Geriatric Population. The 3 D’s Geriatric Dementia, Delirium & Depression

1
Hospital and Local Health District: Westmead Hospital .Emergency Department (WMH – ED).
Western Sydney Local Health District (WSLHD).
1. Overview of the implementation of Aged Care Emergency (ACE) program
Please provide a concise overview of why you applied for funding to implement the ACE
model.
Westmead Hospital applied for funding to implement the ACE model to integrate and sustain an
enhanced Geriatric Rapid Evaluation and Treatment (GReat) model of care that provides timely,
safe and quality care for Residential Aged Care Facility residents requiring urgent and/or
specialist geriatric care.
How did you assess the need for implementation of the ACE model?
A needs assessment occurred by:
· Reviewing the presentation rates to Westmead Emergency department by residents from Residential Aged Care Facilities.
· Consultation and collaboration with Dr Landau and the Geriatric Rapid Evaluation Assessment Team (GReat) on ways to better integrate their existing model of care with the demands on the Emergency Department.
2. Objectives of the implementation of ACE
Please state the objectives you set out to achieve with implementation of the ACE model, was
there any change to this during the project?
1. To increase the number of RACF’s participating in the GReat service model from 20% (8) to 50% (20) within 6 months of implementation of the enhanced model.
The addition of the ACE phone triage as a single point of access and the implementation of the ACE manual has enhanced the GReat service model by the anticipated 50%. In addition the ACE has coordinated appropriate cases to enhance the GReat rapid response to within the day reducing avoidable presentations.
2. To reduce ED Length of Stay for RACF patients from a median of 6 hours 42 minutes to 4 hours within 12 months of implementation.
The data indicates that the median length of stay in ED for Residents from RACF’s has improved, even across the busy winter period, since the ACE model was implemented. In addition, Westmead Emergency Department implemented the ED Models of Care in April 2013 which has utilises early streaming for all presentations to the Hospital. These models have impacted positively on Westmead’s Emergency Department striving to achieve the NEAT target by reducing the median decision to disposition time from 7:39 hrs to 5:30 hrs.

2
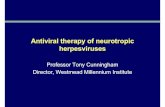
Table 1 Median LOS in ED June to December for residents from RACF’s. Median 7:39 . n= 761. Source: Firstnet business objectives June – December 2012.
Table 2: Median & Average LOS in ED by level of care n=1103. Overall median 5.30 hrs, average 11:46 hrs Source: Firstnet business objectives February – July 2013.
7:27
9:28
7:24
8:018:14
5:32
4:48
0:00
1:12
2:24
3:36
4:48
6:00
7:12
8:24
9:36
10:48
June July August September October November December
Median LOS in EDJune to December 2012
February March April May June July
High Median 7:28 5:16 6:24 4:53 5:05 5:57
High Average 9:22 11:24 7:15 8:44 10:42 14:19
Low Median 4:40 5:00 5:13 4:01 5:35 5:46
Low Average 12:23 12:57 6:34 5:20 5:28 5:55
0:00
2:24
4:48
7:12
9:36
12:00
14:24
16:48
Median & Average LOS in ED by Level of CareFebruary - July 2013

3
3. To establish case management of the acutely unwell elderly patient in the ED through early streaming, early identification of defined Goals of Care and early collaboration with geriatric medicine within 6 months of implementation.
Establishing case management in the ED for acutely unwell elderly patients was enhanced in April 2013, when Westmead Hospital introduced the redesigned “Models of Emergency Care”. Models of Emergency care aim to improve the timeliness, safety and quality of emergency care for all presentations to the emergency department. These models utilise early streaming which has enhanced and integrated with the existing model of care for rapid assessment of Elderly people, Healthcare for Older Persons Earlier (Hope ED).
4. To develop a training and education package for participating GReat RACF staff within 6 months of implementation.
The ACE manual was well received by participating RACF’s within Westmead Hospital catchment
area. Additional support was provided to the interested facilities as face to face educational
training to support the algorithms used in the ACE manual.
Additional educational topics included;
· Cardiac assessment skills in Hypertension, Angina, Cardiac Heart Failure,
· Abdominal assessment skills in pain and the acute abdomen,
· Neurological assessment skill in the use of the Glasgow Come Score, and assessment of
TIA’s, Strokes,
· Wound assessment and management skills,
· Recognition of early signs of systemic inflammatory response/ sepsis.
· Respiratory assessment skills including chest auscultation with respiratory competency
assessment.
3. Scope of the implementation and ACE model used
What were the specifics of the ACE model you implemented in your Hospital?
· Telephone triage and support to staff working in RACF’s to facilitate their decision making and management of their resident’s with non-life threatening acute care needs. The telephone support also facilitated the clinical handover process between the emergency department and the RACF, prior to and post presentation.
· Educational support to enhance the introduction of the ACE manual algorithms.
· Collaborative working relationships with RACF management and clinicians, local GPs, the Wentwest Medicare Local, and other hospital providers.

