Pedi Neck Mass Slides 071031

of 116
Transcript of Pedi Neck Mass Slides 071031
-
8/14/2019 Pedi Neck Mass Slides 071031
1/116
Pediatric Neck MassesPediatric Neck Masses
MarkMarkDomanskiDomanski, M.D., M.D.
MichaelMichael UnderbrinkUnderbrink, M.D., M.D.
Dept. of OtolaryngologyDept. of Otolaryngology
University of Texas MedicalUniversity of Texas MedicalBranch, GalvestonBranch, Galveston
October 31October 31stst, 2007, 20071
-
8/14/2019 Pedi Neck Mass Slides 071031
2/116
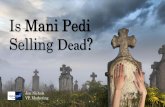
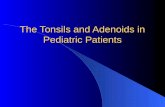
Total % oftotal
Congeital lesions 244 55%Branchial cleft cyst 78 18%
Thyroglossal duct cyst 73 16%Dermoid cyst 43 10%Lymphangioma 34 8%Hemangioma 10 2%Teratoma 2Bronchogenic cyst 2
Thymic cyst 1Myelomeningocele 1
Inflammatory lesions 118 27%
Reactive lympadenopathy 71 16%Undetermined etiology 66 15%
Sinus histiocytosis 5 1%Granulomatous disease 32 7%
Atypical mycobacteria 20 4%Cat scratch disease 6 1%Toxoplasmosis 2Sarcoid 2
Suppurative lympadenitis 10 2%Sialadenitis 5 1%
Non-infammatory benignlesions
23 5%
Inclusion cyst 13 3%Fibromatosis 9 2%Keliod 1
Benign neoplasms 12 3%
Neurofibroma 3 1%
Lipoma 3 1%Lipoblastoma 2Paraganglioma 1Goiter 1Benign mixed tumor 1Osteoblastoma 1
Malignant neoplasms 48 11%
Lymphoma 34 8%Hodgkin's 23 5%Non-Hodkin's 11 2%
Thyroid Carcinoma 6 1%
Rhabdomyosarcoma 2Neuroblastoma 2Fibrous histiocytoma 1Acinic cell carcinoma 1Histiocytosis X 1Chloroma 1
Total 445TorsiglieriTorsiglieri et al., 1988et al., 198822
-
8/14/2019 Pedi Neck Mass Slides 071031
3/116
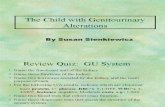
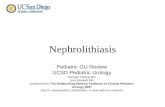
TorsiglieriTorsiglieri et al., 1988et al., 198822
Inflammatory
lesions
27%
Malignant
neoplasms, 11%Benign neoplasms
3%
Non-infammatory
benign lesions
5%
Congenital lesions
54%
N= 445
-
8/14/2019 Pedi Neck Mass Slides 071031
4/116
Initial EvaluationInitial Evaluation
H&PH&P AgeAge
OnsetOnset
Rapidity of growthRapidity of growth Fluctuation in sizeFluctuation in size
PainPain
InfectionInfection TraumaTrauma
TravelTravel
ExposureExposure
PEPE SizeSize
MultiplicityMultiplicity
LateralityLaterality ConsistencyConsistency
ColorColor
MobilityMobility TendernessTenderness
FluctuationFluctuation
Congenital
Inflammatory
Benign
Malignant
-
8/14/2019 Pedi Neck Mass Slides 071031
5/116
Location, Location, Location!Location, Location, Location!
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
6/116
-
8/14/2019 Pedi Neck Mass Slides 071031
7/116
Likely Etiology Determines DirectionLikely Etiology Determines Direction
of Testingof Testing
XX--rayray
U/SU/S
CTCT
MRIMRI
FNAFNA
Surgical BiopsySurgical Biopsy
Tissue CultureTissue Culture
CXRCXR
LabsLabs
PPDPPD Gram stainGram stain
CultureCulture
-
8/14/2019 Pedi Neck Mass Slides 071031
8/116
Pediatric Neck MassesPediatric Neck Masses
1. Congenital lesions1. Congenital lesions 2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions 4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
-
8/14/2019 Pedi Neck Mass Slides 071031
9/116
Pediatric Neck MassesPediatric Neck Masses
1. Congenital lesions1. Congenital lesions 2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions 4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
-
8/14/2019 Pedi Neck Mass Slides 071031
10/116
1. Congenital Lesions1. Congenital Lesions
Branchial cleft cyst 78 18%Thyroglossal duct cyst 73 16%Dermoid cyst 43 10%Lymphangioma 34 8%
Hemangioma 10 2%Teratoma 2Bronchogenic cyst 2
Thymic cyst 1Myelomeningocele 1
-
8/14/2019 Pedi Neck Mass Slides 071031
11/116
EmbryologyEmbryology Ectoderm,Ectoderm,
mesoderm,mesoderm,
endodermendoderm
Incomplete closureIncomplete closure
may result inmay result inbranchial cleftbranchial cleft
anomaliesanomalies
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
12/116
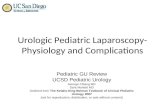
Development of First Four Arches
Nicollas. 20003
Each arch layer gives rise to:
nerve (ectoderm)
artery, muscle and cartilage (mesoderm)
glands (endoderm).
