Rx15 pharma tues_330_burns
58
Pharmacy Track: The Expanding Role of Pharmacists in a Transformed Health Care System Presenter: Anne Burns, RPh, Vice President, Professional Affairs, American Pharmacists Association Moderator: Chauncey Parker, Director, New York/New Jersey High Intensity Drug Trafficking Area (HIDTA), and Member, Rx Summit National Advisory Board April 7, 2015 Westin Peachtree Plaza Hotel Atlanta, GA
-
Upload
opunite -
Category
Healthcare
-
view
169 -
download
1
Transcript of Rx15 pharma tues_330_burns

Pharmacy Track:The Expanding Role of
Pharmacists in a Transformed Health Care System
Presenter:Anne Burns, RPh, Vice President, Professional Affairs,
American Pharmacists Association
Moderator:Chauncey Parker, Director, New York/New Jersey High Intensity Drug Trafficking Area (HIDTA), and Member,
Rx Summit National Advisory Board
April 7, 2015Westin Peachtree Plaza Hotel Atlanta, GA

Disclosures
• Anne Burns, RPh, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Chauncey Parker, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.

Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition

Learning Objectives
1. Describe the evolution toward pharmacists providing direct care to patients as members of integrated health care provider teams.
2. Identify the challenges and barriers to full integration of pharmacists into health care delivery teams.
3. Outline reforms to state laws and regulations that would address obstacles to pharmacists practicing to the full scope of their professional training.
4. Describe the value-added benefits that pharmacists can deliver to decrease Rx drug addiction and misuse when integrated on health care provider teams.

Self Assessment Questions
1. Which of the following is true? a) Pharmacists’ entry level degree is a doctor of
pharmacy
b) Pharmacists’ scope of practice is standardized across the U.S.
c) All states with collaborative practice authority require pharmacists to have advance practice designations
d) A & C
e) All of the above

Self Assessment Questions
2. Barriers to maximizing effectiveness of pharmacists within the health care system include:
a) Laws and regulations governing collaborativepractice agreements
b) Provider recognition that enables compensation for pharmacists’ patient care services
c) Access to health IT systems
d) All of the above

Self Assessment Questions
3. All of the following are pharmacists’ roles in preventing prescription drug abuse EXCEPT:
a) Educating patients and the public on the risks of abuse from prescription drugs
b) Fulfilling corresponding responsibility to ensure prescriptions are legitimate
c) Diagnosing conditions for which prescription drugs with risk of addiction are prescribed
d) Participating in prescription take-back programs

• NGA Center for Best Practices – Provides information, research, policy analysis, technical
assistance and resource development for governors and their staff across a range of policy issues
– Health Division covers issues related to:• Health care service delivery and reform, including payment reform,
health workforce planning, quality improvement, and public health and behavioral health integration within the medical delivery system
• Created a series of issue briefs examining ways states can expand their health care workforce– Fourth paper in series
http://www.nga.org/cms/home/nga-center-for-best-practices/center-divisions/page-health-division/col2-content/list---health-left/list-health-highlight/content-reference-1@/the-expanding-
role-of-pharmacist.html

NGA Paper Outline
• Executive Summary
• Pharmacists’ Clinical Training and Expertise
• Pharmacists’ Current Scope of Practice
• Pharmacists’ Evolving Role in Integrated Care Teams
• Challenges and Barriers to Maximizing the Effectiveness of Pharmacists in the Health Care System

Overview
• Health care system reforms in the delivery and payment of health care services
• States currently defining policies for efficient models of care– Improved quality and health outcomes
– Reduced costs
• Pharmacists represent an opportunity for integration into these models to drive success– Third-largest health profession
– Extensive education and expertise in medication therapy management

Pharmacist Demographics
• There are 275,000 licensed pharmacists in the U.S.1
• Pharmacists practice in multiple care settings
− 65% community pharmacy
− 22% hospitals
− 13%Managed care, nursing homes, health plans, physician offices,
clinics, federal sector
1Bureau of Labor Statistics, NABP Survey of Pharmacy Law

