Rx15 tt tues_330_1_babalonis_2barnes
55
Trending Topics Track Marijuana: Emerging Medical and Legal Issues Presenters: • Shanna Babalonis, PhD, Assistant Professor, Department of Behavioral Science and Center on Drug and Alcohol Research, University of Kentucky • Michael C. Barnes, JD, Executive Director, Center for Lawful Access and Abuse Deterrence (CLAAD), and Member, Rx Summit National Advisory Board Moderator: Nancy Hale, President and CEO, Operation UNITE
-
Upload
opunite -
Category
Healthcare
-
view
312 -
download
0
Transcript of Rx15 tt tues_330_1_babalonis_2barnes
Trending Topics Track
Marijuana: Emerging Medicaland Legal Issues
Presenters:• Shanna Babalonis, PhD, Assistant Professor, Department of
Behavioral Science and Center on Drug and Alcohol Research, University of Kentucky
• Michael C. Barnes, JD, Executive Director, Center for Lawful Access and Abuse Deterrence (CLAAD), and Member, Rx Summit National Advisory Board
Moderator: Nancy Hale, President and CEO, Operation UNITE
Disclosures
• Shanna Babalonis, PhD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Michael C. Barnes, JD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Nancy Hale has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont & Associates-
Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition
Learning Objectives
1. Outline key issues in the national debate regarding marijuana.
2. Describe challenges posed by state laws in conflict with federal policy.
3. Explain in detail isolated plant CBs.4. Compare CBs to medical marijuana as
treatment medications.
Cannabinoids: Pharmacology, Treatment Utility and Abuse Liability
Shanna Babalonis, Ph.D.
University of Kentucky
College of Medicine
Department of Behavioral Science
Center on Drug and Alcohol Research
Disclosures
Shanna Babalonis, PhD has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
Outline- Background on cannabinoids
- Discuss cannabidiol and its treatment potential
- Current medications containing cannabinoids
- Marijuana in the United States – increasing potency and changing make-up of cannabinoids
- Multi-site laboratory trial examining cannabidiol as a potential treatment for marijuana abuse
- Conclusions
Phytocannabinoids- There are approximately 500 phytochemicals that naturally occur in the
marijuana plant
- About 70 of these are unique to the marijuana plant and are called cannabinoids or phytocannabinoids
- Present in the plant’s buds (leaves, stalks, seeds)
- There are several classes of plant-derived cannabinoids, including:
- Δ9 tetrahydrocannabinol (THC)
- cannabinol (CBN, CBDL)
- cannabidiol (CBD, CBDV)
- cannabichromenes (CBC)
- cannabigerols (CBG)
- Others: CBL, CBE, CBT
Phytocannabinoids
- There are approximately 500 phytochemicals that naturally occur in the marijuana plant
- Approximately 66 of these are unique to the marijuana plant and are called cannabinoids or phytocannabinoids
- Present in the plant’s buds (leaves, stalks, seeds)
- There are several classes of plant-derived cannabinoids, including:
- Δ9 tetrahydrocannabinol (THC, THCV)
- cannabinol (CBN, CBDL)
- cannabidiol (CBD, CBDV)
- cannabichromenes (CBC)
- cannabigerols (CBG)
- Others: CBL, CBE, CBT
Psychoactive effects
No known psychoactive effects
Endocannabinoids- There are also endogenous cannabinoids produced in the body called
endocannabinoids
- Examples: Anandamide, 2-AG
- Endogenous ligands at the cannabinoid receptor
- Present in both the CNS and periphery
- Involved in regulation of sleep, memory, inflammation, immune function, insulin sensitivity, fat and energy metabolism, reproduction (ovulation, implantation), expressed in breast milk
- Degraded by naturally occurring enzymes: FAAH (fatty acid amide hydrolase), MAGL (monoacylglycerol lipase)
- Isolated/synthesized endocannabinoids – have not administered to humans (exogenously)
- THC and other cannabinoids exert their action through this system
Cannabinoid Receptors
Cannabinoids exert action at cannabinoid receptors: CB1 and CB2
CB1 receptor - the most abundant GPCR receptor in the CNS
- also located in the periphery (GI tract, cardiac tissue, reproductive system, fat tissue, skeletal muscle)
CB2 receptor - primarily located in the periphery, regulation of immune
function; GI tract
- also present in the brain; less abundant than CB1
Evidence that additional cannabinoid receptors exist (e.g., GPR55)
% o
f M
axim
al E
ffect
100
50
0
Log (Drug)
100
% o
f M
axim
al E
ffec
t
50
0
Log (Drug)
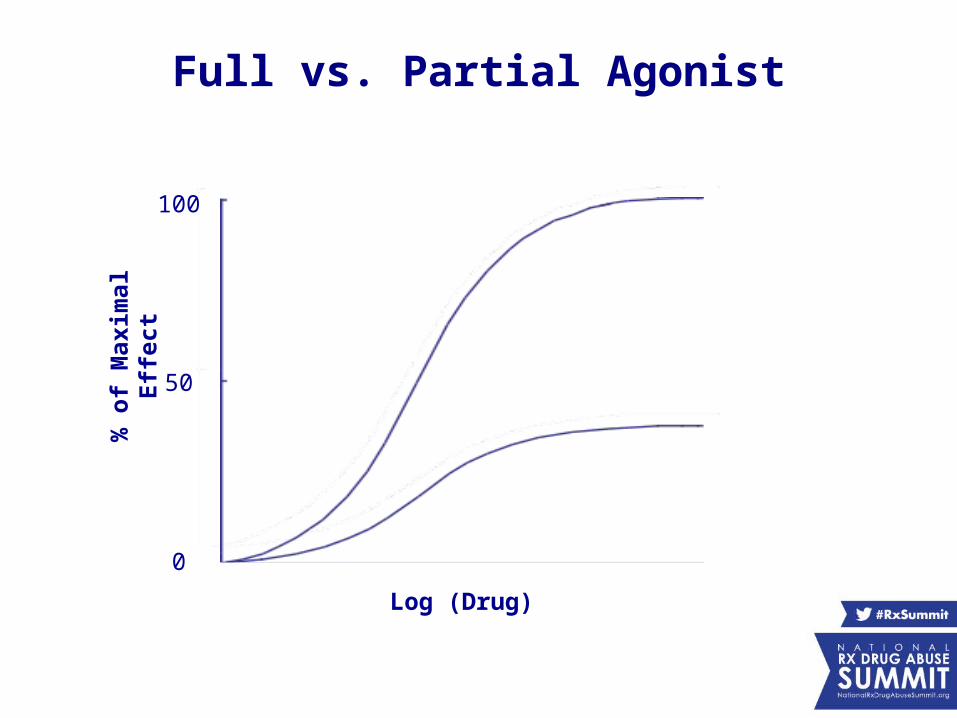
Full vs. Partial Agonist
Cannabinoid Receptor Agonists
Phytocannabinoids
THC - high affinity, partial agonist at CB1
