The Metabolic Syndrome in American Indians: The Strong Heart Study
5
283 MS in american indians JCMS fall 2007 S ince 1988, when Reaven 1 defined the cluster of factors (dyslipidemia, hypertension, and hyperglycemia) that are frequently observed in individuals who develop diabetes and cardiovas- cular disease (CVD), syndrome X, the concept of a constellation of cardiomet- abolic risk factors, has received much attention. 2 Over time, these factors have been further studied and refined and are now often referred to as insulin resistance syndrome or the metabolic syndrome (MS). 3 Although the under- lying cause of MS is not entirely clear, it is thought that MS results from central obesity and insulin resistance (IR). 2 IR is characterized by a diminished response to the biologic effect of insulin and is associated with obesity with a predominantly abdominal distribution of fat, elevated blood pressure (BP) and triglyceride levels, low high-density lipoprotein cholesterol (HDL-C), small low-density lipoprotein cholesterol par- ticle size, and elevations in inflam- matory cytokines. 4 IR has long been known to be a predictor of type 2 diabetes in many populations, includ- ing American Indians (AIs), 5 the group with the highest rates of diabetes in the United States. 6 A high proportion of nondiabetic AIs have IR, and IR is a strong determinant of diabetes in AIs. 5 Diabetes and many aspects of MS, including body fat distribution, high concentrations of plasma insulin, and low concentrations of HDL-C have all been significantly and independently related to increased coronary heart dis- ease (CHD) risk in AIs. 7 CHD rates in AIs exceed rates in other US popula- tions and may result more often in a fatal outcome. 8 us, it is important to identify MS in AIs and treat the factors that comprise it. Such an approach may result in reduced risk of both diabetes and CHD. Definitions of MS Since the syndrome was first postulated, multiple definitions have been promoted by various public health and professional organizations. Although these definitions share many common features, they differ in certain aspects. e World Health Organization (WHO) and International Diabetes Foundation (IDF) definitions each identify a main factor, high insulin and/or fasting glucose levels and presence of central obesity, respectively, that must be present and is associated with other risk factors, whereas the ird Report of the Adult Treatment Panel’s (ATP III’s) definition is based on a combination of factors 9–11 (Table I). e criterion for waist circumference in the IDF defini- tion differs by ethnicity, being lower for Asian populations. No specific criteria for waist circumference have been pro- posed for AIs. Central obesity has been shown to be predictive of type 2 diabetes in Pima Indians after adjusting for percentage of body fat and IR, but not when acute insulin response is also considered. e utility of IR in predicting diabetes in AIs remains strong, however, even after adjusting for central obesity and acute insulin response. 5 In addition, the inter- action between IR and central obesity changes when analyzed in relation to the magnitude of left ventricular mass, a potent marker of preclinical CVD, 12 and a predictor of CVD morbidity and mortality. 13 When added to a prediction model for magnitude of left ventricular mass, IR (assessed by the homeosta- sis model assessment [HOMA] index) Although the underlying cause of the metabolic syndrome (MS) is not entirely clear, it is thought that MS results from central obesity and insulin resistance (IR). IR has long been known to be a predictor of type 2 diabetes in many popula- tions, including American Indians, the group with a rising prevalence of obesity and the highest rate of diabetes in the United States. In addition to being a predictor of diabetes, MS has now been shown to be associated with higher risk of cardio- vascular disease, independent of diabetes, in American Indians as well as in other ethnic groups. Furthermore, MS may carry a risk beyond that of single risk factors. Identifying MS in American Indians and treating the factors that comprise it may reduce risk of both diabetes and cardiovascular disease in this population. (JCMS. 2007;2:283–287) © 2007 Le Jacq Marie Russell, MD; 1 Giovanni de Simone, MD; 2 Helaine E. Resnick, MPH, PhD; 3 Barbara V. Howard, PhD 4 From Phoenix Indian Medical Center, Phoenix, AZ; 1 the Department of Clinical and Experimental Medicine, Federico II University Hospital, Naples, Italy; 2 the Institute for the Future of Aging Services of the American Association of Homes and Services for the Aging, Washington, DC; 3 and MedStar Research Institute, Hyattsville, MD 4 Address for correspondence: Barbara V. Howard, PhD, MedStar Research Institute; Professor of Medicine, Georgetown University; 6495 New Hampshire Avenue, Suite 201, Hyattsville, MD 20783 E-mail: [email protected] REVIEW PAPER e Metabolic Syndrome in American Indians: e Strong Heart Study www.lejacq.com id: 7457 The Journal of Cardiometabolic Syndrome (ISSN 1524-6175) is published quarterly (March, June, Sept., Dec.) by Le Jacq, a Blackwell Publishing imprint, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Copyright © 2007 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ®
-
Upload
marie-russell -
