Web only rx15-le_wed_430_1_mollica_2clark
101
Law Enforcement Track: Trends in Drugs of Choice Presenters: • E. Mick Mollica, President and CEO, LEARN Associates, Inc. • Kelly J. Clark, MD, MBA, FASAM, DFAPA, President-elect, American Society of Addiction Medicine (ASAM), and Member, Rx Summit National Advisory Board Moderator: Chauncey Parker, Director, New York/New Jersey High Intensity Drug Trafficking Area (HIDTA), and Member, Rx Summit National Advisory Board
-
Upload
opunite -
Category
Healthcare
-
view
295 -
download
0
Transcript of Web only rx15-le_wed_430_1_mollica_2clark
Law Enforcement Track:Trends in Drugs of Choice
Presenters:
• E. Mick Mollica, President and CEO, LEARN Associates, Inc.
• Kelly J. Clark, MD, MBA, FASAM, DFAPA, President-elect, American Society of Addiction Medicine (ASAM), and Member, Rx Summit National Advisory Board
Moderator: Chauncey Parker, Director, New York/New Jersey High Intensity Drug Trafficking Area (HIDTA), and Member, Rx Summit National Advisory Board
Disclosures
• E. Mick Mollica has disclosed no relevant, real, or apparent personal or professional financial relationships with proprietary entities that produce healthcare goods and services.
• Chauncey Parker has disclosed no relevant, real, or apparent personal or professional financial relationships with proprietary entities that produce healthcare goods and services.
• Kelly Clark – Employment: Publicis Touchpoint Solutions; Consultant: Grunenthal US
Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition
Learning Objectives
1. Identify trends in which opiates are being abused and how.
2. Prepare law enforcement officers to recognize the signs and respond to the typical behaviors and crimes related to heroin abuse.
3. Explain treatment methods for heroin abuse.
“Why Heroin”
E. Mick Mollica
“Has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.”
“Why Heroin”
• This session will provide a brief overview of the transition from Opiate/pain pills to heroin, Attendees will explore which opiates are abused most frequently and how the substances are abused. In addition, the most current trends of use, Signs and symptoms, stages of addiction associated with behaviors will be examined.
Opiates
• Pain
• Cough
• Diarrhea
• Opiate Treatment
Opiate concerns
Approximately 80% of the world's pain pills are consumed in the United States, according to 2011 congressional testimony from the American Society of Interventional Pain Physicians
One person dies every 19 minutes from a prescription drug overdose in the United States.
Car accidents are no longer the leading cause of accidental deaths in the United States. According to a recent report published by the CDC's National Center for Health Statistics, this dubious distinction now belongs to drug overdose. What's at the root of this trend? A river of prescription painkillers and Heroin.

11:00 PMWhat should it be?
Under the influence
• Constricted pupils and non reactive to any light
• Droopy eye lids (ptosis)
• Raspy voice
• Scratch or rub their face and nose
• Always cold
• Sleepy/lethargic( On the Nod)
• Dehydrated- lots of water to open veins to use.
Opioids/Opiates
• Pain killer
• Use will cause dependence
• Stop using will cause severe W/D
• “Dope Sickness”
• Any other opiate will cease W/D
Newborns have to detox off of opiates
• One baby is born every hour of the day addicted to opiates.
• They have to detox off of opiate addiction with methadone or other opiates.
• They all have the dope sickness
BODY DROPS
• 80% OF HEROIN ADDICTS INJECT WITH SOMEONE ELSE.
• 80% OF OVERDOSE VICTIMS FOUND/TREATED BY EMT’S ARE FOUND ALONE.
• Immunity for calling
• Narcan to everyone

Afghan

Afghan

Poppy Seed Tea
• Lucky8502Hello I'm new to this group and I am writing because I have been abusing poppyseed tea for about 2 months. I use about 2 pounds of seeds everyday and I am scared about the withdrawal. Can anybody give me and indepth view of opium withdrawal and what I can expect
Poppy Seeds
• So I was at a local store the other day that I normally don't shop at and what do I come across but bulk poppy seeds! And only 8 bucks for a whole lbs! With roughly 100mgs of morphine per lbs that's not a bad deal at all! Just thought that was pretty cool! No more WD days for me! $8-16 a day says im good to go!Just thought it was cool to fine them so close to home for so cheap! So awesome!
World Market-Folsom, Ca.
Commonly Abused Prescription Opiate Drugs
Vicodin Oxycontin Oxycodone/Roxicodone Dilaudid Codeine Lortab Methadone Opana
“Drizzlin”-Smoking Oxycontin

New Oxy
New OP/Oxycontin
Microwave/Oven OP
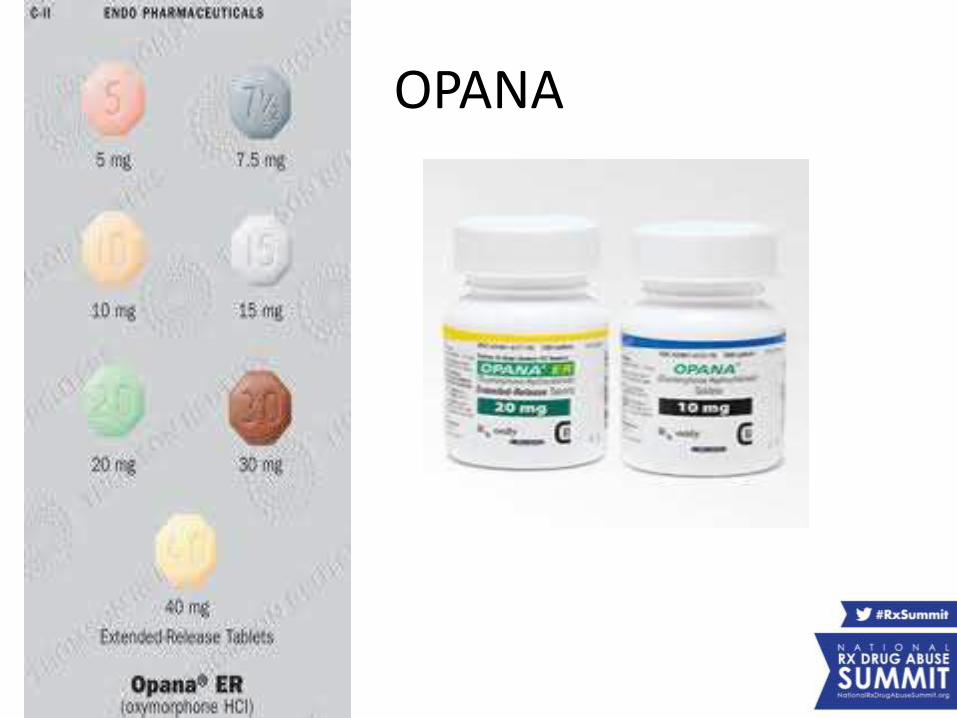
OPANA
OPANA
The June 2 incident was the 11th pharmacy robbery in Fort Wayne this year, an unusually high number for this city of 250,000 people, police spokeswoman Raquel Foster said. In almost every case, the robbers asked specifically for Opana, the trade name for oxymorphone, a powerful prescription painkiller.
