.13
2222 Feature
“I’ve gone back to ketoconazole, because abiraterone is not always covered by insurance.”
—Susan Slovin, MD
a CT scan of the abdomen shows retroperi-toneal lymphadenopathy. The patient under-goes combined androgen blockade. His PSA bottoms out at less than 0.1 seven months after the blockade is started, and he remains on continuous androgen blockade for about three years. His PSA then begins to slowly rise from 0.2 to 0.8 to 1.0 over a six-month period. On bone scan, progression is noted with two more spots in the ribs. A CT scan of the abdomen and pelvis shows resolution of retroperitoneal adenopathy, and the patient feels pretty good. He’s not in any pain, and he has a good appetite and a good performance status. At this point, what would you do? Audience choices are: (1) discontinue bicalu-tamide and monitor for antiandrogen withdrawal syndrome; (2) start sec-ond-line hormonal therapy with ketoconazole and hydrocortisone; (3) give him sipuleucel-T; (4) do numbers 1 and 2; or (5) do numbers 1 and 3. The results are pretty even. Twenty-eight percent would stop the bicalu-tamide and monitor for antiandrogen withdrawal, 24% would give him sipu-leucel-T, 12% would do 1 and 2, and 30% would do antiandrogen withdrawal and sipuleucel-T. At 6 %, it looks like ketocon-azole and hydrocortisone do not have a lot of traction right now.Petrylak: The only times I’ve used ke-toconazole in a patient who’s castrate- resistant is when the patient has non-metastatic disease. Except in that situ-ation, abiraterone has superseded keto-conazole in this clinical state.Slovin: I’ve gone back to ketoconazole,
because abiraterone is not always cov-ered by insurance. Ketoconazole is not as effective, and it has more toxicity, but if you’re in a dither it’s the best one to use. On this particular patient, though,
I could make the argument that if he went into a complete biochemical ra-diographic remission, I would have ra-diated his prostate for local control and maybe used adjuvant hormones for an extra year, and then gotten him off ev-erything. He’s a young guy, and the law does not say one should stay on hor-mones for ever and ever.Dreicer: Clearly we’re going to stop his bicalutamide—that’s a no brainer—and if you’re going to think about immu-nomodulatory therapy, this might be a very good patient to use it in. Even if he has an antiandrogen withdrawal re-sponse, you could argue that that’s okay,
and may make him even a better candidate.
Gomella: The patient’s tes-tosterone is 55 and he’s been getting leuprolide. What would you do at that point?Petrylak: One option would be to put him on abiraterone, which would reduce his tes-tosterone even further. A second would be to put him on degarelix, which could also lower his testosterone. Of course, the final option
is simply to do an orchiectomy.Gomella: An important point, and one that Dr. Crawford has been out in the lead on, is that our LHRH analog thera-pies are one-size-fits-all. If you have a 98-pound gentleman and a 300-pound gentleman, they get the same dose of the LHRH analog, and there are some issues now to suggest that the mode of administration and obesity can actually affect absorption and utility. So, at our shop, we’ve flipped people from gosere-lin to triptorelin, or triptorelin to leup-rolide, and I have to say that we’ve al-ways gotten their testosterone to come down.Crawford: In a study, we looked at pa-tients with T (testosterone) less than 50 who went on sipuleucel-T, and then [investigational] GTx-758 and a couple of other agents, and watched T levels. Twenty-one percent of participants had T levels above about 20. Orchiectomy gets you to 14 to 17. And so, theoreti-cally, these patients aren’t castrate. And maybe the reason 20% to 30% of people respond to secondary androgen abla-tion is because they weren’t totally sup-pressed to begin with.Slovin: While we’re getting serum tes-tosterone levels down, we still are never
100% sure of intratumoral testosterone levels. That’s always sitting in the back-ground.Dreicer: And the testosterone assays most of us use in the hospitals are not very sensitive, especially at the low level.Crawford: You’ve got to also measure the free T level.
Gomella: The patient gets sipuleucel-T and, at one month post-therapy, his PSA contin-ues to rise to 20 and then to 30. His bone scan is stable with no new lesions. He has no complaints and feels well. Six months later, his bone scan stays stable and his PSA goes up to 50. What would you tell him now about the sipuleucel-T?Slovin: I would tell him that we don’t know how long it takes to see a propi-tious antitumor response, and as long as his cancer is stable, it’s fine.
Gomella: In this case, the patient was put on abiraterone and prednisone. Do you think he needed to be there, Rob?Dreicer: I would have been concerned that, in a relatively short period of time, he was going to become symptomatic, and I’d want to obviate that, so I think it’s emi-nently reasonable to have treated him.
Gomella: So the patient is put on the abiraterone/prednisone regimen, and his PSA goes down. Eight months after treatment, it’s down to 3. However, it then goes up to 5 and then, four weeks later, to 9. He has new or recurring ret-roperitoneal adenopathy. His bone scan shows more lesions, and he has lum-bosacral spine pain. He’s failed hormonal therapy, sipuleucel-T, and abiraterone. What would the audience do for this gentleman?The choices are to give (1) enzalutamide, (2) docetaxel/prednisone, or (3) cabazitaxel.Okay, 12% of you said enzalutamide, 72% said docetaxel and prednisone, and 16% said cabazitaxel.It looks like the clear winner here is standard docetaxel and prednisone. Dan, any com-ments about using it in the setting of having pain?Petrylak: The right situation to use it is when the patient is symptomatic. As far as your alternatives, there’s no data for using cabazitaxel in the frontline setting. With enzalutamide, we don’t know what the response rate is after
abiraterone. Also, at this point, it’s not approved for that indication.
Case 3Gomella: The patient is 69 years old and has Gleason 4+3 prostate cancer. His PSA is 9, and his rectal exam shows a T2a nodule. He is staged negative on bone scan and CAT scan, has good GU function, and is sexu-ally active without PDE-5 inhibitors. He has had no previous pelvic radiation or irritable bowel disease, and his prostate size is about 40 ccs on transrectal ultrasound. Since he prefers radiation therapy, his options are brachytherapy, external-beam radiation, brachytherapy plus external-beam, protons, or all of the above.The audience selected all of the above (48%), external-beam (24%), brachytherapy plus ex-ternal-beam (18%), brachytherapy (8%), and protons (2%).Dr. Crawford, what are your thoughts on this gentleman?Crawford: I think he has all of those things available. The current “sexy treatment” seems to be focusing on brachytherapy and how high the dose can go. So that’s what a lot of people are doing.Gomella: Probably mixing brachytherapy
with external-beam would be a top option for him. But it’s almost dealer’s choice.
Gomella: So the next ques-tion is: What’s the benefit of adding hormonal ther-apy in this patient who’s getting radiation therapy? Would people do that?Eighty percent of you say yes, 20% say no.We’re going to assume this man is intermediate or higher-intermediate risk, and that’s probably a rea-sonable choice. Dave, do
you have any thoughts about using an LHRH agonist or antagonist in these settings? Are you still using combined androgen blockade? Crawford: I still believe in combined an-drogen blockade. If you give an agonist, you get a flare, testosterone goes up, the tumor gets bigger, and the prostate gets bigger. If you’re trying to downsize, you’re wasting time. So combined an-drogen blockade makes sense. There’s pretty good evidence about using an an-tagonist where you don’t get that, and some other advantages. So, we tend to use more antagonist activity.
The other trend that’s interesting is that the hormone therapy is kind of going away, except in really high-risk patients, and that it’s being continued
Robert Dreicer, MD
Susan Slovin, MD

Feature
Targeted Therapy News • 5.13
23
for less than two years, while the radia-tion dose is going up. The claim is that there’s less local failure because we’re able to get the gray up so high. But I don’t buy that. My argument is that a lot of these people who are getting hor-mones and radiation with intermediate and advanced disease are actually ben-efiting from treatment of micrometa-static disease with hormone therapy.Gomella: The other question that has been unanswered is: How many of these patients actually recover their testosterone level to some reasonable-ness? That’s something that the radia-tion/oncology community has not been enthusiastic about studying, because they think it’s not an important issue.Crawford: Another thing that never gets talked about is that when you radiate the prostate, you have radiation scatter that hits the testes and lowers testos-terone. If you look at a few studies that have been done, the bump in testoster-one down is not huge. It’s 10%, 20%, maybe even more. What effect does that have?
Gomella: Here’s a question for the audience. If you were going to treat this man with external-beam radiation monotherapy, what is the optimum dose he should receive for local-ized prostate cancer? The choices are (1) 66.6 gray (Gy) at 1.8 Gy/fraction; (2) 72 Gy at 1.8 Gy/frac-tion; (3) 79.2 Gy at 1.8 Gy/fraction; or (4) 80 Gy at 2.0 Gy/fraction.Thirty percent of you say 80 Gy, 23% say 72 Gy, and 6% say 66.6 Gy. Forty percent say 79.2 Gy, and that’s about right. Once you start getting to 80 Gy with external-beam radiation, the toxicity goes up dramatically.Audience member: What’s your opinion about local radiation at this point? Not the complete gland, but focal radiation?Crawford: I think it’s a good idea to do extra loading of the seeds in the area that is involved, and then not as much to cover the rest of the gland.Gomella: It might make theoretic sense from a standard-of-care standpoint, but it’s nowhere in any kind of guidelines.Crawford: They’re actually doing it at Me-morial Sloan-Kettering. And we’re going to be joining them in a trial that will in-volve targeting, loading it to the lesion.Gomella: High-dose radiation therapy is being reconsidered in localized prostate cancer as well. We’re not talking about
focal therapy there, but it’s just another way of getting the radiation into the gland.
Case 4Gomella: Here’s another high-risk patient, an 83-year-old gentlemen with urinary re-tention and an inability to walk. His PSA is over 1000. An MRI of the spine shows a T12 epidural spinal cord compression. He un-dergoes a decompressive laminectomy that shows metastatic carcinoma of the prostate. His bone scan is extensively positive, with le-sions in the left femur, axial and appendicu-lar skeleton, the T12 vertebra, and the ribs. A CAT scan of the abdomen and pelvis shows no evidence of any visceral metastases. The patient is treated with androgen blockade, and seven months after therapy, his PSA is 12. Three months later he has pain in his back. A bone scan shows new lesions. His PSA has bounced up to 80 and he’s put on abiraterone, and now is also given denosum-ab. The bone scan continues to progress six
months after treatment, and his pain worsens. He then goes on docetaxel and prednisone. He gets a good response after eight cycles. His pain improves. However, after two more cycles, his PSA goes up to 10 and then to 20. He gets very bad pain. He has a re-peat bone scan and now he has a lot of problems in his thoracic spine, but no epi-dural lesions.What would you do for this gentleman who’s wracked with pain and has failed multiple therapies? The
choices are to give (1) isotope therapy with samarium; (2) isotope therapy with radi-um-223; (3) palliative focal radiation to the thoracic spine; (4) abiraterone; or (5) enzalu-tamide.Okay, 60% of the group says radium-223. Twenty-three percent went with pallia-tive care, 11% with samarium, and 6% with enzalutamide. No one chose abiraterone.Radium-223 is only available on compassion-ate release at a few centers around the US. Susan, what are your thoughts?Slovin: I could probably make an argu-ment for any of these. The only reason I would be reluctant to use enzalutamide is because he is symptomatic and you want to get him out of his misery. If one were to assume radium-223 was FDA-approved, I probably would be us-ing that, either alone or in concert with another chemotherapy, if we had it, in a clinical trial. Cabazitaxel would be very reasonable, as well.
Petrylak: There is a clinical trial avail-able for this patient in the early stages of his disease. For those patients who do not normalize their PSA to less than 4, SWOG is looking at early abiraterone prior to progression. Second, Susan’s right: You can make an argument for anything here. I wouldn’t be so sure about using enzalutamide, though, be-cause you’ve had already a short initial response to hormones, and you’ve seen abiraterone, so I don’t think he’s going to respond to that. I would agree with going with radium-223.Gomella: Are there any questions from the audience?Audience member: We never really talked about intermittent androgen therapy. What do the panelists think about that?Dreicer: The intermittent therapy ques-tion has been addressed by two ran-domized trials. If a patient has non-metastatic disease, had radiation, and is deemed appropriate for hormones, I think there’s reasonable data from the Canadian trial, which suggests that it’s equivalent.4 The US intergroup trial led by SWOG addressed the question of in-termittent therapy versus continuous in metastatic patients.5 I think the data are
reasonably obvious that intermittent therapy is likely to be inferior to con-tinuous therapy in a majority of those patients. And I think, for the majority of patients, continuous therapy should be
the standard of care. Audience member: What are your thoughts on the role of the sodium fluo-ride PET/CT bone scan?Dreicer: The problem with these new technologies is that they’re beginning to define what we’ve always known was happening. For example, we know that many patients with rapidly short-ening PSA doubling time have systemic disease. We have clinically managed these patients for a long time using the technology that we have. So, if you have a positive bone scan or CT, you say you have radiographic evidence of metastases. So the question is: As we have better tests that resolve things earlier, have we gotten smart enough to intervene and use that information meaningfully? And I would argue right now we’re in a sort of in-between, and it’s going to screw things up for a while. We do trials for nonmetastatic disease based on bone scans. But Mr. X who’s on a trial could go over to the neigh-borhood mobile PET imaging store and learn that he has metastases—even though he was on the trial because we thought he didn’t have metastases. The larger issue that will play out is that, if we are in a value-based care environ-ment and the test helps us take care of people and they do better, it’ll likely get used. If it doesn’t, and it’s a lot more expensive, I think we’ll have to make a choice. TTN
1. National Cancer Institute. The Prostate Cancer
Prevention Trial. National Cancer Institute at the
National Institutes of Health. http://www.cancer.
gov/clinicaltrials/noteworthy-trials/pcpt/Page1.
Accessed March 27, 2013.
