Metabolic Syndrome Audit
1
Normal BMI Overweight Obese Class I Obese Class II Obese Class III 0 2 4 6 8 10 12 Male Female Normal BMI 11 1 Overweight 8 1 Obese Class I 7 0 Obese Class II 0 0 Obese Class III 1 0 BMI CLASSIFICATION NUMBER OF INDIVIDUALS Figure 2. Body Mass Index (BMI) Measurement of Service Users Results A total of 56 adults with intellectual disability were selected for the study. The median age range of individuals included in the study are as follows: 45 Male (80.3%, age range 30 – 69) 11 Female (19.6%, age range 36 to 66). Among the 56 adults, the severity of intellectual disability ranged from moderate to severe. Additionally, 4 individuals had a diagnosis of depression, 2 had a diagnosis of Bipolar Affective Disorder and 1 individual had a diagnosis of generalized Anxiety Disorder. 20 individuals suffered from Epilepsy. During the course of the study 3 new individuals were found to be diabetic on Fasting-plasma glucose measurement (FPG greater than 7.0 mmol/L). Additional, 6 individuals (Male =5, Female =1) were considered to be in the pre-diabetic range (FPG 5.6 – 6.9 mmol/L). In regards to metabolic parameter measurements, we found that 27 males had their available weight and height to obtain respective BMI measurements. Out the 27 males, 8 individuals were classified as overweight and another 8 was classified as obese. Among the females, only 2 individuals had both available weight and height measurements to calculate their respective BMI. In relation to lifestyle factors, there were only 10 males whole reported using alcohol and none of the service users (both male and female) smokes. It is interesting to note that prior to the audit there was no formal measurement and documentation of neither height nor waist measurement in any of the service user’s files. 44 of the males and 11 of the females had their weight checked at least once a year. 28 individuals had their weight checked monthly. Additionally, 29 individuals had their Blood pressure measured at least once yearly, and 9 individuals had their blood pressure measured more than once yearly. In total, 67.8% (N=38) of individuals had their baseline blood pressure measured once a year. With regards to Antipsychotic use, there were 39 individuals on antipsychotic treatment. Out of the 37, 34 were male and 6 were female. Most of the individuals were on single antipsychotic therapy (N=25), while a minority were being treated with dual-antipsychotics (N=14). The antipsychotic used ranged from Typical Antipsychotics– Haloperidol, Chlorpromazine, Zuclopenthixol; Atypical Antipsychotics – Aripiprazole, Risperidone, Olanzapine, Quetiapine. A majority of adults were on Risperidone (N=16) whereas, the second most commonly used antipsychotic was Chlorpromazine (N=13) and the third most commonly used was Haloperidol (N= 10). One individual was on a Depot formulation of Risperidone (Risperdal Consta). Background Patient with intellectual disability have a high rate of physical and psychiatric co-morbidities as compared to the general population. These factors in conjunction with the complex health needs associated with their intellectual disability, limited interpersonal communication, carer dependence, lifestyle and genetic predispositions place these individuals at a higher risk for developing cardiovascular diseases. Furthermore, this population group has a high rate of antipsychotics being prescribed for the management of their co-morbid psychiatric illness. Introduction Metabolic syndrome (MetS) is a cluster of co-occurring metabolic disturbances that interact to increase the likelihood for cardiovascular diseases. These factors include: raised fasting plasma glucose, abdominal obesity, high cholesterol and high blood pressure. 1, 2 Individuals with MetS are three times as likely to have a myocardial infarction or cerebrovascular event, and twice as likely to die from either. The risk for developing Type 2 Diabetes Mellitus is increased five-fold in these individuals. 3 Adults with serious mental illness are at a significantly higher risk for metabolic syndrome and cardio-metabolic problems. 4 There is growing evidence that prescription of atypical antipsychotics with metabolic side-effects have contributed towards these findings. Atypical antipsychotics have been shown to not only cause weight gain, but also lead to dyslipidemia, insulin resistance and hyperglycaemia. 5 Additionally, individuals with mental illness are less likely to attend to their own physical health and are more likely to smoke. 6 Adults with intellectual disability (ID) constitute a group in which antipsychotic use is high, but also have a greater predisposition to develop cardio-metabolic complications. In a cross-sectional study included in the Healthy Aging in Intellectual Disability (HA- ID) study of 980 people with borderline to profound ID, the researchers found that the percentages for diabetes, hypercholesterolemia, and the metabolic syndrome were 45%, 46% and 94% respectively among older persons with Intellectual Disability. 