Rx15 pdmp wed_300_1_stripp_2lev-lucas
53
PDMP Track: Combining PDMP and Other Data to Combat Rx Drug Abuse Presenters: • Richard Stripp, PhD, Chief Scientific and Technical Officer, Cordant Health Solutions • Roneet Lev, MD, Director of Operations, Scripps Mercy Hospital Emergency Department, and Chair, San Diego County (CA) Rx Drug Abuse Medical Task Force • Jonathan Lucas, MD, Chief Deputy Medical Examiner, San Diego County (CA) Moderator: Connie M. Payne, Executive Officer, Statewide Services, Administrative Office of the Courts, and Member, Operation UNITE Board of Directors
-
Upload
opunite -
Category
Healthcare
-
view
333 -
download
6
Transcript of Rx15 pdmp wed_300_1_stripp_2lev-lucas
PDMP Track:Combining PDMP and Other Data
to Combat Rx Drug AbusePresenters:
• Richard Stripp, PhD, Chief Scientific and Technical Officer, CordantHealth Solutions
• Roneet Lev, MD, Director of Operations, Scripps Mercy Hospital Emergency Department, and Chair, San Diego County (CA) Rx Drug Abuse Medical Task Force
• Jonathan Lucas, MD, Chief Deputy Medical Examiner, San Diego County (CA)
Moderator: Connie M. Payne, Executive Officer, Statewide Services, Administrative Office of the Courts, and Member, Operation UNITE Board of Directors
Disclosures
• Richard Stripp, PhD – Employment: Cordant Health Solutions (formerly Sterling Healthcare Services)
• Roneet Lev, MD; Jonathan Lucas, MD; and Connie M. Payne have disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition
Learning Objectives
1. Identify reasons and methods for combining PDMP data with other data.
2. Evaluate the effectiveness of combining laboratory and PDMP data to identify patients who are not taking Rx medication responsibly, based on a nationwide study.
3. Describe a San Diego collaborative project that combines PDMP and medical examiner data.
Combining PDMP and Other Data to Combat Rx Drug Abuse
Disclosure
• Richard Stripp, Chief Scientific & Technical Officer, wishes to disclose he is an employee of Cordant Health Solutions. He will present this content in a fair and balanced manner.
Learning Objectives
1. Identify reasons and methods for combining PDMP data with other data.
2. Evaluate the effectiveness of combining laboratory and PDMP data to identify patients who are not taking Rx medication responsibly, based on a nationwide study.
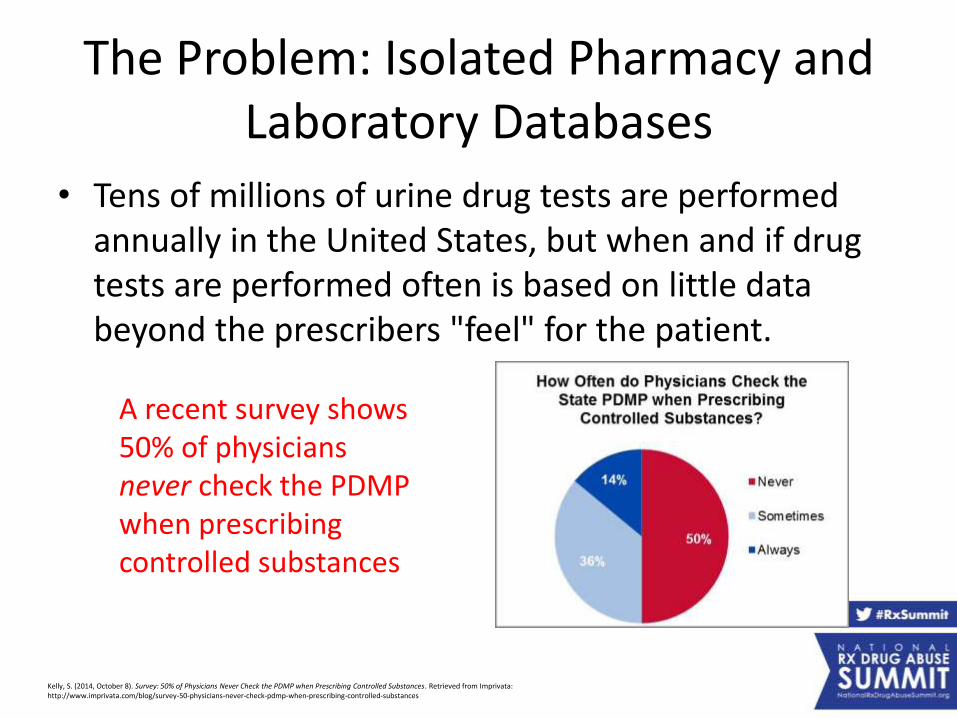
The Problem: Isolated Pharmacy and Laboratory Databases
• Tens of millions of urine drug tests are performed annually in the United States, but when and if drug tests are performed often is based on little data beyond the prescribers "feel" for the patient.
Kelly, S. (2014, October 8). Survey: 50% of Physicians Never Check the PDMP when Prescribing Controlled Substances. Retrieved from Imprivata: http://www.imprivata.com/blog/survey-50-physicians-never-check-pdmp-when-prescribing-controlled-substances
A recent survey shows 50% of physicians never check the PDMP when prescribing controlled substances
The Problem: Not all patients are created equal
• Without guidance based on patient-specific data on who and when to test, physicians struggle with drug testing.
The downstream effects of this are:
• Underutilization• Overutilization• Inflated drug testing
costs
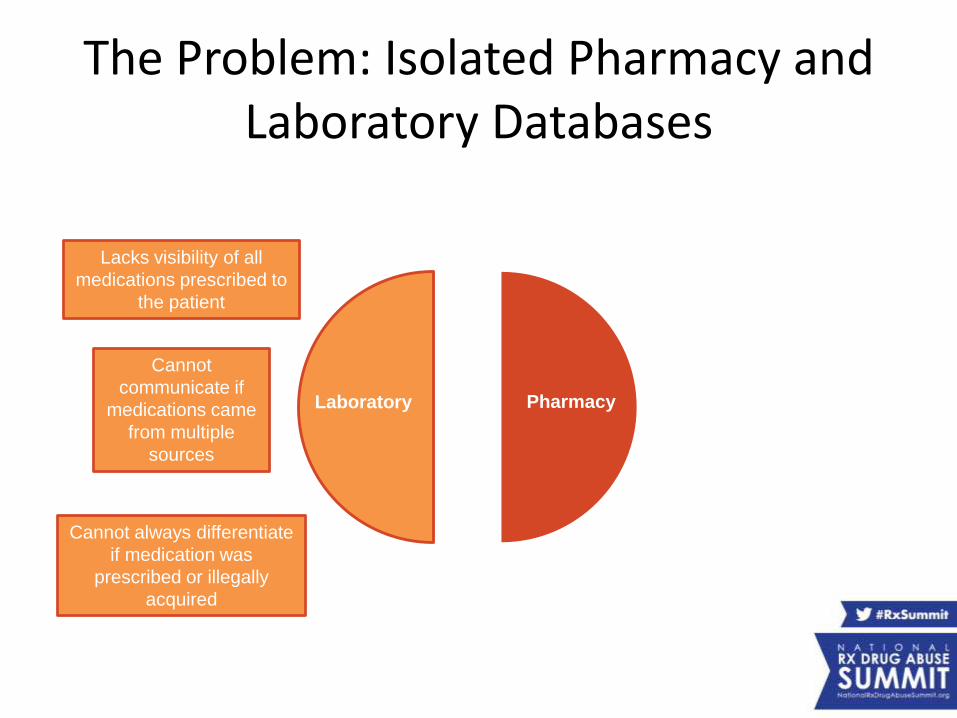
The Problem: Isolated Pharmacy and Laboratory Databases
Laboratory Pharmacy
Lacks visibility of all
medications prescribed to
the patient
Cannot
communicate if
medications came
from multiple
sources
Cannot always differentiate
if medication was
prescribed or illegally
acquired
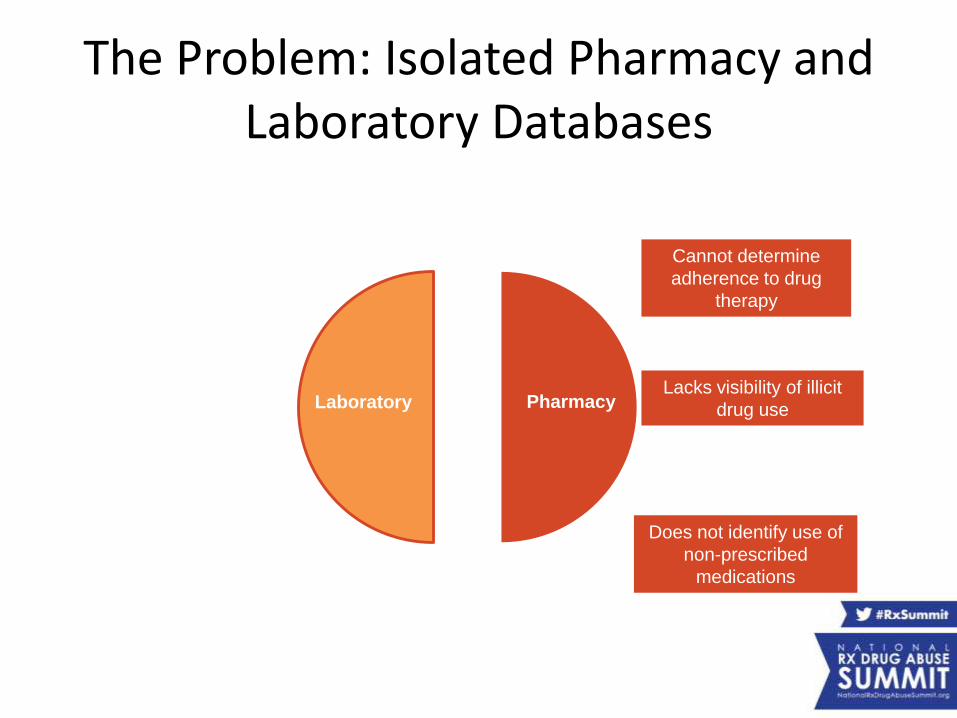
The Problem: Isolated Pharmacy and Laboratory Databases
Laboratory Pharmacy
Cannot determine
adherence to drug
therapy
Lacks visibility of illicit
drug use
Does not identify use of
non-prescribed
medications
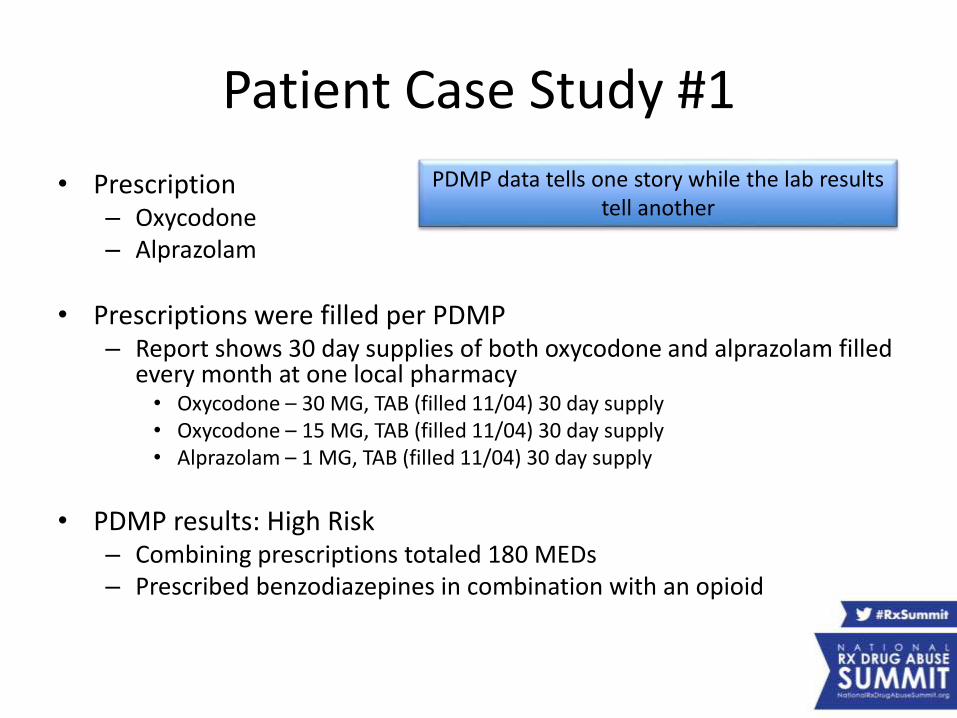
Patient Case Study #1
• Prescription– Oxycodone– Alprazolam
• Prescriptions were filled per PDMP– Report shows 30 day supplies of both oxycodone and alprazolam filled
every month at one local pharmacy• Oxycodone – 30 MG, TAB (filled 11/04) 30 day supply• Oxycodone – 15 MG, TAB (filled 11/04) 30 day supply• Alprazolam – 1 MG, TAB (filled 11/04) 30 day supply
• PDMP results: High Risk– Combining prescriptions totaled 180 MEDs– Prescribed benzodiazepines in combination with an opioid
PDMP data tells one story while the lab results tell another
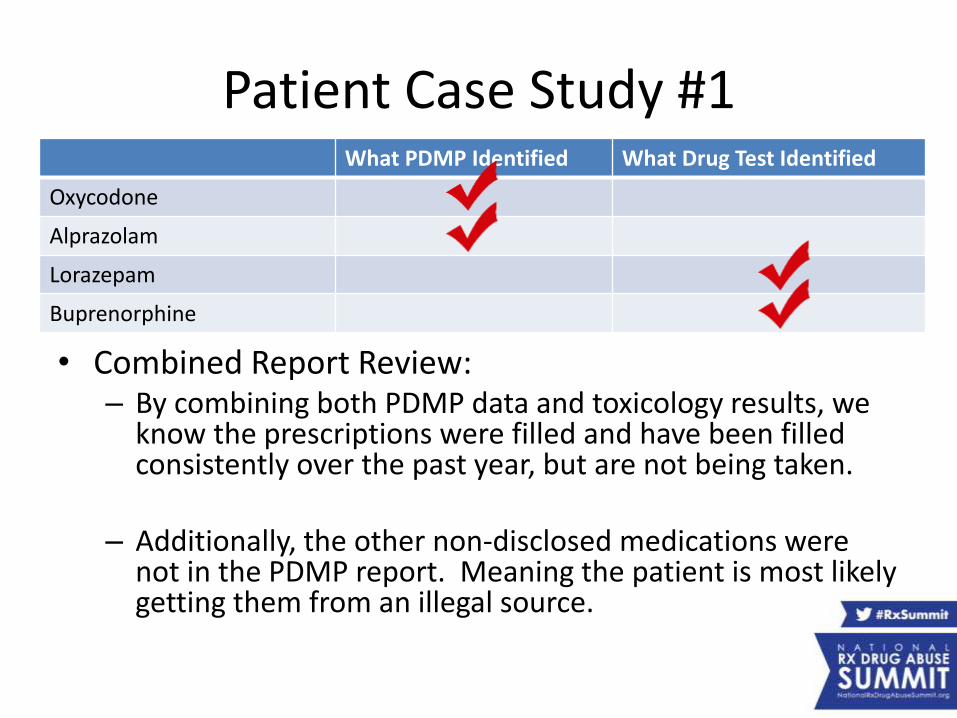
Patient Case Study #1
• Combined Report Review:– By combining both PDMP data and toxicology results, we
know the prescriptions were filled and have been filled consistently over the past year, but are not being taken.
