Kenya: Taking forward action on HRH · the HRH Action Framework (Policy, Education, Partnership,...
50
Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners. Jim Campbell & Barbara Stilwell 24 October 2008 The Capacity Project 6340 Quadrangle Drive Chapel Hill NC 27517 USA Tel: + 1 919 313 9161 www.capacityproject.org Instituto de Cooperación Social ‐ Integrare S.L. Aribau 69, 2‐1 08036 Barcelona Spain Tel: + 34 934 530 788 Email: [email protected] Whilst this report has been jointly commissioned by DFID and PEPFAR/OGAC its contents are solely the responsibility of the authors and do not necessarily represent the official views of DFID, PEPFAR, OGAC, CDC, USAID or any of the implementing partners associated with their activities in Kenya.
Transcript of Kenya: Taking forward action on HRH · the HRH Action Framework (Policy, Education, Partnership,...

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Jim Campbell & Barbara Stilwell
24 October 2008
The Capacity Project 6340 Quadrangle Drive Chapel Hill NC 27517
USA
Tel: + 1 919 313 9161 www.capacityproject.org
Instituto de Cooperación Social ‐ Integrare S.L.
Aribau 69, 2‐1 08036 Barcelona
Spain
Tel: + 34 934 530 788 Email: [email protected]
Whilst this report has been jointly commissioned by DFID and PEPFAR/OGAC its contents are solely the
responsibility of the authors and do not necessarily represent the official views of DFID, PEPFAR, OGAC, CDC, USAID or any of the implementing partners associated with their activities in Kenya.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Abbreviations and Acronyms CoAg Cooperation Agreement CAP Country Assistance Plan (for DFID) COP Country Operational Plan (for PEPFAR) COPRS Country Operational Plan Reporting System CDC Centres for Disease Control and Prevention DFID Department for International Development DPH‐K Development Partners in Health ‐ Kenya FBO Faith Based Organisation GAP Global Aids Program (for CDC) GAVI Global Alliance for Vaccines and Immunisation GFATM Global Fund for AIDS, TB and Malaria GHAP Global HIV/AIDS Programme (for WB) GHWA Global Health Workforce Alliance GoK Government of Kenya HENNET Health NGOs Network HRH‐ AF Human Resources for Health Action Framework HRH Human Resources for Health HSS Health Systems Strengthening IHP International Health Partnership INGO International Non‐Governmental Organisation JPWF Joint Programme of Work and Funding KEPH Kenya Essential Package for Health MoH Ministry of Health MoMS Ministry of Medical Services MoPHS Ministry of Public Health and Sanitation MoPS Ministry of Public Services. MoU Memorandum of Understanding MTEF Medium Term Expenditure Framework MTP Medium Term Plan (2008‐12) NHSSP II National Health Sector Strategic Plan II (2005‐10) NGO Non‐Governmental Organisation OGAC Office of the US Global Aids Coordinator PEPFAR President’s Emergency Programme for AIDS Relief PHC Primary Health Care PSRS Public Service Reform Strategy SBS Sector Budget Support SWAp Sector Wide Approach TBA Traditional Birth Attendant TOR Terms of Reference USAID United States Agency for International Development WB World Bank WHO World Health Organisation
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 2 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Acknowledgements The consultants wish to acknowledge the support of all the individuals from MoMS, MoPHS, development partners, implementing agencies and national organisations who participated in the organisation of the assignment and the subsequent interviews. Particular thanks to Melahi Pons and Tony Daly for their time and insights; to individuals associated with PEPFAR programmes who made time to meet with us despite being involved in the intensity of the annual COP process, and; to Kimani Mungai and his colleagues at the Capacity Project office in Nairobi for hosting and supporting the mission. For further information please contact: Jim Campbell, Director, ICS Integrare: [email protected] Barbara Stilwell, Senior Technical Advisor, Capacity Project: [email protected]
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 3 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Table of Contents
EXECUTIVE SUMMARY ................................................................................................................................. 5
1 BACKGROUND / INTRODUCTION ........................................................................................................ 11
2 NATIONAL PLANS AND STRATEGIES IN KENYA .................................................................................... 12
2.1 NATIONAL PLANS AND STRATEGIES RELATED TO HRH ....................................................................... 14
3 FINDINGS ON PEPFAR AND DFID SUPPORTING ACTIVITIES .................................................................. 23
3.1 ‘PEPFAR’ KENYA ...................................................................................................................... 23 3.2 DFID ....................................................................................................................................... 28
4 DISCUSSION AND RECOMMENDATIONS ............................................................................................. 30
4.1 A STRATEGIC APPROACH TO HRH IN KENYA ................................................................................... 30 4.2 STRENGTHENING HRH ............................................................................................................... 32 4.3 DEVELOPMENT PARTNERS – SUPPORTING ACTIONS ......................................................................... 36 4.4 MATRIX OF RECOMMENDATIONS RESULTING. ................................................................................. 38
ANNEXES ................................................................................................................................................... 41
ANNEX 1 – TERMS OF REFERENCE ............................................................................................................... 41
ANNEX 2 – ITINERARY AND PERSONS MET .................................................................................................. 44
ANNEX 3 – INDICATIVE MODEL: FAST‐TRACK HIRING AND INTEGRATION PLAN (FTHIP) ............................... 45
ANNEX 4 – SELECTED EXTRACTS FROM THE PEPFAR REAUTHORISATION ..................................................... 46
ANNEX 5 – GHWA TASK FORCE ON FINANCING HRH ................................................................................... 47
ANNEX 6 ‐ DOCUMENTS CONSULTED / REFERENCED MATERIALS. ............................................................... 48
ANNEX 7 ‐ CONSIDERATIONS FOR FURTHER COUNTRY VISITS. .................................................................... 50
List of Tables and Figures Table 1: MTEF and AOP planning activities........................................................................................... 13 Table 2: Health Ceilings –Expenditure (Ksh Million) 2007/8 – 2010/11 ............................................... 14 Table 3: Comparison of health personnel indicators in selected countries ......................................... 17 Table 4: Nurse Registration v public sector employment (2004‐2007) ................................................ 18 Figure 1: ‘Information Systems’ –Commentary from the HRH Strategic Plan ...................................... 22 Figure 2: HRH Action Framework .......................................................................................................... 23 Table 5: PEPFAR‐supported health care workers in Kenya ................................................................... 25 Table 6: APHIA II Health Worker Costings 2008/9 (by Province) .......................................................... 26 Table 7: Matrix of recommendations ................................................................................................... 38
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 4 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Executive Summary 1. Background. In response to the critical Human Resources for Health (HRH) shortages in Africa,
the UK Department for International Development (DFID) and Office of the US Global Aids Coordinator (OGAC) responsible for the President’s Emergency Programme for AIDS Relief (PEPFAR) have been in discussion with a number of African countries (Ethiopia, Kenya, Mozambique and Zambia) to develop strategies and country level actions. There is high level political support for this process in the UK and US, highlighted by the joint announcements of President George Bush and Prime Minister Gordon Brown in April and June 2008 and the recent calls to action at the UN High Level Event on the MDGs in September 2008.
2. DFID and OGAC agreed to field a team of two consultants to work with their respective leads in
Kenya in the period 02‐13 September, 2008. The main objective of the assignment was to facilitate agreement and document current flexibilities of funding streams for HRH, building on existing work and within national frameworks for priority actions on HRH.
3. Budgeting and Planning Frameworks. There are overarching processes for budgeting and
planning endorsed in the subsequent layers of policy and strategy (Vision 2030, PSRS, NHSSP, MTP, HRH‐SP) and the annual calendars within the planning and budgeting frameworks (MTEF, JPWF and AOP). An analysis of these planning frameworks highlights that it will be essential for both PEPFAR and DFID to align their activities from October 2008 if they wish to influence the GoK planning and allocation of resources for health systems strengthening and HRH development in the next Budget Outlook Paper, Sector Report and Programme‐based Budget.
4. HRH. A Human Resources for Health Strategic Plan (HRHSP) 2007/8‐2009/10 has been
developed and is aligned with a comprehensive policy framework of national and international health goals and commitments. However, despite the supportive policy framework for HRH development, and implementation strategies that accompany plans and policies, there is little substantial change since 2007. This must be, at least in part, due to the rapidly changing policy and political environment of the country. Post‐election disruptions were severe and had effects that are only partially known. One result was the division of Ministry of Health: the Ministry of Public Health and Sanitation (MOPHS) and the Ministry of Medical Services (MOMS), which has the potential to fragment HRH development and administration.
5. Kenya is one of 57 ‘crisis countries’ with an absolute shortage of health workers, yet there are
many more health professionals registered in Kenya than practice in the public sector. The number of registered and enrolled nurses, for example, rose from 40,081 in 2004 to 55,169 in 2007 whilst employment in the public sector has apparently fallen from 16,146 in 2004 to 15,036 in 2007. A high level of unemployment is reported.
6. The HRHSP has to address staffing issues resulting from the reorganization of health care
delivery into six levels of care, the Essential Package for Health (KEPH) and the staffing standards associated with each level. Perhaps the biggest change will be at the interface between community and the health sector, where it is proposed that a cadre of voluntary workers be introduced. A key concern is the competence of the health workers to give the requisite care in their settings. This is especially important in providing skilled attendance at birth. Currently, all nurses are trained in midwifery, and this is vital. It is not clear, though, how competent community workers will be, nor how Traditional Birth Attendants (existing in parts of Kenya) will be accommodated within the envisaged community health care arrangements.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 5 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
7. To succeed in planning the huge increase in staff required to deliver the KEPH a more dynamic planning mechanism will be required, moving away from planning against an established workforce, to using projections, building scenarios and looking at cost‐effective options. Clearly, coordination across the two Ministries will have to be seamless.
8. Tackling deployment must involve addressing retention and migration factors that have been
identified in previous studies. This may mean designing and testing packages of financial and non‐financial incentives with donor support. It will certainly mean revising the hardship allowances so that health professions are equally compensated.
9. Existing support to Capacity Development. Kenya has experienced an increasing growth in
PEPFAR funding since initial activities commenced. It received nearly $92.5 million in Fiscal Year (FY) 2004, more than $142.9 million in FY 2005, approximately $208.3 million in FY 2006, and $368.1 million in FY 2007. This has risen to $534.8 million in FY 2008.
10. An estimate of the volume of PEPFAR resources targeted to Human Capacity Development
(using specific filters in the database which identify programme activities that have ‘Emphasis Areas’ of capacity support) resulted in a figure for Kenya of $334.3m (62%). This is considerably higher than in Mozambique (39%) and may reflect various factors, including the absorption capacity within Kenya or the interpretation and categorisation of activity descriptions at the time of data entry.
11. Initiatives are underway to provide the GoK with support across most of the six major areas of
the HRH Action Framework (Policy, Education, Partnership, Leadership, Management Systems and Finance). The various initiatives collectively contribute to the foundations for further implementation of the HRH Strategy and its five priority objectives. This is aided by the USAID‐funded Capacity Project that seeks to take a holistic approach to HR management and act as a catalyst in support of government leadership on the HRH agenda.
12. PEPFAR recognises that one of the key challenges in Kenya is human resource management.
Given that there is a pool of qualified, unemployed health care workers (estimates suggest that there are some 6,000 ‐7,360 unemployed health workers) and an additional 7,250 nurses in pre‐service training who may have added difficulty in securing employment given a 5‐year increase in the compulsory retirement age one of the critical factors to address HRH in Kenya will be developing effective mechanisms to engage these trained staff.
13. Various PEPFAR initiatives are engaging health workers. An ongoing survey identifies 7,600
workers support by PEPFAR programmes in COP08. This deserves further consideration on the associated costs, including the transaction and marginal costs. For discussion purposes in this report, indicative calculations would suggest a COP08 investment in the 7,600 health worker salaries of $31million. Whilst there are many caveats to this indicative figure it is nonetheless representative of a major investment and circa 10% of the Capacity Development spend identified from the COPRS.
14. Direct salary support for ‘emergency hires’ is one of the mechanisms. In 2006, over 3,000 health
workers were recruited under PEPFAR and other partner schemes since when there appears to be a considerable expansion. The retention level in one of the schemes is reported as 97‐98%, an incredible success given the wider concerns on terms and conditions and retention in the public
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 6 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
service. Emerging evidence suggests Direct Salary Support to be an effective mechanism in the Kenyan context.
15. Progress since Addis Ababa. Progress since the meeting in Addis Ababa (Jan 08) is positive.
Despite the HRH Strategic Plan not being formally adopted, PEPFAR‐funded activities continue to address the strategic priorities and objectives identified. Given the upheaval in Kenyan society and the former MoH, PEPFAR partners have done well to maintain momentum with their respective counterparts.
16. Alignment with government planning. With an emphasis on strategic partnerships in the
PEPFAR reauthorisation, moving from an ‘emergency’ programme to a development intervention, the current cooperation and coordination modalities can be reviewed. There is recognition of a need for a more deliberate and proactive integration process between the AOP and the COP and vice‐versa. Whilst the current calendar supports the integration of AOP priorities into the COP, there were few examples offered of how PEPFAR’s added value on HRH (with the flexibilities and speed of disbursement) is proactively integrated into the AOP planning process. High‐level discussions with the Permanent Secretaries have been conducted and this process will continue in anticipation of COP2010 but in the case of HRH none of the respondents interviewed indicated that they have been involved in a country‐forum to interpret the PEPFAR reauthorisation and consider, and prepare for, new strategic actions.
17. DFID. DFID has responded to the challenge of maximising the flexibility of donor funding. A new
5‐year programme of support (Joint Support Programme to the Kenya Health SWAp) is in its latter stages of design and specifically articulates ‘increasing amounts of flexible funding will be made available for emerging sector priorities determined with the MoH’. The intention is that flexible funds will be jointly coordinated between GoK, DFID and other development partners based on a mapping of inputs against priorities and reviewed annually.
18. Technical Assistance for the implementation of the HRH Strategic Plan has now been secured
through the IHP mechanism with internal procedures in place to allocate these funds for immediate use and quickly move forward on implementation of the priority HRH activities.