-
8/14/2019 Pedi Neck Mass Slides 071031
13/116
Cyst Sinus Fistula
Schroeder. 20074
Branchial CleftBranchial Cleft AnomaliesAnomalies
-
8/14/2019 Pedi Neck Mass Slides 071031
14/116
Distribution of neck malformations
as cysts, fistulas, or sinusesper Nicollas et. al. (n=191)
Nicollas. 20003
(Sinus)
Total 139 5 47 191
-
8/14/2019 Pedi Neck Mass Slides 071031
15/116Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
16/116
Imagining in Branchial Cleft CystsImagining in Branchial Cleft Cysts
MRIMRI
More reliably confirmsMore reliably confirmscystic naturecystic nature
More precisely definesMore precisely defines
lesionlesion Better to delineateBetter to delineate
glandular tissueglandular tissue
ieie fat planesfat planes
CTCT
Adequate for mostAdequate for mostlesionslesions
Cost, availabilityCost, availability
U/SU/S
cysticcystic vsvs noncysticnoncystic
does not evaluatedoes not evaluateextentextent
Both MRI and CT have difficulty distinguishing branchial
cleft cyst from lymphangioma in children.
BranstetterBranstetter, 20069
-
8/14/2019 Pedi Neck Mass Slides 071031
17/116
11stst
Branchial Cleft Cyst, Type IIBranchial Cleft Cyst, Type II Type IType I
EctodermalEctodermal duplication ofduplication ofEACEAC
Near external auditoryNear external auditory
canalcanal Usually inferior andUsually inferior and
posterior to tragusposterior to tragus
Type IIType II Associated withAssociated with
submandibularsubmandibular glandgland
BranstetterBranstetter, 20069
-
8/14/2019 Pedi Neck Mass Slides 071031
18/116
Type 1 First Branchial Cleft CystType 1 First Branchial Cleft Cyst
Both MRI and CT havedifficulty distinguishingbranchial cleft cyst from
lymphangioma inchildren.
BranstetterBranstetter, 20069
LymphangiomaLymphangioma
mass
auricle
parotid
-
8/14/2019 Pedi Neck Mass Slides 071031
19/116
Branchial CystBranchial Cyst
NoncalcifiedNoncalcified
massmass
CT shows lesionCT shows lesion
under SCMunder SCM
Malik et al 20026
-
8/14/2019 Pedi Neck Mass Slides 071031
20/116
22ndnd Brachial Cleft CystBrachial Cleft Cyst
T2 MRIT2 MRI
Posterior to RPosterior to Rsubmandibularsubmandibularglandgland
Thickened wallsThickened walls
suggest priorsuggest priorhemorrhage orhemorrhage orinfectioninfection
Gujar and Mukherji 20045
-
8/14/2019 Pedi Neck Mass Slides 071031
21/116
Anterior to carotid bifurcationAnterior to carotid bifurcation
Schroeder et al, 20074
-
8/14/2019 Pedi Neck Mass Slides 071031
22/116
Under the anterior SCMUnder the anterior SCM
Schroeder et al, 20074
-
8/14/2019 Pedi Neck Mass Slides 071031
23/116
Exiting skin medial to lateral border of SCMExiting skin medial to lateral border of SCM
Schroeder et al, 20074
-
8/14/2019 Pedi Neck Mass Slides 071031
24/116
Left 2Left 2ndnd
BA FistulaBA Fistula
Anterior to carotid bifurcationAnterior to carotid bifurcation
Under the anterior SCMUnder the anterior SCM
Exiting skin medial to lateral border of SCMExiting skin medial to lateral border of SCM
Schroeder et al, 20074
-
8/14/2019 Pedi Neck Mass Slides 071031
25/116
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
26/116
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
27/116
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
28/116
22ndnd
BA cyst with sinusBA cyst with sinustract extending intotract extending into
the pharynx above thethe pharynx above the
carotid bifurcationcarotid bifurcation
Schroeder et al, 20074
Watch the hypoglossal!
-
8/14/2019 Pedi Neck Mass Slides 071031
29/116
PreauricularPreauricular SinusSinus
Not related to 1Not related to 1stst
branchial cleftbranchial cleft
anomaliesanomalies
Active infectionActive infectionduring excisionduring excision
increases chance ofincreases chance ofrecurrancerecurrance
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
30/116
ThyroglossalThyroglossal Duct CystDuct Cyst persistent tract from thepersistent tract from the
descent of the thyroiddescent of the thyroidfrom the foramenfrom the foramencecumcecum
epithelial liningepithelial lining
composed of eithercomposed of eithersquamoussquamous or respiratoryor respiratoryepitheliumepithelium
confirm normal thyroidconfirm normal thyroidtissuetissue
Learning Radiology.com200711
-
8/14/2019 Pedi Neck Mass Slides 071031
31/116
ThyroglossalThyroglossal Duct CystDuct Cyst CT w/ ContrastCT w/ Contrast
Embedded in theEmbedded in the
strap musclesstrap muscles
Extends deep toExtends deep to
involve the preinvolve the pre--epiglotticepiglottic spacespace
Gujar and Mukherji 20045
-
8/14/2019 Pedi Neck Mass Slides 071031
32/116
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
33/116
Moir. 20048
-
8/14/2019 Pedi Neck Mass Slides 071031
34/116
DermoidDermoid CystsCysts
Ectoderm and mesodermEctoderm and mesoderm 7% of7% ofdermoiddermoid cysts occur in head andcysts occur in head and
neckneck
Thought to be of congenital inclusionThought to be of congenital inclusion
typetype
mean diameter = 1.2 cm (0.6mean diameter = 1.2 cm (0.6--3.3)3.3)
Treatment: complete excisionTreatment: complete excision
Pryor et al 200512
-
8/14/2019 Pedi Neck Mass Slides 071031
35/116
DermoidDermoid CystsCysts Cranial TheoryCranial Theory
GrunwaldGrunwald in 1910in 1910AsAs neuroectodermalneuroectodermal tract recedes,tract recedes, demaldemal
attachementsattachements follow its course and canfollow its course and can
