Rx15 pharma wed_430_1_green_2yamada-dole
65
Pharmacy Track: Expanding Use of Naloxone Presenters: • Traci Green, PhD, MSC, Brown University and Boston University/Boston Medical Center • Ernest J. Dole, PharmD, PhC, FASHP, BCPS, Pain Consultation and Treatment Center, University of New Mexico Hospitals • Mikiko Yamada, PharmD, University of New Mexico College of Pharmacy and Pediatric Neurology Clinic and Pain Consultation and Treatment Center Moderator: CDR Christopher M. Jones, PharmD, MPH, U.S. Food and Drug Administration, and Member, Rx Summit National Advisory Board
-
Upload
opunite -
Category
Healthcare
-
view
230 -
download
1
Transcript of Rx15 pharma wed_430_1_green_2yamada-dole
Pharmacy Track:Expanding Use of Naloxone
Presenters:
• Traci Green, PhD, MSC, Brown University and Boston University/Boston Medical Center
• Ernest J. Dole, PharmD, PhC, FASHP, BCPS, Pain Consultation and Treatment Center, University of New Mexico Hospitals
• Mikiko Yamada, PharmD, University of New Mexico College of Pharmacy and Pediatric Neurology Clinic and Pain Consultation and Treatment Center
Moderator: CDR Christopher M. Jones, PharmD, MPH, U.S. Food and Drug Administration, and Member, Rx Summit National Advisory Board

Disclosures
• Traci Green, PhD, MSC, Employment: Inflexxion
• Ernest Dole, PharmD, PhC, FASHP, BCPS, Speaker Bureau: Millennium Health
• Mikiko Yamada, PharmD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
• CDR Christopher M. Jones, PharmD, MPH, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition
Learning Objectives
1. Explain the operation and benefits of Naloxone collaborative practice agreements with pharmacies.
2. Describe a model for using intranasal Naloxone in a universal precaution manner for patients with chronic non-cancer pain prescribed COT.
3. Evaluate whether co-prescribing intranasal Naloxone for patients receiving COT has a positive impact on overdose deaths involving Rx opioids.

Expanding Use of Naloxone: Novel models for the Pharmacy Setting
Traci C. Green, PhD, MScDeputy Director, Boston Medical Center Injury Prevention Center
Boston Medical School, Department of Emergency Medicine, Boston, MA
Associate Professor of Emergency Medicine & EpidemiologyThe Warren Alpert School of Medicine at Brown University, Rhode Island Hospital
Disclosures-Traci C. Green Traci C. Green PhD, MSc, wishes to disclose her past 12-
month employment at Inflexxion, Inc. , a small business that conducts post-marketing surveillance of Scheduled medications. She will present this content in a fair and balanced manner
Her presentation will include discussion of “off-label” use of the following: Naloxone is FDA approved as an opioid antagonist Naloxone delivered as an intranasal spray with a mucosal atomizer
device has not been FDA approved and is off label use
Funding: CDC National Center for Injury Prevention and Control, 5R21CE001846-02 and 1R21CE002165-01; National Institute on Drug Abuse, 1R21DA029201-02A1

Learning Objective
• Explain the operation and benefits of Naloxone collaborative practice agreements with pharmacies
Roadmap
• Naloxone Mechanics and Evidence
• Pharmacy Based Naloxone Models
• Next steps

Are we bending the epidemic’s curve?
Sources: National Vital Statistics System mortality data. Available at http://www.cdc.gov/nchs/deaths.htm.Chen LH, Hedegaard H, Warner M. Drug-poisoning deaths involving opioid analgesics: United States, 1999–2011. NCHS data brief no. 166. Hyattsville, MD: US Department of Health and Human Services, CDC; 2014. Available at http://www.cdc.gov/nchs/data/databriefs/db166.htm.
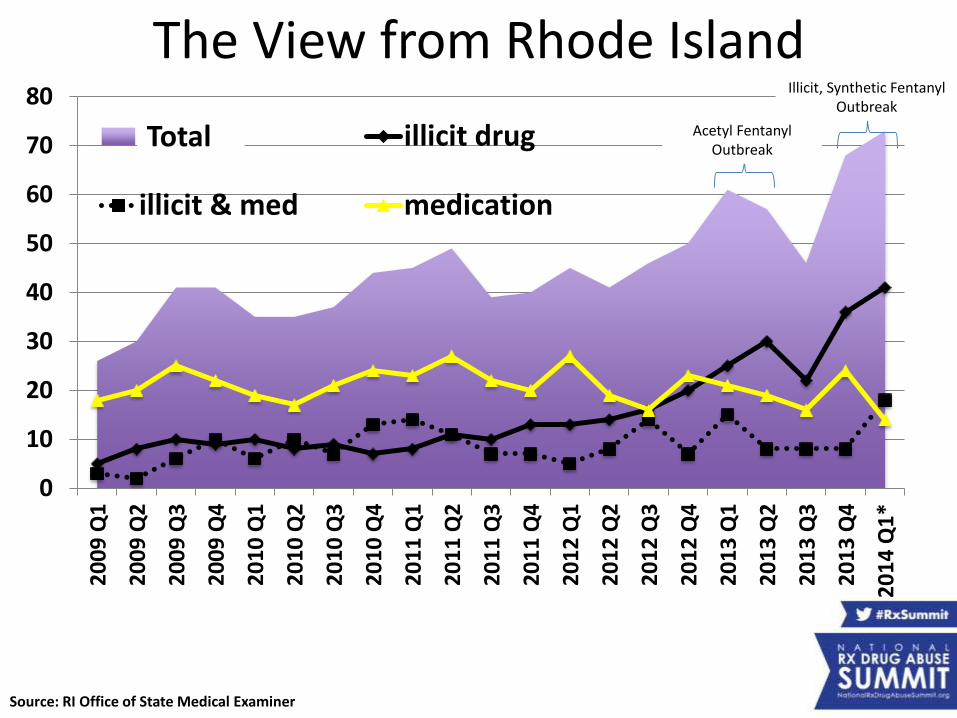
Unintentional drug poisoning deaths Rhode Island 2009-2014
0
10
20
30
40
50
60
70
802
00
9 Q
1
20
09
Q2
20
09
Q3
20
09
Q4
20
10
Q1
20
10
Q2
20
10
Q3
20
10
Q4
20
11
Q1
20
11
Q2
20
11
Q3
20
11
Q4
20
12
Q1
20
12
Q2
20
12
Q3
20
12
Q4
20
13
Q1
20
13
Q2
20
13
Q3
20
13
Q4
20
14
Q1
*
total illicit drug
illicit & med medication
Total
Source: RI Office of State Medical Examiner
Illicit, Synthetic FentanylOutbreak
Acetyl FentanylOutbreak
The View from Rhode Island

