
Babies Remember and Babies Can’t Wait: Translating Research Into Public Policy For Young Children...
54
Babies Remember and Babies Can’t Wait: Translating Research Into Public Policy For Young Children and Families Alicia F. Lieberman, PhD Irving B. Harris Chair of Infant Mental Health University of California San Francisco © Alicia F. Lieberman, Ph.D.
-
Upload
graciela-paper -
Category
Documents
-
view
216 -
download
1
Transcript of Babies Remember and Babies Can’t Wait: Translating Research Into Public Policy For Young Children...

Babies Remember and Babies Can’t Wait:Translating Research Into Public Policy
For Young Children and Families
Alicia F. Lieberman, PhD
Irving B. Harris Chair of Infant Mental Health
University of California San Francisco
© Alicia F. Lieberman, Ph.D.

An Ecological-TransactionalModel of Development
“Development Lasts A Lifetime”
Protective & Risk Factors
“Allostatic load”
Macrosystem: Cultural practices
Exosystem: Neighborhood & community
Microsystem: Family inter-relationships
Ontogenetic development: The Individual
(Bronfenbrenner, 1979; Cicchetti & Lynch,1993; Sameroff, 1993; Rutter,2000)
© Alicia F. Lieberman, Ph.D.

What Is Mental Health?
“The capacity
to love well and to work well”
(Sigmund Freud)
© Alicia F. Lieberman, Ph.D.

What Is Infant Mental Health? The capacity to grow well and to love well
• Experience, express and regulate emotions & recover from dysregulation
• Establish trusting relationships & repair conflict• Explore and learn
Within the society’s cultural values (Lieberman; Zero to Three)
© Alicia F. Lieberman, Ph.D.

Normative, Developmentally
Appropriate Stress
Emotionally Costly Stress
Traumatic Stress
A Continuum From Stress To Trauma And
Secondary Adversities
© Alicia F. Lieberman, Ph.D.

Defining Trauma
• A traumatic event overwhelms the capacity to cope
• Threatens physical or psychological integrity
• Key features of trauma: Unpredictability Horror
Helplessness
(DC:0-3R, 2004; Freud, 1926; Pynoos et al., 1999)
© Alicia F. Lieberman, Ph.D.
Frequent Traumatic Stressors In Childhood
• Exposure to violence Child Abuse Domestic Violence Community Violence
• Accidents Car crashes Near drownings Dog bites
Burns
© Alicia F. Lieberman, Ph.D.

Violence As Paradigm of Childhood Trauma
• More children die from abuse in their first year of life thanat any other time
• Half of child abuse victims are under age 7
• 85% of abuse fatalities are under age 6
• U. S. ranks THIRD among 27 industrialized countries in child maltreatment deaths
(Gentry, 2004; UNICEF, 2003;
Children’s Bureau, 2003)
© Alicia F. Lieberman, Ph.D.

War
Community Violence
Domestic Violence
Child Abuse
Children’s Exposure to Violence
© Alicia F. Lieberman, Ph.D.

Sources of Violence Overlap
• Children exposed to domestic violence– 15 times more likely to be abused than the national
average– 30-70% overlap with child abuse– At serious risk of sexual abuse
• Battered women– Twice more likely to abuse their children than
comparison groups(Osofsky, 2003; Edleson, 1999; Margolin & Gordis, 2000; McCloskey, 1995)
© Alicia F. Lieberman, Ph.D.

Adverse Childhood Experiences Last A Lifetime
• Emotional, physical or sexual abuse
• Domestic violence against the mother
• Household member with mental illness
• Household member with substance abuse
• Household member ever imprisoned
• Absence of one or both parents
• Physical or emotional neglect
Predict the 10 leading causes of adult death/disability
(ACE Study, Felitti et al. 1998)
© Alicia F. Lieberman, Ph.D.