19. Discussions and Recommendations. An initial presentation of findings and recommendations
was held on Friday 11th September with representatives of the two Ministries and DFID.
20. The recommendations are situated within the global context for HRH, the health‐related MDGs and the need to consider Kenya as an actor within this wider framework. The GoK has a unique opportunity to position itself to respond to the global context and to lead a coordinated effort to address the country‐specific characteristics of its health workforce shortages and development requirements. It is against this scenario that the consultants envisage a GoK‐led initiative to achieve the WHO goal of at least 2.3 health workers per 1,000 people and to remove Kenya from the WHO category of an “HRH crisis country”
21. Whilst precise data would be required in the coming months, a common agenda to train and
recruit 20,000 ‐ 25,000 additional health workers under the stewardship of the Ministries of health (working in the public and faith‐based health facilities) would be the core focus. PEPFAR could secure a significant percentage of its 140,000 target in the next five years through this strategic partnership and Kenya could become a model for other country actions in Sub‐Saharan Africa.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 7 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
22. The rationale is based on the many positive elements of HRH, health sector and macro‐economic development that were evident in Kenya during the assignment. An indicative model for a ‘Fast‐Track Hiring and Integration Plan’, with a projection of 21,000 new health care workers is provided as an example. In this model (to be considered a discussion tool) the average annual investment from Development Partners over the 9‐year period 2008‐2017 is calculated at $25.5m – a figure less than PEPFAR’s current investment in health worker salaries discussed earlier. The impact on GoK budgeting and fiscal space for absorption into permanent posts rises from $6.9m in year‐4 to $97m in year‐9.
23. Section 4 of this report provides the detailed discussion on the findings and recommendations.
The table below is a summary of these.
Recommendation Lead Target date Means of Verification
HRH1: Formal adoption of the HRH Strategic Plan by the 2 Permanent Secretaries
MoMs + MoPHS
September 2008
PS letters or equivalent
HRH2: Creation of the shared HRH department/unit reporting to the Permanent Secretaries
MoMs + MoPHS
September 2008
PS letters or equivalent
HRH unit established
HRH3: Creation of the appropriate HRH coordination mechanism linked to the Health Sector Coordination Committee
MoMs + MoPHS
October 2008 PS letters or equivalent
HRH 4: Develop strategic planning functions aligned to government planning frameworks and explore new planning models
HRH department / unit
Report from the Institutional Review
Updates in HRHSP workplan
HRH 5: Commission an analysis of wage ceilings and the fiscal space for scaling‐up HRH in Kenya and link this to the next MTEF and AOP frameworks
HRH department / unit
October 2008 for work commission
(report to be able by early December)
Agreed Terms of Reference
DP agreement to support the TA
Final report.
HRH 6: Continue to strengthen HRIS and enhance workforce surveillance information systems to incorporate distribution, infrastructure, epidemiological and population data compatible with a GIS reporting capacity
HRH department / unit
December 2008 for initial agreements
Agreement with supporting partners noted in minutes of the HRIS TWG.
HRH 7: Conduct a comprehensive review of the legislative, policy and strategic frameworks that impact on HRH
HRH department / unit
October 2008 for work commission
(report to be able by early December)
Agreed Terms of Reference
DP agreement to support the TA
Final report.
HRH 8: Strengthen education and training in HRH planning and management and consider North‐South
HRH department / unit
October 2009 for first courses
Agreements in place between learning institutions
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 8 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 9 of 50
Recommendation Lead Target date Means of Verification
and South‐South partnership approaches
Courses underway
HRH 9: Review and implement the necessary communication activities across the health Ministries and with wider stakeholders
MoMs + MoPHS
December 2008
Communication mechanisms in use (e.g. newsletter, blog)
HRH 10: Review options to deliver the Treat and Retain principles from the Treat, Train & Retain initiative with the introduction of ‘Wellness Centres’ and support to the Positive Practice Environment campaign
HRH department / unit
June 2009 First Wellness centre open and fully functional
HRH 11: Review options for developing health worker skills and competencies in the management of the third stage of labour and implement recommendations resulting
HRH department / unit
April 2009 Training plan available
Development Partners (DPs)
DPs1: All DPs to coordinate themselves to provide a detailed report to the HRH department/unit on the engagement of temporary and contract hires currently engaged through DP support
DFID + USG
December 2008
Summary report to the HRH department/unit
DPs2: Review the administrative models, mechanisms and costs for DP supported health workers and seek to standardise procedures and reduce transaction costs accordingly.
DFID + USG
December 2008
Summary report to the DPH‐K
DPs3: Initiate discussions with JICA on their intended support to Kenya and wider alignment with the Accra Agenda for Action
DFID + USG
November 2008
Meeting Notes
DPs 4: DFID and USG staff in Kenya to engage with GF, GAVI, UNICEF and other key partners to participate in a strategic, aligned approach to HRH
DFID + USG November 2008
Meeting Notes
DPs 5: Initiate discussions on the M&E framework to enable the measurement and review of health workforce scale‐up in Kenya
DFID + USG
November 2008
Meeting Notes
DPs 6: USG to consider an internal review of the existing CDC and USAID aid instruments that enable longer‐term financial commitments in a host country and the innovation required to adapt
USG November 2008
Internal discussions held and resulting actions noted.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 10 of 50
Recommendation Lead Target date Means of Verification
these to PEPFAR legislation
24. These recommendations are for ongoing dialogue and discussion between partners. Many are
complementary to each other and require continuing commitment to working in partnership, applying complementary strengths to take these forward.
25. Target dates are indicative. Representatives from the MoMS, MoPHS, and Development Partners in Health – Kenya (DPH‐K) along with USAID, CDC and DFID should consider and review these further.
26. Once the health Ministries provide their responses, further discussion between PEPFAR and DFID will be required to agree where their respective programming can support the implementation. Where long‐term or short‐term technical assistance is requested, clear agreement should be reached on the lead and capacity to implement within the necessary time frames; especially for actions related to the next round of the MTEF and AOP.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
1 Background / Introduction 1. In response to the critical Human Resources for Health (HRH) shortages in Africa, the UK
Department for International Development (DFID) and Office of the US Global Aids Coordinator (OGAC) responsible for the President’s Emergency Programme for AIDS Relief (PEPFAR) have been in discussion with a number of African countries (Ethiopia, Kenya, Mozambique and Zambia) to develop strategies and country level actions. The aim is to demonstrate the maximum flexibility of disease specific programmes to support broad based primary care in line with countries’ health plans. There is high level political support for this process in the UK and US. This was highlighted by the announcements of President George Bush and Prime Minister Gordon Brown in April and June 2008 committing to actions in the four countries ‘to support partner countries to increase health workforce coverage levels, with a view to work towards the World Health Organization goal of at least 2.3 health workers per 1,000 people’.
2. Further to coordination meetings in Addis Ababa (January 2008) and Kampala (March 2008)
DFID and OGAC agreed to field a team of two consultants to work with their respective leads in Kenya in the period 02‐13 September, 2008. Jim Campbell (INTEGRARE, Spain) was engaged by DFID and Barbara Stilwell (Capacity Project, USA) was made available under existing arrangements with PEPFAR/United States Agency for International Development (USAID). The main objective of the assignment was to facilitate agreement and document current flexibilities of funding streams for HRH (building on existing work and within national frameworks for health reform specific priority actions on HRH). The Terms of Reference (TOR) for the assignment is available as Annex 1.
3. This report presents a summary of the main findings from the country visit. Section 2 details the
context of HRH in Kenya. Section 3 reviews the respective activities of PEPFAR and DFID and their progress since the meeting in Addis Ababa. Opportunities to strengthen HRH development and implementation are presented in Section 4.
4. Method of working:
Pre‐ and on‐arrival briefing meetings were held with Tony Daly, Senior Health & HIV/AIDS, Advisor, DFID and Melahi Pons, Senior Health Sector Program Manager, USAID. These generated a list of key informants.
A list of people interviewed is appended as Annex 2. (Unfortunately and despite repeated efforts some of the key informants were unavailable to meet with the consultants)
Relevant documents were reviewed as an initial step to understanding context, as well as revealing gaps in information. A full list of the documents reviewed is appended as Annex 5.
Interviews were conducted by one or both consultants and the results recorded in note form. Any potential conflict of interest from one of the consultants in reviewing Capacity Project and LATH programming was avoided by having both consultants present in certain interviews and joint agreement on the findings.
5. During the country visit there were a number of developments across the health sector, demonstrating the rapidly changing environment. The Community Health Strategy was launched; a revision to employee health insurance deductions was proposed; the two Permanent Secretaries in the health Ministries were changed; there was an interruption to Global Funds mechanisms after $6m was unaccounted for, and; the announcement of 260 new hires (with GAVI support). All of this was published in the national press and without a robust system of internal communication in the health Ministries, could be deeply disruptive.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 11 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
2 National plans and strategies in Kenya 6. The scope of work had particular requests relating to Kenya’s national policy and planning
frameworks and their relation to HRH plans and priorities:
Liaise with other processes, such as development of a shadow budget and MTEF, and identify how DFID and PEPFAR funds can better align with these
Review public sector strengthening/reform and other HR related initiatives and their implications for increasing resources towards meeting the targeted ratio of health worker per population.HRH.
Review Kenya HRH plans and key priorities 7. Due consideration was therefore given to the wider government initiatives and planning
frameworks in which the health sector and the HRH planning and implementation operates. This includes:
GoK’s Vision2030; Transforming National Development; Medium Term Expenditure Framework (MTEF); Public Service Reform Strategy (PSRS); National Health Sector Strategic Plan II (2005‐10) (NHSSP II); Kenya Essential Package for Health (KEPH); Joint Programme of Work and Funding (JPWF); Ministry of Health’s Medium Term Plan (2008‐12) (MTP); Annual Operational Planning(AOP) process; Health Sector Plan 2007; Health Sector Plan 2008 and; Human Resources for Health Strategic Plan (2007/8‐2009/10) (HRH‐SP) draft of November 2007
Norms and Standards for Health Service Delivery (June 2006)
8. Given the recent and ongoing discussions between development partners and the GoK to advance a Sector Wide Approach (SWAp) for the health sector, the Code of Conduct (August 2007), the draft Joint Financing Agreement (version November 2007) and the Kenya Joint Assistance Strategy (2007‐12) (KJAS) were also reviewed.
9. An analysis of Kenya’s wider policy and planning frameworks are contained within the draft HRHSP. Further information is also available in the Health Sector Plans of 2007 and 2008 respectively. These plans influence the Budget Outlook Paper (BOPA) as part of the MTEF planning cycle and are available from the Ministry of Finance website.
10. In –country personnel from GoK, USAID, CDC and DFID are familiar with the above policies and
frameworks. Of key interest to this assignment are the overarching principles endorsed in the subsequent layers of policy and strategy (Vision 2030, PSRS, NHSSP, MTP, HRH‐SP) and the annual calendars within the planning and budgeting frameworks (MTEF, JPWF and AOP). Section 2.1 discusses the health and HRH implications whilst the planning frameworks are analysed below.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 12 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 13 of 50
11. The planning and budget instruments include the MTEF, the MTP and the AOP. The calendar of activities for the annual preparation and submission of the MTEF and the AOP are detailed below1: Table 1: MTEF and AOP planning activities
MTEF Activity Deadline AOP Activity
Develop MTEF Guidelines (09/10)
August 08
Launch of Sector Working Groups
August 08
Issue MTEF Guidelines September 08 Health Summit and launch of AOP IV (08/09)
Ministerial Public Expenditure Reviews (MPERs)
October – November 08
Develop Budget Outlook Paper (BOPA) with Stakeholder Consultation
October 08
Submission of District Inputs to Ministries
November 08 AOP V (09/10) Planning Schedule developed
Finalise Budget Outlook Paper
November 08
Finalise review of programmes and submit sector report to Treasury
December 08
January 09 Training on AOP V
Sector Hearings with Treasury & Ministry of Planning and National Development
February 09 Facility plans submitted to DHMTs
Publish Sector Reports March 09 District and Provincial plans submitted to HQ
Prepare and submit Budget Strategy Paper
March – April 09 Technical Support and Appraisal of plans
Develop itemised and indicative Programme Based Budgets
April 09
Review and finalisation of budget estimates
May 09 Presentation of plans to the Health Sector Coordination Committee
Publish indicative May 09
1 The calendar is based on 2007/8 procedures as taken from the AOP for the health sector and the Budget Outlook Paper 2008. New guidelines for 2008/9 may contain changes to this schedule of activities.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 14 of 50
MTEF Activity Deadline AOP Activity
Programme Based Budgets
Submission to Cabinet and Parliament
May – June 09
Confirm sector budgets for 09/10
June 09
12. The table highlights that it will be essential for both PEPFAR and DFID to engage in the planning
process for 2009/10 from October 2008 if they wish to influence the GoK resources available for health systems strengthening and HRH development in the next Budget Outlook Paper, Sector Report and Programme‐based Budget. Given the emphasis in the PEPFAR reauthorisation to consider how country activities are developed within a country compact or framework, this presents a timely opportunity for USAID/CDC in Kenya.
13. There are positive signs of improvement in the existing Budget Outlook Paper of 2008. Allocations to the Health sector demonstrate actual and percentage growth in the period July 2007‐June 2011 even if they are still considerably below the 15% commitment in the Abuja Declaration. Projections on the economic outlook as part of the wider macroeconomic framework anticipate 10% growth p.a from 2012/13, which is suggestive of additional resources being available for the next Health Sector Strategic Plan. If overall health spending is also increased in line with the Abuja target, there could be considerable increases in recurrent expenditures.
Table 2: Health Ceilings –Expenditure (Ksh Million) 2007/8 – 2010/11
Expenditure %Share of Government totals
2007/8 Est
2008/9 Ceiling
2009/10 Proj
2010/11 Proj
2007/8 Est
2008/9 Ceiling
2009/10 Proj
2010/11 Proj
Recurrent 22,745 25,209 30,124 30,726 6.7% 7.7% 8.5% 8.5%
Development 11,609 12,191 12,800 13,440 5.8% 7.8% 8.2% 8.2%
Total 34,354 37.400 42,924 44,167 6.4% 7.8% 8.4% 8.4%
Source: GoK, Budget Outlook Paper 2008/09‐2010/11, January 2008.
14. During the mission we were also informed that this year’s budget includes the resources to hire 1,000 health workers2 and to absorb up to 600 health workers who are currently employed through various alternative hiring models, including the USAID supported Emergency Hiring Plan (EHP) (discussed in further depth in section 2.1 and 3.1)
2.1 National plans and strategies related to HRH
15. The health sector in Kenya operates within a national policy environment that is consistently
moving Kenya towards more accessible, equitable and affordable health care. The Economic
2 Further clarification is required on whether the budget line for the 1.000 workers is over and above the replacement of staff that leave existing posts. Attrition is estimated at 1,200 staff per annum (Marsden & Chirchir, 2008).