Category
Documents
-
view
214 -
download
0
Transcript of The Metabolic Syndrome in American Indians: The Strong Heart Study

283MS in american indians JCMS fall 2007
Since 1988, when Reaven1 defined the cluster of factors (dyslipidemia,
hypertension, and hyperglycemia) that are frequently observed in individuals who develop diabetes and cardiovas-cular disease (CVD), syndrome X, the concept of a constellation of cardiomet-abolic risk factors, has received much attention.2 Over time, these factors have been further studied and refined and are now often referred to as insulin resistance syndrome or the metabolic syndrome (MS).3 Although the under-lying cause of MS is not entirely clear, it is thought that MS results from central obesity and insulin resistance (IR).2
IR is characterized by a diminished response to the biologic effect of insulin and is associated with obesity with a predominantly abdominal distribution of fat, elevated blood pressure (BP) and triglyceride levels, low high-density lipoprotein cholesterol (HDL-C), small low-density lipoprotein cholesterol par-ticle size, and elevations in inflam-matory cytokines.4 IR has long been known to be a predictor of type 2 diabetes in many populations, includ-ing American Indians (AIs),5 the group with the highest rates of diabetes in the United States.6 A high proportion of nondiabetic AIs have IR, and IR is a strong determinant of diabetes in AIs.5 Diabetes and many aspects of MS, including body fat distribution, high concentrations of plasma insulin, and low concentrations of HDL-C have all been significantly and independently related to increased coronary heart dis-ease (CHD) risk in AIs.7 CHD rates in AIs exceed rates in other US popula-tions and may result more often in a fatal outcome.8 Thus, it is important to identify MS in AIs and treat the factors that comprise it. Such an approach may result in reduced risk of both diabetes and CHD.
Definitions of MSSince the syndrome was first postulated, multiple definitions have been promoted by various public health and professional organizations. Although these definitions share many common features, they differ in certain aspects. The World Health Organization (WHO) and International Diabetes Foundation (IDF) definitions each identify a main factor, high insulin and/or fasting glucose levels and presence of central obesity, respectively, that must be present and is associated with other risk factors, whereas the Third Report of the Adult Treatment Panel’s (ATP III’s) definition is based on a combination of factors9–11 (Table I). The criterion for waist circumference in the IDF defini-tion differs by ethnicity, being lower for Asian populations. No specific criteria
for waist circumference have been pro-posed for AIs.
Central obesity has been shown to be predictive of type 2 diabetes in Pima Indians after adjusting for percentage of body fat and IR, but not when acute insulin response is also considered. The utility of IR in predicting diabetes in AIs remains strong, however, even after adjusting for central obesity and acute insulin response.5 In addition, the inter-action between IR and central obesity changes when analyzed in relation to the magnitude of left ventricular mass, a potent marker of preclinical CVD,12
and a predictor of CVD morbidity and mortality.13 When added to a prediction model for magnitude of left ventricular mass, IR (assessed by the homeosta-sis model assessment [HOMA] index)
Although the underlying cause of the metabolic syndrome (MS) is not entirely clear, it is thought that MS results from central obesity and insulin resistance (IR). IR has long been known to be a predictor of type 2 diabetes in many popula-tions, including American Indians, the group with a rising prevalence of obesity and the highest rate of diabetes in the United States. In addition to being a predictor of diabetes, MS has now been shown to be associated with higher risk of cardio-vascular disease, independent of diabetes, in American Indians as well as in other ethnic groups. Furthermore, MS may carry a risk beyond that of single risk factors. Identifying MS in American Indians and treating the factors that comprise it may reduce risk of both diabetes and cardiovascular disease in this population. (JCMS. 2007;2:283–287) ©2007 Le Jacq
Marie Russell, MD;1 Giovanni de Simone, MD;2 Helaine E. Resnick, MPH, PhD;3 Barbara V. Howard, PhD4
From Phoenix Indian Medical Center, Phoenix, AZ;1 the Department of Clinical and Experimental Medicine, Federico II University Hospital, Naples, Italy;2 the Institute for the Future of Aging Services of the American Association of Homes and Services for the Aging, Washington, DC;3 and MedStar Research Institute, Hyattsville, MD4
Address for correspondence: Barbara V. Howard, PhD, MedStar Research Institute; Professor of Medicine, Georgetown University; 6495 New Hampshire Avenue, Suite 201, Hyattsville, MD 20783 E-mail: [email protected]
REVIEW PAPER
The Metabolic Syndrome in American Indians: The Strong Heart Study
www.lejacq.com id: 7457
The Journal of Cardiometabolic Syndrome (ISSN 1524-6175) is published quarterly (March, June, Sept., Dec.) by Le Jacq, a Blackwell Publishing imprint, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Copyright ©2007 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511.
