Bordetella pertussis
53
DR.T.V.RAO MD 1 Dr.T.V.Rao MD BORDETELLA PERTUSSIS WHOOPING COUGH
-
Upload
tumalapalli-venkateswara-rao -
Category
Health & Medicine
-
view
5.309 -
download
3
description
Bordetella pertussis
Transcript of Bordetella pertussis

DR.T.V.RAO MD 1
Dr.T.V.Rao MD
BORDETELLA PERTUSSISWHOOPING COUGH

A TRIBUTE TO BORDET - GENGOU
DR.T.V.RAO MD 2

WHAT IS WHOOPING COUGH
DR.T.V.RAO MD 3
• Whooping Cough (Pertussis) is a bacterial infection of the lungs which is caused by a bacterium Bodetella pertussis. It is a very contagious disease which causes coughing with little or no fever. The coughing may be so severe that it leads to vomiting and aspiration.

HOW THE NAME WHOOPING DERIVED
DR.T.V.RAO MD 4
• Whooping cough is an infectious bacterial disease that causes uncontrollable coughing. The name comes from the noise you make when you take a breath after you cough. You may have choking spells or may cough so hard that you vomit.

IDENTIFICATION BODETELLA
DR.T.V.RAO MD 5
• Jules Bordet and Gengou contributed for discovery 1900
• Identified as small bacilli in children with Whooping cough.
• Bodetella pertussis ( Intense cough )
• Other related Bacteria
B.parapertussis
B.brochoseptica
B.avium

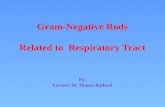
BORDETELLA PERTUSSIS ( B G BACILLUS )
• Gram negative organism
• Small, ovoid,cocobacillus.
• Length is 0.5 microns
• Have bipolar metachromatic granules when stained with Toluidine blue
DR.T.V.RAO MD 6

BODETELLA PERTUSSIS ( B G BACILLUS)
• Small ovoid coccobacillus 0.5 microns
• On repeated cultures becomes become larger thread like bacilli.
• Non motile, Non sporing
• Capsulated – loose on repeated culturing
DR.T.V.RAO MD 7

OTHER CHARACTERS• Do not swell in the
presence of antigen.• Loose clumps of bacilli
appear as thumb print appearance with clear space between the organisms.
• Freshly isolated strains have fimbria.
DR.T.V.RAO MD 8

CULTURE CHARACTERS• Aerobic Not anaerobic• Grows optimally at 350 to 370 c• Preferred medium – Bordet
Gengou glycerin potato blood agar
• Blood for neutralizing inhibitory substances formed during bacterial growth.
• Charcoal also serves the same purpose.
DR.T.V.RAO MD 9

MERCURY DROP COLONIES ON BORDET-GENGOU MEDIUM
• Growth takes longer up to 48 – 72 hours
• On blood agar appear as small dome shaped opaque viscid grayish white retractile
• Resembles bisected pearly or mercury drops
DR.T.V.RAO MD 10

ALUMINUM PAINT APPEARANCE
• Colonies surrounded by hazy zone of hemolysis• Confluent growth
presents as aluminum paint.
DR.T.V.RAO MD 11

BIOCHEMICAL REACTIONS• In active – do not ferment
sugars
• Indole test +
• Reduce Nitrates
• Utilize citrates
• Splits urea
• Catalase +
• Oxidase +
DR.T.V.RAO MD 12

RESISTANCE
DR.T.V.RAO MD 13
• Killed by heat at 550c for 30 mt• Drying and disinfectants kill the
organism• Survive outside for 5 days• 3 days on cloths• Few hours on paper

ANTIGENIC CHARACTERS AND VIRULENCE
DR.T.V.RAO MD 14
• Agglutinogens - Species specific surface agglutinogens with capsule K antigens or fimbria
• 14 agglutinin factors are identified
• Factors 7 is common in all species
• Factor 1- 6 in only B pertussis
• Factor 12 in B.brochoseptica
• Factor 14 in B Para pertussis

VIRULENCE FACTORS
DR.T.V.RAO MD 15
• These virulence factors include adhesions such as filamentous hem agglutinin, agglutinogens, peractin, and fimbriae as well as a number of toxins including pertussis toxin, acetylate cyclase toxin, trachael cytotoxins, Dermonecrtoic toxin and heat-labile toxin (CDC, 2005).