form a sinus or cystform a sinus or cyst
Beware of possible intracranialBeware of possible intracranial
involvementinvolvement
Pryor et al 200512
-
8/14/2019 Pedi Neck Mass Slides 071031
36/116
Orbit is the most common site for dermoids in the head and neck(61%)
Direct excision is sufficient for neck dermoids, more extensiveapproaches (craniotomy, mastoidectomy) are needed for othersites
DiffDiffdxdx: in midline of neck:: in midline of neck: thyroglossalthyroglossal duct cystduct cyst
in head & neck, n = 59
Pryor et al 200512
-
8/14/2019 Pedi Neck Mass Slides 071031
37/116
DermoidDermoid CystsCysts
H & E
CT of dermoid cyst
Pryor et al 200512
-
8/14/2019 Pedi Neck Mass Slides 071031
38/116
TeratomaTeratoma H&N account for ~2% ofH&N account for ~2% of
teratomasteratomas
NewbornNewborn 2.5 yr at2.5 yr at
presentationpresentation All 3 germinal layers presentAll 3 germinal layers present
Mostly benign lesionsMostly benign lesions
amenable to curativeamenable to curative
excisionexcision
WakhluWakhluA et alA et al 200013
-
8/14/2019 Pedi Neck Mass Slides 071031
39/116
TeratomaTeratoma
Prognosis good if noPrognosis good if no
respiratory compromiserespiratory compromise
Usually wellUsually well
differentiated anddifferentiated andrecurrence is uncommonrecurrence is uncommon
Antenatal diagnosis isAntenatal diagnosis isroutine in developedroutine in developed
worldworld
WakhluWakhluA et alA et al 200013
-
8/14/2019 Pedi Neck Mass Slides 071031
40/116
TeratomaTeratoma
Proximity to vitalProximity to vital
structures makes surgerystructures makes surgery
technically demanding.technically demanding.
Evaluate post op thyroidEvaluate post op thyroidand parathyroid function.and parathyroid function.
WakhluWakhluA et alA et al 200013
-
8/14/2019 Pedi Neck Mass Slides 071031
41/116
TeratomaTeratoma 3 germ layers3 germ layers
Arise fromArise from
pluripotentpluripotent
cells andcells and
ectopicectopicembryogenicembryogenic
nonnon--germgermcellscells
WakhluWakhluA et alA et al 200013
-
8/14/2019 Pedi Neck Mass Slides 071031
42/116
TeratomaTeratoma 3 germ layers3 germ layers
WakhluWakhluA et alA et al 200013
-
8/14/2019 Pedi Neck Mass Slides 071031
43/116
TeratomaTeratoma 3 germ layers3 germ layers
WakhluWakhluA et alA et al 200013
-
8/14/2019 Pedi Neck Mass Slides 071031
44/116
HypopharyngealHypopharyngeal TeratomaTeratoma
calcified calcification and fat
Malik et al 20026
T tT t
-
8/14/2019 Pedi Neck Mass Slides 071031
45/116
TeratomaTeratomaT1 MRIT1 MRI
Fatty
Calcified
Gujar and Mukherji 20045
-
8/14/2019 Pedi Neck Mass Slides 071031
46/116
LymphangiomaLymphangioma Benign,Benign, multiloculatedmultiloculated, soft, soft
Posterior neck triangle predominancePosterior neck triangle predominance
MultiMulti--septatedseptated, insinuating lesions, insinuating lesions
Infiltrate and cross tissue planesInfiltrate and cross tissue planes
Most occur by 2 yrs of ageMost occur by 2 yrs of age
Incidence: 1 in 6,000 to 16,000 birthsIncidence: 1 in 6,000 to 16,000 births
BurezqBurezq 200614Head and and Neck Surgery,Head and and Neck Surgery, 200615
-
8/14/2019 Pedi Neck Mass Slides 071031
47/116
Lymphatic Vascular malformationLymphatic Vascular malformation
T1 MRIT1 MRI
High signalHigh signal
representsrepresentsproteinaceousproteinaceousfluidfluid
Crosses tissueCrosses tissueplanesplanes
Gujar and Mukherji 20045
-
8/14/2019 Pedi Neck Mass Slides 071031
48/116
CentrifugalCentrifugal vsvs CentripetalCentripetalCentrifugal theoryCentrifugal theory
the lymphatic system develops asthe lymphatic system develops as mesenchymalmesenchymalspaces that later coalesce into a system ofspaces that later coalesce into a system ofvessels that eventually join the venous system.vessels that eventually join the venous system.
Centripetal theoryCentripetal theory
jugular and posteriorjugular and posterior lymphaticslymphatics form asform asoutgrowths of endothelium from veins into theoutgrowths of endothelium from veins into thesurroundingsurrounding mesenchymemesenchyme..
BurezqBurezq 200614
-
8/14/2019 Pedi Neck Mass Slides 071031
49/116
ClassificationClassificationSize:Size:
MicrocysticMicrocystic: capillary: capillary lymphangiomaslymphangiomas lesions are less than 1 cm in diameterlesions are less than 1 cm in diameter
MacrocysticMacrocystic: cystic: cystic hygromashygromas cysts are larger than 1 cmcysts are larger than 1 cm
CysticCystic hygromashygromas #1 type of#1 type oflymphangiomalymphangioma
Gross et al, 200616
-
8/14/2019 Pedi Neck Mass Slides 071031
50/116
CysticCystic HygromaHygroma
NoncalcifiedNoncalcified
SeptatedSeptated onon
U/SU/S
Malik et al 20026
-
8/14/2019 Pedi Neck Mass Slides 071031
51/116
Cystic CompositionCystic Composition 55--yearyear--old boy withold boy with
lymphangiomalymphangioma
L parotid &L parotid &
parapharyngealparapharyngeal spacespace mixed macromixed macro--
andmicrocysticandmicrocystic typetype
Treated by surgicalTreated by surgicalresectionresection
Gross et al, 200616
Type 1 First Branchial Cleft CystType 1 First Branchial Cleft CystLymphangiomaLymphangioma
-
8/14/2019 Pedi Neck Mass Slides 071031
52/116
Type 1 First Branchial Cleft CystType 1 First Branchial Cleft Cyst
Both MRI and CT havedifficulty distinguishingbranchial cleft cyst from
lymphangioma inchildren.