®

MS in american indians JCMS fall 2007284
does not have an impact independent of waist circumference, although it remains an independent correlate of a measure of arterial stiffness.14
Prevalence of MS in AIsPrevalence rates of MS differ according to the definition of MS used and the popula-tion under study. In AIs, MS prevalence varies substantially (Table II)10 by defini-tion but is high by all criteria, ranging from 44% to 59% in men and 53% to 73% in women, aged 45 to 74 years. Among AIs, the WHO definition yields similar prevalence rates among men and women, because it is not based on sex-spe-cific values for the main criterion, whereas the ATP III and IDF definitions yield higher prevalence rates in women, because one of the most frequently occurring components (and the main criterion in the IDF definition) is sex-specific, with sub-stantially lower cutoff points for women.
The prevalence rates of individu-al MS components, such as BP and
albuminuria, also vary by definition. AIs have a much higher prevalence of MS than the general US popula-tion sampled in the National Health and Nutrition Examination Survey (NHANES).15 Among 8608 partici-pants older than 20 years in the third NHANES, the age-adjusted prevalence rate for MS was 23.9% using the ATP III definition and 25.1% using the WHO definition.
MS as a Predictor of DiabetesDiabetes is a major public health issue in AI communities. Fifteen percent of AIs have diabetes, compared with 8.1% of US non-Hispanic whites.9 MS is a strong predictor of type 2 diabetes in AIs. In the Strong Heart Study (SHS),4 the largest ongoing study of CVD in AIs, 35% of the nondiabetic participants aged 45 to 74 years had MS at baseline. After nearly 8 years, 25% of those who had MS at baseline had developed type 2 diabetes, with a relative risk for CVD
of about 2. This increase in relative risk associated with MS, however, seems less than that seen in the San Antonio Heart Study (relative risk = 6)16 and in the fourth Framingham cohort (relative risk = 7).17 Also important, among AIs there is a clear link between incident arterial hypertension and development of diabetes, as well as prevalence and worsening of central fat distribution, which suggests that early intervention on metabolic risk factors may also help prevent hypertension.18
MS as a Predictor of CVDIn an early analysis of the SHS cohort, at 4.2 years of follow-up, no signifi-cant association was found between MS and incidence of coronary heart disease.4 A subsequent analysis, how-ever, with a follow-up of >8 years, revealed significantly increased risk for combined fatal and nonfatal cardiovas-cular events (including coronary heart disease, stroke, and congestive heart
Table I. Definitions of the Metabolic Syndrome
FactorWHO (Main Criterion +2
Factors)ATP III (Any Combination
of 3 Factors)IDF (Main Criterion +2
Factors)Body mass index >30 kg/m2 or waist/hip >0.9/0.85 — —Abdominal obesity, M/F >102/88 cm waist >94/80 cmTriglycerides ≥150 mg/L ≥150 mg/dL ≥150 mg/dLHigh-density lipoprotein
cholesterol, M/F<35/39 mg/L <40/50 mg/dL <40/50 mg/dL
Blood pressure Hypertension ≥130/≥85 mm Hg Hypertension or >130/85 mm HgHOMA >4.3 or — —Type 2 diabetes present or
≥110 mg/dL— present or
>100 mg/dLFasting glucose ≥110 mg/dLFasting insulin — —Urinary albumin excretion ≥20 mg/min or ≥30 mg/g creatinine — —Abbreviations: ATP III, Third Report of the Adult Treatment Panel; HOMA, homeostasis model assessment; IDF, International Diabetes Foundation; M/F, male/female; WHO, World Health Organization. Reprinted from de Simone et al.21
