Metabolic syndrome,obesity
44
Weight Control Strategies in Metabolic Syndrome Dr Haider Ali Final Year Trainee Cardiology Unit LRH
-
Upload
ali-yousafzai -
Category
Health & Medicine
-
view
79 -
download
2
Transcript of Metabolic syndrome,obesity
Weight Control Strategies in Metabolic
SyndromeDr Haider Ali
Final Year TraineeCardiology Unit LRH

WHAT IS METABOLIC SNYNDROME
• A constellation of interrelated risk factors of metabolic origin which promote the development of ASCVD
• Patients with the metabolic syndrome also are at increased risk for developing type 2 diabetes mellitus
WHAT IS METABOLIC SNYNDROME

Metabolic Syndrome
Central Obesity
High BP
High FBSHigh TG
Low HDL
protein

HOW TO DIAGNOSE METABOLIC SNYNDROME
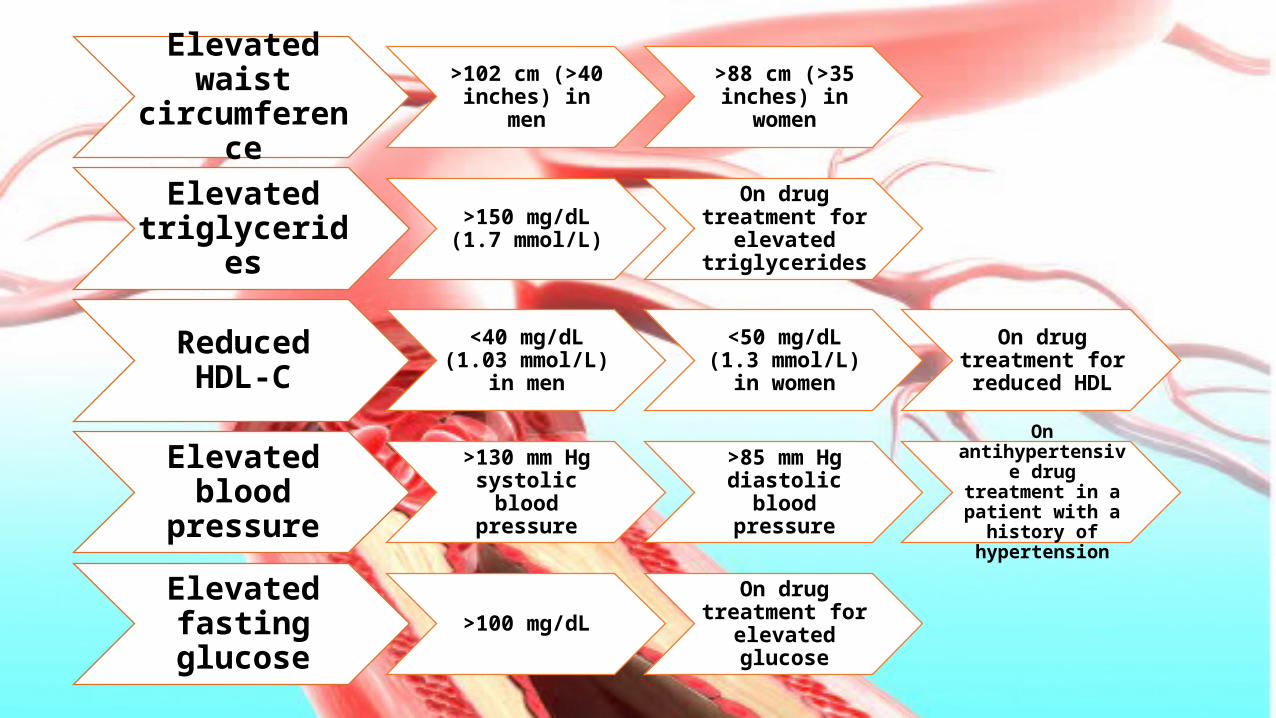
Elevated waist circumference
>102 cm (>40 inches) in men
>88 cm (>35 inches) in women
Elevated triglycerides
>150 mg/dL (1.7 mmol/L)
On drug treatment for elevated triglycerides
Reduced HDL-C <40 mg/dL (1.03 mmol/L) in men
<50 mg/dL (1.3 mmol/L) in women
On drug treatment for reduced HDL
Elevated blood pressure
>130 mm Hg systolic blood
pressure
>85 mm Hg diastolic blood
pressure
On antihypertensive drug treatment in a
patient with a history of hypertension
Elevated fasting glucose
>100 mg/dLOn drug treatment
for elevated glucose
Underlying Risk Factors• The predominant underlying risk factors for the syndrome appear to
be abdominal obesity and insulin resistance
• Other associated conditions can be physical inactivity, aging, and hormonal imbalance