7 Another Dutch study of four hundred and twelve adults with intellectual disability found the prevalence of metabolic syndrome to be 25% of all participants [95% confidence interval (CI) 21.0-29.3%], with a significantly higher risk for people with mild ID. 8 There is limited evidence in the literature surrounding the prevalence of metabolic syndrome among individuals with intellectual disability. This study aims to explore the current practices of screening for metabolic syndrome in a population group with intellectual disability as well as gauge the current prevalence among residential service users. Definition According to the new IDF definition, for a person to be defined as having the metabolic syndrome they must have: Pathogenesis The pathogenesis of the metabolic syndrome and each of its components is complex and not well understood, central obesity and insulin resistance are considered to be the two most accepted hypothesis for metabolic syndrome. A major contributor to the development of insulin resistance is an overabundance of circulating fatty acids, released from an expanded adipose tissue mass. Free fatty acids (FFA) reduce insulin sensitivity in the muscle by inhibiting insulin-mediated glucose uptake. This in turn increases the level of circulating glucose, as a results there is an increase in pancreatic insulin secretion resulting in hyperinsulinemia. In the liver, FFA increases the production of glucose, triglycerides and secretion of very low density lipoproteins (VLDL). The consequence is the reduction in glucose transformation to glycogen and increased lipid accumulation in triglyceride (TG). Under normal conditions, insulin inhibits the secretion of VLDL into the systemic circulation. In the setting of insulin resistance, increased flux of free fatty acids to the liver increases hepatic triglyceride synthesis. Thus leading to hypertriglyceridemia, which is an excellent reflection of the insulin resistant condition and is one of the important criteria for diagnosis of the metabolic syndrome. The other major lipoprotein disturbance in the metabolic syndrome is a reduction in HDL cholesterol. This reduction is a consequence of changes in HDL composition and metabolism as a direct result of decreases in the cholesteryl ester content of the lipoprotein core during increased production of triglyceride Abdominal obesity is another key causative factor for metabolic syndrome. Those who are called metabolically obese, normal- weight individuals, typically having increased amount of visceral adipose tissue. According to current theories, with increases in visceral adipose tissue, there is a higher rate of flux of adipose tissue-derived free fatty acids to the liver through the splanchnic circulation, thus increases in abdominal subcutaneous fat could release large amounts of lipolysis products into the systemic circulation and avoid more direct effects on hepatic metabolism. Insulin is a vasodilator when given intravenously to people of normal weight, with secondary effects on sodium reabsorption in the kidney. In the setting of insulin resistance, the vasodilatory effect of insulin can be lost, but the renal effect on sodium reabsorption is preserved thus directly impacting total blood volume. Additionally, hyperinsulinemia can lead to increased sympathetic nervous system activation and contribute to developing hypertension. 9 Audit on Screening for Metabolic Syndrome in patients with Intellectual Disability Vishnu Pradeep 1 , Tareq Ghani 2 , Nuraini Ibrahim 3 , Mary Kelly 4 1 Senior House Officer, Brothers of Charity, Bawnmore, Limerick 2 Senior House Officer, University Hospital Limerick 3 Senior House Officer, Daughters of Charity, Lisnagry, Limerick 4 Consultant Psychiatrist, Brothers of Charity and Daughters of Charity, Limerick Study Aim This audit aims to examine the practice of monitoring metabolic syndrome in patients with intellectual disability who are in residential care in Brothers of Charity Services, Limerick. Method A single page, two-sided checklist was devised with input from the multi-disciplinary team based in Brothers of Charity Services (BOC), Bawnmore using the parameters for metabolic syndrome as recommended by the new International Diabetes Federation (IDF) definition. It includes information on age, sex, current medications, family history, lifestyle factors, risk factors for metabolic syndrome and frequency of monitoring the aforementioned parameters. Patient information and relevant data were obtained from the medical notes and health record. The study was completed over a period of two months from 9 th February to 25 th of March 2016 on a sample of residential service users attending the Psychiatry of Intellectual Disability services at Bawnmore. The inclusion criteria were set to the following: (1) Is currently a residential service user in the Brothers of Charity, Bawnmore Services; (2) Is aged 18 years or over. The exclusion criteria were as following: (1) Is currently a resident outside the Brothers of Charity, Bawnmore; (2) Patient aged under 18 years. All patients fulfilling the criteria were included in the study. Permission to conduct the study was obtained from the BOC Senior Management team. The study was undertaken with respect for the rights to privacy and in a manner consistent with local policy and international guidelines as set by the World Health Organization and Declaration of Helsinki. See sample of Metabolic Syndrome Monitoring form below: 0 2 4 6 8 10 12 14 16 (Total=13) (Total=17) (Total=2) (Total =3) Hypertension Dyslipidemia Diabetes Ischaemic Heart Disease Number of Individuals Type of Co-Morbidty Figure 1. Cardio-metabolic Co-morbidities in the Sample Population with ID Males Females 0 41 0 41 39 42 0 11 0 8 11 11 Waist Measurement Weight Height BP Fasting Lipids Fasting Glucose 0 5 10 15 20 25 30 35 40 45 Metabolic Parameters Number of Individuals Waist Measurement Weight Height BP Fasting Lipids Fasting Glucose Female (Total N=11) 0 11 0 8 11 11 Male (Total N=45) 0 41 0 41 39 42 Figure 3. Metabolic parameters available during study Female (Total N=11) Male (Total N=45) Results - Metabolic Syndrome From demographic analysis of individuals with metabolic syndrome, there were 10 males and 2 females of age range between 32-69, and 65-55 respectively. An overall prevalence of 