PATHOGENESIS OF B.PERTUSSIS
• Like most Gram negative pathogens, B. pertussis also contains a Lipopolysaccharide coat that acts as an Endotoxin and can aid colonization by agglutinating human cells (Steele, 2004).
DR.T.V.RAO MD 16

VIRULENT MOLECULES
DR.T.V.RAO MD 17

TOXIN – CELLULAR ACTION.
DR.T.V.RAO MD 18

MECHANISM OF INFECTION• 1,2,3 are common
infective strains vaccines contain all the three Agglutinogens promoting virulence by helping bacteria to attach to respiratory epithelial cells
DR.T.V.RAO MD 19

• Pertussis toxin – MW 1,17,000
• Hexamer protein composed of 6 subunits with A – B structure
• A has enzymatic activity it can be toxoided
• Pertussis toxin is the major component of Acellular Pertussis vaccine.
PERTUSSIS TOXIN
DR.T.V.RAO MD 20

NATURE OF TOXIN
DR.T.V.RAO MD 21
• It produces a highly lethal toxin (formerly called Dermonecrtoic toxin) which causes inflammation and local necrosis adjacent to sites where B. pertussis is located. The lethal toxin is a 102 kDa protein composed of four subunits, two with a mw of 24kDa and two with mw of 30 kDa.

PERTUSSIS TOXIN
DR.T.V.RAO MD 22
• Causes pathogenesis• Present only in B.pertussis• Pertussis toxin is expressed on the surface, secreted
into the surrounding medium• Posses Biochemical and Biological activity of producing
lymphocytosis producing factor causes Lymphocytosis• Acts as Histamine sensitizing factor• Islet activating function – causes excessive Insulin
secretion.

FILAMENTOUS HEMAGGLUTININ
DR.T.V.RAO MD 23
• One of the Hemagglutinins produced by B.pertussis • Filamentous Haemagglutinnins adheres
to cilia of the respiratory epithelium and to erythrocytes• Helps in binding to respiratory epithelium

OTHER TOXINS
DR.T.V.RAO MD 24
Adenylate cyclase
• Enters the target cells and acts as toxin• It acts by catalyzing the production of cAmp
by various types of cells.
Heat labile Toxin
• Cytoplasmic protein present in Bordetella• Dermonecrtoic and lethal in Mice

TRACHEAL TOXIN
DR.T.V.RAO MD 25
• L M W – peptidoglycan• Causes ciliary damage, produced by all
Bodetella• It induces ciliary damage in hamster tracheal
ring• Lipolysacchardie acts as in Gram –ve bacilli• Pertactin – OMP produces immunity in mice.

• B pertussis may alter from smooth to rough variation
• Phase I to Phase II Phase III Phase IV( rough stage ) which is rough and avirulent form
VARIATION SMOOTH TO ROUGH
DR.T.V.RAO MD 26

PATHOGENICITY• An obligate parasite
• Intranasal inoculation in mice induces a characteristic patches and intensive pneumonia like In humans
• Incubation is 1 to 2 weeks
DR.T.V.RAO MD 27

• The incubation period (the time between infection and the onset of symptoms) for whooping cough is usually 7 to 10 days, but can be as long as 21 days.
INCUBATION IN WHOOPING COUGH
DR.T.V.RAO MD 28

STAGES OF INFECTION
DR.T.V.RAO MD 29
• 1 Catarrhal• 2 Paroxysmal• 3 Convalescent Each stage lasts 2 weeks Catarrhal stage is Maximal infective Antibiotics are useful.

PAROXYSMAL STAGE
DR.T.V.RAO MD 30
• Cough increases – distinctive bouts• Violent spasms of continuous coughing• With violent act of cough, air enters into empty lung
with characteristic whoop Enters into next stage
• Leads to convalescence• And severity of cough decreases• Total disease lasts for 6- 8 weeks.

VIOLENT PAROXYSMS OF COUGH
DR.T.V.RAO MD 31

COMPLICATIONS
DR.T.V.RAO MD 32
• The violent bouts of cough leads to
Subconjuctival hemorrhage Subcutaneous emphysema Bronchopneumonia Lung collapse Neurological complications Epilepsy, paralysis, mental retardation, blindness,
deafness.

EPIDEMIOLOGY
DR.T.V.RAO MD 33
• Predominately a pediatric disease• Highest in the 1st year of life• Maternal antibodies are not protective.• Females suffers more than males.• World wide in distribution• Epidemics occurs periodically.• In early stage of infection droplets and fomites
contaminated by oropharengeal secretion are infective.
• Non immune rarely escape infection

EPIDEMIOLOGY
DR.T.V.RAO MD 34
• House hold contacts at risk
• Chronic carriers are not known
• B.pertussis - 95 %
• B.parapertussis – 5%
• B.brochoseptica occasionally occur
• Some times Adenovirus, Mycoplasma pneumonia may mimics whooping cough.