"A few years ago, it was OxyContin. Now it's Opana," Foster said. "These people are desperate to get it."
Opana- Street Terms
• Panda
• Panda Bears
• “Going to the Zoo”
Fast-Spreading HIV Outbreak in Indiana Linked to Injection of Painkiller
• February 26th, 2015
• Health officials in Indiana say a fast-spreading outbreak of HIV in Indiana is largely due to injection drug abuse of the prescription painkiller Opana. The powerful drug is more potent, per milligram, than OxyContin.
Codeine and PM
• Purple Drank is an illegal recreational drinkpopular amongst the hip-hop community of the Southern United States. Its main ingredient is prescription-strength cough syrup containing codeine and promethazine.[1]

Codeine & PM /Sprite/VodkaJolly Rancher for flavor, chop-up a vicodin/hydrocodone and sprinkle
on top
Slang Names
• Sippin, LEAN, Dank ,Drankin
• Other terms for Purple Drank include Sizzurp, Drank, Purple Tonic, Southern Lean, Texas Tea, Memphis Mud, Lean, Syrup, P-Flav, Slip, Da Drizzy, Mrs. Drankleworth's, Oil, Tsikuni, Barre, Sir, Cincy Wincy, Nurple, DrankenStein, and Purple Tang.
Pharm Heroin
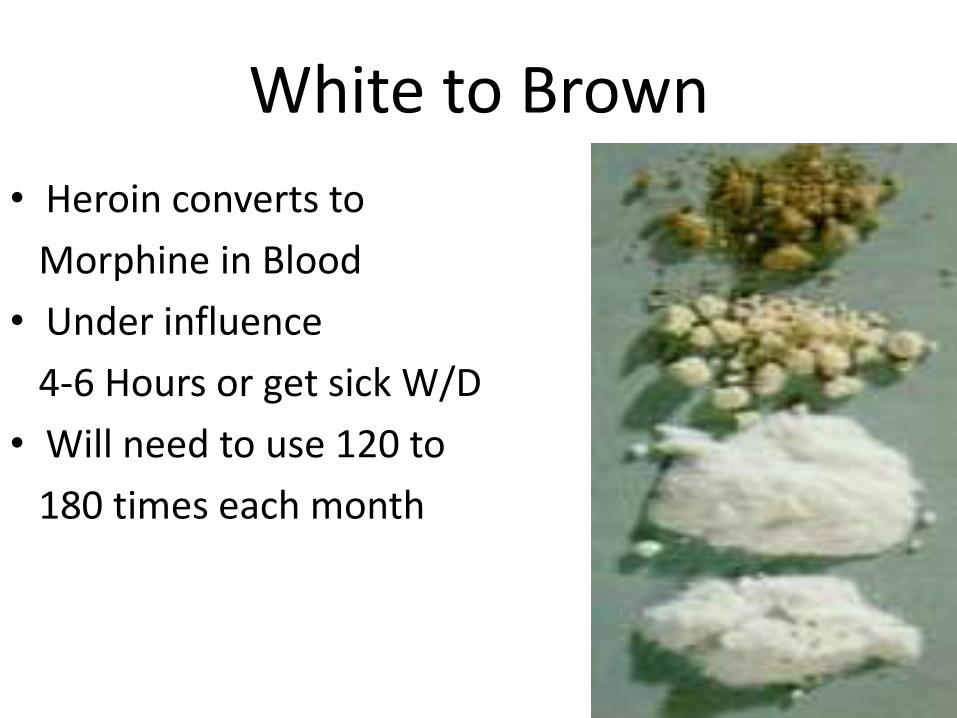
White to Brown
• Heroin converts to
Morphine in Blood
• Under influence
4-6 Hours or get sick W/D
• Will need to use 120 to
180 times each month

September- December 2014Prices
Mexican Black Tar Heroin
• Wholesale-Kilo $20,000-$25,000
• Mexican Ounce (25 Grams) $700-$900
• 1/2 Ounce $425-$650
• 1/4 Ounce $200-$250
• Retail-Gram $50-$100
• 1/2 Gram $40
• 1/10th Gram $10
• Balloons $8-$10
Mexican Brown Heroin
• Wholesale-Kilo $25,000
• Retail-Gram $60-$100
• Southeast Asian (White) Heroin
• Wholesale-Pound $40,000-$42,000
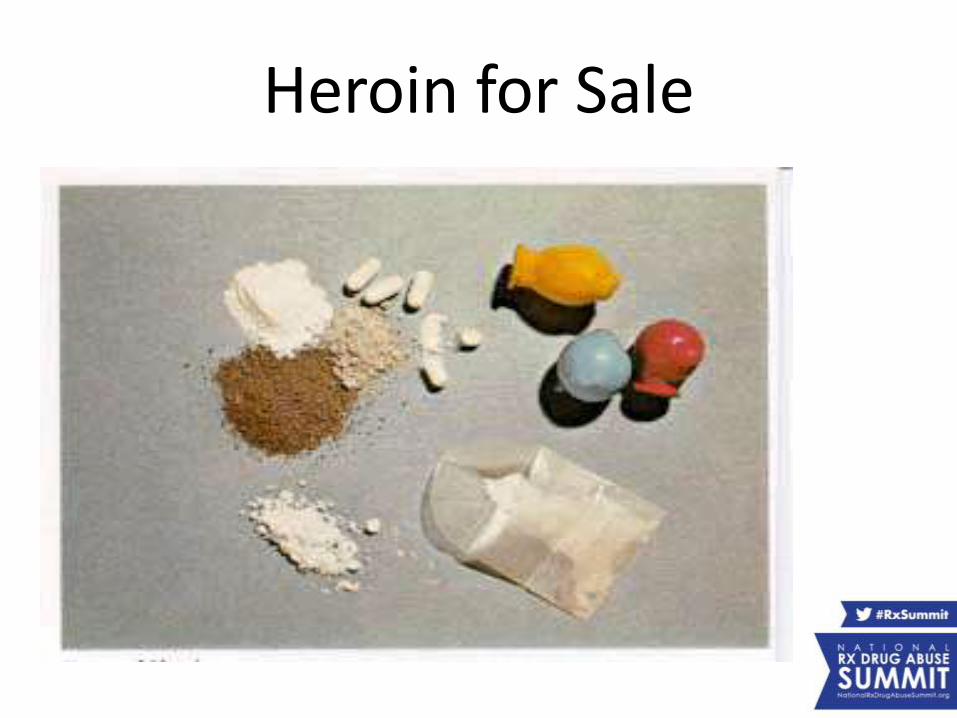
Heroin for Sale
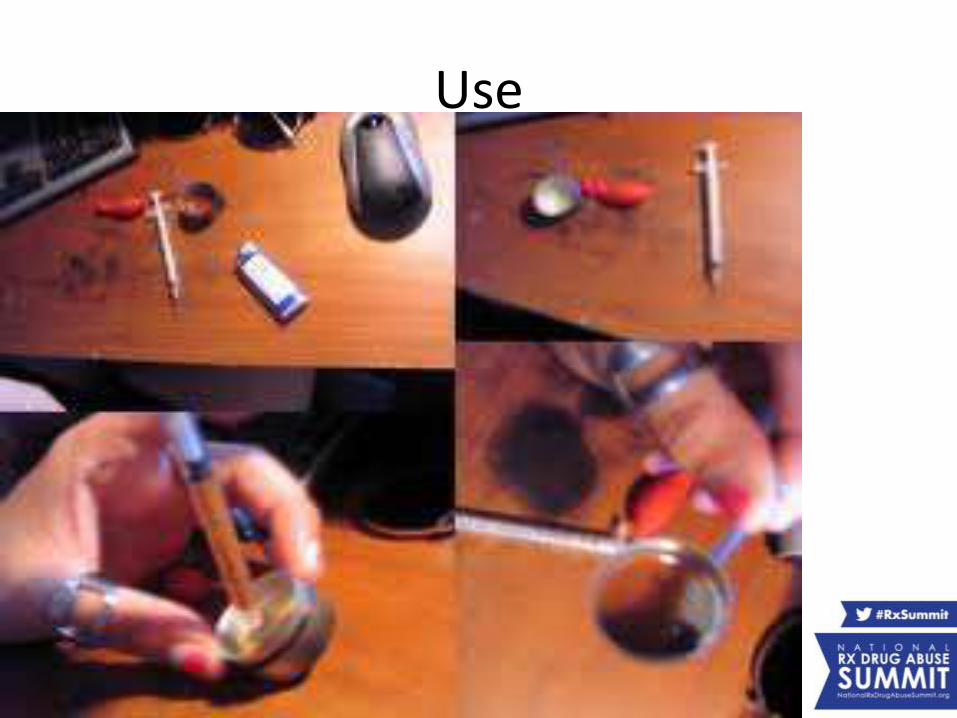
Use