21.4% (N=12) of all service users who participated in the study fit the criteria for metabolic syndrome. Of note, waist measurements were unavailable in around 12 individuals, and 3 of whom fulfilled the 2 sub-criteria for metabolic syndrome thus raising the possibility that these individuals could also have metabolic syndrome. Some of the overall limitation of the study lies in the fact that the sample population included a lower number of females, this is partly due to historical factors in relation to service delivery. Nevertheless, we found that among the male individuals a significant disparity in relation to the incidence of diabetes. There is at least 2 established diabetics, 4 individuals in the pre-diabetic range and an additional 2 newly diagnosed diabetics. There is also an overrepresentation of individuals on antipsychotic therapy (75% N=9). Additionally, the mean BMI among the males is 29.8 (range 22.4 -34.1). 4 males are classified as obese, 2 as overweight and 1 fell within the normal BMI range; parameters for BMI calculation were not available for 3 of the other individuals. One among the two women with metabolic syndrome was classified as overweight. Both the women had hypertension and one of them had dyslipidemia. None of them received antipsychotic treatment. Conclusion In our study we observed that 21.5% of all service users had Metabolic syndrome, this is quite a significant observation as among those who had MetS, 40% had diabetes, another 20% were in the pre-diabetic range; additionally, 42% males with MetS were obese, and finally 75% of individuals (all of whom are male) were on antipsychotic therapy. It is not yet clear from our finding if there is a clear association between MetS and antipsychotic use, but it is clear in various other studies that antipsychotics do dramatically contribute to developing metabolic syndrome. It is interesting to note that dietary intake and activity level have a major impact on the resident’s health. The laxing of dietary rules by care-staff, type of catering provided as well as impact of co-morbid neurological disorders such as epilepsy and cerebral palsy have also a major role to play in snowballing the development of metabolic syndrome. 35.7% of the residents suffer from epilepsy which usually pose an additional challenge due to (1) the refractory nature of the seizures requiring multiple anticonvulsants (2) residual behavioural and psychological impact of the seizures themselves and (3) Cardio- metabolic side-effects of the anticonvulsants. In regards to prescribing practices, our study found that 9 out of 12 individuals with MetS were on antipsychotic treatment. The likely cause as highlighted in various studies lies in the propensity of atypical antipsychotics (especially Olanzapine, Risperidone) to contribute to weight gain, and increases in serum triglyceride levels. In our study, only 6 individuals were on Olanzapine. Interestingly, only 1out of this 6 had developed MetS. Dual-antipsychotic use is another significant factor that we have noticed to contribute towards developing MetS in our study sample. Careful consideration must be made when managing persons at high risk for MetS and if antipsychotic treatment is indicated then an appropriate antipsychotic with a good cardio-metabolic profile must be chosen. It is very clear that patient with intellectual disability remain at a higher risk for cardiovascular complications than the general population. Despite the availability of current clinical guidelines, patients with intellectual disability receiving antipsychotic therapy have poor documentation and management of their metabolic parameters. Our findings provide evidence for the necessity of having strict monitoring of the metabolic parameters and to consider including yearly height and waist measurements to the current panel of metabolic parameters to be followed up. Lack of documentation of family history and metabolic risks such as alcohol and smoking use can lead to omission of important information that could make a worthwhile difference in monitoring at-risk individuals. Although smoking and alcohol use is less in persons with ID, among the 10 males with MetS, 3 individuals reported using alcohol. Finally, the lack of documented family history of cardiovascular history poses a major challenge as it is one of the biggest predictor along with external factors to the likelihood of an individual developing MetS. Strengths and Limitations of the Study The major limitation of the study was the small sample size. Additional factors such as accessibility, availability of knowledgeable care-staff during review process and frequent changes among resident placements contributed to difficulties with obtaining full clinical and non-clinical details. It is currently unclear to the exact cause for the level of metabolic syndrome observed in our study, further longitudinal research is required to better understand if these changes are due to antipsychotic use or other physical or environmental factors. Finally, in a minority of individuals, certain metabolic parameters were unable to be measured due to persistent challenging behaviour; these individuals likely fall under a greater risk for developing metabolic syndrome due to (1) lack of proper metabolic assessment and appropriate intervention (2) risk of polypharmacy in view of management of challenging behaviour (3) Inability to monitor metabolic impact of newly introduced or discontinued psychotropic medications. Some of the strengths of the study lies in its ability to highlight the following: 1. The lack of a formal protocol for measurement of the parameters of metabolic syndrome in individuals