Pharmacists’ Clinical Training and Expertise
• Entry-level degree–PharmD– Required since 2002
– Minimum 6-year requirement (4 professional years, including experiential training)
– Clinical applications of medications
• Pharmacist licensure– NAPLEX exam + meet individual state requirements
• Postgraduate training– Residencies
– Fellowships
– Certificate programs and traineeships

Pharmacists’ Current Scope of Practice
• Regulated by state laws and board of pharmacy regulations
• Four primary domains
– Ensuring appropriate medication therapy and outcomes
– Dispensing medications and devices
– Engaging in health promotion and disease prevention
– Engaging in health systems management

Pharmacists’ Patient Care Process
• Pharmacists use a patient-centered process to deliver a variety of patient care services
http://pharmacist.com/sites/default/files/PatientCareProcess.pdf
http://pharmacist.com/sites/default/files/PatientCareProcess.pdf

Collaborative Practice Authority
• State law authorizes pharmacist to enter into an agreement or protocol with a provider.
• Collaborative practice agreement: A formal agreement in which a licensed provider makes a diagnosis, supervises patient care, and refers patient to a pharmacist under a protocol or agreement that allows the pharmacist to perform specific patient care functions.
• Terminology* for the agreement varies in state law
*Collaborative drug therapy management agreement, collaborative pharmacy practice agreement, consult agreement,
physician-pharmacist agreement, standing order or protocol, simply physician delegation

Current Landscape of CPAs
• 48 states with some sort of CPA authority
• 45 states can modify therapy
• 38 states can initiate therapy
• 18 states have some extra requirement for pharmacist participation beyond licensing
• 10 states allow for multiple patients, physicians, and pharmacists on one agreement
• 6 states have site restrictions (additional 5 with different rules for different sites)
*Information provided by National Alliance of State Pharmacy Associations
16
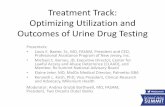
Collaborative Practice Authority

Current State Collaborative Practice Authority Laws
HI
AK
MO
WV
MS
NH
NC
FL
KY
WA
SC
OH
CAMD
DE
TN
MANY
RI
IL
CT
VT
NJ
MI
ME
MN
Collaborative agreements allowed
No collaborative agreements
CPA allowed – very restrictive
ORID
MT ND
SD
NV
UT
AZ NM
TX
WY
CO
NE
OK
KS
IA
WI
IN
PA
VA
AR
AL GA
LA
National Alliance of State Pharmacy Associations, September 2014
CPA: Collaborative Practice Agreement

CPA Authority Examples
State Requirement(s) Scope of Practice:
Iowa
• Initiated by a written protocol or executive by at least one authorized pharmacist and at least one physician
• Collaborative Drug Therapy Management
Wisconsin • None
• Therapeutic alternate drug selections in nursing homes
• Perform any patient care service delegated to the pharmacist by a physician
Washington• Agreement filed with the Pharmacy
Quality Assurance Commission (PQAC)
• Collaborative Drug Therapy Agreement

State Requirement(s): Scope of Practice:
New Mexico (1993)Pharmacist Prescriptive Authority Act (1993)
• Written collaboration with a physician • Recognition as midlevel practitioner• Prescribe and dispense medication for
primary care patients
North Carolina (2000)Clinical PharmacistPractitioner (CPP) Act (2000)
• Meet specific qualifications and receive approval by medical and pharmacy boards
• Drug therapy management agreement specific to an individual patient, physician, pharmacist, and disease
• Implement predetermined drug therapies • Order laboratory tests
Montana (2010)Clinical Pharmacist Practitioner (2010)
• Completed 5 years of clinical practice experience OR
• Completion of a pharmacy residency AND 2 years clinical practice experience AND hold one of the following:
• BPS certification• Nationally recognized certification in an area
of practice as approved by the board and board of medical examiners
• AND written collaboration with a physician
• (6) "Collaborative pharmacy practice" means the practice of pharmacy by a pharmacist who has agreed to work in conjunction with one or more prescribers, on a voluntary basis and under protocol, and who may perform certain patient care functionsunder certain specified conditions or limitations authorized by the prescriber.
• (7) "Collaborative pharmacy practice agreement" means a written and signed agreement between one or more pharmacists and one or more prescribers that provides for collaborative pharmacy practice for the purpose of drug therapy management of patients.
California (2013)Advanced Pharmacy Practice (APP) (2013)
Two of the following criteria:• Certification in a relevant area of practice• Postgraduate residency program• One year of experience providing clinical
services to patients under a CPA or protocol with another practitioner
• Prescribe nicotine replacement products supporting tobacco cessation
• Initiate and administer immunizations for people three years of age and older
• Initiate and furnish hormonal contraception• Order and interpret tests to monitor drug
safety
CPA Authority – Advanced Practice Designation