Adverse Childhood Events And Adult Depression
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
012345+
Odd
s R
atio
Adverse EventsChapman et al, 2004

Adverse Childhood Events And Adult Substance Abuse
0
2
4
6
8
10
12
14
16
0 1 2 3 4+
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5+
%
Self-Report: Alcoholism Self-Report: Illicit Drug UseDube et al, 2002 Dube et al, 2005
%

Adverse Childhood Events And Adult Ischemic Heart
Disease
0
0.5
1
1.5
2
2.5
3
3.5
012345,67,8
Dong et al, 2004 Adverse Events
Odd
s R
atio
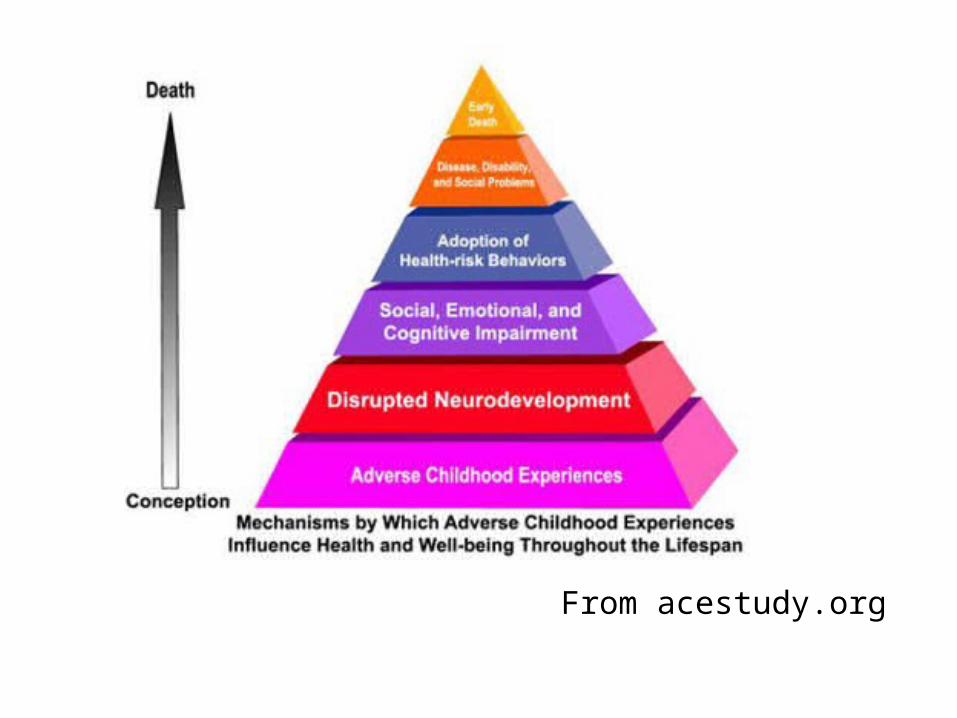
From acestudy.org

National Comorbidity Survey Replication
• The National Comorbidity Survey Replication (NCS-R) sample was collected in 2001-2003 (N= 5692, response rate = 70.9%)
• Face-to-face structured diagnostic interview for 26 DSM Axis I disorders
• The weighted sample is representative of U.S. population on census indicators (age, gender, race, education, marital status, region)
OhioCanDo4Kids.Org

