Record Keeping – Foresight not Hindsight Trevor Warburton ... · Record Keeping – Foresight not...
24
Record Keeping – Foresight not Hindsight Trevor Warburton BSc FCOptom May 2009 Presentation handout www.tjwarburton.co.uk/records.pdf AOP Web Site (under GOS and Regulatory matters) www.aop.org.uk For flashes and floaters: www.aop.org.uk/uploaded_files/flashes_and_floaters_px_info_sheet_final_jan053.pdf For Freedom of Information follow GOS then FoI College of Optometrists (under guidance) www.college-optometrists.org For Flashes and Floaters see other guidance in members area GOC for legislation information (under legislation) www.optical.org Litigation & Record Keeping – Optometry Today Aug 04 www.optometry.co.uk/articles/docs/760e139e9b05f7cd8f0a893c6253eb1a_warburton2 0040820.pdf Staying out of trouble – Will your record keeping help or hinder - Nov 08 www.optometry.co.uk/articles/docs/RecordKeepingWARBURTON.pdf Stockport LOC (for patient information sheets) www.stockportloc.co.uk http://www.stockportloc.co.uk/documents/gos18.exe TJW Freedom of Information publication scheme www.tjwarburton.co.uk/tjwfoi.pdf Data Protection and FoI www.informationcommissioner.gov.uk
Transcript of Record Keeping – Foresight not Hindsight Trevor Warburton ... · Record Keeping – Foresight not...

Record Keeping – Foresight not Hindsight Trevor Warburton BSc FCOptom
May 2009
Presentation handout
www.tjwarburton.co.uk/records.pdf
AOP Web Site (under GOS and Regulatory matters)
www.aop.org.uk
For flashes and floaters:
www.aop.org.uk/uploaded_files/flashes_and_floaters_px_info_sheet_final_jan053.pdf
For Freedom of Information follow GOS then FoI
College of Optometrists (under guidance) www.college-optometrists.org
For Flashes and Floaters see other guidance in members area
GOC for legislation information (under legislation) www.optical.org
Litigation & Record Keeping – Optometry Today Aug 04 www.optometry.co.uk/articles/docs/760e139e9b05f7cd8f0a893c6253eb1a_warburton20040820.pdf
Staying out of trouble – Will your record keeping help or hinder - Nov 08
www.optometry.co.uk/articles/docs/RecordKeepingWARBURTON.pdf
Stockport LOC (for patient information sheets) www.stockportloc.co.ukhttp://www.stockportloc.co.uk/documents/gos18.exe
TJW Freedom of Information publication scheme
www.tjwarburton.co.uk/tjwfoi.pdf
Data Protection and FoI
www.informationcommissioner.gov.uk

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 1
Record Keeping
• Why keep records?
• Rules and Regulations
• Some principles
• Some examples
• Related issues
Why bother?
• Good clinical practice
• Aids future care of the patient
Monitors trends
• Can provide DEFENCE when
things go wrong
Why bother?
• College Guidelines Section 35:
The optometrist has a duty to
ensure that he keeps complete and
legible records of the patients
under his care.
• GOC cases show:
Failure to keep adequate records
may constitute SPM
Rules and Regs
• The Opticians Act 1989
• GOC Rules
• GOS Contract
Similar to previous regs
• Common Law Duty of Care
• Guidelines
The Sight Test
• Opticians Act
refraction with the intent to prescribe
• Sight Test Regs 1989
SI 1989 No 1230…
…when a doctor or optician tests the sight of another person, it shall be his duty: –
(a) to perform, for the purpose of detecting signs of injury, disease or abnormality in the eye or elsewhere –
(i) an examination of the external surface of the eye and its immediate vicinity,
(ii) an intra-ocular examination, either by means of an ophthalmoscope or by such other means as the doctor or optician considers appropriate
(iii) such additional examinations as appear to the doctor or optician to be clinically necessary;
The Sight Test