– Additionally, the other non-disclosed medications were not in the PDMP report. Meaning the patient is most likely getting them from an illegal source.
What PDMP Identified What Drug Test Identified
Oxycodone
Alprazolam
Lorazepam
Buprenorphine
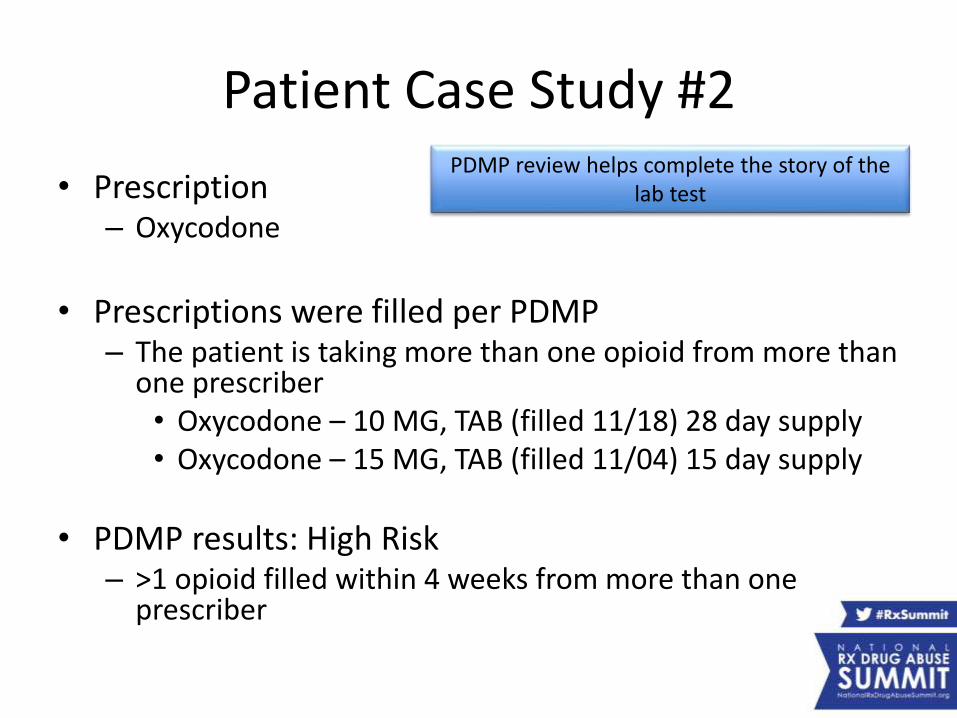
Patient Case Study #2
• Prescription– Oxycodone
• Prescriptions were filled per PDMP– The patient is taking more than one opioid from more than
one prescriber• Oxycodone – 10 MG, TAB (filled 11/18) 28 day supply• Oxycodone – 15 MG, TAB (filled 11/04) 15 day supply
• PDMP results: High Risk– >1 opioid filled within 4 weeks from more than one
prescriber
PDMP review helps complete the story of the lab test
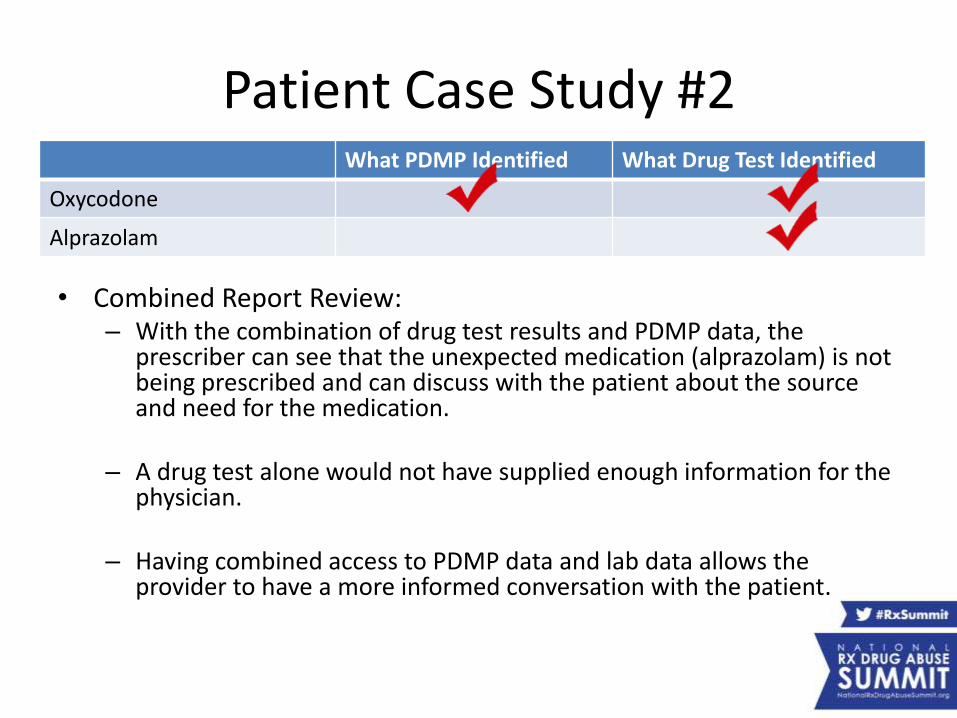
Patient Case Study #2
• Combined Report Review:– With the combination of drug test results and PDMP data, the
prescriber can see that the unexpected medication (alprazolam) is not being prescribed and can discuss with the patient about the source and need for the medication.
– A drug test alone would not have supplied enough information for the physician.
– Having combined access to PDMP data and lab data allows the provider to have a more informed conversation with the patient.
What PDMP Identified What Drug Test Identified
Oxycodone
Alprazolam
Of course the results of one or two case studies cannot predict the behavior of an entire population.
How does combining pharmacy & laboratory data work to identify high risk patients everywhere?
The Study
• Scope
– In April through June 2014, Cordant conducted 257 toxicology screens on 237 injured workers across 48 states.
– Test subjects were selected from the pool of patients meeting key risk identifiers according to PBM data.
The Study
• The Process– Cordant applied the several parameters to the study
group using their pharmacy data to identify potential risk.
– Risk criteria identified about 1/4th of the injured worker population as potentially “high risk”.
– Once patients were identified as potentially high risk, urine samples were collected at the doctor’s office during their next visit and sent to one of Cordant’s five laboratories for testing.
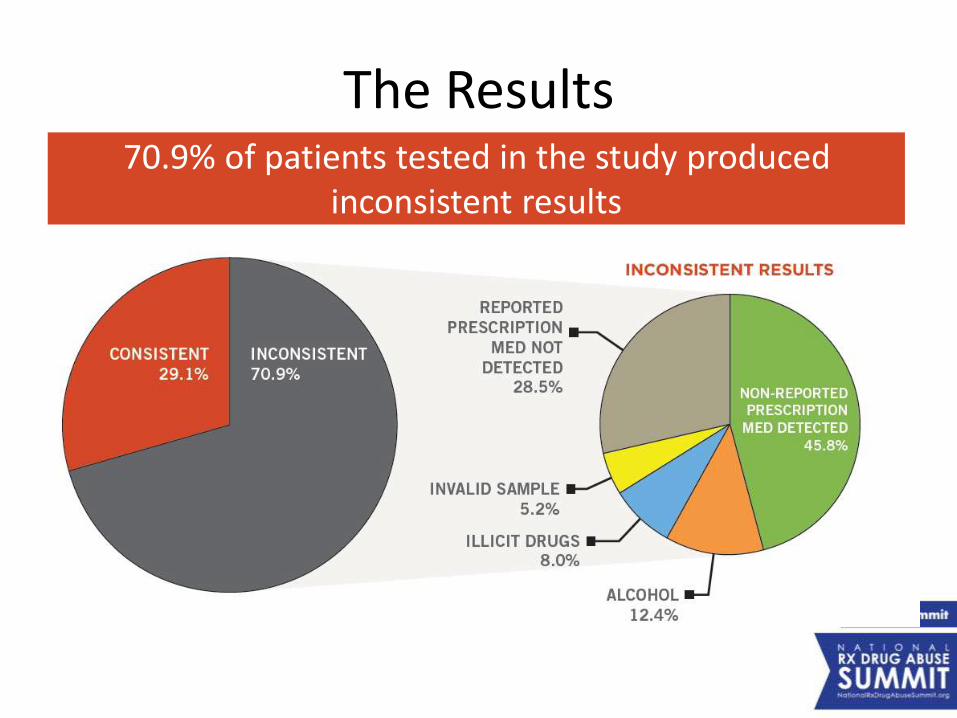
The Results70.9% of patients tested in the study produced
inconsistent results
The Results
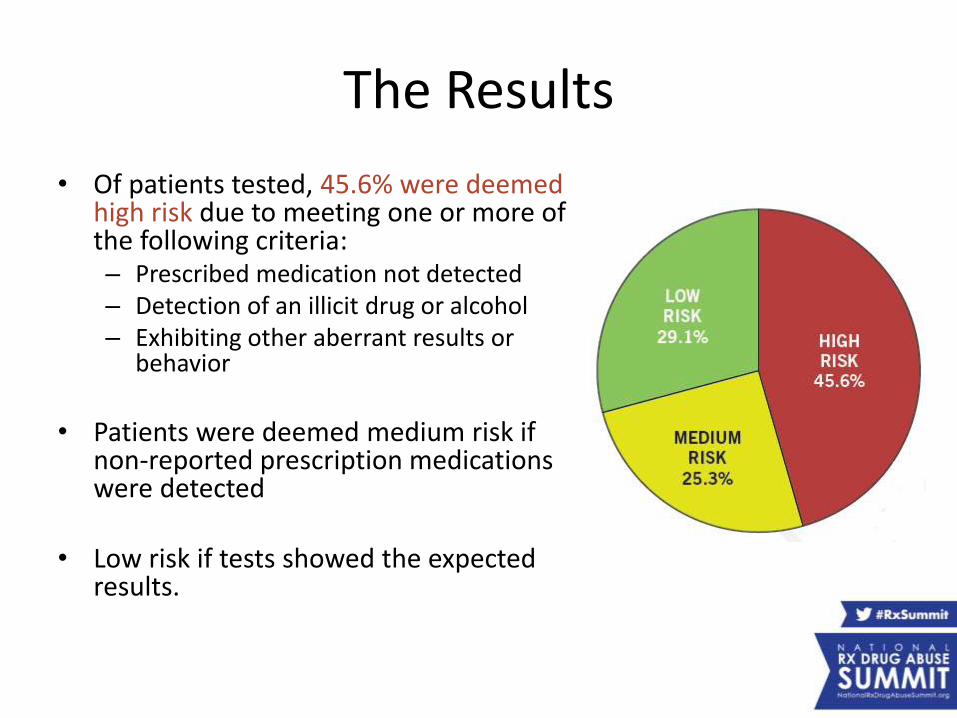
• Of patients tested, 45.6% were deemed high risk due to meeting one or more of the following criteria:– Prescribed medication not detected– Detection of an illicit drug or alcohol– Exhibiting other aberrant results or
behavior
• Patients were deemed medium risk if non-reported prescription medications were detected
• Low risk if tests showed the expected results.