with Intellectual Disability attending the BOC services 2. The clinical impact of central obesity as a key contributing factor towards developing MetS 3. Lack of waist, height or BMI measurements in a significant number of individuals 4. Lack of appropriate documentation of family, alcohol and smoking history Recommendations and Key Points In order to address the highlighted issues, the following recommendations were made: 1. A standardized form would be developed for measurement of parameters of metabolic syndrome in all individuals attending the BOC Services at Bawnmore 2. A follow up audit would be performed to assess compliance in the next 6 months 3. Information obtained from the preliminary study would be disseminated to key staff in order to raise awareness and encourage further development in detecting and managing metabolic syndrome among persons with ID A broad approach towards addressing metabolic syndrome should be considered, it can be subdivided as: Lifestyle Modification 1. There is growing evidence that clinical management of Metabolic syndrome much focus first on lifestyle changes – specifically on weight reduction and increased exercise. 2. Dietary management specifically directed towards limiting carbohydrate intake, rather than the more commonly prescribed reduction in dietary fats is seen to be more effective in reducing the most common symptoms of metabolic syndrome. Dietary adjustment should be the cornerstone for management of all individuals with metabolic syndrome. Pharmacological Interventions 1. Elevated LDL is managed with statins in conjunction with individualized guideline recommended goals 2. Management protocols for reduced HDL remains controversial and at present is limited to diet and lifestyle modifications, and may include treatment with Niacin. Fibrates have been shown to have reduce end-points of cardiovascular disease in patients with atherogenic dyslipidemia and metabolic syndrome 3. Metformin and Thiazolinediones have been observed to be specifically beneficial in metabolic syndrome; but data regarding cardiovascular end-points remain limited Acknowledgements The authors would like to thank the staff at Brothers of Charity Services at Bawnmore for their support with the study. The authors would also like to thank Miss Luna Meschiari for her guidance with statistical analysis and database creation. References: 1. Alberti KG, Zimmet P, Shaw J; IDF Epidemiology Task Force Consensus Group. The metabolic syndrome new worldwide definition. Lancet 2005;366:1059-62 2. Hasnain, M., Vieweg, W. V. R., Fredrickson, S. K., Beatty-Brooks, M., Fernandez, A., & Pandurangi, A. K. (2009). Clinical monitoring and management of the metabolic syndrome in patients receiving atypical antipsychotic medications. Primary Care Diabetes, 3, 5–15. 3. International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. Brussels: International Diabetes Federation; 2006 4. Allison, D. B., Mentore, J. L., Heo, M., Chandler, L. P., Cappelleri, J. C., Infante, M. C., et al. (1999). Antipsychotic-induced weight gain: A comprehensive research synthesis. American Journal of Psychiatry, 156, 1686–1696. 5. De Hert M, Schreurs V, Vancampfort D, Van Winkel R. Metabolic syndrome in people with schizophrenia: a review. World Psychiatry 2009; 8(1): 15-22. 6. Lunsky, Y., Lin, E., Balogh, R., & Klein-Geltink, J. (2011). Diabetes prevalence among persons with serious mental illness and developmental disability. Psychiatric Services, 62, 830. 7. De Winter CF, Batiaanse LP, Hilgenkamp TI. (2012) Cardiovascular risk factors (diabetes, hypertension, hypercholesterolemia and metabolic syndrome) in older people with intellectual disability: results of the HA-ID study. Res Dev Disabil. 2012 Nov- Dec;33(6):1722-31. 8. De Winter CF., Magnilsen KW, Van Alfen JC. (2010). Metabolic Syndrome in 25% of Older people with intellectual disability. Fam Practice. 2011 Apr;28(2):141-4. 9. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III), JAMA 2001; 285:2486–97. “75% of people with Metabolic Syndrome are on Antipsychotics” “ A quarter of the world’s adults have metabolic syndrome” – International Diabetes Federation (2006) 12 5 22 3 11 3 0 5 10 15 20 25 Males Females Number of individuals Antipsychotic Use Figure 5. Antipsychotic use in ID Sample Not on Antipsychotics (Total N=17) On Single Antipscyhotics (Total N=25) On dual-antipscyhotics (Total N=14) “ 21.4% of individuals with ID have Metabolic Syndrome ” 10 2 35 9 0 5 10 15 20 25 30 35 40 Males Females Number of Individuals Sex of Individuals with ID Males Females No Metabolic Syndrome 35 9 Metabolic Syndrome 10 2 Figure 4. Metabolic Syndrome in ID population No Metabolic Syndrome Metabolic Syndrome
-
Upload
tareq-abdel-ghani-md -
Category
Documents
-
view
61 -
download
1
Transcript of Metabolic Syndrome Audit

Normal BMI
Overweight
Obese Class I
Obese Class II
Obese Class III
0
2
4
6
8
10
12
Male Female
Normal BMI 11 1
Overweight 8 1
Obese Class I 7 0
Obese Class II 0 0
Obese Class III 1 0
BM
I C
LA
SS
IFIC
AT
ION
NU
MB
ER
OF
IN
DIV
IDU
AL
S
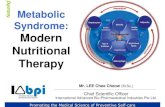
Figure 2. Body Mass Index (BMI) Measurement of Service Users
Results
A total of 56 adults with intellectual disability were selected for the study. The median age range of individuals included in the
study are as follows: 45 Male (80.3%, age range 30 – 69) 11 Female (19.6%, age range 36 to 66). Among the 56 adults, the
severity of intellectual disability ranged from moderate to severe. Additionally, 4 individuals had a diagnosis of depression, 2
had a diagnosis of Bipolar Affective Disorder and 1 individual had a diagnosis of generalized Anxiety Disorder. 20 individuals
suffered from Epilepsy.