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 2
The Sight Test
• No internal examination?
• No external examination?
• One eye…?
GOS Regs
• E.g. to notify the GP after seeing a
patient with
Diabetes
Glaucoma
GOS Regs
• To refer
to an ophthalmic hospital
to the GP
Inform the GP that he has done so
Give the Px a written statement he has
done so
• with details of the referral
GOC Rules
• On referral for instance
Updated in 1999, amended in 2005
Allow for discretion on referral
Allow for referral via booking centres
Require a record of referral to be kept
Require a written report
With booking centres, the urgency of the
case to be indicated
Common Law
• Duty of Care
A practitioner should provide the same
standard of care as that offered in a
similar set of circumstances by a
reasonably competent optometrist
possessing up to date skills.
i.e. The peer viewMay or may not be the same as guidelines
Litigation
• Civil Cases
AOP deals with hundreds
annually
• GOC in 2006/07
129 referred to GOC
22 progressed to full hearing
Your records may be your
best defence

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 3
The Sight Test
• Opticians Act
refraction with the intent to prescribe
• Sight Test Regs 1989
SI 1989 No 1230…
Trends
• Cases referred
0
10
20
30
40
50
60
70
1998 1999 2000 2001 2002 2003 2004
No. cases
• Cases on the books at
AOP
Currently in excess of 1,000
~ 10,700 contracted to GOS
~ 9% or 1 in 11
Trends Trends
GOC
•• OCCSOCCS
•• Investigating CommitteeInvestigating Committee
•• FTP PanelFTP Panel
• Key to a successful defence The right actions
A good record of those actions
• Fully addresses the presenting
symptoms
• Details your investigations
Litigation

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 4
www.aop.org.uk/uploaded_files/pdf/appendix1.pdf
Normal sight test
procedures
• ocular Hx and symptoms
• Best spectacle correction and VA
• basic BV assessment
• external ocular examination
• intra-ocular examination through undilated pupil
• basic field screening for patients judged at risk by the optometrist
• tonometry for patients judged at risk of glaucoma by the optometrist
• maintaining records that show the results of the sight test
• issuing the prescription or statement
• giving verbal advice
• writing a referral letter, if required.
Principles
• Record everything you do
and do everything you record!
• Spot “out of the ordinary” cases
Go the extra mile on recording
• Think defensively
How would this look if…?
• Consider recording findings which prove:
You looked / investigated
You considered alternatives
Principles
• Record
What the patient said
What you said and did
What you found
What you didn’t find!
Your conclusions
Your advice
• Patients have selective memories
• Symptoms become clearer with every
professional they see!!
Principles
• Test your own records
• Select a random record
Why did the patient present?
What did you do and not do?
What was your advice?
Would you be comfortable defending your
actions if you were challenged?
Not
comfortable Comfortable
Can fully
justify
Reason for visit
Past history
Vocational requirements
BV
Refraction
Int & Ext Ocular health
Other investigations
Advice given
Handwriting
Principles Principles
• A record from my practice
(not mine!)
• Compare your own records
A few years ago with now
Most people find they are writing
more now

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 5
11
22
33
44
55
66
77
How not to do it - 2!
Principles
• Keep notes of other Px interactions
Advice by phone
Advice in the waiting room
Give advice in writing if necessary
• And record the fact
Document all dispensing and repairs
Keep it legible!
Tell the patient
I wasn’t told…..
• Common complaint
OPH
R
L
Shorthand
• NAD
not actually done
• ! or
Means what, exactly?!
!
Shorthand
• NAD
not actually done
• ! or
Means what, exactly?!
!
PUPILS
(tick to agree)
DCA, all 3 OK!

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 6
Shorthand
• NAD
not actually done
• ! or
Means what, exactly?
PUPILS
DCA, all 3 OK: Y / N
The abnormal…
• An example that should keep you safe
Not typical
Well above average standard
Not many seen by the AOP are like this

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 7
Record features
Photos?Photos?
Do you need to write Do you need to write
detail as well?detail as well?
Oph.
IA01662ep3
Records
Oph.
R Post. Pole:
CD 0.4
Inf Disc haem
halo of ppa
A/V: 2/3
Early dry pigmentary macchanges
Records
• We hear complaints about this
“How can I be expected to record all
this?”
“I don’t have time”
• Quote from a letter in Optician
“…we are faced with the threat of a year or
more of the totally ghastly, life-changing
experience of a full hearing…”
The Future
• PEARS
• Therapeutics
• Prescribing
• Record what it’s not!