• According to one theory insulin resistance is the essential cause of the metabolic syndrome
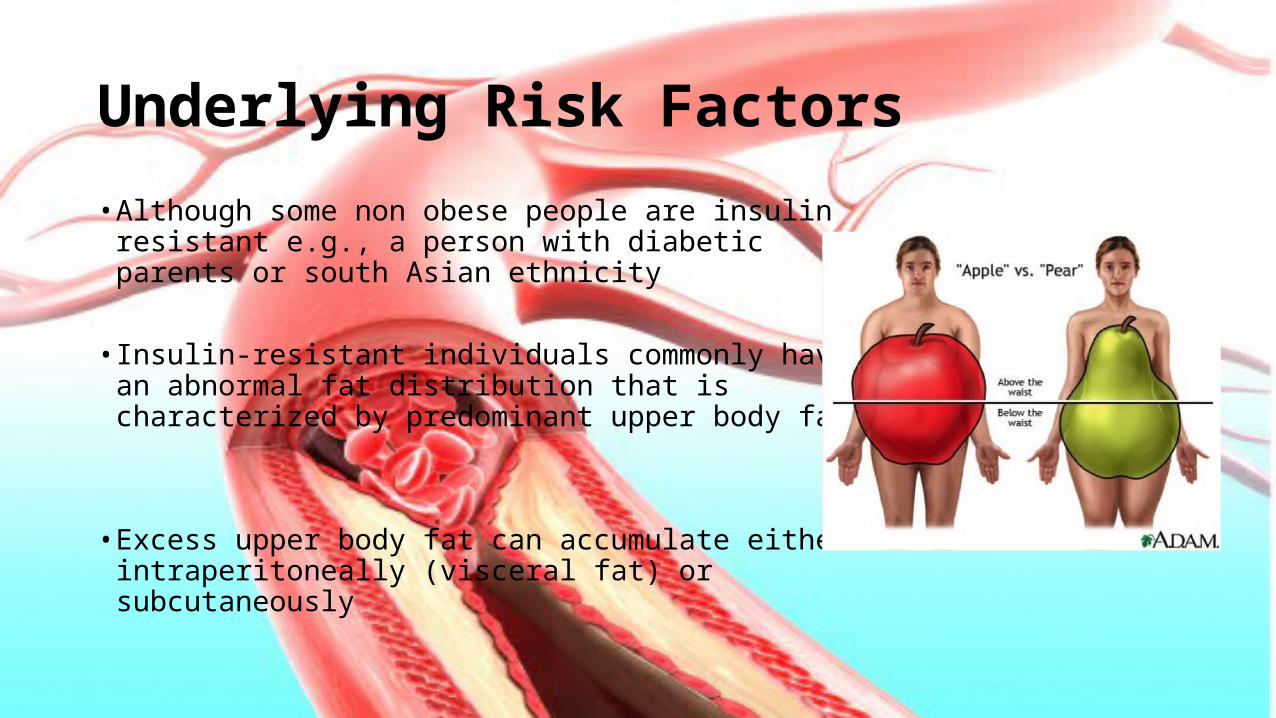
Underlying Risk Factors• Although some non obese people are insulin resistant
e.g., a person with diabetic parents or south Asian ethnicity
• Insulin-resistant individuals commonly have an abnormal fat distribution that is characterized by predominant upper body fat
• Excess upper body fat can accumulate either
intraperitoneally (visceral fat) or subcutaneously
Underlying Risk Factors• A pattern of upper abdominal obesity correlates more strongly with
insulin resistance and the metabolic syndrome than does lower-body obesity
• Upper-body obesity is related with an unusually high release of NEFA from adipose tissue
• Ectopic lipid accumulation in muscle and liver seemingly predisposes to insulin resistance and dyslipidemia
Underlying Risk Factors• The adipose tissue of obesity exhibits abnormalities in the production of several adipokines that may separately affect insulin resistance and/or modify risk for ASCVD
• These includes• Inflammatory cytokines
• Plasminogen activator inhibitor-1 and
• Other bioactive products
Underlying Risk Factors
• At the same time the potentially protective adipokine, adiponectin, is reduced
• These responses appear to heighten the connection between obesity and inflammation
• Insulin-resistant people manifest evidence of low-grade inflammation even without an increase of total body fat
Therapeutic Goals and Recommendations for Clinical Management of Metabolic Syndrome↓weight by 7-10% during year 1 of therapy. Continue weight