The Results
• Toxicology testing revealed high degrees of inconsistent test results among the tested claimants who fit these parameters:
– Prescribed a high medication dosage: 70.9%inconsistent test results.
– On the prescribed opioid for more than two months: 73.8% inconsistent test results.
(Claimants in this group were often prescribed higher doses and for a longer duration than claimants in other groups.)
Conclusion
• Combining pharmacy and laboratory data is extremely effective in identifying high-risk opioid users.– Reduces inflated drug testing costs by identifying those most
likely to abuse or misuse medications.– Improves patient outcomes by giving the physician a more
complete picture
• Getting the right medication to the Patient at the right time, in the right dose, and with the right monitoring requires a combination of:– care coordination– lab and prescription data integration– and clinical expertise
Thank You
Medical Examiner and CURES Correlations
San Diego 2013
Roneet Lev, MD Scripps Mercy HospitalSean PetroOren Lee
Jonathan Lucas, MD San Diego Medical Examiner
24
Disclosures
• Roneet Lev, MD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Jonathan Lucas, MD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
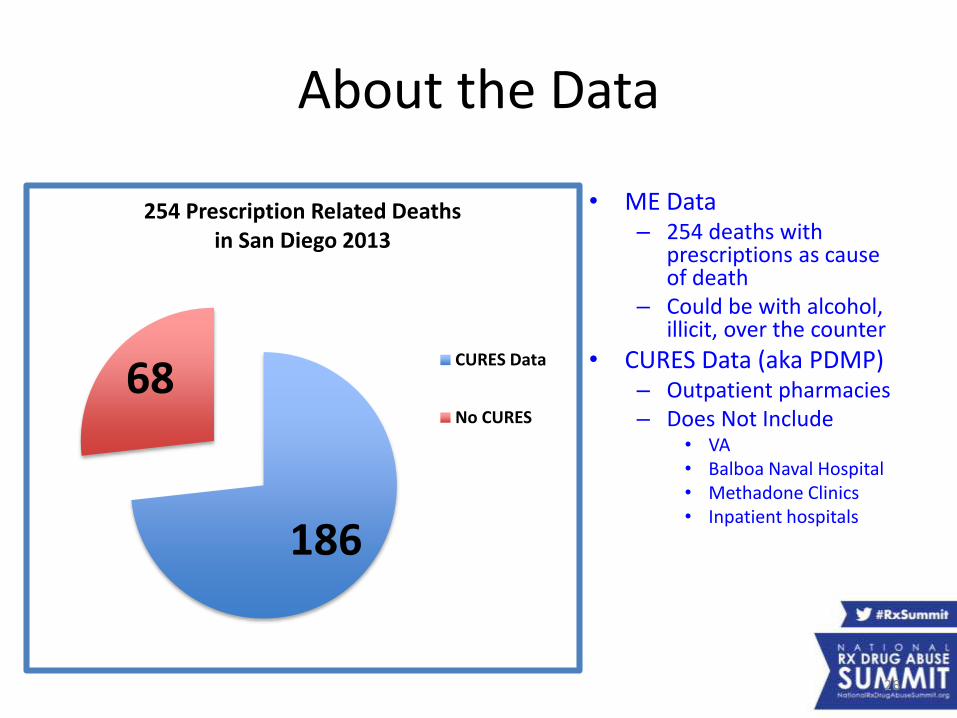
About the Data
• ME Data– 254 deaths with
prescriptions as cause of death
– Could be with alcohol, illicit, over the counter
• CURES Data (aka PDMP)– Outpatient pharmacies– Does Not Include
• VA• Balboa Naval Hospital• Methadone Clinics• Inpatient hospitals
186
68
254 Prescription Related Deaths in San Diego 2013
CURES Data
No CURES
26
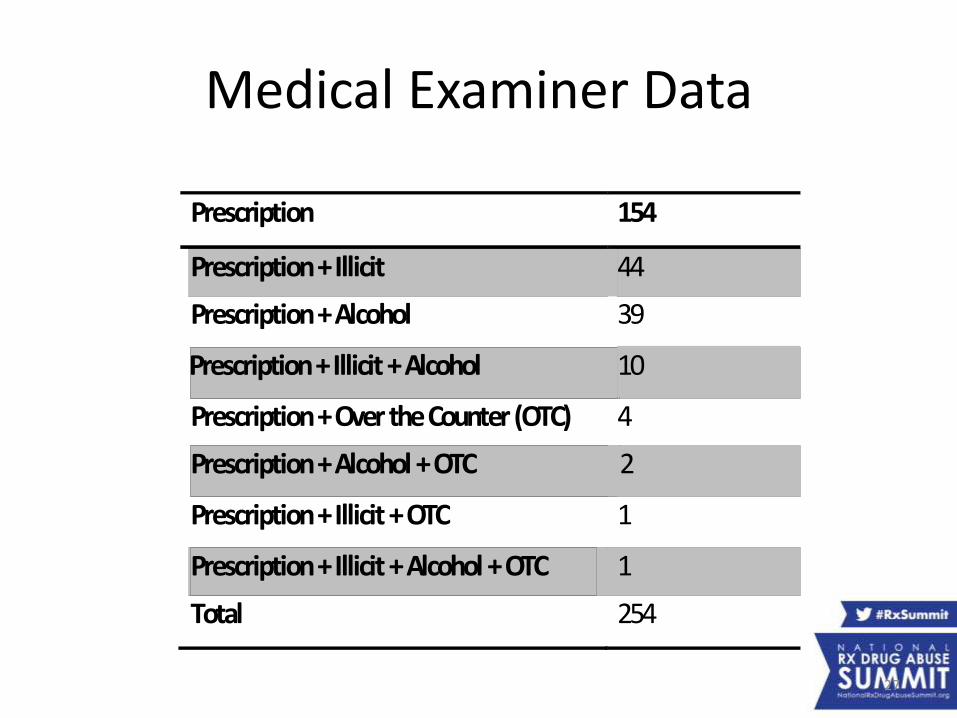
Medical Examiner Data
Prescription 154
Prescription+Illicit 44
Prescription+Alcohol 39
Prescription+Illicit+Alcohol 10
Prescription+OvertheCounter(OTC) 4