2. Roehrborn CG, Barkin J, Siami P, et al. Clinical
outcomes after combined therapy with dutasteride
plus tamsulosin or either monotherapy in men with
benign prostatic hyperplasia (BPH) by baseline
characteristics: 4-year results from the random-
ized, double-blind Combination of Avodart and
Tamsulosin (CombAT) trial. BJU Int. 2011;107(6):
946-954.
3. Lippman SM, Klein EA, Goodman PJ, et al. Effect
of selenium and vitamin E on risk of prostate can-
cer and other cancers: the Selenium and Vitamin
E Cancer Prevention Trial (SELECT). JAMA. 2009;
301(1):39-51.
4. Crook JM, O’Callaghan CJ, Graeme D, et al.
Intermittent androgen suppression for rising PSA
level after radiotherapy. N Engl J Med. 2012;367:
895-903.
5. Hussain M, Tangen CM, Higano CS, et al. Inter-
mittent (IAD) versus continuous androgen depriva-
tion (CAD) in hormone sensitive metastatic pros-
tate cancer (HSM1PC) patients (pts): results of
S9346 (INT-0162), an international phase III trial. J Clin Oncol. 2012;30 (suppl; abstr 4).
“The other trend that’s interesting is that the hormone therapy is kind of going away, except in really high-risk patients, and that it’s being continued for less than two years, while the radiation dose is going up.”
—E. David Crawford, MD
E. David Crawford, MD

Feature
Targeted Therapy News • 5.13
24
In advance of the 2013 American So-ciety of Clinical Oncology (ASCO) an-nual meeting, Targeted Therapy News
spoke with this year’s chair of the Sci-entific Program Committee, Douglas Yee, MD, about key presentations and sessions that attendees can expect.
TTN: As the chair of the scientific committee for this year’s meeting, what are the new types of sessions for this upcoming year or new ways for clinicians and researchers to interact at the meeting?Yee: The one concept we tried last year at the meeting and expanded this year is post-plenary sessions. The plenary session is meant to highlight the highest-impact science sub-mitted to ASCO, but to have a discussion with the presenter about what the results actu-ally mean is difficult because of the thou-sands of people that attend the session. The post-plenary session is a way for the presenter and several discus-sants to really put a spotlight on the ple-nary session data. This is an opportunity for a presentation that is nonscripted and for viewers of the pre-sentation to engage with the presenter and discussants. These sessions take place immediately after the plenary presentations.
TTN: Could you highlight the role of the pre-meeting session? This is a new addition to the annual meeting that started in 2012.Yee: The premeeting has a few impor-tant sessions. There is a session on clinical trials with molecular selection of molecular biomarkers that is par-ticularly relevant in this day and age. As targeted agents move forward in development, they likely work only in a select number of patients within a particular cancer type. In the context of molecular analysis, how do we design trials and develop therapies? The ses-sion is useful for anyone who wants a deep-dive into how to design biomark-er-driven trials.
for both of these scenarios. One of the [sessions] I think that members may not attend as much compared to other sessions are the developmental thera-peutics sessions. In these sessions you can really begin to discuss ‘if we have an EGFR inhibitor and a PI3K inhibi-tor, how do we begin to put those to-gether across different cancer types?’ I think for me that is the aspect of the meeting program that is particularly interesting; how do we use the infor-
TTN: What do you see as a challenge in coor-dinating and planning the meeting?Yee: The general challenge of ASCO has to do with the size and scope of the sci-ence. On one hand, it is an incredible meeting because there is such a broad representation of the latest that is go-ing on in every facet of oncology clini-cal research and the science of oncol-ogy. But at the same time, it is such a big meeting that you don’t necessar-ily get to attend all of the venues you would like and interact with everyone you want to interact with. I think the program committee has been particu-larly conscious of this. We need big
sessions to present the important data, but we also need smaller sessions to foster bet-ter interactions. At the same time, we also want to have sessions where experts in their field can really discuss what they think of new developments in clini-cal and basic science research.
TTN: Translational medi-cine has been a major theme of the meeting and continues to be so for this year. Could you highlight
how scientists and clinical researchers are collaborating and transferring information from the laboratory bench to the clinical setting and vice versa? Are there any ses-sions that will particularly highlight this communication?Yee: I think that is actually a challenge of the state of oncology in general. We now understand that there are spe-cific molecular targets that are critical for tumor biology, and these molecu-lar targets exist across broad types of tumors. We have drugs that have sub-stantial activity in targeting specific tumor types, the HER2 targeted thera-pies in breast cancer, for example. At the same time, there are other drugs available with activity across many cancer types. New therapies that target the mTOR/PI3K pathway, for example, need to be discussed and understood in a deeper way. I think the educational sessions are particularly important
mation obtained from model systems to develop new therapeutics for cancer treatment? At the same time, anyone interested in a particular cancer type can stay on top of their specific field by attending the right sessions. This is what makes the meeting worthwhile—it is an opportunity for people to catch up on what they need to know.
A Guide to ASCO 2013: Key Targeted Trials An Interview with Douglas Yee, MD, Scientific Program Chair
By Anna Azvolinsky, PhD
Douglas Yee, MD
Trial Data to Be Presented at ASCO 2013
1. Colorectal cancer: KRAS/NRAS and BRAF mutation status biomarker analysis in the phase 3 PRIME trial. Abstract #3511. A new, prospective biomarker analysis will be presented from the PRIME ‘203 trial of panitumumab plus FOLFOX versus FOLFOX as first-line treatment for wild-type KRAS metastatic colorectal cancer (mCRC). Patient tumor samples were assessed for additional RAS mutations. The additional mutations in RAS were associated with an inferior progression-free survival and overall survival in the trial, according to the abstract.
2. Breast cancer: A phase II randomized trial of lapatinib with either vinorelbine or capecitabine as first- and second-line therapy for HER2 overexpressing metastatic breast cancer (MBC). Abstract #516.
3. Melanoma: OPTiM: a randomized phase 3 trial of talimogene laherparepvec (T-VEC) vs subcutaneous (SC) granulocyte-macrophage colony-stimulating factor (GM-CSF) for the treatment (tx) of unresected stage IIIB/C and IV melanoma. Abstract #LBA9008.
4. Melanoma: Phase I combination results of nivolumab plus ipilimumab dose-escalation study in metastatic melanoma patients (NCT01024231). Abstract # pending.
5. Ovarian cancer: Randomized, double-blind, phase III trial of pazopanib versus placebo in women who have not progressed after first line chemotherapy for advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer (AOC): Results of an international Intergroup trial (AGO-OVAR16). Abstract #LBA5503.
6. Cervical cancer: Incorporation of bevacizumab in the treatment of recurrent and metastatic cervical cancer: A phase III randomized trial of the Gynecologic Oncology Group. Abstract #3. Results were made public in February 2013 when an interim analysis demonstrated that patients with advanced, recurrent, or persistent cervical cancer not curable with standard treatment who received bevacizumab lived 3.7 months longer than patients treated with chemotherapy alone. This is the first study to demonstrate that a targeted agent significantly improved overall survival in gynecologic cancer.
7. Glioblastoma: Final results of the phase III CENTRIC Trial: cilengitide combined with standard treatment for patients with newly diagnosed glioblastoma with O6-methylguanine-DNA methyltransferase (MGMT) promoter methylation. Abstract #LBA2009.
8. Peripheral T-cell lymphoma: Results of the BELIEF registrational phase 2 trial: Belinostat, a novel pan-histone deacetylase inhibitor (HDACi), in relapsed or refractory peripheral T-cell lymphoma (R/R PTCL). Abstract #8507.
(continued on page 26)

A phase II, multicenter, single-arm study of oral LDK378 in adult patients with ALK-positive non-small cell lungcancer previously treated with chemotherapy and crizotinib
Patients who have had prior chemotherapy and crizotinib
NOW ENROLLING
LDK378 750 mg po qd
Inclusion criteria:• Histologicallyorcytologicallyconfirmed
diagnosis of locally advanced or metastatic non-small cell lung cancer that is anaplastic lymphoma kinase positive
• Age≥18years• Progression of disease during or within 30 days
of last dose of crizotinib • Prior1-3linesofcytotoxicchemotherapy,1of
which must have been a platinum doublet• Crizotinib must be the most recent therapy• Archival tissue sample available
Exclusion criteria:• Systemic anticancer therapy given after the last
dose of crizotinib and prior to starting study drug• Symptomatic central nervous system metastases
that are neurologically unstable or required an increase in steroid dose within 2 weeks prior to study entry
• History of carcinomatous meningitis• Clinicallysignificant,uncontrolledheartdisease• Presence or history of a malignant disease other than
non-small cell lung cancer that has been diagnosed and/or required therapy within the past 3 years
End PointsPrimary: ORRbyRECISTv1.1Secondary:DOR,DCR,TTR,ORRbyBIRCassessment,Safety,PFS,OS
ORR,indicatesoverallresponserate;RECIST,ResponseEvaluationCriteriaInSolidTumors;DOR,durationofresponse;DCR,diseasecontrolrate;TTR,timetoresponse;BIRC,blindedindependentreviewcommittee;PFS,progression-freesurvival;OS,overallsurvival.
© 2013 NovartisNovartis Pharmaceuticals CorporationEast Hanover, New Jersey 07936-1080 5/13 ONC-1064101
LDK378 is an investigational compound. Efficacy and safety has not been established. There is no guarantee that LDK378 will become commercially available.
For more information, please visit www.novartis.com or www.clinicaltrials.gov (NCT01685060)
Unbranded_LDK_Novartis_ClinicalTrials_King.indd 1 5/10/13 9:40 AM

Feature
Targeted Therapy News • 5.13
26
TTN: As a breast cancer clinician and re-searcher, are there any clinical trial sessions or data that you are particularly looking forward to?Yee: For someone trying to stay up to date on the breast cancer field, it is challenging to think about the HER2-positive subset of breast cancer be-cause there are a lot of choices and it is not entirely clear how to best sequence the use of these new drugs. Therapies that target the estrogen receptor are also challenging because there are new therapies that can be used to target the estrogen receptor and other signaling pathways, like the mTOR inhibitors and the new investigational CDK4/6 antagonists, for example. The chal-
lenge is how to bring these new drugs into clinical practice, and, in meaning-ful clinical trials for women with ad-vanced disease, how to control their disease with a goal of prolonging their overall survival and also impacting their quality of life in a positive way. At the same time, how do we take these strategies to the adjuvant setting to op-timize their use when we know that not all patients will benefit from an mTOR inhibitor or the CDK4/6 inhibitor? New trials will begin to address this.
TTN: How will T-DM1, which has recently been approved for HER2-positive metastatic breast cancer, fit into the current treatment paradigm for HER2-positive cancer?Yee: I think T-DM1 is an incredibly interesting development, and this is
the successful use of this strategy on the scale of HER2-positive breast can-cer is a very important advance. It represents another way to treat HER2-positive breast cancer that almost has nothing to do with the mechanism of action of HER2 in the tumor.
How T-DM1 fits into the treatment landscape is not certain and will re-quire further investigation. I am part of the I-SPY 2 clinical trial [NCT01042379], which is bringing certain drugs into the neoadjuvant setting to treat breast
coming from someone who is a lab-oratory-based researcher who is in-terested in the mechanisms of action of growth factor receptors and what they do biologically and how you tar-get them. In many ways, T-DM1 rep-resents something different. T-DM1 has shown us that without fully un-derstanding how a target works bio-logically, we can use an antibody to bind to the target so that it internal-izes a toxin attached to the antibody. So now we have to understand the linker chemistry, the linker between the toxin and the antibody, which is likely the key to how the molecule works or doesn’t work. This concept has been around for some time, but
cancer. We will be offering both pertu-zumab and T-DM1 in the neoadjuvant setting for HER2-breast cancer. The ad-vantage of the trial is that we take and analyze samples to develop biomark-ers to predict response and resistance. Once we understand this—which tu-mors benefit from T-DM1 or pertuzum-ab or trastuzumab or any combina-tion—we will be better able to individ-ualize care for our patients. Right now, the correct sequence of therapies and for which patients with advanced can-cer is not known. Since we don’t know this information, it will be a challenge to use these drugs in the adjuvant set-ting.
TTN: What are the sessions that you will be attending at the annual meeting this year?Yee: One of the best parts of ASCO is attending sessions on topics you know very little about. I am very interested in the educational session on comparative effectiveness research in oncology. The idea is that we can learn from patients that are not enrolled in clinical trials to provide better care. I will also attend sessions on how preclinical research can best guide clinical trial design. I am very interested in the new immu-notherapy developments. I am not an immunotherapist, but one thing that I have learned from attending many ASCO meetings is that you can learn quite a lot about a topic you may not know very well, and then think about how to apply the knowledge to your own clinical practice or research. TTN
Once we understand this—which tumors benefit from T-DM1
or pertuzumab or trastuzumab or any
combination—we will be better able to
individualize care for our patients.
—Douglas Yee, MD
(continued from page 24)

A phase II, multicenter, single-arm study of oral LDK378 in crizotinib-naive adult patients with ALK-positive non-small cell lung cancer
Patients who have had prior chemotherapy
NOW ENROLLING
LDK378 750 mg po qd
Inclusion criteria:• Histologicallyorcytologicallyconfirmed
diagnosis of locally advanced or metastatic non-small cell lung cancer that is anaplastic lymphoma kinase positive
• Age≥18years• 1-3linesofpriorchemotherapy(1ofwhich
must have been a platinum doublet) and progression of disease after last chemotherapy
• Archival tissue sample available
Exclusion criteria:• Prior treatment with an ALK inhibitor• Symptomatic central nervous system
metastases that are neurologically unstable or required an increase in steroid dose within 2 weeks prior to study entry
• History of carcinomatous meningitis• Clinicallysignificant,uncontrolledheartdisease• Presence or history of a malignant disease
other than non-small cell lung cancer that has been diagnosed and/or required therapy within the past 3 years
End PointsPrimary: ORRbyRECISTv1.1Secondary:DOR,DCR,TTR,ORRbyBIRCassessment,Safety,PFS,OS
ORR,indicatesoverallresponserate;RECIST,ResponseEvaluationCriteriaInSolidTumors;DOR,durationofresponse;DCR,diseasecontrolrate;TTR,timetoresponse;BIRC,blindedindependentreviewcommittee;PFS,progression-freesurvival;OS,overallsurvival.