Table II. Prevalence of MS in AIs, per WHO, ATP III, and IDF Definitions of MS: Blood Pressure and Urinary Albumin/Creatinine Ratio Prevalence of
Metabolic Syndrome SBP, mm Hg DBP, mm HgLog10 of Urinary Albumin/
Creatinine RatioMen, % Women, % No MS MS No MS MS No MS MS
WHO 48 53 122±16 133±20 75±9 79±10 0.80±0.59 1.57±0.98ATP III 44 63 121±17 132±20 75±9 78±10 0.91±0.73 1.42±0.96IDF 59 73 120±16 131±19 74±9 78±10 0.92±0.75 1.33±0.93Abbreviations: AIs, American Indians; ATP III, Third Report of the Adult Treatment Panel; DBP, diastolic blood pressure; IDF, International Diabetes Federation; MS, metabolic syndrome; SBP, systolic blood pressure; WHO, World Health Organization. Reprinted from de Simone et al.21
The Journal of Cardiometabolic Syndrome (ISSN 1524-6175) is published quarterly (March, June, Sept., Dec.) by Le Jacq, a Blackwell Publishing imprint, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Copyright ©2007 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511.
®

285MS in american indians JCMS fall 2007
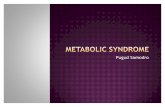
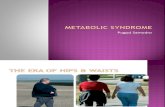
failure) and cardiovascular mortality in both nondiabetic as well as diabetic participants.10 In this last analysis, par-ticipants without diabetes, but with MS as defined by ATP III criteria, had a 40% increased cardiovascular risk (Figure), similar to participants with both diabetes and MS. Using WHO criteria for MS slightly reduced the haz-ard ratio (HR) observed in nondiabetic participants, but amplified the HR of participants with both diabetes and MS. IDF criteria yielded lower HRs that were not statistically significant in nondiabetic participants.
Thus, MS is associated with CVD risk in AIs, but the CVD risk may be lower than that seen in US whites. In white patients in the NHANES cohort who had MS but no prevalent CVD, relative risk for CHD mortality was 2.19 In the Framingham cohort, relative risk for CVD in men and women with MS but without diabetes or prevalent CVD at baseline was 2.9 and 2.25, respec-tively.17,20 However, this difference may be because of variations in the defini-tion of CVD and covariates used in the respective analyses.
Treating MS in AIsDue to the increased risk of CVD asso-ciated with MS in both diabetic and nondiabetic AIs, it is important that
the syndrome is recognized and pro-grams of primary prevention initiated. In April 2005, the Indian Health Service (IHS) published guidelines for the care of adults with prediabetes or MS to assist health care providers in making consistent, quality care available. These guidelines recommend using the ATP III criteria for diagnosing MS. According to the current findings, this suggestion is wise because, although not intended for diabetic individuals, ATP III criteria showed similar prognostic value in dia-betic or nondiabetic SHS participants.21
Treatment should be targeted at each component of MS that is present. Primary goals of treatment are reduction of CVD risk and prevention of type 2 diabetes. A multidisciplinary approach is recommended, with an emphasis on community-based and individual sup-port. The Diabetes Prevention Program (DPP)22 demonstrated that therapeutic lifestyle changes significantly reduce the risk of developing type 2 diabetes. Thus, favorable changes in diet and increased activity levels are emphasized as corner-stones of behavioral interventions. The IHS guidelines support prevention pro-grams that emphasize goal setting, edu-cation and skills development, physical activity, behavior change, and use of community resources. Suggested life-style changes include moderate weight
loss (ie, a 7%–10% reduction in start-ing weight over a 6-month period).