Evolving Role of Pharmacists: Integration into Chronic Care
Delivery Teams

• Integrated care models– Accountable Care Organizations (ACOs)
• Financing model; set of providers accountable for the quality and cost of defined patient population; shares risk and year-end savings if quality & cost thresholds are met (MedPAC)
– Medical Home Models
• Care model: team-based approach to comprehensive primary care coordinated by a primary care provider
• Administrative fee to coordinate care and incentives to meet quality measures for care
• Other names include advanced primary care practices, medical neighborhoods, patient-centered health care homes, health homes
ACOs and Medical Homes
*www.pcpcc.org/PCMH.AHRQ.Gov

Adapted from HealthTeamWorks: http://www.healthteamworks.org/medical-neighborhood/aco.html

Source: www.ahrq.gov
Defining the Medical HomeThe medical home is an approach to primary care that is:
Committed to Quality
and SafetyMaximizes use of health IT, decision
support and other tools
AccessibleCare is delivered with short
waiting times, 24/7 access and
extended in-person hours
CoordinatedCare is organized across the
‘medical neighborhood’
ComprehensiveWhole-person care provided
by a team
Person-Centered Supports patients and families
in managing decisions and
care plans
23

Why Pharmacists Need to be Part of the Team
• Approximately 117 million adults have at least one chronic disease– IOM Estimates that over 100 million Americans live with
chronic pain• 1999 to 2008:
• Percentage of Americans who used two or more prescription drugsincreased from 25% to 31%
• Number of patients using five or more drugs increased from 6% to 11%
• 1999 to 2009:– Average number of prescriptions per capita provided to
Americans has increased from 10.1 to 12.6 • More than 1.5 million preventable medication-related adverse
events occur each year• Inappropriate use of medications costs an estimated $290
billion annually

Collaborative Care Models• Pharmacists as part of the health care team
– Medication management expertise
– Chronic condition management
– Wellness and prevention services
• Practice settings
– Outpatient
• Physician offices and clinics
• Community pharmacies
• Community settings
– Inpatient
• Hospital
• Long-term care
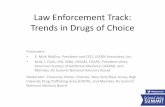
Patient
Pharmacist
Social Worker
Occupational Therapist
Physical Therapist
Lab Technician
Nurse
Physician
Health care team–Patient-centered

• Services that optimize medication use and patient safety for individual patients– Patient-centered– Coordinated with patients’ other healthcare services
• May be stand-alone or a component of disease management services
– Medication reconciliation falls under medication management services
• Medication management terminology – Medication therapy management (MTM)– Comprehensive medication management– Medication management – Medicare Part D MTM
Medication Management
Bluml BM. J Am Pharm Assoc (2003). 2005;45(5):566-72.
Bluml BM. J Am Pharm Assoc (2003). 2005;45(5):566-72

State Program
Minnesota MTM through Medicaid and State Employee Plans
Mississippi The Delta Pharmacy Patient Care Management Project
Ohio MTM Services for Medicaid-Eligible Patients
Washington Clinical Community Pharmacist – project on pharmacist prescribed medications for minor ailments
Patient Administered Naloxone
Iowa MTM services for state employees, 2010
Evolving Role of Pharmacists: State-Specific Models

Maximizing Effectiveness:Pharmacist Integration
• Challenges and barriers:
– Laws and regulations governing Collaborative Practice Agreements (CPAs)
– Provider recognition in state laws and regulations that enable compensation for pharmacists’ direct patient care services
– Access to health IT systems

Policy Approaches – Optimization of Pharmacist Services
Provider Designation
Practice Act
Optimization
Payment for Service
• Practice Act Optimization
• Provider Designation
• Payment for Service
*Information provided by National Alliance of State Pharmacy Associationshttp://www.naspa.us/news/2010/Scope%20of%20Contemporary%20Pharmacy%20Practice.pdf