LDK378 is an investigational compound. Efficacy and safety has not been established. There is no guarantee that LDK378 will become commercially available.
For more information, please visit www.novartis.com or www.clinicaltrials.gov (NCT01685138)
Novartis Pharmaceuticals CorporationEast Hanover, New Jersey 07936-1080 ONC-1064102© 2013 Novartis 5/13
Unbranded_LDK_Novartis_ClinicalTrials_King.indd 2 5/10/13 9:40 AM

Research Profile
Targeted Therapy News • 5.13
28
Working in a laboratory at the National Institutes of Health, Benjamin W. Purow, MD, became the first re-searcher to demonstrate that the Notch pathway plays a role in gliomas. Today, he is pursuing the pathway at the University of Virginia School of Medicine in Char-lottesville. He spends the majority of his time in the lab, where his research focuses on glioblastomas, the most common and most lethal primary brain tumors, with the ultimate goal of developing new therapies for this deadly disease. The remainder of his time is spent in the clinic and with patients in whom these treat-ments may one day be applied.
How does the research in your laboratory relate to Notch signaling and cancer?Our primary focus is on glioblastoma brain tumors, and we are interested in a number of novel therapeu-tic approaches to these and other kinds of cancer. One of the foci of the lab is targeting the Notch pathway in these tumors. But we are also interested in other novel targets such as microRNAs, which we transitioned into through some of our Notch studies several years ago. We are interested in microRNAs both upstream and downstream of Notch (in other words, those that could regulate Notch or that are themselves being regulated by Notch). We have found some microRNAs that sup-press the Notch pathway and offer a potential thera-peutic angle in these tumors, though we face the sig-nificant challenge of efficient delivery to brain tumors.
Why does Notch make a promising target for cancer therapy?Notch has been attracting increasing interest in oncol-ogy in recent years, although the first evidence came from some much older studies that showed that if you engineered a constitutively active form of the Notch protein into mice it could lead to T-cell leukemia. That was a beautiful indication that Notch activity could be causal or at least tumor−promoting in certain can-cers. Since then, Notch has actually been found to play opposing roles in different kinds of cancer. In certain cancers, such as gliomas/glioblastomas, Notch seems to play a pro-tumor role. Interestingly though, in some cancers (such as T-cell leukemia) it plays a “classic” oncogenic role; in others it displays tumor-promoting activity without common mutations or amplifications in the gene. Then there are other cancers where it plays more of a tumor−suppressive role, such as skin and lung cancers and possibly B-cell malignancies, in which the Notch pathway is suppressed to foster tumorigenic activity.
Another reason that interest in the Notch pathway has been enhanced is that we had small-molecule in-hibitors ready and waiting in the wings that had origi-nally been developed for use in Alzheimer patients: the gamma secretase inhibitors (or GSIs), which block the enzymatic processing of a number of different proteins, including Notch. A lot of clinical research thus far has focused on testing these inhibitors in various cancers.
Finally, we tend to think of cancers as very primi-tive kinds of cells, stem cells gone awry, or mature cells that have reverted to a more primitive state, and, since Notch has a key role in maintaining the stem-cell state, it makes sense that it may have a role in fostering the development of cancers. Furthermore, in recent years
we have realized that not all cancer cells are the same, and in a lot of cancers there seems to be a subset called cancer stem cells, which may be the original cells that got the tumor going and replenish the tumor after treat-ment with traditional therapies. By targeting Notch, we may be able to get leverage against these cells and sen-sitize cancers to chemotherapy or radiation treatment.
What is the most significant recent development relating to Notch signaling in cancer?There have been a lot of really fascinating develop-ments in recent years. With respect to the end goal of getting agents approved for use in patients, the trials in T-cell leukemia were actually somewhat disappoint-ing. There were some serious toxicity issues with the GSIs. Researchers are now finding ways to get around this— with weekly dosing, for example—and there are ongoing clinical trials in a number of different cancers. Some of the pharmaceutical companies have been somewhat discouraged by the results of trials with a Notch inhibitor as a single agent, but it seems there may be increasing enthusiasm for combining Notch with other agents to sensitize cancer cells to chemo-therapy or other anticancer agents. Also, Notch (spe-cifically the delta-like ligand 4 [DLL4]) has been found to play an important role in angiogenesis (new blood vessel development). Monoclonal antibodies directed against DLL4 have been shown to significantly disrupt the tumor vasculature. One caveat of this is that it may lead to a certain kind of blood vessel tumor, so further work is clearly needed.
In your opinion, which of the Notch-targeted agents holds the most promise?The gamma-secretase inhibitors are very nonspecific. They block processing of a number of proteins and af-fect a whole range of cellular processes, as well as being very nonspecific within the pathway itself, inhibiting all of the different Notch receptors. There have been hints that we might gain benefits from more selec-tive and targeted inhibition of a single Notch receptor or ligand, and a number of pharmaceutical companies are working on developing antibodies to block these proteins. Interestingly, antibodies that activate cer-tain Notch family members are also being looked at, and these may have interesting applications in tumors where Notch has a tumor-suppressive role. I think these more specific agents probably hold the most promise at the moment.
What are the major hurdles to the development of Notch-targeted anticancer agents?Notch is not an enzyme, so developing drugs to block it has been a challenge. Enzymes, like kinases, are much more easily druggable. It was a bit of luck really that there is a druggable protein that processes Notch, namely gamma-secretase. Another issue has been the diversity and sheer level of complexity within the path-way; there are four Notch receptors and several differ-ent ligands as well, and it’s starting to become clear that they can have different functions within the cell. A third issue is the toxicity I mentioned. It is not harm-less to block Notch, with side effects like severe diar-rhea. All of these present significant challenges in the pursuit of Notch-targeting agents. TTN
Notch Holds Promise, but Presents Obstacles as Cancer Target
Benjamin W. Purow, MDAssociate ProfessorClinical Neurology University of Virginia School
of MedicineCharlottesville, VA

Evidence-Based Oncology
Targeted Therapy News • 5.13
29
Targeted Therapy
Matthew Farber
Bruce J. Gould, MD
Bundled Payment: Practice Savior or Killer?By Kurt Ullman
The new “in” term among those looking to lower the cost of health-care is “bundled payment” (BP).
Although there is still disagreement about what it means, the bundling of payments revolves around oncologists being paid a set fee for managing their patients’ care.
“Five or ten years ago, the oncology spend was not high on the payer’s pri-ority list,” said Mat-thew Farber, direc-tor of Provider Eco-nomics and Public Policy at the Asso-ciation of Commu-nity Cancer Centers in Rockville, Mary-land. “As the num-ber of patients goes up, the number of those who survive increases, and as the general demo-graphic shifts, the cost of cancer care goes up. In addition, the recent run of new (and expensive) drug approvals has caused payer’s focus to turn toward oncology.”
Concerns about BP in cancer treatmentTrue bundled payments would give on-cologists a set amount of money per patient to cover all costs from initial visit through to discharge from care or to hospice. There are concerns that a BP system would not work in cancer treatment, and could cause disruptions in practices.
One reason is that cancers are a very individualized and diverse group of diseases. To say that a payer will offer a set amount of money for two lines of treatment does not address who is responsible should a third be needed. There is enough variability in oncol-ogy that true BP is likely to be prob-lematic.
“Oncologists do not take care of large populations of patients, where you can mitigate the risk of outliers who utilize a lot of costs, time, and energy,” said Bruce J. Gould, MD, medical director of Northwest Georgia Oncology Cen-ters in Marietta, Georgia. “Any payment system has to reflect this so that one or two expensive patients don’t break a practice.”
Because of this, it is important for practices to take a long and close look at their processes and find ways to
streamline them. Physicians, according to both experts, should look to imple-ment established clinical guidelines as a first step. But they will also need to update information-gathering abili-ties through use of electronic medi-cal record (EMR) programs tracking both what they are doing well and where they need to improve.
What practices should considerCompare current treatment modali-ties with guidelines from the National C o m p r e h e n s i v e Cancer Network (NCCN) or other professional sources. Getting a physi-cian to buy in is important, as just one physician opting out of the predeter-mined treatment regimens could harm the program for all. This also highlights the need for ways to monitor compli-ance.
Full commitment to EMR technology is another important part of this puz-zle. Both BP and EOC require practices to have the ability to monitor, docu-ment, and report treatment regimens.
Episode of care a better fit?The model that may be the best pay-ment fit for oncologists is episode of care (EOC). As currently evolving, this model transfers a specific part of the risk to the oncologists, but one that is easier to manage.
Gould’s group is participating in an early pilot study in cooperation with United Healthcare. The participants defined 19 cat-egories for lung, breast, and colon cancers.
“They have tak-en our margins for chemotherapy medications, add-ed extra money for hospitalizations, and that is what we get when a pa-tient is registered
as an EOC fee,” said Gould. “We are still paid a fee for service when we see the patients in our offices and to adminis-ter the medications. The drugs are re-imbursed at Average Sales Price.”
The insurance company knows what its medicine costs will be and the most it has to spend for physician services should its enrollees need hospital treatment. It hopes to save money by giving oncologists incentives to treat patients in the office (where they get paid) and not in the hospital. Hospital in-patient costs are still paid by the in-surance company. The oncologists are only assuming the risk for their in-hos-pital services.
Shifts in how practices make moneyHow practices make their money is shifting, and getting the bulk of in-come from drug charges is past. Other responses by oncologists such as pay for administering medications and in-creasing in-office diagnostic radiology have come under greater scrutiny.
“This gradual reduction in payment is a long-term trend that practices have to recognize to stay afloat,” said Farber. “I think eventually fee for service for both Medicare and private insurers is going down. Instead they will pay for better, more efficient, and less duplica-tive care.”
These systems help analyze costs, an important part of the process when ne-gotiating fees and managing costs.
Business management may play as big a role in a practice’s profitability as the medical management side. For example, the efficiency and accuracy of coding and billing staff will impact cash flow.
“The investment in a strong manage-ment team is not cheap, but will pay dividends and keep practices strong and independent,” said Gould. “Over the last few years, all of the fat has been removed from the system. If you don’t have a lean, mean practice that is collecting every penny due you on the first try, the chances the practice will fold increase.”
How long to get ready? There is some disagreement on how long practices have to get ready for whichever system wins out. Gould thinks the “ability to worry about to-morrow is gone,” with an immediate need to get the office in order.
On the other hand, Farber thinks there is still time for practices to watch the early adopters work out the kinks.
Both agree that keeping track of the various models as they mature is important so that practices are “lean-ing” the right way when approached. They also concur that things like es-tablishing EMRs and familiarizing physicians with guidelines should begin immediately. TTN
Author Affiliation:
From KVU Commu-
nication, Inc, Carmel, IN.
Funding Source: None.
Author Disclosure: Mr Ullman reports no re-
lationship or financial interest with any
entity that would pose a conflict of inter-
est with the subject matter of this article.
Authorship Information: Drafting of the
manuscript; critical revision of the manu-
script for important intellectual content;
and administrative, technical, or logistic
support; and supervision.
“I think eventually fee-for-service for both Medicare and private insurers is going down. Instead, they will pay for better, more efficient, and less duplicative care.”
—Matthew Farber

JOB#: Q23261B CLIENT: Kadcyla DESC: JA Tabloid FILE NAME: GNH_TDM_Q23261B_JA_M04.indd DATE: 2-26-2013 4:34 PM ROUND: 1PG: millerk/Kaminski, Chris AD: Andy Warhol ext: 111 TC: EA AE: None CW: None Last Saved: 2-26-2013 4:34 PMTRIM: 25” x 17” BLEED: None SAFETY: None PROD: Haight INK Spec: 4C PRINT SCALE: 75%FONTS: Univers LT Std (67 Bold Condensed, 47 Light Condensed, 65 Bold, 45 Light, 45 Light Oblique), Conduit ITC (Bold, Medium), Univers (65 Bold, 45 Light, 45 Light Oblique), TT Slug OTF (Regular)
IMAGES: 23261B_JA_2_fn.tif (CMYK; 300 ppi; 100%), Kadcyla_TM_4C.ai (70%, 66%), 23261B_OS chart_pg3.eps (100%), Genentech_AMOTRG_4C.eps (88%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: Macintosh HD:Users:millerk:Des...61 e b:GNH_TDM_Q23261B_JA_M04.inddNOTES: None
GNH_TDM_Q23261B_JA_D01.indd Galley: 2
S&H PharmaGraphics
DISK RELEASE
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
2d1 Q1 Q2Cosmos Communications 718.482.1800
24298a1 03.1.13 133K
KADCYLA™ (ado-trastuzumab emtansine)
Injection for intravenous useInitial U.S. Approval: 2013This is a brief summary of information about KADCYLA. Before prescribing, please see full Prescribing Information.
Do Not Substitute KADCYLA for or with Trastuzumab
WARNING: HEPATOTOXICITY, CARDIAC TOXICITY, EMBRYO-FETAL TOXICITY
• Hepatotoxicity: Serious hepatotoxicity has been reported, including liver failure and death in patients treated with KADCYLA. Monitor serum transaminases and bilirubin prior to initiation of KADCYLA treatment and prior to each KADCYLA dose. Reduce dose or discontinue KADCYLA as appropriate in cases of increased serum transaminases or total bilirubin. (2.2, 5.1)
• Cardiac Toxicity: KADCYLA administration may lead to reductions in left ventricular ejection fraction (LVEF). Evaluate left ventricular function in all patients prior to and during treatment with KADCYLA. Withhold treatment for clinically significant decrease in left ventricular function. (2.2, 5.2)
• Embryo-Fetal Toxicity: Exposure to KADCYLA can result in embryo-fetal death or birth defects. Advise patients of these risks and the need for effective contraception. (5.3, 8.1, 8.6)
1 INDICATIONS AND USAGEKADCYLA™, as a single agent, is indicated for the treatment of patients with HER2-positive, metastatic breast cancer who previously received trastuzumab and a taxane, separately or in combination. Patients should have either:• Received prior therapy for metastatic disease, or• Developed disease recurrence during or within six months of
completing adjuvant therapy.
