Rx15 clinical wed_430_1_wexelblatt-ford_2warner-roussosross
113
Clinical Track: Maternal-Fetal Issues for Physicians Presenters: • Scott L. Wexelblatt, MD, Regional Medical Director for Newborn Services, Cincinnati Children’s Hospital Medical Center • Susan Ford, RN, BSN, BEACON Quality Improvement Coordinator, Ohio Perinatal Quality Collaborative • Tamara D. Warner, PhD, Research Assistant Professor, Department of Pediatrics, University of Florida • Kay Roussos-Ross, MD, Director of Women’s Health, UF Shands Medical Plaza Moderator: Carla S. Saunders, NNP-BC, Advance Practice Coordinator, Pediatrix Medical Group, and Neonatal Nurse Practitioner, East Tennessee Children’s Hospital, and Member, Rx Summit National Advisory Board
-
Upload
opunite -
Category
Healthcare
-
view
177 -
download
0
Transcript of Rx15 clinical wed_430_1_wexelblatt-ford_2warner-roussosross
Clinical Track:Maternal-Fetal Issues
for Physicians
Presenters:
• Scott L. Wexelblatt, MD, Regional Medical Director for Newborn Services, Cincinnati Children’s Hospital Medical Center
• Susan Ford, RN, BSN, BEACON Quality Improvement Coordinator, Ohio Perinatal Quality Collaborative
• Tamara D. Warner, PhD, Research Assistant Professor, Department of Pediatrics, University of Florida
• Kay Roussos-Ross, MD, Director of Women’s Health, UF Shands Medical Plaza
Moderator: Carla S. Saunders, NNP-BC, Advance Practice Coordinator, Pediatrix Medical Group, and Neonatal Nurse Practitioner, East TennesseeChildren’s Hospital, and Member, Rx Summit National Advisory Board
Disclosures
• Scott L. Wexelblatt, MD; Susan Ford, RN, BSN; Tamara D. Warner, PhD; and Kay Roussos-Ross, MD, have disclosed no relevant, real, or apparent personal or professional financial relationships with proprietary entities that produce healthcare goods and services.
• Carla Saunders – Speaker’s bureau: Abbott Nutrition
Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition
Learning Objectives
1. Describe an NAS treatment protocol that has decreased opioid treatment days and the length of hospital.
2. Prepare physicians to screen and counsel pregnant patients about prenatal marijuana use.
3. Outline changes in the potency and use of marijuana during the past 30 years that may affect the developmental outcomes of today’s children with prenatal marijuana exposure.
Maternal-Fetal Issues for Physicians: Optimal Care for Infants with
Neonatal Abstinence Syndrome
Scott Wexelblatt, MD
Susan Ford, RN, BSN
Disclosures
• Scott Wexelblatt, MD has disclosed no relevant, real or apparent personal or profession financial relationship with proprietary entities that produce health care goods and services.
• Susan Ford, RN, BSN, has disclosed no relevant, real or apparent personal or profession financial relationship with proprietary entities that produce health care goods and services.
• Disclaimer: The images of people used in this presentation are for visual representations only.
Learning Objectives
• Describe an NAS treatment protocol that has decreased opioid treatment days and the length of hospital.
– NAS diagnoses increased three-fold from 2002 to 2009, according to a 2012 study in JAMA.
– In this session, clinicians will observe that an Ohio pilot study in six children’s hospitals used a stringent weaning protocol to decrease opioid treatment days and the length of hospital stay.
– This work, which was published in Pediatrics in August 2014, is the largest published cohort of over 530 infants pharmacologically treated for NAS.
– Fifty-two hospitals in Ohio now are incorporating this knowledge for a quality improvement initiative and have a goal to reduce the length of stay by 20 percent by June 30, 2015.
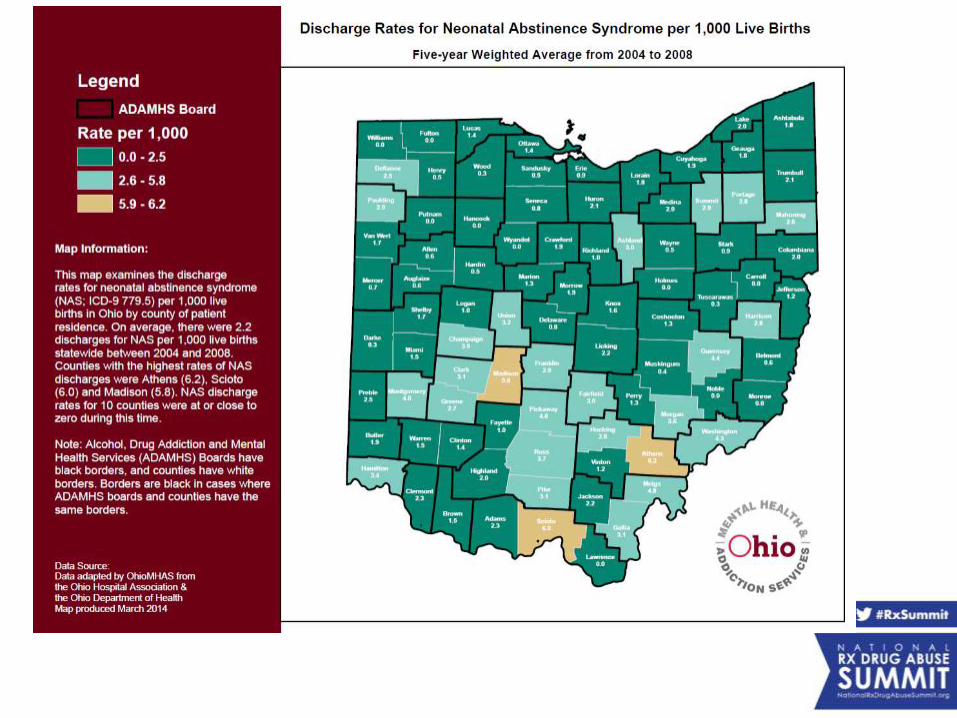
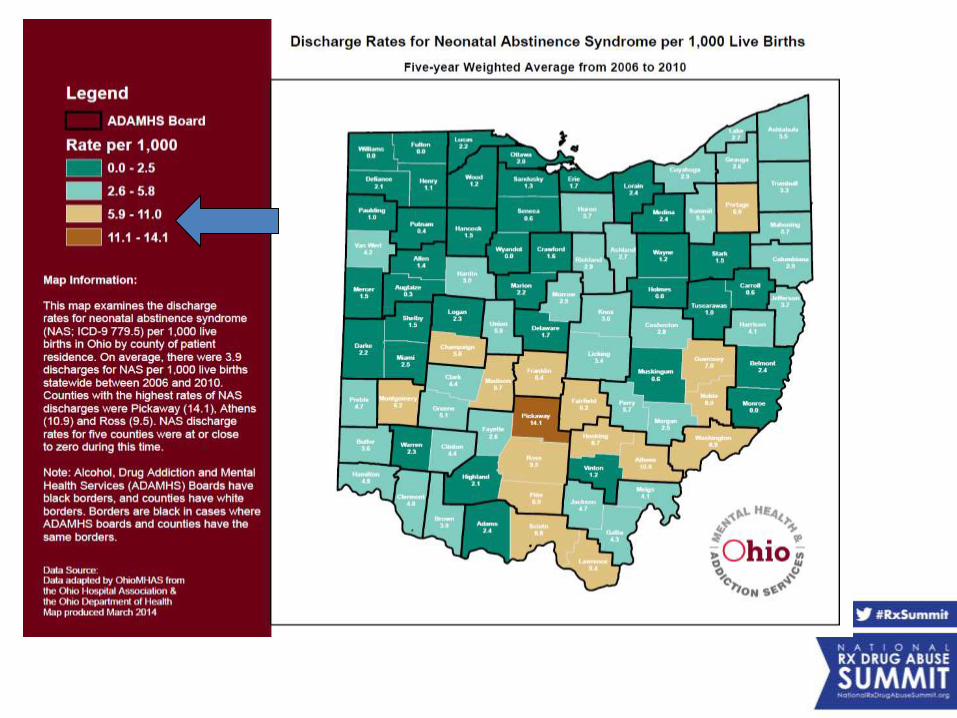
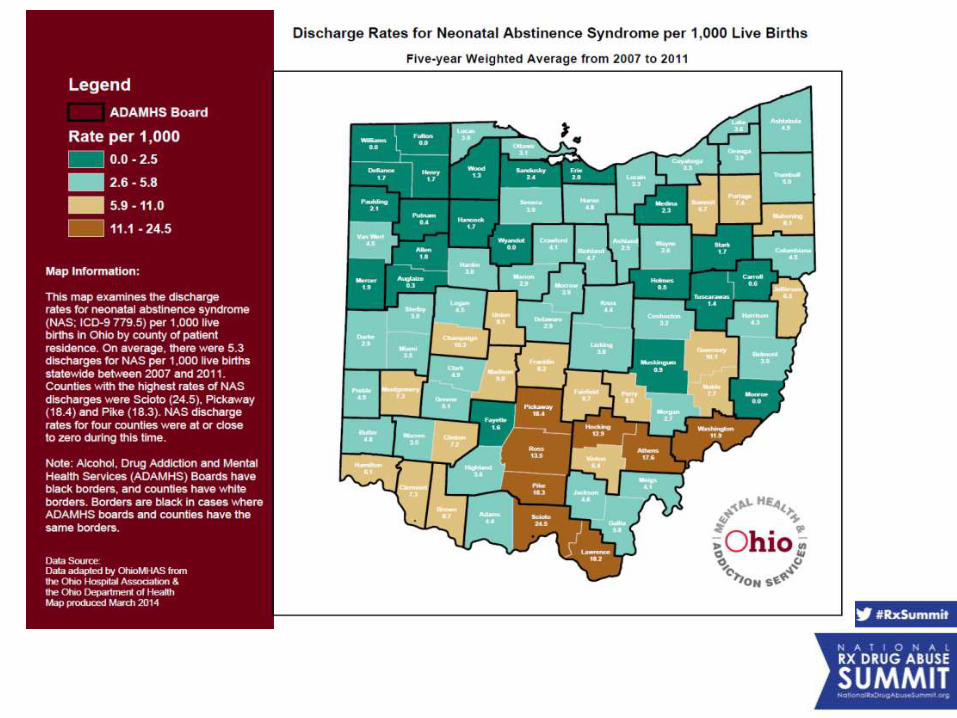
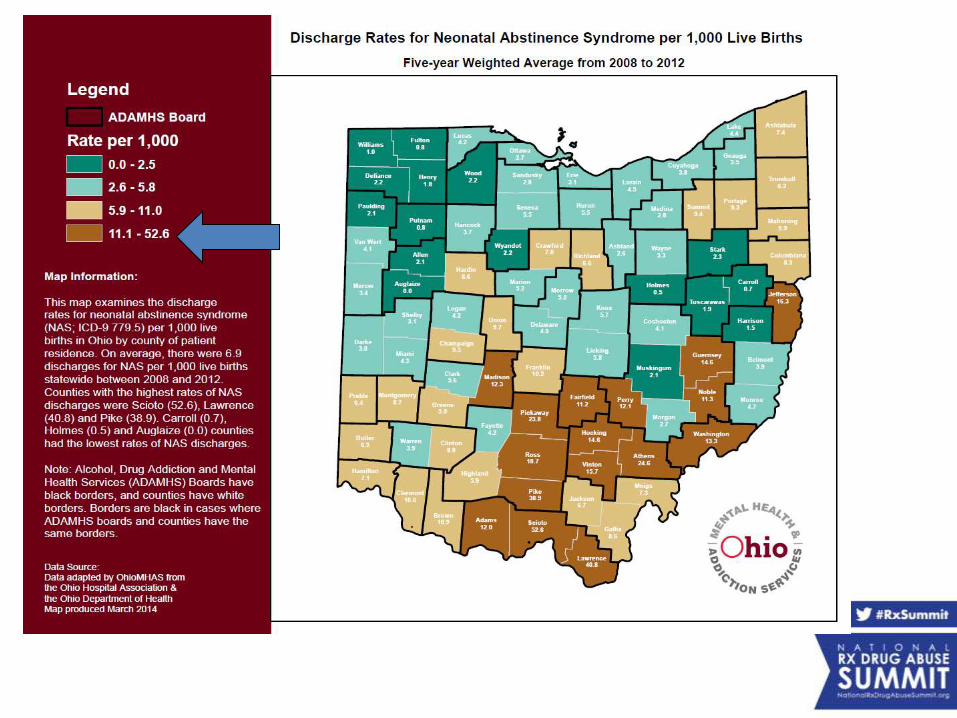
Neonatal Abstinence Syndrome
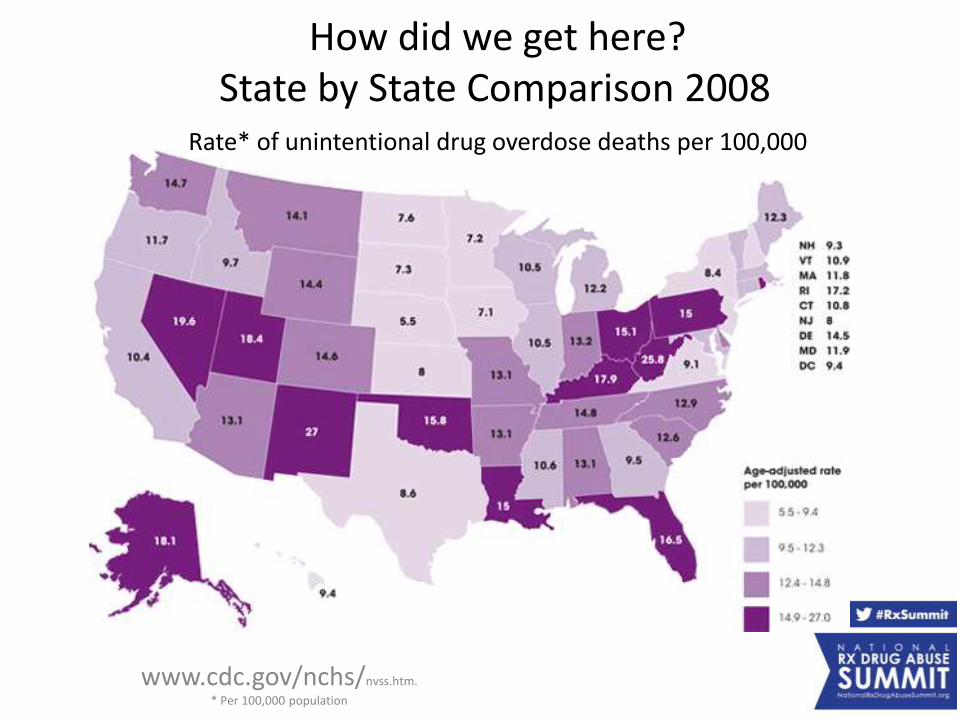
www.cdc.gov/nchs/nvss.htm.