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Recovery Strategy, implemented from 2003‐7, aimed to create an efficient and motivated public service, including the health sector. Kenya Vision 2030 envisions the public sector continuing to contribute to the economic development of the country and that in particular the health sector, the social pillar of Vision 2030, will promote health to reduce the disease burden. To do this, the health sector is being restructured with a new emphasis on improving resources to community health centres. A National Social Health Insurance Fund was proposed in the NHSSP II, to promote equity and efficiency in Kenya’s health financing system. However, implementation of this scheme has stalled, and a working group was formed in 2007 to develop a health financing strategy. Social Health Insurance is still one option being considered, though among others. Kenya has the oldest health insurance mechanisms in Africa, with the National Hospital Insurance Fund (NHIP). The impact of this coverage has improved considerably in recent years, though its benefit ratio remains low in comparison to international standards.
16. The Public Service Reform Strategy (PSRS) aims to ensure that Kenya has an efficient and effective public service that functions ethically, is citizen focused and results oriented. In support of these aims, a Human Resource Management (HRM) strategy has been put in place, to introduce value driven, competency based HRM practices, as well as resolve wage‐bill issues. Performance appraisal has just been introduced throughout the health workforce in support of HRM reforms. The report of the mid‐term review of the implementation of the NHSSP II comments on the slow implementation of the HRH management strategies because of a lack of strong, coordinated leadership at Ministry level. In view of the new Ministry structures, this will continue to be a challenge. The HRM strategy, that focuses on creating a conducive working environment, coupled with results based management, has great potential to improve workforce performance, but only if there are the resources – human and financial – to implement the strategy.
17. Kenya is a signatory to the United Nations Millennium Declaration and is committed to
substantially improving maternal and child health as well as to halting and reversing the spread of HIV/AIDS, Tuberculosis and Malaria by 2015.
18. The health sector is an essential component in achieving Kenya’s vision for health. The National
Health Sector Strategic Plan II (2005‐2010) spells out the MOH’s vision as “An efficient and high quality health care system that is accessible, equitable and affordable for every Kenyan” and the mission as “To promote and participate in the provision of integrated and high quality promotive, preventive, curative and rehabilitative health care services to all Kenyans”. The goal of the health sector as defined in NHSSP II is to reduce health inequalities and to reverse the downward trend in health related outcome and impact indicators of the health sector.
19. The NHSSP II is supported by Annual Operational Plans to promote implementation of the plan.
AOP 4 was reviewed during this consultancy: it is comprehensive and detailed, setting out activities, targets and costs for HRH development from community level upwards. The AOP links national level plans and priorities with local ones. There is, nevertheless, a recognition that training for managers throughout the health system is necessary to ensure that plans are realistic and achievable. Some training has been given, and more is planned. Developing the quality of management and leadership, to plan strategically, manage for results and improve coordination is key to improving outcomes.
20. One of the major strategies in the NHSSP II was the design of a Sector Wide Approach (SWAp) to
foster partnership in the health sector. Partnership has been seen as one way of recognizing the contributions to service delivery and financing of other partners such as NGOs and faith‐based organisations. Building on the goodwill created by efforts at the global level to increase aid
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 15 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 16 of 50
harmonisation and effectiveness based on the Paris Declaration in 20003, beginning July 2005 the ministry embarked on a Kenya Health SWAp design process.
21. As part of the SWAp process, a Joint Program of Work and Funding (JPWF) for 2006‐2010 was
developed in 2006 to elaborate the priority health interventions to achieve the NHSSP II policy objectives. The JPWF was to be adopted in 2006 and used to guide and coordinate the activities implemented by all players in the health sector, with most partners focusing their support to specific aspects of the JPWF and the annual operational plans (AOPs) that are developed in line with JPWF4. However, it remains unclear whether the JPWF was officially adopted.
22. The Kenya Essential Package for Health (KEPH) focuses on public health issues through a
common services approach. It organises the health sector through six levels of care, with staffing norms and standards set out for each level. Level 1 in the KEPH refers to the specific approach to community health described in the Kenya Community Strategy. Implementing the community health strategy will require significant investment in recruiting and retaining staff, and this will be discussed in more detail later in the report. The goal of the KEPH is to contribute to achieving the MDGs through providing integrated health services especially to poor women and children.
23. It is within this comprehensive policy framework of national and international health goals and
commitments that the Human Resources for Health Strategic Plan (HRHSP) 2007/8‐2009/10 has been developed and is aligned. The Plan is a result of a highly participative process, in which key stakeholder representatives reviewed documents and consulted individuals and organizations so that major HRH issues were verified. The HRHSP sets out to achieve 5 key outputs:
Appropriate number and type of health workers in post and equitably distributed Improved retention of health workers in post at all levels Improved institutional and health worker performance Strengthened human resource development systems and practices Strengthened human resource planning and management and leadership at all levels
2.1.1 Implementing Strategic Changes for Human Resources Development
24. Despite the supportive policy framework for HRH development, and implementation strategies
that accompany plans and policies, there is little substantial change. This must be, at least in part, due to the rapidly changing policy and political environment of the country. Post‐election disruptions were severe and had effects that are as yet undocumented. Even before this, the mid‐term review of the NHSSP II noted that:
‘The multiplicity of stakeholders involved in HRH requires robust coordinating structures and mechanisms to ensure ……..coordination across the sector. The fragmentation and weak coordination of the HR function within MOH headquarters is contributing to weak and inefficient HR practices and reduces the sector’s ability to maintain a strategic HR perspective.’ 5
3 The US Government adheres to the principles of the Paris Declaration but is not a signatory 4 Government of Kenya; Ministry of Health. Medium Term Plan 2008‐2012 5 Draft NHSSP II Midterm Review Report August 2007. P43

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 17 of 50
25. Post‐election reorganization has resulted in the Ministry of Health splitting into two: the Ministry of Public Health and Sanitation (MOPHS) and the Ministry of Medical Services (MOMS). This has the potential to fragment HRH development and administration even more. The two Ministries continue to share one building, which could foster communication.
26. In the following sub‐sections each of the five expected outcomes of the HRHSP will be discussed highlighting current issues, achievements and challenges for implementation of the plans for action in the remaining two years of the HRHSP.
2.1.2 Achieving an appropriate number and type of health workers in post, equitably distributed across the country
27. In 2006 the World Health Report identified Kenya as one of 57 ‘crisis countries’ with an absolute
shortage of health workers. The figures used for the calculation of ratios of health workers to population were from 2002, and scrutiny of the more recent figures suggest that even by 2006 Kenya was making progress towards having the requisite number of workers to deliver basic services. Table 3 demonstrates Kenya’s positive progress and comparison to other countries in the region. Table 3: Comparison of health personnel indicators in selected countries
Country Doctors/1000 population
Nurses/Midwives/1000 population
Health workersa/1000 population
Kenya (2007) 0.16 1.53 1.69
Kenya (2003) 0.15 1.33 1.48
Malawi 0.02 0.59 0.61
Mozambique 0.03 0.32 0.35
Uganda 0.08 0.72 0.80
Sources: Kenya MoH data 2007; World Health Report 2006; Kenya Mapping and Verification Exercise, 2004. a Totals based on Doctors, Nurses and Midwives in line with WHO indicator
28. There is still no definitive data source for staffing in the health sector in Kenya. In the public
sector the Integrated Personnel Payroll Database (IPPD) captures staff on the public sector payroll, as well as other biographical information. A nursing database has been developed through a collaboration involving Emory University and CDC, and funded by PEPFAR through CDC. This database is in use by the Chief Nurse and colleagues in the MOMS. Underway are initiatives to develop further profession specific databases and then to align them with the Health Management Information System (HMIS), as well as the data available from the Christian Health Association of Kenya, the private for profit sector, the performance management system, the disciplinary system and the systems for contract staff employed for projects. This would create one comprehensive database, which is essential for projections and planning (see later discussion).
29. Staffing levels currently fall below the establishment norms, and there is a strong urban bias to distribution, so that access to a health worker in rural areas and for hard to reach populations, is poor. It was estimated in the 2004 mapping and verification study6 that 3% of dispensaries have
6 Ministry of Health, December 2004. Human Resources Mapping and Verification Exercise

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 18 of 50
no qualified health staff to administer drugs. There is a reported disparity in staffing of doctors at district level, with almost half the district hospitals having fewer than 6 doctors out of the establishment of 12, while others may have 20 doctors.
30. The data available7 shows that there are many more health professionals registered in Kenya than practice in the public sector. The number of registered and enrolled nurses, for example, rose from 40,081 in 2004 to 55,169 in 2007, on the nursing register. However, the number of nurses employed in the public sector has apparently fallen from 16,146 in 2004 to 15,036 in 2007. What is not known for sure is the number of nurses, or other health workers, in the sub‐sectors (NGO, FBO, PFP, PNFP) or how many are actually unemployed. As there are many applications for a small number of jobs, high unemployment seems likely. Table 4: Nurse Registration v public sector employment (2004‐2007)
registered nurses employed in public sector
% of registered nurses employed in public
sector
2004 40,081 16,146 40%
2007 55,169 15,036 27%
31. The challenges to improving recruitment seem to be twofold. Firstly, there have been
restrictions on public sector recruitment, though recently these have been made more flexible to allow for medical personnel to ‘reach the optimum level ….to achieve the MDGs’. Secondly, the recruitment procedures are cumbersome, lengthy and have been subject to abuse because of lack of sufficient controls. The success of fair, streamlined recruitment has been demonstrated by the Capacity Project and others in their ‘emergency hire’ procedures. Currently recruitment to the public sector is almost three times the rate of attrition, though 2006 is the first year that this has been reported. Over the last 7 years, average recruitment figures have approximately equalled annual attrition, which has not allowed for any scaling up8. In terms of donor support, this does suggest that targeting recruitment has been essential to meet this HRHSP goal.
32. The HRHSP has to address staffing issues resulting from the reorganization of health care
delivery into six levels of care, and the staffing standards associated with each level. Perhaps the biggest change will be at the interface between community and the health sector, where it is proposed that a cadre of voluntary workers – Community Owned Resource Persons (CORPS)‐ be introduced. The CORPS will have a role that centres on empowering the community through education related to health. Each group of 5,000 people will have 50 CORPS, supported by a village health committee and supervised by 2 Community Health Extension Workers (CHEWS), who will be trained community nurses or Public Health Technicians.
33. A key concern moves beyond numbers to the competence of the health workers to give the
requisite care in their settings. This is especially important in providing skilled attendance at birth. Currently, all nurses are trained also in midwifery, and this is vital. It is not clear how competent CORPS and CHEWS will be, or how Traditional Birth Attendants (existing in parts of Kenya) will be accommodated within the envisaged community health care arrangements.
7 Human Resources for Health Strategic Plan 2007/8‐2009/10, Ministry of Health, Government of Kenya. P19 8 Human Resources for Health Strategic Plan 2007/8‐2009/10, Ministry of Health, Government of Kenya.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 19 of 50
34. To succeed in planning the huge increase in staff required to deliver the KEPH a more dynamic planning mechanism will be required, that moves away from planning against an established workforce, to using projections, building scenarios and looking at cost‐effective options, including even doing a competency assessment across the workforce. Other approaches that could be used include a needs‐based assessment, that estimate future health workforce needs based on the projected health service needs (both met and unmet) of the current population, adjusted for age and gender, while demand‐based approaches project future health service requirements based on present health service utilization9.
35. Clearly, coordination across the two Ministries will have to be seamless, and joint planning seems to be essential. Budgetary controls will have to be discussed, against the projections for the GOK taking over the employment of staff hired for projects and programs. Data‐based decision‐making for policy‐makers is an essential part of this process.
36. Deployment of staff to rural areas is a chronic problem in Kenya. For this to change the factors
that influence the decision to move away from less popular facilities has to be better understood, and there is a study underway10. A recent study on the migration of health workers reports on a survey of 12 health facilities. 57% of the staff who responded to the survey reported being unhappy with their jobs and of these, 38% expressed a wish to be posted elsewhere in Kenya. The main reasons for dissatisfaction were poor income, shortage of staff, long work hours and inadequate resources. Also mentioned were poor housing, and lack of opportunities for career improvement11.
37. Tackling deployment must involve addressing the factors that have been identified in previous
studies and will be reinforced by current ones. This may mean designing and testing packages of incentives with donor support. It will certainly mean revising the hardship allowances and ensuring that they compensate all professions equally. Further work is required to map the distribution of health workers and inform this debate.
2.1.3 Improved retention of health workers at all levels
38. Improving retention is related to deployment measures, but also to pay and conditions.
Government salary reviews appear to be attracting health workers back into the public health system, possibly resulting in a reported drop in patient throughput in FBOs. To maximise efficiencies in service delivery, there should be harmonization of terms and conditions across the sector.
39. In general, attrition seems to be low at around 2% per year, though all those leaving may not be
captured on the current data systems. This needs more investigation. 40. Recent hiring initiatives supported by development partners are reporting improved retention
of health workers. The Clinton Foundation initiative, supported by DANIDA, is reporting 97%‐98% retention of its first cohort engaged12. Contributing factors include the high unemployment
9 A full appraisal of planning mechanisms can be found at http://www.capacityproject.org/images/stories/files/techbrief_12.pdf 10 Led by the KEMRI‐Wellcome Trust 11 Mwaniki DL, Dulo CO, (2008) Managing the migration of human resources for health in Kenya: the impact on service delivery’. EQUINET Discussion Paper Series 55. EQUINET, IOM, Kenya Technical Working Group for Managing Migration of Health Workers, EAC and ECSA HC, EQUINET, Harare 12 Personal communication with Gerald Macharia, Country Director, Clinton Foundation.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
amongst health workers, better screening of applicants and their preferred choice of posting, the 3‐year contract duration, and the option to transfer into a government post at the end of contract. In other initiatives the use of a gratuity payment (in lieu of pension contributions) upon completion of the contract is also being reported as a significant motivation promoting similar retention levels. Opening up posts to allow promotion is essential to retention and this is now being done at senior levels.
2.1.4 Improved institutional and health worker performance
41. The National Performance Management Framework will hold institutions and individuals
accountable for the achievement of targeted results. In addition, a new Government Performance Appraisal System is in place, recognising that strengthening staff performance is critical to productivity in the public sector.
42. Improving management and leadership will be essential to support performance improvement and this is already an anticipated output of the HRHSP and will be discussed later in this section.
43. Of equal importance is improving the workplace climate to motivate staff to be more productive,
which includes reducing absences. The Capacity Project is currently implementing a workplace climate improvement program with the support of MSH. This remains a relatively small‐scale programme targeting 14‐20 teams.
44. Addressing wider determinants of productivity will however require additional approaches and
could be tackled as part of the equitable distribution of staff across facilities, levels of care and geographical location.
2.1.5 Strengthened human resource development systems and practices
45. Time constraints prevented a full exploration of the educational system and its responsiveness
to the needs of developing human resources for health. It is clear, though, that the expansion of the workforce, with changing roles and practices, will have educational implications. A National Training Policy has recently been put in place and will underpin developments in pre‐service and in‐service training. New initiatives from the Clinton Foundation (condensing professional education) and the recent report of the GHWA Task Force on Scaling‐up Education and Training offer scope for innovation in medical education which Kenya may wish to review.
46. Comments were made by some interviewees about the outdated educational practices to be found. This is reflected in the HRHSP where it is recommended that as much in‐service training is done on‐the‐job and by coaching and mentoring, to reduce absence from the workplace. Distance learning approaches can also be explored.
47. The number of trainees enrolled in medicine and nursing programs across Kenya has increased
since 2002, though it is reported that limited practicum sites make it difficult for students to get the practice they need. A recent decision has been made to pay the (previously unpaid) intern nurses, studying on the graduate course, who have to undertake practical work in order to qualify. This will add to the attraction of nursing as a profession and may increase intake.
48. It is likely that the graduates of these programs are not all recruited by the public health
system. Further work will be needed to explore the absorption capacity of the system so that joint planning can be done between education and service delivery.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 20 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
2.1.6 Strengthened human resource planning and management and leadership at all levels
49. Key to the success of the HRHSP is the capacity of managers at all levels to envision, lead and
implement change successfully. Currently management is highly centralized at the Ministry level, and while there is a government commitment to decentralization, this has not been put into operation to any great extent.
50. Strategic oversight is required at Ministry level so that HRH plans are dynamic and evolving as the health sector itself evolves. Currently it is not clear that such strategic oversight can be put in place, as the two Ministries have separate HR functions, databases are not harmonized and effective communications within the Ministries seem as yet not to be developed.
51. The systemic nature of human resources development becomes apparent in looking at the
outputs of the HRHSP. It is impossible to undertake effective planning without good data. Ensuring absorption of all students is impossible without good joint planning. Improving recruitment, retention and performance will only be possible with attention to motivation and the workplace climate. The HRHSP tackles all aspects of systems development for HRH and is to be commended.
52. Management Information Systems (MIS). The HRH Strategic Plan, which has considered MIS in
great depth, clearly states the deficiencies in current data and information. PEPFAR’s ongoing activities recognize the need to develop capacity in the more effective use of technology and management information systems. This includes the Emory University‐CDC collaboration to develop a ‘Health Workforce Surveillance System’ and a Human Resource Information System (HRIS) and a national training database within the Capacity Project. A Technical Working Group (TWG) led by the former MoH has oversight of these and other initiatives and how they link to GoK systems, including the national Integrated Personnel and Payroll Database (IPPD).
53. Some confusion seems to exist on the role of the various initiatives and their respective merits, including issues on hardware, software and licensing. This discussion within the TWG is warranted and the respective experts should look to ensure compatibility and sustainability across the initiatives. However, the overarching concern should relate to the demand for information and how the respective initiatives can individually and collectively respond. Areas of demand include personnel administration, management, research and policy/planning development
54. From our initial review, the ongoing approaches appear to have their respective strengths. The
‘workforce surveillance system’ is already being used to influence policy and planning in the nursing workforce, especially related to the prevention and treatment of HIV/AIDS. As it expands the records on Physicians, Laboratory Technicians and Clinical Officers, and given its management linkages with CDC Kenya and Atlanta, it also offers significant potential to develop sector‐wide scenario‐based planning linked to burden of disease and geographical information systems. This functionality would ideally be integrated into their analysis and reporting capabilities in the near future and linked to the development work in the HRH Strategy. In parallel, the HRIS will support the administrative and management requirements associated with employed personnel and will serve to streamline many of the existing HR processes and archives.
55. In terms of ensuring further attention to capacity development the current status of information management and the increasing demand for evidence on which to base education,
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 21 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 22 of 50
training, deployment and longer‐term financing needs requires a comprehensive health sector approach that involves all actors from the wider health economy. The recommendations within the HRH Strategic Plan (see Figure below) remain valid and can serve as the basis for ongoing support. Figure 1: ‘Information Systems’ –Commentary from the HRH Strategic Plan
To plan for the health workforce and to make informed recruitment and deployment decisions requires accurate and up‐to date information for the entire health sector (public and non‐public health workers). The Integrated Personnel and Pay Database (IPPD), data from the Mapping Study and the nursing database developed as part of the Kenya Nursing Workforce Project (led by Centre for Disease Control and the Kenya Nursing Council) have improved the HR information available to plan, manage and develop the health workforce. However there is still a need to improve the consolidation, quality, consistency and utilisation of HR information and a more comprehensive and sector wide HR information system is required for policy formulation and HR decision making across the health sector. Accurate and up‐to‐date information is required on the current numbers of staff in post and distribution across the whole sector, on current and projected supply from the labour market and training institutions to meet service delivery needs and to inform recruitment and deployment decisions. A MoH Human Resource Information Systems (HRIS) Technical Working Group was established in 2006 and is supporting the MoH to strengthen HR information systems.
56. Due consideration should also be given to aligning further HRIS development with guidance from
the World Health Organisation and the Health Metrics Network. The former has recently developed a Toolkit for Monitoring Health Systems Strengthening13 and HMN has issued the Second Edition of its Framework and Standards for Country Information Systems14
13 Available online at: http://www.who.int/healthinfo/statistics/toolkit_hss/en/index.html 14 Available online at: http://www.who.int/healthmetrics/documents/framework/en/index.html