Cumulative Risk Scores
• The NCS-R inquired about adverse childhood antecedents occurring ≤18 years including: 1) sexual abuse, 2) physical abuse, 3) parental depression, 4) parental substance abuse, 5) being a crime victim, 6) loss of a parent and 7) exposure to domestic violence
• For each subject, a Cumulative Risk Score (CRS) was calculated by adding the number of positive childhood antecedents that happened ‘most’ or ‘all’ of the time.
• An “ACE-type” analysis was performed comparing the number of lifetime DSM diagnoses for CRS = 0, 1, 2, 3, and ≥ 4 or more childhood antecedents
OhioCanDo4Kids.Org
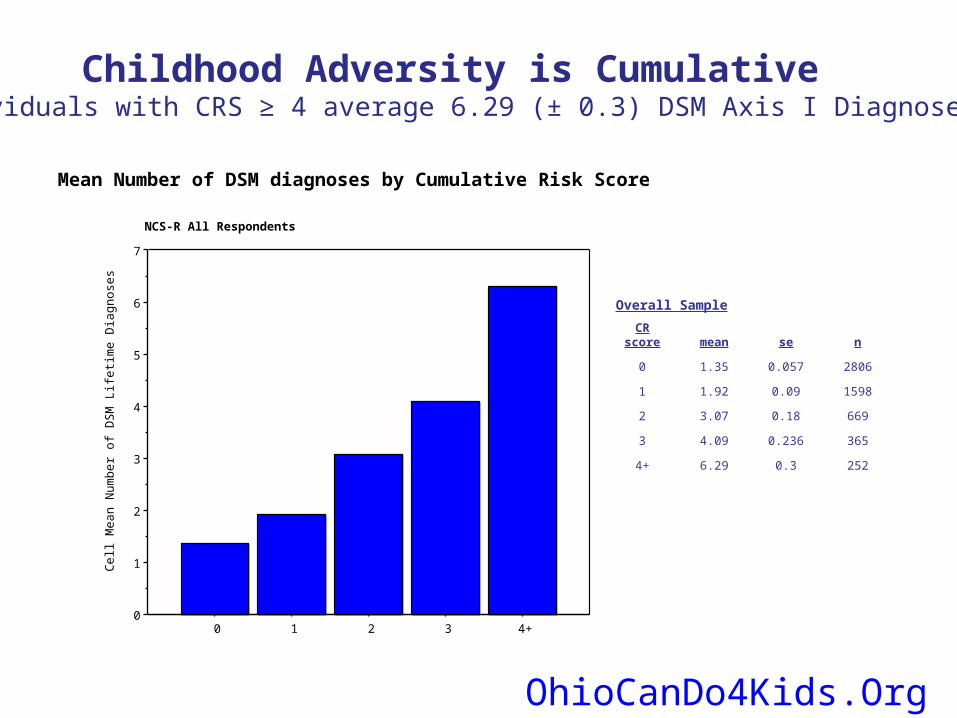
Mean Number of DSM diagnoses by Cumulative Risk Score
2520.36.294+
3650.2364.093
6690.183.072
15980.091.921
28060.0571.350
nsemeanCR score
Overall Sample
0
1
2
3
4
5
6
7
Cel
l Me
an N
umb
er o
f D
SM
Life
time
Dia
gn
ose
s
0 1 2 3 4+
NCS-R All Respondents
Childhood Adversity is CumulativeIndividuals with CRS ≥ 4 average 6.29 (± 0.3) DSM Axis I Diagnoses
OhioCanDo4Kids.Org
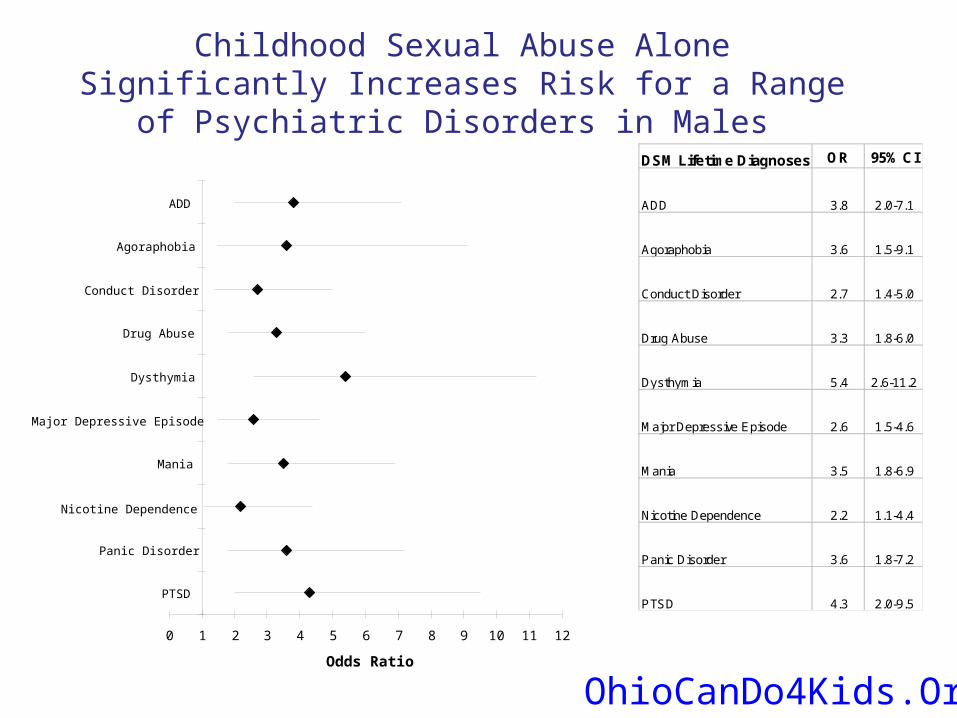
Childhood Sexual Abuse Alone Significantly Increases Risk for a Range of Psychiatric Disorders in Males
0 1 2 3 4 5 6 7 8 9 10 11 12
PTSD
Panic Disorder
Nicotine Dependence
Mania
Major Depressive Episode
Dysthymia
Drug Abuse
Conduct Disorder
Agoraphobia
ADD
Odds Ratio
DSM Lifetime Diagnoses OR 95% CI
ADD 3.8 2.0-7.1
Agoraphobia 3.6 1.5-9.1
Conduct Disorder 2.7 1.4-5.0
Drug Abuse 3.3 1.8-6.0
Dysthymia 5.4 2.6-11.2
Major Depressive Episode 2.6 1.5-4.6
Mania 3.5 1.8-6.9
Nicotine Dependence 2.2 1.1-4.4
Panic Disorder 3.6 1.8-7.2
PTSD 4.3 2.0-9.5
OhioCanDo4Kids.Org

