
DDH Kuliah
47
Developmental Dysplasia of the Hip (DDH)
-
Upload
rizki-rahmiana-harahap -
Category
Documents
-
view
234 -
download
4
description
medic
Transcript of DDH Kuliah

Developmental Dysplasia of the Hip (DDH)

Hip Anatomi


A few facts about DDH
• developmental (not congenital)
• subluxation vs. dislocation vs. instability
• typical vs. teratologic

Causes of typical DDH
• Physiological, Mechanical, & Postural Factors
• ligamentous laxity
• 9:1 female to male preponderance
• first born (60%)
• breech presentation (30-50%)
• family history (20%)
• associated conditions

Consequences of DDH
• Acetabular dysplasia and maldirection
• Excessive femoral anteversion (torsion)
• Muscle contractures
• Avascular necrosis of femoral head

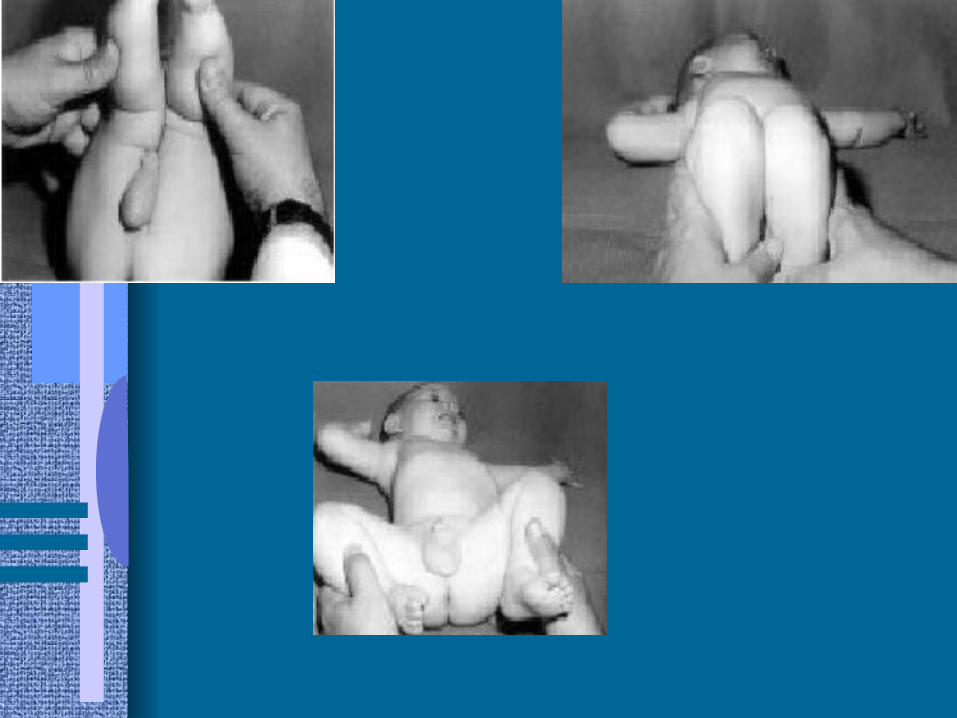
Clinical Manifestations
• In the newborn– limitation of hip abduction– absent normal knee flexion contracture– assymetric number of thigh skinfolds– uneven knee levels– apparent shortening of an extremity

Physical Exam Maneuvers
• A. Barlow Test– dislocates an unstable hip– stabilize pelvis with one hand, then flex and
adduct opposite hip with posterior pressure.– dislocation is felt as a “clunk”– release of posterior pressure spontaneously
relocates femoral head.

Physical Exam Maneuvers (con’t.)
• B. Ortolani Test– reduces a recently dislocated hip– flex and abduct thigh to lift femoral head into
acetabulum– relocation “clunk”– most likely to be positive at 1-2 mos.