loss with goal to ultimately achieve desirable weight
(BMI <25 kg/m2)
Reduced intake of saturated fat, trans
fat, cholesterol
For IFG, delay progression to type 2
DM. For diabetes,HbA1C
<7.0%
Regular moderate-intensity physical activity;
at least 30 min of continuous or intermittent (and preferably >60 min) 5 d/wk, but preferably daily
Reduce BP to at least achieve BP of
<140/90 mm Hg (or <130/80 mm Hg if diabetes present
Reduce thrombotic and fibrinolytic risk factors, initiate low dose aspirin and or
clopidogrel
Therapeutic Goals and Recommendations for Clinical Management of Metabolic Syndrome
Control of Lipid Profile
Life style modification and
Drugs (Statins, Fibrates, Niacin etc)
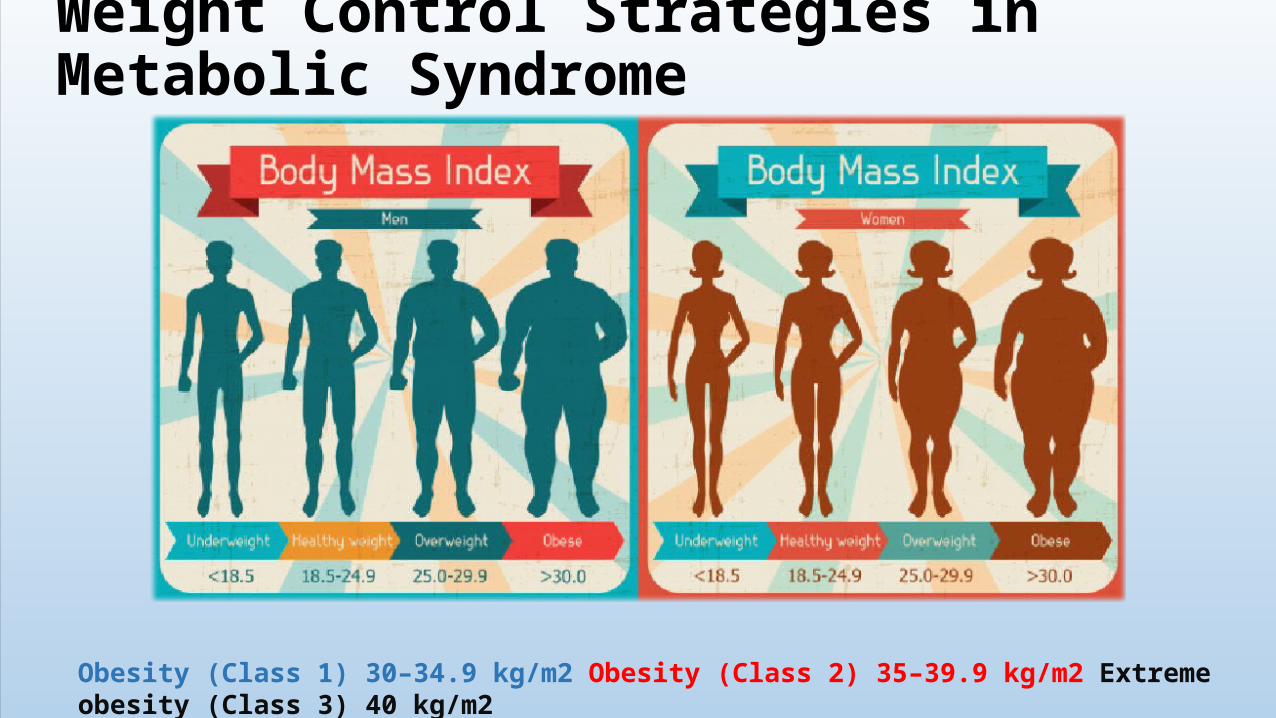
Weight Control Strategies in Metabolic Syndrome
Obesity (Class 1) 30–34.9 kg/m2 Obesity (Class 2) 35–39.9 kg/m2 Extreme obesity (Class 3) 40 kg/m2
What are the Long-Term Deleterious Health Impacts
of Severe Obesity
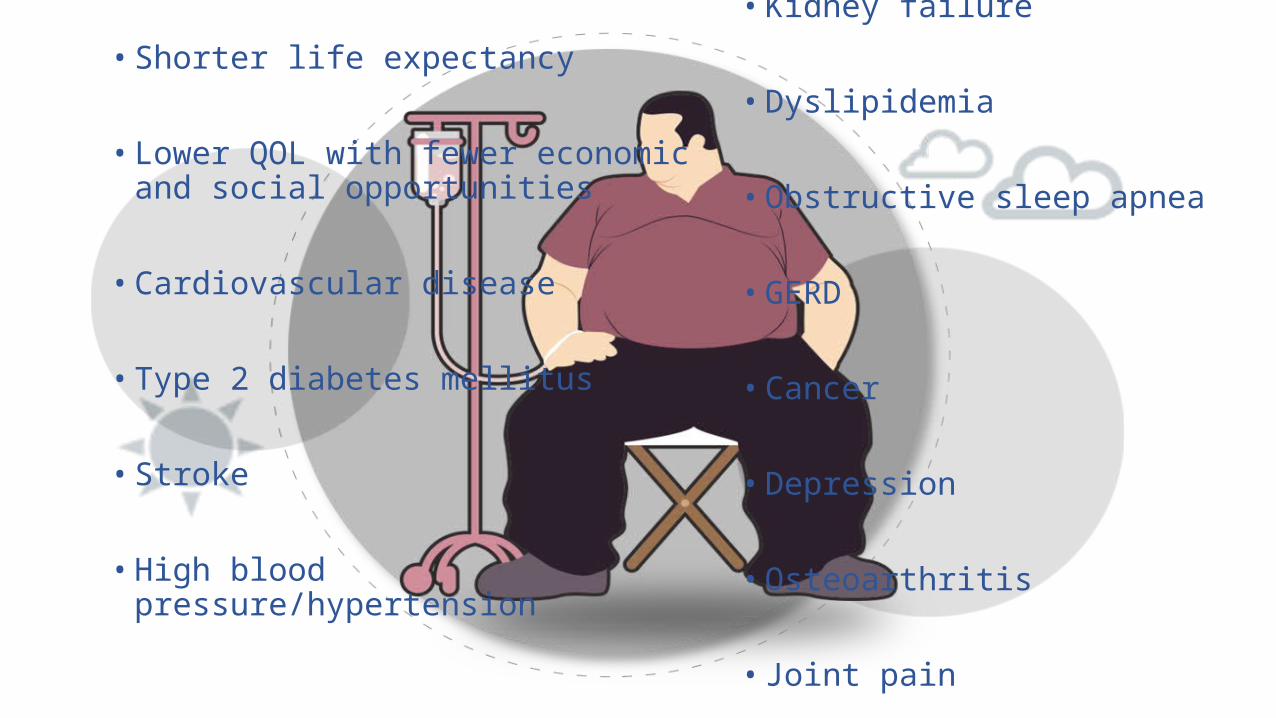
• Shorter life expectancy
• Lower QOL with fewer economic and social opportunities
• Cardiovascular disease
• Type 2 diabetes mellitus
• Stroke
• High blood pressure/hypertension
• Kidney failure
• Dyslipidemia
• Obstructive sleep apnea
• GERD
• Cancer
• Depression
• Osteoarthritis
• Joint pain
Is the patient ready and motivated to lose weight? Evaluation of readiness should include the following:• Reasons and motivation for weight loss,
• Previous attempts at weight loss,
• Support expected from family, friends and foes
• Understanding of risks and benefits,