* Per 100,000 population
How did we get here?State by State Comparison 2008
Rate* of unintentional drug overdose deaths per 100,000
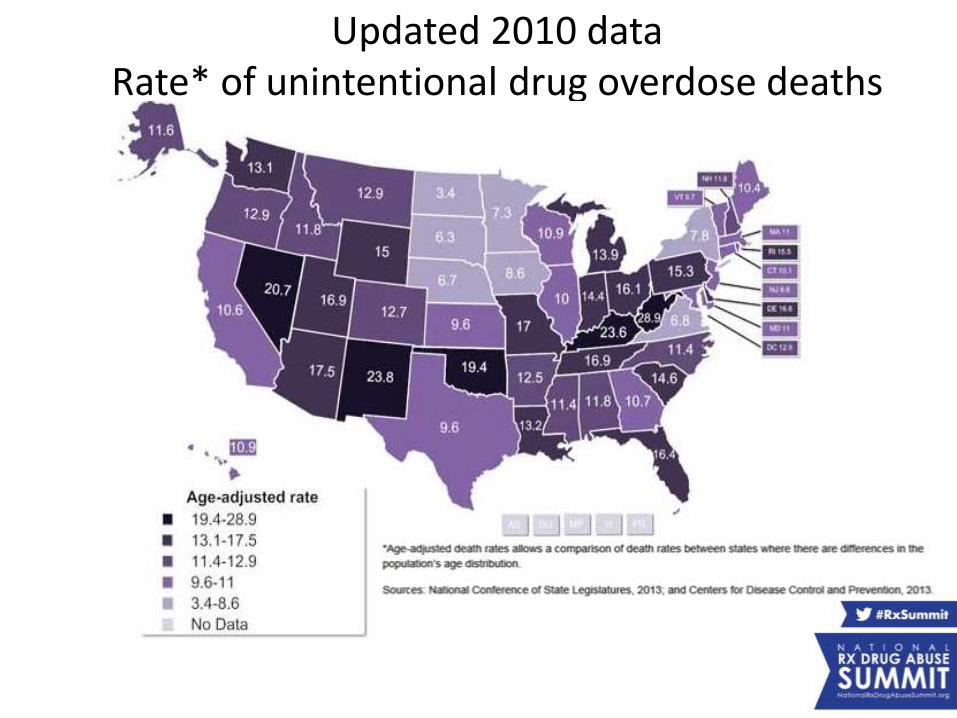
Updated 2010 dataRate* of unintentional drug overdose deaths
per 100,000
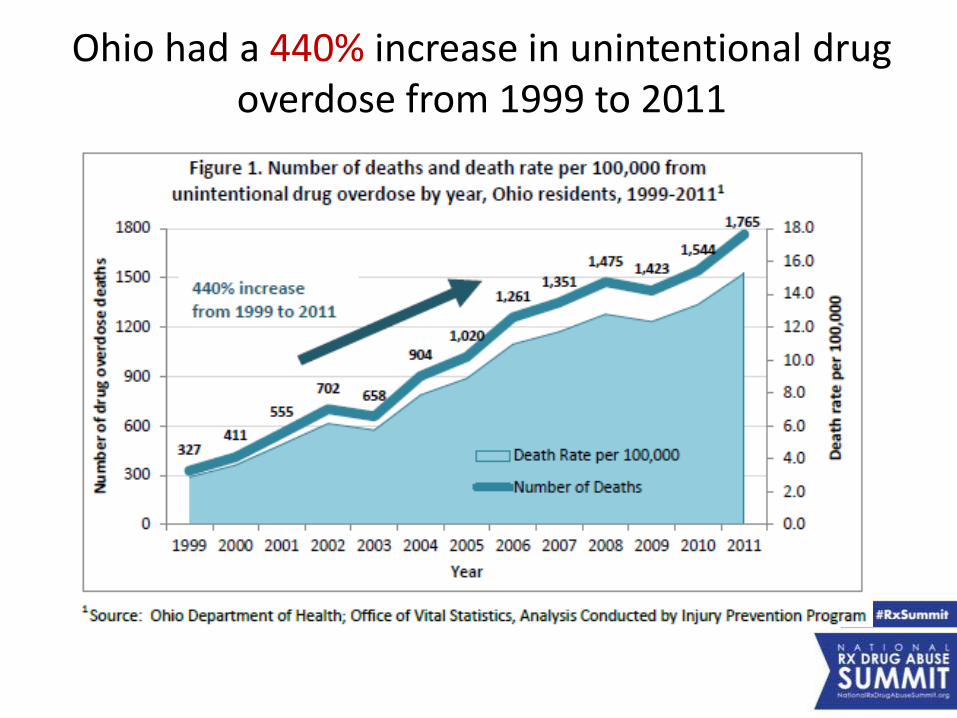
Ohio had a 440% increase in unintentional drug overdose from 1999 to 2011
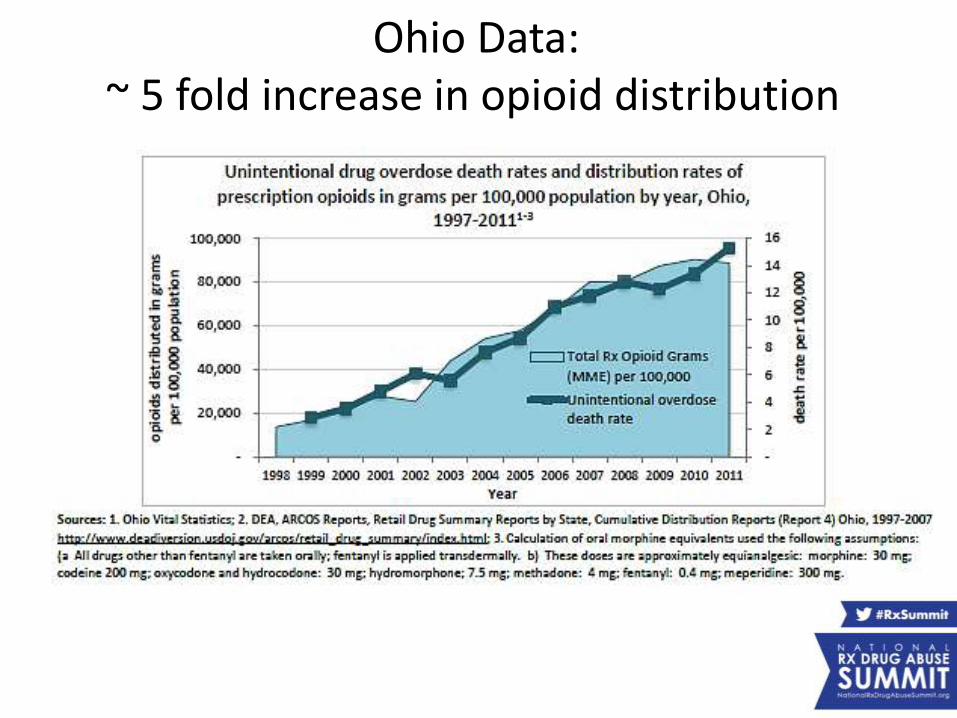
Ohio Data:~ 5 fold increase in opioid distribution
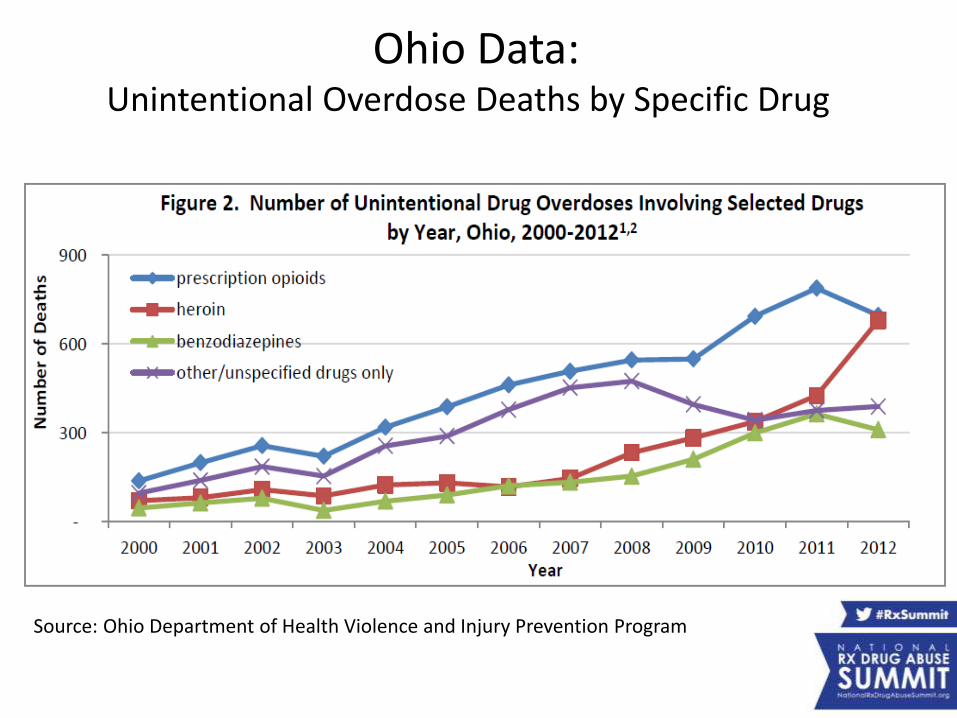
Ohio Data:Unintentional Overdose Deaths by Specific Drug
Source: Ohio Department of Health Violence and Injury Prevention Program
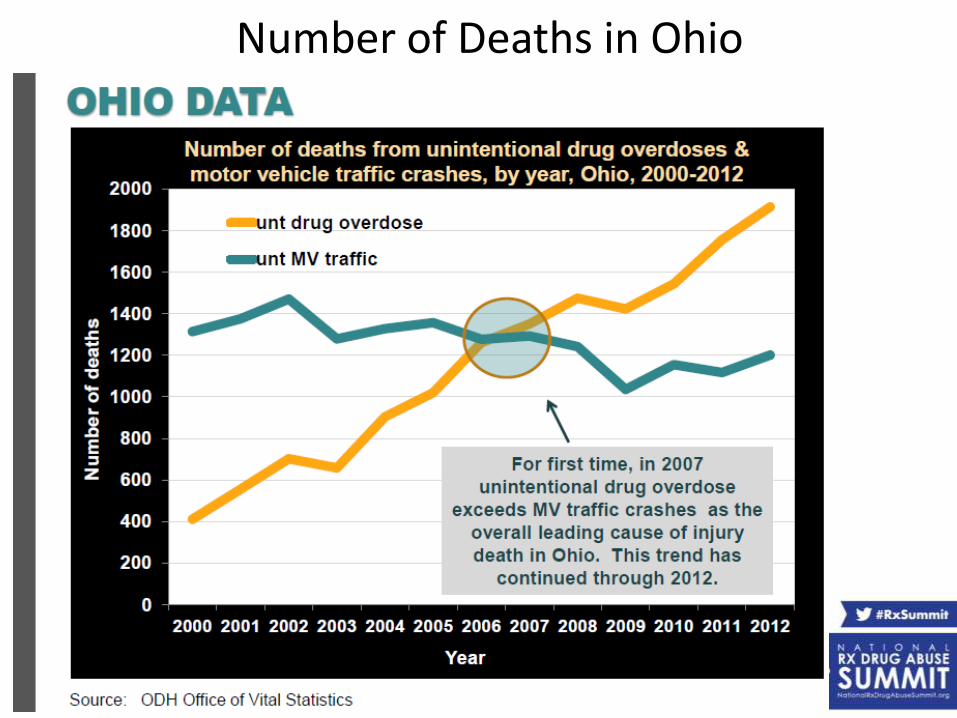
Number of Deaths in Ohio

Ohio Children’s Hospital NAS Consortium
• Organized in January 2012
• Chartered by Governor Kasich to work together to improve care of children
• Neo Inaugural Project: NAS- launched Sept 2012
• Form longitudinal cohort of term infants with narcotic abstinence syndrome.• Infants admitted by 6 Ohio Children’s Hospitals to
total of 20 hospitals.
• Describe the maternal and neonatal characteristics
• Determine the “potentially better practice” for narcotic abstinence treatment.
• Identify variation and areas for future research.