Prescription+Alcohol+OTC 2
Prescription+Illicit+OTC 1
Prescription+Illicit+Alcohol+OTC 1
Total 254
27
“Death Diaries”
CURES Report
28
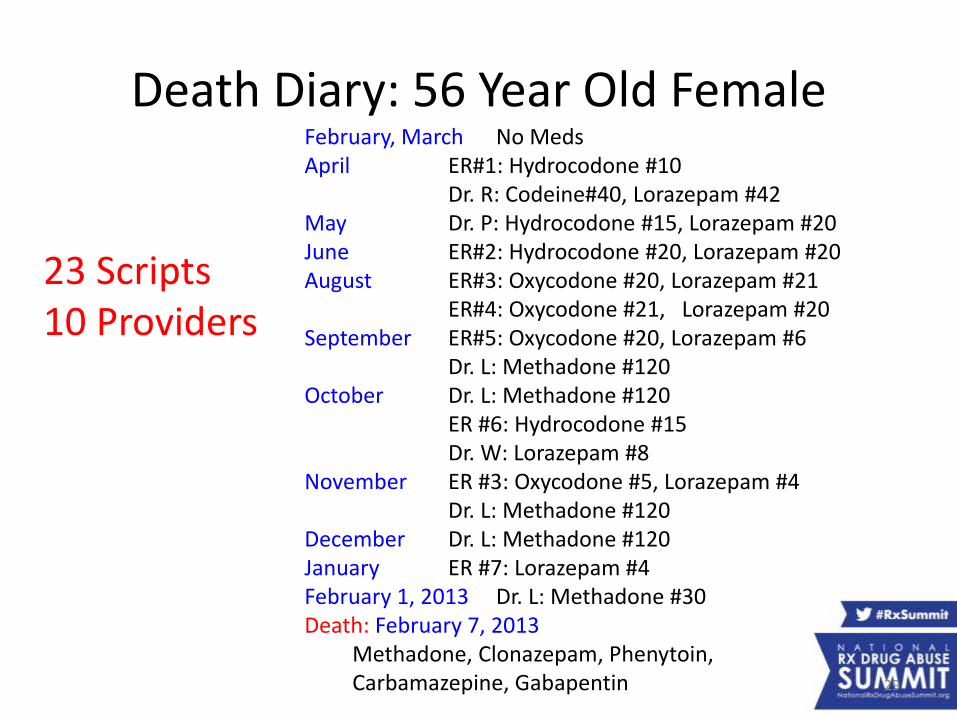
Death Diary: 56 Year Old Female
23 Scripts10 Providers
29
February, March No MedsApril ER#1: Hydrocodone #10
Dr. R: Codeine#40, Lorazepam #42May Dr. P: Hydrocodone #15, Lorazepam #20June ER#2: Hydrocodone #20, Lorazepam #20August ER#3: Oxycodone #20, Lorazepam #21
ER#4: Oxycodone #21, Lorazepam #20September ER#5: Oxycodone #20, Lorazepam #6
Dr. L: Methadone #120October Dr. L: Methadone #120
ER #6: Hydrocodone #15Dr. W: Lorazepam #8
November ER #3: Oxycodone #5, Lorazepam #4Dr. L: Methadone #120
December Dr. L: Methadone #120January ER #7: Lorazepam #4February 1, 2013 Dr. L: Methadone #30Death: February 7, 2013
Methadone, Clonazepam, Phenytoin, Carbamazepine, Gabapentin
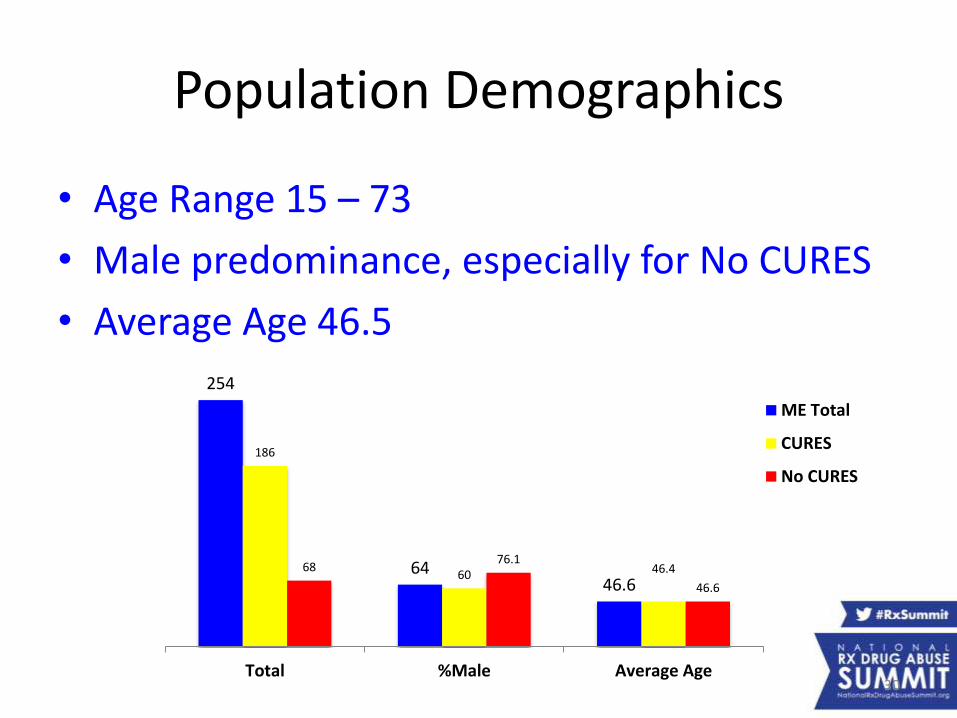
Population Demographics
• Age Range 15 – 73
• Male predominance, especially for No CURES
• Average Age 46.5
254
6446.6
186
60 46.46876.1
46.6
Total %Male Average Age
ME Total
CURES
No CURES
30
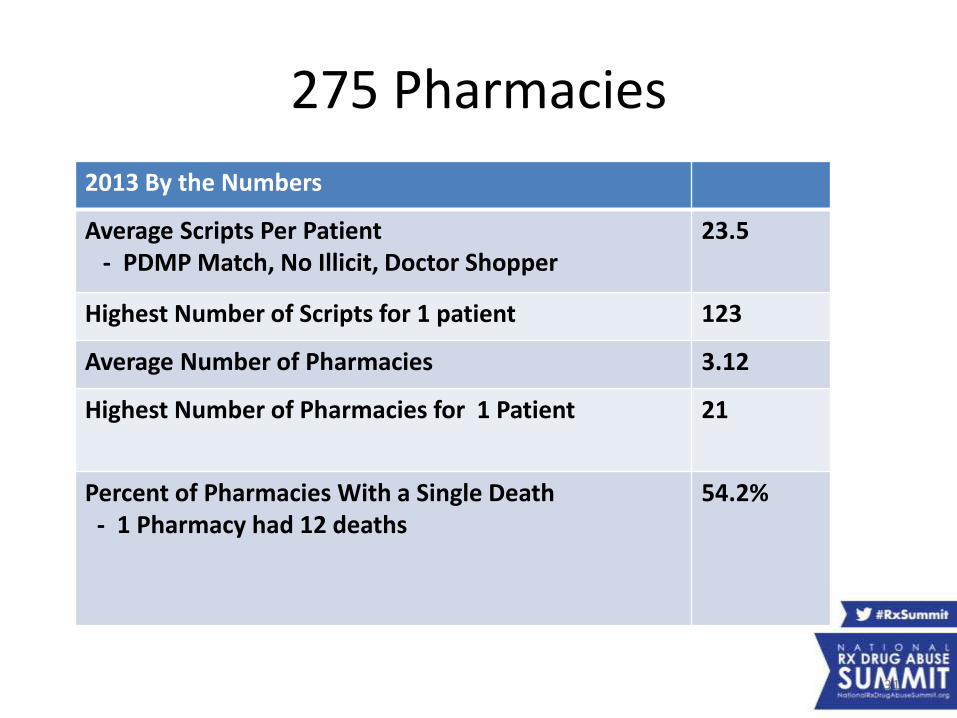
275 Pharmacies
2013 By the Numbers
Average Scripts Per Patient - PDMP Match, No Illicit, Doctor Shopper
23.5
Highest Number of Scripts for 1 patient 123
Average Number of Pharmacies 3.12
Highest Number of Pharmacies for 1 Patient 21
Percent of Pharmacies With a Single Death- 1 Pharmacy had 12 deaths
54.2%
31
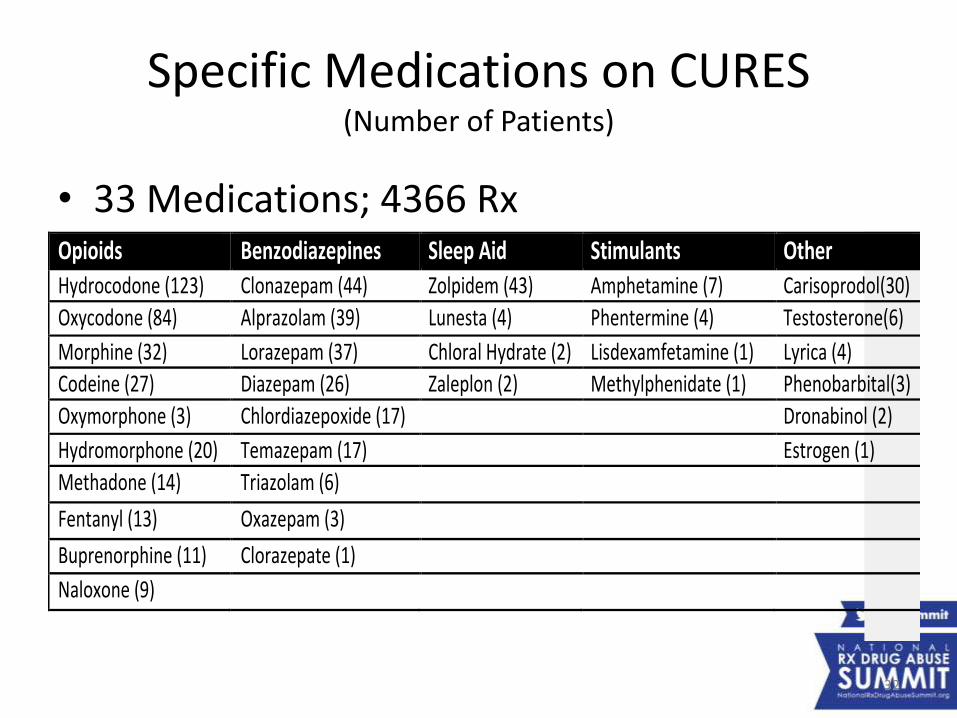
Specific Medications on CURES(Number of Patients)
• 33 Medications; 4366 RxOpioids Benzodiazepines SleepAid Stimulants OtherHydrocodone(123) Clonazepam(44) Zolpidem(43) Amphetamine(7) Carisoprodol(30)
Oxycodone(84) Alprazolam(39) Lunesta(4) Phentermine(4) Testosterone(6)
Morphine(32) Lorazepam(37) ChloralHydrate(2) Lisdexamfetamine(1) Lyrica(4)