also exerts some partial agonist effects at CB2
Endocannabinoids
Anandamide - moderate affinity, full or partial agonists at CB1
- partial agonist at CB2
2-AG - full agonist at CB1 and CB2
Synthetic Cannabinoid Chemicals (K2, Spice)JWH compounds - not part of the marijuana plant – do not occur in nature
- synthetic, lab-made chemicals
- very high affinity, full agonist at CB1 and/or CB2
Cannabidiol (CBD)
- Cannabidiol is present in the marijuana plant in varying levels (depending on the strain) and upon smoking, is absorbed into the lungs, entering the blood and brain
- It is speculated to be a non-psychoactive component of marijuana
- Its mechanism of action is not completely clear
- There is little to no direct activity at CB1 and CB2 receptors; indirect effects on cannabinoid receptors
- Increases availability of endocannabinoids through two mechanisms:
- inhibit uptake of endocannabinoids
- inhibit FAAH and MAGL (enzymes that degrade
endocannabinoids)
CBD: Additional Mechanisms
In cellular preparations and/or animal models CBD has displayed the following effects:
- Potent antioxidant, anti-inflammatory and neuroprotectant - antioxidant effects ≥ vitamin C and E in cellular models
- Analgesic (antinociception, antihyperalgesia)
- thought to be mediated through action at glycine and transient receptor potential
channels (TRPs): TRPV1, TRPV2, TRPA1, TRPM8
- endocannabinoid effects may also contribute to analgesia
- Anticonvulsant (several animal models of seizure) - does not appear to be mediated by activity of endocannabinoids
- Other activity:
- acts as serotonin (5HT1A) agonist (antidepressant, antiemetic, anxiolytic,
anti- cataleptic; may contribute to anticonvulsant effects)- modulates adenosine A2A signaling (also anti-inflammatory)
Cannabidiol: Potential Treatment?
Trials (listed on ClinicalTrials.gov) that are being conducted to determine CBD effects for the treatment of:
Schizophrenia (hypothesis: increases in anandamide decrease symptoms) Solid TumorsGVHD (Graft versus host disease) (anti-inflammatory, immunosuppressive) Fatty Liver Disease Crohn’s Disease, Inflammatory Bowel Disease, Ulcerative ColitisTreatment for Marijuana DependenceOpioid Craving/Relapse Seizure Disorder
CBD/THC Trials
Trials are being conducted to determine CBD/THC combination for the treatment of:
Cancer Pain, Intractable Cancer PainHead and Neck Squamous Cell CarcinomaPostoperative Pain, Anxiety, Nausea/VomitingNeuroprotection in Huntington’s DiseaseCognitive Dysfunction in Schizophrenia Bipolar DisorderADHDMucositis Marijuana DependenceGlioblastomaSpasticity in children with Cerebral PalsyMultiple Sclerosis – spasticity, neuropathic pain, detrusor overactivity
Cannabinoids: Also Schedule I Drugs
All marijuana plant material, oils and resins are currently Schedule I under the US Controlled Substances Act.
Schedule I includes non-pharmaceutical cannabidiol oil and plants with high CBD content.
Medications containing cannabinoids need to be reviewed by the FDA (e.g., safety, abuse liability). There are two examples of cannabinoid based drugs that have gone through this process in the United States:
Marinol (dronabinol) = Schedule III
Cesamet (nabilone) = Schedule II
Pharmaceutical Products Containing Cannabinoids
Marinol® (dronabinol) - oral medication - synthetic THC- marketed for the treatment nausea/vomiting (chemotherapy); appetite stimulant (AIDS)- available in 2.5, 5 or 10 mg capsules
Cesamet® (nabilone)- oral medication- analog of dronabinol- marketed for the treatment of nausea/vomiting (chemotherapy)- available in 1 mg capsules
Products Under Development, NOT FDA-Approved
Sativex® (1:1 ratio of CBD:THC)- buccal spray- approved in several European countries and Canada for MS - clinical trials being conducted for US approval for cancer pain- 2.7 mg THC, 2.5 mg CBD per spray - patients titrate up to about 10-15 sprays/day
Epidiolex® (cannabidiol)- oral solution (bottle of liquid with syringe dropper)
- CBD-only (98% CBD, trace cannabinoids, no THC)- treatment INDs have been issued for pediatric seizure disorder, sites are currently treating patients- doses: 25 mg/mL and 100 mg/mL (doses up to ~1000 mg/day are being tested)
-Both products are products manufactured by GW Pharmaceuticals
Arvisol - controlled release cannabidiol - Phase I trials for schizophrenia - Echo Pharmaceuticals, Netherlands
CBDV (cannabidivarin – analog of CBD) - CBDV only - Phase I trial for epilepsy scheduled to start in United Kingdom
THCV - thought to be psychoactive, although this has not been clearly demonstrated
- in trials for obesity/metabolic syndrome (opposite effect of THC?)