Payment for Services
• Some kind of Payment28
• Some Medicaid Service15
• Medicaid MTM9
• State Employee MTM6
*Information provided by National Alliance of State Pharmacy Associations
30

Evolving Role of Pharmacists: Chronic Care Delivery Teams
• Pharmacists are well positioned to improve care and reduce the costs of treating chronic illnesses– Medication Therapy Management (MTM)
– Medication reconciliation
– Medication adherence services
– Preventive care
– Disease-management services
– Education and behavioral counseling

Pharmacist Roles- Pain ManagementDepending on practice setting and scope of practice, pharmacists can:
• Educate patients on safe and effective use of opioids; risks of addiction, overdose and abuse; and proper disposal
• Perform comprehensive medication reviews and conduct ongoing monitoring of the patient’s medications
• Initiate, modify, and discontinue therapy per scope of practice and CPA
• Develop treatment plans in coordination with other members of the health care team
• Provide drug information and make recommendations to the health care team
• Consult prescription drug monitoring programs

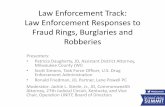
Pharmacist’s Role in Opioid Abuse, Addiction, and Diversion
Patient Care:Pain ManagementAddiction treatment
Enforcement:Prevent diversion
33
Finding an appropriate
balance
DEA enforcement on pharmacists/
pharmacies (e.g. Pharmacy chain pays
$80 million in DEA fines in 2013)
Patient legitimate
need/ access
Collaboration with other healthcare
professionals; concerns (e.g. 2013
AMA policy)

Pharmacist Role –Prevention of Prescription Drug Abuse
• Monitor for signs of abuse– Prescription Monitoring Program (PMP)
• Educate/provide information on treatment
• Involvement with pain contracts
• Take back programs– Iowa’s TakeAway Program
• Over 101,000 pounds disposed since Nov. 2009

Programs Focused on Prevention of Prescription Drug Abuse
• GenerationRx Program
• Pharmacist Recovery Network (PRN)
• Special Interest Groups: eg. APhA-APPM Pain, Palliative Care and Addiction S.I.G.

• 2009: Cardinal Health partnered with The Ohio State University College of Pharmacy
– Educational resources, toolkits, national partnerships, a recognition program, community support of non-profit organizations, and employee and customer community involvement
http://pharmacy.osu.edu/outreach/generation-rx-initiativehttp://www.cardinal.com/us/en/generationrx

• Examples of free resources:
– Youth Educational Toolkit
– Senior/Best Use of Medications Toolkit
– Collegiate Toolkit

Maximizing effectiveness: Pharmacist’s role in prescription drug abuse
• Challenges
– Access to patient medical records
• Health information technology barriers
– Variability in scope of practice across states
• Includes Collaborative Practice Agreements
– Variability in PMP access and reporting requirements across states
– Alignment of incentives

Maximizing Effectiveness: Addressing the Challenges Together
*Stakeholders include physicians, pharmacists, and the supply chain spectrum

Maximizing Effectiveness: Addressing the Challenges Together
• Early 2013– Delays in the dispensing of opioids and other
controlled substances in some pharmacy chains
– Pharmacists scope of practice questioned
• Stakeholder workgroup led by NABP– Document Goal: Provide health care practitioners
with an understanding of their shared responsibility to ensure controlled substances are prescribed and dispensed for legitimate purposes and provide guidance on red flag warning signs that warrant further scrutiny

Consensus Document Highlights
• Summary of challenges faced by physicians, pharmacists, wholesalers and manufacturers– Valuable perspectives gained by all stakeholders
• Factors indicative of substance abuse or diversion– Red flag warning signs for physicians and pharmacists
• Other aberrant medication-related behaviors**Need for balance between legitimate need and
prevention of abuse and diversion**Document does not set standards**Additional follow-up activities planned
http://www.nabp.net/system/rich/rich_files/rich_files/000/000/870/original/consensusdocumentmarch2015.pdf

Challenges and Barriers
• Manufacturers
– REMS restrictions
– Regulatory issues related to abuse-deterrent formulations
– DEA mandates for monitoring of suspicious orders
• Distributors
– DEA mandates for monitoring of suspicious orders
– Record-keeping absent