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 8
Record reasons
• You may be wrong in the end!
• But the decision was correct at the time
• Based on the information available
“Normal” record
• No such thing
• Record of a straightforward Px
Records all findings of investigations
relevant to the presenting symptoms
Another situation
My GP said to see you…
I can see OK
It’s not sore
It looks a mess
• “My eye was all red this morning”

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 9
Nothing is a common optionNothing is a common option
What to record?
c/o red eye from this am. Sent by GP.
No pain or discomfort. Vision OK
Explained this is sub-conj haem. Will
clear in a week or 2. If it doesn’t, or if
any discomfort, see me or GP.
VA: R 6/6 L 6/6 (as previous)
IOP: R 15 L 16 (as previous)
See pic IA0xxx
For CL wearer: Cornea Clear, no stain.
Where to record?
• For an existing patient
On their record
• For a new patient
Create a record
• or as a minimum…
Make a note in a day book
• Px name
• Brief advice
Tonometry
• Record the time of the reading
Saved one domiciliary
practitioner
• Consider recording
the type of drops
GOC critical of one
practitioner for not
doing so
Visual Fields
• If you don’t keep
the plot
Note thresholds
Type of plot
• 26pt MSST
• 26pt SSST
• 24/2
• etc
Store electronically...
• Complete EPR
• If your screener can output images
Hensons can
Humphreys can
• If you have imaging software…

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 10
Backup
• Vital for safety of your data
• Somewhere in the world
A hard drive crashes every 15 secs
• 31% of PC users have lost all data
• Lifetime failure rate for hard drives is
100%
They all fail eventually…
Backup
• Make regular backups
• Take them off site
• Keep them safe and secure
• Check the backup is working…
Online
Online
My system backup
DatabaseDatabase
ArchiveArchive
Mirrored DrivesMirrored Drives

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 11
Referral Letters
• These form part of your record
• They may provide more detail than
your record
• Make sure they don’t get lost
• Make them legible
• Illegible
• No DoB
• ? Glaucoma
No VF
No Disc
appearance
No reason?
• No practice name
• No address
• No practitioner
• Typed
• Word processed
www.stockportloc.co.uk/pub/gos18.exe
Urgent Referrals
• Where are they going?
• Who did you speak to?
• Note it on the record and/or on the
referral letter
• Send the letter with the patient (or fax
in advance)

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 12
A Case
• Age 56; Laser for hyperopia
• Still low plus, ST & specs supplied
• 9 month later, complains:
Poor vision
Went elsewhere, Rx Changed
Wants refund….
• Records are poor!!
How long to keep
them?
• Limitation period
3yrs from the point of realising
a negligent act has occurred
How long to keep
them?
Identified 2 years later, advanced
Treated for 3 years, unsuccessfully
Deteriorates further for a year or so
Registered blind
Someone says:
• “what about when you saw that
optician?”
8 years on you get a letter…..
• Suppose you missed STR
How long to keep
them?
• Not long enough…!
• GOS Regs
7 years
• AOP advise:
10 years for adults
Children till they are 26
• And it is 10 years since you last saw them
The deceased for 10 years
• If your employer destroys them sooner
It may be you that suffers
How long to keep
them?