Consortium Objectives:
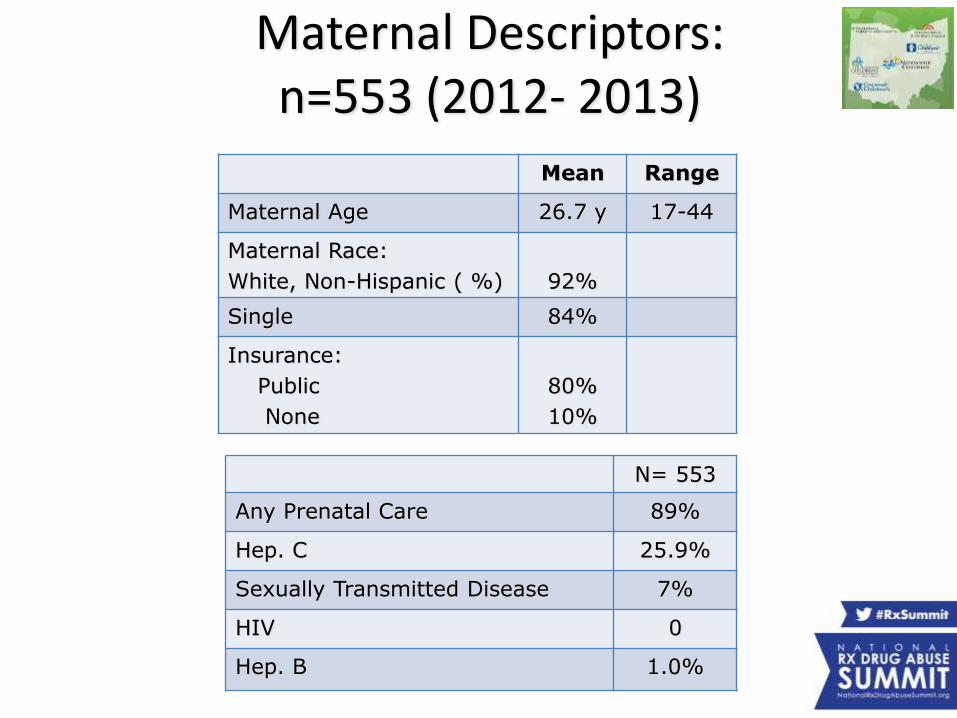
Maternal Descriptors: n=553 (2012- 2013)
Mean Range
Maternal Age 26.7 y 17-44
Maternal Race:
White, Non-Hispanic ( %) 92%
Single 84%
Insurance:
Public
None
80%
10%
N= 553
Any Prenatal Care 89%
Hep. C 25.9%
Sexually Transmitted Disease 7%
HIV 0
Hep. B 1.0%
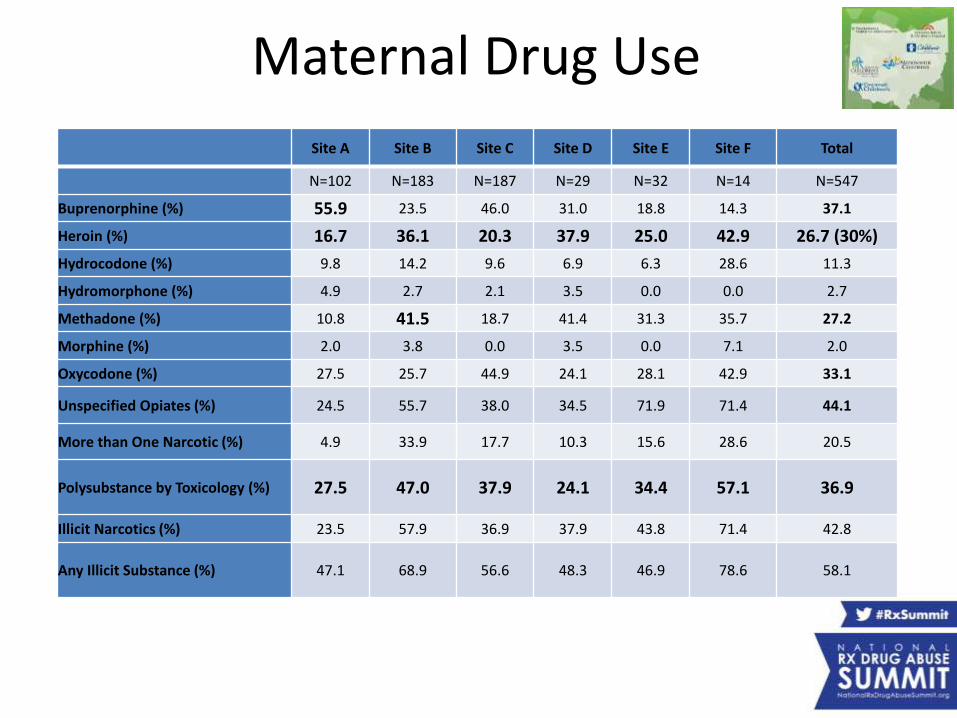
Maternal Drug Use
Site A Site B Site C Site D Site E Site F Total
N=102 N=183 N=187 N=29 N=32 N=14 N=547
Buprenorphine (%) 55.9 23.5 46.0 31.0 18.8 14.3 37.1
Heroin (%) 16.7 36.1 20.3 37.9 25.0 42.9 26.7 (30%)
Hydrocodone (%) 9.8 14.2 9.6 6.9 6.3 28.6 11.3
Hydromorphone (%) 4.9 2.7 2.1 3.5 0.0 0.0 2.7
Methadone (%) 10.8 41.5 18.7 41.4 31.3 35.7 27.2
Morphine (%) 2.0 3.8 0.0 3.5 0.0 7.1 2.0
Oxycodone (%) 27.5 25.7 44.9 24.1 28.1 42.9 33.1
Unspecified Opiates (%) 24.5 55.7 38.0 34.5 71.9 71.4 44.1
More than One Narcotic (%) 4.9 33.9 17.7 10.3 15.6 28.6 20.5
Polysubstance by Toxicology (%) 27.5 47.0 37.9 24.1 34.4 57.1 36.9
Illicit Narcotics (%) 23.5 57.9 36.9 37.9 43.8 71.4 42.8
Any Illicit Substance (%) 47.1 68.9 56.6 48.3 46.9 78.6 58.1
Needle exchange program…
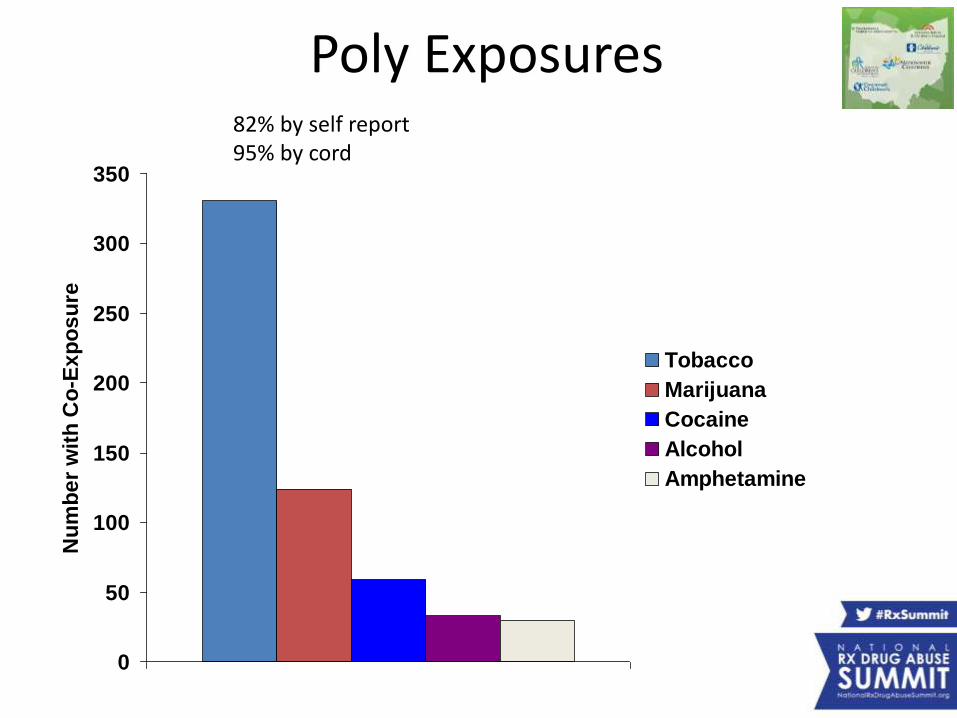
Updated data through 994 mothers:• Heroin use: 30% (n=298)• Hepatitis C rate: 26% (n=257)
• Under current law, needle exchanges can be created in Ohio only with a declared local health emergency.
Prevention Not Permission Portsmouth City Health Department
0
50
100
150
200
250
300
350
Nu
mb
er
wit
h C
o-E
xp
os
ure
Tobacco
Marijuana
Cocaine
Alcohol
Amphetamine
Poly Exposures82% by self report95% by cord
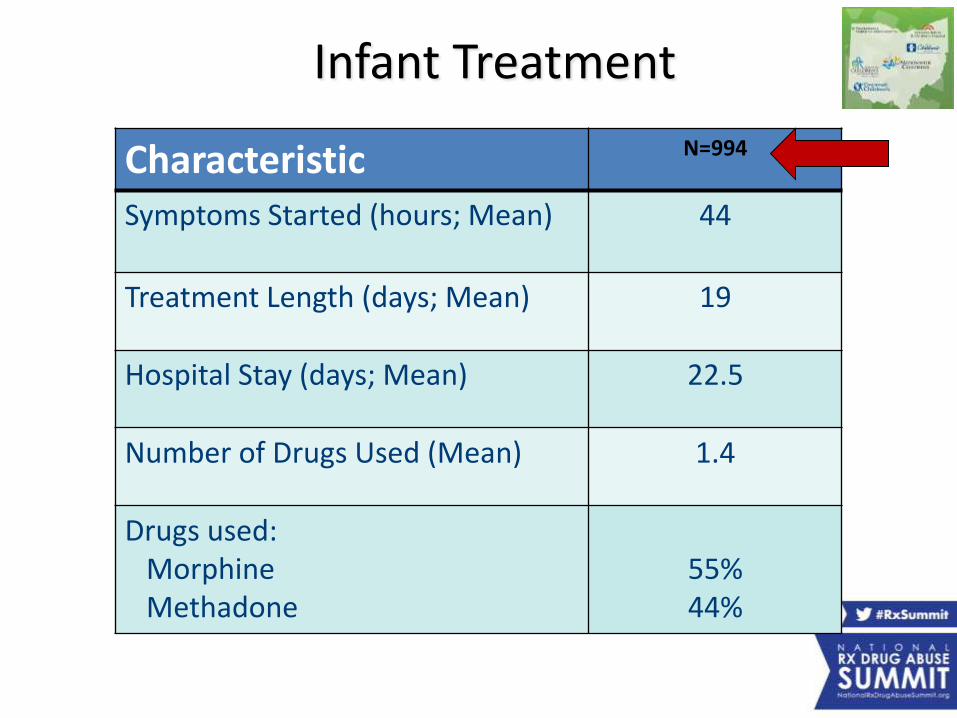
Infant Treatment
Characteristic N=994
Symptoms Started (hours; Mean) 44
Treatment Length (days; Mean) 19
Hospital Stay (days; Mean) 22.5
Number of Drugs Used (Mean) 1.4
Drugs used:MorphineMethadone
55%44%
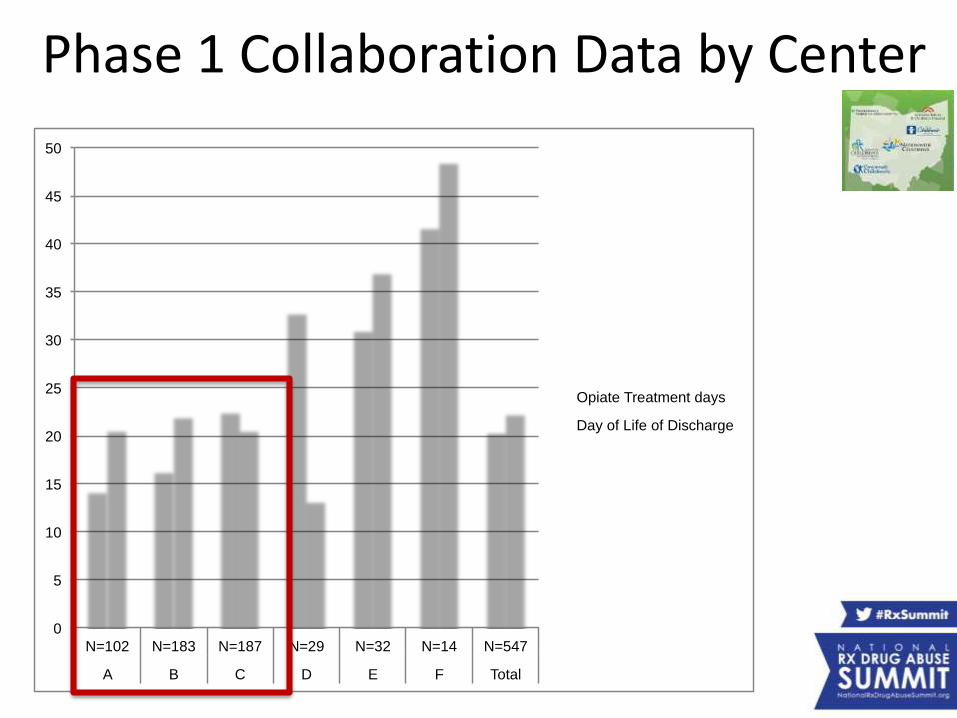
Phase 1 Collaboration Data by Center
0
5
10
15
20
25
30
35
40
45
50
N=102 N=183 N=187 N=29 N=32 N=14 N=547
A B C D E F Total
Opiate Treatment days
Day of Life of Discharge
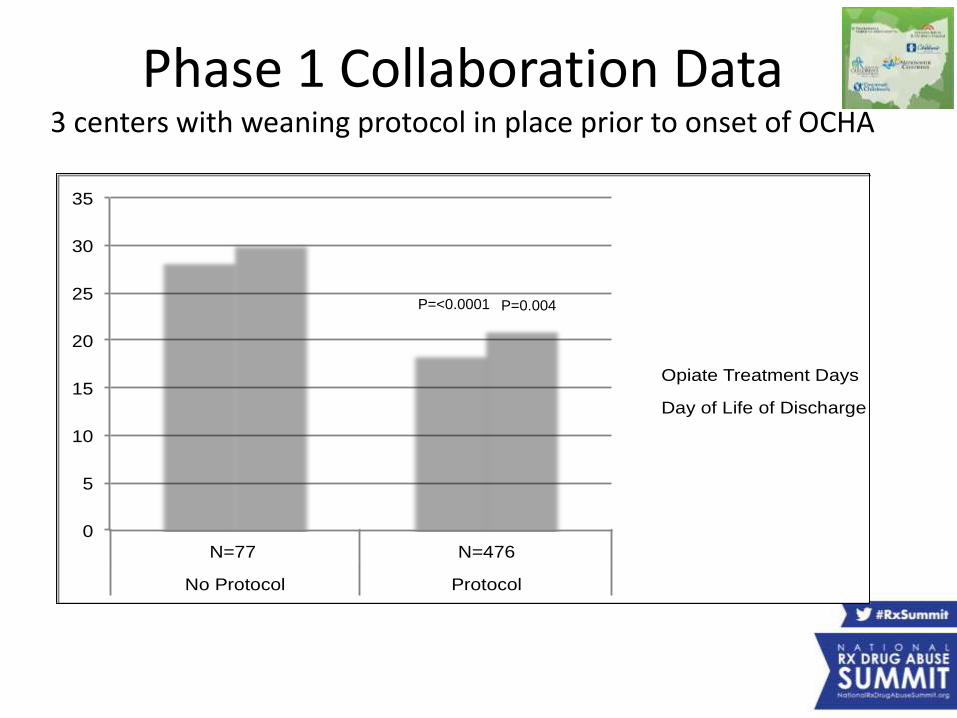
Phase 1 Collaboration Data3 centers with weaning protocol in place prior to onset of OCHA
0
5
10
15
20
25
30
35
N=77 N=476
No Protocol Protocol
Opiate Treatment Days
Day of Life of Discharge
P=<0.0001 P=0.004