Other cannabinoids and different combinations of cannabinoids are also under development for various indications
Products Under Development, NOT FDA-Approved

CBD: Phase II, Phase III
Cancer Pain - Phase III trials in progress with Sativex® (THC/CBD)
- most recent Phase III trial did not demonstrate
efficacy
Multiple Sclerosis - Sativex® (THC/CBD) approved in several European countries,
Australia and Canada
- Phase III U.S. Trials are planned
Neuropathic Pain - Phase II trials in progress
Cannabidiol – Seizure Disorder- To date there have been no controlled clinical trials that demonstrate its
efficacy; however, trials are currently underway
- Being explored primarily for the treatment for intractable seizure disorders (i.e., Dravet Syndrome, Lennox Gastaut)
- Preliminary data from GW Pharmaceuticals from their open-label study of (Epidiolex) indicate that only a small sub-set of pediatric seizure patients have complete remission
- Physicians in Colorado (patients taking non-pharmaceutical CBD) report similar findings; also report that CBD appears to worsen symptoms in a sub-set of patients
- Non-pharmaceutical oils prepared from strains of marijuana with very high CBD content and low THC content (e.g., Charlotte's Web):- may contain contaminates- may not contain CBD- may be prepared under less-than-sterile conditions- purity is unknown
Whole Plant Marijuana: Potential as Medicine?
– May be a less-than-ideal medicine due to: – Schedule I status – Most commonly combusted and inhaled (e.g., exposure to carcinogens)– Abuse liability – Not all cannabinoids in the plant are beneficial– Examples: THC is not safe for all populations (e.g., seizure disorder, mental
illnesses) – No assurances of potency, cannabinoid content
- Advocates frequently cite the “entourage effect” – cannabinoids can enhance the effects of other cannabinoids (e.g., mutually synergistic)- However, the proper ratios of cannabinoids have not been determined - This effect could be potentially replicated with pharmaceutical cannabinoids
that have been thoroughly tested
THC Content Increasing High THC content marijuana is now widely available in street marijuana, medicinal marijuana and legalized recreational marijuana
Mean THC content of marijuana in the US:
1970s: 1 - 2 %
1990s: 3 - 4%
2010s: 10 - 15%
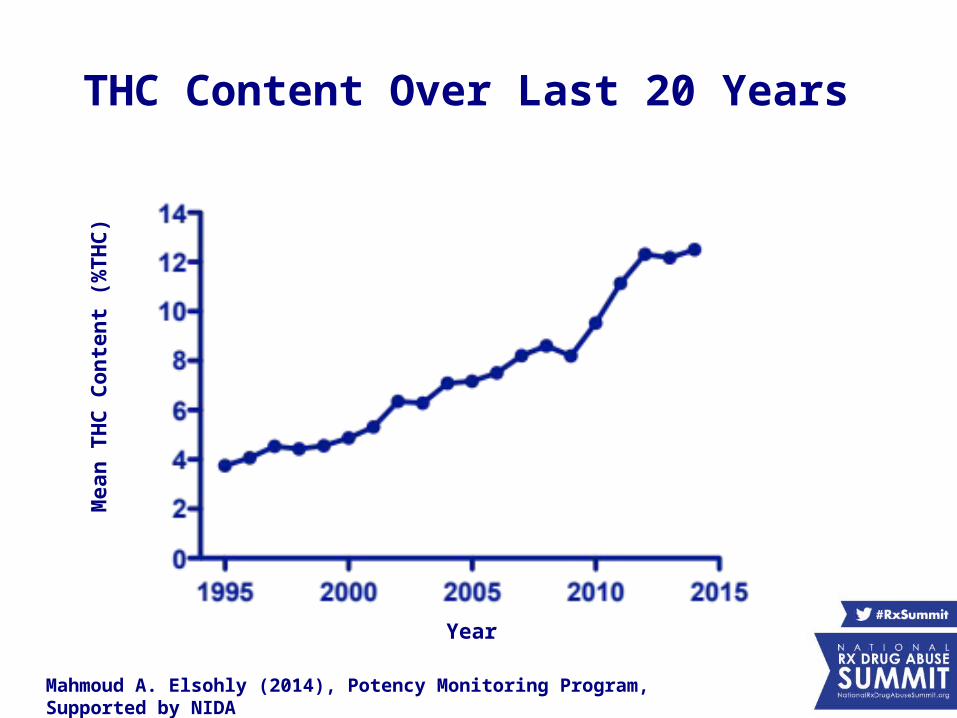
THC Content Over Last 20 Years
Mahmoud A. Elsohly (2014), Potency Monitoring Program, Supported by NIDA
Year
Mea
n T
HC
Co
nte
nt
(%T
HC
)
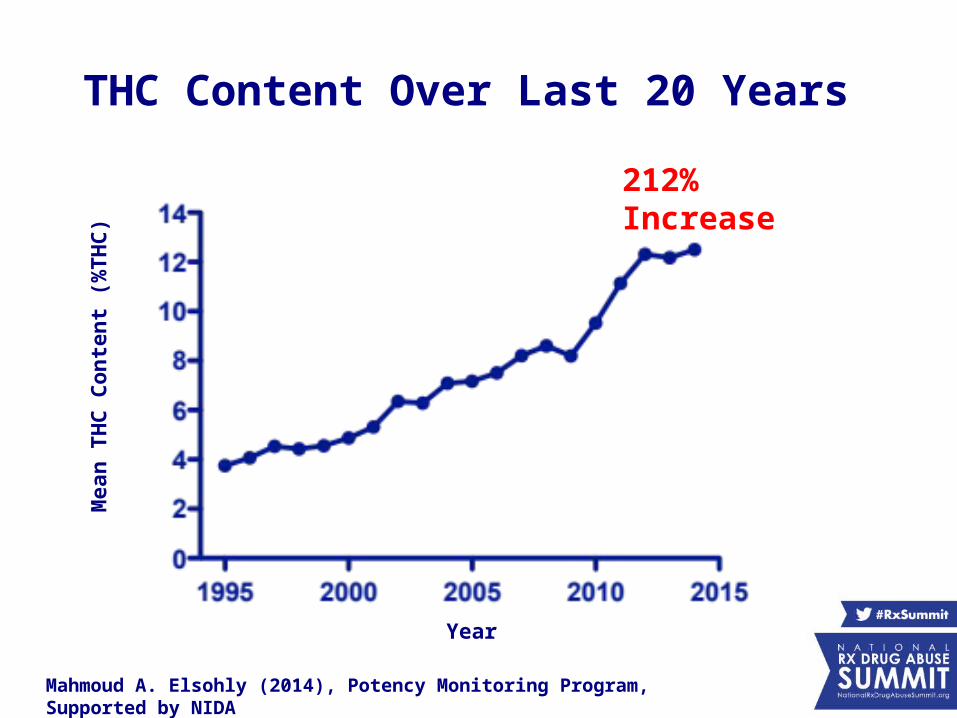
THC Content Over Last 20 Years
Mahmoud A. Elsohly (2014), Potency Monitoring Program, Supported by NIDA
Year
Mea
n T
HC
Co
nte
nt
(%T
HC
)
212% Increase
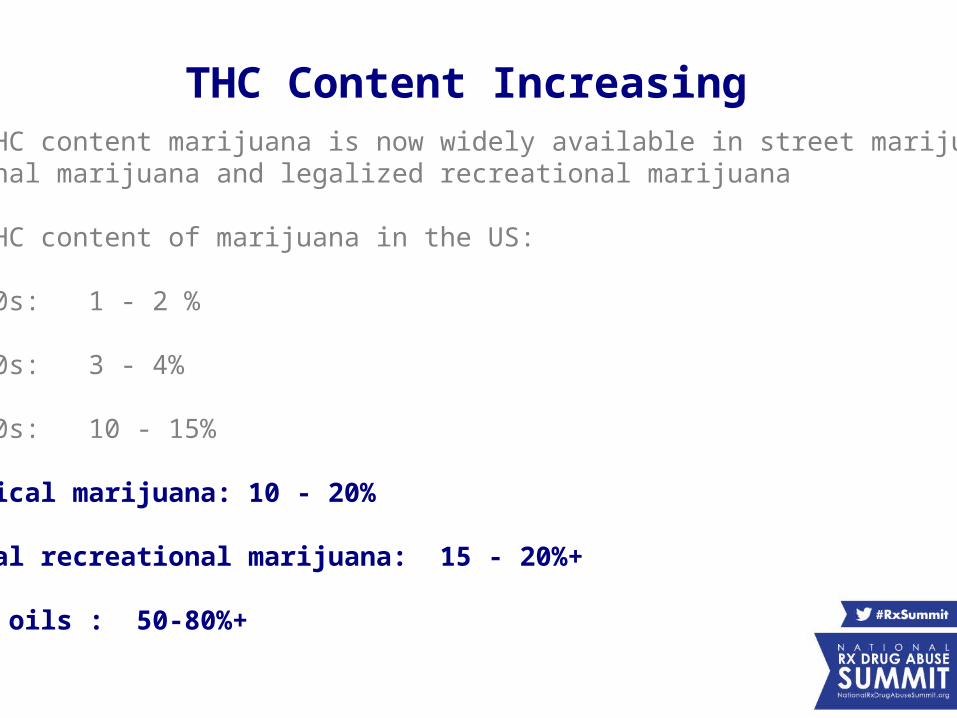