• Attitudes toward physical activity,
• Time availability
• Potential barriers to the patient’s adoption of change
Goals of therapy• Reduce weight and maintain it for the long term
• The prevention of further weight gain should be the minimum goal
• An initial weight loss of 10 % of body weight achieved over 6 months is a recommended target
• The rate of weight loss should be 1 to 2 pounds per week

Goals of therapy• Greater rates of weight loss do not achieve better long-term results
• After the first 6 months of weight loss therapy, the priority should be weight maintenance achieved through combined changes in diet, physical activity, and behavior
• Further weight loss can be considered after a period of weight maintenance

Dietary Therapy• Caloric intake should be reduced by 500 - 1,000 calories/day from the
current level this will produce the recommended weight loss of 1-2 pounds per week
• The diet should be, but not too low in calories(less than 800 kcal/day)
• In general, diets containing 1,000 to 1,200 kcal/day should be selected for most women
• A diet between 1,200 and 1,600 kcal/day should be chosen for men or women whose wt > 165 pounds or more, or who exercise regularly
Dietary Therapy
• If the patient can stick with the 1,600 kcal/day diet but does not lose weight then switch 1,200 kcal/day diet
• If a patient on either diet is hungry, you may want to increase the calories by 100 to 200 per day
• Although dietary fat is a rich source of calories, reducing dietary fat without reducing calories will not produce weight loss