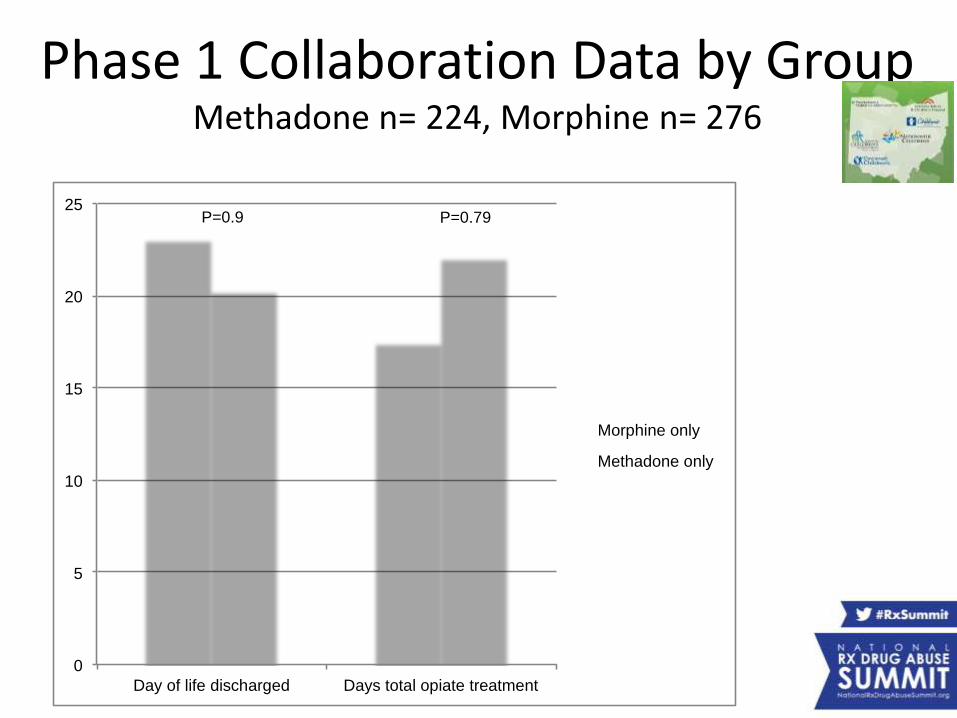
Phase 1 Collaboration Data by GroupMethadone n= 224, Morphine n= 276
0
5
10
15
20
25
Day of life discharged Days total opiate treatment
Morphine only
Methadone only
P=0.79P=0.9
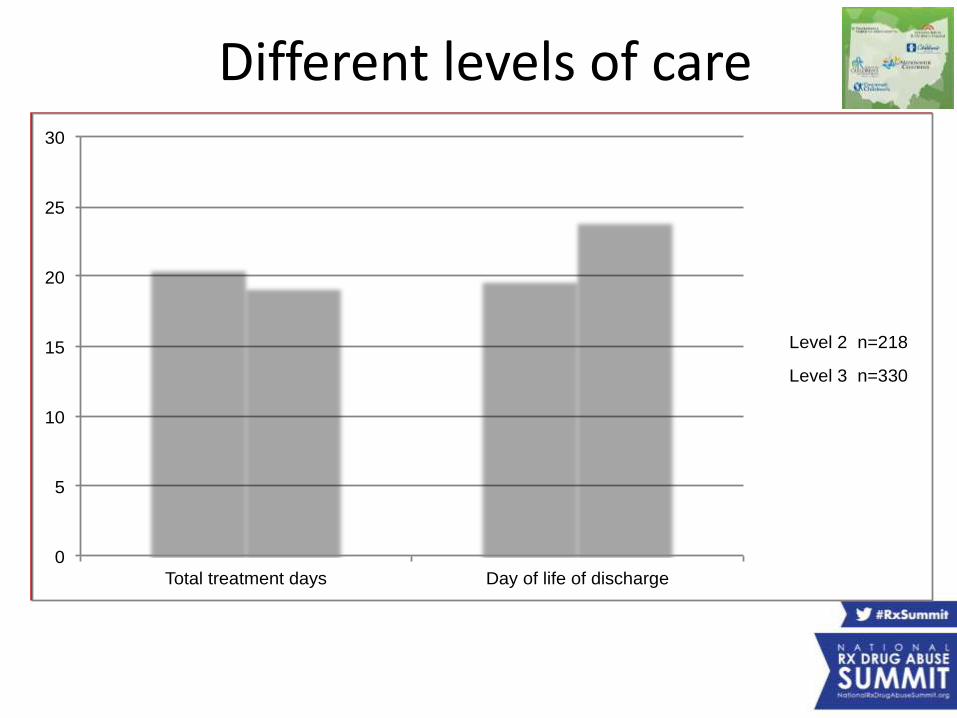
Different levels of care
0
5
10
15
20
25
30
Total treatment days Day of life of discharge
Level 2 n=218
Level 3 n=330
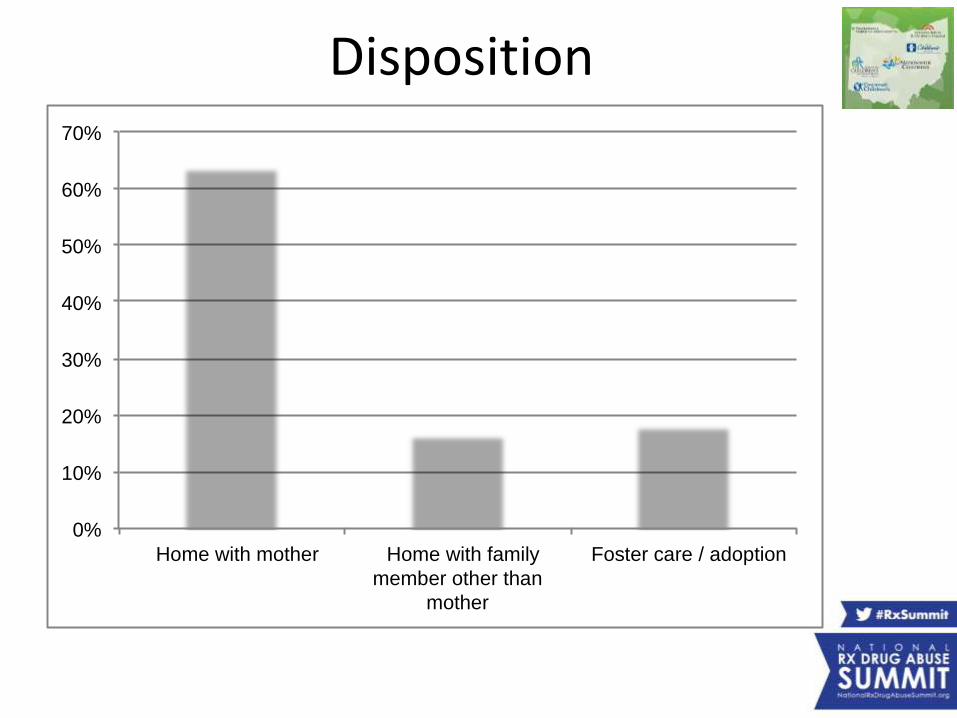
0%
10%
20%
30%
40%
50%
60%
70%
Home with mother Home with family
member other than
mother
Foster care / adoption
Disposition
OCHA Publication
Paper in Pediatrics August 2014
Neonatal Narcotic Abstinence Syndrome:
A Multicenter Cohort Study of Treatments and Hospital Outcomes
Eric S Hall, PhD1*, Scott L Wexelblatt, MD1*, Moira Crowley, MD2,
Jennifer L Grow, MD3, Lisa R Jasin, MSN, NNP-BC4, Mark A Klebanoff,
MD5, Richard E McClead, MD6, Jareen Meinzen-Derr, PhD1,7, Vedagiri K
Mohan, MD8, Howard Stein, MD8, and Michele C Walsh, MD, MS Epi2
on behalf of the OCHNAS Consortium
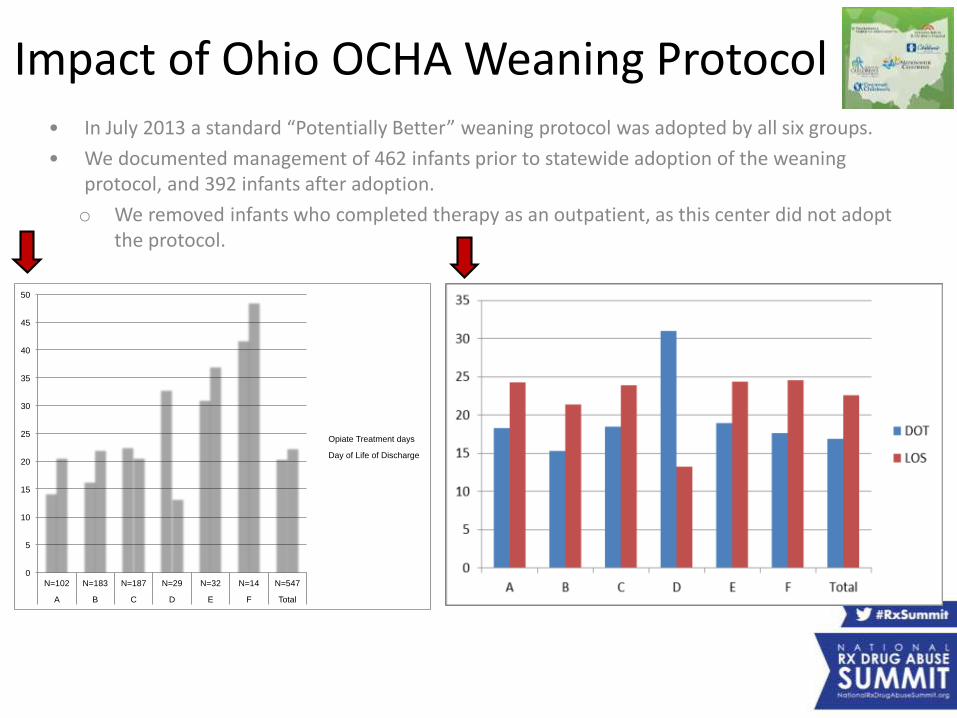
Impact of Ohio OCHA Weaning Protocol• In July 2013 a standard “Potentially Better” weaning protocol was adopted by all six groups.
• We documented management of 462 infants prior to statewide adoption of the weaning protocol, and 392 infants after adoption.
o We removed infants who completed therapy as an outpatient, as this center did not adopt the protocol.
0
5
10
15
20
25
30
35
40
45
50
N=102 N=183 N=187 N=29 N=32 N=14 N=547
A B C D E F Total
Opiate Treatment days
Day of Life of Discharge
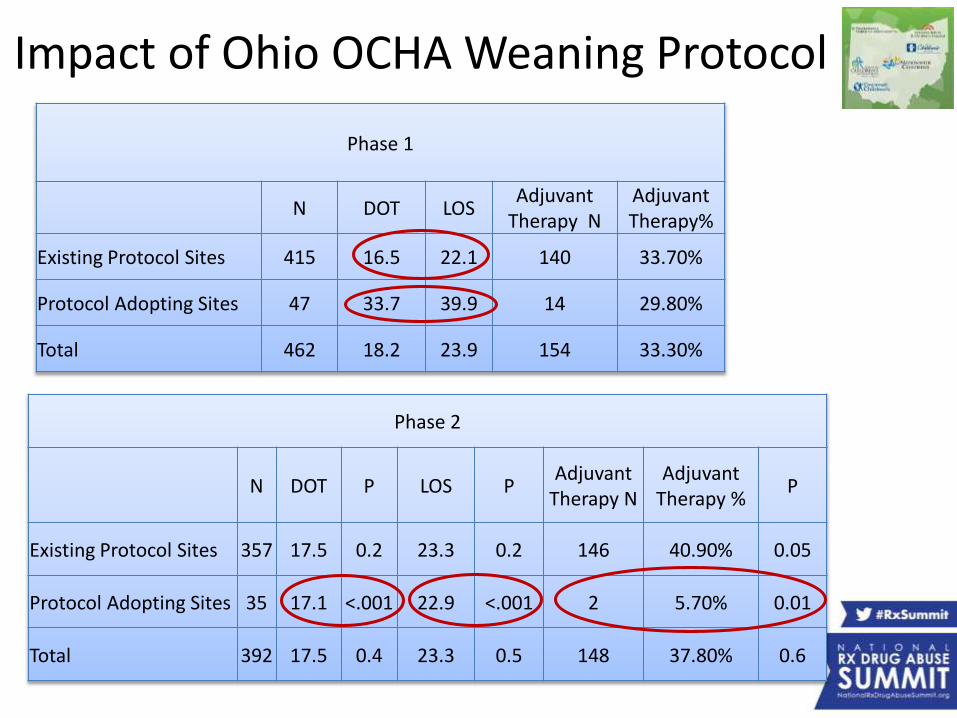
Phase 2
N DOT P LOS PAdjuvant
Therapy NAdjuvant
Therapy %P
Existing Protocol Sites 357 17.5 0.2 23.3 0.2 146 40.90% 0.05
Protocol Adopting Sites 35 17.1 <.001 22.9 <.001 2 5.70% 0.01
Total 392 17.5 0.4 23.3 0.5 148 37.80% 0.6
Phase 1
N DOT LOSAdjuvant
Therapy NAdjuvant Therapy%
Existing Protocol Sites 415 16.5 22.1 140 33.70%
Protocol Adopting Sites 47 33.7 39.9 14 29.80%
Total 462 18.2 23.9 154 33.30%
Impact of Ohio OCHA Weaning Protocol
Conclusions: • Adoption of standard opioid weaning guidelines for
NAS reduced the duration of opiate exposure and
length of hospital stay.
• Outcomes among infants managed by providers with
existing explicit weaning protocols were sustained
after statewide adoption.