BranstetterBranstetter, 20069
LymphangiomaLymphangioma
mass
auricle
parotid
BurezqBurezq et al 2006et al 2006
-
8/14/2019 Pedi Neck Mass Slides 071031
53/116
BurezqBurezq et al, 2006et al, 2006(expert opinion)(expert opinion)
1. Error in establishing a communication1. Error in establishing a communication
between the lymphatic and venous systembetween the lymphatic and venous system CysticCystic hygromahygroma
2. Error in morphogenesis of lymphatic system:2. Error in morphogenesis of lymphatic system:
this includes other types of lymphaticthis includes other types of lymphatic
malformationsmalformations microcysticmicrocystic,, macrocysticmacrocystic and mixed lymphatic lesionsand mixed lymphatic lesions
BurezqBurezq 200614
-
8/14/2019 Pedi Neck Mass Slides 071031
54/116
ManagementManagement -- ControversialControversial Spontaneous resolution?Spontaneous resolution?
Formation of new lymphatic channels?Formation of new lymphatic channels?
Serial aspiration?Serial aspiration?
SclerosantSclerosantAgents?Agents? OKOK--432 (432 (lyophiliziedlyophilizied mixture of lowmixture of low--virulence group Avirulence group ASterpSterp
pyogenspyogens
Surgical Excision?Surgical Excision? Is the surgical risk out weigh the benefit in a benign lesionIs the surgical risk out weigh the benefit in a benign lesion
BurezqBurezq 200614
-
8/14/2019 Pedi Neck Mass Slides 071031
55/116
Success with Serial AspirationsSuccess with Serial Aspirations
BurezqBurezq 200614
-
8/14/2019 Pedi Neck Mass Slides 071031
56/116
Success with OKSuccess with OK--432432
Supraclavicular macrocysticlymphangioma
Gross et al, 200616
-
8/14/2019 Pedi Neck Mass Slides 071031
57/116
HemangiomaHemangioma Less than 1/3 present at birthLess than 1/3 present at birth
Usually seen in 1Usually seen in 1stst few months of life andfew months of life and
enlarge progressivelyenlarge progressively
90% cases involutes spontaneously90% cases involutes spontaneously
SclerosingSclerosing agents controversialagents controversial
-
8/14/2019 Pedi Neck Mass Slides 071031
58/116
GlutGlut--11
erythrocyteerythrocyte--type glucose transportertype glucose transporter
found only infound only in microvascularmicrovascular endothelia of bloodendothelia of bloodtissuetissuebarriers such as in the central nervous system, retina,barriers such as in the central nervous system, retina,placenta,placenta, ciliaryciliary muscle, andmuscle, and endoneuriumendoneurium of peripheralof peripheralnervesnerves
HemangiomasHemangiomas stain consistently for Glutstain consistently for Glut--1, in all stages1, in all stagesof development and involution whereas vascularof development and involution whereas vascularmalformations did notmalformations did not
Mo et al, 200617
MacArther, 200618
-
8/14/2019 Pedi Neck Mass Slides 071031
59/116
Pediatric Neck MassesPediatric Neck Masses 1. Congenital lesions1. Congenital lesions
2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions
4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
-
8/14/2019 Pedi Neck Mass Slides 071031
60/116
Pediatric Neck MassesPediatric Neck Masses 1. Congenital lesions1. Congenital lesions
2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions
4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
-
8/14/2019 Pedi Neck Mass Slides 071031
61/116
2. Inflammatory Lesions2. Inflammatory LesionsReactive lympadenopathy 71 16%
Undetermined etiology 66 15%Sinus histiocytosis 5 1%
Granulomatous disease 32 7%Atypical mycobacteria 20 4%
Cat scratch disease 6 1%Toxoplasmosis 2Sarcoid 2
Suppurative lympadenitis 10 2%Sialadenitis 5 1%
When does cervicalWhen does cervical
-
8/14/2019 Pedi Neck Mass Slides 071031
62/116
lymphadenopathylymphadenopathy require FNA?require FNA?
Benign reactive lymph node may persistBenign reactive lymph node may persist
for weeks to monthsfor weeks to months
Lymphoma can present the same wayLymphoma can present the same way
Rapkiewicz et al 200721
-
8/14/2019 Pedi Neck Mass Slides 071031
63/116
To FNA or not to FNA?To FNA or not to FNA? ReactiveReactive lymphadenopathylymphadenopathy the most likelythe most likely
etiology of pediatric neck massesetiology of pediatric neck masses
DiagnosticDiagnostic dilemadilema: a mass that does not: a mass that does notresolve after initial treatmentresolve after initial treatment
Rapkiewicz et al 200721
-
8/14/2019 Pedi Neck Mass Slides 071031
64/116
FNA ancillary studiesFNA ancillary studies Gram stain, cultureGram stain, culture
Acid fast stainAcid fast stain
ImunocytochemistryImunocytochemistry
CytogeneticsCytogenetics
Rapkiewicz et al 200721
Limitations to FNA
-
8/14/2019 Pedi Neck Mass Slides 071031
65/116
Limitations to FNALimitations to FNA
A lesion may not be homogenousA lesion may not be homogenous
FNA samples only part of the massFNA samples only part of the mass
May miss the true lesionMay miss the true lesion
Unable to appreciate histologicalUnable to appreciate histological
architecturearchitecture
Rapkiewicz et al 200721
Time to contemplate open biopsyTime to contemplate open biopsy
-
8/14/2019 Pedi Neck Mass Slides 071031
66/116
Enlarging massEnlarging mass
Poor response to medical treatmentPoor response to medical treatment
Suspicious clinical courseSuspicious clinical course
Unusual image findingsUnusual image findings
Systemic symptomsSystemic symptoms
Rapkiewicz et al 200721
Case F R
-
8/14/2019 Pedi Neck Mass Slides 071031
67/116
CaseCase
F.R.F.R.