Source: MMWR, Rudd et al., http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6339a1.htm?s_cid=mm6339a1_w
Change in Heroin & prescription opioid overdose death rates from 2010 to 2012, 28 states

Overdose mortality, 2012
12
Important demographic differences to consider for public health response

,
B=Heroin only overdose deaths*Greater urban concentration*more deaths occurring in public
D=Prescription opioid overdose deaths•Greater suburban/small town distribution•*more deaths occurring at home
Source: Green et al., Epidemiologic trends and geographic patterns of fatal opioid intoxications in Connecticut, USA: 1997-2007. Drug and Alcohol Dependence, 2011.PMC3095753
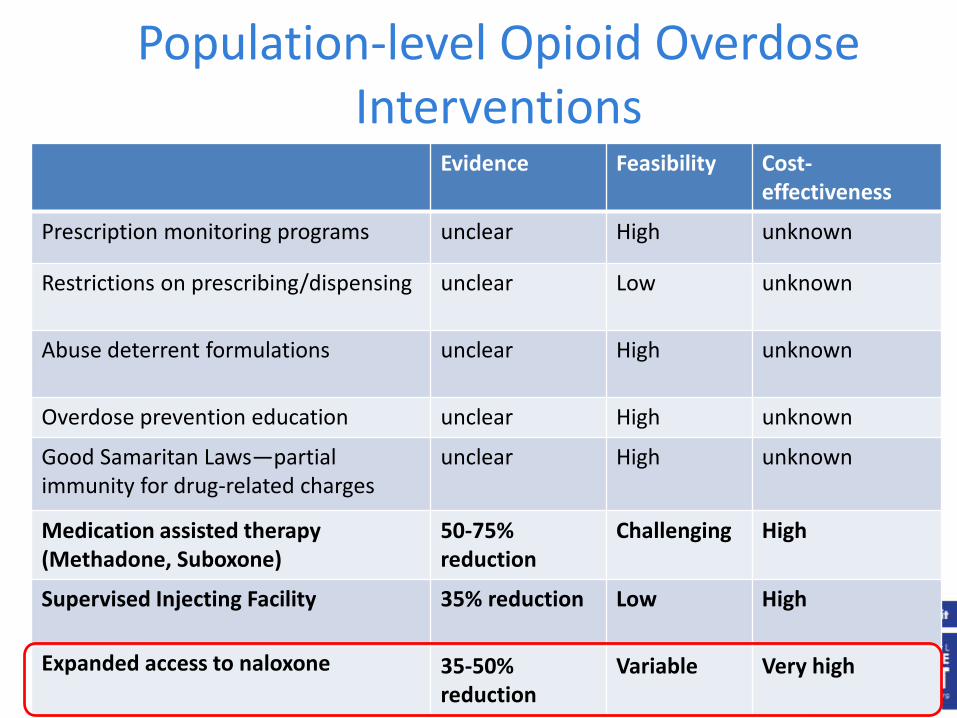
Population-level Opioid Overdose Interventions
Evidence Feasibility Cost-effectiveness
Prescription monitoring programs unclear High unknown
Restrictions on prescribing/dispensing unclear Low unknown
Abuse deterrent formulations unclear High unknown
Overdose prevention education unclear High unknown
Good Samaritan Laws—partial immunity for drug-related charges
unclear High unknown
Medication assisted therapy (Methadone, Suboxone)
50-75% reduction
Challenging High
Supervised Injecting Facility 35% reduction Low High
Expanded access to naloxone 35-50% reduction
Variable Very high
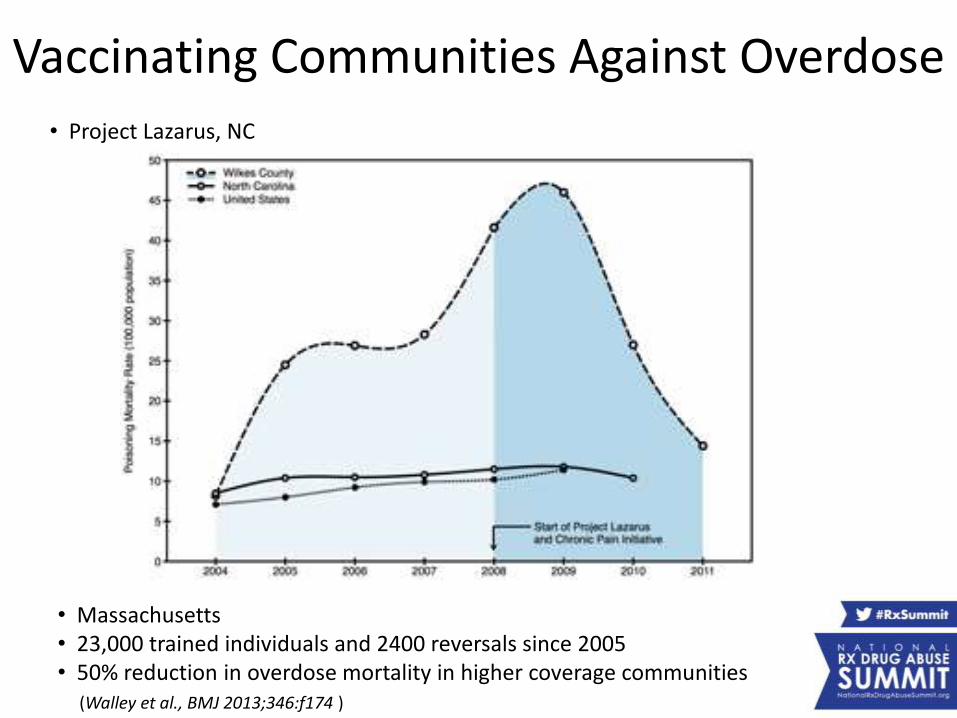
Vaccinating Communities Against Overdose
• Massachusetts• 23,000 trained individuals and 2400 reversals since 2005• 50% reduction in overdose mortality in higher coverage communities
(Walley et al., BMJ 2013;346:f174 )
• Project Lazarus, NC
Risk Factors for Unintentional Opioid Poisoning
Change in TOLERANCE
using opioids ALONE, by oneself
MIXING opioids with other central nervous system depressing substances (alcohol, benzodiazepines)
ILLNESS
Extreme DOSE
Sporer 2007, Binswanger 2007, Green 2012