4
In what ways did you deviate from the documented NSW ACE model and why?
The ACE model implemented at Westmead deviated from the NSW ACE model to enable integration with the GReat service model. The GReat model is based on a Nurse Practitioner role and had existed in the Westmead catchment area visiting high care RACF’s for a year prior to the commencement of the ACE model. It was decided that the ACE CNC’s role would focus on education and triage whilst the Nurse Practitioner’s role was to focus on direct patient care within the RACF. In addition, the ACE CNC monitored the NSW Ambulance Status Board for non-life threatening acute care resident’s referred to Westmead, to improve the outreach service offered by GReat with the aim to reduce avoidable emergency department presentations.
The outcomes involved the interception of 56 referrals to the Booked NSW Ambulance Board. The ACE consult service contributed to 4 bookings remaining in the RACF. The reasons varied from discussion on End of Life issues or follow up with GP review. There were 7 ACE referral s to the GReat NP for rapid same day assessment, of which 3 remained in the facility with the additional 4 referred to the hospital either by the GReat NP, the RACF afterhours or diverted to another hospital within the WSLHD based on triage category.
At times of access block in WMH, the ACE role was used to phone triage the RACF referrals to WMH ED to alternate hospitals across the WSLHD. The total number of diversion was 15.
How did you determine the elements of the model that would suit your Hospital’s
purposes?
Consultation and collaboration by the Emergency Department with the Geriatric department
determined two elements of the NSW ACE model that suited Westmead’s requirements. Firstly,
that the ACE CNC role would implement the ACE manual into the RACF’s whilst addressing
additional educational needs to support the RACF clinicians. Secondly, by using the ACE CNC
as a single point of access, referrals could be centralised, and the GReat Nurse Practitioner and
other models of care could enhance their delivery of timely, safe and quality care to residents in
Residential Care Facilities.
4. Methodology used in the implementation
This section should evaluate the success or otherwise of the methodology used to implement the
model of care. What were the barriers and enablers to project success or otherwise?
Barriers experienced within Westmead Hospital to the implementation of the NSW ACE model
included, standardising addresses through iPm for data collection. Staff shortages in Information
Technology delayed the development of an electronic telephone consultation sheet for ACE
documentation. Integration with the GReat service required a process of negotiation over a period
of time which slowed the ACE implementation.
Barriers experienced with external providers included, delayed engagement by RACF’s to inform
the ACE CNC prior to the referral of a resident to hospital. In addition, at times there was a