Physical Exam Maneuvers (con’t)

Other Clinical Manifestations
• In older children– limping, waddling, toe walking– increased lumbar lordosis– leg length discrepancy

Clicks vs. Clunks
• Clicks– benign adventitial sounds– secondary to several causes– not predictive of DDH
• Clunks– feeling of true dislocation or reduction– positive examination

Imaging
• Ultrasound– most useful during first four weeks of life– visualization of cartilage– recommended only as an adjunct to PE
• Radiograph– more useful by 4 to 6 months of age– cheap, less operator dependent

Ultrasound

Radiograph


Treatment
• Treatment is age specific
• Neonate– Goal: maintain hip in flexed and abducted
position to maintain femoral head reduction and tighten ligamentous structures.
– Pavlik harness or Frejka splint for 1-2 mos.

Arthrogram
1. Limbus - 'Rose thorn sign' of inverted labrum between femoral head & acetabulum
2. Hour glass constriction of capsule - by psoas tendon
3. Capsular distension 4. Medial pooling of dye (normal = < 7mm) 5. Confirms reduction after surgery


Treatment
• 1-6 months– Pavlik harness for 3-4 weeks.– Closed surgical reduction if harness fails.



Save Zone Position
20-550

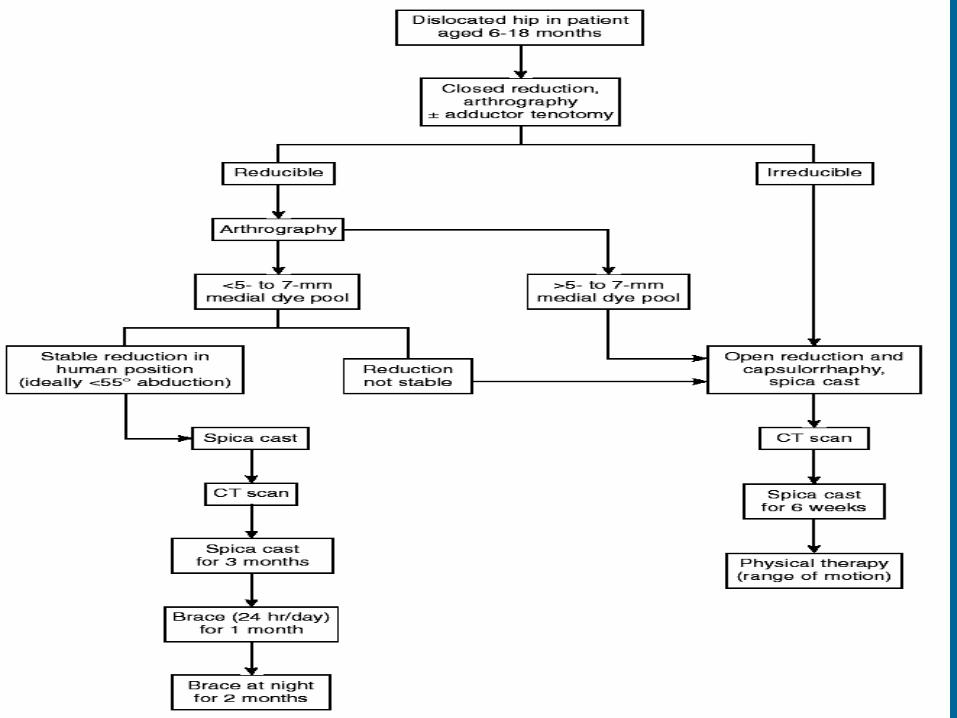
Treatment
• 6-18 mos.
– Closed or open surgical reduction
– Hip spica cast

Pathology
Treatment
• 18 mos.-8 years– Open reduction with pelvic and/or femoral
osteotomy

Pelvic osteotomies
• Salter’s innominate
• Pemberton
• Osteotomies to free the acetabulum - Steel & Dega
• Chiari displacement osteotomy