88 y/oy/o female,female, hxhx + PPD several yrs prior+ PPD several yrs prior
Presents with R cervicalPresents with R cervical adenopathyadenopathy
FNA suggestsFNA suggests granulomagranuloma
Repeat FNARepeat FNA--> same result> same result
AFB stain and cultures negativeAFB stain and cultures negative
ClarithromycinClarithromycin andand ethambutolethambutol startedstarted
Rapkiewicz et al 200721
Case F R
-
8/14/2019 Pedi Neck Mass Slides 071031
68/116
CaseCase
F.R.F.R.
AdenopathyAdenopathy and pain increasedand pain increased
Third FNA nonThird FNA non--diagnosticdiagnostic
CT shows bulky homogenousCT shows bulky homogenous
lymphadenopathylymphadenopathy of R upper spinalof R upper spinalaccessory and upper jugular chains.accessory and upper jugular chains.
Open biopsy displayedOpen biopsy displayed Hodgkin'sHodgkin'slymphoma.lymphoma.
Rapkiewicz et al 200721
Reactive Lymphadenopathy
-
8/14/2019 Pedi Neck Mass Slides 071031
69/116
ReactiveReactive
LymphadenopathyLymphadenopathy
33--yearyear--old childold child
MultipleMultiple hypoechoichypoechoiclesionslesions
variable shape andvariable shape andsizessizes
consistent withconsistent withreactive lymphreactive lymphnodesnodes
Malik et al 20026
Enlarged Lymph Node
-
8/14/2019 Pedi Neck Mass Slides 071031
70/116
Enlarged Lymph NodeEnlarged Lymph Node
NonspecificNonspecific
Cause:Cause:
cryptococcalcryptococcal
adenitisadenitis
YeastlikeYeastlikefungusfungus
Gujar and Mukherji 20045
AtypicalAtypical mycobacteriamycobacteria: ex:: ex:
-
8/14/2019 Pedi Neck Mass Slides 071031
71/116
cryptococcuscryptococcus
Saprobe inSaprobe in
naturenature
worldwideworldwide
distributiondistribution Found in soilFound in soil
Portal of entryPortal of entryis lungis lung
AtypicalAtypical mycobacteriamycobacteria: ex:: ex:
-
8/14/2019 Pedi Neck Mass Slides 071031
72/116
cryptococcuscryptococcus Associated w/Associated w/
AIDSAIDS organorgan
transplantationtransplantation
LymphoreticularLymphoreticulardiseasesdiseases
pts lackpts lack
apprarentapprarentpredisposingpredisposingfactorsfactors
BartonellaBartonella henselaehenselae
-
8/14/2019 Pedi Neck Mass Slides 071031
73/116
BartonellaBartonella henselaehenselae
HypoechoicHypoechoic massesmasses
with irregular rim ofwith irregular rim ofisoechoicisoechoic tissuetissue
Biopsy: Cat ScratchBiopsy: Cat Scratch
DiseaseDisease
Malik et al 20026
BartonellaBartonella henselaehenselae
-
8/14/2019 Pedi Neck Mass Slides 071031
74/116
BartonellaBartonella henselaehenselae
GramGram coccobacilluscoccobacillus
22-- 14 day incubation14 day incubation
DxDx: requires prolonged: requires prolonged
incubation (2 + weeks)incubation (2 + weeks) Rx: erythromycin 1Rx: erythromycin 1--4 m4 m
(unclear efficacy)(unclear efficacy)
Normally benign courseNormally benign course
Malik et al 20026
In heart valve
PeritonsillarPeritonsillar AbcessAbcess
-
8/14/2019 Pedi Neck Mass Slides 071031
75/116
PeritonsillarPeritonsillarAbcessAbcess
Soft tissue density inSoft tissue density in
submentalsubmental spacespace
Malik et al 20026
RetropharyngealRetropharyngeal
-
8/14/2019 Pedi Neck Mass Slides 071031
76/116
AbscessAbscess Widening ofWidening of
prevertebralprevertebral spacespace
Malik et al 20026
Retropharyngeal Space AbscessRetropharyngeal Space Abscess
-
8/14/2019 Pedi Neck Mass Slides 071031
77/116
et op a y gea Space bscessp y g p
Gujar and Mukherji 20045
-
8/14/2019 Pedi Neck Mass Slides 071031
78/116
RetropharyngealPeritonsillar
Malik et al 20026
SppurativeSppurative Cervical AdenitisCervical Adenitis
-
8/14/2019 Pedi Neck Mass Slides 071031
79/116
pppp
hypoechoic
Malik et al 20026
Thyroid AbscessThyroid Abscess
-
8/14/2019 Pedi Neck Mass Slides 071031
80/116
yy
Malik et al 20026
Pediatric Neck MassesPediatric Neck Masses
-
8/14/2019 Pedi Neck Mass Slides 071031
81/116
1. Congenital lesions1. Congenital lesions
2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions
4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
Pediatric Neck MassesPediatric Neck Masses
-
8/14/2019 Pedi Neck Mass Slides 071031
82/116
1. Congenital lesions1. Congenital lesions
2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions
4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
3. Non3. Non--inflammatory Benigninflammatory Benign
-
8/14/2019 Pedi Neck Mass Slides 071031
83/116
LesionsLesionsInclusion cyst 13 3%
Fibromatosis 9 2%Keloid 1
Inclusion CystInclusion Cyst
-
8/14/2019 Pedi Neck Mass Slides 071031
84/116
AcquiredAcquired dermoiddermoid cystscysts
result from a part of the skin being traumaticallyresult from a part of the skin being traumaticallyimplanted in the deeper layers afterimplanted in the deeper layers after ectopicectopic formationformationof aof a dermal cyst l ined w ithdermal cyst l ined w ith squamoussquamousepitheliumepithelium ..