How to identify an opioid overdose
Respiratory depression (shallow/no breathing)
Pinpoint pupils
Blue or grayish lips/fingernails
No response to stimulus
Gurgling/ heavy wheezing or snoring sound
Typically occurs over 1-3 hours
•Opioids repress the urge to breathe and decrease the body’s/brain’s response to carbon dioxide, leading to respiratory depression (decrease rate of breathing) and death

Effective Interventions for Opioid Overdose
• Naloxone (Narcan), an intranasal or intramuscular-administered opioidantagonist used to reverserespiratory depression caused by opioids
• Call or TEXT 911
• Rescue breathing
• An ANTIDOTE for OPIOID overdose
• Naloxone is an opioid receptor antagonist at mu, kappa, and delta receptors
• Works at the opioid receptor to displace opioid agonists
• Shows little to no agonist activity
• Shows little to no pharmacological effect in patients who have not received opioids
Naloxone
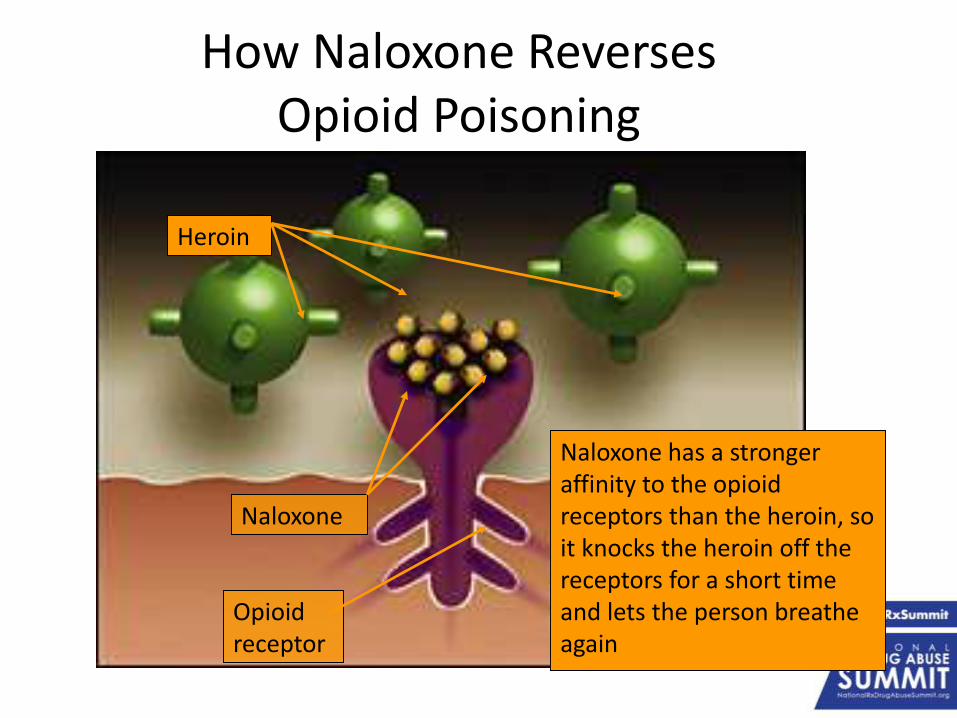
How Naloxone Reverses Opioid Poisoning
Naloxone has a stronger affinity to the opioid receptors than the heroin, so it knocks the heroin off the receptors for a short time and lets the person breathe again
Opioid receptor
Naloxone
Heroin