Impact of Ohio OCHA Weaning Protocol
0
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Nu
mb
er o
f D
ays
Infants Treated for NAS through 2014
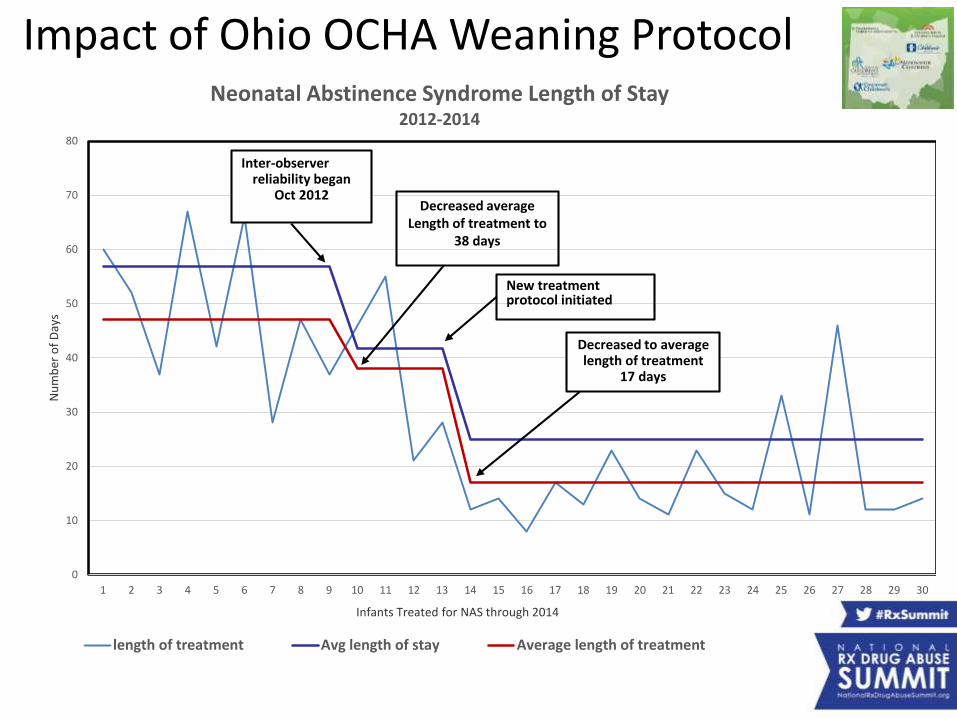
Neonatal Abstinence Syndrome Length of Stay2012-2014
length of treatment Avg length of stay Average length of treatment
Inter-observerreliability began
Oct 2012Decreased average
Length of treatment to 38 days
New treatment protocol initiated
Decreased to average length of treatment
17 days
Impact of Ohio OCHA Weaning Protocol

The OPQC NAS Project is funded by The Ohio Department of
Medicaid

Social Media
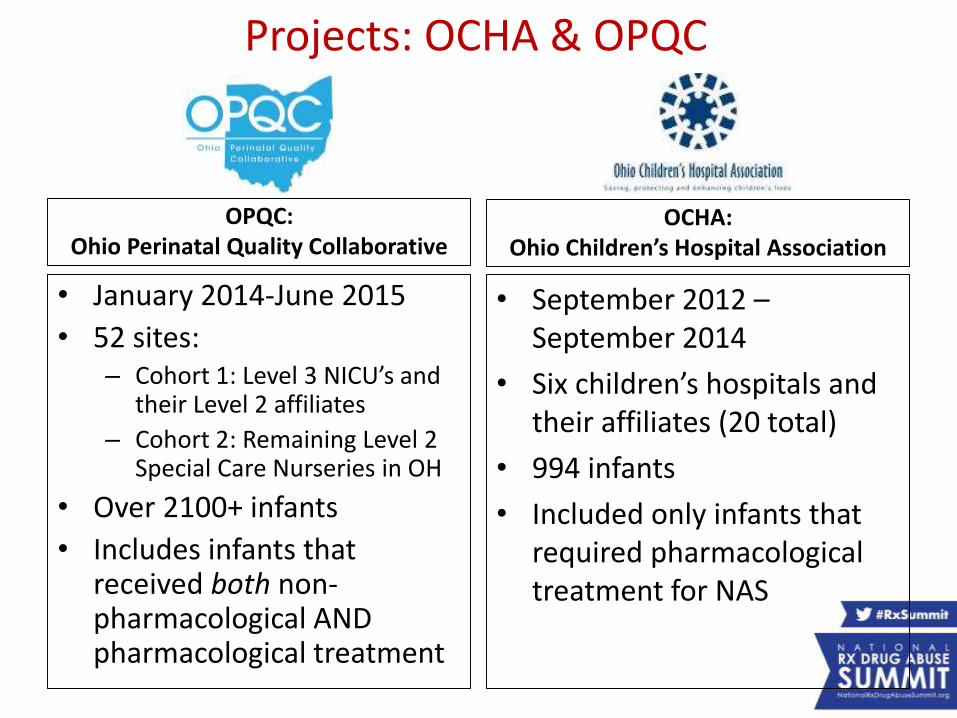
Projects: OCHA & OPQC
OCHA: Ohio Children’s Hospital Association
• September 2012 –September 2014
• Six children’s hospitals and their affiliates (20 total)
• 994 infants
• Included only infants that required pharmacological treatment for NAS
OPQC: Ohio Perinatal Quality Collaborative
• January 2014-June 2015
• 52 sites:– Cohort 1: Level 3 NICU’s and
their Level 2 affiliates
– Cohort 2: Remaining Level 2 Special Care Nurseries in OH
• Over 2100+ infants
• Includes infants that received both non-pharmacological AND pharmacological treatment
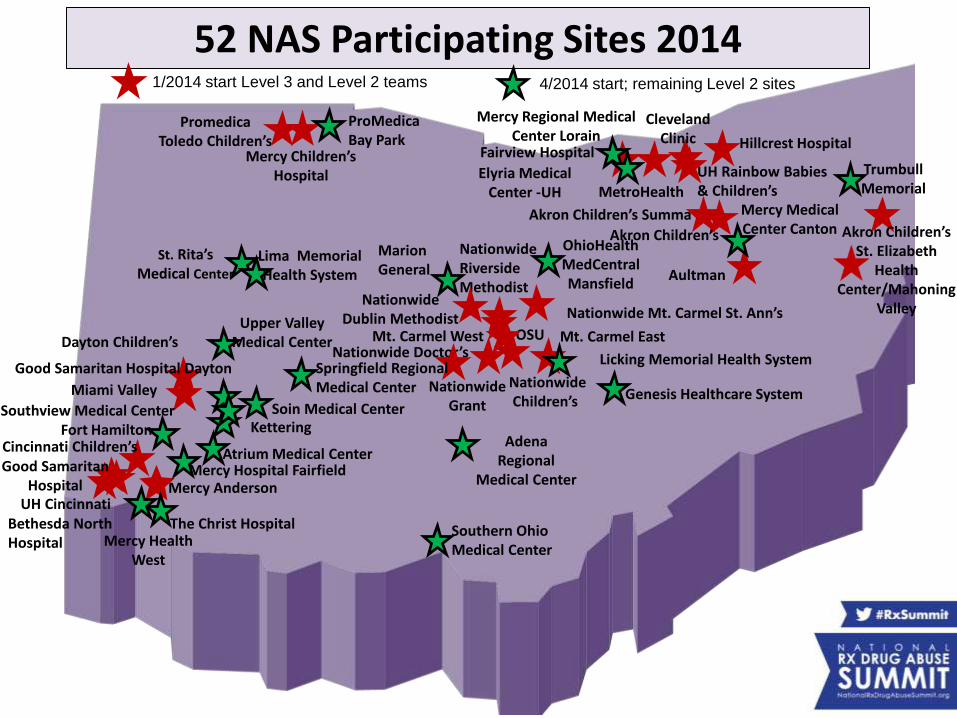
PromedicaToledo Children’s
Miami Valley
Mercy Anderson
Aultman
Mt. Carmel EastOSU
UH Rainbow Babies & Children’s
Bethesda North Hospital
Nationwide Dublin Methodist
Akron Children’s Summa
Cincinnati Children’s
Hillcrest HospitalFairview Hospital
ClevelandClinic
Dayton Children’s
NationwideRiverside Methodist
Nationwide Grant
Nationwide Mt. Carmel St. Ann’s
UH Cincinnati
Good Samaritan Hospital
MetroHealth
Mt. Carmel WestNationwide Doctor’s
Akron Children’s
NationwideChildren’s
Mercy Children’s Hospital
Atrium Medical Center
Fort Hamilton
Mercy Hospital Fairfield
Mercy Medical Center Canton
The Christ Hospital
St. Rita’sMedical Center
Southview Medical Center
Good Samaritan Hospital Dayton
Kettering
Mercy Health West
Southern Ohio Medical Center
Genesis Healthcare System
OhioHealth MedCentral Mansfield
Marion General
Elyria Medical Center -UH
Mercy Regional Medical Center Lorain
ProMedica Bay Park
Lima Memorial Health System
Springfield RegionalMedical Center
Adena Regional
Medical Center
Soin Medical Center
Upper Valley Medical Center
Licking Memorial Health System
52 NAS Participating Sites 20141/2014 start Level 3 and Level 2 teams
Akron Children’s St. Elizabeth
Health Center/Mahoning
Valley
Trumbull Memorial
4/2014 start; remaining Level 2 sites
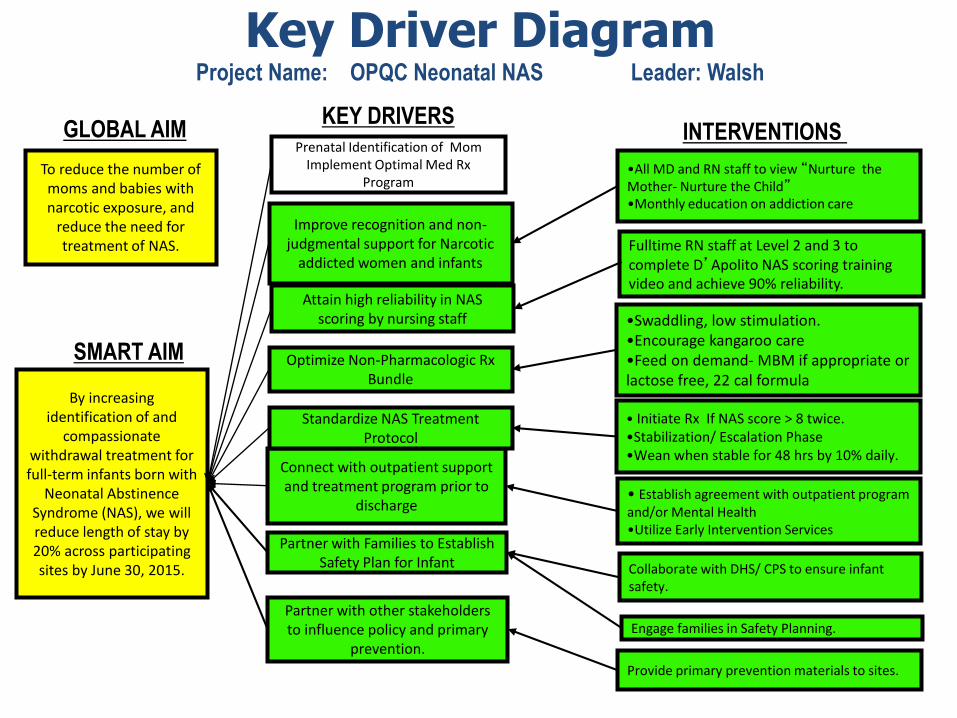
Key Driver DiagramProject Name: OPQC Neonatal NAS Leader: Walsh
SMART AIM
KEY DRIVERSINTERVENTIONS
By increasing identification of and
compassionate withdrawal treatment for full-term infants born with
Neonatal Abstinence Syndrome (NAS), we will reduce length of stay by 20% across participating sites by June 30, 2015.
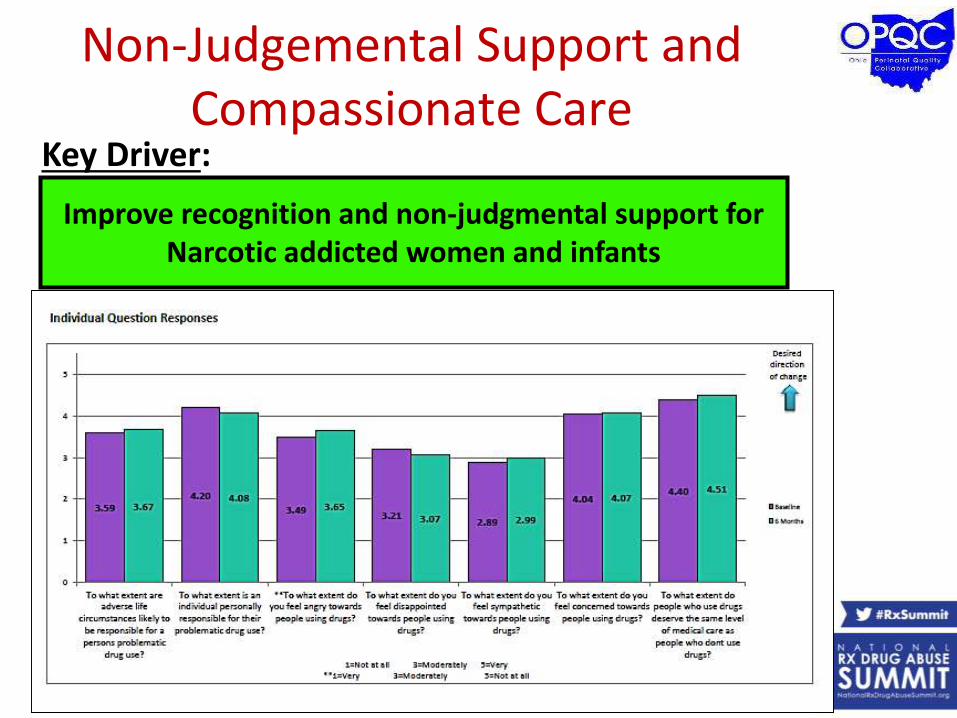
Improve recognition and non-judgmental support for Narcotic
addicted women and infants
Connect with outpatient support and treatment program prior to
discharge
Standardize NAS Treatment Protocol
Optimize Non-Pharmacologic Rx Bundle
• Initiate Rx If NAS score > 8 twice.•Stabilization/ Escalation Phase•Wean when stable for 48 hrs by 10% daily.
•Swaddling, low stimulation.•Encourage kangaroo care•Feed on demand- MBM if appropriate or lactose free, 22 cal formula
•All MD and RN staff to view “Nurture the Mother- Nurture the Child”•Monthly education on addiction care
Attain high reliability in NAS scoring by nursing staff
Partner with Families to Establish Safety Plan for Infant
Fulltime RN staff at Level 2 and 3 to complete D’Apolito NAS scoring training video and achieve 90% reliability.
• Establish agreement with outpatient program and/or Mental Health•Utilize Early Intervention Services
Collaborate with DHS/ CPS to ensure infant safety.
Prenatal Identification of MomImplement Optimal Med Rx
Program
Engage families in Safety Planning. Partner with other stakeholders to influence policy and primary
prevention.
Provide primary prevention materials to sites.
To reduce the number of moms and babies with narcotic exposure, and
reduce the need for treatment of NAS.
GLOBAL AIM
Improve Consistency in Modified Finnegan Scoring
• All sites use same tool
• Train RN staff to 90% reliability in scoring using D’Apolito Training System
• In Pilot work, we were able to see drop in max score when training completed
• OPQC has sent out DVD’s to each site
Attain high reliability in NAS scoring by nursing
staff
Intervention:
Fulltime RN staff at Level 2 and 3 to complete D’Apolito NAS scoring training video and achieve 90% reliability.
Non-Pharmacologic Management of Infants with NAS
• Feeding on Demando Breast Milk Feeds
(contraindicated if Mom not in Treatment program/still using illicit drugs/HIV+)
o Low Lactose Formula
o 22 kcal/oz feeds
• Swaddling
• Low Stimulation
• Rooming In
Other interventions in the literature: Skin-to-Skin/Kangaroo Care Rocker Beds Massage therapy Music therapy Aromatherapy (lavender,
mother’s scent) Color Therapy (B&W
more soothing?)
Optimize Non-Pharmacologic Rx Bundle
Key Driver:
Key Driver:
Intervention:
Pharmacological Bundle
Standardize NAS Treatment Protocol
• Initiate Rx If NAS score > 8 twice.•Stabilization/ Escalation Phase•Begin wean when stable for 48hrs•Discharge home after 48hrs (Morphine) to 72hrs (Methadone)
Source: https://neoadvances.org
Source: https://abcnews.com
Key Driver:
Intervention:
Relationships with Support Services
•Establish agreement with outpatient program and/or Mental Health Services•Utilize Early Intervention Services
Connect with outpatient support and treatment
program prior to dischargeExamples of organizations our hospital teams have partnered with:• County Drug Courts• MAT Treatment Centers• Homeless Shelters (gender specific)• ADAMHS Board (Alcohol, Drug Addiction
and Mental Health Services) throughout the state of Ohio• Under Ohio law, the ADAMHS Board is one of