injections
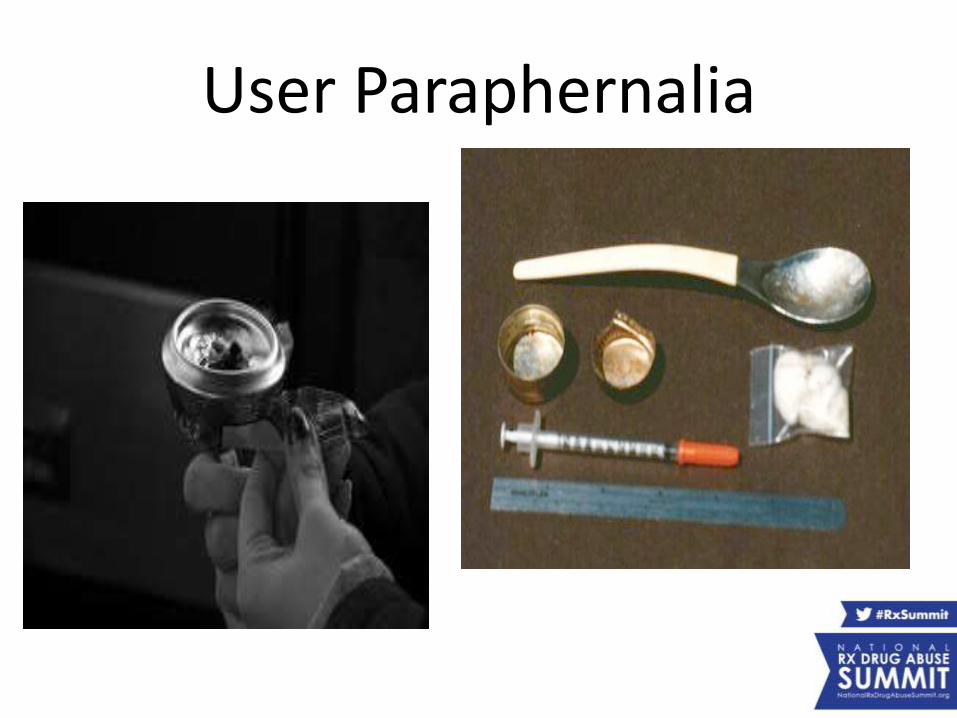
User Paraphernalia
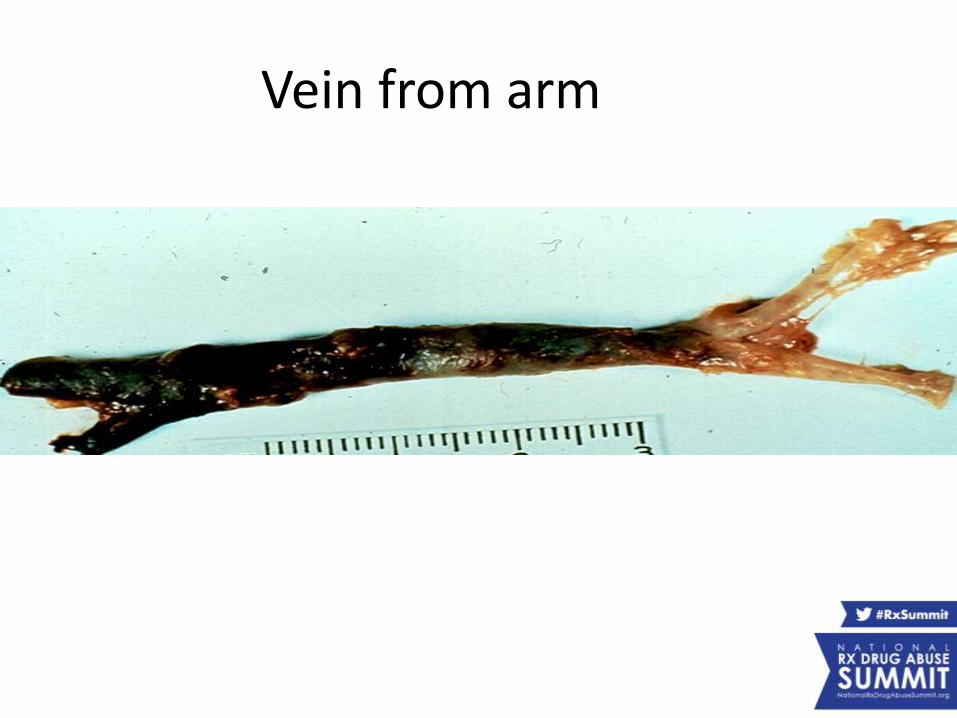
Vein from arm

Vein from inside
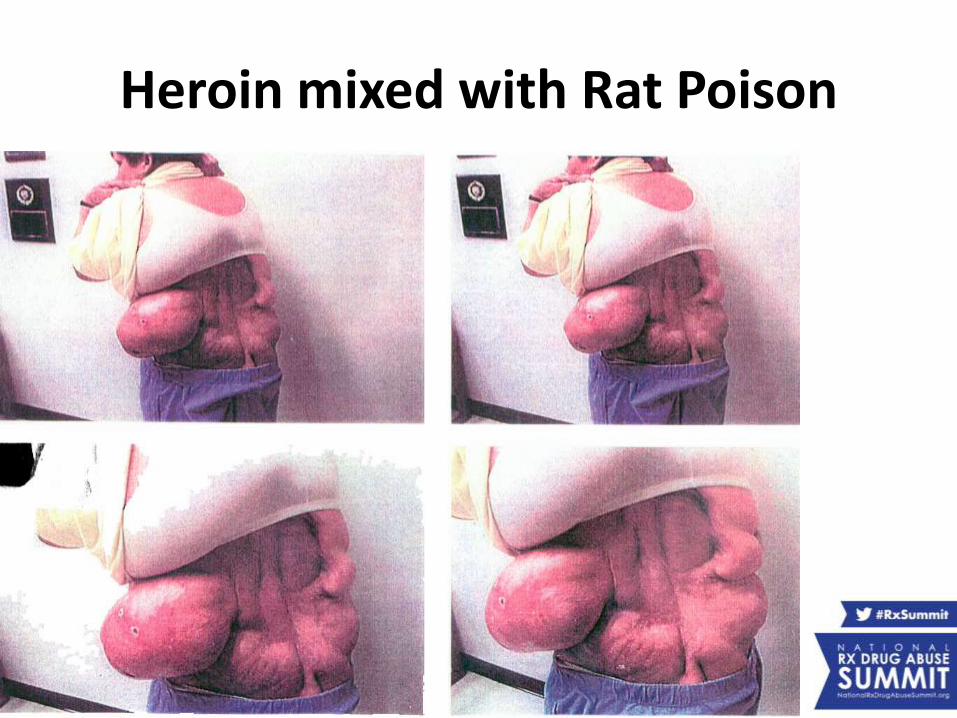
Heroin mixed with Rat Poison
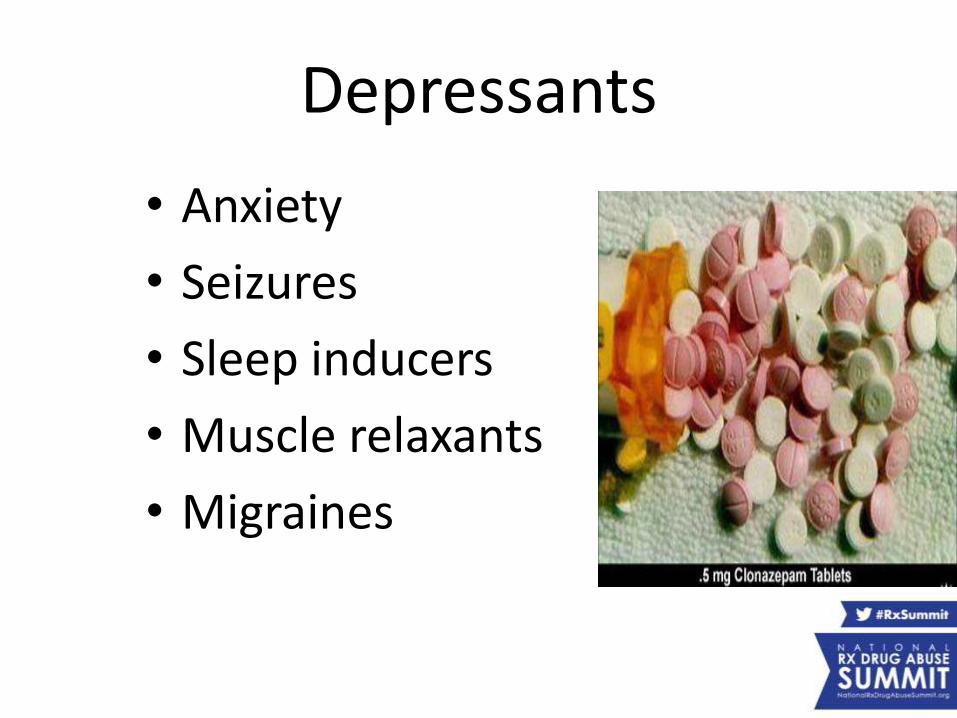
Depressants
• Anxiety
• Seizures
• Sleep inducers
• Muscle relaxants
• Migraines
Soma with Hydrocodone
The most popular "load" or "combo" involving Soma is the partnering of carisoprodol and hydrocodone. Called "Somadin" or "Somadone," carisoprodol enhances the effect of hydrocodone and creates a more intense and longer acting euphoria. A typical "Somadone" load involves 600 mg of Soma and 10-15 mg of hydrocodone. Tolerant users may take up to 1050 mg of carisoprodoland 20 mg of hydrocodone at one sitting. More provocative users will combine the drug with oxycodone, perhaps by smoking the combined contents of Percocet and Soma tablets.