5
delayed process of RACF engagement due to internal RACF system issues. GP referrals to
ACE, although many of these were direct to the GReat Nurse Practitioner. The number of
presentations afterhours.
Enablers experienced within Westmead Hospital included the willingness of the Emergency
department to support ACE with data and patient care coordination.
Enablers experienced with external providers included the collaboration with the Wentwest
Medicare Local to address system issues with RACF and GP’s. The willingness of the RACF
management to implement the ACE manual at most target RACF’s within Westmead Hospital’s
catchment area.
What was your communication strategy and how effective was it?
The communication strategy utilised by the ACE role included meetings with external service
providers and within Westmead. These meetings were considered to be an effective
communication strategy to receive feedback and plan to improve the delivery of healthcare. The
ACE role was involved in Bimonthly DON meetings with RACF. This was found to be an effective
strategy to promote the ACE role and manual whilst developing an understanding of system
issues within the Residential care facilities. Monthly meetings with the Wentwest Medicare Local
and NSW Ambulance were effective for strategically planning to engage with facilities about ways
to better manage system issues. Fortnightly meetings with the GReat Nurse Practitioner were
effective at focusing on clinician issues at the point of care. Monthly meetings with the Westmead
sponsorship were effective at promoting the role of ACE to the executive to address system
issues across the WSLHD.
What recommendations would you offer other Hospitals about to commence
implementation of ACE?
In scoping for the implementation of ACE, the following recommendations are made to support
RACF engagement. This includes direct consultation with RACF management regarding the
need for additional support to suit their education needs; the likelihood of RACF clinicians
engaging with a central referral source in the emergency department prior to notifying NSW
Ambulance; the role that the ACE CNC has in improving Clinical handover between the
Emergency department and Residential Aged Care Facilities.
In scoping for the implementation of ACE within your hospital, the following recommendations can
be made; clear role definitions between the Emergency department and the Geriatric departments
can build solid communication, collaboration and develop governance of this patient group;
engaging with information technology prior to the implementation phase so that an electronic
system means that the progress of ACE can be tracked by other clinicians working within the
Hospital.

6
5. Measures of success of the implementation of ACE
Please include data as follows pre and post implementation of ACE (as indicated in the NSW
ACE Model of Care document)
Please include analysis of your data to demonstrate that objectives were met and impact of the
implementation of the ACE model.
The analysis of the following data requires consideration of several factors:
· There are a number of RACF’s inclusive of Nursing Homes/Hostels and independent living units within Westmead Hospital’s catchment area. Some of these RACF’s offer additional support and advice by their Nursing staff to the resident’s in low /Independent living . It was considered that the principles of the ACE model could be used to support and advise nurses working within RACF’s who are accountable to any level of resident.
· Implementation of the ACE manual facilitated closer scrutinising of the data which contributed to the post data being more comprehensive.
· The integration of ACE with the GReat model increased the data scope so all RACF’s presenting to Westmead Emergency Department, between February and July 2013 were included.
· From July 1st 2013, ageing in place could impact on further categorising of RACF residents by levels of care.
· The ACE CNC role commenced on December 17th 2012 for a 12 month period.
Number of ED Presentations from RACF’s.
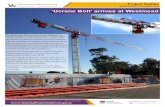
The number of presentations from RACF’s to Westmead Emergency Department during implementation of the ACE model from February to July 2013 n = 1103 ( Table 3). The data collected was compared to the addresses supplied by NSW Ambulance booked transfers from RACF’s to WMH for the financial year 2012 – 2013. The total number of NSW Booked Ambulance transfers to WMH- ED during the financial year was 1808. In addition a review of the RACF address and consultation with the resident or family was used to categorise the presentation into High or Low care. A further breakdown into triage categories according to High or Low care RACF (tables 4,5 & 6) pre and post ACE implementation indicate that generally presenting issues for RACF residents are triaged as category 3 to 5.
On review of the 6 months of data, the overall trend does not indicated a significant change to
presentation rates since the introduction of the ACE model.

7
Table 3: Number of presentations by level of care n=1103 Source: Firstnet business objectives February – July 2013.
93
117
154 149138
146
35
35
51 56
54
75
0
50
100
150
200
250
February March April May June July
Number of Presentations by RACF Level of Care
High Low

8
Table 4: Triage categories for presentations from RACF’s. June to December 2012, n=769. Source: Firstnet business objectives June to December 2012.
Table 5: Low level care presentation by Triage category n=306. Source: Firstnet business objectives February – July 2013.
17%
213%
320%
427%
533%
Triage catgories for presentations from RACF's June- December 2012
2 0 1 0 0 2
6 12 11
19
1314
10
19
26 1421
25
14
8
13 2316
34
0
0
0
0
4
0
0
10
20
30
40
50
60
70
80
February March April May June July
Low Level Care Presentations by Triage Category
Cat 5 Cat 4 Cat 3 Cat 2 Cat 1