Codeine(27) Diazepam(26) Zaleplon(2) Methylphenidate(1) Phenobarbital(3)
Oxymorphone(3) Chlordiazepoxide(17) Dronabinol(2)
Hydromorphone(20) Temazepam(17) Estrogen(1)
Methadone(14) Triazolam(6) Fentanyl(13) Oxazepam(3) Buprenorphine(11) Clorazepate(1) Naloxone(9)
32
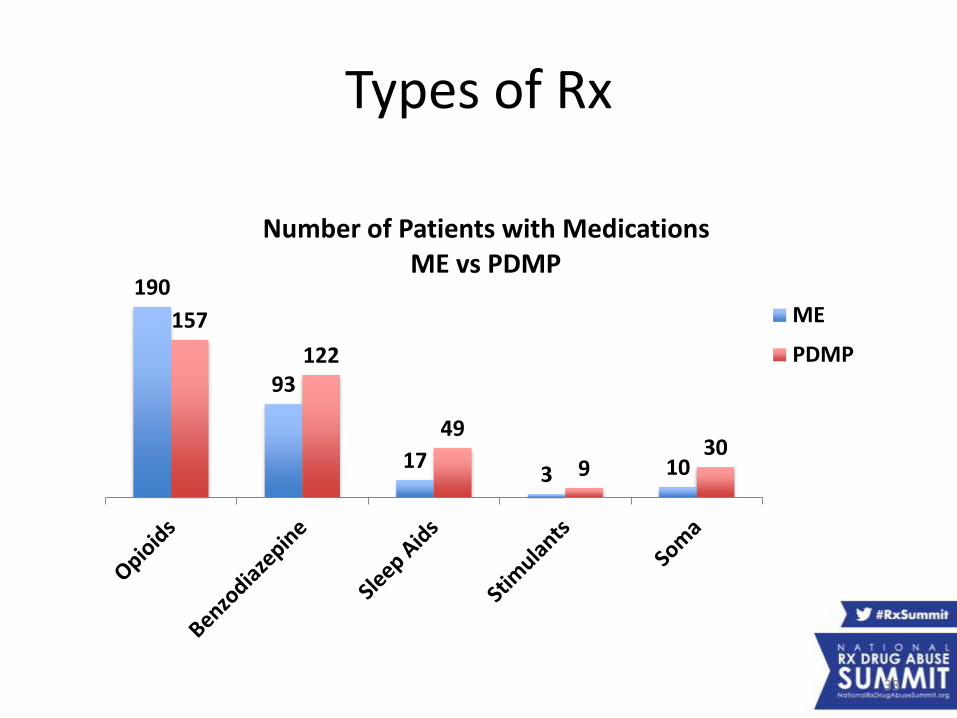
Types of Rx
190
93
173 10
157
122
49
930
Number of Patients with MedicationsME vs PDMP
ME
PDMP
33
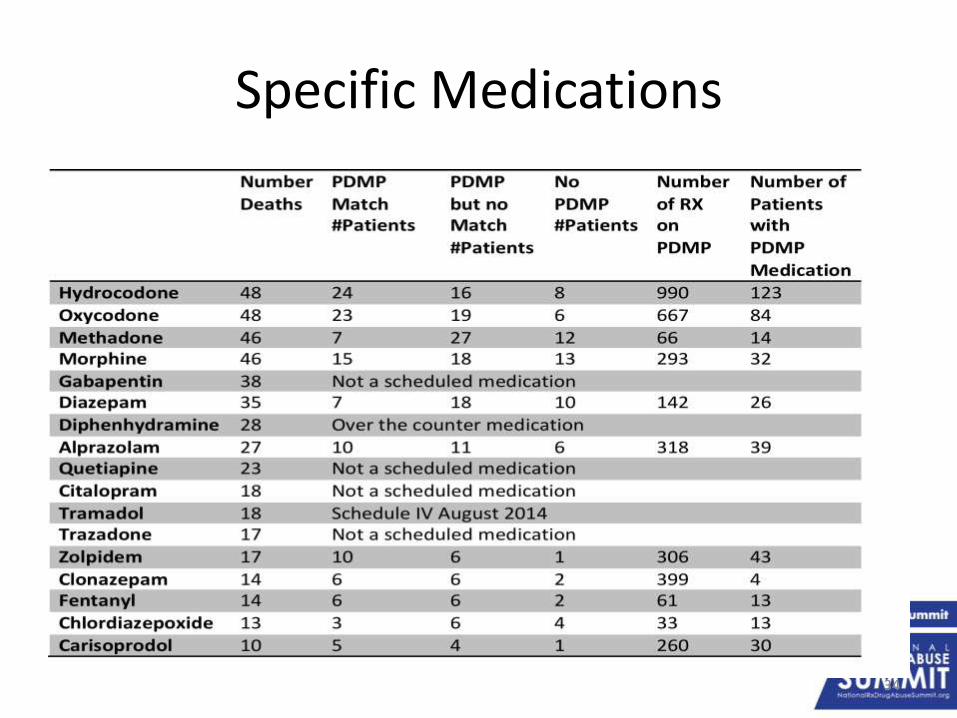
Specific Medications
34
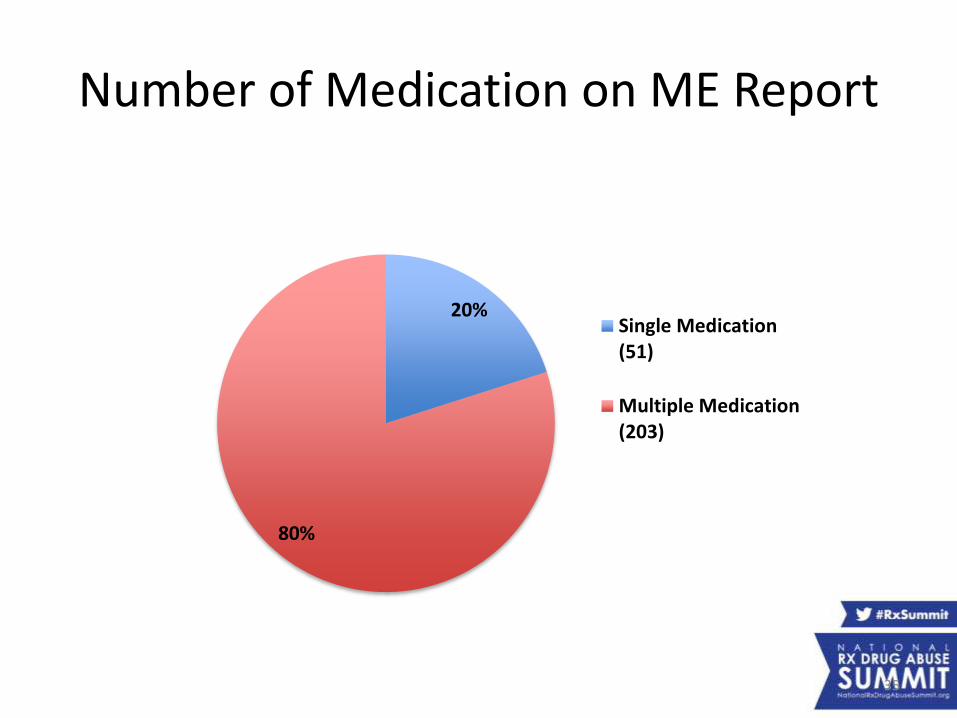
Number of Medication on ME Report
35
20%
80%
Single Medication(51)
Multiple Medication(203)
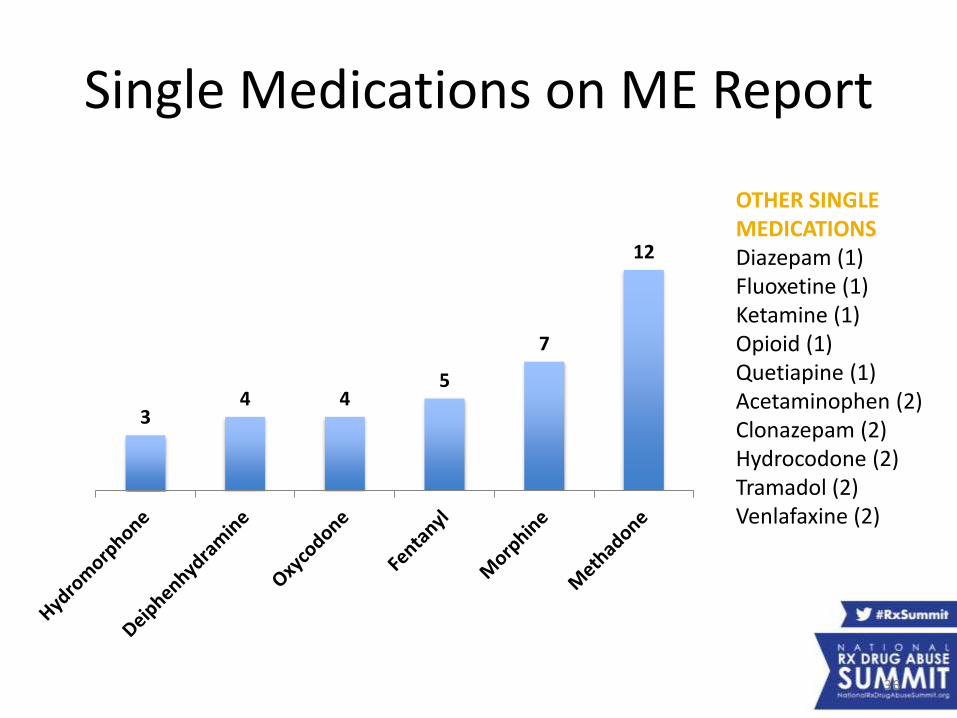
Single Medications on ME Report
36
34 4
5
7
12
OTHER SINGLE MEDICATIONSDiazepam (1)Fluoxetine (1)Ketamine (1)Opioid (1)Quetiapine (1)Acetaminophen (2)Clonazepam (2)Hydrocodone (2)Tramadol (2)Venlafaxine (2)
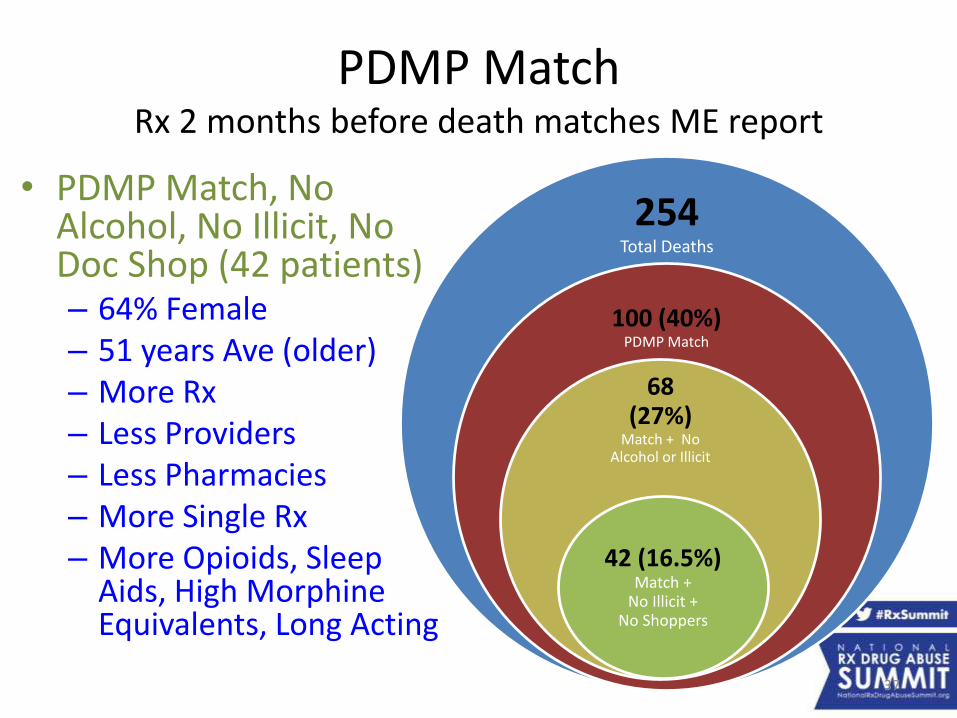
PDMP MatchRx 2 months before death matches ME report
• PDMP Match, No Alcohol, No Illicit, No Doc Shop (42 patients)– 64% Female– 51 years Ave (older) – More Rx– Less Providers– Less Pharmacies– More Single Rx– More Opioids, Sleep
Aids, High Morphine Equivalents, Long Acting
254Total Deaths
100 (40%)PDMP Match
68 (27%)
Match + No Alcohol or Illicit
42 (16.5%) Match +
No Illicit + No Shoppers
37
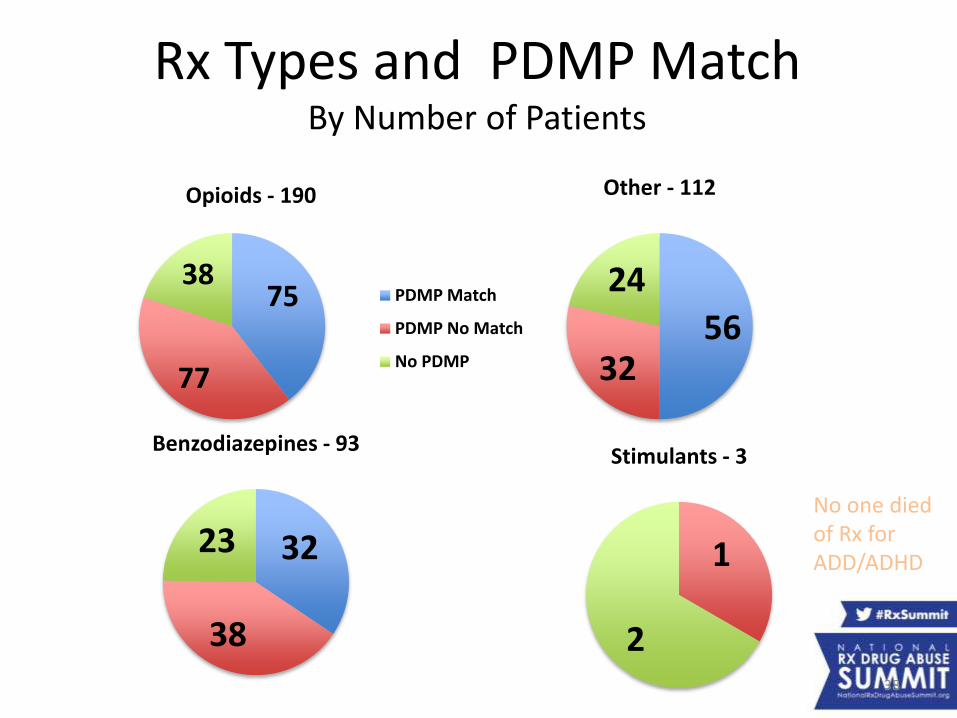
Rx Types and PDMP MatchBy Number of Patients
75
77
38
Opioids - 190
PDMP Match
PDMP No Match
No PDMP
32
38
23
Benzodiazepines - 93
1
2
Stimulants - 3
5632
24
Other - 112
No one died of Rx for ADD/ADHD
38
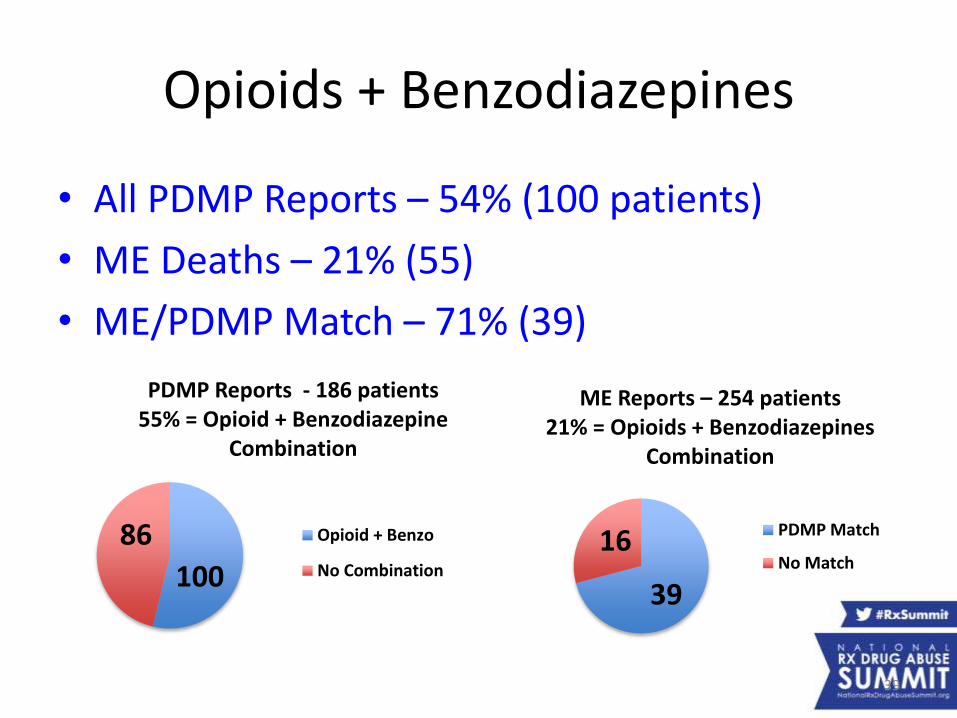
Opioids + Benzodiazepines
• All PDMP Reports – 54% (100 patients)
• ME Deaths – 21% (55)
• ME/PDMP Match – 71% (39)
39
16
ME Reports – 254 patients21% = Opioids + Benzodiazepines
Combination
PDMP Match
No Match100
86
PDMP Reports - 186 patients55% = Opioid + Benzodiazepine