Pakistan
OnaxOnax bars, similar to xanax, manufactured in Pakistan
by Ocean Manufacturing. May or may not contain Alprazolam (unknown). Not governed, regulated or approved by FDA in the United States. Parcel Interdiction Unit working USPS, FEDEX, UPS, etc are seizing these through Charleston County Sheriffs Office in Charleston SC (College town). Also seeing a lot on search warrants on younger, college aged, targets. Manufacturing practices are unknown so not all are registering any type controlled substance in lab tests.
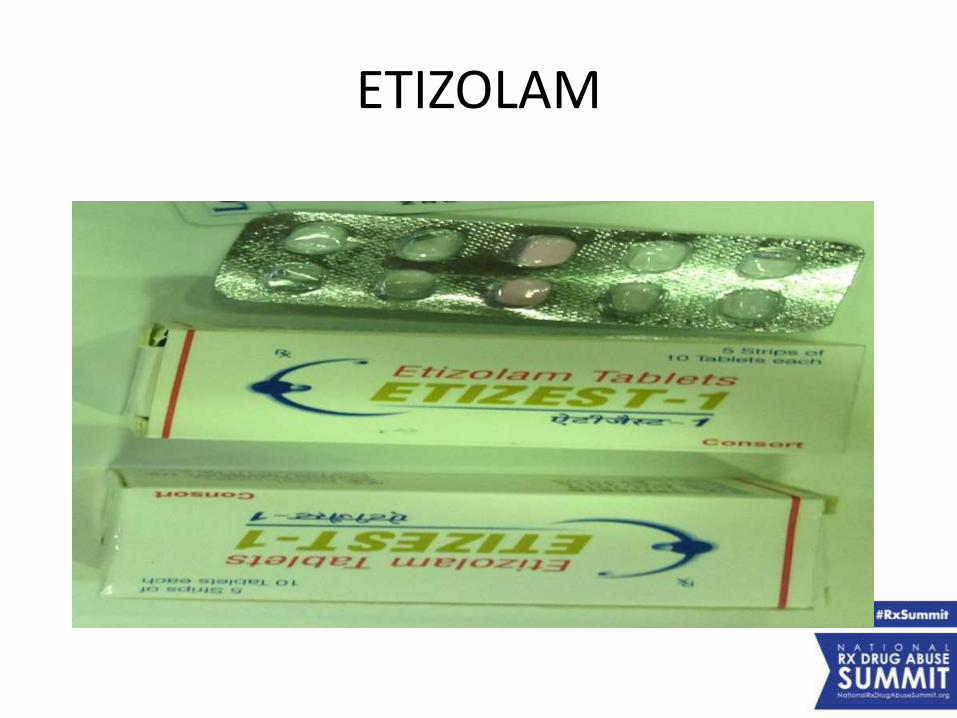
ETIZOLAM
ETIZOLAM
• As of August 2014 Etizolam is not authorized for medical use in the U.S. However, it currently remains unscheduled and is legal for research purposes. As its closest derivative is a Schedule IV drug under Federal Scheduling Guidelines, it does not fall under the Federal Analog Act, which only applies to Schedule I and II drugs.
• The state of Arkansas has proposed listing Etizolam as a Schedule I drug under their drug scheduling guidelines] along with the state of Mississippi .
