B3. To Drug or Not to Drug: Dementia, Behaviours and Dilemma. Elisabeth Antifeau.
19
Elisabeth Antifeau, RN, MScN, GNC(C) Community Integration Health Services Practice Lead, Complex/Special Populations and Palliative Care/End of Life. Interior Health Nelson, BC
-
Upload
bcpsqc -
Category
Healthcare
-
view
275 -
download
0
Transcript of B3. To Drug or Not to Drug: Dementia, Behaviours and Dilemma. Elisabeth Antifeau.

Elisabeth Antifeau, RN, MScN, GNC(C)
Community Integration Health Services
Practice Lead, Complex/Special Populations
and Palliative Care/End of Life.
Interior HealthNelson, BC

Disclosure - Elisabeth Volunteer Director on the BC Psychogeriatric Association
Board since 2006 – currently holding the Practice Supports Portfolio
June 2014 – Received an honorarium from Medical Pharmacies Group Ltd. to deliver an unrestricted educational event for residential nursing staff on the topic of NON-pharmacological interventions for BPSD.
Within my IH role, I am the representative for Interior Health on various provincial and cross agency working groups addressing dementia, behaviours and system level supports.

Dementia, Behaviours and DilemmasElisabeth
Getting on the same page about dementia, behaviours (BPSD) and dilemmas
How big a problem is it?
Principles of caring for people with BPSD
What can be done? Approaches and tools…
Highlights of the BPSD Algorithm www.bcbpsd.ca
Janice:
Behavioural Support Planning
Clinical example(s)
Questions and Answers – both presentations

Dementia – DSM-V
Mild to Major Neurocognitive Disorder due to:
Alzheimer Disease
Lewy Body Disease
Frontotemporal lobar degeneration
Vascular Disease
Parkinson’s Disease etc.
With/Without Behavioural Disturbance

“Behavioural Disturbance”
A behavioural continuum ranging from mild to severe that includes the following characteristics:
Dangerous
Distressing
Damaging
Disturbing
Persistent

What is BPSD?BPSD = Behavioural and Psychological Symptoms of Dementia are the neuropsychiatric symptoms that arise from advancing dementia:
Symptoms can include:
Behaviours = wandering, verbal and physical aggression, sexually or socially inappropriate, resisting care etc.
Psychiatric = depression, delusions, psychosis, apathy
Symptoms will vary with the type and stage of dementia.
Terminology reflects the lens: paradigm shift is needed
“Challenging”, “Difficult” vs. “Responsive” Behaviours
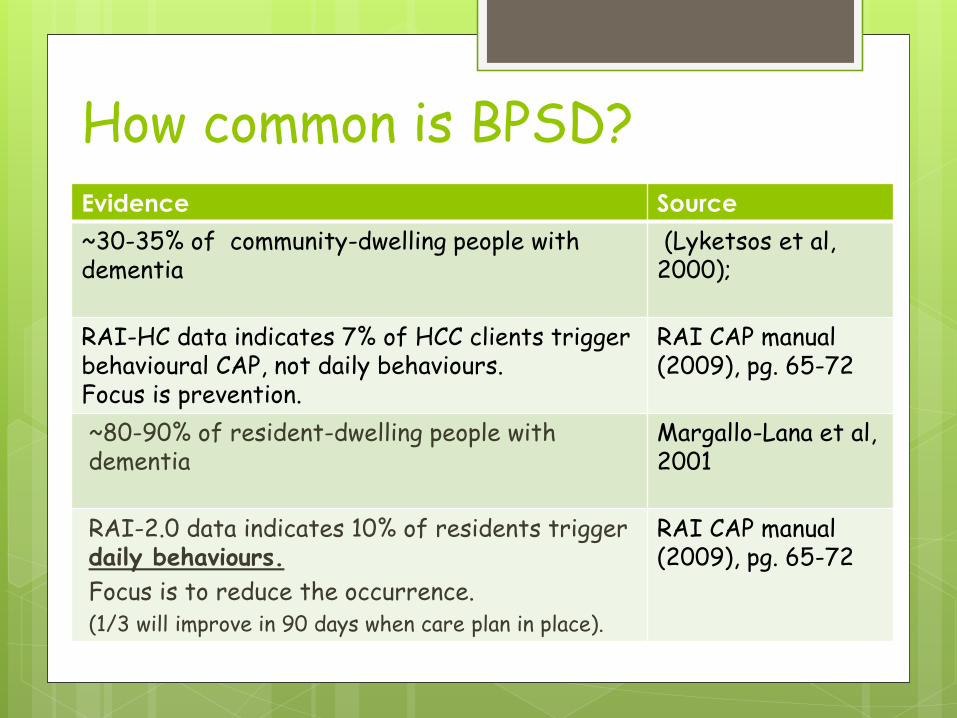
How common is BPSD?Evidence Source
~30-35% of community-dwelling people with dementia
(Lyketsos et al, 2000);
RAI-HC data indicates 7% of HCC clients trigger behavioural CAP, not daily behaviours.Focus is prevention.
RAI CAP manual (2009), pg. 65-72
~80-90% of resident-dwelling people with dementia
Margallo-Lana et al, 2001
RAI-2.0 data indicates 10% of residents trigger daily behaviours.
Focus is to reduce the occurrence. (1/3 will improve in 90 days when care plan in place).
RAI CAP manual (2009), pg. 65-72