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 23 of 50
3 Findings on PEPFAR and DFID supporting activities 57. The TOR requested the mission consider the following three key elements with respect to
PEPFAR and DFID support:
Assess current support for HRH supported by PEPFAR and DFID through review of respective country assistance plans, and identify future opportunities for expanding and improving such support, both direct and indirect, to increase its impact on HR capacity building
Document the extent of current PEPFAR support to human capacity building. Review results specifically referring to Kenya of the initial PEPFAR‐DFID HRH meeting in Ethiopia and consider progress made
3.1 ‘PEPFAR’ Kenya
58. Kenya has experienced an increasing growth in PEPFAR funding since initial activities commenced. It received nearly $92.5 million in Fiscal Year (FY) 2004, more than $142.9 million in FY 2005, approximately $208.3 million in FY 2006, and $368.1 million in FY 2007. This has risen to $534.8 million in FY 200815
59. Capacity Development. The 2008 Country Operational Plan (COP) and Reporting System (COPRS) were reviewed to estimate the volume of resources targeted to Human Capacity Development. The exercise that was conducted in Mozambique (using specific filters in the database which identify programme activities that have ‘Emphasis Areas’ of capacity support16) was repeated, resulting in a figure for Kenya of $334.3m (62%). This is considerably higher than in Mozambique (39%) and may reflect various factors, including the absorption capacity within Kenya or the interpretation and categorisation of activity descriptions at the time of data entry. Time restrictions limited a detailed assessment of this higher percentage, however, the information gathered from interviews and meetings presented a positive focus on capacity development which may not be fully appreciated outside of the immediate implementing partners and US Agencies17.
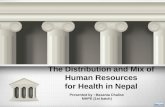
Figure 2: HRH Action Framework 60. PEPFAR recognises that one
of the key challenges in Kenya is human resource management18. Initiatives are underway to provide the GoK with support across most of the six major areas of the HRH Action Framework (Policy, Education, Partnership, Leadership, Management Systems and
15 Data taken from PEPFAR website: http://www.pepfar.gov/press/81596.htm 16 ‘Human Capacity Development’ + ‘Local Organisation Capacity Building’ + ‘Wraparound Programmes’. 17 Whilst this report refers to ‘PEPFAR’, the actual implementation is through various agencies. USAID and CDC manage the majority of funds and partner activities. 18 PEPFAR. Kenya: 2008 Country Profile. http://www.pepfar.gov/press/81596.htm

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 24 of 50
Finance)19. Examples include: supporting the development of an HRH Strategy; pre‐service and in‐service training across various cadres and services supported by a Training Policy; data management and development on service‐delivery and the health workforce ‐ including a Health Workforce Surveillance System and a Human Resource Information System; and direct salary support. An HIV/AIDS Fellowship programme modelled on success in Uganda and Zimbabwe sets out to enhance human capacity for the longer‐term requirements.
61. The various initiatives collectively contribute to the foundations for further implementation of
the HRH Strategy and its five priority objectives. This is aided by the USAID‐funded Capacity Project that seeks to take a holistic approach to HR management and act as a catalyst in support of government leadership on the HRH agenda. Capacity Project activities include the secondment of advisory staff in positions which may influence change; policy and strategy development; HR Information Systems and; active leadership in the Emergency Hiring Plan (EHP).
62. Direct Salary Support. The PEPFAR initiatives providing direct salary support to health workers
merits further exploration. The available evidence suggests that unless critical cadres of health workers are expanded, the former MoH’s ambitious coverage and treatment targets within the KEPH and NHSSP II (supported by PEPFAR interventions) will be difficult if not impossible to achieve.
63. Given that there is a pool of qualified, unemployed health care workers (estimates suggest that
there are some 6,00020 ‐7,36021 unemployed health workers) and an additional 7,250 nurses in pre‐service training22 who may have added difficulty in securing employment given a 5‐year increase in the compulsory retirement age23 24 one of the critical factors to address HRH in Kenya will be developing effective mechanisms to engage these trained staff.
64. The EHP is supporting the former MoH to rapidly hire, train and deploy health workers to
facilities where there are persistent staffing shortages. The Mid‐Term Review of this initiative (February 2008) reported that 849 workers had been deployed to 200 government and faith‐based facilities in 66 of the neediest districts in Kenya. Salaries are paid using PEPFAR funds with checks and balances on attendance. Salary disbursement is via Deloitte as a third‐party payment agency.
65. Further work had been undertaken with the MoH Planning Unit and the Ministry of Planning and
National Development to ensure that all EHP‐supported posts are factored into the GoK’s MTEF budget forecasts in order to absorb these staff into the government payroll. As indicated earlier, the 2008/9 Budget allows for the absorption of up to 600 health workers, which includes the first‐wave of 113 PEPFAR‐funded recruits from May 2006 (entering the government payroll in May 2009).
19 The HRH Action Framework is available at: http://www.capacityproject.org/framework/ 20 Personal communication with Kimani MUNGAI, Capacity Project, Kenya. 21 Adano U. (2008). The health worker recruitment and deployment process in Kenya: an emergency hiring program. Human Resources for Health 2008, 6:19 22 Data provided by Health Workforce Surveillance System (Emory/CDC project) from student indexing. 23 During the mission we were informed of a policy decision to amend the compulsory retirement age from 55 years to 60 years for public servants. This may have a considerable impact on retirement, career progression and new intakes, with nursing as the largest cadre being most affected. 24 Calculations from the Health Workforce Surveillance System suggest that in the next 5 years 2,639 experienced nurses will be retained in the public sector as a result of this policy decision.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 25 of 50
66. Aside from the EHP mechanism, there are various other models to deploy and fund health workers’ salaries. The Global Fund, GAVI, UNICEF and the Clinton Foundation (with DANIDA funding) have all established similar initiatives to support health workers’ salaries on a temporary basis. The models, duration of contract and mechanisms for payment transfer vary, but the principle remains the same. Over 3,000 health workers were recruited under these schemes in 200625. As discussed earlier, the retention level in one of the schemes is reported as 97‐98%26, an incredible success given the wider concerns on terms and conditions and retention in the public service. Definitive figures for 2007 and 2008 are not readily available but there appears to be an expansion of these hiring mechanisms by various partners and this will require further analysis (see Table 5 for an indication of PEPFAR support).
67. Whilst the diversity in the mechanisms and approaches is expected across Development
Partners, it was also noted that PEPFAR funds are supporting salaries in various models. A survey to count PEPFAR‐supported Health Care Workers for COP 2009 was underway at the time of the visit and figures originating from COP07 and COP08 were also made available. COP09 returns suggest that there are almost 10,000 health workers supported by PEPFAR funding.
Table 5: PEPFAR‐supported health care workers in Kenya
Agency COP07 COP08~ COP09*
USAID 2656 2897 5612
CDC 3469 4702 3917
DOD 256 347 369
Totals 6381 7946 9898
~COP08 – incomplete reporting so figures may be higher *COP09 –returns from implementing partners at time of this report, so figures may be higher.
68. Whilst these ‘head‐count’ figures have to be treated with some caution (they are based on
projected COP activities rather than actual attainment27) they represent a major investment in the Kenyan health system across a wide‐range of professional and clinical cadres addressing service‐delivery, community interventions, management, administration, research, policy/planning and advisory roles. The current survey tool, however, does not enable a breakdown of their roles beyond three categories or a calculation of the actual PEPFAR dollars invested in health workers’ salaries.
69. It is the diversity of support that has led to diversity in the hiring models. CDC holds Cooperative Agreements direct with Parastatal Organisations and contribute salary payments. APHIA II projects with USAID employ differing procedures to make salary payments to an estimated 496 workers. An implementing partner in Central Province makes payment to the Provincial Health Office which subsequently manages the payroll for 120 workers (a model similar to a capacity building initiative noted in Mozambique). Other partners work though Faith‐Based Organisations. New initiatives are planned to support Community Health Workers in COP09 and the mechanisms for this intervention are also likely to differ.
25 Marsden & Chirchir (2008) Mid‐Term Evaluation of the Kenya EHP. 26 Personal communication with Gerald MACHARIA, Country Director, Clinton Foundation. 27 A visit to Central Province reviewed the process of engagement for one of the CDC projects. A negative difference of 10.5% was noted between projected COP activities and actual hires.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 26 of 50
70. Given the projected scale of PEPFAR support in FY08 (7,600 workers) it deserves further consideration on the associated costs, including the transaction and marginal costs. APHIA II salary contributions are estimated at $2.65 million for their 496 hires28. A figure of $1.91 million has been projected to cover the salary costs of 661 hires from the EHP29. Salary costs per health worker are therefore in the range of $2,895 – $5,350 per annum using these calculations. Taking these as indicative of the salaries offered across other PEPFAR initiatives, and for discussion purposes in this report, an average rate would suggest a COP08 investment in the 7,600 health worker salaries of $31million (range $22 – $41 million). Whilst there are many caveats to these indicative calculations the figure is nonetheless representative of a major investment and circa 10% (range 7%‐12%) of the Capacity Development spend identified from the COPRS30.
71. It was noted that the consolidation of the various hiring models is under discussion and some
work has been initiated to integrate the APHIA II hires into the Capacity Project system. Progress in this area is welcomed to enable greater analysis and interpretation of the PEPFAR‐funded hires and their potential absorption into the government payroll. But whilst this will facilitate planning and scenario‐building and addresses financial management concerns there needs to be similar attention to cost. As an example the administrative overheads associated with the integration of the APHIA II hires into the Capacity Project model range from 6%‐13% (see Table 6 below) as against 11% in the Capacity Project model3132. The range in gratuity allowances is also of note (12%‐23%) and would ideally be standardised.
Table 6: APHIA II Health Worker Costings 2008/9 (by Province)
W este r n $ % o f sa la ry Ny anza $ % of sal ar yS a la rie s 452 ,753 Sa la r ie s 2 17 ,014
G ra tu i ty 60 ,092 13% Gra tu ity 34 ,991 16%
A dm i n is tr a tion 30 ,696 7% Ad m in is t ra ti on 20 ,754 10%A ve r a ge sa la r y 5 ,521 Av e ra g e sa la ry 4 ,173
N EP $ % o f sa la ry Na ir obi $ % of sal ar y
S a la rie s 146 ,589 Sa la r ie s 1 64 ,710 G ra tu i ty 31 ,828 22% Gra tu ity 19 ,841 12%
A dm i n is tr a tion 16 ,778 11% Ad m in is t ra ti on 10 ,290 6%A ve r a ge sa la r y 3 ,665 Av e ra g e sa la ry 5 ,883
E a s te r n $ % o f sa la ry Centr a l $ % of sal ar y
S a la rie s 89 ,081 Sa la r ie s 87 ,849 G ra tu i ty 14 ,469 16% Gra tu ity 20 ,643 23%
A dm i n is tr a tion 11 ,258 13% Ad m in is t ra ti on 10 ,812 12%
A ve r a ge sa la r y 4 ,454 Av e ra g e sa la ry 3 ,993
C oa st $ % o f sa la ry Rift V al le y $ % of sal ar yS a la rie s 443 ,274 Sa la r ie s 5 21 ,020
G ra tu i ty 73 ,256 17% Gra tu ity 86 ,608 17%A dm i n is tr a tion 41 ,882 9% Ad m in is t ra ti on 47 ,137 9%
A ve r a ge sa la r y 3 ,789 Av e ra g e sa la ry 3 ,859 Source: adapted from data provided by the Capacity Project, 2008.
28 USAID/Capacity Project – internal document 29 Marsden & Chirchir (2008) Mid‐Term Evaluation of the Kenya EHP. 30 The indicative figures should not be taken out of context of this report and require more detailed investigation to ascertain the precise values and percentages. 31 Personal communication with Kimani MUNGAI. 32 Under previous arrangements APHIA II partners calculated overhead or indirect costs between 20‐30%. (Personal communication with Melahi PONS)