During the course of the study 3 new individuals were found to be diabetic on Fasting-plasma glucose measurement (FPG
greater than 7.0 mmol/L). Additional, 6 individuals (Male =5, Female =1) were considered to be in the pre-diabetic range (FPG
5.6 – 6.9 mmol/L). In regards to metabolic parameter measurements, we found that 27 males had their available weight and
height to obtain respective BMI measurements. Out the 27 males, 8 individuals were classified as overweight and another 8
was classified as obese. Among the females, only 2 individuals had both available weight and height measurements to
calculate their respective BMI.
In relation to lifestyle factors, there were only 10 males whole reported using alcohol and none of the service users (both male
and female) smokes. It is interesting to note that prior to the audit there was no formal measurement and documentation of
neither height nor waist measurement in any of the service user’s files. 44 of the males and 11 of the females had their weight
checked at least once a year. 28 individuals had their weight checked monthly. Additionally, 29 individuals had their Blood
pressure measured at least once yearly, and 9 individuals had their blood pressure measured more than once yearly. In total,
67.8% (N=38) of individuals had their baseline blood pressure measured once a year.
With regards to Antipsychotic use, there were 39 individuals on antipsychotic treatment. Out of the 37, 34 were male and 6
were female. Most of the individuals were on single antipsychotic therapy (N=25), while a minority were being treated with
dual-antipsychotics (N=14). The antipsychotic used ranged from Typical Antipsychotics– Haloperidol, Chlorpromazine,
Zuclopenthixol; Atypical Antipsychotics – Aripiprazole, Risperidone, Olanzapine, Quetiapine. A majority of adults were on
Risperidone (N=16) whereas, the second most commonly used antipsychotic was Chlorpromazine (N=13) and the third most
commonly used was Haloperidol (N= 10). One individual was on a Depot formulation of Risperidone (Risperdal Consta).
Background
Patient with intellectual disability have a high rate of physical and psychiatric co-morbidities as compared to the general population.
These factors in conjunction with the complex health needs associated with their intellectual disability, limited interpersonal
communication, carer dependence, lifestyle and genetic predispositions place these individuals at a higher risk for developing
cardiovascular diseases. Furthermore, this population group has a high rate of antipsychotics being prescribed for the management
of their co-morbid psychiatric illness.
Introduction
Metabolic syndrome (MetS) is a cluster of co-occurring metabolic disturbances that interact to increase the likelihood for
cardiovascular diseases. These factors include: raised fasting plasma glucose, abdominal obesity, high cholesterol and high blood
pressure.1, 2 Individuals with MetS are three times as likely to have a myocardial infarction or cerebrovascular event, and twice as
likely to die from either. The risk for developing Type 2 Diabetes Mellitus is increased five-fold in these individuals.3
Adults with serious mental illness are at a significantly higher risk for metabolic syndrome and cardio-metabolic problems.4 There is
growing evidence that prescription of atypical antipsychotics with metabolic side-effects have contributed towards these findings.
Atypical antipsychotics have been shown to not only cause weight gain, but also lead to dyslipidemia, insulin resistance and
hyperglycaemia.5 Additionally, individuals with mental illness are less likely to attend to their own physical health and are more
likely to smoke.6
Adults with intellectual disability (ID) constitute a group in which antipsychotic use is high, but also have a greater predisposition
to develop cardio-metabolic complications. In a cross-sectional study included in the Healthy Aging in Intellectual Disability (HA-
ID) study of 980 people with borderline to profound ID, the researchers found that the percentages for diabetes,
hypercholesterolemia, and the metabolic syndrome were 45%, 46% and 94% respectively among older persons with Intellectual
Disability. 7 Another Dutch study of four hundred and twelve adults with intellectual disability found the prevalence of metabolic
syndrome to be 25% of all participants [95% confidence interval (CI) 21.0-29.3%], with a significantly higher risk for people with
mild ID.8
There is limited evidence in the literature surrounding the prevalence of metabolic syndrome among individuals with intellectual
disability. This study aims to explore the current practices of screening for metabolic syndrome in a population group with
intellectual disability as well as gauge the current prevalence among residential service users.
Definition
According to the new IDF definition, for a person to be defined as having the metabolic syndrome they must have:
A. Central obesity (defined as waist circumference ≥ 94cm for Europid men and ≥ 80cm for Europid women, with ethnicity specific
values for other groups)
B. Plus, any two of the following four factors:
1. Raised TG level: ≥ 150 mg/dL (1.7 mmol/L), or specific treatment for this lipid abnormality
2. Reduced HDL cholesterol: < 40 mg/dL (1.03 mmol/L) in males and < 50 mg/dL (1.29 mmol/L) in females, or
specific treatment for this lipid abnormality
3. Raised blood pressure: systolic BP ≥ 130 or diastolic BP ≥ 85 mm Hg, or treatment of previously diagnosed
hypertension
4. Raised fasting plasma glucose (FPG) ≥ 100 mg/dL (5.6 mmol/L), or previously diagnosed type 2 diabetes If
above 5.6 mmol/L or 100 mg/dL, OGTT is strongly recommended but is not necessary to define presence of the
syndrome.