Trends in Drugs of Choice: Heroin Addiction Treatment
Kelly J. Clark, MD, MBA, FASAM, DFAPAPresident-Elect, American Society of Addiction Medicine
Kelly J. Clark, MDDisclosure
• Medical director, Orexo (2014)
• Consultant, Grunenthal, USA (2014)
Warnings
• I will oversimplify
• Doctors think about public health instead of public safety, but these are tightly linked
– Infectious diseases
– Second hand smoke
– Drunk/drugged driving; violence
and abuse/neglect of vulnerable people
Public Safety + Public Health
Rx Drugs of Abuse (1)
• Opioids
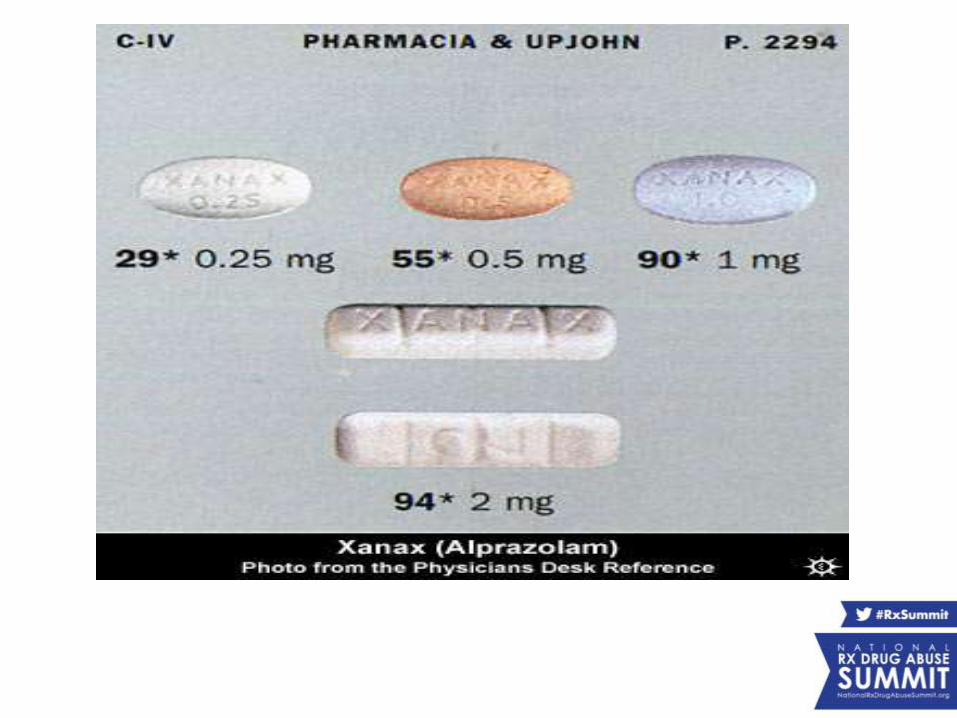
• Benzos (Xanax, Klonopin)
• Barbiturates (Soma)
• Amphetamines / stimulants (Ritalin, Concerta)
• Muscle relaxants (Soma)
• Hypnotics (“z drugs”- Ambien)
Rx Drugs of Abuse (2)
• Anabolic steroids
• Anti-retrovirals (HIV drugs)
• GHB (date rape drug)
• Quetiapine (Seroquel)
• Anti-epileptics (gabapentin)
Before we focus on opioids, a word about Kentucky’s #1 Killer
• One specific drug is found in nearly 45% of overdose autopsies in Kentucky
• ------ Alprazolam (Xanax) , a Benzo
Why is the cocktail so bad?
• Opioids act on one part of the brain cells
• Benzos on a different part
• Soma (barbiturate-like) on a third part
• And alcohol has it’s own effect
– When taken together, the sedative effects on the brain multiple beyond what happens with any one taken alone
The brain forgets to tell the body to breathe!!!
Opioids(substances that activate opioid receptors)
• Medical effects/Side Effects • sedation, decreased pain, decreased breathing drive, decreased gut motility;• euphoria, sweating, dry mouth, small pupils
• Withdrawal (this isn’t like cocaine or meth: think the Flu)• chills, goosebumps, muscle and GI cramps,• big pupils, agitation, insomnia,• “fluids coming out” – vomiting, diarrhea, sweating, watery eyes/nose, drooling
• Intoxication • Decreased drive to breathe death• Especially likely when combined with benzos, soma, alcohol, sleeping pills• Addiction not necessary for drug-induced death
• Medical Uses• Pain, cough, diarrhea, air hunger, opioid addiction

Opioid Withdrawal: SCARY!
If someone is addicted:
• What’s the first thing they think in the morning?
- “how am I gonna get pills and not get sick?”
• What are they going to do if they run out of pills?
– get opioids any possible way to avoid getting sick (ER, steal from the neighbor’s left over supply, knock out a tooth, doctor shop, or get heroin)
Some Language
• Abuse (SAMHSA): maladapted pattern of substance use leading to significant impairment or distress
• Misuse (SAMHSA) incorrect use of the medication by patients (wrong time, wrong dose, wrong purpose)
• Diversion: medication leaving the legal distribution channels (Manufacture, transport, pharmacy, patient)
Addiction
• Chronic, relapsing, primary disorder of brain reward, motivation, memory.
• Inability to consistently abstain despite negative consequences of use
• Craving
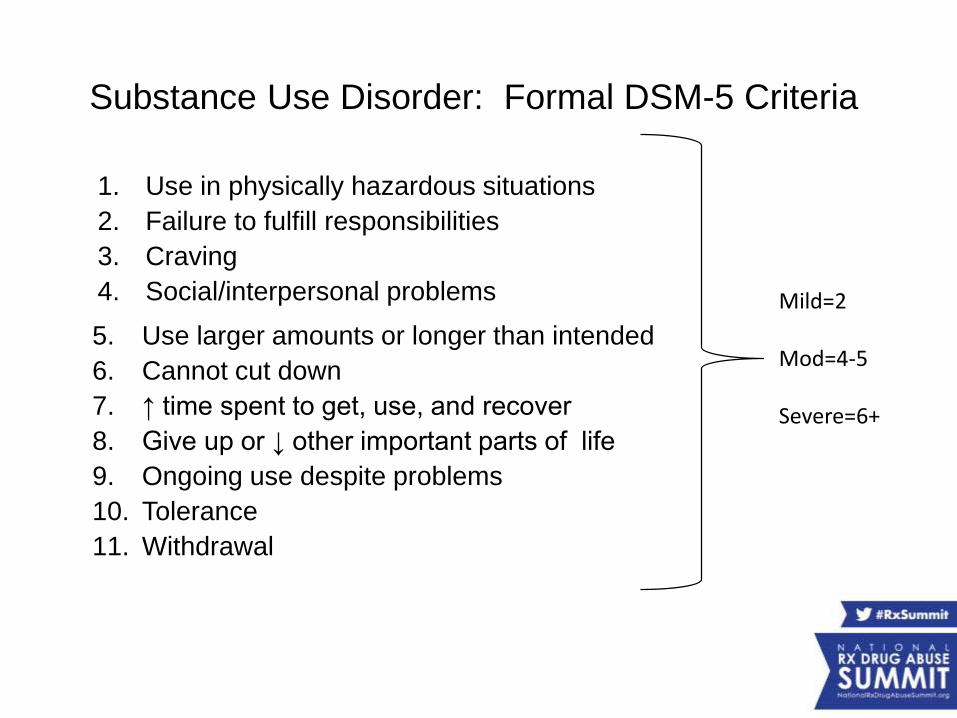
5. Use larger amounts or longer than intended
6. Cannot cut down
7. ↑ time spent to get, use, and recover
8. Give up or ↓ other important parts of life
9. Ongoing use despite problems
10. Tolerance
11. Withdrawal
Substance Use Disorder: Formal DSM-5 Criteria
1. Use in physically hazardous situations
2. Failure to fulfill responsibilities
3. Craving
4. Social/interpersonal problems Mild=2-3
Mod=4-5
Severe=6+
Making the Diagnosis
• People loose control of their drug use
• People loose control of their lives because of their drug use
Clearly Addicted : Now What?