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 27 of 50
72. nuary meeting was to finalise and
73. In addition the Chair also took the decision to approve the recommendation of this assignment
4. A further area of attention noted in Ethiopia was the need to maximise the flexibilities of donor
75. Despite the HRH Strategic Plan not being formally adopted, PEPFAR‐funded activities continue to
76. Alignment with government planning. As evident in the Mozambique case‐study, PEPFAR
77. Tec assistance is often provided to enable government officials to develop their AOPs, and
78. If difficulties do arise in financing and disbursement, several respondents indicated this was
79. Wit an emphasis on strategic partnerships in the PEPFAR reauthorisation, moving from an
Progress since Addis Adaba. One of the key priorities at the Jaimplement the HRH plan. PEPFAR support via the Capacity Project enabled the completion of the draft HRH Plan which was duly shared with the former MoH in late 2007. As discussed earlier, events in Kenya and the division of the former MoH to two Ministries has meant that the HRH Plan has not been formally adopted for implementation. However, at the debriefing meeting with Ministry staff on Friday 12th September, a decision was taken by the Chair, Dr. Sharrif, to have the document submitted to both the new Permanent Secretaries for signature and adoption by Friday 19th September. A small working group would then convene to revisit the plan and update the 3‐year workplan and implementation schedule.
in respect to common management arrangements for HRH across the two Ministries. Building on an original proposal in the HRH Strategy that an HRH unit/department be established to coordinate the implementation of the Strategy, this has become even more imperative with the separation of roles and responsibilities into two health Ministries. Similarly, the creation of an HRH unit/department as part of the overall strategy was to be submitted to the new Permanent Secretaries for their adoption.
7
funding. PEPFAR’s reauthorisation in July 2008 can be seen as a positive step forward that will enable greater flexibility. Much though will depend on the innovation and direction of activities at country level to maximise on the potential of the new PEPFAR legislation and the central buy‐in to enable this. Options for discussion are presented in Section 4.
address the strategic priorities and objectives identified. Given the upheaval in Kenyan society and the former MoH, PEPFAR partners have done well to maintain momentum with their respective counterparts.
mechanisms for planning and financial disbursement in Kenya are generally viewed positively. The planning process for the annual COP is not specifically aligned to the GoK’s AOP and MTEF process, but respondents offered positive examples of joint planning and development with government partners at central, provincial and district levels.
hnical
the resulting priorities are subsequently integrated into the prime partners’ COP submissions to PEPFAR. Once the COP is collated, it is subsequently reviewed with GoK representatives. For the COP09, this review is scheduled at the end of October 2008. The GoK will thus be informed of activities and indicative PEPFAR funding levels in advance of finalising their Budget Outlook Paper (BOPA) in November and the next round of MTEF preparations (see Table 1).
often due to insufficient planning in the COP process by the implementing partner or a lack of attention to the ‘burn‐rate’ (anticipated monthly expenditures against the workplan). Checks and balances for more serious financial infringements exist and are applied in some instances; however detailed examples of this within the PEPFAR portfolio were not explored further.
h
‘emergency’ programme to a development intervention, the current cooperation and coordination modalities may need to be reviewed. There is recognition of a need for a more

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 28 of 50
deliberate and proactive integration process between the AOP and the COP and vice‐versa 33. Whilst the current calendar supports the integration of AOP priorities into the COP, there were few examples offered of how PEPFAR’s added value on HRH (with the flexibilities and speed of disbursement) is proactively integrated into the AOP planning process. High‐level discussions with the Permanent Secretaries have been conducted and this process will continue in anticipation of COP2010 but in the case of HRH none of the respondents interviewed indicated that they have been involved in a country‐forum to interpret the PEPFAR reauthorisation and consider, and prepare for, new strategic actions.
80. It was encouraging to learn that USAID is initiating a health sector coordination and information‐
sharing forum for its prime partners (within the MSH/Leadership and Management for Sustainability activities); that the Capacity Project provides a similar coordination role on HRH; and that Country Directors of the respective APHIA II projects meet monthly to review and share information on implementation. A vacancy announcement for an HRH officer to work in USAID Kenya was published during the visit and this post could also lend itself to improved alignment in future.
81. Further consideration on how to strengthen alignment and develop longer‐term financial
commitments would be of value. The opportunity from the PEPFAR reauthorisation to develop country compacts or frameworks could offer a forum to address this. Exploring the full range of aid instruments available to USG should factor into this review. Contractual instruments such as the ‘Implementation Letter’ or ‘Earmarked Funding’ provide for longer‐term financial commitments direct to a host country government/institution. An exploration of what innovation is needed to apply these existing USG tools to a PEPFAR strategic compact with Kenya could enable the alignment and long‐term financing discourse and be of real value to the HRH agenda and the rapid scale‐up of the health workforce.
3.2 DFID
82. DFID is currently spending around £20 million per year in the health sector (excluding HIV/AIDS
funding). Communicable disease management (Malaria Control, Treated Bednets and Immunisation) is a significant proportion of the overall programming, with further activities on Essential Health Services, health systems and reproductive health.
83. Capacity Development. The Essential Health Services programme includes particular support to capacity development within the former MoH on health systems, policy development and stewardship. The internal processes for the development of Annual Operational Plans (AOPs) are supported and greater linkages with the MTEF process are being developed. Project activities in Nyanza Province and at all other levels of intervention are derived from the respective AOPs.
84. DFID’s resident Health and HIV/AIDS advisor is currently the nominated representative for HRH
from the Development Partners group and DFID plays an instrumental role in the development of sector stewardship and coordination (e.g. through the SWAp development, Code of Conduct, Roadmap, IHP coordination).
85. A new 5‐year programme of support (Joint Support Programme to the Kenya Health SWAp) is in its latter stages of design. The new programme will provide a similar bilateral funding commitment, £100m over 5 years, with emphasis areas that include: equitable access and
33 Personal communication from Melahi PONS

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
utilisation of essential health services; implementation of the HRH Strategic Plan; sector support mechanisms to enhance budget efficiency and effectiveness, and; sector stewardship and governance. Additional DFID funding (£7m over 3 years) has been secured to support Kenya’s participation as a first‐wave country in the International Health Partnership (IHP). HRH is identified as the top priority. Both of the new funding interventions have been developed in cooperation and alignment with the former MoH and Development Partners.
86. Progress since Addis Ababa: Similar to PEPFAR‐funded activities, the DFID programming and
coordination has continued to engage with the former MoH and its decentralised representatives at Provincial and District level despite the upheavals since January 2008.
87. DFID has responded to the challenge of maximising the flexibility of donor funding. The new five‐
year programme specifically articulates ‘increasing amounts of flexible funding will be made available for emerging sector priorities determined with the MoH’. The intention is that flexible funds will be jointly coordinated between GoK, DFID and other development partners based on a mapping of inputs against priorities and reviewed annually.
88. Technical Assistance and/or funding for the implementation of the HRH Strategic Plan has now
been secured through additional DFID funding in support of Kenya’s participation in the IHP with internal procedures in place to allocate these funds for immediate use and quickly move forward on implementation of the priority HRH activities.
89. The combination of both funding streams enables the DFID country office to take an active
stance in HRH development. Both the immediate priorities, subsequent work identified and options identified from this joint exercise with OGAC/PEPFAR can be addressed. A number of areas for DFID consideration are suggested in the following section.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 29 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 30 of 50
4 Discussion and recommendations 90. An initial presentation of findings and recommendations was held on Friday 11th September with
representatives of the two Ministries and DFID. Representatives from the Capacity Project and Emory/CDC also attended. Due to time constraints the debriefing concentrated on the key points as part of a wider vision to address HRH in Kenya. The vision and key points are expanded in this report.
4.1 A strategic approach to HRH in Kenya
“we need to make new history today, and make it happen now.......first, on health, that we recruit and train a million health workers, saving the lives of three million mothers and seven million children”. Prime Minister Gordon Brown, speech to the UN General Assembly, 25 September 2008.34
91. The consultants have taken account of the global context for HRH, the health‐related MDGs and the need to consider Kenya as an actor within this wider framework. The UN High‐level Event on the Millennium Development Goals (September 2008), the High‐level meeting of the General Assembly on Africa’s Development Needs35 (September 2008), the Third High Level Forum on Aid Effectiveness (September 2008), the reauthorisation of PEPFAR (July 2008), the recent G8 meeting in Japan (July 2008), the announcements of President George Bush and Prime Minister Gordon Brown (April and June 2008), the MDG Africa Recommendations (June 2008), the 4th Tokyo International Conference on African Development, TICAD IV, (May 2008), the Kampala Declaration on HRH (March 2008), the first ECSA Health Community HRH five‐year strategy (February 2008), and the Global Campaign for the Health MDGs (September 2007) all contribute to this wider framework.
92. There is therefore a set of global circumstances in favour of HRH and health systems
strengthening, which the US Government, DFID and many other development partners have endorsed. In addition, there are the particular announcements of PEPFAR and JICA to specifically address the shortage of health workers in Africa ‐ with commitments to ‘at least 140,000’ and ‘100,000’ respectively.
93. As a result the GoK has a unique opportunity to position itself to respond to the global emphasis
on HRH and to lead a coordinated effort to address the country‐specific characteristics of its health workforce shortages and development requirements. It is against this scenario that the consultants envisage a GoK‐led initiative to achieve the WHO goal of at least 2.3 health workers per 1,000 population and to remove Kenya from the WHO category of an “HRH crisis country” as described in the 2006 World Health Report.
94. Whilst precise data would be required in the coming months, a common agenda to train and
recruit 20,000 ‐ 25,000 additional health workers under the stewardship of the Ministries of health (working in the public and faith‐based health facilities) would be the core focus.
34 The full transcript is available at: http://www.number10.gov.uk/Page16943. Prime Minister Brown also announced a Taskforce on Innovative Financing for Health Systems to help save 10 million mothers and newborns. It will help to provide over 1 million new health workers and ensure 400m extra births take place in a good quality facility. This Taskforce will report to the Italian G8 Summit in 2009 35 The meeting summary is available at: http://www.un.org/News/Press/docs/2008/ga10748.doc.htm