9
Table 6: Low level care presentation by Triage category n=797.. Source: Firstnet business objectives February – July 2013.
Hospital LOS and Bed Days
The median Hospital LOS and Bed days can be compared across tables 7 and 8. System
improvements could reduce Hospital LOS for residents from RACF’s inclusive of High and Low
care residents by utilising early discharges from Hope ED with the GReat Nurse Practitioner
follow up in the RACF. A further recommendation is to extend the hours of HOPE ED as table 9
indicates there is a greater number of discharges of this patient cohort from the Emergency
Department compared to HOPE ED. In addition the ACE CNC and the GReat Nurse Practitioner
have worked with RACF’s to promote review in HOPE ED during business hours.
4 3 6 6 105
2621
27 29
33 39
25 36
49 48
46 40
35
50
6654 41 51
2
6
5
10
8
11
0
20
40
60
80
100
120
140
160
180
February March April May June July
High Level Care Presentations by Triage Category
Cat 5 Cat 4 Cat 3 Cat 2 Cat 1

10
Table 7: Median LOS in Westmead Hospital for residents from RACF’s . n=769. Source: Firstnet business objectives June –December 2012.
Table 8: Median & Average LOS in Westmead Hospital by level of care n=1103. Source: Firstnet business objectives February – July 2013.
6
5
4.5
4 4 4 4
0
1
2
3
4
5
6
7
June July August September October November December
Median Hosptial LOS June to December 2012 for patients from RACF's.
February March April May June July
High Median 1.3 2.1 3.9 2.6 2.0 3.1
High Average 4.6 4.5 5.2 4.3 3.8 4.3
Low Median 3.2 1.6 2.5 2.8 3.3 3.2
Low Average 4.4 4.8 4.4 5.9 7.2 5.9
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
Median & Average LOS in Hospital Days by Level of Care

11
Table 9: Comparison of Westmead ED to HOPE ED discharges.
Source: Firstnet business objectives February – July 2013.
Health Outcomes Related Data
The pre and post Health outcomes were compiled from the main diagnoses and indicated trends
in reasons for presentation from RACF’s in the WSLHD to Westmead Hospital. A percentage
involved multiple diagnoses which were not reflected in the trends. The issues identified in the
legend highlight broader system issues; RACF protocols. i.e falls; chronic disease management
by GP’s/ mediation reviews; and quality end of life planning discussions. Highlighting these
health outcomes support the need for additional education by the ACE CNC and coordination of
services involving the GReat Nurse Practitioner.
0
10
20
30
40
50
60
February March April May June July
Comparison of Westmead ED to HOPE ED discharges.
D/C ED HOPE ED Total presentations to HOPE ED

12
Table 10 : Health Outcomes n=769. Pre ACE implementation. Source: Firstnet Business objectives June – December 2012.
Table 11: Health Outcomes n=306. Low/ILU RACF. Source: Firstnet business objectives February – July 2013 and Cerner Geriatric discharge summaries.
12%
4%
4%
2%
11%
3%
1%
1%
62%
Health Outcomes June - December 2012.
Falls
Fracture
CCF/COPD
UTI
URTI/pneumonia
Aspiration pneumonia
Lines
Deceased 48hrs
Other
10%
7%
7%
8%
2%
1%
2%
1%
62%
Health Outcomes February - July 2013Low/ILU Care RACF
Fall
Fracture
CCF/COPD
UTI
URTI/pneumonia
Aspiration pneumonia
Lines
Deceased 48hrs
Other

13
Table 12: Health Outcomes n= 797 High care RACF. Source: Firstnet business objectives February – July 2013 and Cerner Geriatric discharge summaries.
ACE Phone Call Record
The ACE Phone record has been combined with the GReat Nurse Practitioner phone record and can be viewed as the total calls. The total number of calls to the ACE service from February to July 2013 was 33. Whilst some of the calls were deemed to be support calls, 20 remained in the facility, 8 of those calls were referred to the GReat NP for follow up. The other 13 RACF residents presented to WMH, however only 4 residents presented during the time that the ACE nurse was working. Thus it can be difficult to determine if the case management role or the ACE Nurse had a significant impact on the ED LOS. In addition the ACE CNC followed up on discharges from the Emergency department promoting
standards of care and providing further education opportunities. This process was also used to
identify issues that facilitated follow up within the facility by the GReat Nurse Practitioner. There
were 12 referral to the GReat NP post discharge from WMH ED.
10%
7%
3%
4%
8%
6%
4%
4%
54%
Health Outcomes February - July 2013High care RACF
Fall
Fracture
CCF/COPD
UTI
URTI/pneumonia
Aspiration pneumonia
Lines
Deceased 48hrs
Other