50 Boards coordinating the public behavioral health system in Ohio.
Key Driver:
Non-Judgemental Support and Compassionate Care
Improve recognition and non-judgmental support for Narcotic addicted women and infants
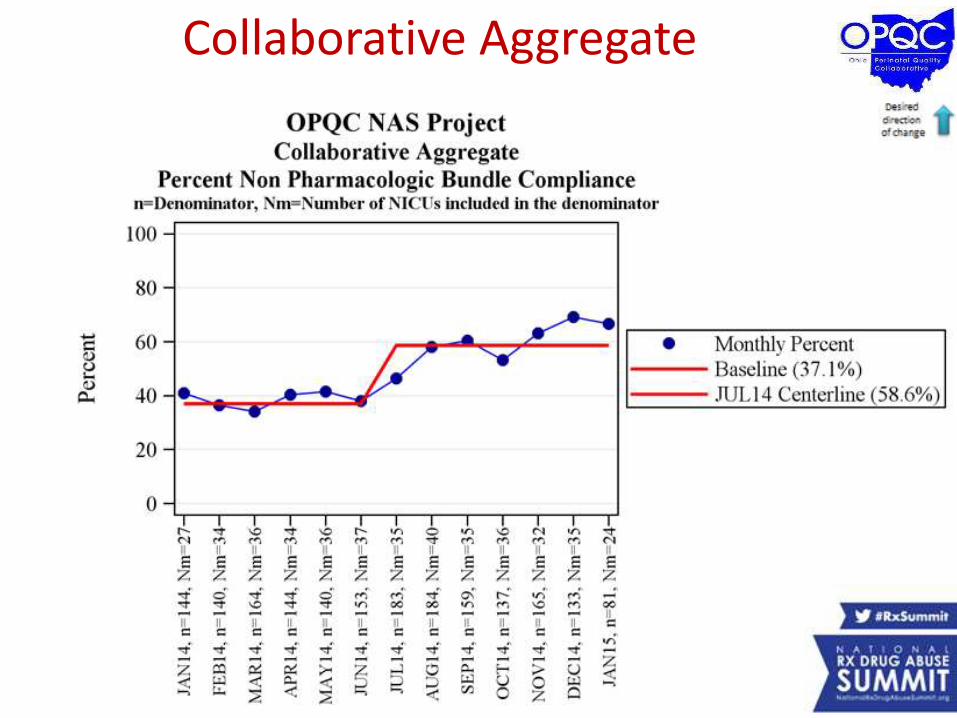
Collaborative Aggregate
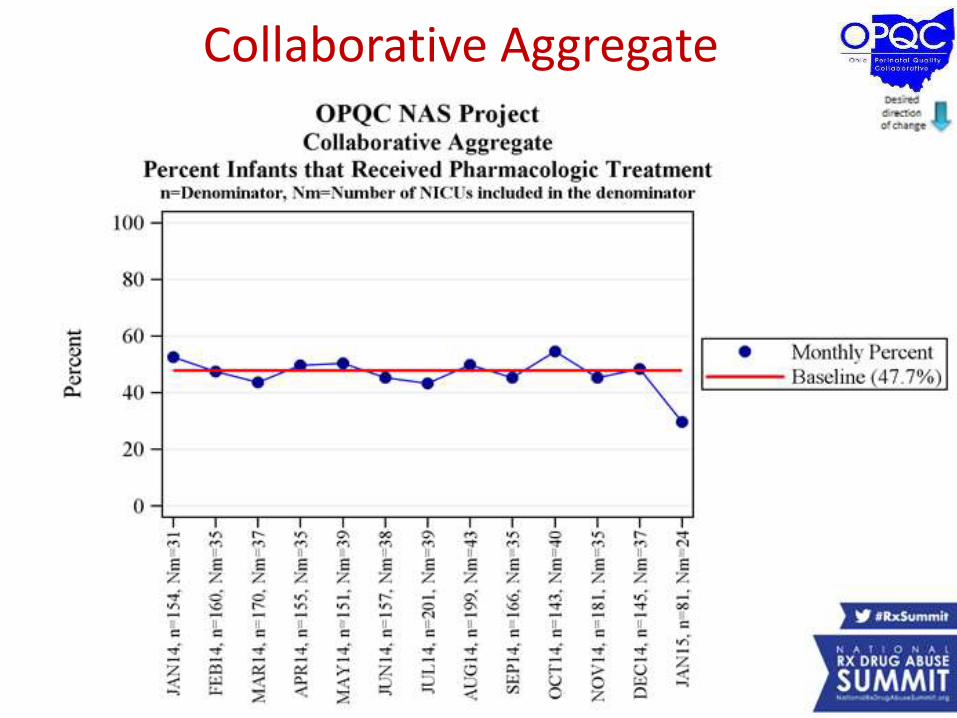
Collaborative Aggregate
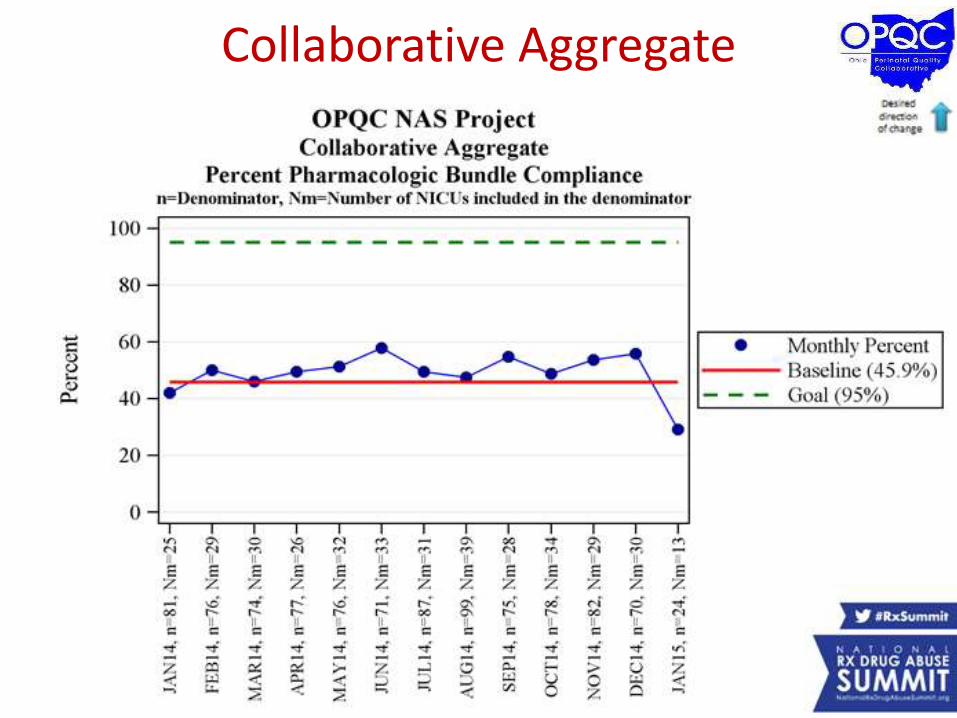
Collaborative Aggregate
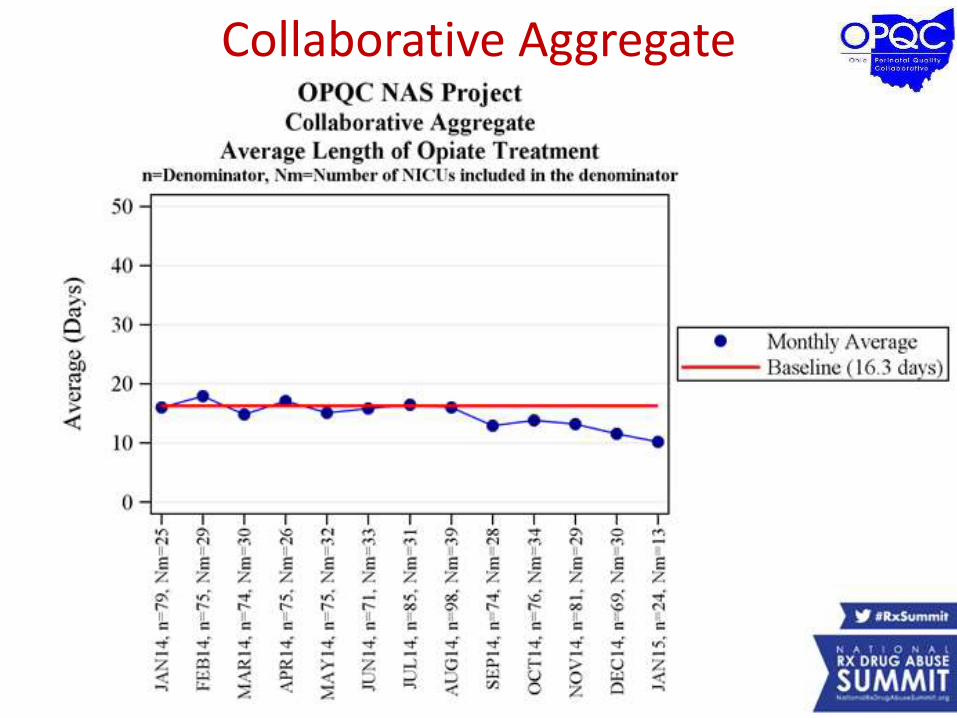
Collaborative Aggregate
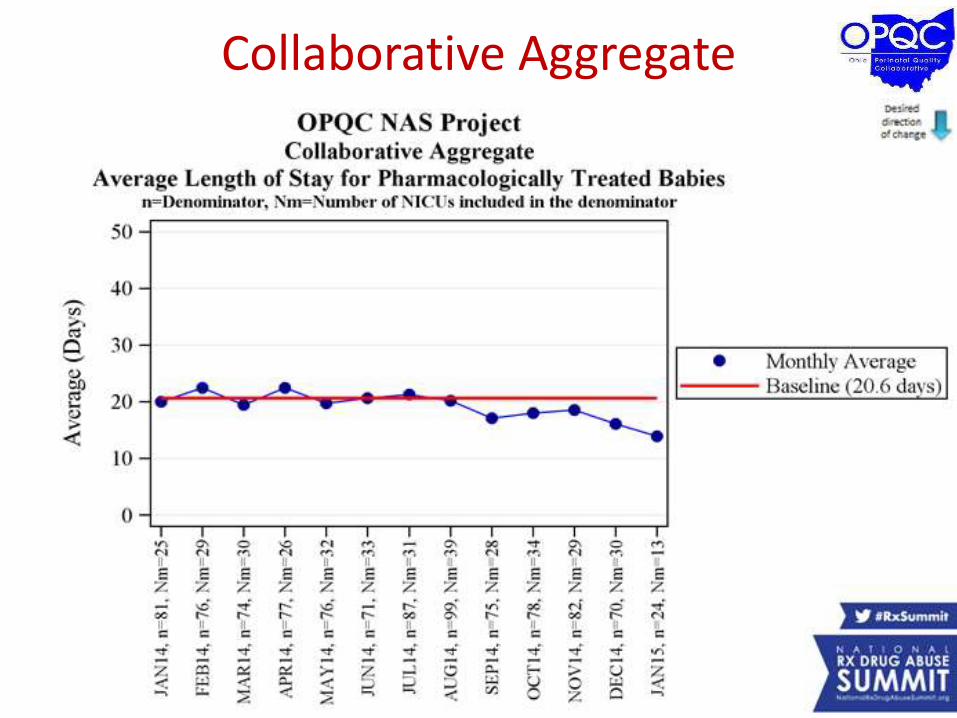
Collaborative Aggregate
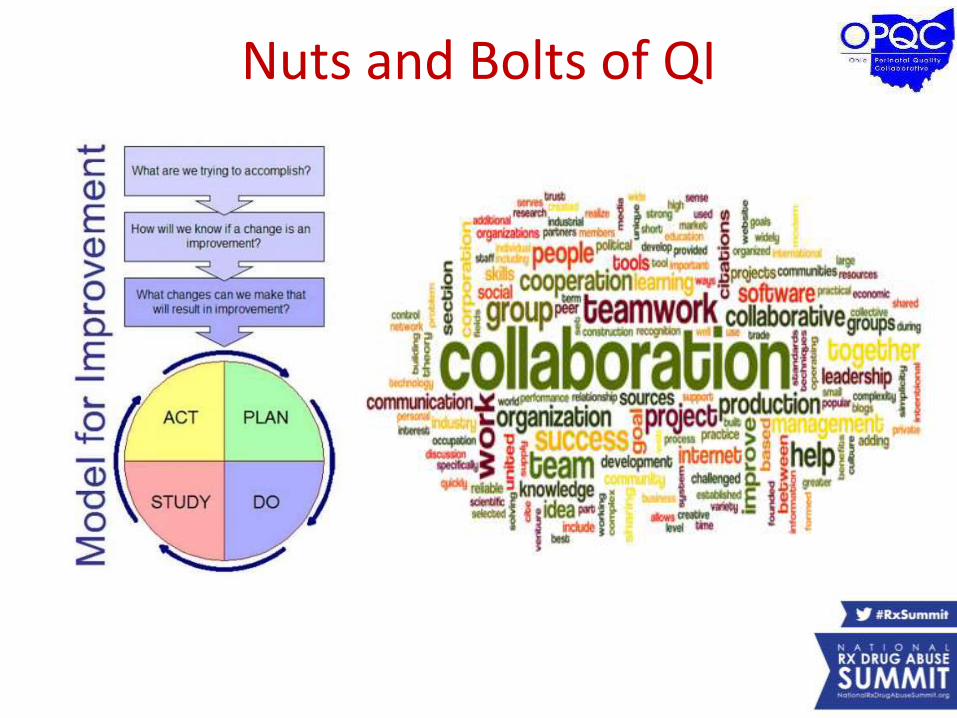
Nuts and Bolts of QI

• 21 Outpatient OB Centers• 48 NICU’s and Special Care Nurseries • Centers for Disease Control and Prevention• Ohio Department of Health• Ohio Department of Medicaid• Ohio Hospital Association• Ohio Children's Hospital Association• Ohio Child Welfare Training Program• Government Resource Center• State Board of Nursing• State Board of Medicine • State Board of Dentistry• Graham's Foundation • Ohio Department of Mental Health and Addiction
Services • XIX Recovery Support Services• North Carolina Perinatal Quality Collaborative• First Step Home• Brigid’s Path• Lily’s Place• The Turning Point Program• Ohio Managed Care Organizations • Ohio Collaborative to Prevent Infant Mortality

It’s Not Your Mother’s Marijuana:Effects on Maternal-Fetal Health and
the Developing Child
Dr. Kay Roussos-Ross, MDDirector of Women’s Health, Dept. of Ob/Gyn
University of Florida
Dr. Tamara Warner, Ph.D.Research Assistant Professor, Dept. of Pediatrics
University of Florida
Disclosures
Dr. Roussos-Ross and Dr. Warner have no conflicts of interest to disclose.
Objectives
• Prepare physicians to screen and counsel pregnant patients about prenatal marijuana use.
• Outline changes in the potency and use of marijuana during the past 30 years that may affect the developmental outcomes of today’s children with prenatal marijuana exposure.
Clinics in Perinatology (December 2014) Vol. 41, Issue 4, pages 877-894.
DOI: http://dx.doi.org/10.1016//j.clp.2014.08.009
Part 1
Pro-Marijuana Advocacy Efforts and Changes in Marijuana Potency and Use
Societal Shift in Attitudes About Marijuana

States Legalizing “Medical” Marijuana
1. Alaska2. Arizona3. California4. Colorado5. Connecticut6. DC7. Delaware8. Hawaii9. Illinois10. Maine11. Maryland12. Massachusetts
13. Michigan14. Minnesota15. Montana16. Nevada17. New Hampshire18. New Jersey19. New Mexico20. New York21. Oregon22. Rhode Island23. Vermont24. Washington
Pending Legislation in 2015(as of 2/19/15)
1. Florida
2. Georgia
3. Indiana
4. Kansas
5. Kentucky
6. Missouri
7. Nebraska
8. North Dakota
9. Pennsylvania
10. South Carolina
11. Tennessee

States Legalizing Recreational Marijuana
Legal Status of Medical Marijuana?
• Marijuana is a Schedule I drug under the Controlled Substance Act, a federal law that preempts action taken by individual states to legalize its use, cultivation and distribution.
• When used for medicinal purposes, marijuana should be considered a pharmaceutical agent governed by the Food Drug & Cosmetic Act – Regulatory oversight including evaluation of its
safety & efficacy by the Food & Drug Administration.
Does legalizing marijuana result in higher marijuana use?