Physical Activity• The current recommendation is for patients to perform regular
moderate-intensity physical activity for at least 30 minutes continuously at least 5 days per week (ideally, 7 days per week)
• Achieving moderate intensity activity for 120 to 150 minutes a week may reduce the risk of developing metabolic syndrome
• Among patients who already have metabolic syndrome, physical activity correlates with a much lower (about 50%) risk of developing coronary heart disease
Pharmacologic TherapyCorrection of LDL-C and HDL-C levels• Management of elevated LDL-C includes consideration of all statins at
all indicated ranges.
• The choice of drug and dose should be individualized to the patient and titrated to achieve guideline-recommended goals
• Management of reduced HDL-C remains controversial, but starts with diet/exercise modifications and may include niacin
Pharmacologic TherapyCorrection of LDL-C and HDL-C levels
• Fibrate therapy may be considered for elevated triglyceride and low HDL-C levels
• Niacin raises low HDL-C levels and reduces cardiovascular events but may exacerbate hyperglycemia, especially in high doses (>1500 mg/day)

Pharmacologic Therapy pills pic• Drugs approved for reducing weight
• Orlistat
• Indications: • BMI>30
• >27 if concomitant risk factors exist
• When life style changes of 6 months did not promote weight loss

Behavior TherapyStrategies, that provide tools for overcoming barriers to compliance with dietary therapy and/or increased physical activity are helpful in achieving weight loss and weight maintenance
Specific strategies include