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 31 of 50
95. PEPFAR could secure a significant percentage of its 140,000 target in the next five years36 through this strategic partnership and Kenya could become a model for other country actions in Sub‐Saharan Africa.
96. Ministers and Permanent Secretaries from MoMS, MoPHS and the Ministry of Public Services are
encouraged to grasp this opportunity to take Kenya forward. The UN High‐Level Event on the MDGs and the launch of the First Year Report from the Global Campaign for the Health MDGs on the same day are both calling for a status review in 2010. Global stakeholders are therefore searching for initiatives at country‐level that can be successfully developed and replicated.
97. This should be promoted in positive terms. It is not an extension of the ‘Emergency’ hiring plan,
but a ‘Fast‐Track Hiring and Integration Plan’ which builds on the proven success of earlier models. OGAC, DFID and other partners (including JICA and the health systems strengthening opportunities from the Global Fund and GAVI) would subsequently provide support to the GoK, assisting in the necessary steps to realise this vision as part of their commitments to the Global Campaign for the Health MDGs and their own respective development or programme approaches.
98. The rationale is based on the many positive elements of HRH, health sector and macro‐economic
development that were evident in Kenya during the assignment. It is consistent with the GOK’s Vision2030, the National Health Sector Strategic Plan and the implementation of the Kenyan Essential Package for Health and aligned with the priorities and underlying purposes of the International Health Partnership, the PEPFAR reauthorisation and the Code of Conduct signed by development partners.
99. Annex 3 provides an indicative model for the ‘Fast‐Track Hiring and Integration Plan’, with a
projection of 21,000 new health care workers as an example. In this model the average annual investment from Development Partners over the 9‐year period 2008‐2017 is calculated at $25.5m – a figure less than PEPFAR’s current investment in health worker salaries discussed earlier. The impact on GoK budgeting and fiscal space for absorption into permanent posts rises from $6.9m in year‐4 to $97m in year‐937. Commitments in the Accra Agenda for Action (September 2008) and Kenya’s own Code of Conduct for the health SWAp should be operational at this time; facilitating the predictability of aid financing and sector budget support in addition to the domestic growth in health expenditures. The costs in this model are based on the estimates to engage the first wave of EHP hires in 2009 ($2,900). This and other assumptions will need more detailed analysis and review in the coming months and hence it should be considered as a discussion tool at this stage.
36 Since returning from the country assignment, the consultants have had sight of the draft guidance for reporting on the 140,000 ‘new health workers’ in the PEPFAR reauthorisation (Titled: ‘Human Resources for Health. For reporting on Legislative Goal. Target 140,000). Correspondence on the guidance is ongoing. It will be important to ensure that central guidance, in addition to meeting congressional reporting requirements, is supportive of the spirit of the PEPFAR reauthorization; promotes the strategic thinking that will need to be developed at country level; promotes the use and development of government monitoring and evaluation systems; requires partners to provide detailed data for country planning; and enables cross‐country comparison of the innovation and impact. 37 The GoK’s forecast for its macroeconomic framework is to have 10% pa growth effective from 2012/13. BOPA (2008).The integration of the first tranche of health workers is timed for 2011/12 onwards, coinciding with the projected increases in public expenditure.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
4.2 Strengthening HRH
100. A strategic approach to HR development in Kenya would respond to domestic needs and the
global calls for action and require concrete steps to be taken to advance this agenda. Some of these steps are also essential elements to advance the ongoing strengthening of HRH, are consistent with the HRHSP and the health sector ‘Roadmap’, and should be considered irrespective of the adoption of the above proposal. Opportunities are outlined for supporting HRH development in new ways. Recommendation HRH1: Formal adoption of the HRH Strategic Plan by the two Permanent Secretaries. Recommendation HRH2: Creation of the shared HRH department/unit reporting to the Permanent Secretaries
101. The division of the former MoH into two (MoMS + MoPHS) has created new dynamics in the stewardship of the health sector. HRH is a common function for both Ministries and there is value in adopting common management arrangements. The proposal to have a shared HRH department/unit reporting to the two Permanent Secretaries was agreed at the debriefing with the government health officials, as was the adoption of the HRH Strategic Plan (with an immediate update of the three‐year workplan). These are critical elements of the institutional and organisational strengthening required.
102. The HRH department/unit will need to perform a range of functions to support the
Ministries. The HRHSP sets out an organisational model encompassing administration (personnel issues and management), Strategic Planning and HR Development. The competencies and staffing in these sub‐departments will be different, as particular skills are required for each role. A review of the staffing and roles to perform its functions will ideally be coordinated with the DFID‐funded institutional review (as agreed by the previous Permanent Secretaries) and take account of the USAID willingness (via the Capacity Project) to provide long‐term technical assistance to this new department/unit.
103. Once the HRHSP and the new department/unit are confirmed by the Permanent Secretaries,
and the three‐year workplan updated, there needs to be due attention to securing the projected resources in the upcoming AOP and MTEF frameworks. The costings in the current HRHSP can serve as the basis for this review and engagement. Recommendation HRH3: Creation of the appropriate HRH coordination mechanism linked to the Health Sector Coordination Committee.
104. Many examples have been identified where Development Partners and their implementing agencies actively support the development of HRH and the expansion of the health workforce. Coordination of these initiatives is welcomed to promote alignment to country leadership. The HRHSP refers to the formation of a high level Multi‐Stakeholder HRH Steering Group, but it is not clear that this has been established or has terms of reference. With the wider macro‐economic issues related to public service employees, there is an argument for broader stakeholder participation from the GoK and the health economy. Securing the participation of these stakeholders alongside the existing agencies who engage on HRH will enable broader consensus, engagement and actions, and can improve understanding among stakeholders of the requirements for more flexible fiscal space for HRH development.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 32 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 33 of 50
Recommendation HRH 4: Develop strategic planning functions aligned to government planning frameworks and explore new planning models.
105. A cross‐Ministry HRH unit will foster cooperation between the Ministries on health workforce deployment, but should also take on a strategic planning function that is currently lacking in the country. In particular this relates to the methods of planning and projecting workforce needs. Currently planning is done against establishment figures, which have remained the same for many years. If one established post is unfilled at the end of a fiscal year, that post is then lost. This means that in effect the workforce is in danger of shrinking. Elsewhere we refer to the need to maximise absorptive capacity in the health labour market as the retirement age is increased and the number of health workers qualifying is scaled up. Projections based on health need will be required to accommodate new workers, and most importantly, to budget for them.
106. New models of planning can be used not only to improve predictions for workforce need,
but also to explore the use and costs of different models. Exercises such as scenario building and computer modelling can be run by an HRH unit with the stakeholder group, so that all understand the implications of choices, which become more robust as they are based on realistic data.
Recommendation HRH 5: Commission an analysis of wage ceilings and the fiscal space for scaling‐up HRH in Kenya and link this to the next MTEF and AOP frameworks.
107. A specific element of the strategic planning is budgetary and financial predication and
management and one of the bottlenecks to policy implementation is often financing. A recent AED study in four countries [Zambia, Lesotho, Côte d’Ivoire, and Malawi] cited this as a key constraint38.
108. Feedback from the interviews and document review in Kenya suggest this barrier is being addressed 39; even if there is a lingering sense amongst some civil servants that previous IMF conditionality continues to impose restrictions on government wage ceilings and recurrent expenditures. Within the planning cycle, we were encouraged to learn that there is increasing awareness that the absence of evidence and informed reason in discussions with other government entities responsible for budget and financing diminishes the emphasis on HRH. A core function of the new HRH department/unit is the development of evidence to inform policy and planning and attract the necessary financial resources. This is particularly apparent with recurrent expenditure for salaries and allowances. The competencies to undertake the macro‐economic analyses, engaging cross‐government staff, and providing scenario‐based estimates linked to economic growth needs to be nurtured and developed. In the immediate term, the health Ministries are encouraged to engage external technical assistance to support an analysis of wage ceilings and fiscal space for HRH and link with the MTEF and AOP planning frameworks.
109. DFID, through its financial support to the IHP, is a logical partner to support this technical assistance and would be in strong position to link this to: their wider macro‐economic development and governance activities supporting the GoK; the recent World Bank study in
38 AED (2008). Using Human Resource for Health Data: Health policy and program planning examples from four African countries. Africa’s Health in 2010 project. http://africahealth2010.aed.org/PDF/Using_Human_Resource_for_Health_Data.pdf 39 Earlier commentary highlights some of the positive policy and financing developments (i.e. increase in health expenditures; HRM policy to enhance public sector efficiency and remuneration)

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 34 of 50
three African countries on Wage Ceilings40 and; the Financing HRH Task Force convened by the Global Health Workforce Alliance (GHWA) (see Annex 5 for further information on the Resource Requirements Tool that this Task Force is developing).
110. In parallel due consideration should be given to develop technical capacity in the HR
department/unit to undertake similar exercises in subsequent MTEF and AOP frameworks. The initial technical assistance provided by DFID could be extended to incorporate this capacity development.
Recommendation HRH 6: Continue to strengthen HRIS and enhance workforce surveillance information systems to incorporate distribution, infrastructure, epidemiological and population data compatible with a GIS reporting capacity.
111. Underpinning strong HRH development is good data to inform strategic planning. Currently
workforce data is not easily accessible, incomplete and stored in several sites. The current TWG and the programs by Emory‐CDC and Capacity Project are working to improve and coordinate the data available, and this is urgent. For future planning, policy, development and research functions further work should be initiated to enable enhanced workforce surveillance compatible with GIS software, with links to the mapping of health facilities, public sector staffing and distribution and the burden of disease. This is especially important with the six new levels of health service delivery, as a rational and equitable deployment model is established. Understanding better the competencies of the workforce as well as their roles, will assist managers in meeting staffing requirements.
Recommendation HRH 7: Conduct a comprehensive review of the legislative, policy and strategic frameworks that impact on HRH.
112. The wider government reforms in public service, decentralisation and human resource
management will have consequences for HRH planning and implementation. To ensure the continuing alignment of the HRHSP with the overarching government reforms we would encourage a review of the legislative, policy and strategy frameworks that impact on HRH, taking account of the roles and responsibilities of the respective health Ministries and their oversight of production, recruitment, deployment, development and retention of the health workforce. The review should identify gaps and/or bottlenecks in the frameworks for stewardship of the health workforce, revisiting progress on the formation of policies and guidelines advocated for in the HRHSP, and recommend actions to address them. Subsequently incorporate the actions into the planning and implementation schedules with development partner support as required. Recommendation HRH 8: Strengthen education and training in HRH planning and management and consider North‐South and South‐South partnership approaches.
113. There is a need throughout the sector to develop skills in HRH planning and management, as
well as in leadership to promote and manage change. It is recommended that opportunities are embedded within the education sector in Kenya – perhaps with twinned institutions or regional bodies (i.e. ECSA) from neighbouring countries and from the UK or US – for HRH training at post‐
40 Kenya, Rwanda and Zambia plus the Dominican Republic. Initial evidence from the study suggests that whilst government wage bill restrictions do have an impact it may not be as significant a constraint to scaling up the health workforce. The published report should be examined once it is available. Personal correspondence with Marko Vujicic, World Bank.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 35 of 50
graduate level. Developing a regional centre of excellence in Kenya in HRH training is an option that could be considered as part of the WHO encouragement of an African Observatory41 .
Recommendation HRH 9: Review and implement the necessary communication activities across the health Ministries and with wider stakeholders.
114. Communication within the Ministries could be compromised by the new structures and is already showing signs of being under stress. This is hardly surprising given the recent and ongoing changes. Nevertheless, it is an opportunity to explore ways of improving organizational communication. There is an upcoming review of the organizational effectiveness of the Ministries, funded by DFID and an existing analysis and recommendations from 2007 on Health Communication Activities42 (where internal communication was one of the focus areas). We would encourage further attention to the communication strategies, building on the support provided.
Recommendation HRH 10: Review options to deliver the Treat and Retain principles from the Treat, Train & Retain initiative with the introduction of ‘Wellness Centres’ and support to the Positive Practice Environment campaign.
115. Several sources reported that health workers are significantly affected by HIV/AIDS, and this
is causing absence from work, and sadly, deaths. Kenya is already addressing issues of retention and training, scaling up intake of students, and testing out new models of employment that streamline and improve retention. The missing link here is treatment of health workers, and it is recommended that ‘wellness centres’ be introduced, using the same model that has been tested in Swaziland and other countries in the region. The rationale for this is the persistent stigma among health workers about infection with HIV, again reported to us by several sources. The International Council for Nurses is an experienced partner in establishing these centres and could be actively supported by the Kenya Nursing Council.
116. The International Council of Nurses (alongside the International Hospital Federation,
International Pharmaceutical Federation, World Confederation for Physical Therapy, World Dental Federation, and World Medical Association) has also recently released a set of international guidelines on workplace incentives, which recognise the value of the Positive Practice Environment in the motivation and retention of staff. The campaign is now being rolled out at the country level in Uganda, Zambia and Vietnam. Consideration should be given to funding Kenya’s inclusion in the campaign thus supporting one of the priority objectives in the HRHSP to address retention.
Recommendation HRH 11: Review options for developing health worker skills and competencies in the management of the third stage of labour and implement recommendations resulting.
117. A key concern in implementing the Community Health Strategy is whether there will be enough skilled birth attendants in place. Training as many health providers as possible to manage the third stage of labour could go a long way towards reducing the high maternal
41 www.who.afro.int 42 Review of Health Communication activities: A Situational Analysis. OCTOBER 2007. Steadman Group.