4 CONTRAINDICATIONSNone.
5 WARNINGS AND PRECAUTIONS
5.1 HepatotoxicityHepatotoxicity, predominantly in the form of asymptomatic, transient increases in the concentrations of serum transaminases, has been observed in clinical trials with KADCYLA [see Adverse Reactions (6.1)]. Serious hepatobiliary disorders, including at least two fatal cases of severe drug-induced liver injury and associated hepatic encephalopathy, have been reported in clinical trials with KADCYLA. Some of the observed cases may have been confounded by comorbidities and/or concomitant medications with known hepatotoxic potential.
Monitor serum transaminases and bilirubin prior to initiation of KADCYLA treatment and prior to each KADCYLA dose. Patients with known active hepatitis B virus or hepatitis C virus were excluded from Study 1 [see Clinical Studies (14.1)]. Reduce the dose or discontinue KADCYLA as appropriate in cases of increased serum transaminases and/or total bilirubin [see Dosage and Administration (2.2)]. Permanently discontinue KADCYLA treatment in patients with serum transaminases > 3 x ULN and concomitant total bilirubin > 2 x ULN. KADCYLA has not been studied in patients with serum transaminases > 2.5 x ULN or bilirubin > 1.5 x ULN prior to the initiation of treatment.
In clinical trials of KADCYLA, cases of nodular regenerative hyperplasia (NRH) of the liver have been identified from liver biopsies (3 cases out of 884 treated patients). Two of these three cases of NRH were observed in the randomized trial (Study 1) [see Adverse Reactions (6.1)]. NRH is a rare liver condition characterized by widespread benign transformation of hepatic parenchyma into small regenerative nodules; NRH may lead to non-cirrhotic portal hypertension. The diagnosis of NRH can be confirmed only by histopathology. NRH should be considered in all patients with clinical symptoms of portal hypertension but with normal transaminases and no manifestations of cirrhosis. Upon diagnosis of NRH, KADCYLA treatment must be permanently discontinued.
5.2 Left Ventricular DysfunctionPatients treated with KADCYLA are at increased risk of developing left ventricular dysfunction. A decrease of LVEF to < 40% has been observed in patients treated with KADCYLA. In the randomized trial (Study 1), left ventricular dysfunction occurred in 1.8% of patients in the KADCYLA-treated group and 3.3% of patients in the lapatinib plus capecitabine-treated group [see Adverse Reactions (6.1)].
Assess LVEF prior to initiation of KADCYLA and at regular intervals (e.g. every three months) during treatment to ensure the LVEF is within the institution’s normal limits. Treatment with KADCYLA has not been studied in patients with LVEF < 50% prior to initiation of treatment. If, at routine monitoring, LVEF is < 40%, or is 40% to 45% with a 10% or greater absolute decrease below the pretreatment value, withhold KADCYLA and repeat LVEF assessment within approximately 3 weeks. Permanently discontinue KADCYLA if the LVEF has not improved or has declined further [see Dosage and Administration (2.2)]. Patients with a history of symptomatic congestive heart failure (CHF), serious cardiac arrhythmia, or history of myocardial infarction or unstable angina within 6 months were excluded from Study 1 [see Clinical Studies (14.1)].
5.3 Embryo-Fetal Toxicity KADCYLA can cause fetal harm when administered to a pregnant
woman. There are no adequate and well-controlled studies of KADCYLA in pregnant women and no reproductive and developmental toxicology studies have been conducted with ado-trastuzumab emtansine. Nevertheless, treatment with trastuzumab, the antibody component of KADCYLA, during pregnancy in the postmarketing setting has resulted in oligohydramnios, some associated with fatal pulmonary hypoplasia, skeletal abnormalities and neonatal death. DM1, the cytotoxic component of KADCYLA, can be expected to cause embryo-fetal toxicity based on its mechanism of action.
If KADCYLA is used during pregnancy, or if the patient becomes pregnant while receiving KADCYLA, apprise the patient of the potential hazard to the fetus [see Use in Specific Populations (8.1)].Verify pregnancy status prior to the initiation of KADCYLA. Advise patients of the risks of embryo-fetal death and birth defects and the need for contraception during and after treatment. Advise patients to contact their healthcare provider immediately if they suspect they may be pregnant. If KADCYLA is administered during pregnancy or if a patient becomes pregnant while receiving KADCYLA, immediately report exposure to the Genentech Adverse Event Line at 1-888-835-2555. Encourage women who may be exposed during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720 [see Patient Counseling Information (17)].
5.4 Pulmonary ToxicityCases of interstitial lung disease (ILD), including pneumonitis, some leading to acute respiratory distress syndrome or fatal outcome have been reported in clinical trials with KADCYLA. Pneumonitis at an incidence of 0.8% (7 out of 884 treated patients) has been reported, with one case of grade 3 pneumonitis. Signs and symptoms include dyspnea, cough, fatigue, and pulmonary infiltrates. These events may or may not occur as sequelae of infusion reactions. In the randomized trial (Study 1), the overall frequency of pneumonitis was 1.2% [see Adverse Reactions (6.1)].
Permanently discontinue treatment with KADCYLA in patients diagnosed with ILD or pneumonitis.
Patients with dyspnea at rest due to complications of advanced malignancy and co-morbidities may be at increased risk of pulmonary toxicity.
5.5 Infusion-Related Reactions, Hypersensitivity ReactionsTreatment with KADCYLA has not been studied in patients who had trastuzumab permanently discontinued due to infusion-related reactions (IRR) and/or hypersensitivity; treatment with KADCYLA is not recommended for these patients.
Infusion-related reactions, characterized by one or more of the following symptoms − flushing, chills, pyrexia, dyspnea, hypotension, wheezing, bronchospasm, and tachycardia have been reported in clinical trials of KADCYLA. In the randomized trial (Study 1), the overall frequency of IRRs in patients treated with KADCYLA was 1.4% [see Adverse Reactions (6.1)]. In most patients, these reactions resolved over the course of several hours to a day after the infusion was terminated. KADCYLA treatment should be interrupted in patients with severe IRR. KADCYLA treatment should be permanently discontinued in the event of a life-threatening IRR [see Dosage and Administration (2.2)]. Patients should be observed closely for IRR reactions, especially during the first infusion.
One case of a serious, allergic/anaphylactic-like reaction has been observed in clinical trials of single-agent KADCYLA. Medications to treat such reactions, as well as emergency equipment, should be available for immediate use.
5.6 ThrombocytopeniaThrombocytopenia, or decreased platelet count, was reported in clinical trials of KADCYLA (103 of 884 treated patients with ≥ Grade 3; 283 of 884 treated patients with any Grade). The majority of these patients had Grade 1 or 2 events (< LLN to ≥ 50,000/mm3) with the nadir occurring by day 8 and generally improving to Grade 0 or 1 (≥ 75,000 /mm3) by the next scheduled dose. In clinical trials of KADCYLA, the incidence and severity of thrombocytopenia were higher in Asian patients. Independent of race, the incidence of severe hemorrhagic events in patients treated with KADCYLA was low.
In the randomized trial (Study 1), the overall frequency of thrombocytopenia was 31.2% in the KADCYLA-treated group and 3.3% in the lapatinib plus capecitabine-treated group [see Adverse Reactions (6.1)]. The incidence of ≥ Grade 3 thrombocytopenia was 14.5% in the KADCYLA-treated group and 0.4% in the lapatinib plus capecitabine-treated group. In Asian patients, the incidence of ≥ Grade 3 thrombocytopenia was 45.1% in the KADCYLA-treated group and 1.3% in the lapatinib plus capecitabine-treated group.
Monitor platelet counts prior to initiation of KADCYLA and prior to each KADCYLA dose [see Dosage and Administration (2.2)]. KADCYLA has not been studied in patients with platelet counts <100,000/mm3 prior to initiation of treatment. In the event of decreased platelet count to Grade 3 or greater (< 50,000/mm3) do not administer KADCYLA until platelet counts recover to Grade 1 (≥ 75,000/mm3) [see Dosage and Administration (2.2)]. Patients with thrombocytopenia (< 100,000/mm3) and patients on anti-coagulant treatment should be closely monitored during treatment with KADCYLA.
5.7 NeurotoxicityPeripheral neuropathy, mainly as Grade 1 and predominantly sensory, was reported in clinical trials of KADCYLA (14 of 884 treated patients with ≥ Grade 3; 196 of 884 treated patients with any Grade). In the randomized trial (Study 1), the overall frequency of peripheral neuropathy was 21.2% in the KADCYLA-treated group
and 13.5% in the lapatinib plus capecitabine-treated group [see Adverse Reactions (6.1)]. The incidence of ≥ Grade 3 peripheral neuropathy was 2.2% in the KADCYLA-treated group and 0.2% in the lapatinib plus capecitabine-treated group.
KADCYLA should be temporarily discontinued in patients experiencing Grade 3 or 4 peripheral neuropathy until resolution to ≤ Grade 2. Patients should be clinically monitored on an ongoing basis for signs or symptoms of neurotoxicity [see Nonclinical Toxicology (13.2)].
5.8 HER2 TestingDetection of HER2 protein overexpression or gene amplification is necessary for selection of patients appropriate for KADCYLA therapy because these are the only patients studied for whom benefit has been shown [see Indications and Usage (1), Clinical Studies (14.1)]. In the randomized study (Study 1), patients with breast cancer were required to have evidence of HER2 overexpression defined as 3+ IHC by Dako Herceptest™ or evidence of overexpression defined as FISH amplification ratio ≥ 2.0 by Dako HER2 FISH PharmDx™ test kit. Only limited data were available for patients whose breast cancer was positive by FISH and 0 or 1+ by IHC.
Assessment of HER2 status should be performed by laboratories with demonstrated proficiency in the specific technology being utilized. Improper assay performance, including use of sub- optimally fixed tissue, failure to utilize specified reagents, deviation from specific assay instructions, and failure to include appropriate controls for assay validation, can lead to unreliable results.
5.9 Extravasation In KADCYLA clinical studies, reactions secondary to extravasation have been observed. These reactions, observed more frequently within 24 hours of infusion, were usually mild and comprised erythema, tenderness, skin irritation, pain, or swelling at the infusion site. Specific treatment for KADCYLA extravasation is unknown. The infusion site should be closely monitored for possible subcutaneous infiltration during drug administration.
6 ADVERSE REACTIONS The following adverse reactions are discussed in greater detail in other sections of the label: • Hepatotoxicity [See Warnings and Precautions (5.1)]• Left Ventricular Dysfunction [See Warnings and Precautions (5.2)]• Embryo-Fetal Toxicity [See Warnings and Precautions (5.3)]• Pulmonary Toxicity [See Warnings and Precautions (5.4)]• Infusion-Related Reactions, Hypersensitivity Reactions [See
Warnings and Precautions (5.5)]• Thrombocytopenia [See Warnings and Precautions (5.6)]• Neurotoxicity [See Warnings and Precautions (5.7)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In clinical trials, KADCYLA has been evaluated as single-agent in 884 patients with HER2-positive metastatic breast cancer. The most common (frequency ≥ 25%) adverse drug reactions (ADRs) seen in 884 patients treated with KADCYLA were fatigue, nausea, musculoskeletal pain, thrombocytopenia, headache, increased transaminases, and constipation.
The ADRs described in Table 6 were identified in patients with HER2-positive metastatic breast cancer treated in a randomized trial (Study 1) [see Clinical Studies (14.1)]. Patients were randomized to receive KADCYLA or lapatinib plus capecitabine. The median duration of study treatment was 7.6 months for patients in the KADCYLA-treated group and 5.5 months and 5.3 months for patients treated with lapatinib and capecitabine, respectively. Two hundred and eleven (43.1%) patients experienced ≥ Grade 3 adverse events in the KADCYLA-treated group compared with 289 (59.2%) patients in the lapatinib plus capecitabine-treated group. Dose adjustments for KADCYLA were permitted [see Dosage and Administration (2.2)]. Thirty-two patients (6.5%) discontinued KADCYLA due to an adverse event, compared with 41 patients (8.4%) who discontinued lapatinib, and 51 patients (10.5%) who discontinued capecitabine due to an adverse event. The most common adverse events leading to KADCYLA withdrawal were thrombocytopenia and increased transaminases. Eighty patients (16.3%) treated with KADCYLA had adverse events leading to dose reductions. The most frequent adverse events leading to dose reduction of KADCYLA (in ≥ 1% of patients) included thrombocytopenia, increased transaminases, and peripheral neuropathy. Adverse events that led to dose delays occurred in 116 (23.7%) of KADCYLA treated patients. The most frequent adverse events leading to a dose delay of KADCYLA (in ≥ 1% of patients) were neutropenia, thrombocytopenia, leukopenia, fatigue, increased transaminases and pyrexia.
Table 6 reports the ADRs that occurred in patients in the KADCYLA-treated group (n=490) of the randomized trial (Study 1). Selected laboratory abnormalities are shown in Table 7. The most common ADRs seen with KADCYLA in the randomized trial (frequency > 25%) were nausea, fatigue, musculoskeletal pain, thrombocytopenia, increased transaminases, headache, and constipation. The most common NCI–CTCAE (version 3) ≥ Grade 3 ADRs (frequency >2%) were thrombocytopenia, increased transaminases, anemia, hypokalemia, peripheral neuropathy and fatigue.