• self-monitoring of both eating habits and physical activity,• stress management,• stimulus control,• problem solving,• contingency management,• cognitive restructuring, and• social support
Surgery• Weight loss surgery should be reserved for patients in whom efforts at
medical therapy have failed and who are suffering from the complications of extreme obesity
• GI surgery (gastric restriction [vertical or gastric bypass) is an intervention weight loss option for motivated subjects with acceptable operative risks
• An integrated program must be in place to provide guidance on diet, physical activity, and behavioral and social support both prior to and after the surgery
Surgery• Surgery is an option for the following patients: • BMIs >= 40• >= 35 with comorbid conditions
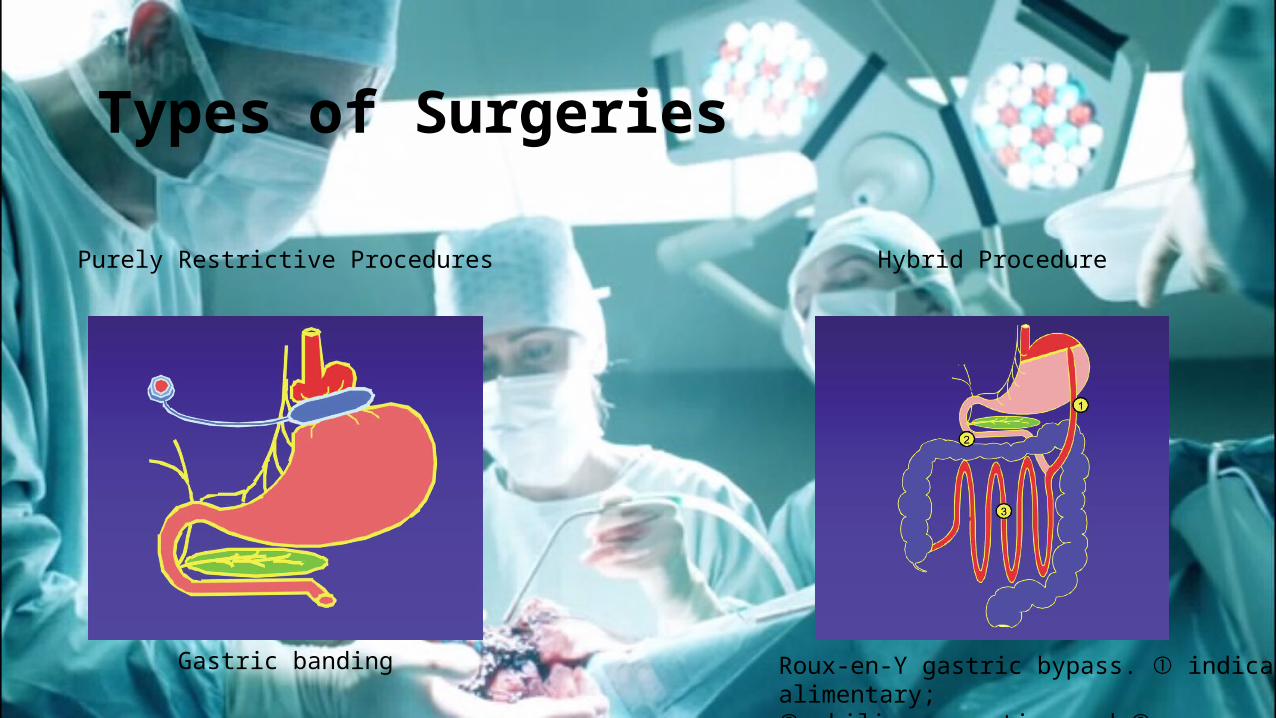
Types of Surgeries
Gastric banding
Purely Restrictive Procedures Hybrid Procedure
Roux-en-Y gastric bypass. indicates alimentary;➀➁, biliopancreatic; and , common➂
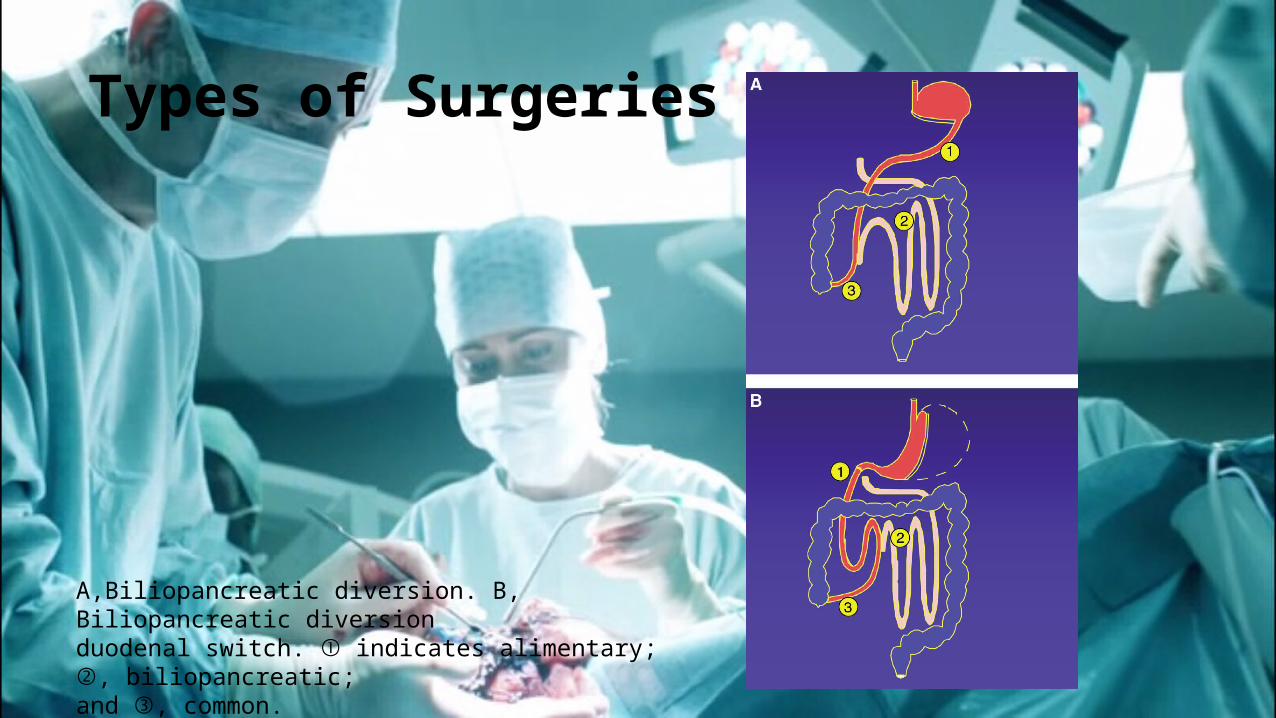
Types of Surgeries
A,Biliopancreatic diversion. B, Biliopancreatic diversionduodenal switch. indicates alimentary; , biliopancreatic;➀ ➁and , common.➂
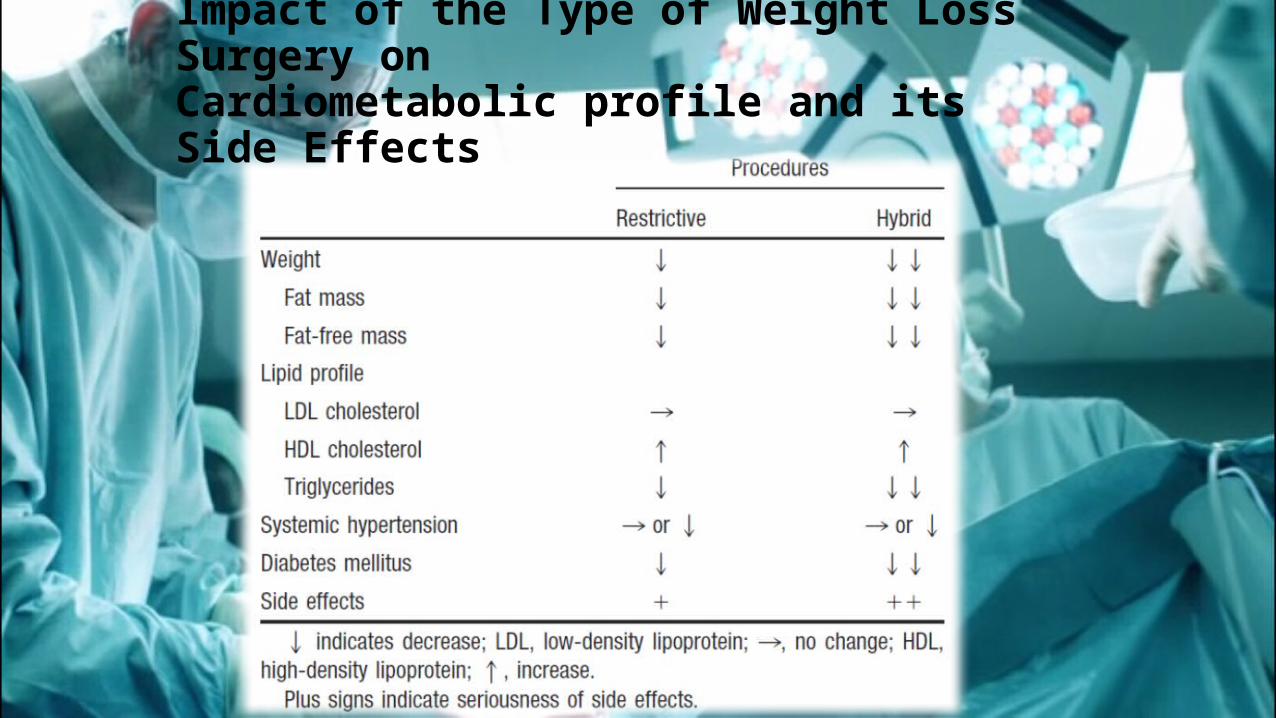
Impact of the Type of Weight Loss Surgery onCardiometabolic profile and its Side Effects

Early ComplicationsThe severely obese patient is at risk of developing several general complications. They include
• thromboembolism (1%)
• pulmonary or respiratory insufficiency (<1%)
• hemorrhage(1%)
• peritonitis (1%)
• wound infection (2%)