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
mortality rate in Kenya. Even Traditional Birth Attendants could be considered for this, given the special needs of the people. Certainly all nurses, clinical officers, CHEWS and possibly CORPS, especially if attached to hard to reach and nomadic communities, should be considered for this training.
118. Interventions that have been piloted in Kenya, such as maternal houses and the use of community midwives, should be assessed for impact on maternal and neonatal mortality as well as suitability for wider implementation.
4.3 Development Partners – supporting actions
119. Many of the above discussion points and recommendations will engage the DPs in review
and subsequent implementation at the invitation of the health Ministries. The points below are separated on the basis that they specifically apply to DP actions, some of which can be taken forward in coordination with the existing partner forums (i.e. HENNET, DPH‐K) Recommendation DPs1: All DPs to coordinate themselves to provide a detailed report to the HRH department/unit on the engagement of temporary and contract hires currently engaged through DP support.
120. Through the appropriate coordination mechanisms, development partners, their implementing agencies and civil society need to assist the HRH department/unit in producing verifiable data on the existing support to temporary and contract hires in the health workforce. An exercise reported in the Marsden & Chirchir evaluation of the EHP can be updated and extended to enable this, capturing the latest data on external support (i.e. GFATM, GAVI, UNICEF, PEPFAR). The data should be of value to the GoK as the ‘client’ and provide a level of detail greater than partner reporting to their respective headquarters. The objective is to enable the health Ministries to engage in the next MTEF and AOP planning frameworks with accurate data and projections. The data should be consolidated to enable a comprehensive overview of numbers, distribution, cadres and financial commitments (salaries, gratuities, incentives etc). Linking this to the existing Capacity Project database for the emergency hires (already established to track direct hires and associated salary costs) would seem logical, as would cross‐checks with databases on individual cadres and government employees.
121. PEPFAR support to this process is essential. The scale of support identified in their ongoing
survey instrument suggests they are engaging the vast majority of the contracted health workers, with significant numbers of health workers outside of the EHP mechanism: many within parastatal organisations such as KEMRI. Whilst it is recognised that the current survey instrument is designed to minimise the reporting burden for country activities, the absence of a comprehensive overview of health worker support impedes HRH planning. An internal assessment of the PEPFAR supported health workers should identify the same comprehensive level of information as those health workers engaged under the Emergency Hiring Plan (cadre, post, location, salary, gratuity etc, etc) to enable a single data set and subsequent reports to be generated. This exercise will also enable: a PEPFAR baseline to be created that will be of value to the future measurement and evaluation of the new health worker target in the PEPFAR reauthorisation; distinguish existing hires from future new hires and; act as a pilot mechanism to engage the implementing partners in the strategic thinking and necessary steps to ensure 2009‐2013 reporting is of value to the health Ministries and the US Congress.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 36 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Recommendation DPs2: Review the administrative models, mechanisms and costs for DP supported health workers and seek to standardise procedures and reduce transaction costs accordingly.
122. PEPFAR is taking major steps in addressing the gaps in the health workforce and the
assistance should be recognised. Moving forward, there needs to be further attention to the details, models, contract duration, transaction costs, retention levels and personnel management as well as higher‐level engagement on absorption into the government payroll. Whilst there is confidence in the Capacity Project model the APHIA II example earlier suggests the transfer will still maintain a range of administration costs. Further work to assess the models and costs would be beneficial. It would be preferable to see administration costs (both as % of salary and per health worker) being lowered overall given the marginal costs of expanding the scheme. The same will apply to the many other models currently utilised by Development Partners. Involving a neutral party in this review, or engaging the Clinton Foundation (who have experience from their own model) as a third party to PEPFAR and DFID may be appropriate. Recommendation DPs3: Initiate discussions with JICA on their intended support to Kenya and wider alignment with the Accra Agenda for Action.
123. The mission was unable to meet with JICA officials in Kenya to ascertain how the TICAD IV announcement to support 100,000 new health workers will be developed in particular respect to Kenya’s needs. DFID and USAID country staff are similarly yet to be informed. Japan is a signatory to the Code of Conduct in Kenya and a member of the Development Partners forum. Discussions should be initiated at country level (and HQ levels) to explore potential synergies in approaches and demonstrable alignment with the IHP’s country compact and the Accra Agenda for Action. Recommendation DPs 4: DFID and USG staff in Kenya to engage with GF, GAVI, UNICEF and other key partners to participate in a strategic, aligned approach to HRH
124. The Global Fund, GAVI and more recently UNICEF are all involved in the engagement of contract/temporary hires. Future applications to the Global Fund and GAVI, responding to the health systems strengthening windows, may expand these initiatives. There will be considerable benefit in engaging the GF and GAVI representation in Kenya and their respective head offices to seek their participation in a strategic, aligned approach to HRH which is also linked with the IHP’s country compact and the Accra Agenda for Action.
Recommendation DPs 5: Initiate discussions on the M&E framework to enable the measurement and review of health workforce scale‐up in Kenya.
125. The PEPFAR reauthorisation, TICAD IV announcement and the latest call from Prime Minister Gordon Brown at the High Level meeting on the MDGs all promote an immediate scaling‐up of the health workforce. Kenya has an opportunity to access the financial support to enable this. At the country level there will be a need to develop the capacity to measure and evaluate the scaling‐up of the health workforce. Individual DPs will need to report to their constituencies on the resources utilised and results but at the same time should ensure that they are developing the GoK capacity for measurement and work from one common M&E framework. DPs should therefore seek to review and harmonise their M&E approaches and simultaneously position Kenya to be a leading example of good practice.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 37 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Recommendation DPs 6: USG to consider an internal review of the existing CDC and USAID aid instruments that enable longer‐term financial commitments in a host country and the innovation required to adapt these to PEPFAR legislation.
126. The METF and AOP frameworks establish a clear calendar of planning activities and seek the engagement of development partners to be supportive of these. The PEPFAR planning process and financial disbursement is currently able to align itself to the priorities established in the AOP schedule, but further work may be required on how it can proactively influence future strategic actions.
127. As PEPFAR positions itself to transition from an ‘emergency’ intervention to a broader public health and development approach it has the opportunity to consider how best to develop a strategic compact or framework with Kenya. As part of the internal thinking we would encourage a review of the current aid instruments available in CDC and USAID that enable longer‐term financial commitments to development programming and what level of innovation would be required to adapt these to be consistent with the new PEPFAR legislation.
4.4 Matrix of recommendations resulting.
128. The following table presents the above recommendations, by lead, target date and means of
verification.
Table 7: Matrix of recommendations
Recommendation Lead Target date Means of Verification
HRH1: Formal adoption of the HRH Strategic Plan by the 2 Permanent Secretaries
MoMs + MoPHS
September 2008
PS letters or equivalent
HRH2: Creation of the shared HRH department/unit reporting to the Permanent Secretaries
MoMs + MoPHS
September 2008
PS letters or equivalent
HRH unit established
HRH3: Creation of the appropriate HRH coordination mechanism linked to the Health Sector Coordination Committee
MoMs + MoPHS
October 2008 PS letters or equivalent
HRH 4: Develop strategic planning functions aligned to government planning frameworks and explore new planning models
HRH department / unit
Report from the Institutional Review
Updates in HRHSP workplan
HRH 5: Commission an analysis of wage ceilings and the fiscal space for scaling‐up HRH in Kenya and link this to the next MTEF and AOP frameworks
HRH department / unit
October 2008 for work commission
(report to be able by early December)
Agreed Terms of Reference
DP agreement to support the TA
Final report.
HRH 6: Continue to strengthen HRIS and enhance workforce surveillance
HRH department /
December 2008 for
Agreement with supporting partners
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 38 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 39 of 50
Recommendation Lead Target date Means of Verification
information systems to incorporate distribution, infrastructure, epidemiological and population data compatible with a GIS reporting capacity
unit initial agreements
noted in minutes of the HRIS TWG.
HRH 7: Conduct a comprehensive review of the legislative, policy and strategic frameworks that impact on HRH
HRH department / unit
October 2008 for work commission
(report to be able by early December)
Agreed Terms of Reference
DP agreement to support the TA
Final report.
HRH 8: Strengthen education and training in HRH planning and management and consider North‐South and South‐South partnership approaches
HRH department / unit
October 2009 for first courses
Agreements in place between learning institutions
Courses underway
HRH 9: Review and implement the necessary communication activities across the health Ministries and with wider stakeholders
MoMs + MoPHS
December 2008
Communication mechanisms in use (e.g. newsletter, blog)
HRH 10: Review options to deliver the Treat and Retain principles from the Treat, Train & Retain initiative with the introduction of ‘Wellness Centres’ and support to the Positive Practice Environment campaign
HRH department / unit
June 2009 First Wellness centre open and fully functional
HRH 11: Review options for developing health worker skills and competencies in the management of the third stage of labour and implement recommendations resulting
HRH department / unit
April 2009 Training plan available
Development Partners (DPs)
DPs1: All DPs to coordinate themselves to provide a detailed report to the HRH department/unit on the engagement of temporary and contract hires currently engaged through DP support
DFID + USG
December 2008
Summary report to the HRH department/unit
DPs2: Review the administrative models, mechanisms and costs for DP supported health workers and seek to standardise procedures and reduce transaction costs accordingly.
DFID + USG
December 2008
Summary report to the DPH‐K
DPs3: Initiate discussions with JICA on their intended support to Kenya and wider alignment with the Accra Agenda for Action
DFID + USG
November 2008
Meeting Notes

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 40 of 50
Recommendation Lead Target date Means of Verification
DPs 4: DFID and USG staff in Kenya to engage with GF, GAVI, UNICEF and other key partners to participate in a strategic, aligned approach to HRH
DFID + USG November 2008
Meeting Notes
DPs 5: Initiate discussions on the M&E framework to enable the measurement and review of health workforce scale‐up in Kenya
DFID + USG
November 2008
Meeting Notes
DPs 6: USG to consider an internal review of the existing CDC and USAID aid instruments that enable longer‐term financial commitments in a host country and the innovation required to adapt these to PEPFAR legislation
USG November 2008
Internal discussions held and resulting actions noted.
129. These recommendations are for ongoing dialogue and discussion between partners. Many
are complementary to each other and require continuing commitment to working in partnership, applying complementary strengths to take these forward.
130. Target dates are indicative. Representatives from the MoMS, MoPHS, and Development Partners in Health – Kenya (DPH‐K) along with USAID, CDC and DFID should consider and review these further.
131. Once the health Ministries provide their responses, further discussion between PEPFAR and DFID will be required to agree where their respective programming can support the implementation. Where long‐term or short‐term technical assistance is requested, clear agreement should be reached on the lead and capacity to implement within the necessary time frames; especially for actions related to the next round of the MTEF and AOP.
END

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Annexes Annex 1 – Terms of Reference Kenya: Taking forward Action on Human Resources for Health (HRH) in selected African Countries with DFID/OGAC and other partners. Background: 1. In response to the critical HRH shortages in Africa, DFID and Office of the US Global Aids
Coordinator (OGAC) responsible for PEPFAR have been in discussion with a number of African countries to develop strategies and country level actions to help address these crucial gaps. The overarching aim is to demonstrate the maximum flexibility of disease specific programmes to support broad based primary care in line with countries’ health plans.
2. An initial operational meeting was held in Ethiopia in January 2008 with US, UK and country
representatives from Ethiopia, Zambia, Mozambique and Kenya (PEPFAR, DFID overlap countries). Some initial progress was made and a matrix was produced for each country highlighting key short‐ to mid‐term priorities that could be potentially funded. However, these required further work and details on priority areas for each country.
3. Emerging from the 2008 G8 and other high‐level international fora, there is high level political
support for this process in the UK and US, provided that the efforts result in specific actions and commitments in each country. However, there is a short political window to demonstrate success. As such, technical support is required to develop costed options of priority short‐ to mid‐term actions for these countries. To avoid this activity running counter to existing country‐level processes, every effort should be made to ensure close coordination and linkages with existing country systems and HRH working groups. In Kenya, this activity should be undertaken with support from the Ministry of Medical Services (MoMS), the Ministry of Public Health and Sanitation (MoPHS), and DFID and US country teams, with a keen focus on operational level activities. Discussions should also include relevant Government of Kenya (GoK) staff, USG, DFID, Danida, Clinton Foundation, WHO and other agencies with significant involvement in HR support.
Purpose: 4. To build on existing activities within both Kenya’s national frameworks for HR and broader
health and public sector reform by documenting current funding streams supporting HRH in Kenya, identifying flexibilities of such funding streams, and facilitating agreement around specific short‐ and mid‐term priority actions to expand and enhance support on HRH in Kenya..
Scope of Work for Kenya Consultancy 5. The consultant(s) will:
a. Review public sector strengthening/reform and other HR related initiatives and their implications for increasing resources towards meeting the targeted ratio of health worker per population.HRH.
b. Review Kenya HRH plans and key priorities, including:
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 41 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
• A draft HRH strategic plan has been developed and widely accepted by stakeholders.
• A list of priority HRH activities was developed at the mid‐term review of the Kenya National Health Strategic Plan (NHSP), conducted in November 2007, and the Ministry of Health’s Annual Operation Plan 4 is also close to completion.
• The consultant(s) should identify priority interventions in increasing the number of health workers and funding gaps..
c. Assess current support for HRH supported by PEPFAR and DFID through review of
respective country assistance plans, and identify future opportunities for expanding and improving such support, both direct and indirect, to increase its impact on HR capacity building. This assessment should include but not be limited to:
• DFID Kenya was recently successful in mobilising additional funding for IHP‐related activities (£1m in FY08; £3m in FY09; £3m in FY10). It is also finalising the design of a new health programme (£100 million over 5‐6 years). Most of FY08’s IHP funding will be channelled through DFID’s Essential Health Services Project. The remainder (most) will be added to the new health programme. HR has been identified as the top priority for IHP funding. The consultant(s) should describe in detail the recommended future areas of DFID HR support, expected outputs, budget estimates and recommended funding arrangements.
• With PEPFAR funding, USAID Kenya has supported HRH strengthening through a number of mechanisms and activities. These include activities undertaken by the Capacity Project, the APHIA Projects, the Emory University‐CDC collaboration and program‐specific training conducted by various other PEPFAR‐supported projects.
• The Capacity Project follow‐on 5‐year award is expected to start November 1, 2008 with the following anticipated results: 1. Strengthened and institutionalized HRH strategies, plans, policies and
practices at the national and provincial levels that will promote the provision of quality HIV/AIDS, Family Planning/Reproductive Health (FP/RH), Maternal and Child Health (MCH), malaria and TB services at the community level.
2. Improved opportunities for addressing the knowledge and skills needed by workers at all levels, including the community, for the provision of quality services for HIV/AIDS, FP/RH, MCH, malaria, TB and primary health care in general.
3. Workforce performance systems in place to improve productivity and retention for the delivery of HIV/AIDS, FP/RH, MCH, malaria and TB services, particularly at the community level.
• With PEPFAR funding, Kenya will implement a management and leadership strengthening program through the Leadership and Management for Sustainability Program of USAID. An assessment has been completed and the activities are expected to commence October 2008.
• With PEPFAR funding, CDC Kenya will implement a fellowship program with a focus on short‐ and longer‐term training of high‐level HIV program managers.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 42 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
d. Review results specifically referring to Kenya of the initial PEPFAR‐DFID HRH meeting in Ethiopia and consider progress made.
e. Document the extent of current PEPFAR support to human capacity building.. This will
require use of information extracted from the PEPFAR Country Operation Plan (COP) and should cover the following areas: i) Identify programme elements which are directly contributing to government
directed or managed programmes, such as the Emergency Hiring Program, financing of pre‐service training and scholarships, and investments in curriculum development, identifying the level of investment where possible. The overall purpose of which is to quantify to extent to which PEPFAR funds are already being used to strengthen human capacity building. .
ii) Identify challenges to the predictability of PEPFAR financing – documenting the timeframe between budget submission, budget approval and financial disbursement, and assessing the implications of any delays for joint planning with government. Identify how better understanding of this process can give a clearer indication of when annual funds will arrive in country, in order to facilitate planning on the basis of a realistic and predictable indication of key dates. This information should be provided within the context of National AIDS Control Council’s ongoing efforts to coordinate and harmonise support to the national AIDS response and existing health sector planning cycle milestones. Make recommendations for increasing the predictability through all funding channels.
a. The consultants should liaise with other processes, such as development of a
shadow budget and MTEF, and identify how DFID and PEPFAR funds can better align with these.
g. Following the recent structural changes within government, highlight the obstacles and opportunities to implementing HHR going forward, and recommend how best this should proceed in terms of decision‐making, consultation, coordination, etc. h. Present outputs to stakeholders, including MoMS, MoPHS, US, UK and other relevant partners. Timeframe: 6. The consultancy is expected to start early September 2008. Output: 7. A draft report that responds to the above SoW, which highlights current investments, flexibilities
and opportunities for enhancing support to HRH and priority short‐ and mid‐term options for action and funding in Kenya, including agreed country matrix outlining costed priorities. The report will be submitted within fourteen (14) days of the consultant(s) departing from Kenya. The draft will then be amended within fourteen (14) days of receiving comments from relevant parties.
Inputs: 8. Up to xx days shared between up to two consultants, who possess a background in health
systems, targeted disease programming, and human resources for health, with strong facilitation and writing skills and demonstrated experience of working in Africa.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 43 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 44 of 50
Annex 2 – Itinerary and persons met
Date Time Barbara Stilwell Jim Campbell
Tue 2nd pm Arrive Nairobi
Wed 3rd am Briefing: Tony Daly (DFID), Melahi Pons (USAID), Kimani Mungai (Capacity Project)
pm Dr Sharrif & Mr. Kaloki (MoPH)
Thur 4th am Mrs. Ndegwa (MoMS) Prof. Peter Nyarango, Ruth Okowa (HENNET)
pm Dr. Richard Pandame (Liverpool LVCT) Rose Maina (DRH)
Dr. Samuel Mwenda (CHAK)
Fri 5th am Dr. Suleh (KMA) Melahi Pons (USAID) Jerusha Karuthiru (USAID)
Kethi Mullei (KEMRI‐Wellcome Trust)
pm Mrs. Ndegwa (MoH) Mette Kjaer (AMREF)
Prof Miriam Were (NACC)
Mon 8th am Dr. George Gatiri, PMO, Central province Rankesh Mutisya Willy, Rose Ruthut, Gitowga Kamenya
pm Paul Kaudo, Felix Wachanga, Jonah Mwangi, Monica Kimani (Thika DH)
Tue 9th am
Dr. Job Obwaka (Engenderhealth) Peter Mwarogo (FHI)
Melahi Pons, (USAID) Patricia Riley, Alexandra Zuba, Agnes Waudo, Andrew Kamenju, Rose Kiriinya
(EMORY/CDC), Esther Ndivo (Capacity Project)
pm Kimani Mungai (Capacity Project)
Wed 10th
am Faith Mbehero (Kenya Nursing Association)
Karen Caldwell (MSH) Gerald Macharia (Clinton Foundation)
pm Charles Dulo (AED) Dr.Sharrif (MoPHS)
Winston Majale, Cecilia Amahaya (USAID)
Thur 11th
am Miano Munene (HERAF)
Tony Daly (DFID), Melahi Pons (USAID)
pm Dr. Kumar (UNICEF) Jonathan Mermin (CDC)
Fri 12th am Debrief: Dr.Sharrif, Mr. Kaloki (MoPHS), Tony Daly (DFID) Kimani Mungai (Capacity Project) Alexandra Zuba (EMORY/CDC)
pm Anja Minnick, Thomas George, Grace Okubo (CDC)
23:45 depart Nairobi