Diet. Balanced intake of nutrients is needed to achieve and maintain weight loss and prevent chronic disease, including MS, type 2 diabetes, and CVD.23 Less than half of the participants in the Strong Heart Dietary Study24 met dietary guidelines for reduction of chronic disease, which include total fat intake of ≤30% of total energy, saturated fat intake of ≤7% of total energy, cholesterol intake of ≤300 mg/d, sodium intake of ≤2400 mg/d, and fiber intake of ≥20 g/d. Among AIs, dietary fat intake is higher than the recommended daily allowance (RDA) of 30% of total caloric intake, ranging from 31% to 47%.25 Nutrient intake also differs in AIs by geographic area and sex.24 The Navajo Health and Nutrition Survey26 revealed that fruits and vegetables were consumed less than once per day per person, with food items such as frybread, mutton, bacon, sausage, soft drinks, coffee, and tea providing 41% of the energy and 15% to 46% of macronutrients. The low percentage of AIs who met dietary guidelines in this study was attributed to cost, availability, and shelf-life of specific food products. Dietary recommendations must consider an individual’s readiness to change and cultural background.
Figure. The metabolic syndrome as a predictor of cardiovascular (CV) disease, Third Report of the Adult Treatment Panel (ATP III) criteria. HR indicates hazard ratio. Reprinted from de Simone et al.21
The Journal of Cardiometabolic Syndrome (ISSN 1524-6175) is published quarterly (March, June, Sept., Dec.) by Le Jacq, a Blackwell Publishing imprint, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Copyright ©2007 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511.
®

MS in american indians JCMS fall 2007286
Key recommendations from Dietary Guidelines 2005 and the American Heart Association to reduce risk of MS are listed in Table III.23,27
Individuals should reduce caloric intake and modify fat intake by engag-ing in behaviors, such as eating smaller portions, increasing intake of fruits and vegetables, consuming white-meat poultry, consuming fish that is high in omega-3 fatty acids, decreasing alcohol consumption to no more than 1 drink per day for women and 3 drinks per day for men, and choosing water and diet soda instead of juices and non-diet soda. Tribal governments and tribal communities should engage in innova-tive programs and foster partnerships to increase access to healthier foods. Public health promotion should focus on the relationship between chronic disease and unhealthy eating behaviors and encourage healthy eating behaviors in the reservation-based schools, health clinics, and facilities for the elderly.
Physical Activity. Regular physical activity decreases the risk for CVD and the components of MS, including prediabetes, diabetes, hypertension, and obesity.28 This may be particularly
true in AI communities. Increased activity levels have been shown to be inversely related to MS among AI women.29 Total physical activity level is strongly related to increased high-density lipoprotein cholesterol in AIs.30 Unfortunately, according to the National Health Interview Survey, 1999–2003,31 50% of AIs indicated that they never participate in any leisure time physical activity. A comparison of survey results from baseline examination for Healthy People 2000 to baseline results for Healthy People 2010 indicates that the number of AIs never engaging in physical activity has increased from 1991 to 1997.32 The SHS has reported that at the baseline examination of participants aged 45 to 74 years, conducted from July 1989 through January 1992, 53%, 32%, and 32% of men from Arizona, Oklahoma, and North and South Dakota, respectively, reported participating in no leisure physical activity over the past week. Similarly, 60%, 42%, and 40% of the women from Arizona, Oklahoma, and North and South Dakota, respectively, reported no leisure time activity in the past week.30 Barriers to physical exercise on AI reservations include lack
of safe walking trails, community centers, gymnasiums, and child care.33 The IHS guidelines for exercise mirror those of the Diabetes Prevention Program, with a goal of 150 minutes of exercise per week. They recommend using the Frequency, Intensity, Time, Type (FITT) principle to develop an appropriate exercise program (Table IV).34
Other Interventions. Pharmacotherapy is indicated to decrease BP and lipid and glucose levels when lifestyle changes are not adequate to correct them. BP must be aggressively treated when 2 other risk factors are present, or if diabetes is present, to reduce the risk of CVD. Individuals should also undergo screening for depression, which is a barrier against weight loss, and referral to a behavioral health specialist as appropriate. Tobacco use should be assessed and cessation counseling and/or intervention offered, as appropriate.
ConclusionsMS prevalence rates among AIs are alarming. MS has been shown to be a risk factor for CVD, independent of diabetes, and must be aggressively diagnosed and treated. The IHS, as the predominant provider of health care to AIs, has recognized this trend and has published guidelines for the care of adults with prediabetes or MS.29
The cornerstones of treatment for MS lie in dietary and physical activ-ity interventions. Interventions such as these can be challenging in the AI population because of high cost and lack of access to healthy foods and safe places to exercise.