Higher use in states that:
• Allow home cultivation
• Allow legal dispensaries
Lower use (and treatment admissions) in states that:
• Restrict broad access by requiring annual registration of patients
A: Yes, but it depends on the specific aspects of state laws and policies.
Unintended Consequences of Pro-Marijuana Advocacy Efforts?
• Growing pro-marijuana advocacy efforts are taking place in a very different environment than the 1960s.
• In the absence of strong public health messages about the possible dangers of marijuana, marijuana use may increase among pregnant women.
It’s Not Your Mother’s Marijuana
• The potency of marijuana has significantly increased in potency during the past 40 years.
• The amount of marijuana consumed, on average, among young adults also seems to increasing significantly.
• Marijuana is perceived as relatively “safe” and, in some areas, the cost is comparable to tobacco.
Increased Potency of Marijuana
• Potency is measured by the percentage of Δ9-
tetrahydrocannabinol (THC), the most psychoactive of the 70 cannabinoids found in marijuana.
• From the 1970s to the 2000s, there has been an estimated 6- to 7-fold increase in the percentage of THC found in seized marijuana.
Increased Potency of Marijuana
“It is now possible to mass product plants with potencies inconceivable when concerted monitoring efforts started 40 years ago.”
-- Mehmedic et al. (2010)
Potency Trends of Δ9-THC and Other Cannabinoids in
Confiscated Cannabis Preparations from 1993 to 2008
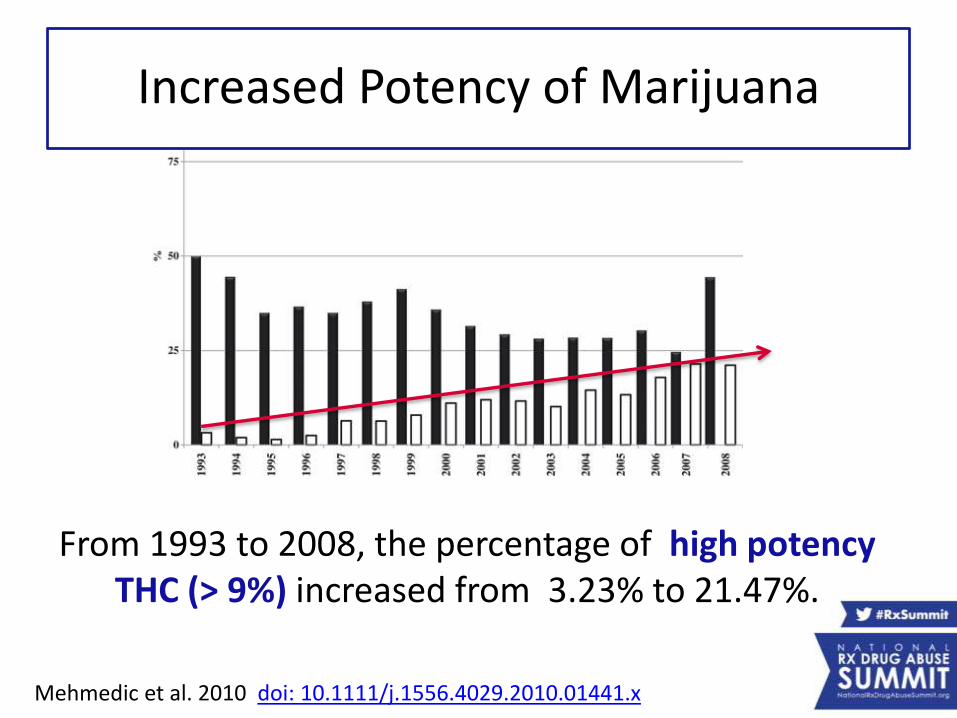
Increased Potency of Marijuana
From 1993 to 2008, the percentage of high potency THC (> 9%) increased from 3.23% to 21.47%.
Mehmedic et al. 2010 doi: 10.1111/j.1556.4029.2010.01441.x
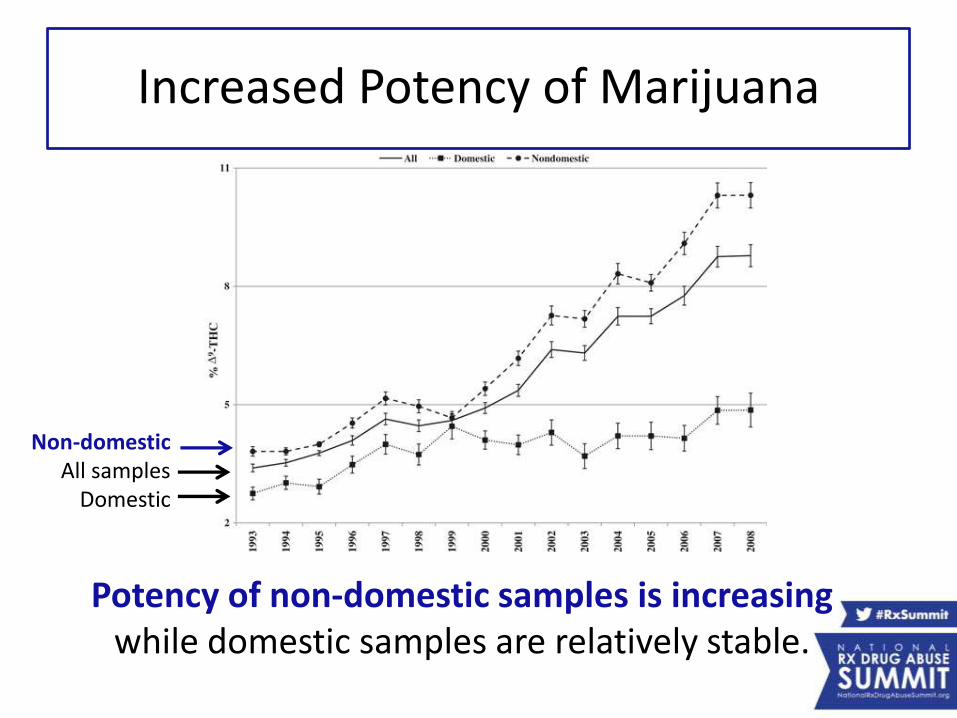
Increased Potency of Marijuana
Potency of non-domestic samples is increasing while domestic samples are relatively stable.
Non-domesticAll samples
Domestic
But There’s More
• There are more than 100 different cannabinoids found in marijuana.
• Not all cannabinoids have psychoactive properties.
• Cannabidiol (CBD) is non-psychotropic and displays many beneficial properties:– Antipsychotic
– Antihyperalgesic
– Anticonvulsant
– Neuroprotective
– Antiemetic properties
The Ratio is Important, Too
• As the percentage of THC has been increasing, the percentage of CBD has been decreasing.
• This is particularly true in sinsemilla – the flowering tops of unfertilized female plants with no seeds, which is gaining market share (commonly called “skunk”)
The Ratio is Important, Too
• The higher ratio of THC/CBD likely makes the marijuana even more potent & dangerous.
– Increased risk for cannabis dependence
– Increased treatment seeking for cannabis-related problems
– Increased vulnerability to psychosis
–May predispose users to adverse psychiatric effects
Amount of Marijuana Use
• Amount of marijuana consumed, on average, may be increasing among younger adults, especially minorities
• Growing popularity of blunts (marijuana-filled cigars) compared to joints and pipes
Amount of Marijuana Use
• Blunts contain significantly more marijuana
–1 blunt = 1.5 joints
–1 blunt = 2.5 pipes
• Blunts are often shared among several people making it difficult to quantify individual usage
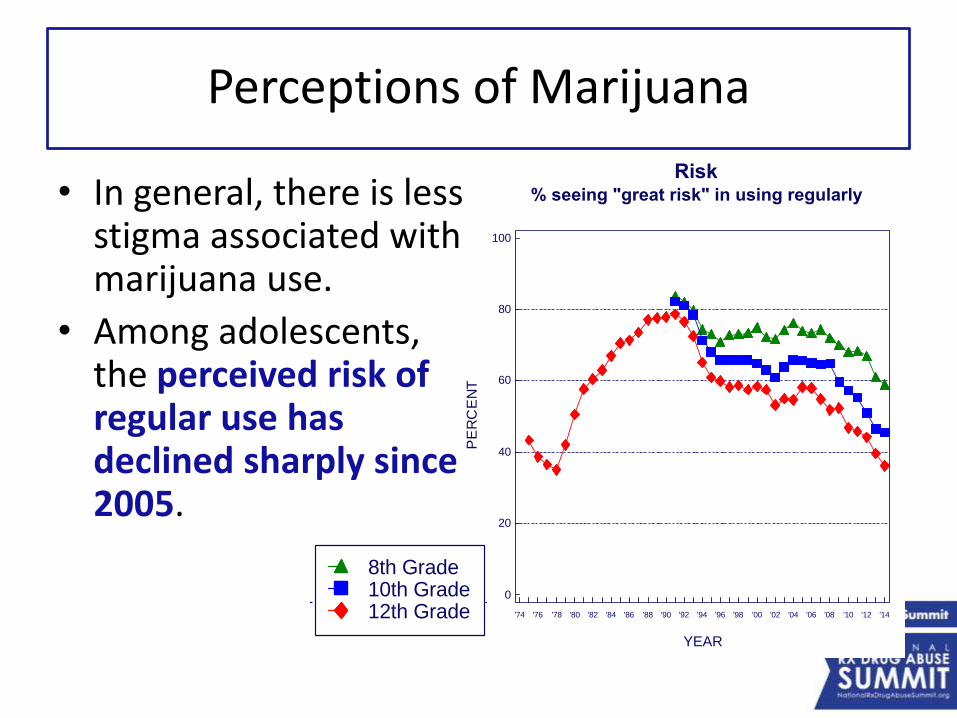
FIGURE 6
Marijuana: Trends in Annual Use, Risk, Disapproval, and Availability
Grades 8, 10, and 12
Source. The Monitoring the Future study, the University of Michigan.
Use% who used in last 12 months
Risk% seeing "great risk" in using regularly
Disapproval% disapproving of using regularly
Availability% saying "fairly easy" or "very easy" to get
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
8th Grade10th Grade12th Grade
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
Perceptions of Marijuana
• In general, there is less stigma associated with marijuana use.
• Among adolescents, the perceived risk of regular use has declined sharply since 2005.
FIGURE 6
Marijuana: Trends in Annual Use, Risk, Disapproval, and Availability
Grades 8, 10, and 12
Source. The Monitoring the Future study, the University of Michigan.
Use% who used in last 12 months
Risk% seeing "great risk" in using regularly
Disapproval% disapproving of using regularly
Availability% saying "fairly easy" or "very easy" to get
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
8th Grade10th Grade12th Grade
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
PE
RC
EN
T
0
20
40
60
80
100
YEAR
'74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '06 '08 '10 '12 '14
Perceptions of Marijuana
• One study of urban pregnant women found that marijuana was perceived as “safer” to use during pregnancy than cigarettes or alcohol.
• Misperceptions may be due to the relative absence of strong public health messages.
• Cost of marijuana was comparable to tobacco; price is no longer a deterrent.
Part 2
The Epidemiology of Marijuana Use Among Pregnant Women: Who Uses?
Epidemiology of Marijuana Use Among Pregnant Women
• Most commonly used illicit drug during pregnancy.
• Estimated 115,000 pregnant women annually.
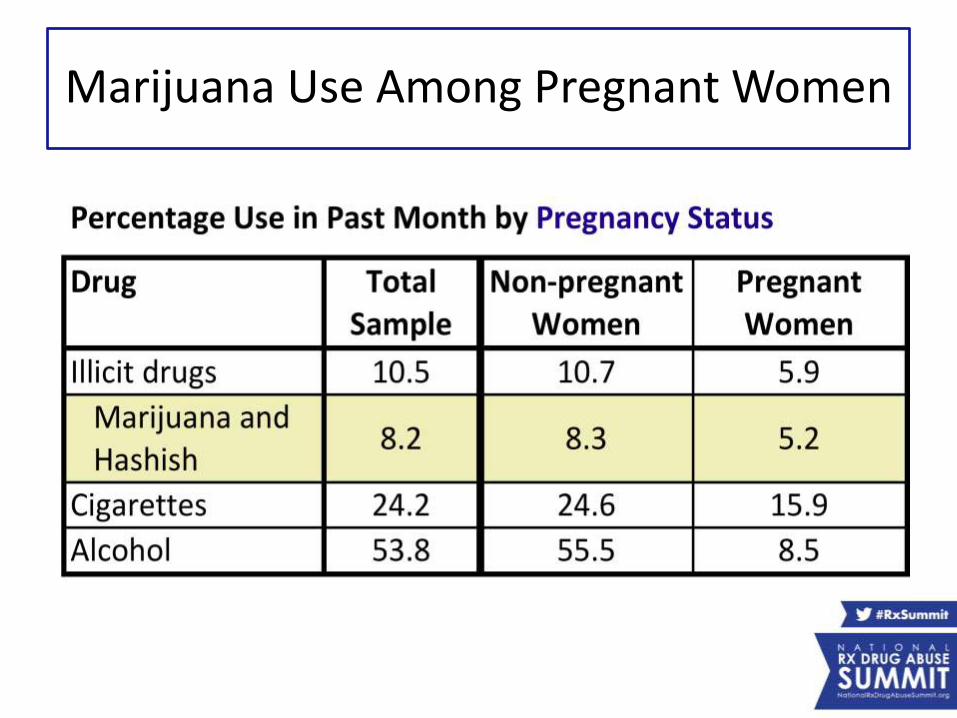
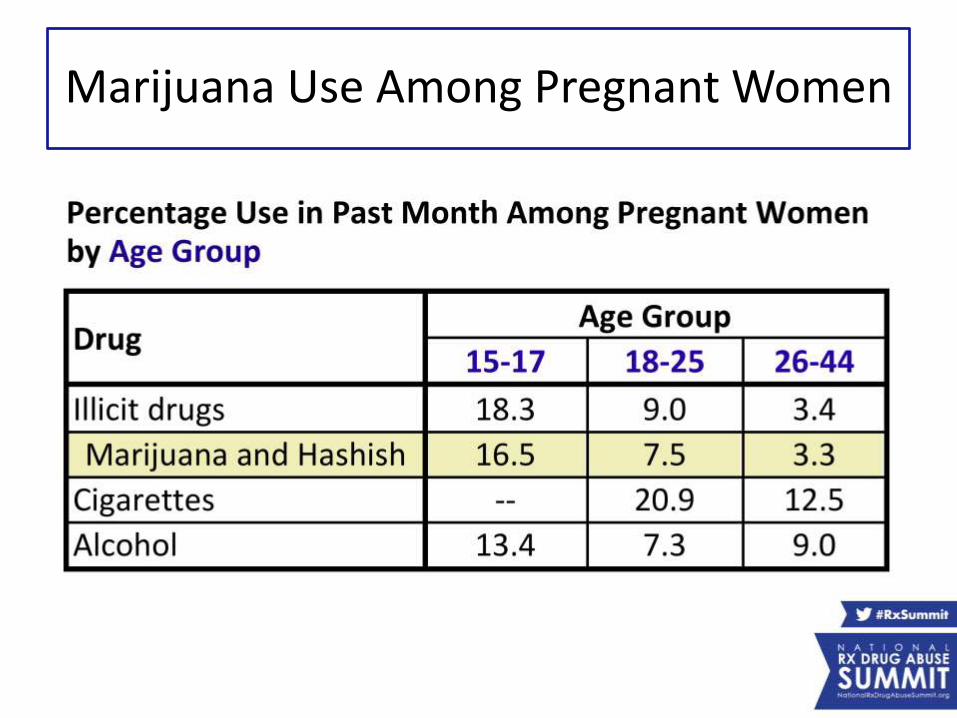
Marijuana Use Among Pregnant Women
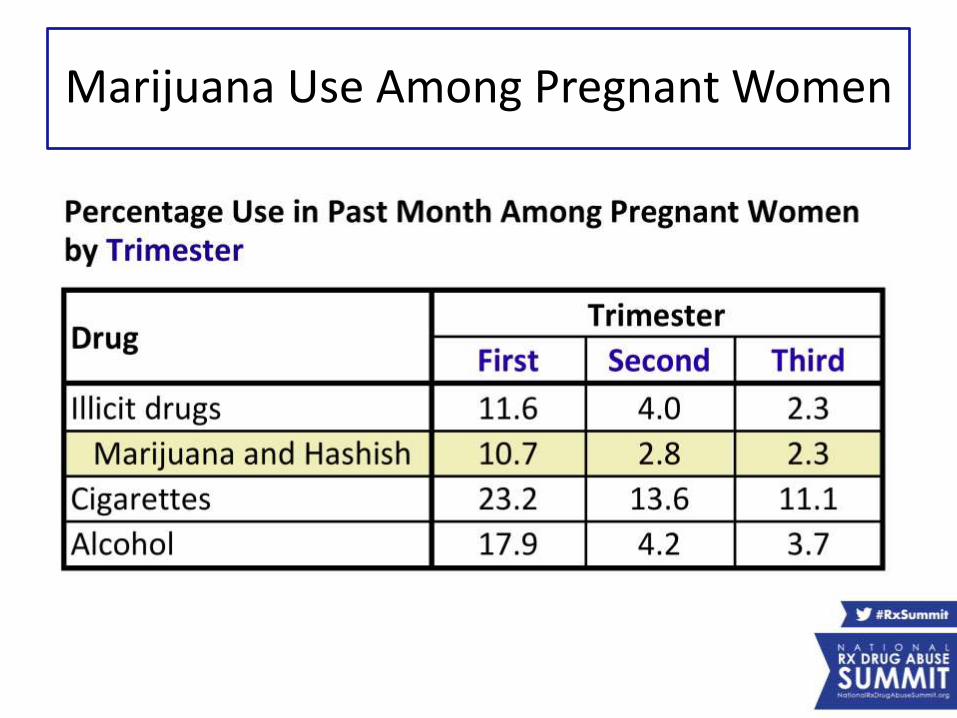
Marijuana Use Among Pregnant Women
Marijuana Use Among Pregnant Women
Epidemiology: Bottom Line #1
Teratogen = causes birth defects
• Cigarettes are the most commonly used teratogen (15.9%)
• Alcohol is 2nd most commonly used teratogen (8.5%)
• While marijuana is the commonly used illicit drug, it is not the most common teratogen.