Childhood Sexual Abuse Alone Significantly Increases Risk for a Range of Psychiatric Disorders in Females
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
PTSD
Oppositional Defiant Disorder
Nicotine Dependence
Mania
Major Depressive Episode
Intermittent Explosive Disorder
Drug Abuse
Bipolar I
Alcohol Dependence
ADD
Odds Ratio
DSM Lifetime Diagnoses OR 95% CI
ADD 2.5 1.7-3.9
Alcohol Dependence 4.7 3-7.3
Bipolar I 6.6 3.4-13
Drug Abuse 5.2 3.8-7.1
Intermittent Explosive Disorder 3.1 2.3-4
Major Depressive Episode 2.4 1.9-3
Mania 3.6 2.3-5.5
Nicotine Dependence 2.6 1.6-4.3
Oppositional Defiant Disorder 4.1 2.3-7.1
PTSD 4.8 3.4-6.8
OhioCanDo4Kids.Org

Conclusions From NCSR Data
• Increasing Childhood Risk Scores (CRS) are associated with an increased number of DSM diagnoses on structured interview in a nationally representative sample
• Individuals with CRS ≥ 4 average more than 6 DSM diagnoses
• Diagnoses in individuals with a high CRS cross multiple DSM diagnostic categories
OhioCanDo4Kids.Org

Infant Mental Health Disorders
• Increasing awareness that young children
can have emotional problems
• Two diagnostic classifications provide a basis for studies of construct validity– Research Diagnostic Criteria (2003)– DC: 0-3-Revised (2005)