Adverse Drug Reactions (MedDRA)
System Organ Class
KADCYLA(3.6 mg/kg)
n=490Frequency rate %
Lapatinib (1250 mg) + Capecitabine (2000 mg/m2)
n=488Frequency rate %
All grades (%)
Grade 3 – 4 (%)
All grades (%)
Grade 3 – 4 (%)
Blood and Lymphatic System Disorders
Neutropenia 6.7 2.0 9.0 4.3
Anemia 14.3 4.1 10.5 2.5
Thrombocyto-penia 31.2 14.5 3.3 0.4
Cardiac Disorders
Left ventricular dysfunction 1.8 0.2 3.3 0.4
Eye Disorders
Lacrimation increased 3.3 0 2.5 0
Dry eye 3.9 0 3.1 0
Vision blurred 4.5 0 0.8 0
Conjunctivitis 3.9 0 2.3 0
Gastrointestinal Disorders
Dyspepsia 9.2 0 11.5 0.4
Stomatitis 14.1 0.2 32.6 2.5
Dry Mouth 16.7 0 4.9 0.2
Abdominal pain 18.6 0.8 17.6 1.6
Vomiting 19.2 0.8 29.9 4.5
Diarrhea 24.1 1.6 79.7 20.7
Constipation 26.5 0.4 11.1 0
Nausea 39.8 0.8 45.1 2.5
General Disorders and Administration
Peripheral edema 7.1 0 8.2 0.2
Chills 7.6 0 3.1 0
Pyrexia 18.6 0.2 8.4 0.4
Asthenia 17.8 0.4 17.6 1.6
Fatigue 36.3 2.5 28.3 3.5
Hepatobiliary Disorders
Nodular regenerative hyperplasia*
0.4 ND 0 0
Portal hyperten-sion* 0.4 0.2 0 0
Immune System Disorders
Drug hypersen-sitivity 2.2 0 0.8 0
Injury, Poisoning, and Procedural
Infusion-related reaction 1.4 0 0.2 0
Infections and Infestations
Urinary tract infection 9.4 0.6 3.9 0
Investigations
Blood alkaline phosphatase increased
4.7 0.4 3.7 0.4
Increased transaminases 28.8 8.0 14.3 2.5
Metabolism and Nutrition Disorders
Hypokalemia 10.2 2.7 9.4 4.7
Musculoskeletal and Connective Tissue Disorders
Myalgia 14.1 0.6 3.7 0
Arthralgia 19.2 0.6 8.4 0
Musculoskeletal pain 36.1 1.8 30.5 1.4
Nervous System Disorders
Dysgeusia 8.0 0 4.1 0.2
Dizziness 10.2 0.4 10.7 0.2
Peripheral neuropathy 21.2 2.2 13.5 0.2
Headache 28.2 0.8 14.5 0.8
Psychiatric Disorders
Insomnia 12.0 0.4 8.6 0.2
Respiratory, Thoracic, and Mediastinal Disorders
Pneumonitis 1.2 0 0 0
Dyspnea 12.0 0.8 8.0 0.4
Cough 18.2 0.2 13.1 0.2
Epistaxis 22.5 0.2 8.4 0
Skin and Subcutaneous Tissue Disorders
Pruritus 5.5 0.2 9.2 0
Rash 11.6 0 27.5 1.8
Vascular Disorders
Hypertension 5.1 1.2 2.3 0.4
Table 7 Selected Laboratory Abnormalities
Parameter KADCYLA(3.6 mg/kg)
Lapatinib (1250 mg) +Capecitabine (2000 mg/m2)
All Grade
%Grade 3
%Grade 4
%All
Grade %
Grade 3 %
Grade 4 %
Increased bilirubin 17 <1 0 57 2 0
Increased AST 98 7 <1 65 3 0
Increased ALT 82 5 <1 54 3 0
Decreased platelet count 83 14 3 21 <1 <1
Decreased hemoglobin 60 4 1 64 3 <1
Decreased neutrophils 39 3 <1 38 6 2
Decreased potassium 33 3 0 31 6 <1
Table 6 Summary of Adverse Drug Reactions Occurring in Patients on the KADCYLA Treatment Arm in the Randomized Trial (Study 1)
* Nodular Regenerative Hyperplasia and Portal Hypertension occurred in the same patient.
ND = Not determined
6.2 ImmunogenicityAs with all therapeutic proteins, there is the potential for an immune response to KADCYLA.
A total of 836 patients from six clinical studies were tested at multiple time points for anti-therapeutic antibody (ATA) responses to KADCYLA. Following KADCYLA dosing, 5.3% (44/836) of patients tested positive for anti-KADCYLA antibodies at one or more post-dose time points. The presence of KADCYLA in patient serum at the time of ATA sampling may interfere with the ability of this assay to detect anti-KADCYLA antibodies. As a result, data may not accurately reflect the true incidence of anti-KADCYLA antibody development. In addition, neutralizing activity of anti-KADCYLA antibodies has not been assessed.
Immunogenicity data are highly dependent on the sensitivity and specificity of the test methods used. Additionally, the observed incidence of a positive result in a test method may be influenced by several factors, including sample handling, timing of sample collection, drug interference, concomitant medication and the underlying disease. Therefore, comparison of the incidence of antibodies to KADCYLA with the incidence of antibodies to other products may be misleading. Clinical significance of anti-KADCYLA antibodies is not yet known.
7 DRUG INTERACTIONSNo formal drug-drug interaction studies with KADCYLA have been conducted. In vitro studies indicate that DM1, the cytotoxic component of KADCYLA, is metabolized mainly by CYP3A4 and to a lesser extent by CYP3A5. Concomitant use of strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, clarithromycin, atazanavir, indinavir, nefazodone, nelfinavir, ritonavir, saquinavir, telithromycin, and voriconazole) with KADCYLA should be avoided due to the potential for an increase in DM1 exposure and toxicity. Consider an alternate medication with no or minimal potential to inhibit CYP3A4. If concomitant use of strong CYP3A4 inhibitors is unavoidable, consider delaying KADCYLA treatment until the strong CYP3A4 inhibitors have cleared from the circulation (approximately 3 elimination half-lives of the inhibitors) when possible. If a strong CYP3A4 inhibitor is coadministered and KADCYLA treatment cannot be delayed, patients should be closely monitored for adverse reactions.
8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyPregnancy Category D [see Warnings and Precautions (5.3)]
Risk Summary
KADCYLA can cause fetal harm when administered to a pregnant woman. There are no adequate and well-controlled studies of KADCYLA in pregnant women. No reproductive and developmental toxicology studies have been conducted with ado-trastuzumab emtansine. Nevertheless, two components of KADCYLA (trastuzumab and DM1) are known or suspected to cause fetal harm or death when administered to a pregnant woman. If KADCYLA is administered during pregnancy, or if a patient becomes pregnant while receiving KADCYLA, apprise the patient of the potential hazard to the fetus. Patients should be advised to use effective contraception during treatment with KADCYLA and for 6 months following the last dose of KADCYLA.
If KADCYLA is administered during pregnancy or if a patient becomes pregnant while receiving KADCYLA, immediately report exposure to the Genentech Adverse Event Line at 1-888-835-2555. Encourage women who may be exposed during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720 [see Patient Counseling Information (17)].
Human Data
In the post-marketing setting, treatment with trastuzumab during pregnancy has resulted in cases of oligohydramnios, some associated with fatal pulmonary hypoplasia, skeletal abnormalities and neonatal death. These case reports described oligohydramnios in pregnant women who received trastuzumab either alone or in combination with chemotherapy. In some case reports, amniotic fluid index increased after trastuzumab was stopped. In one case, trastuzumab therapy resumed after the amniotic fluid index improved, and oligohydramnios recurred.
Animal Data
There were no reproductive and developmental toxicology studies conducted with ado-trastuzumab emtansine. DM1, the cytotoxic
component of KADCYLA, disrupts microtubule function. DM1 is toxic to rapidly dividing cells in animals and is genotoxic, suggesting it has the potential to cause embryotoxicity and teratogenicity. In studies where trastuzumab was administered to pregnant monkeys at doses up to 25 mg/kg (about 7 times the clinical dose), trastuzumab crossed the placental barrier during the early and late phases of gestation. The resulting concentrations of trastuzumab in fetal blood and amniotic fluid were approximately 33% and 25%, respectively, of those present in the maternal serum but were not associated with adverse findings.
8.3 Nursing MothersIt is not known whether KADCYLA, specifically, is excreted in human milk, but IgG is known to be excreted in human milk. In lactating monkeys, trastuzumab was excreted in small amounts (about 0.3% of maternal serum concentrations) in breast milk after post-partum doses of 25 mg/kg (about 7 times the clinical dose of KADCYLA). Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from KADCYLA, a decision should be made whether to discontinue nursing or discontinue KADCYLA, taking into account the importance of the drug to the mother [see Warnings and Precautions (5.3)].
8.4 Pediatric UseSafety and effectiveness of KADCYLA have not been established in pediatric patients.
8.5 Geriatric UseOf 495 patients who were randomized to KADCYLA in the randomized trial (Study 1) [see Clinical Studies (14.1)], 65 patients (13%) were ≥ 65 years of age and 11 patients (2%) were ≥ 75 years of age. In patients ≥ 65 years old (n=138 across both treatment arms) the hazard ratios for progression-free survival (PFS) and Overall Survival (OS) were 1.06 (95% CI: 0.68, 1.66) and 1.05 (95% CI: 0.58, 1.91), respectively.
Population pharmacokinetic analysis indicates that age does not have a clinically meaningful effect on the pharmacokinetics of ado-trastuzumab emtansine [see Clinical Pharmacology (12.3)].
8.6 Females of Reproductive PotentialKADCYLA can cause embryo-fetal harm when administered during pregnancy. Counsel patients regarding pregnancy prevention and planning. Advise females of reproductive potential to use effective contraception while receiving KADCYLA and for 6 months following the last dose of KADCYLA.
If KADCYLA is administered during pregnancy or if the patient becomes pregnant while receiving KADCYLA, immediately report exposure to the Genentech Adverse Event Line at 1-888-835-2555. Encourage women who may be exposed during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720 [see Patient Counseling Information (17)].
8.7 Renal ImpairmentNo dedicated renal impairment trial for KADCYLA has been conducted. Based on the population pharmacokinetics, as well as analysis of Grade 3 or greater adverse drug reactions and dose modifications, dose adjustments of KADCYLA are not needed in patients with mild (creatinine clearance [CLcr] 60 to 89 mL/min) or moderate (CLcr 30 to 59 mL/min) renal impairment. No dose adjustment can be recommended for patients with severe renal impairment (CLcr less than 30 mL/min) because of the limited data available [see Clinical Pharmacology (12.3)].
8.8 Hepatic ImpairmentIn vitro studies in human liver microsomes indicates that DM1 is metabolized by CYP3A4/5. The influence of hepatic impairment on the pharmacokinetics of ado-trastuzumab emtansine conjugate has not been determined.
10 OVERDOSAGEThere is no known antidote for overdose of KADCYLA. In clinical trials, overdose of KADCYLA has been reported at approximately two times the recommended dose which resulted in Grade 2 thrombocytopenia (resolved 4 days later) and one death. In the fatal case, the patient incorrectly received KADCYLA at 6 mg/kg and died approximately 3 weeks following the overdose; a cause of death and a causal relationship to KADCYLA were not established.
KADCYLA™ (ado-trastuzumab emtansine)
Manufactured by:Genentech, Inc. 4862200A Member of the Roche Group Initial U.S. Approval: 02/131 DNA Way KADCYLA is a trademarkSouth San Francisco, CA of Genentech, Inc. 94080-4990 02/13 TDM0001661000U.S. License No: 1048 ©2013 Genentech, Inc.
S:6.875”
S:9.875”
T:15.5”
T:10.5”
B:17.5”
B:11.5”
S:6.875”

JOB#: Q23261B CLIENT: Kadcyla DESC: JA Tabloid FILE NAME: GNH_TDM_Q23261B_JA_M04.indd DATE: 2-26-2013 4:34 PM ROUND: 1PG: millerk/Kaminski, Chris AD: Andy Warhol ext: 111 TC: EA AE: None CW: None Last Saved: 2-26-2013 4:34 PMTRIM: 25” x 17” BLEED: None SAFETY: None PROD: Haight INK Spec: 4C PRINT SCALE: 75%FONTS: Univers LT Std (67 Bold Condensed, 47 Light Condensed, 65 Bold, 45 Light, 45 Light Oblique), Conduit ITC (Bold, Medium), Univers (65 Bold, 45 Light, 45 Light Oblique), TT Slug OTF (Regular)
IMAGES: 23261B_JA_2_fn.tif (CMYK; 300 ppi; 100%), Kadcyla_TM_4C.ai (70%, 66%), 23261B_OS chart_pg3.eps (100%), Genentech_AMOTRG_4C.eps (88%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: Macintosh HD:Users:millerk:Des...61 e b:GNH_TDM_Q23261B_JA_M04.inddNOTES: None
GNH_TDM_Q23261B_JA_D01.indd Galley: 2
S&H PharmaGraphics
DISK RELEASE
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
2d1 Q1 Q2Cosmos Communications 718.482.1800
24298a1 03.1.13 133K
KADCYLA™ (ado-trastuzumab emtansine)
Injection for intravenous useInitial U.S. Approval: 2013This is a brief summary of information about KADCYLA. Before prescribing, please see full Prescribing Information.