Epidemiology: Bottom Line #2
• Young adolescents (ages 15 to 17) have the highest rate of marijuana use during pregnancy (16.5%)
• Marijuana use is highest (10.7%) during the first trimester then declines significantly.
• Use rebounds quickly after delivery.
Who Uses Illicit Drugs During Pregnancy?
• Pre-pregnancy BMI is underweight
• No folic acid supplementation
• Alcohol use
• Cigarette smoking
• Partners are drug users
• Intimate partner violence
• Lower levels of education
• Lower levels of income
• Higher rates of unemployment
Common Factors
Who Uses Marijuana During Pregnancy?
• Excessive weight gain during pregnancy
• More likely to be nulliparous (no other children)
• More likely to have had an induce abortion in the past
Possible Unique Factors*
Data from a population-based study using the National Birth Defects Prevention Study with a small sample (n = 189).
Part 3
Issues Related to Marijuana Use During Pregnancy
Recommendations
American Society of Addiction Medicine
• Prenatal education about all drugs for all pregnant women
• Universal screening to identify “at risk” women including repeated follow-up assessments
• Culturally competence public prevention programs to educate the public about realistic dangers of drug use in pregnancy
• Education of health care providers in the care and managements of women with evidence of drug use before, during, and after pregnancy
• Women who are pregnant should receive priority admission to substance treatment facilities.
Recommendations
American Society of Addiction Medicine
• Prenatal education about all drugs for all pregnant women
• Universal screening to identify “at risk” women including repeated follow-up assessments
• Culturally competence public prevention programs to educate the public about realistic dangers of drug use in pregnancy
• Education of health care providers in the care and managements of women with evidence of drug use before, during, and after pregnancy
• Women who are pregnant should receive priority admission to substance treatment facilities.
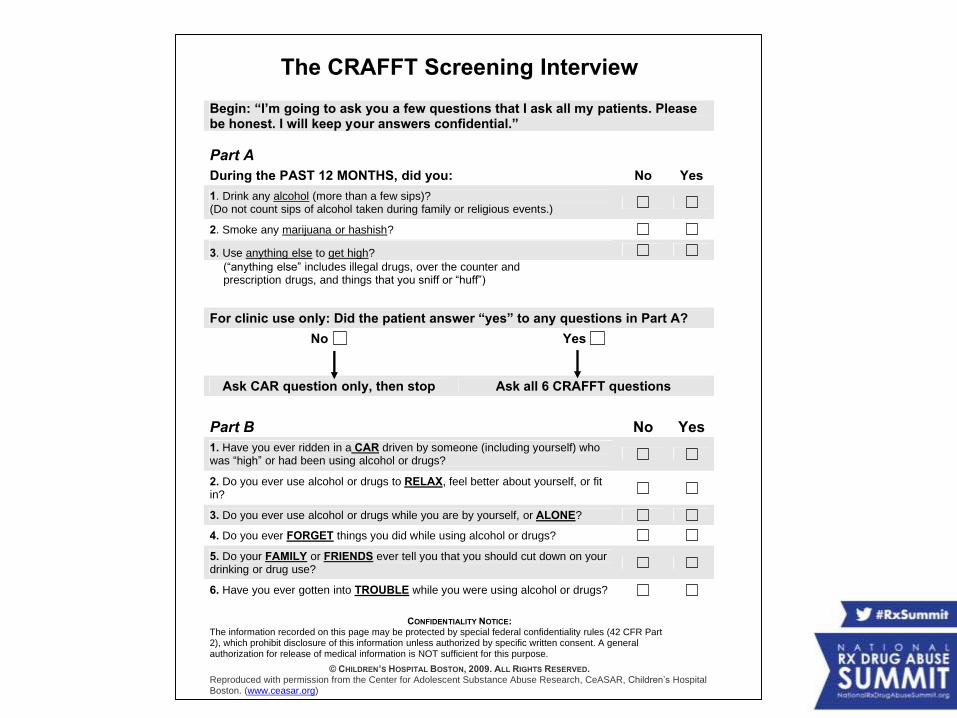
The CRAFFT Screening Interview
Begin: “I’m going to ask you a few questions that I ask all my patients. Please be honest. I will keep your answers confidential.”
Part A
During the PAST 12 MONTHS, did you: No Yes
1. Drink any alcohol (more than a few sips)? (Do not count sips of alcohol taken during family or religious events.)
2. Smoke any marijuana or hashish?
3. Use anything else to get high?
(“anything else” includes illegal drugs, over the counter and prescription drugs, and things that you sniff or “huff”)
For clinic use only: Did the patient answer “yes” to any questions in Part A?
No Yes
Ask CAR question only, then stop Ask all 6 CRAFFT questions
Part B No Yes
1. Have you ever ridden in a CAR driven by someone (including yourself) who was “high” or had been using alcohol or drugs?
2. Do you ever use alcohol or drugs to RELAX, feel better about yourself, or fit in?
3. Do you ever use alcohol or drugs while you are by yourself, or ALONE?
4. Do you ever FORGET things you did while using alcohol or drugs?
5. Do your FAMILY or FRIENDS ever tell you that you should cut down on your drinking or drug use?
6. Have you ever gotten into TROUBLE while you were using alcohol or drugs?
CONFIDENTIALITY NOTICE: The information recorded on this page may be protected by special federal confidentiality rules (42 CFR Part 2), which prohibit disclosure of this information unless authorized by specific written consent. A general authorization for release of medical information is NOT sufficient for this purpose.
© CHILDREN’S HOSPITAL BOSTON, 2009. ALL RIGHTS RESERVED. Reproduced with permission from the Center for Adolescent Substance Abuse Research, CeASAR, Children’s Hospital Boston. (www.ceasar.org)
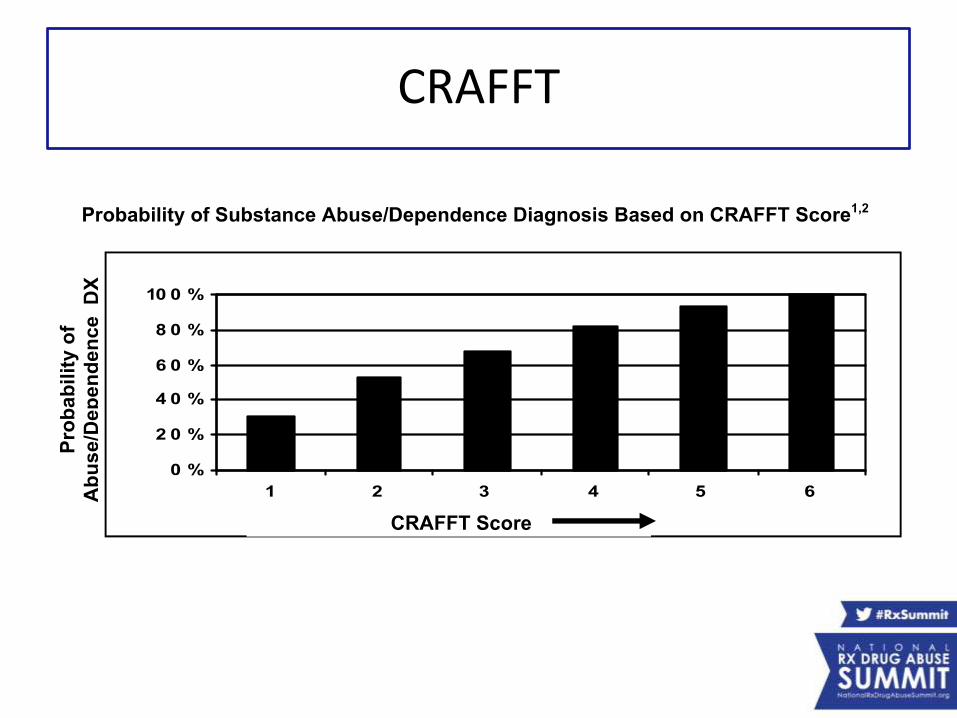
CRAFFT
Part 4
The Developmental Effects of Prenatal Marijuana Exposure
Longitudinal Studies
1. The Ottawa Prenatal Prospective Study (OPPS) began in 1978 and enrolled a predominantly middle-class, low-risk, Caucasian sample from Ottawa, Canada
2. The Maternal Health Practice and Child Development Study (MHPCD) started in 1982 and enrolled a high-risk, low socioeconomic status mixed Caucasian and African-American sample from Pittsburgh, Pennsylvania
Longitudinal Studies
3. The Generation R study started in 2010 and recruited a multi-ethnic population-based cohort in Rotterdam, The Netherlands
Difficult Research
• It is difficult to ascertain developmental effects that are specific to prenatal marijuana exposure.
• Why? Most pregnant women who use marijuana also smoke cigarettes and/or drink alcohol.
• Researchers are actually assessing the effects related to polysubstance exposure.
Possible Pregnancy-Related Effects of Prenatal Marijuana Use
• Decreased male fertility
• Decreased ovulation
• Altered hormones– Prolactin, follicle-stimulating hormone, luteinizing
hormone, and estrogen
• Altered oviductal transport, embryo implantation, and maintenance of pregnancy
Possible Pregnancy-Related Effects of Prenatal Marijuana Use
• Altered placental blood flow
• Intrauterine growth restriction
• Decreased gestational age
• Decreased birth weight
Neonatal Period
• No neonatal withdrawal syndrome identified
• Neurobehavior – no consistent results during first week of life
Minimal or No Effects on Child Development
• Minimal, inconsistent effect on general cognition
• Altered sleep patterns
• No effect on language
• Minimal effect on motor development
• Minimal effects on growth and pubertal development
Consistent Negative Effects on Child Development
• Poorer executive functioning skills and attention (ages 3 to 16)
– Attention, impulsivity, problem-solving, reasoning
• Increased conduct and behavior problems (ages 6 to 21)
– Greater risk of initiating cigarette smoking and marijuana use during adolescence
Key Points
• Pro-marijuana advocacy may result in an increase in the prevalence of marijuana use during pregnancy.
• Today’s marijuana is 6- to 7-times more potent than it just 20 years ago.
• Average marijuana consumption may be higher owing to the growing popularity of blunts compared to joints and pipes.
In the absence of strong public health messagesand the growing pro-marijuana movement,
marijuana use among pregnant women could increase in coming years.
This may be particularly true among young adolescents who already report the highest use
among all pregnant women.
Key Points
We Need to Get the Word Out
To date, the documented effects of prenatal marijuana exposure on fetal outcomes and child
development have been minimal.
However, given the increased potency and average use, the consequences of marijuana use
among pregnant women could be more significant and serious than in past decades.
Key Points
Key Points
• Intersecting political forces and medical issues mandate that physicians:
– Be knowledgeable about marijuana use by their patients and
– Be prepared to counsel their patients about the effects of prenatal marijuana use on fertility, pregnancy, and exposed offspring
• Kay, I created the following 2 slides based on the key points from our paper. I decided to simply the messages into the 3 “Key Points” slides. Keep or delete these – your choice!
Key Points
• Adverse fetal outcomes related to maternal marijuana use remain unclear.
• Associations have been found with:
– Infertility
– Placental complications
– Fetal growth restriction
Key Points
• Long-term effects of prenatal marijuana use on exposed offspring are difficult to ascertain because polysubstance abuse is the norm (cigarettes and alcohol).
Clinical Track:Maternal-Fetal Issues
for Physicians
Presenters:
• Scott L. Wexelblatt, MD, Regional Medical Director for Newborn Services, Cincinnati Children’s Hospital Medical Center
• Susan Ford, RN, BSN, BEACON Quality Improvement Coordinator, Ohio Perinatal Quality Collaborative
• Tamara D. Warner, PhD, Research Assistant Professor, Department of Pediatrics, University of Florida
• Kay Roussos-Ross, MD, Director of Women’s Health, UF Shands Medical Plaza
Moderator: Carla S. Saunders, NNP-BC, Advance Practice Coordinator, Pediatrix Medical Group, and Neonatal Nurse Practitioner, East TennesseeChildren’s Hospital, and Member, Rx Summit National Advisory Board