kuliah PPHN.pptx
31
PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN ( PPHN ) Nazardi Oyong Subb perinatologi FK-UR / RSUD AA Pekanbaru
-
Upload
kahfi-rakhmadian-kira -
Category
Documents
-
view
227 -
download
0
Transcript of kuliah PPHN.pptx
PPHN and iNO: An evidence-based approach
PersistentPulmonaryhypertension of thenewborn( pphn )Nazardi OyongSubb perinatologi FK-UR / RSUD AA Pekanbaru1PPHNIs a major clinical problem in the neonatal intensive care unit.Can contribute significantly to morbidity and mortality in both term and preterm infants.Hypoxemic respiratory failure or PPHN can place newborns at risk for death, neurologic injury, and other morbidities.Incidence is estimated at 0.2% of liveborn term infants.
2Fetal circulati adaptionNeonatal pulomonary vasculatureEtiologi and mecanismTreatment
3 Fetus - from 8 weeks until birth organs mature to support external life Fetal circulation umbilical-placental circuit via umbilical cord circulatory shunts to bypass Liverductus venosus to inferior vena cava Lungs @ foramen ovale between right & left atria@ ductus arteriosus connects pulmonary artery to aorta1. Circulatory ADAPTATION4
5CIRCULATORY ADAPTATION
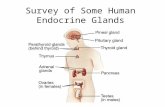
Umbilical veinDuctus venosusForamen OvaleDuctus arteriosusPulmonary circ.Systemic circ.Umbilical artery6
CIRCULATORY ADAPTATION
DUCTUS VENOSUS
BY PASS I7CIRCULATORY ADAPTATION
FORAMEN OVALE
BY PASS II8CIRCULATORY ADAPTATION
PATENT DUCTUS ARTERIOSUS
BY PASS III9CIRCULATORY ADAPTATION
FETAL CIRCULATION High pulmonary resistanceLow resistance in systemic blood flowRIGHT to LEFT shunt Foramen Ovale(Left arterial pressure low because returned lung blood is low and right atrial pressure high due to large volume of blood from placenta)Ductus arteriosus(High pulmonary resistance, Low fetal systemiv blood and prostaglandin function)10CIRCULATORY ADAPTATION
NEONATAL CIRCULATION Profound changes of circulation at birth Increased pulmonary blood flow due to the drops of pulmonary resistance - lung expansions. Venous return from lung increase. Left arterial press. is raised; Right art.press.decrease foramen ovale closed. Systemic resistance higher than pulmonary resistance (24 hours) Prostaglandin function Ductus close Constrict umbilical arteries and placental blood stops. 11NEONATAL ADAPTATION
FETALCIRCULATIONNEONATALCIRCULATION12NEONATAL ADAPTATION
CIRCULATORY ADAPTATIONFetusNewbornPulmonary circulationActive, less develop.Active, increased developmentForamen ovaleOpenCloseDuctus arteriosus BotaliOpenCloseDuctus Venosus ArantiiOpenCloseSystemic circulationActive with low resistanceActive with increase resistance13Circulatory ADAPTATION
14NEONATAL ADAPTATION
FETAL PULMONARY DEVELOPMENTAlveoli present : 25 weeks fill with lung fluidsBreathing movements: Intermittently Lung developments Control of breathing
Fetus : gas exchange placenta15NEONATAL ADAPTATION
FIRSTBREATHMechanicalProprioceptiveChemoreceptorTemperatureTouchDiafragmNeonatal RespirationIrregularAbdominal respirationPain16NEONATAL ADAPTATION
PULMONARY ADAPTATION CHAIN OF EVENTS AFTER FIRST BREATH : Converts fetal to adult circulation Empties the lung fluids. Begin pulmonary function.THE NEWBORN RESPIRATIONBEGIN17PULMONARY ADAPTATION
FETUSNEWBORNAlveolusColapsDevelopsPulmonary vesselsNon activeActivePulmonary resistanceHighDecreasePulmonary bloodLowIncreaseOxygen needsPlacentaLungCO2 excretionPlacentaLung18PPHNPersistent fetal circulationKombinasi :High pressure in the pulmonary arteryRight to the left shunting from pulmonary vascular bedStructurally normal heart
19Fetal circulati adaptionNeonatal pulomonary vasculatureEtiologi and mecanismTreatment
202. Neonatal pulomonary vasculatureSesnsitif to ; PaO2, PH, stressBecome hyperreaktive and constrictCause increase pressureNeonatal heart cannot force blood flow to the lungRight to the left shunt ( for ovale & duct arteriosus )Infant become : hipoxemia, acidemia
21
The fetal pulmonary circulation undergoes striking developmental . changes in vascular growth, structure, and function.-Because the placenta, not the lung, serves as the organ of gas exchange, less than 10% of the combined ventricular output is circulated through the pulmonary vascular bed, and most of the right ventricular output crosses the ductus arteriosus to the aorta .22Despite increases in pulmonary vascular surface area, PVR (pulmonary vascular resistance ) increases with gestational age when corrected for lung or body weight, suggesting that vascular tone actually increases during late gestation and is high prior to birth.
23Pathways involved in maintaining high pulmonary vascular tone in utero:
low oxygen tension
2) mediators such as endothelin-1 (ET-1) and leukotrienes.
3) basal production of vasodilator products : prostacyclin (PGI2) and nitric oxide (NO) is relatively low
4) the fetal vasculature also has the interesting ability to oppose vasodilation.
24Normal Pulmonary Vascular TransitionThe pulmonary vascular transition at birth is characterized by :rapid increase in pulmonary blood flow
reduction in PVR
clearance of lung liquid.
25Central role in the pulmonary vascular transition :
1. Pulmonary endothelial cells
2. NO 3. Arachidonic acid metabolites
26At the time of birth, multiple factors regulate these pathways:
mechanical distention of the lung
a decrease in carbon dioxide tension
3. an increase in oxygen tension in the lungs.
27Fetal circulati adaptionNeonatal pulomonary vasculatureEtiologi and mecanismTreatment
28PPHN is categorized into:
Parenchymal lung disease (meconium aspiration syndrome, respiratory distress syndrome, sepsis)Idiopathic (or "black-lung") Pulmonary hypoplasia (as seen in congenital diaphragmatic hernia).29 Treatment of PPHN
1.Initial Therapies-Treat metabolic derangements: correct acidosis, hypoglycemia, hypocalcemia-Optimize lung recruitment: mechanical ventilation, high-frequency oscillatory ventilation, surfactant-Optimize cardiac output and left ventricular function: vasopressors, inotropic agents2. Pulmonary Vasodilators-Inhaled nitric oxide3.Future Therapies-Phosphodiesterase Inhibitors (sildenafil)-Inhaled prostacyclin analogs (iloprost, prostacyclin)-Recombinant superoxide dismutase
30terimakasih31