Pathogenesis
The pathogenesis of the metabolic syndrome and each of its components is complex and not well understood, central obesity and
insulin resistance are considered to be the two most accepted hypothesis for metabolic syndrome. A major contributor to the
development of insulin resistance is an overabundance of circulating fatty acids, released from an expanded adipose tissue mass.
Free fatty acids (FFA) reduce insulin sensitivity in the muscle by inhibiting insulin-mediated glucose uptake. This in turn increases
the level of circulating glucose, as a results there is an increase in pancreatic insulin secretion resulting in hyperinsulinemia. In the
liver, FFA increases the production of glucose, triglycerides and secretion of very low density lipoproteins (VLDL). The consequence
is the reduction in glucose transformation to glycogen and increased lipid accumulation in triglyceride (TG).
Under normal conditions, insulin inhibits the secretion of VLDL into the systemic circulation. In the setting of insulin resistance,
increased flux of free fatty acids to the liver increases hepatic triglyceride synthesis. Thus leading to hypertriglyceridemia, which
is an excellent reflection of the insulin resistant condition and is one of the important criteria for diagnosis of the metabolic
syndrome. The other major lipoprotein disturbance in the metabolic syndrome is a reduction in HDL cholesterol. This reduction is a
consequence of changes in HDL composition and metabolism as a direct result of decreases in the cholesteryl ester content of the
lipoprotein core during increased production of triglyceride
Abdominal obesity is another key causative factor for metabolic syndrome. Those who are called metabolically obese, normal-
weight individuals, typically having increased amount of visceral adipose tissue. According to current theories, with increases in
visceral adipose tissue, there is a higher rate of flux of adipose tissue-derived free fatty acids to the liver through the splanchnic
circulation, thus increases in abdominal subcutaneous fat could release large amounts of lipolysis products into the systemic
circulation and avoid more direct effects on hepatic metabolism.
Insulin is a vasodilator when given intravenously to people of normal weight, with secondary effects on sodium reabsorption in the
kidney. In the setting of insulin resistance, the vasodilatory effect of insulin can be lost, but the renal effect on sodium reabsorption is
preserved thus directly impacting total blood volume. Additionally, hyperinsulinemia can lead to increased sympathetic nervous
system activation and contribute to developing hypertension.9
Audit on Screening for Metabolic Syndrome in patients with Intellectual Disability
Vishnu Pradeep1, Tareq Ghani2, Nuraini Ibrahim 3, Mary Kelly4
1Senior House Officer, Brothers of Charity, Bawnmore, Limerick 2Senior House Officer, University Hospital Limerick
3Senior House Officer, Daughters of Charity, Lisnagry, Limerick 4Consultant Psychiatrist, Brothers of Charity and Daughters of Charity, Limerick
Study Aim
This audit aims to examine the practice of monitoring metabolic syndrome in patients with intellectual disability who are in
residential care in Brothers of Charity Services, Limerick.
Method
A single page, two-sided checklist was devised with input from the multi-disciplinary team based in Brothers of Charity Services
(BOC), Bawnmore using the parameters for metabolic syndrome as recommended by the new International Diabetes Federation
(IDF) definition. It includes information on age, sex, current medications, family history, lifestyle factors, risk factors for metabolic
syndrome and frequency of monitoring the aforementioned parameters. Patient information and relevant data were obtained from
the medical notes and health record. The study was completed over a period of two months from 9th February to 25th of March 2016
on a sample of residential service users attending the Psychiatry of Intellectual Disability services at Bawnmore. The inclusion
criteria were set to the following: (1) Is currently a residential service user in the Brothers of Charity, Bawnmore Services; (2) Is aged
18 years or over. The exclusion criteria were as following: (1) Is currently a resident outside the Brothers of Charity, Bawnmore; (2)
Patient aged under 18 years. All patients fulfilling the criteria were included in the study. Permission to conduct the study was
obtained from the BOC Senior Management team. The study was undertaken with respect for the rights to privacy and in a manner
consistent with local policy and international guidelines as set by the World Health Organization and Declaration of Helsinki.
