Trauma and Infants - Werry Workforce and Infants.pdf · Bruce Perry, M.D., ... “Babies remember...
40
Trauma and Infants Marion Doherty Koanga Tupu (ADHB) & Chie Yumoto Whakatupu Ora (CMDHB) 1 17/11/2016
Transcript of Trauma and Infants - Werry Workforce and Infants.pdf · Bruce Perry, M.D., ... “Babies remember...

Trauma and Infants
Marion DohertyKoanga Tupu (ADHB)
&
Chie YumotoWhakatupu Ora (CMDHB)
117/11/2016

Outline
Unique aspects of trauma in infancy and young childhood
Development of attachment and its role in managing the impact of trauma
Tips and resources for CAMHS clinicians
217/11/2016
“It is an ultimate irony that at the time when the human is most vulnerable to the effects of trauma – during infancy and childhood – adults generally presume the most resilience.”
Bruce Perry, M.D., Ph.D.
317/11/2016

At what age can children begin to feel fearful?
A) 3 months
C) 9 months
B) 6 months
D) 12 months
17/11/2016 4
At what age can children begin to feel fearful?
A) 3 months
Zero to Three National Parent Survey Report (2016)
17/11/2016 5
At what age can children give an explanation in terms of cause and effect?
A) 18 months
C) 36 months
B) 24 months
D) 48 months
17/11/2016 6

At what age can children give an explanation in terms of cause and effect?
C) 36 months
California Department of Education (2005)
17/11/2016 7

“Babies remember traumatic events in their bodies” – Alicia Lieberman
Babies and toddlers are directly affected by trauma
They are also affected if their main caregiver is suffering consequences of the trauma
817/11/2016

Types of Trauma
Accidents Physical Trauma Child Abuse and Neglect (including Emotional) Exposure to Domestic or Community Violence Natural Disasters Traumatic or Sudden Death in the Family Medical Procedures War, Terrorism, Crime
917/11/2016
Common Reactions in Infants Unusually high levels of distress when separated
from their primary caregiver “Frozen watchfulness”— a ‘shocked look’ Appears to be numb and a bit “cut off” Loss of playful and engaging behaviour Loss of eating skills, poor appetite, low weight Sleep difficulties or nightmares Being more unsettled and more difficult to soothe Slipping back in their physical skills & language Becoming more aggressive
1017/11/2016
Contributing Factors
Single incident or Repetitive? Reminders or not? Any physical injuries? Any secondary stresses? Emotional support before, during or right
after traumatic experience? Quality of the relationship with caregiver prior
to trauma
1117/11/2016

Video clip - Developing Brain
“Toxic Stress Derails Healthy Development”
17/11/2016 12
17/11/2016 13
Cerebral Cortex
Memory Attention
Thinking
Language
PerceptualAwareness
Reasoning

1417/11/2016
Positive Tolerable Toxic
Brainwave (2015)
17/11/2016 15

"There is no such thing as a baby ... if you set out to describe a baby, you will find you are describing a baby and someone. A baby can not exist alone, but is essentially part of a relationship '' (Winnicott, 1947)
17/11/2016 16

Infants experience trauma through relationship
17/11/2016 17

Parent as Emotional Mirror
Mirror neurons – present from birth – parts of our brain that react “as if” we’ve experienced/done something -
Heart racing when watching sport Stomach turning when seeing someone else disgusted Recoiling when someone else hit
Allow us to learn about emotions and ourselves and empathise with others
17/11/2016 18

Mirroring –Reflection versus Distortion
Marked Mirroring – parents using their own subtle facial expressions to mirror the baby and then ‘marks’ this expression with a reassuring expression
No marking – not containing and can be traumatising because it is overwhelming
Incongruent mirroring – baby’s sense of themselves is affected – development of false self
17/11/2016 19