Combination
Opioid + Benzo
No Combination
39
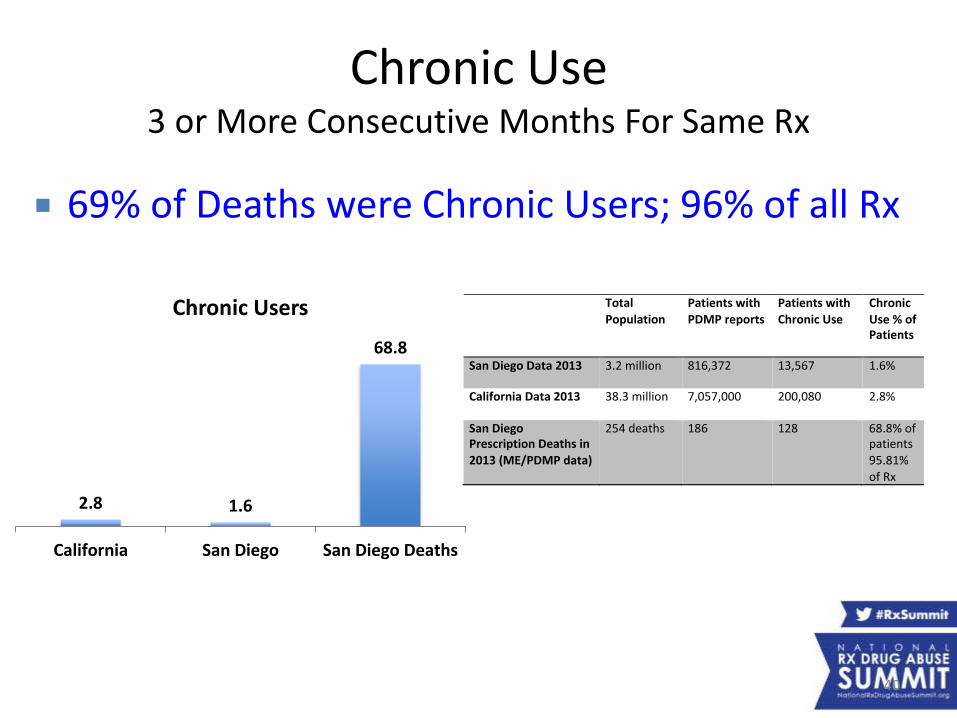
Chronic Use3 or More Consecutive Months For Same Rx
Total
Population
Patientswith
PDMPreports
Patientswith
ChronicUse
Chronic
Use%ofPatients
SanDiegoData2013 3.2million 816,372 13,567 1.6%
CaliforniaData2013 38.3million 7,057,000 200,080 2.8%
SanDiegoPrescriptionDeathsin
2013(ME/PDMPdata)
254deaths 186 128 68.8%ofpatients
95.81%ofRx
69% of Deaths were Chronic Users; 96% of all Rx
2.8 1.6
68.8
California San Diego San Diego Deaths
Chronic Users
40
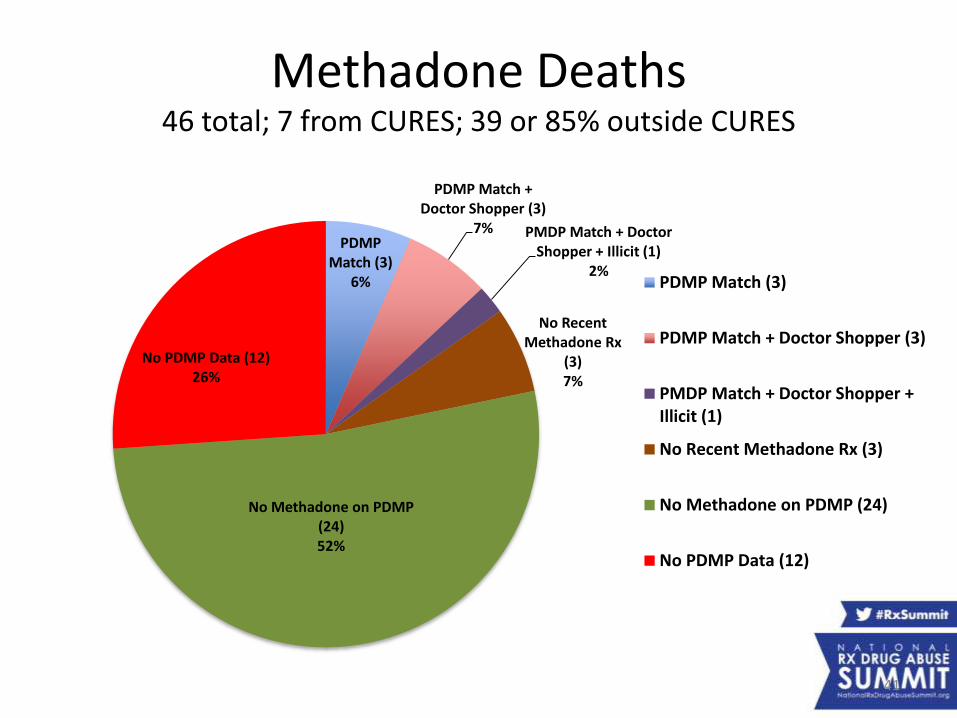
Methadone Deaths46 total; 7 from CURES; 39 or 85% outside CURES
41
PDMP Match (3)
6%
PDMP Match + Doctor Shopper (3)
7% PMDP Match + Doctor Shopper + Illicit (1)
2%
No Recent Methadone Rx
(3)7%
No Methadone on PDMP (24)52%
No PDMP Data (12)26%
PDMP Match (3)
PDMP Match + Doctor Shopper (3)
PMDP Match + Doctor Shopper +Illicit (1)
No Recent Methadone Rx (3)
No Methadone on PDMP (24)
No PDMP Data (12)
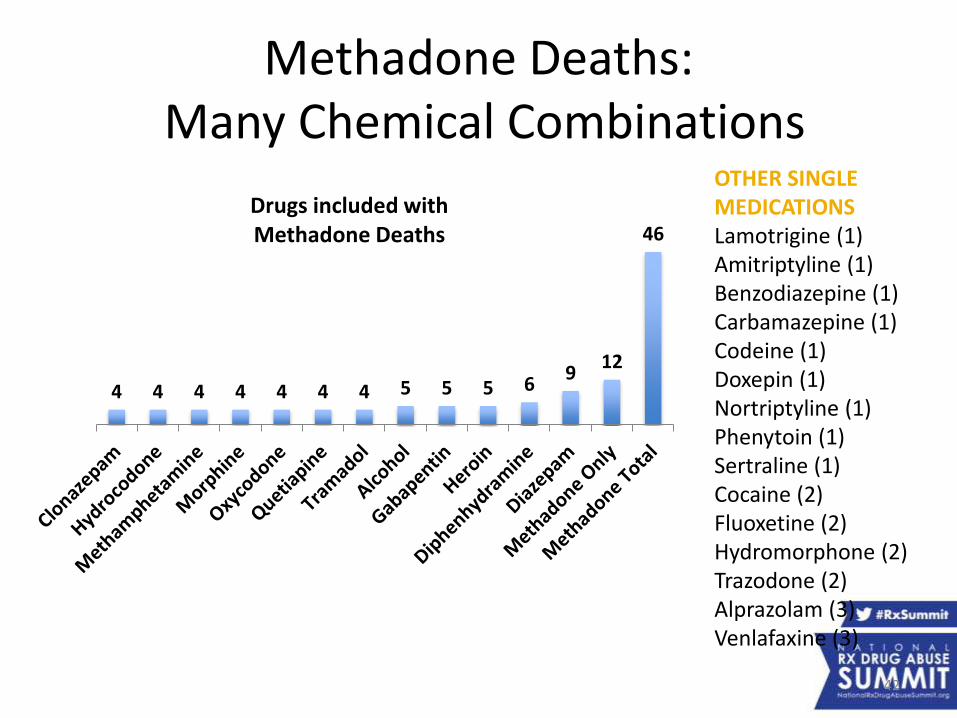
Methadone Deaths: Many Chemical Combinations
42
4 4 4 4 4 4 4 5 5 5 69
12
46
Drugs included with Methadone Deaths
OTHER SINGLE MEDICATIONSLamotrigine (1)Amitriptyline (1)Benzodiazepine (1)Carbamazepine (1)Codeine (1)Doxepin (1)Nortriptyline (1)Phenytoin (1)Sertraline (1)Cocaine (2)Fluoxetine (2)Hydromorphone (2)Trazodone (2)Alprazolam (3)Venlafaxine (3)
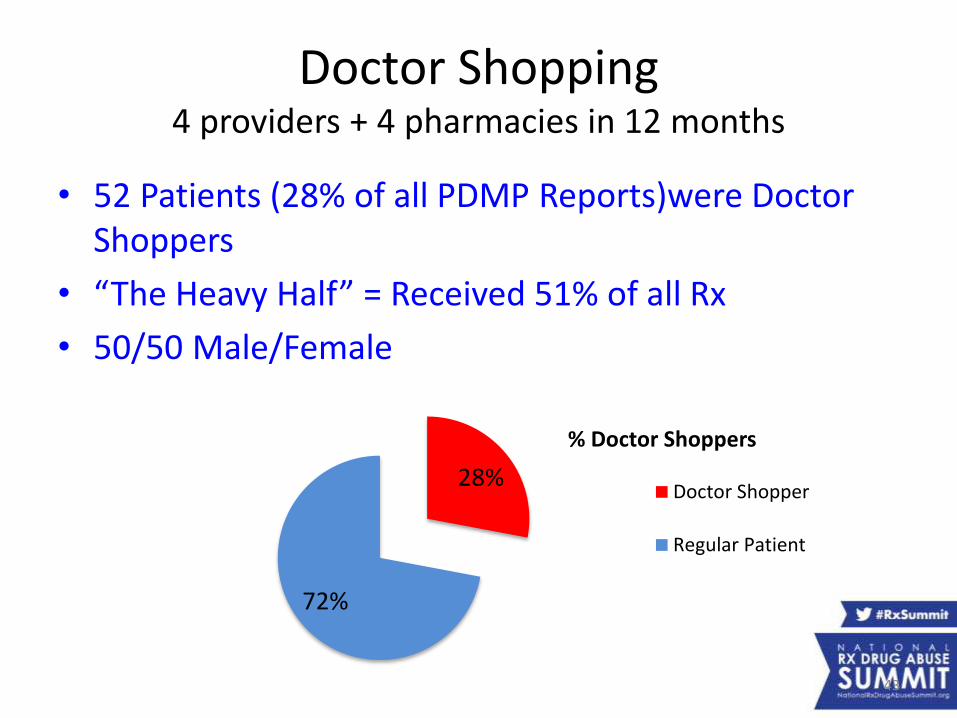
Doctor Shopping4 providers + 4 pharmacies in 12 months
• 52 Patients (28% of all PDMP Reports)were Doctor Shoppers
• “The Heavy Half” = Received 51% of all Rx
• 50/50 Male/Female
28%
72%
% Doctor Shoppers
Doctor Shopper
Regular Patient
43
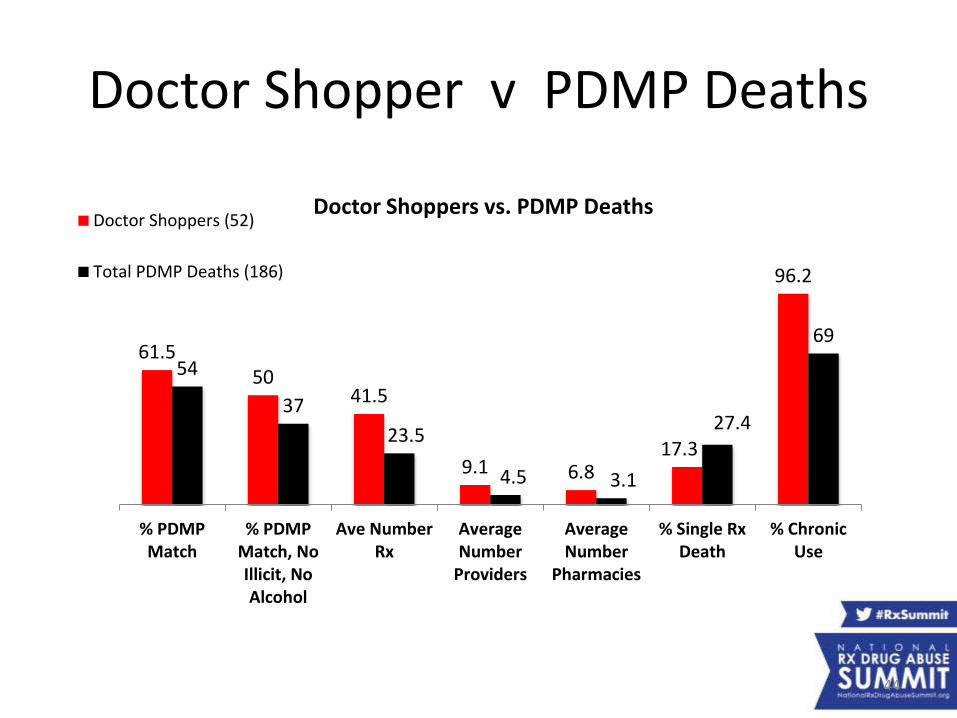
Doctor Shopper v PDMP Deaths
61.550
41.5
9.1 6.817.3
96.2
54
37
23.5
4.5 3.1
27.4
69
% PDMPMatch
% PDMPMatch, NoIllicit, NoAlcohol