• Not scheduled or controlled
– Fewer barriers to access
• Cannot be abused
– No euphoria from naloxone
– No effect if opioids are not present
• Effective, inexpensive, easy to administer
• Naloxone has shown success in take-home programs facilitated by community outreach programs in various states
Why use Naloxone
• Reverses clinical and toxic effects of opioid overdose
– Reverses respiratory depression, hypotension, sedation
– Restores breathing
– Reverses analgesia
– Patients can enter withdrawal after naloxone administration
Pharmacology
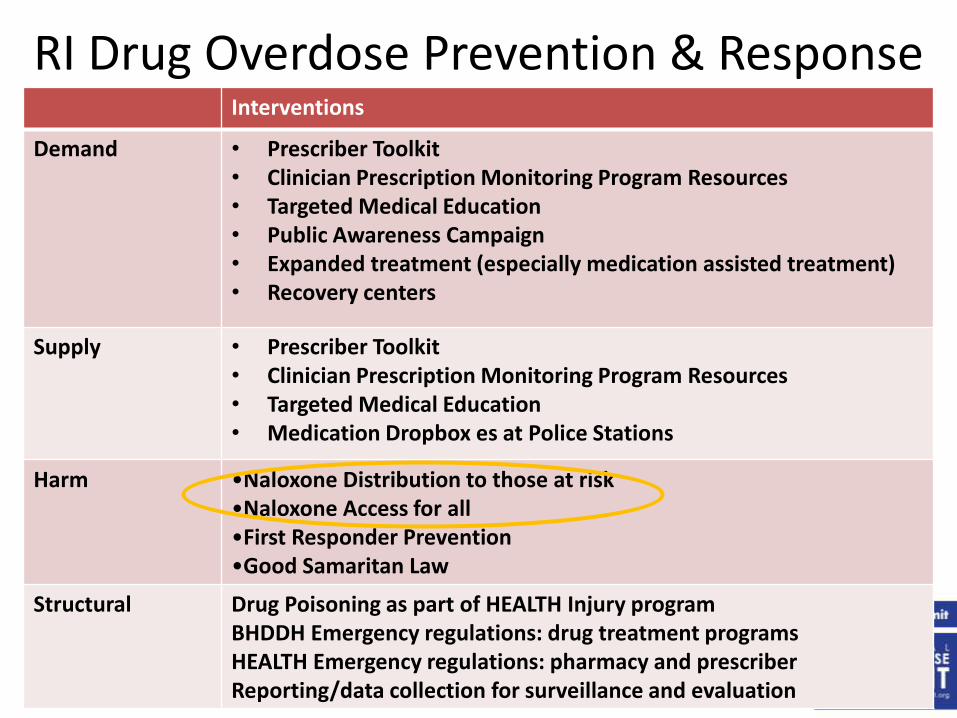
RI Drug Overdose Prevention & ResponseInterventions
Demand • Prescriber Toolkit• Clinician Prescription Monitoring Program Resources• Targeted Medical Education• Public Awareness Campaign• Expanded treatment (especially medication assisted treatment)• Recovery centers