14
Table 13 : Phone calls to GREAT/ACE by RACF & ACE to RACF’s. Source: Phone log ACE/GReat.
Table 14: Telephone call outcomes to ACE. February to July 2013. Source: Phone log ACE/GReat.
0
5
10
15
20
25
Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
Phone Calls to GReat/ACE by RACF & From ACE to RACF
GREAT ACE From ACE
0
1
2
3
4
5
6
7
Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
ACE Phone Call Outcomes February to July 2013
Remained in RACF
WMH

15
Rates of re-presentation to the Westmead ED.
Table 15 compares the rates of re-presentation to Westmead ED after discharge from either the
Emergency department or the Geriatric wards. Analysis of this data identifies that the likelihood
of re-representation occurs when a resident is new to the RACF, presents monthly to the
Emergency department and there are issues with indwelling devices. Implementation of a 48hr
follow up criteria within the GReat model could address re-presentation rates.
Table 15: Rates of re-presentation to the same ED within 48hrs. Source: Firstnet Business objectives June – December 2012.
Collaborative meetings
· Bimonthly DON meetings with RACF.
· Monthly meetings with the Wentwest Medicare Local and NSW Ambulance.
· Fortnightly meetings with the GReat Nurse Practitioner.
· Monthly meetings with the Westmead sponsorship.
Adverse outcomes monitoring (IIMS)
The potential for adverse outcomes from involvement by the ACE model were monitored
but none were identified.
0
1
2
3
4
5
6
February March April May June July
Rates of Re-presentation to Westmead ED within 48 HoursFebruary to July 2013
Low Ward Low ED High Ward High ED

16
Compliments and complaints
There were many compliments related directly to the ACE Manual being a useful tool that
reflected what some RACF’s in the WSLHD had wanted to develop within their
organisation. Compliments were also directed toward the telephone support offered by
the ACE CNC to the clinicians.
Complaints were direct to the ACE CNC and focused on communication issues between
the RACF and Hospital.
6. Discussion
Was the implementation of ACE successful, why or why not? What were the lessons learnt during
this implementation? What impact has this model had on management patients from Residential
Aged Care Facilities? What would you do differently next time and why? What strategies did you
put in place to ensure sustainability of ACE?
The main issue that has impacted on the success of the ACE Model is that the majority of RACF
presentation occurred after hours, tables 16 and 17. Afterhours included 16:30 to 08:00,
Monday to Friday and on weekends. Westmead Hospital does not have ASET nurse
representation in the Emergency department or HOPE ED. In addition the HOPE ED was open
only from 8:00 till 16:30. Many of the RACF’s had suggested an Afterhours service which at the
time of implementation the ACE service could not provide. As a result of the data collection
supplied by ACE, times for HOPE ED will be extended to 20:00. Afterhours RACF presentations
to Westmead’s emergency department are streamed within the Emergency department. The
introduction of the ED Models of Care has decreased the decision disposition from a median of
7:39 to 5:30 hours.
The implementation of the ACE manual was well received by the engaged RACF’s. Verbal
feedback, to the ACE CNC, on the phone support service included comments like, “it is good to
have a link to the hospital,” “it’s valuable to get a second opinion”. The education sessions were
acknowledged as informative and interesting.
The ACE implementation of a phone triage system dependent on the RACF clinicians phoning
prior to referral to hospital was not predominantly successful. It was deemed appropriate by the
Westmead Executive to liaise with the RACF after a resident was referred to the NSW Ambulance
Booking system. This strategy at times facilitated the engagement of the GReat Nurse
Practitioner to review the resident in the facility. The positive outcomes achieved suggest that
this strategy could be developed to sustain the rapid response time of the GReat model.
In contrast to the GReat Model which focuses on the expert nurse model, implementation of the
ACE model focused on clinician empowerment within the RACF by education and support.
Integrating the two models provided lessons in adopting a systems approach across the
Emergency department and Aged Care Services.