Ave NumberRx
AverageNumber
Providers
AverageNumber
Pharmacies
% Single RxDeath
% ChronicUse
Doctor Shoppers vs. PDMP DeathsDoctor Shoppers (52)
Total PDMP Deaths (186)
44
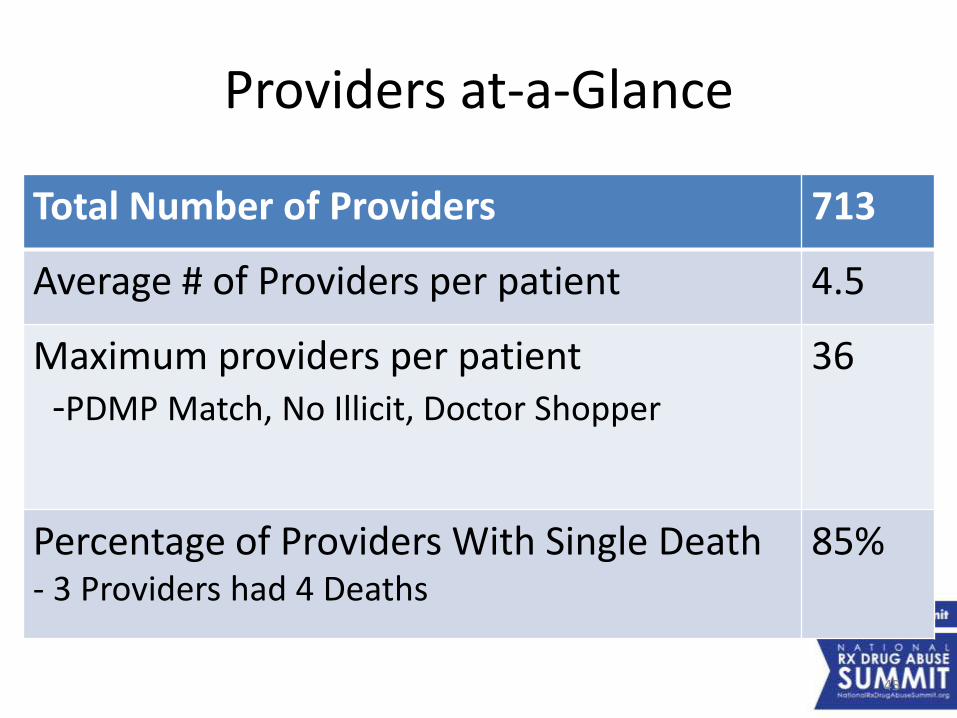
Providers at-a-Glance
Total Number of Providers 713
Average # of Providers per patient 4.5
Maximum providers per patient -PDMP Match, No Illicit, Doctor Shopper
36
Percentage of Providers With Single Death- 3 Providers had 4 Deaths
85%
45
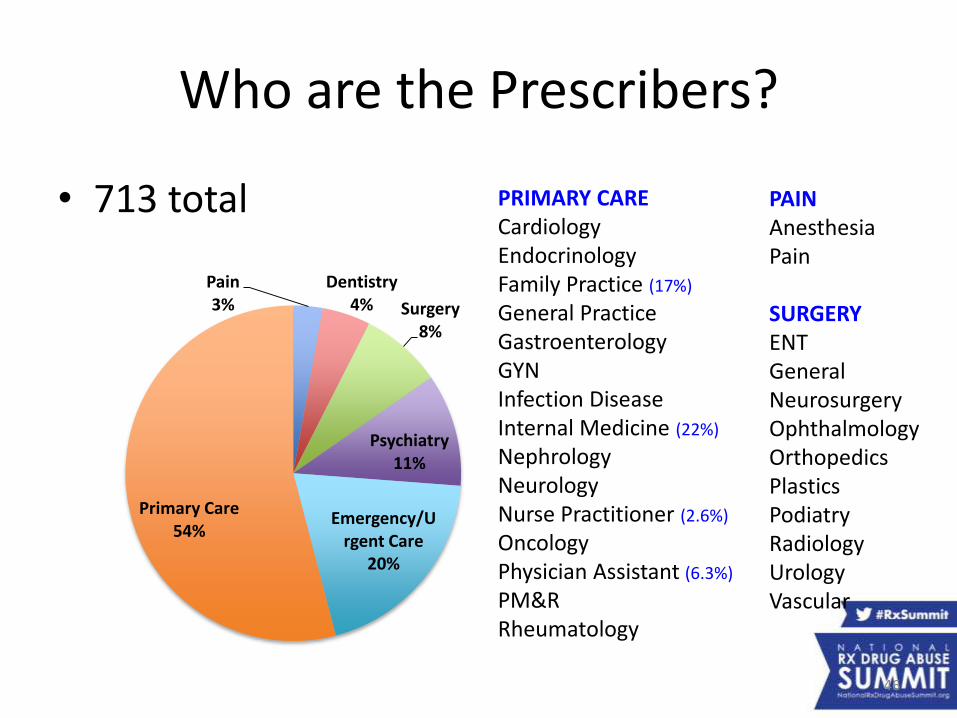
Who are the Prescribers?
• 713 total
Pain3%
Dentistry4% Surgery
8%
Psychiatry11%
Emergency/Urgent Care
20%
Primary Care54%
PRIMARY CARECardiologyEndocrinologyFamily Practice (17%)
General PracticeGastroenterologyGYNInfection DiseaseInternal Medicine (22%)
NephrologyNeurologyNurse Practitioner (2.6%)
OncologyPhysician Assistant (6.3%)
PM&RRheumatology
PAINAnesthesiaPain
SURGERYENTGeneralNeurosurgeryOphthalmologyOrthopedicsPlasticsPodiatryRadiologyUrologyVascular
46
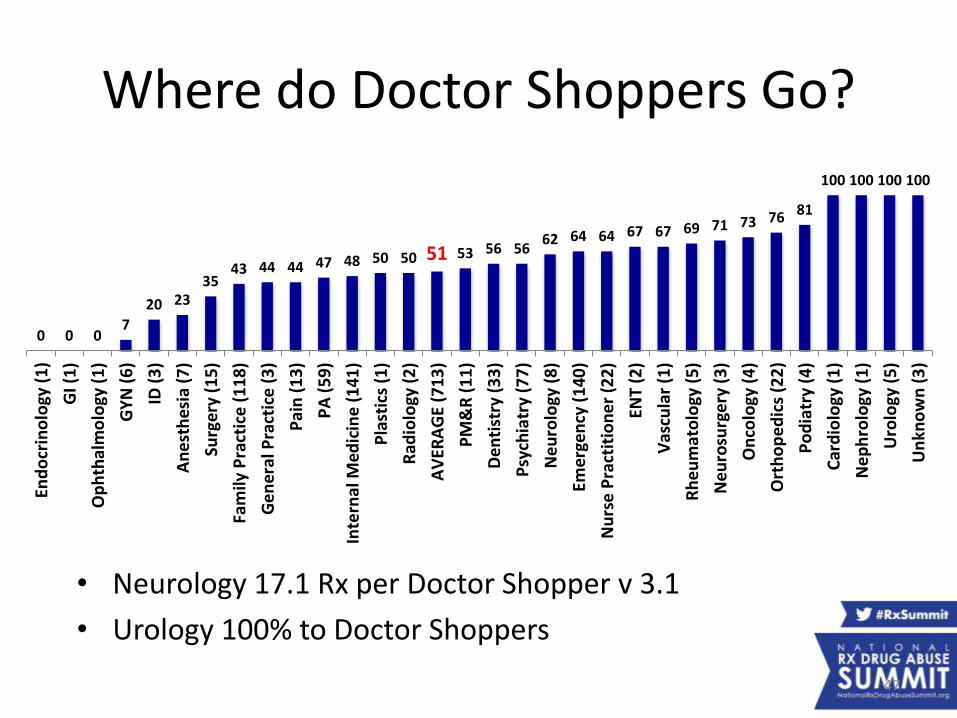
Where do Doctor Shoppers Go?
• Neurology 17.1 Rx per Doctor Shopper v 3.1
• Urology 100% to Doctor Shoppers
0 0 07
20 2335
43 44 44 47 48 50 50 51 53 56 5662 64 64 67 67 69 71 73 76 81
100 100 100 100
End
ocr
ino
logy
(1
)
GI (
1)
Op
hth
alm
olo
gy (
1)
GY
N (
6)
ID (
3)
An
est
hes
ia (
7)
Surg
ery
(15
)
Fam
ily P
ract
ice
(1
18
)
Ge
ner
al P
ract
ice
(3
)
Pai
n (
13
)
PA
(5
9)
Inte
rnal
Med
icin
e (
14
1)
Pla
stic
s (1
)
Rad
iolo
gy (
2)
AV
ERA
GE
(71
3)
PM
&R
(1
1)
Den
tist
ry (
33
)
Psy
chia
try
(77
)
Ne
uro
logy
(8
)
Eme
rge
ncy
(1
40
)
Nu
rse
Pra
ctit
ion
er
(22
)
ENT
(2)
Vas
cula
r (1
)
Rh
eu
mat
olo
gy (
5)
Ne
uro
surg
ery
(3
)
On
colo
gy (
4)
Ort
ho
pe
dic
s (2
2)
Po
dia
try
(4)
Car
dio
logy
(1
)
Ne
ph
rolo
gy (
1)
Uro
logy
(5
)
Un
kno
wn
(3
)
47
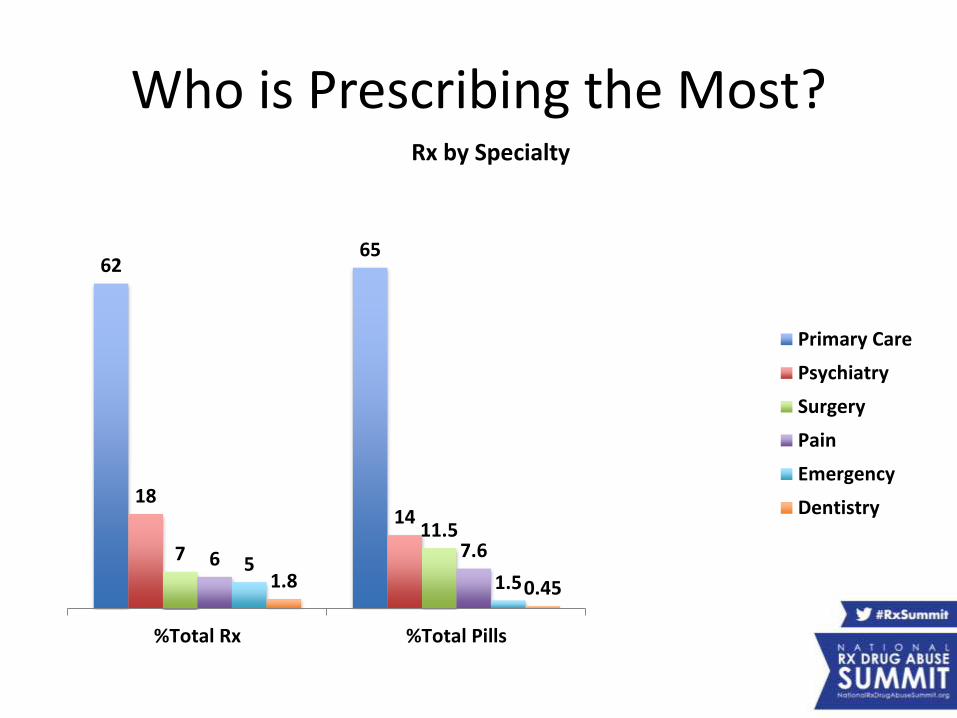
Who is Prescribing the Most?