Do Not Substitute KADCYLA for or with Trastuzumab
WARNING: HEPATOTOXICITY, CARDIAC TOXICITY, EMBRYO-FETAL TOXICITY
• Hepatotoxicity: Serious hepatotoxicity has been reported, including liver failure and death in patients treated with KADCYLA. Monitor serum transaminases and bilirubin prior to initiation of KADCYLA treatment and prior to each KADCYLA dose. Reduce dose or discontinue KADCYLA as appropriate in cases of increased serum transaminases or total bilirubin. (2.2, 5.1)
• Cardiac Toxicity: KADCYLA administration may lead to reductions in left ventricular ejection fraction (LVEF). Evaluate left ventricular function in all patients prior to and during treatment with KADCYLA. Withhold treatment for clinically significant decrease in left ventricular function. (2.2, 5.2)
• Embryo-Fetal Toxicity: Exposure to KADCYLA can result in embryo-fetal death or birth defects. Advise patients of these risks and the need for effective contraception. (5.3, 8.1, 8.6)
1 INDICATIONS AND USAGEKADCYLA™, as a single agent, is indicated for the treatment of patients with HER2-positive, metastatic breast cancer who previously received trastuzumab and a taxane, separately or in combination. Patients should have either:• Received prior therapy for metastatic disease, or• Developed disease recurrence during or within six months of
completing adjuvant therapy.
4 CONTRAINDICATIONSNone.
5 WARNINGS AND PRECAUTIONS
5.1 HepatotoxicityHepatotoxicity, predominantly in the form of asymptomatic, transient increases in the concentrations of serum transaminases, has been observed in clinical trials with KADCYLA [see Adverse Reactions (6.1)]. Serious hepatobiliary disorders, including at least two fatal cases of severe drug-induced liver injury and associated hepatic encephalopathy, have been reported in clinical trials with KADCYLA. Some of the observed cases may have been confounded by comorbidities and/or concomitant medications with known hepatotoxic potential.
Monitor serum transaminases and bilirubin prior to initiation of KADCYLA treatment and prior to each KADCYLA dose. Patients with known active hepatitis B virus or hepatitis C virus were excluded from Study 1 [see Clinical Studies (14.1)]. Reduce the dose or discontinue KADCYLA as appropriate in cases of increased serum transaminases and/or total bilirubin [see Dosage and Administration (2.2)]. Permanently discontinue KADCYLA treatment in patients with serum transaminases > 3 x ULN and concomitant total bilirubin > 2 x ULN. KADCYLA has not been studied in patients with serum transaminases > 2.5 x ULN or bilirubin > 1.5 x ULN prior to the initiation of treatment.
In clinical trials of KADCYLA, cases of nodular regenerative hyperplasia (NRH) of the liver have been identified from liver biopsies (3 cases out of 884 treated patients). Two of these three cases of NRH were observed in the randomized trial (Study 1) [see Adverse Reactions (6.1)]. NRH is a rare liver condition characterized by widespread benign transformation of hepatic parenchyma into small regenerative nodules; NRH may lead to non-cirrhotic portal hypertension. The diagnosis of NRH can be confirmed only by histopathology. NRH should be considered in all patients with clinical symptoms of portal hypertension but with normal transaminases and no manifestations of cirrhosis. Upon diagnosis of NRH, KADCYLA treatment must be permanently discontinued.
5.2 Left Ventricular DysfunctionPatients treated with KADCYLA are at increased risk of developing left ventricular dysfunction. A decrease of LVEF to < 40% has been observed in patients treated with KADCYLA. In the randomized trial (Study 1), left ventricular dysfunction occurred in 1.8% of patients in the KADCYLA-treated group and 3.3% of patients in the lapatinib plus capecitabine-treated group [see Adverse Reactions (6.1)].
Assess LVEF prior to initiation of KADCYLA and at regular intervals (e.g. every three months) during treatment to ensure the LVEF is within the institution’s normal limits. Treatment with KADCYLA has not been studied in patients with LVEF < 50% prior to initiation of treatment. If, at routine monitoring, LVEF is < 40%, or is 40% to 45% with a 10% or greater absolute decrease below the pretreatment value, withhold KADCYLA and repeat LVEF assessment within approximately 3 weeks. Permanently discontinue KADCYLA if the LVEF has not improved or has declined further [see Dosage and Administration (2.2)]. Patients with a history of symptomatic congestive heart failure (CHF), serious cardiac arrhythmia, or history of myocardial infarction or unstable angina within 6 months were excluded from Study 1 [see Clinical Studies (14.1)].
5.3 Embryo-Fetal Toxicity KADCYLA can cause fetal harm when administered to a pregnant
woman. There are no adequate and well-controlled studies of KADCYLA in pregnant women and no reproductive and developmental toxicology studies have been conducted with ado-trastuzumab emtansine. Nevertheless, treatment with trastuzumab, the antibody component of KADCYLA, during pregnancy in the postmarketing setting has resulted in oligohydramnios, some associated with fatal pulmonary hypoplasia, skeletal abnormalities and neonatal death. DM1, the cytotoxic component of KADCYLA, can be expected to cause embryo-fetal toxicity based on its mechanism of action.
If KADCYLA is used during pregnancy, or if the patient becomes pregnant while receiving KADCYLA, apprise the patient of the potential hazard to the fetus [see Use in Specific Populations (8.1)].Verify pregnancy status prior to the initiation of KADCYLA. Advise patients of the risks of embryo-fetal death and birth defects and the need for contraception during and after treatment. Advise patients to contact their healthcare provider immediately if they suspect they may be pregnant. If KADCYLA is administered during pregnancy or if a patient becomes pregnant while receiving KADCYLA, immediately report exposure to the Genentech Adverse Event Line at 1-888-835-2555. Encourage women who may be exposed during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720 [see Patient Counseling Information (17)].
5.4 Pulmonary ToxicityCases of interstitial lung disease (ILD), including pneumonitis, some leading to acute respiratory distress syndrome or fatal outcome have been reported in clinical trials with KADCYLA. Pneumonitis at an incidence of 0.8% (7 out of 884 treated patients) has been reported, with one case of grade 3 pneumonitis. Signs and symptoms include dyspnea, cough, fatigue, and pulmonary infiltrates. These events may or may not occur as sequelae of infusion reactions. In the randomized trial (Study 1), the overall frequency of pneumonitis was 1.2% [see Adverse Reactions (6.1)].
Permanently discontinue treatment with KADCYLA in patients diagnosed with ILD or pneumonitis.
Patients with dyspnea at rest due to complications of advanced malignancy and co-morbidities may be at increased risk of pulmonary toxicity.
5.5 Infusion-Related Reactions, Hypersensitivity ReactionsTreatment with KADCYLA has not been studied in patients who had trastuzumab permanently discontinued due to infusion-related reactions (IRR) and/or hypersensitivity; treatment with KADCYLA is not recommended for these patients.
Infusion-related reactions, characterized by one or more of the following symptoms − flushing, chills, pyrexia, dyspnea, hypotension, wheezing, bronchospasm, and tachycardia have been reported in clinical trials of KADCYLA. In the randomized trial (Study 1), the overall frequency of IRRs in patients treated with KADCYLA was 1.4% [see Adverse Reactions (6.1)]. In most patients, these reactions resolved over the course of several hours to a day after the infusion was terminated. KADCYLA treatment should be interrupted in patients with severe IRR. KADCYLA treatment should be permanently discontinued in the event of a life-threatening IRR [see Dosage and Administration (2.2)]. Patients should be observed closely for IRR reactions, especially during the first infusion.
One case of a serious, allergic/anaphylactic-like reaction has been observed in clinical trials of single-agent KADCYLA. Medications to treat such reactions, as well as emergency equipment, should be available for immediate use.
5.6 ThrombocytopeniaThrombocytopenia, or decreased platelet count, was reported in clinical trials of KADCYLA (103 of 884 treated patients with ≥ Grade 3; 283 of 884 treated patients with any Grade). The majority of these patients had Grade 1 or 2 events (< LLN to ≥ 50,000/mm3) with the nadir occurring by day 8 and generally improving to Grade 0 or 1 (≥ 75,000 /mm3) by the next scheduled dose. In clinical trials of KADCYLA, the incidence and severity of thrombocytopenia were higher in Asian patients. Independent of race, the incidence of severe hemorrhagic events in patients treated with KADCYLA was low.
In the randomized trial (Study 1), the overall frequency of thrombocytopenia was 31.2% in the KADCYLA-treated group and 3.3% in the lapatinib plus capecitabine-treated group [see Adverse Reactions (6.1)]. The incidence of ≥ Grade 3 thrombocytopenia was 14.5% in the KADCYLA-treated group and 0.4% in the lapatinib plus capecitabine-treated group. In Asian patients, the incidence of ≥ Grade 3 thrombocytopenia was 45.1% in the KADCYLA-treated group and 1.3% in the lapatinib plus capecitabine-treated group.
Monitor platelet counts prior to initiation of KADCYLA and prior to each KADCYLA dose [see Dosage and Administration (2.2)]. KADCYLA has not been studied in patients with platelet counts <100,000/mm3 prior to initiation of treatment. In the event of decreased platelet count to Grade 3 or greater (< 50,000/mm3) do not administer KADCYLA until platelet counts recover to Grade 1 (≥ 75,000/mm3) [see Dosage and Administration (2.2)]. Patients with thrombocytopenia (< 100,000/mm3) and patients on anti-coagulant treatment should be closely monitored during treatment with KADCYLA.
5.7 NeurotoxicityPeripheral neuropathy, mainly as Grade 1 and predominantly sensory, was reported in clinical trials of KADCYLA (14 of 884 treated patients with ≥ Grade 3; 196 of 884 treated patients with any Grade). In the randomized trial (Study 1), the overall frequency of peripheral neuropathy was 21.2% in the KADCYLA-treated group
and 13.5% in the lapatinib plus capecitabine-treated group [see Adverse Reactions (6.1)]. The incidence of ≥ Grade 3 peripheral neuropathy was 2.2% in the KADCYLA-treated group and 0.2% in the lapatinib plus capecitabine-treated group.
KADCYLA should be temporarily discontinued in patients experiencing Grade 3 or 4 peripheral neuropathy until resolution to ≤ Grade 2. Patients should be clinically monitored on an ongoing basis for signs or symptoms of neurotoxicity [see Nonclinical Toxicology (13.2)].
5.8 HER2 TestingDetection of HER2 protein overexpression or gene amplification is necessary for selection of patients appropriate for KADCYLA therapy because these are the only patients studied for whom benefit has been shown [see Indications and Usage (1), Clinical Studies (14.1)]. In the randomized study (Study 1), patients with breast cancer were required to have evidence of HER2 overexpression defined as 3+ IHC by Dako Herceptest™ or evidence of overexpression defined as FISH amplification ratio ≥ 2.0 by Dako HER2 FISH PharmDx™ test kit. Only limited data were available for patients whose breast cancer was positive by FISH and 0 or 1+ by IHC.
Assessment of HER2 status should be performed by laboratories with demonstrated proficiency in the specific technology being utilized. Improper assay performance, including use of sub- optimally fixed tissue, failure to utilize specified reagents, deviation from specific assay instructions, and failure to include appropriate controls for assay validation, can lead to unreliable results.
5.9 Extravasation In KADCYLA clinical studies, reactions secondary to extravasation have been observed. These reactions, observed more frequently within 24 hours of infusion, were usually mild and comprised erythema, tenderness, skin irritation, pain, or swelling at the infusion site. Specific treatment for KADCYLA extravasation is unknown. The infusion site should be closely monitored for possible subcutaneous infiltration during drug administration.
6 ADVERSE REACTIONS The following adverse reactions are discussed in greater detail in other sections of the label: • Hepatotoxicity [See Warnings and Precautions (5.1)]• Left Ventricular Dysfunction [See Warnings and Precautions (5.2)]• Embryo-Fetal Toxicity [See Warnings and Precautions (5.3)]• Pulmonary Toxicity [See Warnings and Precautions (5.4)]• Infusion-Related Reactions, Hypersensitivity Reactions [See
Warnings and Precautions (5.5)]• Thrombocytopenia [See Warnings and Precautions (5.6)]• Neurotoxicity [See Warnings and Precautions (5.7)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In clinical trials, KADCYLA has been evaluated as single-agent in 884 patients with HER2-positive metastatic breast cancer. The most common (frequency ≥ 25%) adverse drug reactions (ADRs) seen in 884 patients treated with KADCYLA were fatigue, nausea, musculoskeletal pain, thrombocytopenia, headache, increased transaminases, and constipation.
The ADRs described in Table 6 were identified in patients with HER2-positive metastatic breast cancer treated in a randomized trial (Study 1) [see Clinical Studies (14.1)]. Patients were randomized to receive KADCYLA or lapatinib plus capecitabine. The median duration of study treatment was 7.6 months for patients in the KADCYLA-treated group and 5.5 months and 5.3 months for patients treated with lapatinib and capecitabine, respectively. Two hundred and eleven (43.1%) patients experienced ≥ Grade 3 adverse events in the KADCYLA-treated group compared with 289 (59.2%) patients in the lapatinib plus capecitabine-treated group. Dose adjustments for KADCYLA were permitted [see Dosage and Administration (2.2)]. Thirty-two patients (6.5%) discontinued KADCYLA due to an adverse event, compared with 41 patients (8.4%) who discontinued lapatinib, and 51 patients (10.5%) who discontinued capecitabine due to an adverse event. The most common adverse events leading to KADCYLA withdrawal were thrombocytopenia and increased transaminases. Eighty patients (16.3%) treated with KADCYLA had adverse events leading to dose reductions. The most frequent adverse events leading to dose reduction of KADCYLA (in ≥ 1% of patients) included thrombocytopenia, increased transaminases, and peripheral neuropathy. Adverse events that led to dose delays occurred in 116 (23.7%) of KADCYLA treated patients. The most frequent adverse events leading to a dose delay of KADCYLA (in ≥ 1% of patients) were neutropenia, thrombocytopenia, leukopenia, fatigue, increased transaminases and pyrexia.
Table 6 reports the ADRs that occurred in patients in the KADCYLA-treated group (n=490) of the randomized trial (Study 1). Selected laboratory abnormalities are shown in Table 7. The most common ADRs seen with KADCYLA in the randomized trial (frequency > 25%) were nausea, fatigue, musculoskeletal pain, thrombocytopenia, increased transaminases, headache, and constipation. The most common NCI–CTCAE (version 3) ≥ Grade 3 ADRs (frequency >2%) were thrombocytopenia, increased transaminases, anemia, hypokalemia, peripheral neuropathy and fatigue.