17
Table 16: Total presentations with % AfterHours by level of care. Source: Firstnet Business objectives June – December 2012.
Table 17: Total presentations After Hours with % on Weekend. Source: Firstnet Business objectives June – December 2012.
93 39 51 56 54 75
93
117
154148 138
146
88.2%
41.0%
45.1%
37.5%
42.6%
38.7%
66.7%
52.1%
40.3%
50.0%
54.3%
45.2%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
0
50
100
150
200
250
February March April May June July
Total Presentations with % After Hours by Level of Care
Total Low Total High % AHRS Low % AHRS High
82
16
23 21 23
29
62
61
62 74 75
66
8.5%
50.0%
60.9%
47.6%
60.9%
48.3%
59.4%
63.9%
56.5%
47.3%
62.7%
50.0%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
0
20
40
60
80
100
120
140
160
February March April May June July
Total Presentations After Hours with % on Weekend
AHRS Low AHRS High %WEND Low % WEND High

18
7. Conclusion
Where to from here? Please include plans for further evaluation of the impact of ACE on your Hospital and sustainability of this model in your Local Health District..
The ACE model has collaborated closely with the GReat model, NSW Ambulance service and the Medicare Local. The sustainability of the ACE Model could benefit these other service providers to coordinate resources within the WSLHD.
Collaboration with the GReat model has identified the need to review the processes of it’s existing model. This includes enhancing the rapid evaluation process from over a day to within a day, by developing the ACE role to receive and coordinate referrals. This would maximise the GReat Nurse Practitioner’s time in resident review. .During the ACE project, the ACE CNC coordinated 7 referrals from the NSW booked ambulance board to involve the GReat NP in same day rapid assessment. This prevented 3 Hospital admissions and could be developed further by combining the Nurse Practitioner and NSW ambulance in an innovative model that assesses residents within the RACF prior to transfer. To address the high rate of presentations to the Emergency department on the weekend, additional support could be provided by increasing the availability of the GReat Nurse Practitioner to a weekend day.
To address the high rate of presentations to the Emergency department on the weekend, additional support could be provided by increasing the availability of the GReat Nurse Practitioner to a weekend day.
A preliminary comparative review was undertaken of NSW Ambulance transfers to Westmead and Blacktown Hospitals from RACF’s within Westmead and Blacktown’s catchment area for the Financial year 2012/2013. The data indicated that there are 1808 transfers to Westmead Hospital and 762 to Blacktown Hospital. To address this issue, a systems review of NSW Ambulance transfers across WSLHD could benefit identifying health outcomes where early triaging of RACF residents to Hospitals within the WSLHD could expedite treatment. The PACU system which exists in NSLHD is an example of a successful model.

19
Table 18: NSW Ambulance booked transfers to WMH ED from RACF for financial year 2012/2013. Source NSW Ambulance data.
A preliminary comparative review was undertaken of NSW Ambulance transfers to Westmead and Blacktown Hospitals from RACF’s within Westmead and Blacktown’s catchment area for the Financial year 2012/2013. The data indicated that there are 1808 transfers to Westmead Hospital and 762 to Blacktown Hospital. To address this issue, a systems review of NSW Ambulance transfers across WSLHD could benefit identifying health outcomes where early triaging of RACF residents to Hospitals within the WSLHD could expedite treatment. The Patient Access and Transport Unit (PATU) model of care which exists in Northern Sydney Local Health District (NSLHD) is an example of a successful model.
The ACE CNC collaboration with the Wentwest Medicare local has contributed to their develop-
ment of Telehealth conferencing. In addition, Health pathways, could be developed to ensure
that trends in health outcomes can be developed to guide GP’s in managing the care of RACF
residents.
0
200
400
600
800
1000
1200
1400
1600
1800
WMH BTH
NSW Ambulance RACF presentations for financial year 2012/2013

20
Joanne Edwards
Director of Nursing & Midwifery
Westmead Hospital
Signature: ____________________________
Date: _______________________________
Richard Chrystal
Executive Director of Nursing
Western Sydney Local Health District
Signature: ____________________________
Date: _______________________________
Shaun Drummond
Executive Director Operations
Westmead Hospital
Signature: ____________________________
Date: _______________________________