6265
1814
711.5
6 7.65
1.51.8 0.45
%Total Rx %Total Pills
Rx by Specialty
Primary Care
Psychiatry
Surgery
Pain
Emergency
Dentistry
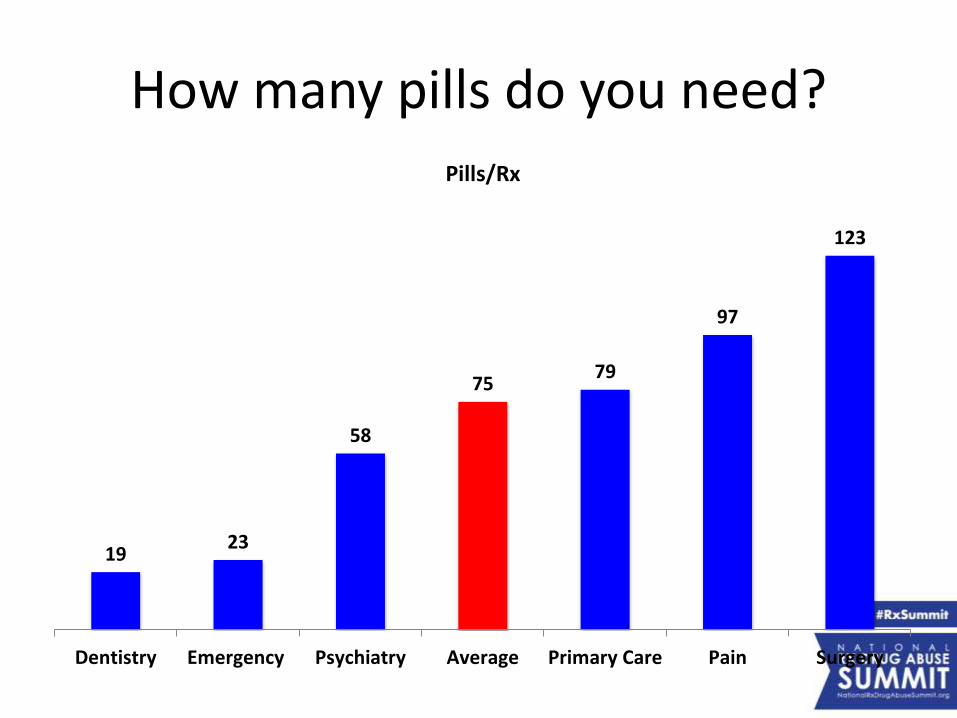
How many pills do you need?
1923
58
7579
97
123
Dentistry Emergency Psychiatry Average Primary Care Pain Surgery
Pills/Rx
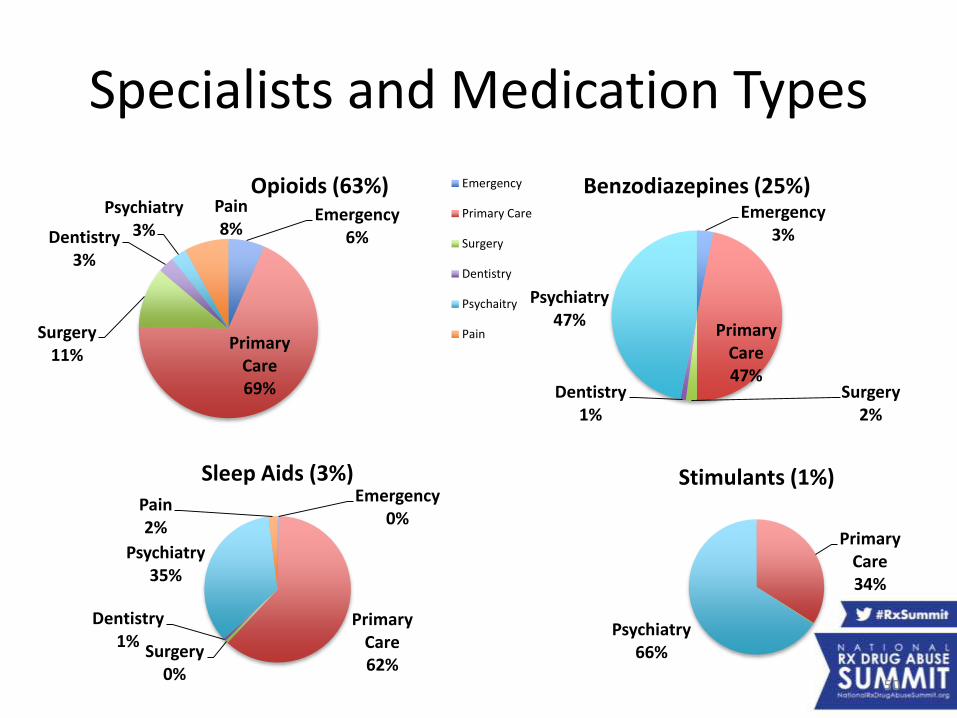
Specialists and Medication Types
Emergency6%
Primary Care69%
Surgery11%
Dentistry3%
Psychiatry3%
Pain8%
Opioids (63%) Emergency
Primary Care
Surgery
Dentistry
Psychaitry
Pain
Emergency3%
Primary Care47%
Surgery2%
Dentistry1%
Psychiatry47%
Benzodiazepines (25%)
Emergency0%
Primary Care62%
Surgery0%
Dentistry1%
Psychiatry35%
Pain2%
Sleep Aids (3%)
Primary Care34%
Psychiatry66%
Stimulants (1%)
50
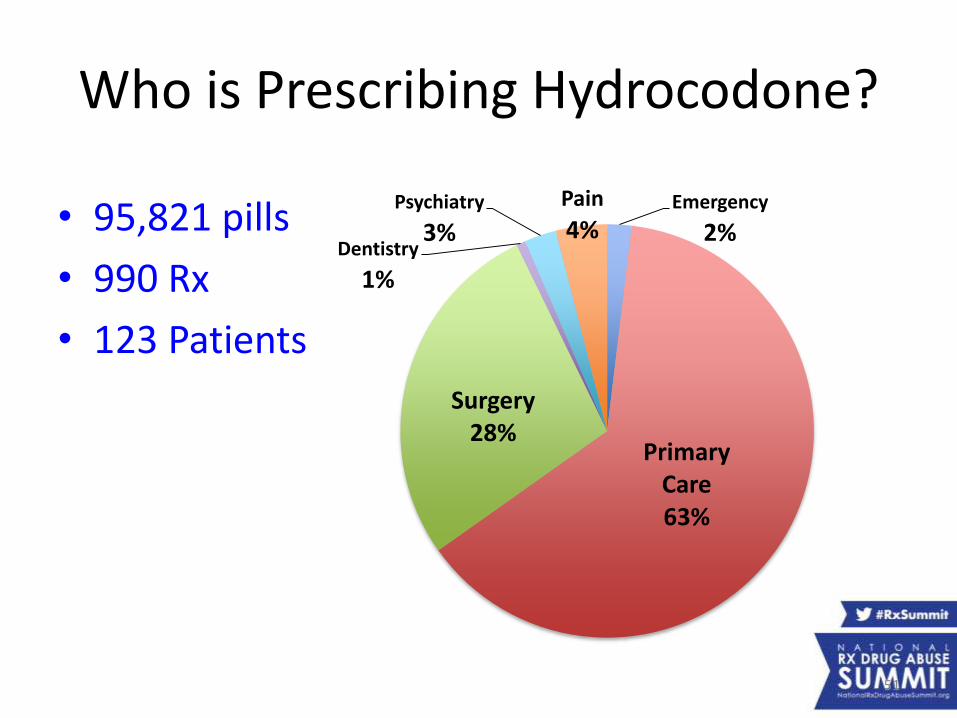
Who is Prescribing Hydrocodone?
• 95,821 pills
• 990 Rx
• 123 Patients
Emergency
2%
Primary Care63%
Surgery28%
Dentistry
1%
Psychiatry
3%
Pain
4%
51
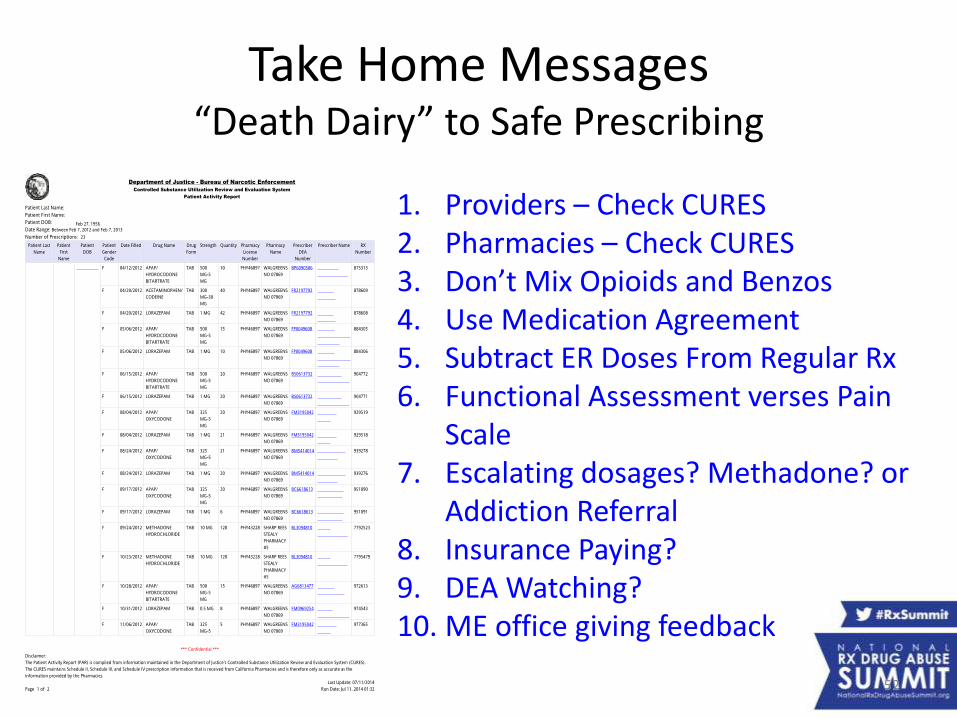
Take Home Messages“Death Dairy” to Safe Prescribing
1. Providers – Check CURES2. Pharmacies – Check CURES3. Don’t Mix Opioids and Benzos4. Use Medication Agreement5. Subtract ER Doses From Regular Rx6. Functional Assessment verses Pain
Scale7. Escalating dosages? Methadone? or
Addiction Referral8. Insurance Paying?9. DEA Watching?10. ME office giving feedback
52
PDMP Track:Combining PDMP and Other Data
to Combat Rx Drug AbusePresenters:
• Richard Stripp, PhD, Chief Scientific and Technical Officer, CordantHealth Solutions
• Roneet Lev, MD, Director of Operations, Scripps Mercy Hospital Emergency Department, and Chair, San Diego County (CA) Rx Drug Abuse Medical Task Force
• Jonathan Lucas, MD, Chief Deputy Medical Examiner, San Diego County (CA)
Moderator: Connie M. Payne, Executive Officer, Statewide Services, Administrative Office of the Courts, and Member, Operation UNITE Board of Directors