Adverse Drug Reactions (MedDRA)
System Organ Class
KADCYLA(3.6 mg/kg)
n=490Frequency rate %
Lapatinib (1250 mg) + Capecitabine (2000 mg/m2)
n=488Frequency rate %
All grades (%)
Grade 3 – 4 (%)
All grades (%)
Grade 3 – 4 (%)
Blood and Lymphatic System Disorders
Neutropenia 6.7 2.0 9.0 4.3
Anemia 14.3 4.1 10.5 2.5
Thrombocyto-penia 31.2 14.5 3.3 0.4
Cardiac Disorders
Left ventricular dysfunction 1.8 0.2 3.3 0.4
Eye Disorders
Lacrimation increased 3.3 0 2.5 0
Dry eye 3.9 0 3.1 0
Vision blurred 4.5 0 0.8 0
Conjunctivitis 3.9 0 2.3 0
Gastrointestinal Disorders
Dyspepsia 9.2 0 11.5 0.4
Stomatitis 14.1 0.2 32.6 2.5
Dry Mouth 16.7 0 4.9 0.2
Abdominal pain 18.6 0.8 17.6 1.6
Vomiting 19.2 0.8 29.9 4.5
Diarrhea 24.1 1.6 79.7 20.7
Constipation 26.5 0.4 11.1 0
Nausea 39.8 0.8 45.1 2.5
General Disorders and Administration
Peripheral edema 7.1 0 8.2 0.2
Chills 7.6 0 3.1 0
Pyrexia 18.6 0.2 8.4 0.4
Asthenia 17.8 0.4 17.6 1.6
Fatigue 36.3 2.5 28.3 3.5
Hepatobiliary Disorders
Nodular regenerative hyperplasia*
0.4 ND 0 0
Portal hyperten-sion* 0.4 0.2 0 0
Immune System Disorders
Drug hypersen-sitivity 2.2 0 0.8 0
Injury, Poisoning, and Procedural
Infusion-related reaction 1.4 0 0.2 0
Infections and Infestations
Urinary tract infection 9.4 0.6 3.9 0
Investigations
Blood alkaline phosphatase increased
4.7 0.4 3.7 0.4
Increased transaminases 28.8 8.0 14.3 2.5
Metabolism and Nutrition Disorders
Hypokalemia 10.2 2.7 9.4 4.7
Musculoskeletal and Connective Tissue Disorders
Myalgia 14.1 0.6 3.7 0
Arthralgia 19.2 0.6 8.4 0
Musculoskeletal pain 36.1 1.8 30.5 1.4
Nervous System Disorders
Dysgeusia 8.0 0 4.1 0.2
Dizziness 10.2 0.4 10.7 0.2
Peripheral neuropathy 21.2 2.2 13.5 0.2
Headache 28.2 0.8 14.5 0.8
Psychiatric Disorders
Insomnia 12.0 0.4 8.6 0.2
Respiratory, Thoracic, and Mediastinal Disorders
Pneumonitis 1.2 0 0 0
Dyspnea 12.0 0.8 8.0 0.4
Cough 18.2 0.2 13.1 0.2
Epistaxis 22.5 0.2 8.4 0
Skin and Subcutaneous Tissue Disorders
Pruritus 5.5 0.2 9.2 0
Rash 11.6 0 27.5 1.8
Vascular Disorders
Hypertension 5.1 1.2 2.3 0.4
Table 7 Selected Laboratory Abnormalities
Parameter KADCYLA(3.6 mg/kg)
Lapatinib (1250 mg) +Capecitabine (2000 mg/m2)
All Grade
%Grade 3
%Grade 4
%All
Grade %
Grade 3 %
Grade 4 %
Increased bilirubin 17 <1 0 57 2 0
Increased AST 98 7 <1 65 3 0
Increased ALT 82 5 <1 54 3 0
Decreased platelet count 83 14 3 21 <1 <1
Decreased hemoglobin 60 4 1 64 3 <1
Decreased neutrophils 39 3 <1 38 6 2
Decreased potassium 33 3 0 31 6 <1
Table 6 Summary of Adverse Drug Reactions Occurring in Patients on the KADCYLA Treatment Arm in the Randomized Trial (Study 1)
* Nodular Regenerative Hyperplasia and Portal Hypertension occurred in the same patient.
ND = Not determined
6.2 ImmunogenicityAs with all therapeutic proteins, there is the potential for an immune response to KADCYLA.
A total of 836 patients from six clinical studies were tested at multiple time points for anti-therapeutic antibody (ATA) responses to KADCYLA. Following KADCYLA dosing, 5.3% (44/836) of patients tested positive for anti-KADCYLA antibodies at one or more post-dose time points. The presence of KADCYLA in patient serum at the time of ATA sampling may interfere with the ability of this assay to detect anti-KADCYLA antibodies. As a result, data may not accurately reflect the true incidence of anti-KADCYLA antibody development. In addition, neutralizing activity of anti-KADCYLA antibodies has not been assessed.
Immunogenicity data are highly dependent on the sensitivity and specificity of the test methods used. Additionally, the observed incidence of a positive result in a test method may be influenced by several factors, including sample handling, timing of sample collection, drug interference, concomitant medication and the underlying disease. Therefore, comparison of the incidence of antibodies to KADCYLA with the incidence of antibodies to other products may be misleading. Clinical significance of anti-KADCYLA antibodies is not yet known.
7 DRUG INTERACTIONSNo formal drug-drug interaction studies with KADCYLA have been conducted. In vitro studies indicate that DM1, the cytotoxic component of KADCYLA, is metabolized mainly by CYP3A4 and to a lesser extent by CYP3A5. Concomitant use of strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, clarithromycin, atazanavir, indinavir, nefazodone, nelfinavir, ritonavir, saquinavir, telithromycin, and voriconazole) with KADCYLA should be avoided due to the potential for an increase in DM1 exposure and toxicity. Consider an alternate medication with no or minimal potential to inhibit CYP3A4. If concomitant use of strong CYP3A4 inhibitors is unavoidable, consider delaying KADCYLA treatment until the strong CYP3A4 inhibitors have cleared from the circulation (approximately 3 elimination half-lives of the inhibitors) when possible. If a strong CYP3A4 inhibitor is coadministered and KADCYLA treatment cannot be delayed, patients should be closely monitored for adverse reactions.
8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyPregnancy Category D [see Warnings and Precautions (5.3)]
Risk Summary
KADCYLA can cause fetal harm when administered to a pregnant woman. There are no adequate and well-controlled studies of KADCYLA in pregnant women. No reproductive and developmental toxicology studies have been conducted with ado-trastuzumab emtansine. Nevertheless, two components of KADCYLA (trastuzumab and DM1) are known or suspected to cause fetal harm or death when administered to a pregnant woman. If KADCYLA is administered during pregnancy, or if a patient becomes pregnant while receiving KADCYLA, apprise the patient of the potential hazard to the fetus. Patients should be advised to use effective contraception during treatment with KADCYLA and for 6 months following the last dose of KADCYLA.
If KADCYLA is administered during pregnancy or if a patient becomes pregnant while receiving KADCYLA, immediately report exposure to the Genentech Adverse Event Line at 1-888-835-2555. Encourage women who may be exposed during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720 [see Patient Counseling Information (17)].
Human Data
In the post-marketing setting, treatment with trastuzumab during pregnancy has resulted in cases of oligohydramnios, some associated with fatal pulmonary hypoplasia, skeletal abnormalities and neonatal death. These case reports described oligohydramnios in pregnant women who received trastuzumab either alone or in combination with chemotherapy. In some case reports, amniotic fluid index increased after trastuzumab was stopped. In one case, trastuzumab therapy resumed after the amniotic fluid index improved, and oligohydramnios recurred.
Animal Data
There were no reproductive and developmental toxicology studies conducted with ado-trastuzumab emtansine. DM1, the cytotoxic
component of KADCYLA, disrupts microtubule function. DM1 is toxic to rapidly dividing cells in animals and is genotoxic, suggesting it has the potential to cause embryotoxicity and teratogenicity. In studies where trastuzumab was administered to pregnant monkeys at doses up to 25 mg/kg (about 7 times the clinical dose), trastuzumab crossed the placental barrier during the early and late phases of gestation. The resulting concentrations of trastuzumab in fetal blood and amniotic fluid were approximately 33% and 25%, respectively, of those present in the maternal serum but were not associated with adverse findings.
8.3 Nursing MothersIt is not known whether KADCYLA, specifically, is excreted in human milk, but IgG is known to be excreted in human milk. In lactating monkeys, trastuzumab was excreted in small amounts (about 0.3% of maternal serum concentrations) in breast milk after post-partum doses of 25 mg/kg (about 7 times the clinical dose of KADCYLA). Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from KADCYLA, a decision should be made whether to discontinue nursing or discontinue KADCYLA, taking into account the importance of the drug to the mother [see Warnings and Precautions (5.3)].
8.4 Pediatric UseSafety and effectiveness of KADCYLA have not been established in pediatric patients.
8.5 Geriatric UseOf 495 patients who were randomized to KADCYLA in the randomized trial (Study 1) [see Clinical Studies (14.1)], 65 patients (13%) were ≥ 65 years of age and 11 patients (2%) were ≥ 75 years of age. In patients ≥ 65 years old (n=138 across both treatment arms) the hazard ratios for progression-free survival (PFS) and Overall Survival (OS) were 1.06 (95% CI: 0.68, 1.66) and 1.05 (95% CI: 0.58, 1.91), respectively.
Population pharmacokinetic analysis indicates that age does not have a clinically meaningful effect on the pharmacokinetics of ado-trastuzumab emtansine [see Clinical Pharmacology (12.3)].
8.6 Females of Reproductive PotentialKADCYLA can cause embryo-fetal harm when administered during pregnancy. Counsel patients regarding pregnancy prevention and planning. Advise females of reproductive potential to use effective contraception while receiving KADCYLA and for 6 months following the last dose of KADCYLA.
If KADCYLA is administered during pregnancy or if the patient becomes pregnant while receiving KADCYLA, immediately report exposure to the Genentech Adverse Event Line at 1-888-835-2555. Encourage women who may be exposed during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720 [see Patient Counseling Information (17)].
8.7 Renal ImpairmentNo dedicated renal impairment trial for KADCYLA has been conducted. Based on the population pharmacokinetics, as well as analysis of Grade 3 or greater adverse drug reactions and dose modifications, dose adjustments of KADCYLA are not needed in patients with mild (creatinine clearance [CLcr] 60 to 89 mL/min) or moderate (CLcr 30 to 59 mL/min) renal impairment. No dose adjustment can be recommended for patients with severe renal impairment (CLcr less than 30 mL/min) because of the limited data available [see Clinical Pharmacology (12.3)].
8.8 Hepatic ImpairmentIn vitro studies in human liver microsomes indicates that DM1 is metabolized by CYP3A4/5. The influence of hepatic impairment on the pharmacokinetics of ado-trastuzumab emtansine conjugate has not been determined.
10 OVERDOSAGEThere is no known antidote for overdose of KADCYLA. In clinical trials, overdose of KADCYLA has been reported at approximately two times the recommended dose which resulted in Grade 2 thrombocytopenia (resolved 4 days later) and one death. In the fatal case, the patient incorrectly received KADCYLA at 6 mg/kg and died approximately 3 weeks following the overdose; a cause of death and a causal relationship to KADCYLA were not established.
KADCYLA™ (ado-trastuzumab emtansine)
Manufactured by:Genentech, Inc. 4862200A Member of the Roche Group Initial U.S. Approval: 02/131 DNA Way KADCYLA is a trademarkSouth San Francisco, CA of Genentech, Inc. 94080-4990 02/13 TDM0001661000U.S. License No: 1048 ©2013 Genentech, Inc.