Challenges and Barriers
• Prescribers/Physicians
– Difficulty in objectively assessing pain (pain involves multiple sensory inputs and is influenced by many factors)
– Multi-faceted practice environment with high demands on time
– Lack of reimbursement for non-pharmacologic approaches and multi-disciplinary care contribute to use of opiates

Challenges and Barriers
• Pharmacists
– Corresponding Responsibility – legal responsibility to ensure the legitimacy of a controlled substance prescription
• May require outreach to prescriber
– Multi-faceted practice environment with high demands on time
– Lack of information needed to assess the prescription (could be facilitated through HIT solutions)
– PMP reporting requirements vary greatly from state to state
– Continuous tension between patient care and policing

“Red Flag” Categories: Prescribers
• Initial Visit/Presentation
• Medication Taking/Supply
• Patient Behavior/Communication
• Treatment plan related
• Illicit/illegal

“Red Flag” Examples: Physician
• Patients travel to prescriber’s practice as a group and all request controlled substance prescriptions on same day
• Patient exhibits multiple unexplained dose escalations or other non-adherence to the treatment plan
• Patient behavior or PDMP report provides evidence that the patient is obtaining controlled substance prescriptions from multiple health care practitioners without the prescribers’ knowledge of the other prescriptions.

“Red Flag” Categories: Pharmacist
• Presentation of the prescription
• Patient behavior
• Medication taking/supply
• Illicit/illegal

“Red Flag” Examples: Pharmacist
• Patients travel in groups and/or have unexplainable common factors in their relationships with each other
• Patient presents several prescriptions written for controlled and non-controlled substances, but only wants the controlled substance medication(s) dispensed
• Patient presents prescriptions for large quantities or large number of prescriptions for controlled substances
• Patient indicates that drugs will be shared with others or sold

Maximizing Effectiveness: Addressing the Challenges Together
• Pharmacist may need to communicate with physician to validate prescription legitimacy– Need for efficient and effective communication
mechanisms to share information
• PMPs show promise in monitoring for patterns of abuse
• Collect best practice examples
• Education and collaboration among all key stakeholders can help prevent and discourage prescription drug abuse

Goal- Collaborative Efforts
• Collaboration between patients, prescribers, and pharmacists is imperative for success
– Pharmacist management of medication use strives to provide patient-centered medication therapy with the goal of positive patient outcomes
J Am Pharm Assoc (2003) 2010;50:e35-e69. Dol:10.1331/JAPHA.2010.10510.

Summary and Future Direction
• Pharmacist expertise and integration into team-based models of care could lead to improved savings and health outcomes
• Select states have developed policies which allow pharmacists to practice at the top of their professional training
• All states should coordinate efforts to address the following: – Collaborative practice agreements (CPAs)– Pharmacist recognition as health care providers– Access to health IT systems– Aligned payment policies for pharmacist services
• Pharmacists are well-positioned to assist in efforts to prevent prescription drug abuse.– Specific training on medication management– Broad access to patients in varied settings

Self Assessment Questions
1. Which of the following is true? a) Pharmacists’ entry level degree is a doctor of
pharmacy
b) Pharmacists’ scope of practice is standardized across the U.S.
c) All states with collaborative practice authority require pharmacists to have advance practice designations
d) A & C
e) All of the above

Self Assessment Questions
2. Barriers to maximizing effectiveness of pharmacists within the health care system include:
a) Laws and regulations governing collaborativepractice agreements
b) Provider recognition that enables compensation for pharmacists’ patient care services
c) Access to health IT systems
d) All of the above

Self Assessment Questions
3. All of the following are pharmacists’ roles in preventing prescription drug abuse EXCEPT:
a) Educating patients and the public on the risks of abuse from prescription drugs
b) Fulfilling corresponding responsibility to ensure prescriptions are legitimate
c) Diagnosing conditions for which prescription drugs with risk of addiction are prescribed
d) Participating in prescription take-back programs