Acknowledgments and disclosures: This study was supported by the National Heart, Lung, and Blood Institute. The authors acknowledge the assistance and cooperation of the Indian communities, without whose sufficient support this study would not have been possible. The views expressed in this paper are those of the authors and do not necessarily reflect those of the Indian Health Service. We thank Rachel Schaperow, MedStar Research Institute, Hyattsville, MD, for editing the manuscript.
Table III. Recommendations to Reduce Risk of the Metabolic Syndrome (MS)Recommendation MS Factor Affected
Total calories Balanced to achieve and maintain weight loss
Abdominal obesity
Saturated fat <7% Blood pressureTotal fat 25%–35% of daily caloric intake Triglyceride levelFiber 20–30 g/d Fasting glucose levelCholesterol <300 mg/d High-density lipopro-
tein levelTriglyceride level
Carbohydrates 50–60 total calories Triglyceride levelFasting glucose level
Sodium <2300 mg/d Blood pressureOmega-3 fatty acids Consume fish 2 times per wk and oils
and foods rich in a-linolenic acidTriglyceride level
Table IV. Frequency, Intensity, Time, Type (FITT) Guidelines for Aerobic ExerciseBeginning Goal
Frequency 3–5 d/wk 5–7 d/wkIntensity Low-moderate ModerateTime 30 min intermittent or continuous, as tolerated 30–60 min, continuousType: Aerobic exercise includes walking, bicycling, swimming, and cross-country skiing.
The Journal of Cardiometabolic Syndrome (ISSN 1524-6175) is published quarterly (March, June, Sept., Dec.) by Le Jacq, a Blackwell Publishing imprint, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Copyright ©2007 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511.
®

287MS in american indians JCMS fall 2007
RefeRences 1 Reaven GM. Banting Lecture 1988. Role of
insulin resistance in human disease. Diabetes. 1988;37:1595–1607.
2 Kaplan NM. The deadly quartet. Upper-body obesity, glucose intolerance, hypertriglyceri-demia, and hypertension. Arch Intern Med. 1989;149:1514–1520.
3 Bjorntorp P. Metabolic implications of body fat distribution. Diabetes Care. 1991; 14:1132–1143.
4 Resnick HE, Jones K, Ruotolo G, et al. Insulin resistance, the metabolic syndrome, and risk of incident cardiovascular disease in non-diabetic American Indians: The Strong Heart Study. Diabetes Care. 2003;26:861–867.
5 Lillioja S, Mott DM, Spraul M, et al. Insulin resistance and insulin secretory dysfunction as precursors of non-insulin dependent diabetes mellitus: prospective studies of Pima Indians. N Engl J Med. 1993;329:1988–1992.
6 Lee ET, Howard BV, Savage PJ, et al. Diabetes and impaired glucose tolerance in three American Indian populations aged 45–74 years. The Strong Heart Study. Diabetes Care. 1995;18:599–610.
7 Howard BV, Lee ET, Cowan LD, et al. Coronary heart disease prevalence and its relation to risk factors in American Indians: The Strong Heart Study. Am J Epidemiol. 1995;142:254–268.
8 Howard BV, Lee ET, Cowan LD, et al. Rising tide of cardiovascular disease in American Indians: The Strong Heart Study. Circulation. 1999;99:2389–2395.
9 World Health Organization. Definition of metabolic syndrome in definition, diagnosis and classification of diabetes and its complica-tions. Report of a WHO consultation. Part 1: Diagnosis and classification of diabetes mel-litus. WHO/NCD/NCS/99.2. Geneva, Switzerland: World Health Organization, Department of Noncommunicable Disease Surveillance; 1999.
10 Alberti G. Introduction to the metabolic syn-drome. Eur Heart J Suppl. 2005;7:3–5.
11 Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–3421.
12 Devereux RB, Alderman MH. Role of
preclinical cardiovascular disease in the evo-lution from risk factor exposure to devel-opment of morbid events. Circulation. 1993;88:1444–1455.
13 Vakili BA, Okin PM, Devereux RB. Prognostic implications of left ventricular hypertrophy. Am Heart J. 2001;141:334–341.