Prevalence of Psychiatric Diagnosis In Toddlers and Preschoolers
2-5 year olds recruited from pediatric
public health clinic
(Egger, 2004)
Durham Pediatric Durham Pediatric SampleSample
n=307n=307
Any emotional Any emotional disorderdisorder 10.6%10.6%
Any behavioral Any behavioral disorderdisorder 11.3%11.3%
Any disorderAny disorder 17.4%17.4%
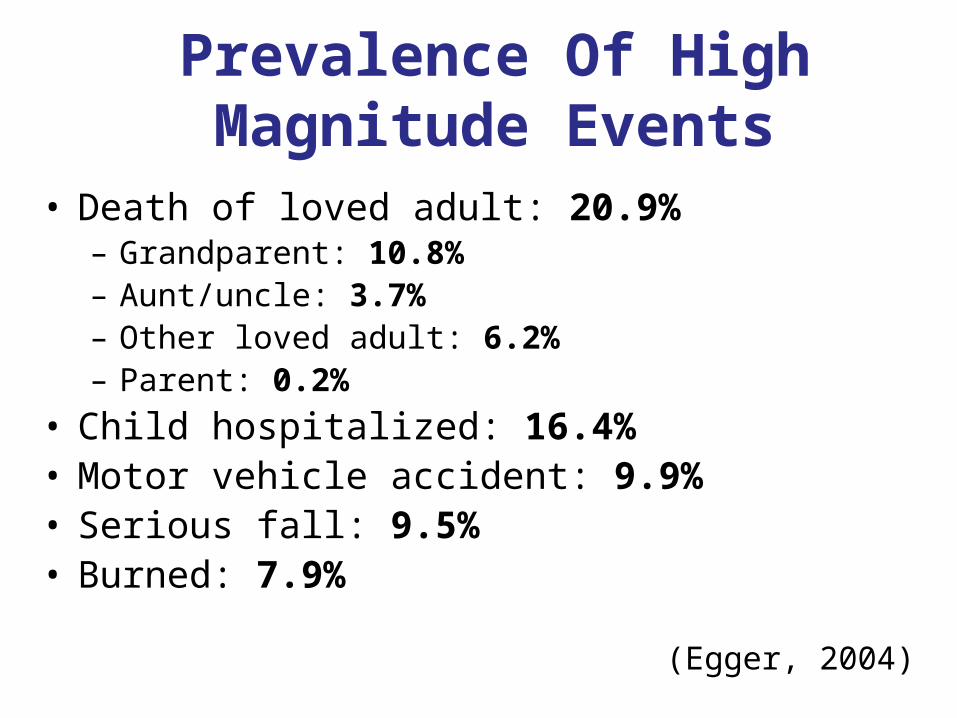
Prevalence Of High Magnitude Events
• Death of loved adult: 20.9%– Grandparent: 10.8%– Aunt/uncle: 3.7%– Other loved adult: 6.2%– Parent: 0.2%
• Child hospitalized: 16.4%• Motor vehicle accident: 9.9%• Serious fall: 9.5%• Burned: 7.9%
(Egger, 2004)

Stressors Happen To Young Children
• 52.5% experienced at least one major stressor
• No gender or race differences
• Preschoolers more likely to experience a major stressor, but 42% of 2-year olds had experienced at least one such event
(Egger, 2004)

Cumulative Stressors And Psychiatric Disorders
0%10%20%30%40%50%60%70%80%90%
100%
% w
ith
a D
SM
-IV
dis
ord
er
1 2 3 4 5 6 ormore
Low mag
High mag
Egger, 2004

Childhood Adversity And Minority Status
• Minority children are more likely to be poor
• Traumatic events cluster when there is poverty
• The impact of traumatic events is cumulative
• Minority children are more vulnerable to a traumatic event due to cumulative effect of adversities and less access to services
(Oser & Cohen, 2003; Flores et al., 2002;U.S. Surgeon General’s Report, 2001 )

When Systems Compound Adversity: Child Welfare
and Foster Care
No race differences in abuse and neglect reportsChildren of color are:
• more often placed in out of home care• subjected to more placement changes• kept longer in foster care• less likely to be reunified with parents
(Casey Family Programs Child Welfare Fact Sheet, 2005)

The Forgotten Mental Health Needs of Children in Child Welfare
• About half of these children have a diagnosed mental health need
• 75% of diagnosed children did not receive mental health treatment within 12 months of a child abuse or neglect investigation
• Children of color are disproportionally affected
(Pre-publication Copy: Improving the Quality of Health Care for Mental and Substance-Use Conditions, Institute of Medicine, 2006)

The Body Remembers
(As cited by Felitti & Anda, 2003; Source CDC)

Traumatic StressIn Infants And Young Children
• Re-experiencing trauma (flashbacks, nightmares)
• Numbing (social withdrawal, play constriction)
• Increased arousal (attention problems, hypervigilance)
• New Symptoms Aggression Sexualized behavior New fears Loss of developmental milestones (Regression)
© Alicia F. Lieberman, Ph.D.

Early Social Consequences Of Aggression
• Gilliam (2005): Pre-K students expelled at a rate 3x higher than K-12 peers (6.67 v. 2.09)
0
5
10
15
20
25
30
Expulsion
PrivateStateK-12

A Continuum of Services
Normative Stress
Costly Stress
Traumatic Stress
Prevention Intervention Treatment
© Alicia F. Lieberman, Ph.D.