THC Content Increasing High THC content marijuana is now widely available in street marijuana, medicinal marijuana and legalized recreational marijuana
Mean THC content of marijuana in the US:
1970s: 1 - 2 %
1990s: 3 - 4%
2010s: 10 - 15%
Medical marijuana: 10 - 20%
Legal recreational marijuana: 15 - 20%+
THC oils : 50-80%+
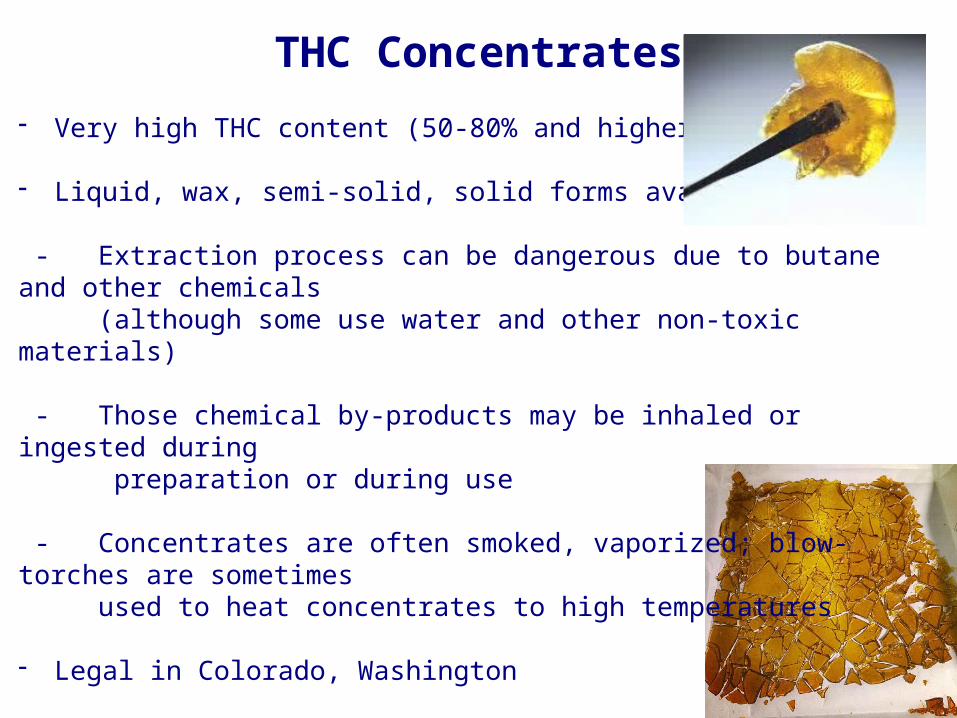
THC Concentrates
- Very high THC content (50-80% and higher)
- Liquid, wax, semi-solid, solid forms available
- Extraction process can be dangerous due to butane and other chemicals (although some use water and other non-toxic materials)
- Those chemical by-products may be inhaled or ingested during preparation or during use
- Concentrates are often smoked, vaporized; blow-torches are sometimes used to heat concentrates to high temperatures
- Legal in Colorado, Washington
- Terms: shatter, dabbing/dabs, oils, wax, butter
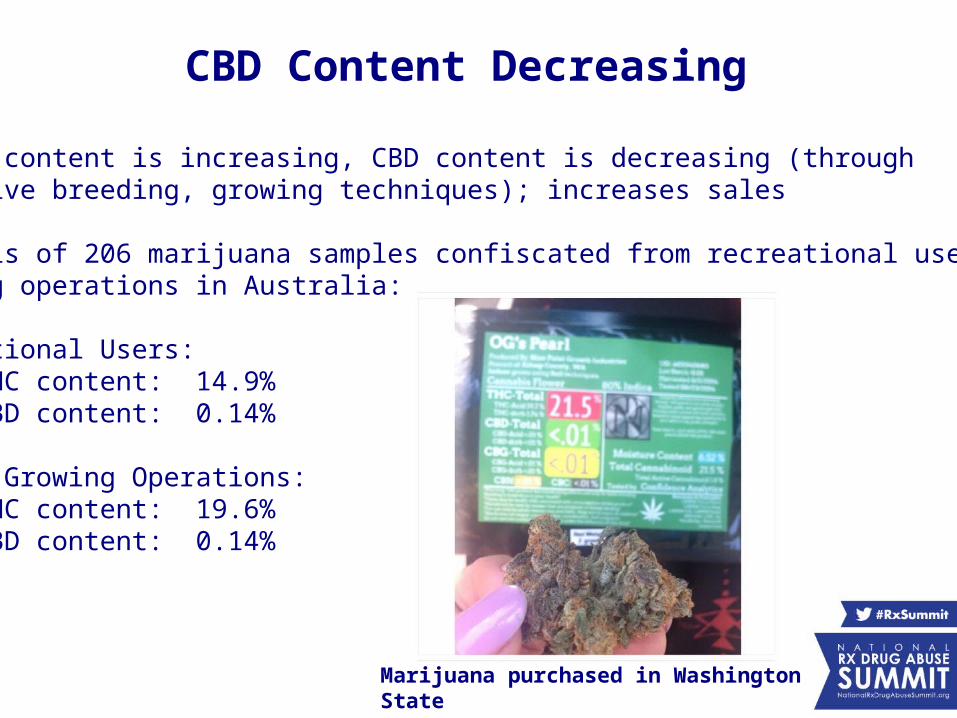
CBD Content Decreasing
As THC content is increasing, CBD content is decreasing (through selective breeding, growing techniques); increases sales
Analysis of 206 marijuana samples confiscated from recreational users and growing operations in Australia:
Recreational Users: Mean THC content: 14.9%Mean CBD content: 0.14%
Indoor Growing Operations: Mean THC content: 19.6%Mean CBD content: 0.14%
Marijuana purchased in Washington State
CBD Reduces Risk of THC?