14 de Simone G, Devereux RB, Palmieri V, et al. Relation of insulin resistance to markers of preclinical cardiovascular disease: the Strong Heart Study. Nutr Metab Cardiovasc Dis. 2003;13:140–147.
15 Ford ES, Giles WH. A comparison of the prevalence of the metabolic syndrome using two proposed definitions. Diabetes Care. 2003;26:575–581.
16 Lorenzo C, Okoloise M, Williams K, et al. The metabolic syndrome as a predictor of type 2 diabetes. Diabetes Care. 2003;26:3153–3159.
17 Wilson PW, D’Agostino RB, Parise H, et al. Metabolic syndrome as a precursor of cardio-vascular disease and type 2 diabetes mellitus. Circulation. 2005;112:3066–3072.
18 de Simone G, Devereux RB, Chinali M, et al; Strong Heart Study Investigators. Risk factors for arterial hypertension in adults with initial optimal blood pressure: the Strong Heart Study. Hypertension. 2006;47(2):162–167.
19 Malik S, Wong ND, Franklin SS, et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular dis-ease, and all causes in United States adults. Circulation. 2004;110:1245–1250.
20 Alexander CM, Landsman PB, Teutsch SM, et al. NCEP-defined metabolic syndrome, dia-betes, and prevalence of coronary heart disease among NHANES III participants age 50 years and older. Diabetes. 2003;52:1210–1214.
21 De Simone G, Devereux RB, Chinali M, et al. Prognostic impact of metabolic syn-drome by different definitions in a population with high prevalence of obesity and diabe-tes: the Strong Heart Study. Diabetes Care. 2007;7:1851–1856.
22 Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabe-tes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403.
23 Dietary Guidelines for Americans 2005. Department of Health and Human Services. http://www.health.gov/dietaryguidelines/dga2005/document/html/executivesummary.
htm. Accessed June 12, 2007. 24 Zephier EM, Ballew C, Mokdad A, et al.
Intake of nutrients related to cardiovascular disease risk among three groups of American Indians: The Strong Heart Dietary Study. Prev Med. 1997;26:508–515.
25 Story M, Strauss K, Gilbert T, et al. Nutritional Health and Diet related Concerns. In: Rhoades ER, ed. American Indian Health: Innovations in Health Care, Promotion, and Policy. Baltimore and London: The Johns Hopkins University Press; 2000:201–220.
26 Ballew C, White LL, Strauss KF, et al. Intake of nutrients and food sources of nutrients among the Navajo Indians: findings from the Navajo Health and Nutrition Survey. J Nutr. 1997;127:2085S–2093S.
27 Lichtenstein AH, Appel LJ, Brands M, et al. Diet and lifestyle recommendations revi-sion 2006: a scientific statement from the American Heart Association Nutrition com-mittee. Circulation. 2006;114:82–96.
28 US Department of Health and Human Services. Physical Activity and Health: A Report of the Surgeon General. Atlanta, GA: US Dept of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health promotion; 1996.
29 Irwin ML, Ainsworht BE, Mayer-Davis EJ, et al. Physical activity and the metabolic syn-drome in a tri-ethnic sample of women. Obes Res. 2002;10:1030–1037.
30 Yurgalevitch SM, Kriska AM, Welty TK, et al. Physical activity and lipids and lipoproteins in American Indians ages 45–74. Med Sci Sports Exerc. 1998;30(4):543–549.
31 Advance Data From Vital and Health Statistics, No 356, April 27, 2005. http://www.cdc.gov/nchs/data/ad/ad356.pdf. Accessed September 14, 2007.
32 Crespo CJ. Encouraging physical activity in minorities: eliminating disparities by 2010. Phys Sports Med. 2000;28(10):36–46.
33 Harnack L, Story M, Holy Rock B. Diet and physical activity patterns of Lakota adults. J Am Diet Assoc. 1999;99:829–835.
34 IHS Guidelines for Care of Adults With Prediabetes and/or the Metabolic Syndrome in Clinical Settings. www.ihs.gov/medicalprograms/diabetes. Accessed September 14, 2007.
The Journal of Cardiometabolic Syndrome (ISSN 1524-6175) is published quarterly (March, June, Sept., Dec.) by Le Jacq, a Blackwell Publishing imprint, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Copyright ©2007 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511.
®