Video clip – Mirroring
17/11/2016 20

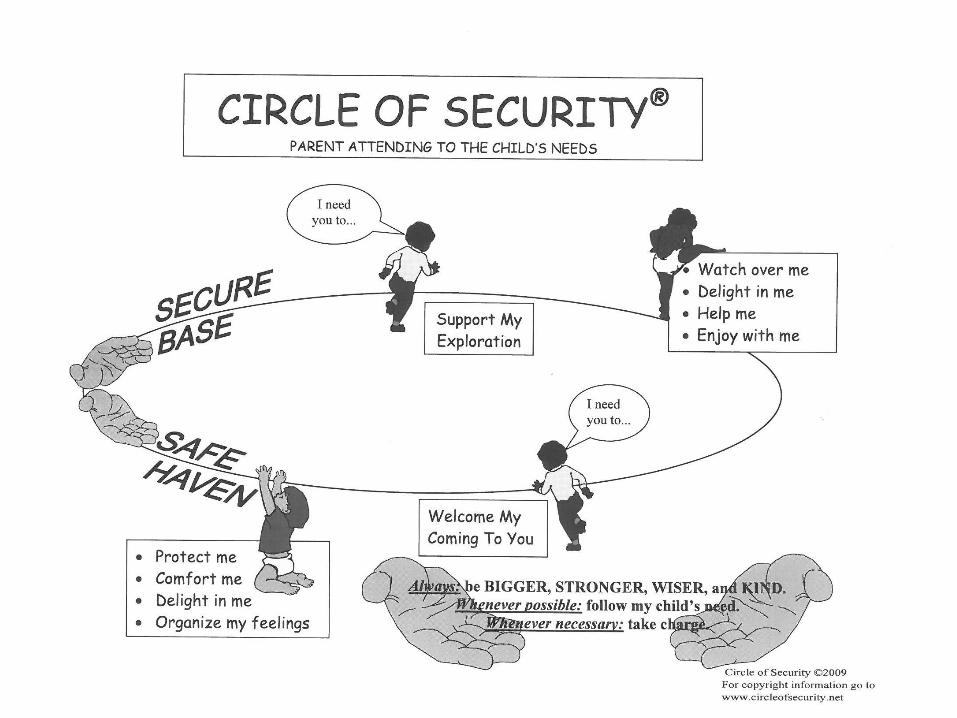
Infant Attachment
• A secure attachment is the most desirable outcome for the infant – the knowledge that their caregiver will consistently respond when they are distressed
• “..what is believed to be essential for mental health is that the infant and young child should experience a warm, intimate and continuous relationship with his mother (or permanent mother substitute) in which both find satisfaction and enjoyment” (Bowlby, 1973)17/11/2016 21
17/11/2016 22
Infants adapting their responses
By the age of one, infants learn to adapt their emotional displays – in response to what is most comfortable for the caregiver
Infants can dial down their distress to stay in relationship with their caregivers
Cortisol and stress are still high despite looking “fine”
Case example - daughter turning away from Mother when distressed
17/11/2016 23
Infants can also increase their displays of distress/neediness in order to stay in relationship with their caregivers.
Parents can cue infants to look after their own emotional needs – not attuned
17/11/2016 24

Disorganised Attachment
Abuse and scary behaviour from a care-giver feels life-threatening for the child. The care-giver should be the source of safety but instead is the source of fear and terror.
The child is stuck in an awful dilemma: her survival instincts tell her to flee to safety (the attachment figure), but safety may be in the very person who is frightening her.
17/11/2016 25
“Disorganized attachment arises from fright without solutions. Parents can frighten their children in different, often unconscious, ways. It might be through abuse or neglect, but it could also be through unresolved trauma and loss in the parent’s own life that leaves him or her feeling afraid, which unintentionally scares the child”. http://www.youngminds.org.uk/17/11/2016 26

Video clip- Dr Dan Siegel
17/11/2016 27

Therapy/Support
Therapeutic assessment – to pull the whole story together and acknowledge loss and pain
Relationship therapy for Mother and child Individual therapy for father Work with couple to support their
relationship
17/11/2016 28

Outcome
Father less stressed and more able to parent “with joy”
Mother able to both take control and soothe child
Parents now looking at their relationship and the future
17/11/2016 29

Tips & Resources
17/11/2016 30

17/11/2016 31
Identifying Trauma
Clinical assessment should review the specifics of the traumatic experiences: Reactions of the child and caregivers Changes in the child’s behaviour Resources in the environment to stablise the child Quality of the child’s primary attachment
relationships Ability of caregivers to facilitate the child’s healthy
development
17/11/2016 32

Instruments for Assessment
Traumatic Stress in Children: Child Behaviour Checklist (CBCL): Aged 1 ½ – 5 PTSD Semi-Structured Interview and Observation
Record: Aged 0 – 4 Traumatic Events Screening Inventory- Parent
Report Revised: Aged 0 – 6
Parenting Stress and Strengths: Parenting Stress Index Life Stressor Checklist- Revised
17/11/2016 33

What can CAMHS clinicians do?
Goal = Help caregivers re-establish security and stability for the child and the family Avoid any unnecessary separations from
important caregivers Maintain the child’s routines and schedules Answer the child’s questions in language they can
understand Learn to recognise and manage the child’s signs of
stress and understand cues for what is going on
17/11/2016 34

What can CAMHS clinicians do?
Expect the child may temporarily regress in their development or become ‘clingy’
Help the child expand their “feelings” vocabulary Avoid exposing the child to reminders of the
trauma, where possible Show love and affection Find ways to have fun and relax together Accept support and take time out to recharge
themselves
17/11/2016 35

Resources for Caregivers
National Child Traumatic Stress Network: http://www.nctsn.org/resources/audiences/paren
ts-caregivers
After the Injury: https://www.aftertheinjury.org/
Center on Social and Emotional Foundations for Early Learning “Family Tools”: http://csefel.vanderbilt.edu/resources/family.html
17/11/2016 36
When to seek more help…
Impact of trauma is preventing development of close relationship between the child and the caregiver
The child continues to slip backwards in development
If the trauma is severe or chronic If the caregiver is emotionally unwell with
stress, grief, anxiety or depression
17/11/2016 37

Self-Care
Take care of yourself!! Get supervision
17/11/2016 38

17/11/2016 39
“Ki te kore nga putake e mākukungia e kore te rakau e tupu”- If the roots of the tree are not watered the tree will never grow

17/11/2016 40