There are a few reports that indicate CBD reduces the high and psychoactive effects of marijuana; reduces anxiety/paranoia
However, this evidence is relatively weak:
- Animal studies have provided mixed results - A few human studies that have suggested that CBD can decrease the
euphoric, anxiogenic and motor impairing effects of marijuana
- case studies or using non-standardized measurements
- Several small correlational studies have associated high THC, low CBD marijuana with increased anxiety and a younger age of
onset of first psychotic episode
Multisite Trial: Cannabidiol Effects on Smoked Marijuana
- The National Institute on Drug Abuse (NIDA) funded a 3-site trial that examined oral CBD alone and in combination with smoked marijuana
- Conducted to determine if CBD decreases the abuse liability of smoked marijuana and assess CBD as a potential treatment for marijuana abuse and dependence
- Sites included: University of Kentucky, Columbia University, Medical University of South Carolina
- Recently completed, 31 participants
Methods
Participants - healthy adults, ages 18 – 50 - frequent marijuana smokers (4x per week)
- not seeking treatment for marijuana use
Study Design - 8 week outpatient study - 1 session per week (due to
CBD half-life)
Drugs - oral cannabidiol: 0, 200, 400, 800 mg- smoked marijuana: 0, 5.6% THC (half of a marijuana cigarette)
- each dose combination tested once
- CBD administered 90 minutes prior to marijuana
MethodsMeasures
Subjective, physiological, psychomotor, and cognitive assessments were collected at regular intervals (7.5 hrs)
Drug self-administration, measures reinforcing effect of a drug
- participants forego a portion of their study earnings
to smoke additional puffs (50 cents/puff)
- opportunity to smoke up to 3 additional puffs
- 2.5 hrs after sampling marijuana
Study Objectives
1) Assess the safety and abuse liability of oral CBD alone
2) Determine CBD effects on the reinforcing, subjective, cognitive, and physiological effects of smoked marijuana
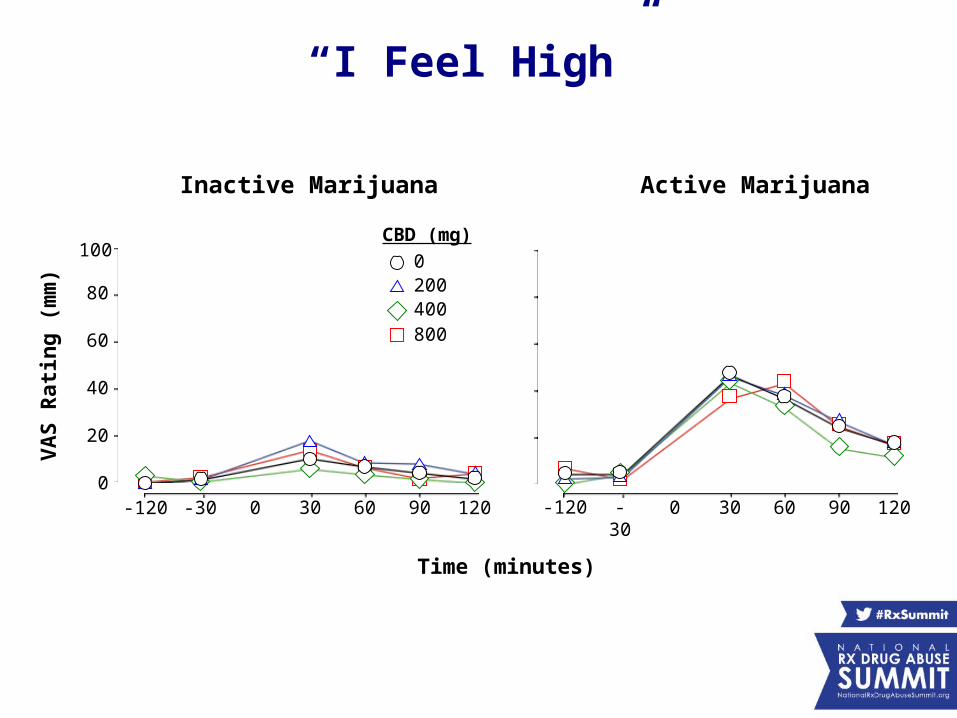
“I Feel High”
0
20
40
60
80
100
VA
S R
atin
g (
mm
)
0 60 12030 90 0 60 12030 90-30 -30-120-120
Time (minutes)
0200400
CBD (mg)
800
Inactive Marijuana Active Marijuana
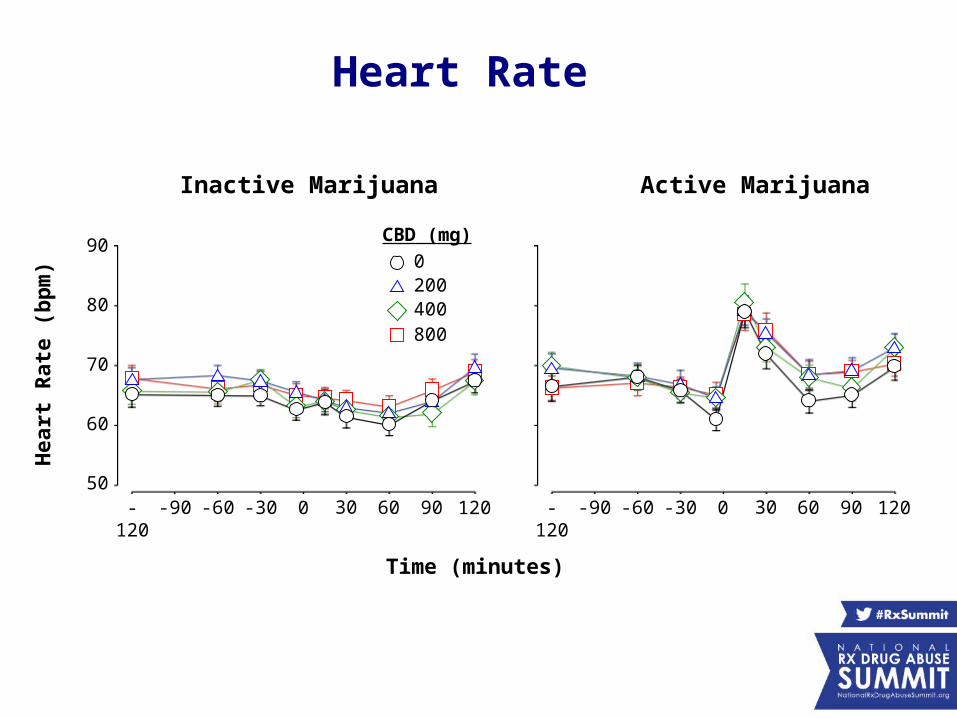
Heart Rate
-120 0 120-60 60
0200400
CBD (mg)
800
-30-90 30 90 -120 0 120-60 60-30-90 30 90
Inactive Marijuana Active Marijuana