Supply • Prescriber Toolkit• Clinician Prescription Monitoring Program Resources• Targeted Medical Education• Medication Dropbox es at Police Stations
Harm •Naloxone Distribution to those at risk•Naloxone Access for all•First Responder Prevention•Good Samaritan Law
Structural Drug Poisoning as part of HEALTH Injury programBHDDH Emergency regulations: drug treatment programsHEALTH Emergency regulations: pharmacy and prescriberReporting/data collection for surveillance and evaluation
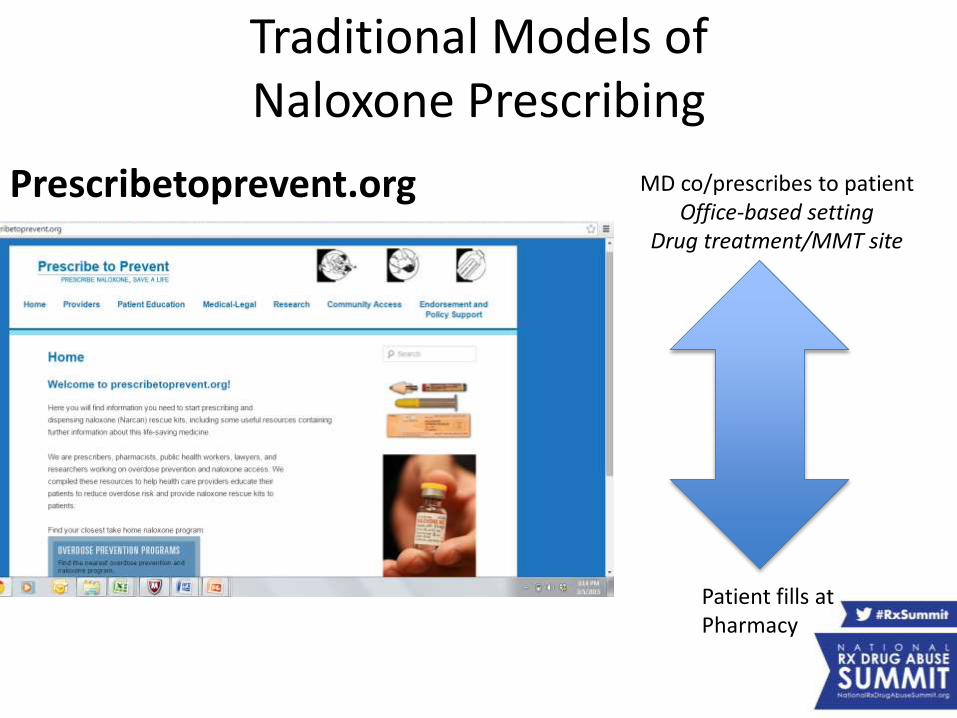
Traditional Models of Naloxone Prescribing
Prescribetoprevent.org MD co/prescribes to patientOffice-based setting
Drug treatment/MMT site
Patient fills atPharmacy
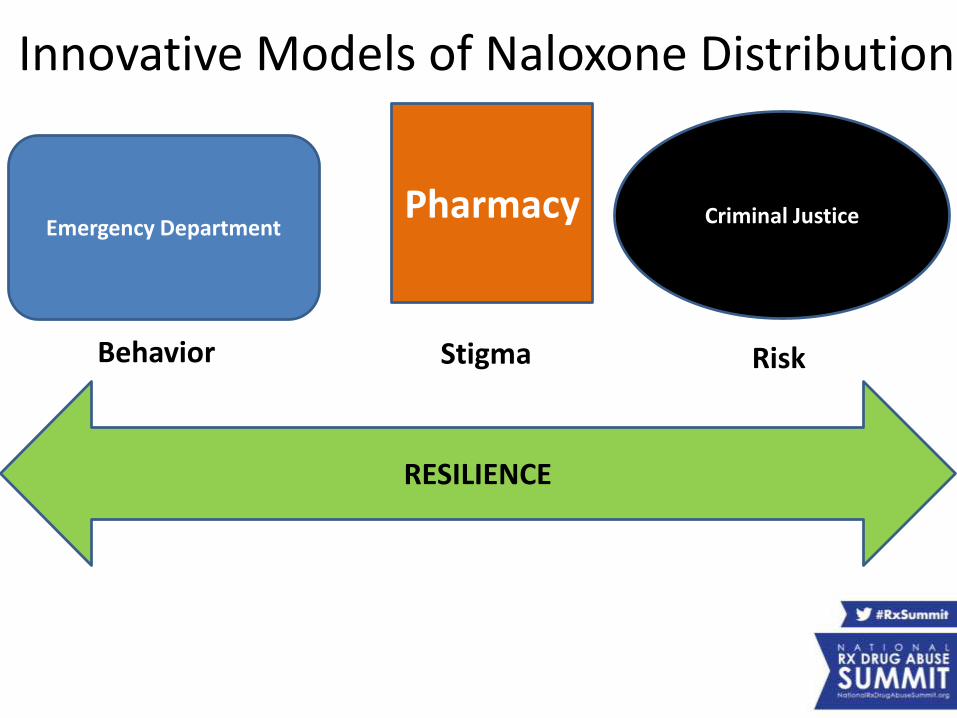
Innovative Models of Naloxone Distribution
Pharmacy
RESILIENCE
Behavior RiskStigma
Emergency DepartmentCriminal Justice