Late Complications• Gastric obstruction and band “slippage,” occurs in restrictive surgeries• Gastric obstruction associated with gastric bypass or sleeve gastrectomy is due to stenosis of
the gastric outlet secondary to scar tissue and may be treated with endoscopic dilation• Marginal ulceration between the stomach pouch and the small intestine after gastric bypass
surgery is relatively rare but when present is a frequent source of abdominal pain and anemia• Incisional hernias• Device-related complications with the gastric band include malfunction of the band, tubing, or
reservoir component• Hypoglycemia has been reported after gastric bypass and can typically be managed
successfully with diet modulations• Steatorrhea, diarrhea, and bacterial overgrowth are more common with malabsorptive
procedures than gastric banding
Effects of Bariatric Surgery on Metabolic Syndrome
• Bariatric surgery provides the greatest sustainable weight loss
• An average weight loss of 50% of excess weight at 5 years may be considered a success
• An average percent excess body weight loss of 61% is accompanied by improvements in type 2 diabetes mellitus, systemic hypertension, obstructive sleep apnea, and dyslipidemia
• Bariatric surgical procedures have also been shown to be effective in reversing the prevalence of the metabolic syndrome or the insulin resistance syndrome
Effects of Bariatric Surgery on Metabolic Syndrome
• Surgery results in significant improvements in circulating lipid concentrations and dyslipidemia