Congenital inclusionCongenital inclusion dermoiddermoid cysts form alongcysts form alongthe lines of embryologic fusion and contain boththe lines of embryologic fusion and contain both
dermal and epidermal derivatives.dermal and epidermal derivatives. DermoidDermoid cysts of the head and neck are thought to becysts of the head and neck are thought to be
the congenital inclusion type.the congenital inclusion type.
Pryor et al 200512
Inclusion CystInclusion Cyst
-
8/14/2019 Pedi Neck Mass Slides 071031
85/116
many cysts originate from themany cysts originate from the infundibularinfundibular
portion of the hair follicle, and the moreportion of the hair follicle, and the moregeneral term,general term, epidermoidepidermoid cystcyst, is favored, is favored
Becker et a, 200519
Epidermal Inclusion CystEpidermal Inclusion Cyst
-
8/14/2019 Pedi Neck Mass Slides 071031
86/116
Cyst containing keratinous material true epidermis with a granular layerand adjacent laminated keratinousmaterial
Becker et al, 200519
TorticollisTorticollis
-
8/14/2019 Pedi Neck Mass Slides 071031
87/116
FibromatosisFibromatosis ColliColli
-
8/14/2019 Pedi Neck Mass Slides 071031
88/116
SCMSCM
IsoechoicIsoechoic massmass
CT showsCT shows isodenseisodense
mass R sidemass R side
Note normal SCM onNote normal SCM on
L sideL side
Malik et al 20026
FibromatosisFibromatosis ColliColli -- FNAFNA
-
8/14/2019 Pedi Neck Mass Slides 071031
89/116
PaucicellularPaucicellular
specimenspecimen
Bland spindleBland spindlecell cytologycell cytology
r/or/o nodularnodular fascitisfascitis andand fibrosarcomafibrosarcoma
Rapkiewicz et al 200721
FibromatosisFibromatosis ColliColli
-
8/14/2019 Pedi Neck Mass Slides 071031
90/116
r/or/o nodularnodular fascitisfascitis andand fibrosarcomafibrosarcoma
Ro 200720
-
8/14/2019 Pedi Neck Mass Slides 071031
91/116
Moir. 20042
Pediatric Neck MassesPediatric Neck Masses
-
8/14/2019 Pedi Neck Mass Slides 071031
92/116
1. Congenital lesions1. Congenital lesions
2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions
4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
Pediatric Neck MassesPediatric Neck Masses
-
8/14/2019 Pedi Neck Mass Slides 071031
93/116
1. Congenital lesions1. Congenital lesions
2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions
4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
4. Benign Neoplasms4. Benign Neoplasms
-
8/14/2019 Pedi Neck Mass Slides 071031
94/116
Neurofibroma 3 1%
Lipoma 3 1%Lipoblastoma 2Paraganglioma 1Goiter 1Benign mixed tumor 1Osteoblastoma 1
NeurofibromaNeurofibroma
-
8/14/2019 Pedi Neck Mass Slides 071031
95/116
solitary lesionsolitary lesion
vsvs part of the generalized syndrome ofpart of the generalized syndrome of
neurofibromatosisneurofibromatosis NFNF--1, aka von Recklinghausen disease1, aka von Recklinghausen disease
NFNF--22
Believed to arise from Schwann cell butBelieved to arise from Schwann cell butorigin uncertainorigin uncertain
NeurofibromaNeurofibroma
-
8/14/2019 Pedi Neck Mass Slides 071031
96/116
solitary lesionsolitary lesion
vsvs part of the generalized syndrome ofpart of the generalized syndrome of
neurofibromatosisneurofibromatosis NFNF--1, aka von Recklinghausen disease1, aka von Recklinghausen disease
NFNF--22
Believed to arise from Schwann cell butBelieved to arise from Schwann cell butorigin uncertainorigin uncertain
NeurofibromaNeurofibroma
-
8/14/2019 Pedi Neck Mass Slides 071031
97/116
T2 MRIT2 MRI
Central low T2Central low T2
signal issignal ischaracteristic ofcharacteristic of
neurofibromasneurofibromas
Gujar and Mukherji 20045
LipomaLipoma
-
8/14/2019 Pedi Neck Mass Slides 071031
98/116
LipoblastomaLipoblastoma
http://www.microscopyu.com/galleries/pathology/lipomalarge.html -
8/14/2019 Pedi Neck Mass Slides 071031
99/116
Rare benignRare benign mesynchymalmesynchymal
tumor oftumor ofembryonalembryonal fatfat
May clinically andMay clinically and radiologicallyradiologicallymimic amimic a hemangiomahemangioma
Collections ofCollections oflipoblastslipoblastsmultivuolatedmultivuolated w/ round nucleiw/ round nuclei
FNA
LipoblastomaLipoblastoma
-
8/14/2019 Pedi Neck Mass Slides 071031
100/116
ResemblesResembles
embryological adiposeembryological adiposetissuetissue
Surgical specimen
LipomaLipoma LipoblastomaLipoblastoma
http://www.microscopyu.com/galleries/pathology/lipomalarge.html -
8/14/2019 Pedi Neck Mass Slides 071031
101/116
NeonatalNeonatal
GoiterGoiter
http://www.microscopyu.com/galleries/pathology/lipomalarge.html -