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 13
• Treat appointment diaries as records
Patients get confused about where they
went
• If you are accused
And you can’t find a record
• You may have a problem
If the diary and your records show you
were seeing other patients
• You may be home and dry
How long to keep
them?
• What if a practice changes hands?
• In the contract of sale
Require the records to be maintained
safely
Allow access in the event of a claim
How long to keep
them?
Rx & CL Spec.
• Legal requirement to provide
Rx following a sight test
CL Spec. following fitting and check-ups
• CL Specification
Name & address of patient
Name and Reg No. of practitioner
Practice address
Date fitting was completed
Expiry date
Sufficient details to allow replication
CL Supply
• AOP & College view of aftercare
Basic advice
• On lens care
• The need for routine professional care
• Contact details for emergency care
• Supplier must arrange “aftercare”
“in so far as, and for so long as, may be
reasonable in the particular case”
• I provide at annual check-up
• Make a note on the record
• Care & advice leaflets
• Make a virtue of providing the specification

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 14
• Make a virtue of providing the specification
Data Protection
• Register with Information
Commissioner if:
Any personal data is held on computer
• Or could be
• E.g. field screener that could store records
Data Protection
• Patient is entitled to:
Copy of record
Explanation of record
• You may charge
Up to £10 for electronic information• Even if supplied as hard copy
Up to £50 for access to manual records• Where hard copies are provided
Data Protection
• Do you need consent to keep a record?
Not written at present
Legal advice says note verbal consent on record
But doesn’t Px consent by being there…?
• If you take data off site
Protect it !!!
Encryption / password protection
Don’t leave it in the car
Freedom of
Information
• Statement of available information
About the practice
The practitioners
Service provided
Complaints procedures
NHS fees
Data protection
Charges for information
Freedom of
Information
• 31st October 2003
Publication scheme in place
• Saying how information is to be made
available
• 1st January, 2005
Public can request the information

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
May 2009 15
Freedom of
Information
Just complete
the blanks
Keep handy to
supply if
requested
Complaints
• In the event of a complaint
• CONTACT YOUR INSURERS IMMEDIATELY
• Most policies only respond if you have
notified insurers of a potential claim
• DO NOT ADOPT THE OSTRICH APPROACH
Insurance
• Professional Indemnity
Cover against being sued
• Defence Cover
For the GOC
Insurance
Covers claims where original incident occurred during the period of cover
• Common in larger companies
• Probably does not cover work outside company
• Insurance cover for that period lasts for ever (but maybe not for GOC)
• Does not cover incidents prior to period of cover
• May be possible to buy “run-on” cover
• Claims occurring cover
Insurance
Covers claims made during the period of cover
Common personal cover (AOP)
Covers all periods prior to commencing cover
No cover when insurance ceases
Need to maintain cover during periods off work
Buy run-off insurance on retirement
• Claims made cover
Mr A Age 70 April 2003 Mr A Age 68 April 2001
Remember…• How will it look?

Record Keeping – Foresight not Hindsight
Trevor Warburton BSc FCOptom
June 2008 16
Resources
AOP Web Site (under GOS and Regulatory matters)
www.aop.org.uk
For flashes and floaters:
www.aop.org.uk/uploaded_files/flashes_and_floaters_px_info_sheet_final_jan053.pdf
For Freedom of Information follow GOS then FoI
College of Optometrists (under guidance)
www.college-optometrists.org
For Flashes and Floaters see other guidance in members area
GOC for legislation information (under legislation)
www.optical.org
Stockport LOC (for patient information sheets)
www.stockportloc.co.uk
www.stockportloc.co.uk/pub/gos18.exe
Litigation & Record Keeping – Optometry Today Aug 04
www.optometry.co.uk/articles/docs/760e139e9b05f7cd8f0a893c6253eb1a_warburton20040820.pdf
TJW Freedom of Information publication scheme
www.tjwarburton.co.uk/tjwfoi.pdf
Data Protection and FoI
www.informationcommissioner.gov.uk