• TG levels are consistently reduced both immediately and after long-term follow-up. Greater impacts are seen after RYGB, with reductions of up to 50% to 60%, in contrast to gastric procedures, in which triglyceride levels are reduced by only 16% to 25%
• Most studies have also shown a significant increase in HDL cholesterol (13% to 47%) after weight loss surgery
• Moderate diet-induced weight loss (10% body weight) decreases liver fat content and improves liver biochemistries
• Weight loss induced by bariatric surgery can decrease steatosis, inflammation, and fibrosis and may reverse cirrhosis
• A meta analysis showed, obstructive sleep apnea improvement by 80%
• Results are most often reported as improvements in symptoms associated with sleep apnea such as snoring and daytime sleepiness or with polysomnogram reports at 6 to 18 months after a given surgical procedure
Effects of Bariatric Surgery on Metabolic Syndrome
• Weight loss has beneficial impacts on functional and structural cardiac status. Indeed, weight loss as little as 8 kg can be associated with a significant decrease in left ventricular mass
• In bariatric surgery, improvements in left ventricular systolic function occur mainly in severely obese individuals whose systolic function was significantly depressed preoperatively
• Bariatric surgery also has been associated with clinically significant improvement in left ventricular systolic function in patients with severe cardiomyopathy such as patients awaiting heart transplantation
Effects of Bariatric Surgery on Metabolic Syndrome
Metabolic Syndrom
Diet
Exercise
Drugs
Surgery
Thank You