Options
• Do nothing
• Femoral osteotomies
• Pelvic osteotomies
• Combination
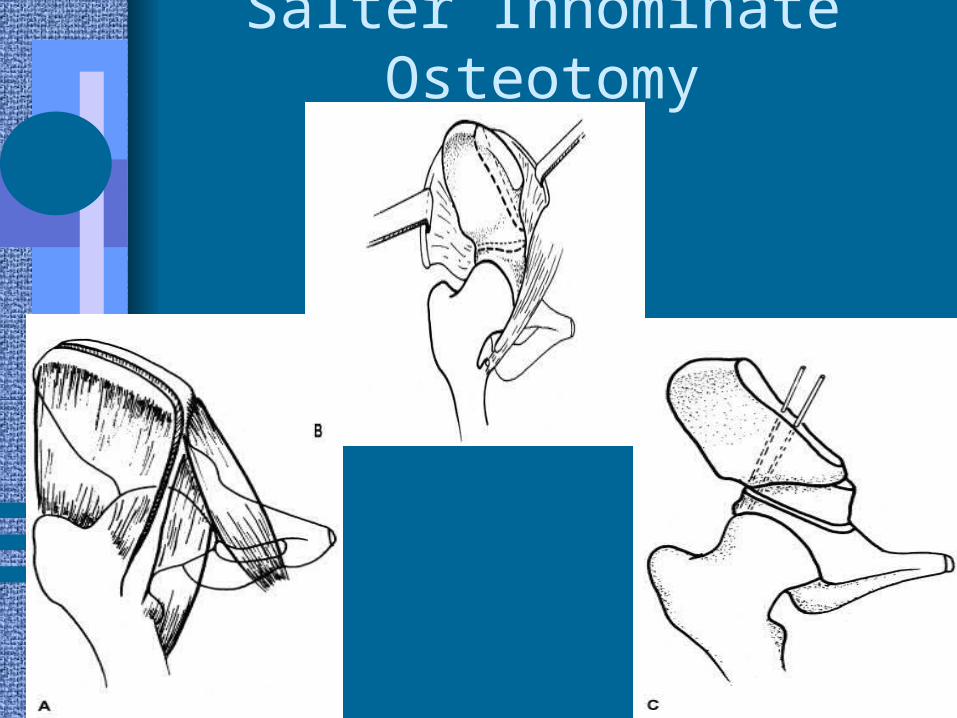
Salter Innominate Osteotomy