References
• National Governors Association. NGA Center for Best Practices: The Expanding Role of Pharmacists in a Transformed Health Care System. http://www.nga.org/cms/home/nga-center-for-best-practices/center-divisions/page-health-division/col2-content/list---health-left/list-health-highlight/content-reference-1@/the-expanding-role-of-pharmacist.html. Accessed March 5, 2015.
• Brian W. Ward, Jeannine S. Schiller, and Richard A. Goodman, “Multiple Chronic Conditions Among US Adults: A 2012 Update,” Preventing Chronic Disease 11 (April 17, 2014), doi:10.5888/pcd11.13
• Qiuping Gu et al. NCHS Data Brief, Prescription Drug Use Continues to Increase: U.S. Prescription Drug Data for 2007–2008, U.S. Centers for Disease Control and Prevention, September 2010, http://www.cdc.gov/nchs/data/databriefs/db42.htm (accessed September 12, 2014).0389.
• Kaiser Family Foundation, “Prescription Drug Trends” (May 2010), http://kaiserfamilyfoundation.files.wordpress.com/2013/01/3057-08.pdf (accessed September 15, 2014).
• Institute of Medicine of the National Academies, Preventing Medication Errors, National Academies Press, 2007, p. 124.
• New England Health Institute. Thinking Outside the Pillbox: A System-wide Approach to Improving Patient Medication Adherence for Chronic Disease. http://www.nehi.net/writable/publication_files/file/pa_issue_brief_final.pdf. Accessed March 5, 2015

References
• National Alliance of State Pharmacy Associations. Scope of Contemporary Pharmacy Practice.http://www.naspa.us/news/2010/Scope%20of%20Contemporary%20Pharmacy%20Practice.pdf. Accessed March 5, 2015
• The Iowa Legislature. https://www.legis.iowa.gov/docs/ACO/IAC/LINC/09-18-2013.Rule.657.8.34.pdf. Accessed March 5, 2015.
• Wisconsin State Legilsature. 2013 Wisconsin Act 294. https://docs.legis.wisconsin.gov/2013/related/acts/294. Accessed March 5, 2015
• Washington State Department of Health. http://www.doh.wa.gov/Portals/1/Documents/Pubs/690212.pdf. Collaborative Drug Therapy Agreement. Accessed March 5, 2015.
• Community Pharmacy Foundation. Clinical Community Pharmacist Protocol. http://www.communitypharmacyfoundation.org/grants/details.asp?grants_id=70773. Accessed March 5, 2015.
• Prescribe to Prevent. http://prescribetoprevent.org/pharmacists/. Accessed March 5, 2015.
• HealthTeamWorks. http://www.healthteamworks.org/medical-neighborhood/aco.html. Accessed March 5, 2015.
• Iowa Pharmacy Association. http://www.iarx.org/takeaway. Accessed March 5, 2015.

References
• Prescreiption Drug Monitoring Program Training and Technical Assistance Center. http://www.pdmpassist.org/content/prescription-drug-monitoring-frequently-asked-questions-faq. Accessed March 5, 2015.
• Cardinal Health and Ohio State University. http://www.cardinal.com/us/en/generationrx. Accessed March 5, 2015.
• Pharmacy Recovery Network. http://usaprn.org/apha-appm---pain-palliative/. . Accessed March 5, 2015.
• National Association of Boards of Pharmacy Consensus Document. Stakeholders’ Challenges and Red Flag Warning Sings Related to Prescribing and Dispensing Controlled Substances. http://www.nabp.net/system/rich/rich_files/rich_files/000/000/870/original/consensusdocumentmarch2015.pdf. Accessed March 12, 2015.
• Holiday CVS, L.L.C., d/b/a CVS/Pharmacy Nos. 219 and 5195; Decision and Order; 77 FR 108, 62,315 (Dept of Justice Oct. 12, 2012).
• www.deadiversion.usdoj.gov/fed_regs/actions/2012/fr1012.htm. Accessed March 5, 2015.
• East Main Street Pharmacy; Affirmance of Suspension Order 75 FR 207, 66149 (Dept of Justice Oct. 27, 2010). www.deadiversion.usdoj.gov/fed_regs/actions/2010/fr1027_3.htm. Accessed March 5, 2015.
• J Am Pharm Assoc (2003) 2010;50:e35-e69. Dol:10.1331/JAPHA.2010.10510.