Hea
rt R
ate
(bp
m)
50
60
70
80
90
Time (minutes)
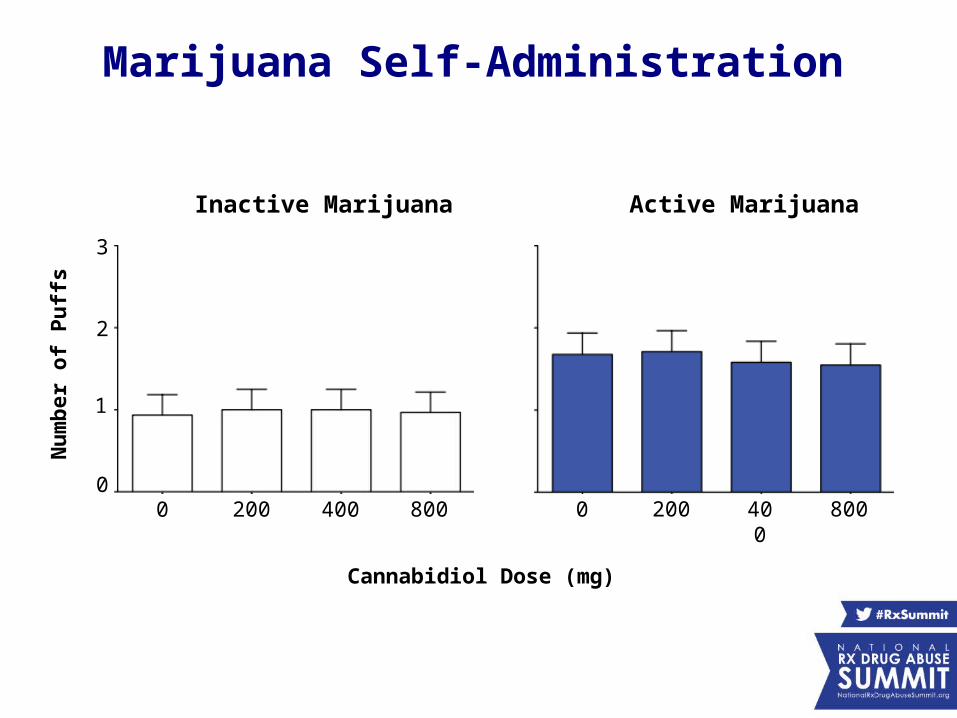
Marijuana Self-Administration
0
1
2
3
Nu
mb
er o
f P
uff
s
0 400200 800 0 400200 800
Inactive Marijuana Active Marijuana
Cannabidiol Dose (mg)
- Oral CBD was safely tolerated in a population of frequent marijuana smokers (≤ 800 mg)
- CBD was placebo-like on all measures tested and there was no signal for CBD to decrease marijuana subjective effects or physiological
effects (no change in marijuana-induced increases in heart rate)
- CBD did not display abuse liability in this population and did not alter the abuse liability of smoked marijuana
- In this acute interaction study, there was no signal for CBD as a treatment for marijuana abuse
Study Conclusions
Summary
- There is preclinical evidence indicating that cannabidiol acts as an antioxidant, anti-inflammatory, analgesic, neuroprotectant and anticonvulsive; however, there have been no controlled trials demonstrating efficacy in humans
- Clinical trials are underway for numerous indications; treatment INDs have been issued for pharmaceutical-grade cannabidiol oil for the treatment of pediatric seizure disorders
- Whole plant marijuana does not appear to be an ideal medication (not all cannabinoids are beneficial for every condition, high THC content); several new cannabinoid-based medications are in development and under testing
Summary
- THC content in marijuana is increasing (12 fold+ increase since 1970s); however, it does not appear that CBD, even at relatively high doses, decreases the positive or aversive drug effects of marijuana
- The long term safety of cannabidiol has not been established; given that cannabinoid receptors/endocannabinoids are ubiquitous in the brain and periphery (particularly in cardiac tissue, reproductive system, GI tract), requires careful examination
Marijuana: Emerging Medical and Legal Issues
Michael C. BarnesApril 7, 2015
Conflict of Interest DisclosureThe Center for Lawful Access and Abuse Deterrence (CLAAD) receives funding
from businesses in the health care industry that share CLAAD’s mission to reduce prescription drug fraud, diversion, misuse, and abuse while advancing consumer access to high-quality health care. CLAAD’s funders include pharmaceutical companies, treatment centers, and laboratories, and are disclosed on its website, www.claad.org.