Cross-System Collaboration:Prevention, Intervention, Treatment
Infant Mental Health Services
Zeanah, Stafford & Nagle, 2005

Quality Of Early Child Care • NICHD 10-site prospective, longitudinal study • N= 1364 newborns from infancy through school age• Impact of variations in early child care experiences
– Smaller group sizes– Lower child-adult ratios – Skilled, warm, responsive caregivers– Safe, clean, stimulating physical environments
• Fewer than 50% of centers met NAEYC standards• 20% failed to meet any of the standards for infants• On average, 8% of centers are accredited across U.S.
Childcare Quality Matters
• Quality of care was most important predictor of
-- Peer relations -- Attention span -- Memory skills
-- Vocabulary
• Quality of parent-child relationship quality a better predictor than child care variables
(NICHD Study of Early Child Care)

Goal of Early Intervention:Creating Angels In The Nursery
• Benevolent experiences also last a lifetime
• Re-creating relationships, recreating the self
• The intervenor as agent of hope
• Life as “chiaroscuro”:
Interplay of light and darkness
© Alicia F. Lieberman, Ph.D.

Parent As Protective Shield

Nurse Family PartnershipNational Outcomes
Reductions in:• Child abuse & neglect 79%• Emergency room visits 56%• Maternal substance abuse 44%• Maternal arrests 69%• Subsequent pregnancies 32%
Increase in work engagement: 83%
Reductions in:• Child arrests 56%• Child convictions 81%

Treatment Goals:Safety In The Relationship Safety In The Sense of Self

Therapeutic Objectives• Affect Regulation
• Normalization of traumatic response
• Trust in bodily sensations
• Reciprocity in relationships
• Differentiate remembering and reliving
• Engagement in learning
© Alicia F. Lieberman, Ph.D.

Individualizing Treatment: Theoretical Integrations
• Developmentally Informed• Attachment focus• Trauma-based • Psychoanalytic theory• Social Learning processes• Cognitive–Behavioral strategies• Culturally attuned
(Lieberman & Van Horn, 2005)
© Alicia F. Lieberman, Ph.D.

Child-Parent PsychotherapyIntervention Modalities
1. Promote development: Play, language, touch
2. Unstructured/reflective developmental guidance
3. Modeling protective behaviors
4. Interpretation: linking past and present
5. Emotional support
6. Concrete assistance, case management, crisis intervention
© Alicia F. Lieberman, Ph.D.
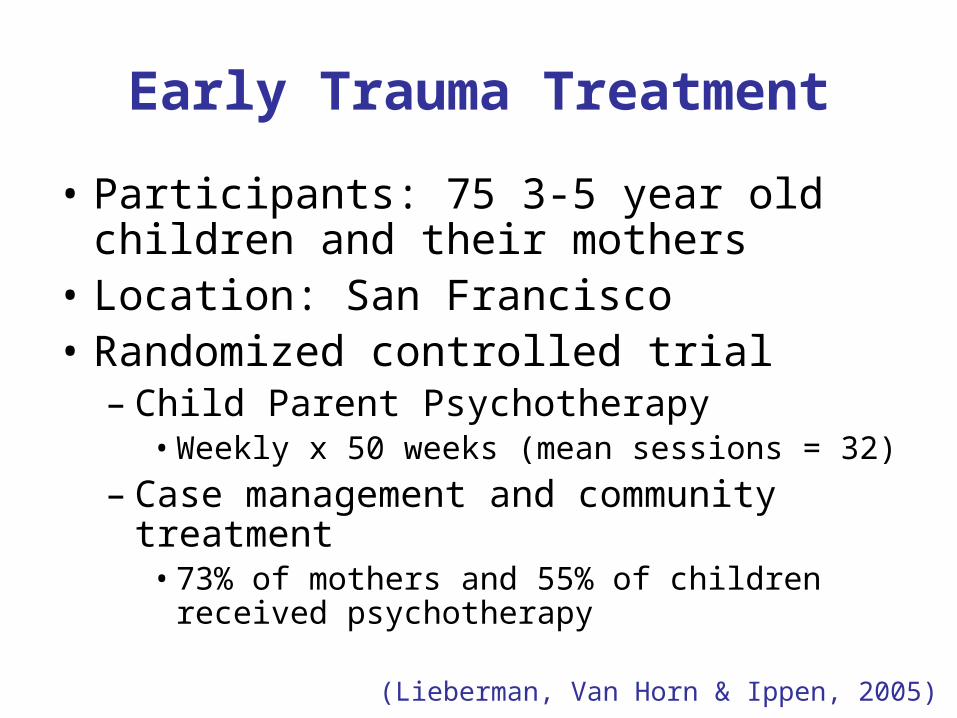
Early Trauma Treatment
• Participants: 75 3-5 year old children and their mothers
• Location: San Francisco• Randomized controlled trial
– Child Parent Psychotherapy• Weekly x 50 weeks (mean sessions = 32)
– Case management and community treatment• 73% of mothers and 55% of children received
psychotherapy
(Lieberman, Van Horn & Ippen, 2005)