• Boot Strap it!
• Make new lifestyle choices!
• Just Say “NO”!
• Ummm….does this work for other chronic diseases?
First, let’s mention the Magic “NOTs”
• What’s not opioid addiction treatment:
– 12 step approaches (AA, NA)
– Detoxification
– Naloxone
• What people want:
– To go away for a rest and come back “cured”
– Sadly, there is NO EFFECTIVENESS DATA
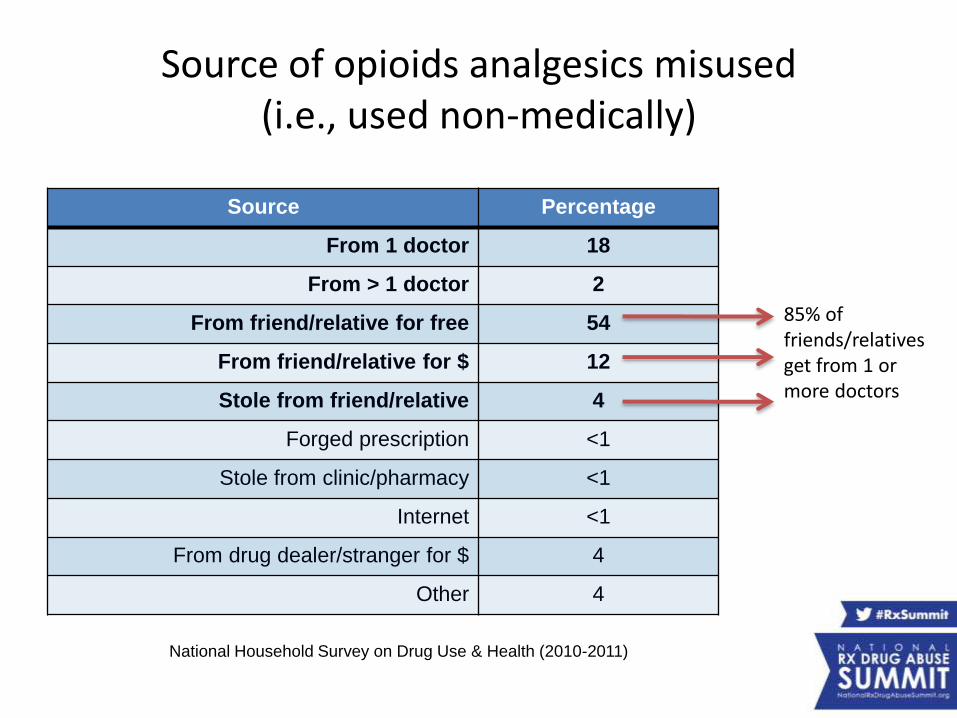
Source of opioids analgesics misused (i.e., used non-medically)
Source Percentage
From 1 doctor 18
From > 1 doctor 2
From friend/relative for free 54
From friend/relative for $ 12
Stole from friend/relative 4
Forged prescription <1
Stole from clinic/pharmacy <1
Internet <1
From drug dealer/stranger for $ 4
Other 4
National Household Survey on Drug Use & Health (2010-2011)
85% of friends/relatives get from 1 or more doctors
Clearly Addicted : Now What?
• What kinds of treatment are given?
• Where does treatment happen?
• Who gives this treatment?
• How does someone decide on where, who, what, and for how long?
• Who pays for treatment?
Treatment history
• Many illnesses were once considered “moral failings”. These included not just psychiatric disorders, but those caused by infections, genetic and hormone disorders.
• Spiritually-based programs, starting with AA, were the basis for the approach to addiction in the US because there was no medical treatment
• Many, many people were told in AA and by therapists that they were not in recovery because they were taking Prozac and therefore drugging away their feelings and not working on their issues
• Chestnut Lodge Lawsuit established the convention that patients are entitled to appropriate treatment
Or more visually,the one-size-fits-all approach
The Treatment Framework:Bio-Psycho-Social-Spiritual Care
• Bio: Safe detoxification, medication management, attention to medical issues
• Psycho: individual counseling, attention to psychiatric issues
• Social: family and group counsellng and educational work
• Spiritual: AA, NA, 12 step approaches and others
Why can’t people “just stop”?
• Addiction is a Chronic Brain Disease
• Changes in brain after last use of opioids persist at least 3 years – untrue of cocaine
• Data is overwhelming: the evidence base supports primary treatment with medication treatment
Where does treatment happen?(hint: sleep over or not sleep over)
• Inpatient = sleep over– Inpatient Detox (benzos, barbs, booze)
– Detox is not “treatment of addiction”
– Residential short term
– Residential long term ( half way houses, group homes)
• Outpatient = leaves facility to sleep.– Outpatient medication and counselling offices
– Intensive Outpatient (3 hors at 3 times a week)
– Partial Hospital (4 hours at 5 times a week)
Who provides treatment?