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Annex 3 – Indicative Model: Fast‐Track Hiring and Integration Plan (FTHIP)
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 45 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Annex 4 – Selected Extracts from the PEPFAR reauthorisation
Tom Lantos and Henry J. Hyde United States Global Leadership Against HIV/AIDS, Tuberculosis and Malaria Reauthorization Act of 2008
Selected Extracts
Section 4. PURPOSE. ‘‘(6) helping partner countries to—‘‘(A) strengthen health systems;‘‘(B) expand health workforce; and ‘‘(C) address infrastructural weaknesses.’’. POLICY, PLANNING and COORDINATION. STRATEGY. Section 101(A)(4)(J): ‘help partner countries to train and support retention of health care professionals and paraprofessionals, with the target of training and retaining at least 140,000 new health care professionals and paraprofessionals with an emphasis on training and in country deployment of critically needed doctors and nurses and to strengthen capacities in developing countries, especially in sub‐Saharan Africa, to deliver primary health care with the objective of helping countries achieve staffing levels of at least 2.3 doctors, nurses, and midwives per 1,000 population, as called for by the World Health Organization; POLICY, PLANNING and COORDINATION. REPORT. Section 101(b)(2)(R): A description of the strategy to—‘‘(i) strengthen capacity building within the public health sector; ‘‘(ii) improve health care in those countries; ‘‘(iii) help countries to develop and implement national health workforce strategies; ‘‘(iv) strive to achieve goals in training, retaining, and effectively deploying health staff BILATERAL EFFORTS. General Assistance and Programmes. POLICY. Section 104A(b)(1)(A)(vi) “train and support retention of health care professionals, paraprofessionals, and community health workers in HIV/AIDS prevention, treatment, and care, with the target of providing such training to at least 140,000 new health care professionals and paraprofessionals with an emphasis on training and in country deployment of critically needed doctors and nurses; BILATERAL EFFORTS. General Assistance and Programmes. POLICY. Section 104A(b)(1) (B)” strengthen the capacity to deliver primary health care in developing countries, especially in sub‐Saharan Africa” C) “support and help countries in their efforts to achieve staffing levels of at least 2.3 doctors, nurses, and midwives per 1,000 population, as called for by the World Health Organization” BILATERAL EFFORTS. General Assistance and Programmes. COMPACTS AND FRAMEWORK AGREEMENTS. Section 104A(e).— ‘‘(2) ELEMENTS.—Compacts on HIV/AIDS authorized undersubsection (d)(8) shall include the following elements: ‘‘(E) Compacts shall contain— ‘‘(vi) consideration of the methods by which the compact will— ‘‘(I) strengthen the health care capacity, including factors such as the training, retention, deployment, recruitment, and utilization of health care workers http://frwebgate.access.gpo.gov/cgi‐bin/getdoc.cgi?dbname=110_cong_bills&docid=f:h5501enr.txt.pdf
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 46 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Annex 5 – GHWA Task Force on Financing HRH One of the 5 core strategies of the Global Health Workforce Alliance (GHWA) is to address global challenges in HRH. In December 2007, it established the Task Force on Financing Human Resources for Health (TF‐HRH) to focus on three key areas: 1. Building awareness on the importance of economic and financing issues within the global
movement to address HRH 2. Collating evidence on financing HRH 3. Developing and testing, in selected pilot countries, a decision tool (subsequently titled the
Resource Requirements Tool or RRT) for use by country planners and decision‐makers to estimate and project the costs of desired health workforce scale‐up and development.
The TF‐FHRH, hosted by the Results for Development Institute in Washington, DC, is to complete its work in 2008 and report back to the GHWA Board on its findings. The RRT has been applied in Ethiopia and Liberia in collaboration with the respective Ministries of Health and the World Bank. A further pilot is planned in Asia. Subsequently the World Bank is applying the RRT in Ghana, Sierra Leone and Zambia. The RRT enables country planners to review three key areas: Employment, Pre‐Service Education and Ability to Fund. The combination hence enables a detailed understanding of the indicative resource requirements to scale‐up the health workforce and engages wider government Ministries in assessing the fiscal space and medium‐term budget impacts. Current pilots suggest the work can be undertaken over a period of four to five weeks in‐country, engaging national personnel at all stages of the process. The RRT has the potential to support the development work required in Kenya and provide a rapid appraisal that will link to the current calendar of activities for the next MTEF and AOP planning schedules. Further information on the work of the Task Force is available from: Marty Makinnen (Director, Task Force Secretariat) email: [email protected]
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 47 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
Annex 6 ‐ Documents consulted / referenced materials. GoK & MoH Annual Operational Plan (AOP 4) – Stakeholders Presentations Budget Outlook Paper 2008/09‐2010/11, January 2008 Health Sector Strategic Plan II (2005‐10) (NHSSP II) Health Sector Strategic Plan II (2005‐10) (NHSSP II) – Mid Term Review Report (August 2007) Health Sector Plan 2007 Health Sector Plan 2008 Human Resources for Health Strategic Plan (2007/8‐2009/10) (HRH‐SP) draft of November 2007 Joint Programme of Work and Funding (JPWF) Joint Financing Agreement, draft of November 2007 Kenya Essential Package for Health (KEPH) Kenya National HIV/AIDS Strategic Plan (2005/6 – 2009/10) NACC, June 2005. Kenya Health Sector Wide Approach – Code of Conduct (August 2007) Medium Term Expenditure Framework (MTEF) Ministry of Health. Medium Term Plan 2008‐2012 Public Service Reform Strategy (PSRS) Report from the JRM Steering Committee Retreat (November 2007) Review of Health Communication activities: A Situational Analysis. OCTOBER 2007 Vision2030: Transforming National Development Reports and documents
DFID (2008) Programme Memorandum. Joint Support Programme to the Kenya Health SWAp draft as of May 2008. DFID (2008) Health programme design. Institutional risk assessment of health sector. Draft terms of reference. DFID HRC (2007) First annual OPR DFID support to the delivery of Essential Health Services. HENNET (2008) SWAP Workshop IOM (undated) Managing the Migration of HRH in Kenya Kenya Joint Assistance Strategy (2007‐12) Harmonization Alignment and Coordination (HAC) donor working group 2007. Marsden & Chirchir (2008) Mid‐Term Evaluation of the Kenya EHP. Capacity Project PEPFAR (2008) Instructions for Counting PEPFAR‐supported Health Care Workers for COP 2009 Stilwell, B (2008) Increasing skill‐mix and productivity in the health workforce in NEP: a concept note. Unknown (2008) Brief – Health Sector Kenya Unknown (2007) Kenya addresses it health workforce challenges Published documents/literature
Accra High Level Forum (2008) Accra Agenda for Action. http://www.accrahlf.net/ Adano, U. (2008). The health worker recruitment and deployment process in Kenya: an emergency hiring program. Human Resources for Health 2008, 6:19 http://www.human‐resources‐health.com/content/pdf/1478‐4491‐6‐19.pdf
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 48 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
AED (2008). Using Human Resource for Health Data: Health policy and program planning examples from four African countries. Africa’s Health in 2010 project. http://africahealth2010.aed.org/PDF/Using_Human_Resource_for_Health_Data.pdf CHAK (2007) The HRH Challenge in Church Health Facilities: Which Way Forward? Report of CHAK Annual Health Conference. Chankova et al (2006). Rising to the challenges of HRH in Kenya: Developing Empirical evidence for decision‐making. PHRplus, Abt Associates. Global Campaign for the Health MDGs (2008) First year report. http://www.norad.no/default.asp?V_ITEM_ID=9263 Global Heath Workforce Alliance (2008) “Promoting Synergy between Partners” Meeting Notes, Addis Ababa, Ethiopia: 10‐11 January 2008. IOM (March 2007) PEPFAR Implementation: Progress and Promise. http://www.iom.edu/CMS/3783/24770/41804.aspx MDG Africa Steering Group (2008) Achieving the Millennium Development Goals in Africa Recommendations of the MDG Africa Steering Group. Mwaniki DL and Dulo CO, (2008) Managing the migration of human resources for health in Kenya: the impact on service delivery’. EQUINET Discussion Paper Series 55. EQUINET, IOM, Kenya Technical Working Group for Managing Migration of Health Workers, EAC and ECSA HC, EQUINET, Harare PEPFAR (2008) Kenya: 2008 Country Profile. http://www.pepfar.gov/press/81596.htm Riley, P et al (2008) Developing a Nursing Database System in Kenya. Health Research and Educational Trust. US Government (2008). Tom Lantos and Henry J. Hyde United States Global Leadership Against HIV/AIDS, Tuberculosis and Malaria Reauthorization Act of 2008. http://frwebgate.access.gpo.gov/cgi‐bin/getdoc.cgi?dbname=110_cong_bills&docid=f:h5501enr.txt.pdf
WHO (2006) World Health Report.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 49 of 50

Kenya: Taking forward action on Human Resources for Health (HRH) with DFID/OGAC and other partners.
October 2008. Jim Campbell (Integrare, Spain) and Barbara Stilwell (Capacity Project, USA) Page 50 of 50
Annex 7 ‐ Considerations for further country visits. The collaboration between OGAC and DFID envisages visits to four countries (Ethiopia, Kenya, Mozambique and Zambia). With two visits to Ethiopia and Zambia remaining the following suggestions are put forward for consideration: 1. The pre‐departure and initial country briefings should endeavor to include all the lead
representatives of PEPFAR programming at country level. 2. Further lead‐time is encouraged to ensure that the individuals and organisations identified in the
list of key informants are available to meet with the consultants whilst in‐country. 3. Relevant documentation will ideally be made available as early as possible. If key documents are
not available electronically, it would be helpful to have copies available on arrival. 4. The consultants will ideally be hosted in either the DFID, USAID or CDC offices (security
arrangements permitting) of the country. The comparison between the Mozambique and Kenya country visits where one was hosted by CDC and the other by an implementing partner of USAID programming suggests the former was far more beneficial for daily interaction, access to COPRS data and discussion of the mission and its findings.
5. Country exercises to count the number of health workers supported by PEPFAR programming would ideally be available in advance of the arrival. Where possible these should be reviewed for accuracy against actual implementation rather than original projections.
6. Country representatives of PEPFAR programming are encouraged to enable the consultants to have access to the COPRS, with the consultants signing confidentially agreements as required.
7. DFID and PEPFAR representation at the debriefing with the Ministry of Health is essential to promote the strength and commitment to the OGAC/DFID partnership.
8. A focus‐group discussion (1 day) with government and PEPFAR implementing partners could prove invaluable. The focus‐group could be used as a means to initiate the strategic thinking at country level on the new PEPFAR target for health workers, review central guidance, and consider country mechanisms for the ongoing M&E of this target.
9. A minimum of 10 days is recommended for in‐country work with a further 5 days’ reading and
analysis time. Report writing has, for the first two country visits, taken approximately 2 weeks after the end of the visit.