Resilience & Fatal Overdose Prevention• The storytelling we do, not just to survive a
traumatic event, but to grow from it
• Individuals and communities have extraordinary resilience
• Community resilience:
– anticipation, vulnerability reduction, response, recovery

Resilience & Fatal Overdose Prevention• Individual resilience:
– Genetics – Realistic optimism– Strong moral compass– Spiritual sense– Mental/physical fitness– Psychological flexibility– Ability to face one’s fears– Meaningful community service/altruism– Skills in finding purpose & meaning– Availability of resilient role models
– Social support network

Models of Pharmacy Based Naloxone
Collaborative Pharmacy Practice
Agreement
Standing Order
Furnish upon request
Pharmacist prescribes
1 MD ManyPharmDs/Pharmacies
1 MD
1+ Pharmacies
Anyone can be patient
Rhode IslandWashington
Only MD’s patients
Massachusetts
Anyone can be patient
California
Anyone can be patient
New Mexico
Many PharmDs PharmD writes script
MD notified of provision MD notified of provision



RI Collaborative Practice Agreement for Naloxone (CPAN)
• Pharmacist-initiated prescription & distribution of naloxone
• 2011 Pharmacy Board created CPAN
– Pilot: 5 sites
– Statewide expansion following 2013 acetyl fentanyl outbreak
• All Walgreens (26 stores, 95 pharmacists)
• All CVS (63 stores, 295 pharmacists), independent, hospital pharmacies
• Naloxone on Medicaid, private insurer formularies

• Pharmacist – attends compulsory training online
– initiates therapy (naloxone prescription) based on eligibility
– obtains informed consent and release of PHI
– educates the patient on overdose response and furnishes naloxone prescription
– contacts the physician listed on the CPA if medical consultation is needed & alerts them of the medication dispensed within 7 days

• Voluntarily request
– Does not have to be someone at risk of overdose- can be a friend, family member, etc.
• Recipient of emergency medical care for acute opioid poisoning
• Suspected illicit or nonmedical opioid user
• High dose opioid prescription (>100 morphine mg equivalents daily)
• Methadone prescription to opioid naïve patient
Eligible patients to participate in CPAN
Opioid prescription and:
history of smoking
COPD
Respiratory illness or obstruction
renal dysfunction or hepatic disease
Known or suspected concurrent alcohol abuse
Concurrent benzodiazepine prescription
Concurrent SSRI or TCA anti-depressant prescription
Recently released prisoners from a correctional facility
Released from opioid detoxification or mandatory abstinence program
Patients entering a methadone maintenance treatment program
Patients that may have difficulty accessing emergency medical services
Acknowledgement of Informed consent and authorization for release of protected health information
DRAFT SAMPLE DRAFT SAMPLE

• Intramuscular injection into large muscle
– Naloxone HCl solution 0.4mg/ml 1 ml single use vial
• Dispense 2 (two) vials
• 2 (two) syringes - OR -
– Naloxone HCl solution 0.4mg/ml 10 ml multi-dose vial
• 1 (one) vial
• 9 (nine) syringes
• Intranasal
– Naloxone HCl solution 1mg/1ml prefilled 2 ml Luer-Jet syringes
• 2 (two) pre-filled syringes
• At least 1 (one) nasal drug delivery device
• No refills - Total amount dispensed not to exceed 10 mL
Protocol: Dispensing
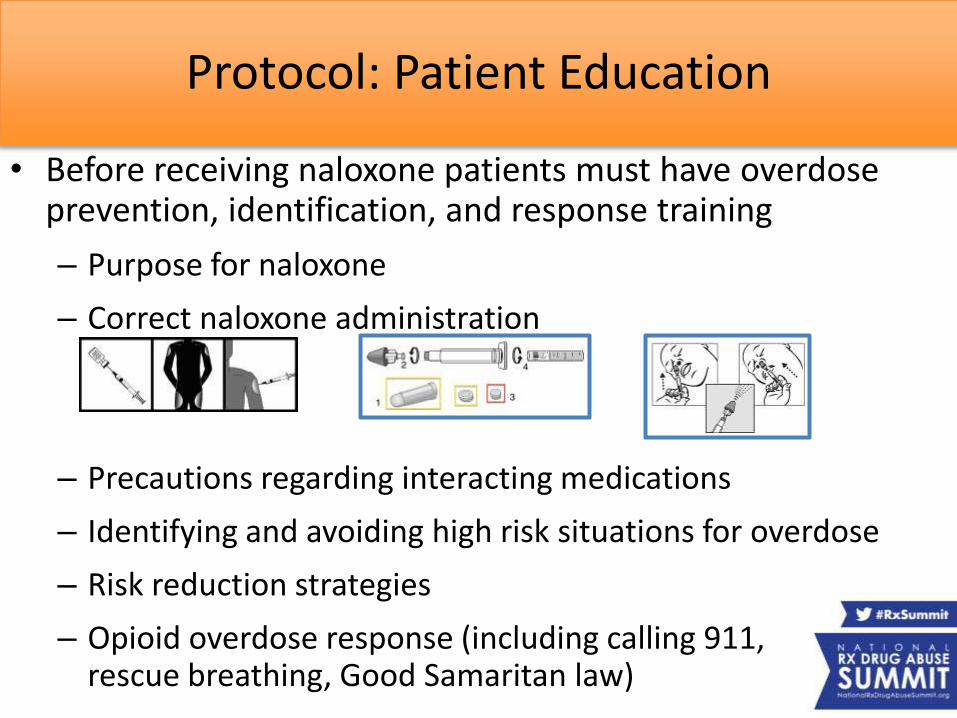
• Before receiving naloxone patients must have overdose prevention, identification, and response training
– Purpose for naloxone
– Correct naloxone administration
– Precautions regarding interacting medications
– Identifying and avoiding high risk situations for overdose
– Risk reduction strategies
– Opioid overdose response (including calling 911, rescue breathing, Good Samaritan law)
Protocol: Patient Education