• Since the early symptoms are so non-specific, pertussis is usually not diagnosed until the appearance of the characteristic cough. Pertussis can be confirmed by taking cultures of respiratory fluids for examination in the laboratory. This involves taking a sample of secretions from the nose or throat and identifying the pertussis bacteria in the secretion
HOW WHOOPING COUGH DIAGNOSED
DR.T.V.RAO MD 35

• Isolation by culture• PCR• Direct fluorescent
antibody• Serological testing
DIAGNOSIS
DR.T.V.RAO MD 36http://medinfo.ufl.edu/year2/mmid/bms5300/images/d7053.jpg

• Microscopy
• Culture.
• Microscopy – Demonstration of Bacilli in respiratory secretions.
• Florescent Antibody methods
LABORATORY DIAGNOSIS
DR.T.V.RAO MD 37

DR.T.V.RAO MD 38

• Culture plate held at 10-15 cm infront of the mouth when the patient is coughing spontaneously or induced cough
• Droplets of respiratory exhaled impinge on the media.
• Helpful as bed side investigation
COUGH PLATE METHOD
DR.T.V.RAO MD 39

COUGH PLATE METHOD
DR.T.V.RAO MD 40

NASOPHARYNGEAL SWAB• Secretion from the
posterior pharyngeal wall are collected with cotton swab on a bent wire passed from the oral cavity
• A West’s post nasal swab is used for collection of specimen.
DR.T.V.RAO MD 41

PER NASAL SWAB• Swab on a flexible wire
is passed along the floor of the nasal cavity and material collected from Pharyngeal wall
• Dacron or Calcium alginate swabs are better
DR.T.V.RAO MD 42

TRANSPORT MEDIUM• Transferred into
Casamio acid solution at pH 7.2 in modified Stuarts medium Glycerin potato blood agar of Bordet Gengou
• Adding Pencillin becomes more selective
DR.T.V.RAO MD 43

IDENTIFICATION OF BACTERIA• The culture plates are
incubated at 360c
• The bacteria are identified by Microscopy and slide agglutination
• Immunofluorescence methods
DR.T.V.RAO MD 44

• Paired serum sample for detection of antibodies
• Gel precipitation testing
• Complement fixation test
• Detection of Ig A by ELISA from nasopharyngeal secretions.
SEROLOGY
DR.T.V.RAO MD 45

EARLY IMMUNIZATION IS BEST SOLUTION TO PREVENT THE PERTUSSIS
DR.T.V.RAO MD 46

HOW WHOOPING PREVENTED• Pertussis can be
prevented by the pertussis vaccine, which is part of the DTaP (diphtheria, tetanus, a cellular pertussis) vaccine. These important immunizations are routinely given in five doses before a child's sixth birthday.
DR.T.V.RAO MD 47

PROPHYLAXIS
DR.T.V.RAO MD 48
• Alum absorbed vaccine is better• Administered in combination with Diphtheria, and
tetanus toxoid• B pertussis acts as an adjuvant• Early immunization, is essential in prevention of
infection.• Later doses are given at the interval of 4 – 6 weeks
intervals, before 6 moths 3 doses are completed.

BOOSTER DOSES
DR.T.V.RAO MD 49
• A booster at the end of the 1st year• Another dose at 4th year• Chemoprophylaxis with Erythromycin when exposed to contacts in
the vicinity• Complications with vaccination Post vaccinial encephalopathy 5 – 10 million doses Neurotic complications Stop further vaccination Do not vaccinate after 7 years

ADVANTAGES OF ACELLULAR VACCINE
DR.T.V.RAO MD 50
• An acellular vaccine containing whole antigen has been developed and found to elicit good antibody response with fewer side effects. It has replaced the classical vaccine in Japan since 1981 with success, with fewer out breaks and less side effects. whooping cough vaccine can be made from various components of the Bodetella pertussis bacterium, rather than the whole organism. This "acellular" vaccine works well but has fewer side effects than the traditional "whole cell" version.

• Contain the Pertussis bacilli
• Contain PT FHA Agglutinogens 1, 2, 3
• Produces immunity in 90 % of individuals
• Immunity in only 50 % by 12th year
ACELLULAR VACCINES
DR.T.V.RAO MD 51

• Penicillin is not useful
• 10 days of Erythromycin is useful in early infection
• Chloramphenicol and Cotromoxazole are effective.
TREATMENT
DR.T.V.RAO MD 52

• Programme Created by Dr.T.V.Rao MD for Medical and Paramedical Students
DR.T.V.RAO MD 53