See sample of Metabolic Syndrome Monitoring form below:
0
2
4
6
8
10
12
14
16
(Total=13) (Total=17) (Total=2) (Total =3)
Hypertension Dyslipidemia Diabetes Ischaemic Heart Disease
Nu
mb
er o
f In
div
idu
als
Type of Co-Morbidty
Figure 1. Cardio-metabolic Co-morbidities in the Sample Population with ID
Males Females
0
41
0
41
39
42
0
11
0
8
11
11
Waist Measurement
Weight
Height
BP
Fasting Lipids
Fasting Glucose
0 5 10 15 20 25 30 35 40 45
Met
abo
lic P
aram
eter
s
Number of Individuals
Waist Measurement Weight Height BP Fasting Lipids Fasting Glucose
Female (Total N=11) 0 11 0 8 11 11
Male (Total N=45) 0 41 0 41 39 42
Figure 3. Metabolic parameters available during study
Female (Total N=11) Male (Total N=45)
Results - Metabolic Syndrome
From demographic analysis of individuals with metabolic syndrome, there were 10 males and 2 females of age range between
32-69, and 65-55 respectively. An overall prevalence of 21.4% (N=12) of all service users who participated in the study fit the
criteria for metabolic syndrome. Of note, waist measurements were unavailable in around 12 individuals, and 3 of whom
fulfilled the 2 sub-criteria for metabolic syndrome thus raising the possibility that these individuals could also have metabolic
syndrome. Some of the overall limitation of the study lies in the fact that the sample population included a lower number of
females, this is partly due to historical factors in relation to service delivery. Nevertheless, we found that among the male
individuals a significant disparity in relation to the incidence of diabetes. There is at least 2 established diabetics, 4 individuals
in the pre-diabetic range and an additional 2 newly diagnosed diabetics. There is also an overrepresentation of individuals on
antipsychotic therapy (75% N=9). Additionally, the mean BMI among the males is 29.8 (range 22.4 -34.1). 4 males are classified as
obese, 2 as overweight and 1 fell within the normal BMI range; parameters for BMI calculation were not available for 3 of the
other individuals. One among the two women with metabolic syndrome was classified as overweight. Both the women had
hypertension and one of them had dyslipidemia. None of them received antipsychotic treatment.
Conclusion
In our study we observed that 21.5% of all service users had Metabolic syndrome, this is quite a significant observation as among
those who had MetS, 40% had diabetes, another 20% were in the pre-diabetic range; additionally, 42% males with MetS were obese,
and finally 75% of individuals (all of whom are male) were on antipsychotic therapy. It is not yet clear from our finding if there is a
clear association between MetS and antipsychotic use, but it is clear in various other studies that antipsychotics do dramatically
contribute to developing metabolic syndrome. It is interesting to note that dietary intake and activity level have a major impact on
the resident’s health. The laxing of dietary rules by care-staff, type of catering provided as well as impact of co-morbid neurological
disorders such as epilepsy and cerebral palsy have also a major role to play in snowballing the development of metabolic syndrome.
35.7% of the residents suffer from epilepsy which usually pose an additional challenge due to (1) the refractory nature of the seizures
requiring multiple anticonvulsants (2) residual behavioural and psychological impact of the seizures themselves and (3) Cardio-
metabolic side-effects of the anticonvulsants.
In regards to prescribing practices, our study found that 9 out of 12 individuals with MetS were on antipsychotic treatment. The
likely cause as highlighted in various studies lies in the propensity of atypical antipsychotics (especially Olanzapine, Risperidone) to
contribute to weight gain, and increases in serum triglyceride levels. In our study, only 6 individuals were on Olanzapine.
Interestingly, only 1out of this 6 had developed MetS. Dual-antipsychotic use is another significant factor that we have noticed to
contribute towards developing MetS in our study sample. Careful consideration must be made when managing persons at high risk
for MetS and if antipsychotic treatment is indicated then an appropriate antipsychotic with a good cardio-metabolic profile must be
chosen.
It is very clear that patient with intellectual disability remain at a higher risk for cardiovascular complications than the general
population. Despite the availability of current clinical guidelines, patients with intellectual disability receiving antipsychotic therapy
have poor documentation and management of their metabolic parameters. Our findings provide evidence for the necessity of having
strict monitoring of the metabolic parameters and to consider including yearly height and waist measurements to the current panel
of metabolic parameters to be followed up. Lack of documentation of family history and metabolic risks such as alcohol and
smoking use can lead to omission of important information that could make a worthwhile difference in monitoring at-risk
individuals. Although smoking and alcohol use is less in persons with ID, among the 10 males with MetS, 3 individuals reported
using alcohol. Finally, the lack of documented family history of cardiovascular history poses a major challenge as it is one of the
biggest predictor along with external factors to the likelihood of an individual developing MetS.
Strengths and Limitations of the Study
The major limitation of the study was the small sample size. Additional factors such as accessibility, availability of knowledgeable
care-staff during review process and frequent changes among resident placements contributed to difficulties with obtaining full
clinical and non-clinical details. It is currently unclear to the exact cause for the level of metabolic syndrome observed in our study,
further longitudinal research is required to better understand if these changes are due to antipsychotic use or other physical or
environmental factors. Finally, in a minority of individuals, certain metabolic parameters were unable to be measured due to
persistent challenging behaviour; these individuals likely fall under a greater risk for developing metabolic syndrome due to (1) lack
of proper metabolic assessment and appropriate intervention (2) risk of polypharmacy in view of management of challenging
behaviour (3) Inability to monitor metabolic impact of newly introduced or discontinued psychotropic medications.