Improved Naloxone Access through CPAN
• Doubled community naloxone distribution in 2014• Increased geographic reach of community naloxone
programs• Natural partnerships between treatment centers, local
pharmacies• Adds another community resource for addiction
• Extend & build opportunities across healthcare continuum for treatment, recovery
• Reduces stigma– chance to address addiction, overdose with pharmacists– builds support for survivors, families to boost resiliency
RESILIENCE
Barriers & Next Steps
Barriers • Supply & products• Billing, co-pays• Reimbursement for patient counseling time• Time (pharmacist, patient)• Stigma: reaching high risk populations
Next steps • Study Social Marketing of Naloxone• More extensive evaluation, document efforts• Compare and contrast pharmacy based naloxone models• Integrate into curriculum for health professionals and
pharmacy students • Disseminate, Scale up

Risk-Benefit Analysis
• Concerns about increasing naloxone availability:
– Unsafe administration
– Lack of follow up care
– Additional opioids will be used to counter the withdrawal effects
– Persons administering naloxone may be intoxicated themselves
– Seizures, arrhythmias possible in patients with preexisting heart disease
– Availability may encourage riskier, more frequent or higher volume drug use
• Many concerns disproven by data from various community outreach programs
• Naloxone dispensing is relatively new. Data should be continuously collected to gauge full range of benefits, risks, impact


Mikiko Yamada, Pharm.D., M.S., Ph.C.1,2
Ernest Dole, Pharm.D.Ph.C.1,2
Joanna G. Katzman, M.D., MPH2,3
1 University of New Mexico College of Pharmacy2 University of New Mexico Hospital
Pain Consultation and Treatment Center3 University of New Mexico School of Medicine
Intranasal naloxone (INN) used as universal precautions for chronic, noncancer pain (CNCP) patients
on Chronic Opioid Therapy (COT)
Disclosure
• Ernest Dole, PharmD, PhC, FASHP, BCPS has disclosed that he is on the speakers bureau for Millennium Health
• Mikiko Yamada, PharmD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services

• History
• Study-team members
• Support for INN study
• Timeline of INN study
• Study design – Inclusion and exclusion criteria
– How we are different from other major naloxone studies
• Recruitment model
• Patient education
• Recruitment status
• Future plan
Outline
• July 2013– Project started at UNMH Pain Consultation and Treatment
Center (PCTC) with NM Department of Health• Protocol, informed-consent form, study-related materials
• December 2013– IRB application
• January 2014– Modifications of protocol, informed-consent form
• April 2014– IRB approval
• July 2014– Started patient recruitment
History

• Principal investigator
– Joanna Katzman, MD (neurosurgery)
• Co-investigators
– Krishna J. Chari, Psy.D (psychiatry); Ernest Dole, Pharm.D. (pharmacy); Daniel Duhigg, DO (psychiatry); Eugene Koshkin, MD (anesthesiology); Cynthia Olivas, RN (Project ECHO); Brian Starr, MD (anesthesiology); Mikiko Yamada, Pharm.D. (pharmacy)
• Significant contributors from DOH
– Melissa Heinz-Bennett, MPH; Luigi Garcia Saavedra, MPH
Study Team
• Department of Health
– INN kits for all study participants
Support for INN Study
• Timeline of INN study
– Five study visits per year
• Initial, three follow-ups, exit visit
Study Design
End of
study
• Inclusion criteria
A. All patients on COT for CNCP at UNMH PCTC age 18 or older
Study Design

• Exclusion criteria
A. Subjects who are allergic to naloxone and its inactive ingredients
• Inactive ingredients: buffering agents
B. Subjects whose pain etiology is cancer pain or acute pain
C. Subjects pregnant or breastfeeding
• If the study team identities pregnancy of a study subject, the subject will be withdrawn from the study
D. Subject younger than 18
E. Subjects unwilling to sign a consent form
Study Design
• How our study population is unique compared with other studies:
– Includes ALL patients on COT for CNCP regardless of amount of prescribed opioids
• Possible future opioid prescription model
– Universal precautions
– Analogous to the use of an EpiPen® for patients with a history of anaphylaxis, or a glucagon pen and/or sugar tablets being dispensed to patients who use insulin to treat diabetes
Study Design

• Goal of number of study population
– 500 patients per year
• COT prescribed for patients with CNCP at PCTC or outside PCTC
– Primary care physician
– Other pain specialists
» e.g., rheumatologist, neurologist
Study Design