8/14/2019 Pedi Neck Mass Slides 071031
102/116
GoiterGoiter
CT shows large peripheral rimCT shows large peripheral rimenhancing, low attenuationenhancing, low attenuationmassmass
1: 4000 live births1: 4000 live births
Female 2x = MaleFemale 2x = Malepredominancepredominance
Delayed ossification at boneDelayed ossification at boneendsends
Malik et al, 20026Rovet et al, 200310
-
8/14/2019 Pedi Neck Mass Slides 071031
103/116
Pediatric Neck MassesPediatric Neck Masses
-
8/14/2019 Pedi Neck Mass Slides 071031
104/116
1. Congenital lesions1. Congenital lesions
2. Inflammatory lesions2. Inflammatory lesions
3. Non3. Non--inflammatory benign lesionsinflammatory benign lesions
4. Benign4. Benign neoplasmsneoplasms
5. Malignant5. Malignant neoplasmsneoplasms
5. Malignant Neoplasms5. Malignant Neoplasms
-
8/14/2019 Pedi Neck Mass Slides 071031
105/116
Lymphoma 34 8%Hodgkin's 23 5%
Non-Hodkin's 11 2%Thyroid Carcinoma 6 1%Rhabdomyosarcoma 2
Neuroblastoma 2Fibrous histiocytoma 1Acinic cell carcinoma 1Histiocytosis X 1Chloroma 1
LymphomaLymphoma
-
8/14/2019 Pedi Neck Mass Slides 071031
106/116
Third most common pediatric cancerThird most common pediatric cancer
Incidence: 11Incidence: 11--20 per million children20 per million children
Geographical varianceGeographical variance 50 % of50 % of
childhood cancers in equatorial Africachildhood cancers in equatorial Africa Due to high incidence ofDue to high incidence ofBurkittBurkittss lymphomalymphoma
Male predominance 2.5:1Male predominance 2.5:1
Beware theBeware the supraclavicularsupraclavicular mass!mass!
-
8/14/2019 Pedi Neck Mass Slides 071031
107/116
35% of patients35% of patients
with H&Nwith H&Nlymphomalymphomapresent with apresent with asupraclavicularsupraclavicular
massmass
35% of pts with35% of pts with
suprclavicularsuprclavicularmasses hadmasses hadlymphomalymphoma
Turkington et al 200522 TorsiglieriTorsiglieri et al., 1988et al., 198822
NeuroblastomaNeuroblastoma
-
8/14/2019 Pedi Neck Mass Slides 071031
108/116
NoncontrastNoncontrast T1T1
MRIMRI
Mass (arrow)Mass (arrow)lateral to carotidlateral to carotid
arteryartery(arrowhead).(arrowhead).
Gujar and Mukherji 20045
RhabdomyosarcomaRhabdomyosarcoma -- CTCT
-
8/14/2019 Pedi Neck Mass Slides 071031
109/116
Ill definedIll defined
enhancing softenhancing soft
tissue densitytissue density
areas of necrosisareas of necrosis
Malik et al 20026
RhabdomyosarcomaRhabdomyosarcoma
of the Masticator Spaceof the Masticator Space
-
8/14/2019 Pedi Neck Mass Slides 071031
110/116
pp
NonNon--contrast T1contrast T1 intermediateintermediatesignalsignal
T2T2 increased signalincreased signal
Gujar and Mukherji 20045
TorsiglieriTorsiglieri et al., 1988et al., 198822
-
8/14/2019 Pedi Neck Mass Slides 071031
111/116
Inflammatory
lesions
27%
Malignant
neoplasms, 11%
Benign neoplasms
3%
Non-infammatory
benign lesions
5%
Congenital lesions
54%
N= 445
Total % oftotal
Congeital lesions 244 55%Branchial cleft cyst 78 18%Thyroglossal duct cyst 73 16%Dermoid cyst 43 10%Lymphangioma 34 8%Hemangioma 10 2%
Non-infammatory benignlesions
23 5%
Inclusion cyst 13 3%Fibromatosis 9 2%
Keliod 1
-
8/14/2019 Pedi Neck Mass Slides 071031
112/116
gTeratoma 2Bronchogenic cyst 2Thymic cyst 1
Myelomeningocele 1Inflammatory lesions 118 27%
Reactive lympadenopathy 71 16%Undetermined etiology 66 15%Sinus histiocytosis 5 1%
Granulomatous disease 32 7%Atypical mycobacteria 20 4%Cat scratch disease 6 1%Toxoplasmosis 2Sarcoid 2
Suppurative lympadenitis 10 2%
Sialadenitis 5 1%
Benign neoplasms 12 3%Neurofibroma 3 1%Lipoma 3 1%Lipoblastoma 2Paraganglioma 1Goiter 1Benign mixed tumor 1Osteoblastoma 1
Malignant neoplasms 48 11%Lymphoma 34 8%Hodgkin's 23 5%Non-Hodkin's 11 2%
Thyroid Carcinoma 6 1%Rhabdomyosarcoma 2
Neuroblastoma 2Fibrous histiocytoma 1Acinic cell carcinoma 1Histiocytosis X 1Chloroma 1
Total 445TorsiglieriTorsiglieri et al., 1988et al., 198822
ConclusionsConclusions
-
8/14/2019 Pedi Neck Mass Slides 071031
113/116
Initial evaluation (H&P)Initial evaluation (H&P)
Congenital, infectious, benign, malignantCongenital, infectious, benign, malignant Beware of tuberculosis, cat scratchBeware of tuberculosis, cat scratch
disease, atypical infectionsdisease, atypical infections
Beware of systemic symptomsBeware of systemic symptoms
Beware theBeware the supraclavicularsupraclavicular massmass
Consider FNA or biopsy in the mass thatConsider FNA or biopsy in the mass thatdoes not resolve with treatment.does not resolve with treatment.
