BRONCHIAL ASTHMA Islamic University Nursing College.
27
BRONCHIAL ASTHMA Islamic University Islamic University Nursing College Nursing College
-
Upload
cory-small -
Category
Documents
-
view
233 -
download
6
Transcript of BRONCHIAL ASTHMA Islamic University Nursing College.

BRONCHIAL ASTHMA
Islamic University Islamic University
Nursing College Nursing College

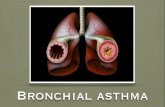
DefinitionAsthma is a chronic inflammatory disease of
the airways which develops under the allergens
influence, associates with bronchial
hyperresponsiveness and reversible obstruction and
manifests with attacks of dyspnea, breathlessness,
cough, wheezing, chest tightness and sibilant rales
more expressed at breathing-out.

EpidemiologyAccording to epidemiological studies asthma
affects 1-18% of population of different countries.
Only in 2006 more than 300 million patients
suffered from asthma all over the world, 250
thousands of patients die of asthma. The incidence of
asthma is higher in countries with increased air
pollution.

causes
Allergic reactions to plants, foreign
bodies in the air way.

Etiology
The allergens
are divided into:
•Communal,
•Industrial,
•Occupational,
•Natural
•Pharmacological

Сommunal allergens are contained in the air of
apartment houses. They are:
House-dust mites which live in carpets سجادة,
mattresses and upholstered المنجد ;furnitureاالثاث
Vital products of domestic insects (e.g.,
cockroachالصرصور);
Tobacco smoke during active or passive smoking;
Various communal aerosols and synthetic
detergents.

Among the industrial allergens nitric, carbonic,
sulfuric oxides, formaldehyde, ozone and emissions of
biotechnological industry - main components of industrial
and photochemical.
The most important occupational allergens are
dust of stock buildings, mills مطاحن , weaving-mills, book
depositories etc.
Natural allergens are represented by plant pollen
(especially ambrosia عطور, wormwood and goose-foot pollen)
and different respiratory, particularly viral, infections.

Some allergens which may cause asthma
House-dust mites which live in carpets, mattresses and upholstered furniture
Spittle, excrements, hair and fur of domestic animals
Plant pollen
Pharmacological agents (enzymes, antibiotics, vaccines, serums)
Food components (stabilizers, genetically
modified products)
Dust of book depo-sitories

Asthma Triggers
©2010

Trigger-factors, which provoke
bronchospasm, are: a simultaneous penetration
of a large quantity of allergen, viral respiratory
infection, hyperventilation, physical exertion,
emotional stress, becoming too cold, adverse
weather conditions, administration of some
medicines (aspirin, -blockers).

Pathophysiology
Asthma pathophysiology is quite
difficult and insufficiently studied. Undoubtedly,
in most cases the disease is based on 1 type
hypersensitivity reaction. The genesis of
any allergic reaction may be divided into
immune, pathochemical and pathophysio-
logic phases.

Classifications of Asthma
1. Spasmodic: sporadic in nature with varying
intervals of free and difficulty due to
precipitating factors often readily defined.
2. Continuous: some shortness of breath on
occasion, transit wheezing on strenuous
exercise and wheezy rales hard deep
inspiration.

Classifications of Asthma cont…
3. Intractable: persistent wheezing
requiring regular daily medication for either
control of symptoms or ability to function.
4. Status Asthmaticus: sever attach in
which patient deteriorates in spite of
adequate treatment.


Clinical manifestationsClassic signs and symptoms of asthma are:
Attacks of expiratory dyspnea
Shortness of breath
Cough.
Chest tightness
Wheezing (high-pitched whistling sounds when
breathing out)
Sibilant rales

In typical cases in development of asthma exacerbation there are 3 periods – prodromal period, the height period and the period of reverse changes.
At the prodromal period:
vasomotoric nasal reaction with profuse watery discharge,sneezing, dryness in nasopharynx, paroxysmal cough with viscous sputum, emotional lability, excessive sweating, skin itch and other symptoms may occur.

At the peack of exacerbation there are:
expiratory dyspnea
forced position with supporting on arms
poorly productive cough
cyanotic skin and mucous tunics
hyperexpansion of thorax with use of all accessory muscles
during breathing
at lung percussion: tympanitis, shifted downward lung
borders
at auscultation: diminished breath sounds, sibilant rales,
prolonged breathing-out, tachycardia.
in severe exacerbations: the signs of right-sided heart
failure (swollen neck veins, hepatomegalia), overload of
right heart chambers on ECG.

At the period of the reverse changes,
Which comes spontaneously or under
pharmacologic therapy.
Dyspnea and breathlessness relieve or
disappear.
Sputum becomes not so viscous.
Cough turns to be productive.
Patient breathes easier.

Asthmatic statusThe severe and prolonged asthma exacerbation with
intensive progressive respiratory failure, hypoxemia,
hypercapnia, respiratory acidosis, increased blood viscosity and
the most important sign is blockade of bronchial 2-receptors.
Stages:
1st - refractory response to 2-agonists (relaxation of the smooth
muscles)
2nd - “silent” lung because of severe bronchial obstruction and
collapse of small and intermediate bronchi;
3rd stage – the hypercapnic coma.

In many cases asthma, particularly intermittent,
manifests with few and atypical signs:
episodic appearance of wheezing;
cough, heavy breathing occurring at night;
cough, hoarseness after physical activity;
“seasonal” cough, wheezing, chest tightness
the same symptoms occurring during contact with
allergens, irritants;
lingering course of acute respiratory infections.

DiagnosisTypical clinical manifestations and lung function assessment are sufficient for diagnosis of asthma.

Management1. Avoiding the contact with allergen. If it is impossible, the
specific hyposensitization with standard allergens should
be performed. It is rather effective in case of monoallergy,
in intermittent and mild persistent asthma, in remission
phase.
2. Elimination of trigger factors (rational job placement,
changing the residence, psychological and physical
adaptation, careful drug using) is the second condition for
successful asthma treatment.
3. Optimally selected medical care is the base of asthma
management.

Combined inhaled drugs (corticosteroids with 2-agonists) (nebulasers, turbuhalers, spasers, spinhalers, sinchroners) enhance the effectiveness of asthma therapy.

Management of asthmatic status
Oxygen
Systemic corticosteroids (Hydrocortisone 200mg or
Prednisolone 50 mg/day per)
Inhalations of short-acting 2-agonists - Salbutamol 5mg or
Fenoterol 2mg through nebulaser – 3 times at 1st hour, then
once an hour till distinct improvement of patient’s condition is
achieved; then 3-4 times a day.
Inhaled anticholinergic drugs or Aminophylline IV.
If ineffective - artificial lung ventilation.

Prognosis
In case of early detection and adequate
treatment the prognosis for the disease is
favourable.
It becomes serious in severe persistent
and poorly controlled (insensitive for
corticosteroids) asthma.

The examination of working capacity
The patients with unfavorable for the
disease conditions of work need the job
replacement.
Physical labours with severe asthma are
disable to work.

Prophylaxis
Preservation of the environment,
healthy life-style (smoking cessation,
physical training) – are the basis of primary
asthma prophylaxis. These measures in
combination with adequate drug therapy
are effective for secondary prophylaxis.