Recruitment ModelSame-day clinic-study visit
Standard careIdentify a potential study candidate
Regular clinic visitClinician
Study visitStudy educator
Ask the patient if he/she is interested in the Naloxone study
(5 minutes)
StopNo future study
participation
No
Start informed-consent process(5 minutes)
Same-day appointment
Not same-day appointment
Assessment, education, and distribution of
naloxone(20 minutes)
Different dayor
next regular clinic visit
Yes
Recruitment ModelSame-day clinic-study visit
• How same-day clinic-study visit affects recruitment?– Increase study population
• Patients do not have to come back to clinic just for INN study education– Convenient for patients
– Save time and extra commute
– Less loss to follow up
– Effective clinic flow• Does not place an extra burden on staff members at
PCTC
• Does not impede patient flow because exam rooms are not tied up

Patient Education
• Education components
– The public health crisis in NM
• NM ranks 3rd for unintentional drug overdose deaths in the United States
• If needed patient’s are encourage to use the INN for others than it was prescribed for
– What is a drug overdose looks like
• Symptoms, what to do, what not to do
– How to use INN• Demonstrate how to assemble INN kit
Patient Education
• Educators
– Pharmacists
• Dr. Dole and Dr. Yamada
– Nurse
• Cynthia Olivas
– Medical/pharmacy students
• APPE students and third-year medical/pharmacy students
– Great opportunity to learn about public health issue
– Exposure to research
– Research assistants– Department of Neurosurgery
• Recruitment status
– Study started on July 22, 2014
– Participants at PCTC: 114 patients as of 2.26.2015
Recruitment Status

• INN study will last two years from July 2014
• The team will recruit at least 500 patients
• Study data will be shared with DOH
• Enroll patients from Alcohol and Substance Abuse Program (ASAP) at University of New Mexico
Future Plan

Pharmacist Prescribing Naloxone Under Protocol in New Mexico
• Pharmacist Education and Training– Live CE every 2 years
• Patient Consent– Patient is screened and evaluated by the Pharmacist
for the risk of overdose.
– Patient consent form must be completed and signed before the prescribing and dispensing of naloxone.
– Notify the patient’s primary care provider with the consent of the patient within 15 days of the original prescription.
Pharmacist Prescribing Naloxone Under Protocol in New Mexico
• Patient Screening Criteria– Prescribed long-acting opioid (oxycodone ER,
oxymorphone ER, morphine ER, transdermal fentanyl, methadone or buprenorphine).
– A high daily dose of opioid prescribed. Inclusion and exclusion criteria will be included in the Pharmacist’s training
– Prescribed opiates or opioid use greater than 30 days. – History of or current polyopioid use. – Concurrent prescription or OTC medication that could
potentiate the CNS and respiratory depressant properties of opioid medications, such as benzodiazepines, antipsychotics, carisoprodol, and/or antihistamine use.

Pharmacist Prescribing Naloxone Under Protocol in New Mexico
• Patient Screening Criteria (continued)– Elderly patients (> 65) receiving an opioid
prescription. – Households with people at risk of overdose, such as
children and/or someone with a substance abuse disorder.
– Patients who may have difficulty accessing emergency medical services (distance, remoteness, lack of transportation, homelessness, and/or without phone services).
– Patients as determined by the Pharmacist using their professional judgment

Pharmacist Prescribing Naloxone Under Protocol in New Mexico
• Patient RecordsOnce the patient is identified to be at high risk, the Pharmacist will
provide overdose prevention education and training, which includes proper administration of nasal naloxone and the required immediate medical follow-up after proper use of naloxone.
Face-to-face education is required on the proper use of the naloxone, including a plan for overdose prevention and adverse effects. A designated rescue person or persons must be identified by the patient.
Patients will be provided with educational materials and a handout describing caregiver medication administration.
Family member, caregiver, and/or friend are strongly encouraged to attend the appointment at the discretion of the prescribing Pharmacist, to also receive training at the time the patient receives the naloxone.
Pharmacist Prescribing Naloxone Under Protocol in New Mexico
• Patient Records (continued)Follow-up training and reinforcement is encouraged, the Pharmacist
will provide their contact information for any questions or concerns.
In the event the naloxone is used or expired, the patient will return to the Pharmacist to request a new prescription; a thorough evaluation will be completed by the Pharmacist regarding the events leading to naloxone use and to determine whether appropriate medical follow-up was completed, as required.
On site documentation of reported use to summarize approximate time/date naloxone was used, number of doses used, name of patient
Questions and comments
Pharmacy Track:Expanding Use of Naloxone
Presenters:
• Traci Green, PhD, MSC, Brown University and Boston University/Boston Medical Center
• Ernest J. Dole, PharmD, PhC, FASHP, BCPS, Pain Consultation and Treatment Center, University of New Mexico Hospitals
• Mikiko Yamada, PharmD, University of New Mexico College of Pharmacy and Pediatric Neurology Clinic and Pain Consultation and Treatment Center
Moderator: CDR Christopher M. Jones, PharmD, MPH, U.S. Food and Drug Administration, and Member, Rx Summit National Advisory Board