Early Trauma Treatment
• Findings– Children
• Reduced number of posttraumatic symptoms in CPP but not controls
• Reduced number of behavior problems in CPP but not controls
– Mothers• Reduced number of posttraumatic symptoms for
CPP and controls• Reduced mothers’ distress for CPP but not
controls
(Lieberman, Van Horn & Ippen, 2005)

Percentage of Children Diagnosed with PTSD
0
5
10
15
20
25
30
35
40
45
50
Intake Completion
Child/ParentPsychotherapyComparison
(Lieberman, Van Horn & Ippen, 2005)

Percentage of Mothers Diagnosed with PTSD
0
5
10
15
20
25
30
35
40
45
50
Intake Completion
Child/ParentPsychotherapyComparison
Lieberman, Van Horn & Ippen, 2005

Empirical Support For Relationship-Based Treatment
• Five randomized studies with about 500 children and mothers
• Infants, toddlers, preschoolers• Anxious attachment, child maltreatment, maternal depression, domestic violence• Range of SES, multicultural samples• Consistent findings of CPP efficacy• Measures: Cognitive performance, quality of attachment,
quality of child-mother relationship, mental representations, maternal and child diagnoses
(Lieberman et al., 1991; Cicchetti et al., 1999, 2000; Toth et al., 2002; Toth et
al., 2006; Lieberman et al., 2005, 2006)

Treatment Is Not Enough: Ecology Matters
Protective & Risk Factors
“Allostatic load”
Macrosystem: cultural practices
Exosystem:neighborhood & community
Microsystem: family inter-relationships
Ontogenetic development: individual adaptation
(Bronfenbrenner, 1979; Cicchetti & Lynch,1993; Sameroff, 1993; Rutter,2000)
© Alicia F. Lieberman, Ph.D.
Trauma As A Supra-ClinicalPhenomenon
“This ecological-transactional approach, although long recommended, is seldom implemented. …child trauma is seen only as a clinical phenomenon… This narrow focus must be super-ceded by the ubiquity of trauma as the frequent cause of physical and mental illness, school underachievement and failure, substance abuse, maltreatment, and criminal behavior… we are dealing with a supra-clinical problem that can only be resolved by going beyond the child’s individual clinical needs to enlist a range of coordinated services for the child and the family.” (Harris, Lieberman & Marans, 2007)
© Alicia F. Lieberman, Ph.D.

A Compelling Conclusion
• “The overarching question of whether we can intervene successfully in young children’s lives has been answered in the affirmative and should be put to rest.”
• “However, interventions that work are rarely simple, inexpensive, or easy to implement”.
(From Neurons to Neighborhoods, 2000)

What Can We Do?• Promote family-friendly policies - child safety net, family leave, childcare• Early intervention: “Pre-K, starting at birth for those who need it”*• Promote inter-system coordination: - early identification and referral• Fund training to build and preserve capacity
- primary care providers- childcare providers- infant mental health providers- child protection workers
(*Sam Meisels, 2006)

Translating Research Into Public Policy
Three examples:• National Child Traumatic Stress Network (NCTSN): Raising the standard of care (SAMHSA)
• Safe Start Initiative: Creating models of community collaboration (OJJDP)
• Court Team: Judicial system-Early Intervention partnership (OJJDP)











![[Maurice Lieberman] Keyboard Harmony Improvisati(BookFi.org)](https://static.fdocuments.us/doc/165x107/577ccf351a28ab9e788f28df/maurice-lieberman-keyboard-harmony-improvisatibookfiorg.jpg)