S:6.875”
S:9.875”
T:15.5”
T:10.5”
B:17.5”
B:11.5”
S:6.875”

JOB#: Q23261B CLIENT: Kadcyla DESC: JA Tabloid FILE NAME: GNH_TDM_Q23261B_JA_D01.indd DATE: 2-28-2013 2:50 PM ROUND: 1PG: vazz/millerk AD: Andy Warhol ext: 111 TC: EA AE: None CW: None Last Saved: 2-28-2013 2:50 PMTRIM: 25” x 17” BLEED: None SAFETY: None PROD: Haight INK Spec: 4C PRINT SCALE: 75%FONTS: Univers LT Std (67 Bold Condensed, 47 Light Condensed, 65 Bold, 45 Light, 45 Light Oblique), Conduit ITC (Bold, Medium), Univers (65 Bold, 45 Light, 45 Light Oblique), TT Slug OTF (Regular)
IMAGES: 23261B_JA_2_fn.tif (CMYK; 300 ppi; 100%), Kadcyla_TM_4C.ai (70%, 66%), 23261B_OS chart_pg3.eps (100%), Genentech_AMOTRG_4C.eps (88%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: Macintosh HD:Users:vazz:Deskto...JA_D01:GNH_TDM_Q23261B_JA_D01.inddNOTES: None
GNH_TDM_Q23261B_JA_D01.indd Galley: 2
S&H PharmaGraphics
DISK RELEASE
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
2d1 Q1 Q2Cosmos Communications 718.482.1800
24298a1 03.1.13 133C M Y K
Months
Prop
ortio
n su
rviv
ing
(%)
00
20
40
60
80
100
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
10
30
50
70
90HR=0.68295% CI: 0.55, 0.85P=0.0006
KADCYLA (n=495)No. of events: 149
lapatinib + capecitabine (n=496)No. of events: 182
No. at risk:
lapatinib + capecitabine
KADCYLA 495 485 474 457 439 418 349 293 242 197 164 136 111 86 62 38 28 13 5496 471 453 435 403 368 297 240 204 159 133 110 86 63 45 27 17 7 4
30.9 months
25.1 months
InthePhaseIIIEMILIAtrial(N=991)versuslapatinib+capecitabine:
Single-agent KADCYLA signifi cantly improved survival1
© 2013 Genentech USA, Inc. All rights reserved. TDM0001176100 Printed in USA. (02/13)
PleaseseebriefsummaryoffullPrescribingInformationonfollowingpagesforadditionalimportantsafetyinformation,includingBoxedWARNINGS.For more information on KADCYLA, please visit KADCYLA.com
NOW APPROVED
AdditionalImportantSafetyInformationPulmonary Toxicity• Cases of interstitial lung disease (ILD), including
pneumonitis, some leading to acute respiratory distress syndrome or fatal outcome have been reported in clinical trials with KADCYLA. In EMILIA the overall frequency of pneumonitis was 1.2%
• Treatment with KADCYLA should be permanently discontinued in patients diagnosed with ILD or pneumonitis
Infusion-Related Reactions, Hypersensitivity Reactions• Treatment with KADCYLA has not been studied
in patients who had trastuzumab permanently discontinued due to infusion-related reactions (IRR) and/or hypersensitivity reactions; treatment with KADCYLA is not recommended for these patients. In EMILIA, the overall frequency of IRRs in patients treated with KADCYLA was 1.4%
• KADCYLA treatment should be interrupted in patients with severe IRR and permanently discontinued in the event of a life-threatening IRR
Thrombocytopenia• In EMILIA, the incidence of ≥ Grade 3 thrombocytopenia
was 14.5% in the KADCYLA-treated group and 0.4% in the comparator group
• Monitor platelet counts prior to initiation of KADCYLA and prior to each KADCYLA dose. Institute dose modifications as appropriate
Neurotoxicity• In EMILIA, the incidence of ≥ Grade 3 peripheral
neuropathy was 2.2% in the KADCYLA-treated group and 0.2% in the comparator group
• Monitor for signs or symptoms of neurotoxicity. KADCYLA should be temporarily discontinued in patients experiencing Grade 3 or 4 peripheral neuropathy until resolution to ≤ Grade 2
HER2 Testing• Detection of HER2 protein overexpression or gene
amplification is necessary for selection of patients appropriate for KADCYLA. Perform using FDA approved tests by laboratories with demonstrated proficiency
Extravasation• In KADCYLA clinical studies, reactions secondary to
extravasation have been observed and were generally mild. The infusion site should be closely monitored for possible subcutaneous infiltration during drug administration
Nursing Mothers• Discontinue nursing or discontinue KADCYLA taking
into consideration the importance of the drug to the mother
Pregnancy Registry• Encourage women who may be exposed to KADCYLA
during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720
Adverse Reactions• The most common ADRs seen with KADCYLA in
EMILIA (frequency > 25%) were nausea, fatigue, musculoskeletal pain, thrombocytopenia, increased transaminases, headache, and constipation. The most common NCI-CTCAE (version 3) ≥ Grade 3 ADRs (frequency >2%) were thrombocytopenia, increased transaminases, anemia, hypokalemia, peripheral neuropathy and fatigue
You are encouraged to report side effects to Genentech and the FDA. You may contact Genentech by calling 1-888-835-2555. You may contact the FDA by visiting www.fda.gov/ medwatch or calling 1-800-FDA-1088.
References: 1. KADCYLA Prescribing Information. Genentech, Inc. February 2013. 2. Verma S, Miles D, Gianni L, et al; EMILIA Study Group. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med. 2012;367:1783-1791.
• KADCYLA increased median OS by 5.8 months vs lapatinib + capecitabine1
• 50% improvement in median PFS for KADCYLA vs lapatinib + capecitabine (9.6 months vs 6.4 months; HR=0.650; 95% CI: 0.55, 0.77; P<0.0001)1
• The most common NCI-CTCAE (version 3) adverse reactions (ARs) Grades ≥3 (frequency >2%) were thrombocytopenia, increased transaminases, anemia, hypokalemia, peripheral neuropathy, and fatigue1
Patients received KADCYLA (3.6 mg/kg IV, q3w) or lapatinib (1250 mg po qd, Days 1-21) + capecitabine (1000 mg/m2 po bid, Days 1-14) until disease progression or unacceptable toxicity. Primary endpoints were progression-free survival (PFS) assessed by independent review committee, OS, and safety.1,2
PRIMARYENDPOINT:OVERALLSURVIVAL(OS)
T:20.5”
B:22.5”
T:13”
B:15.625”
S:19.5”
S:12”

JOB#: Q23261B CLIENT: Kadcyla DESC: JA Tabloid FILE NAME: GNH_TDM_Q23261B_JA_D01.indd DATE: 2-28-2013 2:50 PM ROUND: 1PG: vazz/millerk AD: Andy Warhol ext: 111 TC: EA AE: None CW: None Last Saved: 2-28-2013 2:50 PMTRIM: 25” x 17” BLEED: None SAFETY: None PROD: Haight INK Spec: 4C PRINT SCALE: 75%FONTS: Univers LT Std (67 Bold Condensed, 47 Light Condensed, 65 Bold, 45 Light, 45 Light Oblique), Conduit ITC (Bold, Medium), Univers (65 Bold, 45 Light, 45 Light Oblique), TT Slug OTF (Regular)
IMAGES: 23261B_JA_2_fn.tif (CMYK; 300 ppi; 100%), Kadcyla_TM_4C.ai (70%, 66%), 23261B_OS chart_pg3.eps (100%), Genentech_AMOTRG_4C.eps (88%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: Macintosh HD:Users:vazz:Deskto...JA_D01:GNH_TDM_Q23261B_JA_D01.inddNOTES: None
GNH_TDM_Q23261B_JA_D01.indd Galley: 2
S&H PharmaGraphics
DISK RELEASE
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
2d1 Q1 Q2Cosmos Communications 718.482.1800
24298a1 03.1.13 133C M Y K
Months
Prop
ortio
n su
rviv
ing
(%)
00
20
40
60
80
100
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
10
30
50
70
90HR=0.68295% CI: 0.55, 0.85P=0.0006
KADCYLA (n=495)No. of events: 149
lapatinib + capecitabine (n=496)No. of events: 182
No. at risk:
lapatinib + capecitabine
KADCYLA 495 485 474 457 439 418 349 293 242 197 164 136 111 86 62 38 28 13 5496 471 453 435 403 368 297 240 204 159 133 110 86 63 45 27 17 7 4
30.9 months
25.1 months
InthePhaseIIIEMILIAtrial(N=991)versuslapatinib+capecitabine:
Single-agent KADCYLA signifi cantly improved survival1
© 2013 Genentech USA, Inc. All rights reserved. TDM0001176100 Printed in USA. (02/13)
PleaseseebriefsummaryoffullPrescribingInformationonfollowingpagesforadditionalimportantsafetyinformation,includingBoxedWARNINGS.For more information on KADCYLA, please visit KADCYLA.com
NOW APPROVED
AdditionalImportantSafetyInformationPulmonary Toxicity• Cases of interstitial lung disease (ILD), including
pneumonitis, some leading to acute respiratory distress syndrome or fatal outcome have been reported in clinical trials with KADCYLA. In EMILIA the overall frequency of pneumonitis was 1.2%
• Treatment with KADCYLA should be permanently discontinued in patients diagnosed with ILD or pneumonitis
Infusion-Related Reactions, Hypersensitivity Reactions• Treatment with KADCYLA has not been studied
in patients who had trastuzumab permanently discontinued due to infusion-related reactions (IRR) and/or hypersensitivity reactions; treatment with KADCYLA is not recommended for these patients. In EMILIA, the overall frequency of IRRs in patients treated with KADCYLA was 1.4%
• KADCYLA treatment should be interrupted in patients with severe IRR and permanently discontinued in the event of a life-threatening IRR
Thrombocytopenia• In EMILIA, the incidence of ≥ Grade 3 thrombocytopenia
was 14.5% in the KADCYLA-treated group and 0.4% in the comparator group
• Monitor platelet counts prior to initiation of KADCYLA and prior to each KADCYLA dose. Institute dose modifications as appropriate
Neurotoxicity• In EMILIA, the incidence of ≥ Grade 3 peripheral
neuropathy was 2.2% in the KADCYLA-treated group and 0.2% in the comparator group
• Monitor for signs or symptoms of neurotoxicity. KADCYLA should be temporarily discontinued in patients experiencing Grade 3 or 4 peripheral neuropathy until resolution to ≤ Grade 2
HER2 Testing• Detection of HER2 protein overexpression or gene
amplification is necessary for selection of patients appropriate for KADCYLA. Perform using FDA approved tests by laboratories with demonstrated proficiency
Extravasation• In KADCYLA clinical studies, reactions secondary to
extravasation have been observed and were generally mild. The infusion site should be closely monitored for possible subcutaneous infiltration during drug administration
Nursing Mothers• Discontinue nursing or discontinue KADCYLA taking
into consideration the importance of the drug to the mother
Pregnancy Registry• Encourage women who may be exposed to KADCYLA
during pregnancy to enroll in the MotHER Pregnancy Registry by contacting 1-800-690-6720
Adverse Reactions• The most common ADRs seen with KADCYLA in
EMILIA (frequency > 25%) were nausea, fatigue, musculoskeletal pain, thrombocytopenia, increased transaminases, headache, and constipation. The most common NCI-CTCAE (version 3) ≥ Grade 3 ADRs (frequency >2%) were thrombocytopenia, increased transaminases, anemia, hypokalemia, peripheral neuropathy and fatigue
You are encouraged to report side effects to Genentech and the FDA. You may contact Genentech by calling 1-888-835-2555. You may contact the FDA by visiting www.fda.gov/ medwatch or calling 1-800-FDA-1088.
References: 1. KADCYLA Prescribing Information. Genentech, Inc. February 2013. 2. Verma S, Miles D, Gianni L, et al; EMILIA Study Group. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med. 2012;367:1783-1791.
• KADCYLA increased median OS by 5.8 months vs lapatinib + capecitabine1
• 50% improvement in median PFS for KADCYLA vs lapatinib + capecitabine (9.6 months vs 6.4 months; HR=0.650; 95% CI: 0.55, 0.77; P<0.0001)1
• The most common NCI-CTCAE (version 3) adverse reactions (ARs) Grades ≥3 (frequency >2%) were thrombocytopenia, increased transaminases, anemia, hypokalemia, peripheral neuropathy, and fatigue1
Patients received KADCYLA (3.6 mg/kg IV, q3w) or lapatinib (1250 mg po qd, Days 1-21) + capecitabine (1000 mg/m2 po bid, Days 1-14) until disease progression or unacceptable toxicity. Primary endpoints were progression-free survival (PFS) assessed by independent review committee, OS, and safety.1,2
PRIMARYENDPOINT:OVERALLSURVIVAL(OS)
T:20.5”
B:22.5”
T:13”
B:15.625”
S:19.5”
S:12”

JOB#: Q23261B CLIENT: Kadcyla DESC: JA Tabloid FILE NAME: GNH_TDM_Q23261B_JA_D01.indd DATE: 2-28-2013 2:50 PM ROUND: 1PG: vazz/millerk AD: Andy Warhol ext: 111 TC: EA AE: None CW: None Last Saved: 2-28-2013 2:50 PMTRIM: 25” x 17” BLEED: None SAFETY: None PROD: Haight INK Spec: 4C PRINT SCALE: 75%FONTS: Conduit ITC (Bold), Univers LT Std (67 Bold Condensed, 57 Condensed), TT Slug OTF (Regular)
IMAGES: 23261B_JA_1_fn.tif (CMYK; 300 ppi; 100%), Kadcyla_TM_4C.ai (108%)INKS: Cyan, Magenta, Yellow, BlackDOC PATH: Macintosh HD:Users:vazz:Deskto...JA_D01:GNH_TDM_Q23261B_JA_D01.inddNOTES: None
GNH_TDM_Q23261B_JA_D01.indd Galley: 1
S&H PharmaGraphics
DISK RELEASE
DATE
SIGNOFF
PG QC TC AD CD CW AE/AS ED PROD
2d1 Q1 Q2Cosmos Communications 718.482.1800
24298a1 03.1.13 133C M Y K
The first antibody-drug conjugate (ADC) for HER2-positive (HER2+) metastatic breast cancer
NOW APPROVED
IndicationKADCYLA™ (ado-trastuzumab emtansine) injection, for intravenous use, as a single agent, is indicated for the treatment of patients with HER2-positive (HER2+), metastatic breast cancer (MBC) who previously received trastuzumab and a taxane, separately or in combination. Patients should have either: received prior therapy for metastatic disease, or developed disease recurrence during or within six months of completing adjuvant therapy.
Important Safety InformationBoxed WARNINGS: HEPATOTOXICITY, CARDIAC TOXICITY, EMBRYO- FETAL TOXICITY• DoNotSubstituteKADCYLAfororwithTrastuzumab• Hepatotoxicity:Serioushepatotoxicityhasbeenreported,includingliverfailureanddeathinpatientstreatedwithKADCYLA.MonitorserumtransaminasesandbilirubinpriortoinitiationofKADCYLAtreatmentandpriortoeachKADCYLAdose.ReducedoseordiscontinueKADCYLAasappropriateincasesofincreasedserumtransaminasesortotalbilirubin
• CardiacToxicity:KADCYLAadministrationmayleadtoreductionsinleftventricularejectionfraction(LVEF).EvaluateleftventricularfunctioninallpatientspriortoandduringtreatmentwithKADCYLA.Withholdtreatmentforclinicallysignificantdecreaseinleftventricularfunction
• Embryo-FetalToxicity:ExposuretoKADCYLAcanresultinembryo-fetaldeathorbirthdefects.Advisepatientsoftheserisksandtheneedforeffectivecontraception
PleaseseebriefsummaryoffullPrescribingInformationonfollowingpagesforadditionalimportantsafetyinformation,includingBoxedWARNINGS.
T:10.25”
B:11.25”
S:12”
T:13”
B:15.625”S:9.25”