BibliographyBibliography
-
8/14/2019 Pedi Neck Mass Slides 071031
114/116
1.1. NeoReviews.orgNeoReviews.org,,http://neoreviews.aappublications.org/case27/case.shtmlhttp://neoreviews.aappublications.org/case27/case.shtml, 10/18/07., 10/18/07.
2.2.
TorsiglieriTorsiglieri
AJAJ
JrJr
, Tom LW, Ross AJ 3rd, Wetmore RF, Handler SD,, Tom LW, Ross AJ 3rd, Wetmore RF, Handler SD,
PotsicPotsic
WP. Pediatric neck masses: guidelines for evaluation.WP. Pediatric neck masses: guidelines for evaluation. IntInt JJ PediatrPediatrOtorhinolaryngolOtorhinolaryngol.. 1988 Dec;16(3):1991988 Dec;16(3):199--210.210.
3.3. Nicollas R, Guelfucci B, Roman S, Triglia JM.Nicollas R, Guelfucci B, Roman S, Triglia JM. Congenital cysts andCongenital cysts andfistulas of the neck.fistulas of the neck. IntInt JJ PediatrPediatrOtorhinolaryngolOtorhinolaryngol. 2000 Sep. 2000 Sep29;55(2):11729;55(2):117--24.24.
4.4. Schroeder JWSchroeder JW JrJr,, MohyuddinMohyuddin N,N, MaddalozzoMaddalozzo J. Branchial anomalies inJ. Branchial anomalies inthe pediatric population.the pediatric population. OtolaryngolOtolaryngol Head NeckHead Neck SurgSurg. 2007. 2007Aug;137(2):289Aug;137(2):289--95.95.
5.5. GujarGujarS, Gandhi D,S, Gandhi D, MukherjiMukherji SK. Pediatric head and neck masses. TopSK. Pediatric head and neck masses. TopMagnMagn ResonReson Imaging. 2004 Apr;15(2):95Imaging. 2004 Apr;15(2):95--101.101.
6.6. MalikMalikA,A, OditaOdita J, Rodriguez J,J, Rodriguez J, HardjasudarmaHardjasudarma M. Pediatric neck masses:M. Pediatric neck masses:a pictorial review for practicing radiologists.a pictorial review for practicing radiologists. CurrCurrProblProbl DiagnDiagn RadiolRadiol..2002 Jul2002 Jul--Aug;31(4):146Aug;31(4):146--57.57.
Bibliography (cont)Bibliography (cont)
http://neoreviews.aappublications.org/case27/case.shtmlhttp://neoreviews.aappublications.org/case27/case.shtmlhttp://neoreviews.aappublications.org/case27/case.shtmlhttp://neoreviews.aappublications.org/case27/case.shtmlhttp://neoreviews.aappublications.org/case27/case.shtmlhttp://neoreviews.aappublications.org/case27/case.shtmlhttp://neoreviews.aappublications.org/case27/case.shtml -
8/14/2019 Pedi Neck Mass Slides 071031
115/116
7.7. ROH,ROH, JL.JL.LymphomasLymphomas of the head and neck in the pediatricof the head and neck in the pediatricpopulation, International journal of pediatricpopulation, International journal of pediatric otorhinolaryngologyotorhinolaryngology,,
Volume 71, Issue 9, September 2007, Pages 1471Volume 71, Issue 9, September 2007, Pages 1471--1477.1477.8.8. MoirMoirCR. Neck Cysts, Sinuses,CR. Neck Cysts, Sinuses, ThyroglossalThyroglossal DuctDuct CytsCyts, and, and
Branchial Cleft Anomalies, Operative Tech in GenBranchial Cleft Anomalies, Operative Tech in Gen SurgSurg, v 6, n 4, v 6, n 4(Dec), 2004: 281(Dec), 2004: 281--295.295.
9.9. BranstetterBranstetterBF, Branchial Cleft Cysts,BF, Branchial Cleft Cysts, EmedicineEmedicine,,
http://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htm Oct 24, 2006.Oct 24, 2006.10.10. RovetRovet JF. Congenital hypothyroidism: an analysis of persistingJF. Congenital hypothyroidism: an analysis of persisting
deficits and associated factors. Childdeficits and associated factors. Child NeuropsycholNeuropsychol. 2002. 2002Sep;8(3):150Sep;8(3):150--62.62.
11.11. ThyroglossalThyroglossal Duct Cyst, LearningDuct Cyst, Learning Radiology.comRadiology.com,,http://www.learningradiology.com/archives06/COW%20231http://www.learningradiology.com/archives06/COW%20231--Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlThyroglossal%20Duct%20Cyst/tgdccorrect.html, accessed, accessed10/30/2007.10/30/2007.
http://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htmhttp://www.emedicine.com/radio/topic107.htmhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.htmlhttp://www.emedicine.com/radio/topic107.htm -
8/14/2019 Pedi Neck Mass Slides 071031
116/116
http://www.histopathology-india.net/FC.htmhttp://www.emedicine.com/derm/topic860.htm