Some of the strengths of the study lies in its ability to highlight the following:
1. The lack of a formal protocol for measurement of the parameters of metabolic syndrome in individuals with Intellectual
Disability attending the BOC services
2. The clinical impact of central obesity as a key contributing factor towards developing MetS
3. Lack of waist, height or BMI measurements in a significant number of individuals
4. Lack of appropriate documentation of family, alcohol and smoking history
Recommendations and Key Points
In order to address the highlighted issues, the following recommendations were made:
1. A standardized form would be developed for measurement of parameters of metabolic syndrome in all individuals attending
the BOC Services at Bawnmore
2. A follow up audit would be performed to assess compliance in the next 6 months
3. Information obtained from the preliminary study would be disseminated to key staff in order to raise awareness and encourage
further development in detecting and managing metabolic syndrome among persons with ID
A broad approach towards addressing metabolic syndrome should be considered, it can be subdivided as:
Lifestyle Modification
1. There is growing evidence that clinical management of Metabolic syndrome much focus first on lifestyle changes – specifically
on weight reduction and increased exercise.
2. Dietary management specifically directed towards limiting carbohydrate intake, rather than the more commonly prescribed
reduction in dietary fats is seen to be more effective in reducing the most common symptoms of metabolic syndrome. Dietary
adjustment should be the cornerstone for management of all individuals with metabolic syndrome.
Pharmacological Interventions
1. Elevated LDL is managed with statins in conjunction with individualized guideline recommended goals
2. Management protocols for reduced HDL remains controversial and at present is limited to diet and lifestyle modifications, and
may include treatment with Niacin. Fibrates have been shown to have reduce end-points of cardiovascular disease in patients
with atherogenic dyslipidemia and metabolic syndrome
3. Metformin and Thiazolinediones have been observed to be specifically beneficial in metabolic syndrome; but data regarding
cardiovascular end-points remain limited
Acknowledgements
The authors would like to thank the staff at Brothers of Charity Services at Bawnmore for their support with the study. The authors
would also like to thank Miss Luna Meschiari for her guidance with statistical analysis and database creation.
References:1. Alberti KG, Zimmet P, Shaw J; IDF Epidemiology Task Force Consensus Group. The metabolic syndrome new worldwide
definition. Lancet 2005;366:1059-622. Hasnain, M., Vieweg, W. V. R., Fredrickson, S. K., Beatty-Brooks, M., Fernandez, A., & Pandurangi, A. K. (2009). Clinical
monitoring and management of the metabolic syndrome in patients receiving atypical antipsychotic medications. Primary Care Diabetes, 3, 5–15.
3. International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. Brussels: International Diabetes Federation; 2006
4. Allison, D. B., Mentore, J. L., Heo, M., Chandler, L. P., Cappelleri, J. C., Infante, M. C., et al. (1999). Antipsychotic-induced weight gain: A comprehensive research synthesis. American Journal of Psychiatry, 156, 1686–1696.
5. De Hert M, Schreurs V, Vancampfort D, Van Winkel R. Metabolic syndrome in people with schizophrenia: a review. World Psychiatry 2009; 8(1): 15-22.
6. Lunsky, Y., Lin, E., Balogh, R., & Klein-Geltink, J. (2011). Diabetes prevalence among persons with serious mental illness and developmental disability. Psychiatric Services, 62, 830.
7. De Winter CF, Batiaanse LP, Hilgenkamp TI. (2012) Cardiovascular risk factors (diabetes, hypertension, hypercholesterolemia and metabolic syndrome) in older people with intellectual disability: results of the HA-ID study. Res Dev Disabil. 2012 Nov-Dec;33(6):1722-31.
8. De Winter CF., Magnilsen KW, Van Alfen JC. (2010). Metabolic Syndrome in 25% of Older people with intellectual disability. Fam Practice. 2011 Apr;28(2):141-4.
9. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection,
Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III), JAMA 2001; 285:2486–97.
“75% of people with Metabolic
Syndrome are on Antipsychotics”
“A quarter of the world’s adults have metabolic syndrome”
– International Diabetes Federation (2006)
12
5
22
3
11
3
0
5
10
15
20
25
Males Females
Nu
mb
er o
f in
div
idu
als
Antipsychotic Use
Figure 5. Antipsychotic use in ID Sample
Not on Antipsychotics (Total N=17) On Single Antipscyhotics (Total N=25) On dual-antipscyhotics (Total N=14)
“21.4% of individuals with ID have Metabolic Syndrome ”
10
2
35
9
0 5 10 15 20 25 30 35 40
Males
Females
Number of Individuals
Sex
of
Ind
ivid
ual
s w
ith
ID
Males Females
No Metabolic Syndrome 35 9
Metabolic Syndrome 10 2
Figure 4. Metabolic Syndrome in ID population
No Metabolic Syndrome Metabolic Syndrome





![Metabolic Syndrome[1]](https://static.fdocuments.us/doc/165x107/577cd7141a28ab9e789dffc3/metabolic-syndrome1.jpg)