• Primarily by counselors with the equivalent of high school, associates or bachelor’s degrees – historically high rates of those in recovery
– Most addiction treatment providers are not able to be individually licensed
• Some individually licensed therapists
• Physicians
Deciding what, where, when,who, and how much
• ASAM Criteria determine appropriate level of care (where), and how much care
• Patient preference (without guidance)• Provider Preference (without independent
license)• Payer Preference (without science)
– Payers generally required to pay medically necessary only; not coerced care
– Limits not evidence-based
“Psychosocial”
• Individual therapy
• Group /family therapy
• 12 step groups
• Non-12 step programs ( Rational Recovery, etc)
Therapeutic Approaches
• Motivational Enhancement
• Mindfulness
• Cognitive Behavioral– Reframing
– Relapse prevention planning
– Contingency management
While these are evidence-based, much care provided is called “Supportive Counseling”
“Social”
• Primarily environmental interventions:
– including family education/treatment, change “playmates and playpens”
– Supportive residence:
• Rehab, RTC, halfway house, group home, etc
– Structured time:
• Daily group counseling
• “90 in 90” = 90 meetings in 90 days
Spiritual: 12 Steps (AA/NA)• Spawned other 12 step programs like Narcotic Anonymous
• Some people have great difficulty with spiritual bent
• Fellowship at Meetings, 1:1 work with Sponsor
• Homework / Self-help with the readings
• Evidence is that this is an effective program for alcoholics
• No evidence of effectiveness for opioid addiction
• AA is not a “treatment” program – it is a mutual support program
• Patients on Medication are largely UNWELCOME at NA meetings
Medication Assisted Treatment ( MAT)Methadone, Buprenorphine, Naltrexone
• TRI analyzed data in 2013
• HUNDREDS of positive effectiveness studies
• All three medications have modest or better cost effectiveness in maintenance
• NO evidence for effectiveness of detox
• All three medications are underutilized
Goals of Medication Treatment
• Decreased annual death rates• Decreased drug-related disease (Hep C, HIV)• Improved work, educational and family functioning• Decreased involvement with criminal justice system
(consider that the goal of using insulin is not go get off insulin; it is to best manage diabetes with the least medical and functional impairments)

Who encourages use of MAT?
BIO (psychosocial spiritual):
• Methadone – Specialized licensed facilities (OTPs) dispense
– Illegal to prescribe on a pad; no 10 mg pills
– Efficacy data better than nearly almost all medication treatments for any medical condition: 50 years of data
• Buprenorphine– Brand names Subutex ( mono product)
– Brand names Suboxone, Zubsolv, Bunavail
– Can be prescribed in physician offices or dispensed by OTPs
– Physicians must have Data 2000 waver/ “X number”
• Oral naltrexone; and injectable naltrexone (Vivitrol)– IM once monthly when stabilized on oral naltrexone
– Weaker effectiveness data
Methadone:Specialized, Licensed Opioid Treatment Programs
• Physical, blood work, treatment plans with updates
• Drink their methadone dose daily as dispensed by a nurse /pharmacist 6-7 days per week
• Mostly self-pay
• Mandatory counseling (approx. monthly)
• Mandatory diversion control– Random call backs
– Random drug screens
– Take homes earned over months of compliance
Bupe Office Based Opioid Tx (OBOT)
• No required diversion control– No pill/strip counts– No random drug screens or tests
• No required treatment planning• No required physical exam• No required supervised dosing• No required counseling
JUST LIKE OTHER OPIOIDS and BENZOS
How methadone and bupe work
When these medications are given regularly:
Sit on opioid receptors and prevents a “high” when other opioids used
Prevents withdrawal
Controls craving
What medications don’t do
• Decrease use of non-opioids
• Produce “addiction to methadone/bupe”• No “lose control of use, lose control of life”
• There is physiologic dependence with methadone and bupe as with ongoing use of all opioid agonists
• Cure an acute illness
naltrexone (also for alcohol addiction)
• Oral naltrexone – Must dose daily
• ER Naltrexone (Vivitrol)– Stabilize first on oral naltrexone
– One shot per month,
– Special ordered, refrigerated
– Cost $700-$1000 ish
– Issues: cost, insurance coverage, operations
Opioid dependence in pregnancy• Treatment of choice is methadone maintenance through pregnancy,
although bupe may be preferred in some cases as NAS is less severe with bupe.
• NAS severity is not correlated with maternal dose of methadone or bupe.
• If detox is required, this should be done in the second trimester
• Detoxification may require HLOC at a substance abuse/psych unit of a general hospital with OB-GYN resources
• Methadone tx and bupe are safer than other opioids in pregnancy, due to its long lasting effects, and decrease risks related to street-use of drugs
• Breastfeeding is encouraged
First dose of bupe
• IF patient non-physiologically dependent
get high
• IF physiologically dependent and in withdrawal
stops withdrawal
• IF physiologically dependent and receptors occupied by pain pills/heroin
immediate withdrawal
Issues with bupe
• Federal 30/100 pt limit, DEA visits, lack of health plan payments including no Medicaid coverage until this year led to clinic practice models that look to DEA like pill mills:
– Cash only
– Long distances pts drive
– Ongoing prescriptions for controlled drugs
– Short clinic hours
– No board certification of specialists
– High billing for drugs tests ( $1000s per specimen)
(All but the last 2 are normally seen also in psychiatric practice)
Diversion issues with bupe
• Patients getting rx for more than they need and selling additional ( “2 large” tabs/strips saturate >94% of mu opioid receptors)
• Decreased availability of pain pills heroin and bupe
• “self treating” with street maintenance bupe
• “self managing withdrawal” with street bupe
Help with Diversion Issues:Practice Guidelines
• ASAM Guidelines due April 2015
– Indicate what should be part of treatment
– Need further research on best practice with best outcomes in effect and cost-effectiveness
• Federation of State Medical Board Guidelines

So remember,
Public Safety
+
Public Health
Gratitude
Law Enforcement Track:Trends in Drugs of Choice
Presenters:
• E. Mick Mollica, President and CEO, LEARN Associates, Inc.
• Kelly J. Clark, MD, MBA, FASAM, DFAPA, President-elect, American Society of Addiction Medicine (ASAM), and Member, Rx Summit National Advisory Board
Moderator: Chauncey Parker, Director, New York/New Jersey High Intensity Drug Trafficking Area (HIDTA), and Member, Rx Summit National Advisory Board