CLAAD is managed by DCBA Law & Policy. DCBA also provides legal and policy counsel to professionals and businesses whose activities align with CLAAD’s mission. To avoid conflicts of interest, DCBA adheres to the District of Columbia Rules of Professional Conduct §§ 1.7-1.9.
Preview
• Legal Status of Marijuana• Federal Supremacy• Concerns Related to the Current System• Federal Drug Authority• Broader Implications• Where To Go From Here• Issues on the Horizon
Legal Status of Marijuana
• WA, CO, OR, AK, and DC have legalized marijuana.
• Ballot initiatives in 2016: AZ, CA, MA, ME, NV.• 23 States and DC have legalized marijuana for
medicinal purposes. (National Conference of State Legislatures)
• Clear trend toward legalization.
Legal Status of Marijuana
• Under Federal law, marijuana is illegal.– CSA: Schedule I; “no accepted medical use.”
• Current Congress is divided, but support is increasing.– Support: Harry Reid (D), Nancy Pelosi (D), Rand Paul
(R).– Oppose: Mitch McConnell (R), John Boehner (R).– A bill to bar the DoJ from preventing state
implementation of marijuana laws passed the House in the 113th Congress.
Federal Supremacy• Gonzales v. Raich (2004) – upheld the CSA classification.
– The Interstate Commerce Clause (Art. III, § 8, cl. 3) authorizes Congress to regulate purely intrastate activities that have a substantial effect on interstate commerce.
– Local marijuana cultivation and use affects national supply and demand, so local use is part of the national market.
• 10th Amendment reserves for the States Plenary Police Powers.– Includes legislating for the protection of citizens’ health, safety and welfare.
(The Best of Both Worlds: Applying Federal Commerce and State Police Powers to Reduce Prescription Drug Abuse, 16 Md. J. Health Care L. & Pol’y 271 (2013))
• When in conflict, fed. law prevails (Art. VI, cl. 2). – Complex pre-emption tests. (State Legalization of Recreational Marijuana:
Selected Legal Issues, Congressional Research Service (2014))
Concerns Regarding the Current System
• Who has the final say?– State and federal law conflict; citizens can use marijuana
in accordance with state law but be arrested and prosecuted under federal law.
• DOJ: Marijuana is illegal, but federal enforcement is limited.– Federal enforcement will focus on particularly harmful
categories of sales, such as to minors, or those that benefit criminal enterprise.
– Outside of those “enforcement priorities,” DoJ leaves it to the states.
Federal Drug Authority
• Maine foreign drug importation law.– 2013 Maine law permitted citizens to purchase
drugs from certain foreign countries (not FDA regulated).
– Federal court decision (Feb. 2015).• Federal government regulates foreign commerce.• Maine law is pre-empted by federal law.• Compromised the “tightly regulated structure” set up
by federal law.
State Actions & Implications
• ER Hydrocodone: FDA approved, states pushed back.– Mass. enacted an emergency medication ban that was struck
down.– Ruling: Supremacy Clause gives the FDA ruling more weight
than a contrary state determination. (Zogenix v. Deval Patrick, Civ. Action No. 14-11689-RWZ (D. Mass. 2014))
• Broad undermining of Constitutional rights and federal law.– Even if there are “bigger fish to fry,” selective enforcement is ill-
advised policy. Consider politicized women’s health issues. – Ex: ID, KS, MO and AK passed the 2nd Amendment Preservation
Act, which prohibits state law enforcement officials from enforcing federal gun control laws.
Where To Go From Here
• Political will has changed, and the economics are simple.– As of 2011, 77% of Americans support marijuana for medicinal
purposes (CBS News Poll).– As of 2013, 52% of Americans favor legalizing marijuana use
(Pew Research Center).– As supply increases, use will increase. (Office of National Drug
Control Policy, A Comprehensive Approach: Reducing the Supply of Illegal Drugs, (1999) (“When illegal drugs are readily available, the likelihood increases that they will be abused.”))
• Treatment providers must be prepared.
Where To Go From Here
• Impossible to defy public will.• Unilateral armament in public battles.• How to regulate marijuana? Like alcohol? Like tobacco?• Consider the important issues that are on the horizon.
– A North American Opiate Medication Initiative (NAOMI) study indicates that treating longtime addicts with heroin is a safe and effective treatment for heroin addiction and is more cost-effective than methadone. (Sheryl Ubelacker, Medical Heroin: Study Says Giving Long-Term Addicts the Real Deal More Efficient Than Methadone, Huffington Post, (Mar. 12, 2012))
Issues on the Horizon
“Rather than having them [use heroin] in the back alley, why don’t we attract them into a clinic where they will be in contact with doctors and nurses and counselors, we stabilize them by getting them out of a life of crime.”
– Martin Shechter, Epidemiologist at the University of British Columbia & Study Contributor
Conclusion
• Thanks to Cindy Lackey, Nancy Hale, Karen Kelly, and co-presenters
• Questions and discussion at end of session• Contact
– LinkedIn.com/in/michaelcbarnes– @mcbtweets– www.claad.org– @claad_coalition
• Thank you
Trending Topics Track
Marijuana: Emerging Medicaland Legal Issues
Presenters:• Shanna Babalonis, PhD, Assistant Professor, Department of
Behavioral Science and Center on Drug and Alcohol Research, University of Kentucky
• Michael C. Barnes, JD, Executive Director, Center for Lawful Access and Abuse Deterrence (CLAAD), and Member, Rx Summit National Advisory Board
Moderator: Nancy Hale, President and CEO, Operation UNITE