Why is BPSD Important? Quality of Life issue
Continuum of Behavioral Escalation/cycling
Resident/Visitor/Staff Safety
Staff continuity/sustainability

Core Behavioral Principles
Behaviours are one of the 4 red flags in dementia care that always needs further assessment: pay attention to changes in behavior, function, thinking
and mood;
ALL Behaviour has meaning – sleuth it out
Presume changes are reversible until proven otherwise
Avoid diagnostic overshadowing

Core Behavioral Principles
Don’t take behaviour personally
Target one behaviour at a time
Target Antecedents<<BEHAVIOUR>>Consequences
Be realistic: success is measured by decreases in intensity, frequency and duration of behaviours, rarely extinguishment.

Behavioural principles – cont’d
Integrated, wholistic, and person-centred approaches are needed**:
Non-pharmacological
Pharmacological
**Not a linear relationship

Tools and ApproachesApproaches
PIECES
Gentle Persuasion Approach (GPA)
Eden Alternative
Others
Tools
BC BPSD Algorithm (2014)
Behavioural Support Plan
Guidelines and Protocols
Never underestimate the therapeutic use of self

BC BPSD Algorithm - History and background
2007-2009 –antipsychotic use in residential care is problematic
2011 – Ministry of Health provincial review = increased use of antipsychotic drugs in res care
2001/02 = was 37%
April 2010 to June 2011 – rose to 50.3%
2012 – Ministry Res Care/BPSD guidelines developed
2013 - Provincial Working Group was struck to achieve provincial consensus on all content within the algorithm.
2014 – electronic version released via the BC Patient Safety and Quality Council website. Purchased domain “BC BPSD”

BC BPSD Algorithm Highlights: The interactive algorithm is compatible
with multiple devices:
http://bcbpsd.ca/

BC BPSD Algorithm Highlights…
PDF vs. JPEG formats Branded vs. No Logo

BC BPSD Algorithm Highlights:
Opening Message
Two Parts
Tool bars:
• Screen Corners
• Screen Bottom
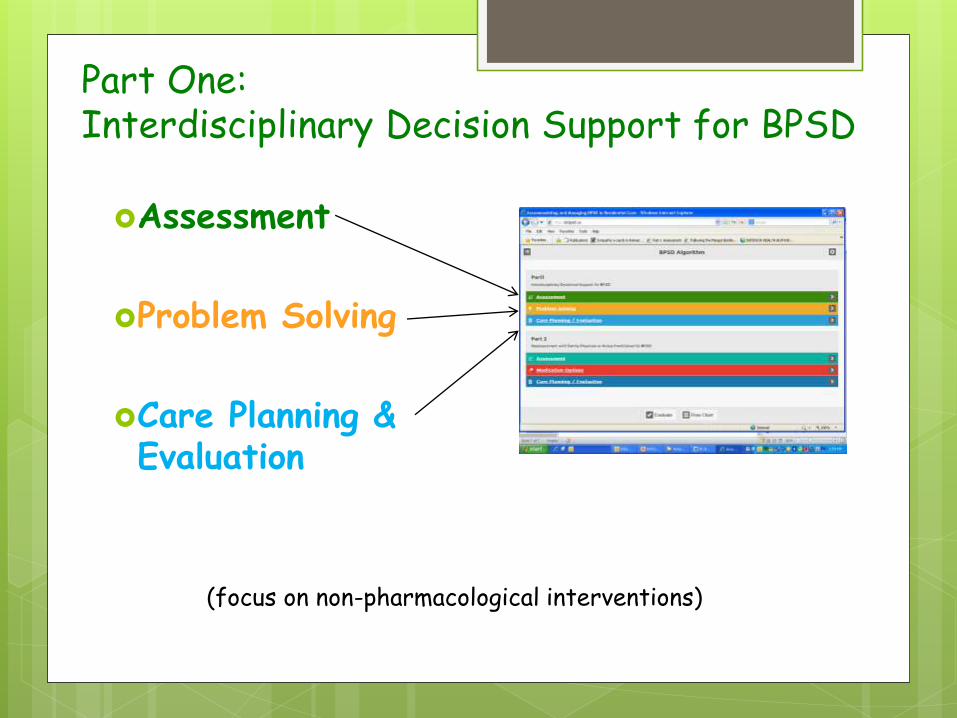
Part One: Interdisciplinary Decision Support for BPSD
Assessment
Problem Solving
Care Planning & Evaluation
(focus on non-pharmacological interventions)

Part Two: Reassessment with GP/NP
Assessment
Medication Options
Care Planning & Evaluation
(focus on layering in appropriate pharmacological interventions)
Summary
Behaviour is…
• Responsive
• Multifactorial
• Complex
• Quintessentially and
uniquely part of
being human
Addressing BPSD skillfully can improve quality of life.