Pemberton osteotomy

Dega Osteotomy
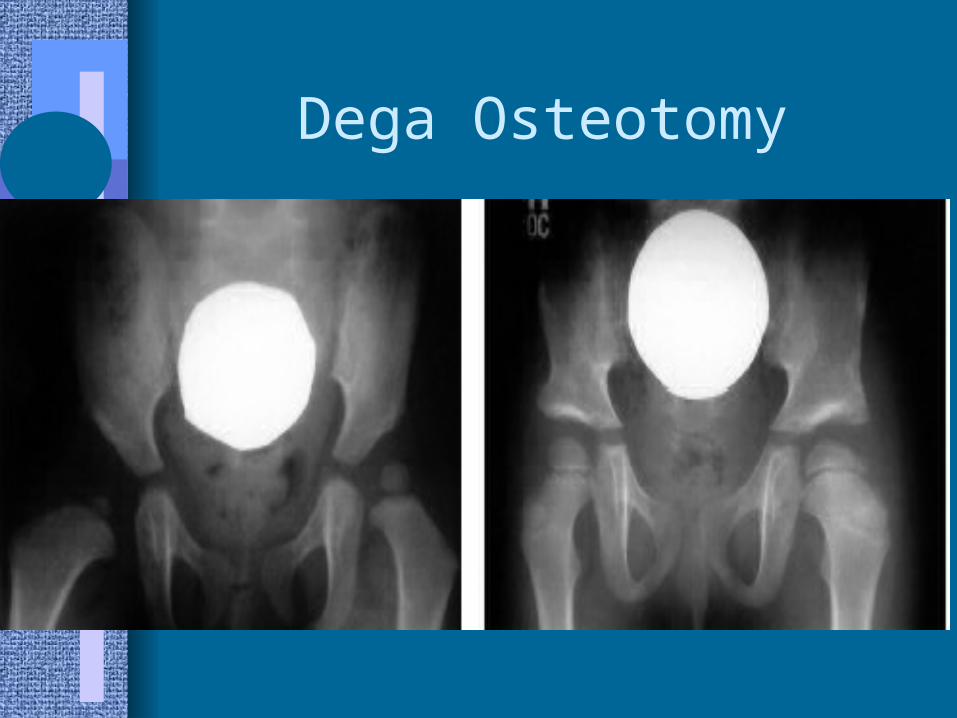
Dega Osteotomy

Chiarry Osteotomy

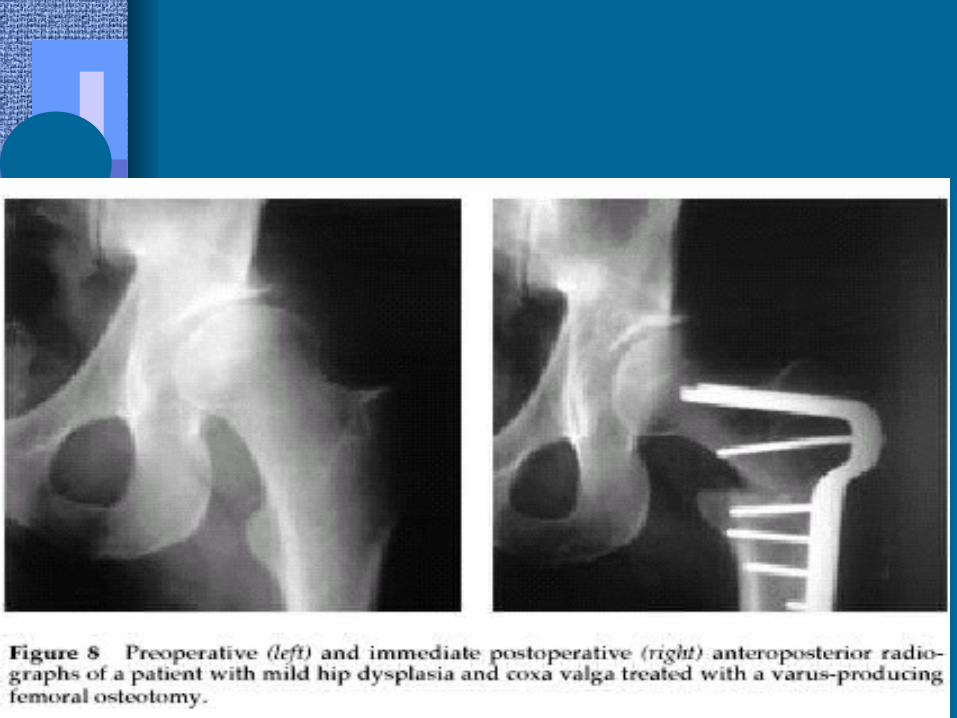
Femoral osteotomy (Shortening)

Surgical Treatment in Adults:
1. Nonarthroplasty Options1. Pelvic Osteotomy
2. Bernese Periacetabular Osteotomy
3. Femoral Osteotomy
4. Arthrodesis


Pelvic Osteotomy


2. Arthroplasty Options

Alternative methods


Complication’s
• The most common complication of treatment of DDH is osteonecrosis of the femoral head
• Growth disturbance of proximal femoral physis
• Gait abnormality

Summary
• DDH is an evolving process
• Proper serial exams are imperative to prevent deformity
• Know clicks from clunks
• Earlier treatment=better outcomes


