Membership of the Association ofOptometrists (AOP) provides acomprehensive package of professionalindemnity insurance against claims fordamages and an in-house legal team, whichprovides advice and defence in disciplinarycases. Costs in GOC disciplinary cases canbe in excess of £20,000, so if you insureelsewhere, make sure you read the smallprint and know what you are covered for.Some policies require that you adhere toparticular guidelines and keepcomprehensive records in order tomaintain cover. If a claim crops up relatingto a patient you saw five years ago, can yoube sure the record will be comprehensive?Can you rely purely on an employer’sinsurance, rather than maintainingpersonal insurance cover? The answer is– it depends.
In a civil case, the patient will suewhoever has the deepest pockets. This islikely to be a company rather than anindividual. In defending itself, thecompany will have to defend the actionsof the optometrist, but even where the
Communication
individual is not at fault, the company’sinsurer may choose to settle the claim early,possibly admitting negligence, in order toavoid the greater costs of lengthy litigation.But look at a different scenario; theoptometrist does something the companyregards as unacceptable. The company takesdisciplinary action against the optometristconcerned, which may lead to dismissal. Ifthe matter is then reported to the GOC, thecompany has no reason to assist, so theoptometrist is now on their own. This iswhen personal insurance and defence coveris required. It may be unlikely, but that isthe point of insurance.
The AOP deals with hundreds of caseseach year, both civil and disciplinary. Manycan be dealt with at an early stage andprevented from progressing to courts or atribunal. Of the 59 cases referred to theGOC in the year to September 2003, 45were investigated and, after submissions bythe AOP on behalf of the practitionerinvolved, did not proceed to a disciplinaryhearing. The remainder required defendingat a full hearing. What is clear is that one of
We live in an increasingly litigious age in which consumers areencouraged to expect the highest standards, and to complainif they are not delivered – optometry is no exception.
Practitioners may find that they are asked to account for theiractions by various different bodies, including the Optical ConsumerComplaints Service (OCCS), the small claims court, higher-level courtsand the General Optical Council (GOC).
Trevor Warburton BSc, FCOptom
20 | August 20 | 2004 OT
the keys to a successful defence is goodrecord keeping. Whilst this is a mantra thathas been heard time and time again,practitioners can still be heard complainingalong the lines of, “How do they expect usto find the time to write all this down?”
So although keeping thorough records isobviously good clinical practice, there isanother entirely selfish reason for it;namely self-defence. As any practitionerwho has been involved in a GOC hearingwill testify, extra time spent completingrecords is a small price to pay. Whilstthorough and appropriate clinicalinvestigations are obviously a necessity forall patients, a good record of thoseinvestigations increases the likelihood thatthe GOC Investigating Committee will notproceed with a hearing and, if it does,improves the chances of a successfuldefence.
Notification of GOC proceedings bringswith it over 12 months of stress, anxietyand uncertainty, with the possibility oferasure from the Register and loss of yourlivelihood. To quote from a recent letter toOT (12/03/04): “…we are faced with thethreat of a year or more of the totally ghastly,life-changing experience of a full hearing…”.The strain that this puts on the practitionerand their family cannot beover-emphasised. Do not be the nextpractitioner to experience years of stressand strain. At the very least, ensure thatyour records will provide you with afighting chance of a good defence.
What is a ‘good record’?A good record involves writing down whatthe patient said, what you said to thepatient, what you did, what you found,what you did not find and yourconclusions, including your advice. Youshould think defensively, particularly inunusual cases. Ask yourself how the casewill look if anyone questions you about it.If your record shows an increase in CDratio from 0:2 last time, to 0:4 this time,and IOP from 14mmHg to 19mmHg, youmay well think it all still looks normal, butjust suppose it isn’t? If you have notchecked the visual fields you have no proofthat there was no field loss at the time ofthe second examination and so will havemore difficulty defending your actions. Thecourts and the GOC will not be interestedin who might be paying for theseprocedures, only in the fact that you didn’tdo them.
Try selecting a record at random fromnine or 12 months ago. Ask yourself if youcan tell why the patient presented to you.What did you do? What didn’t you do?
Litigation and record keepingBetter to be safe than sorry
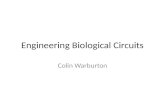
Figure 1
Sample patient record card

Communication Trevor Warburton BSc, FCOptom
22 | August 20 | 2004 OT
What advice did you give? Would you feelcomfortable defending your actions if youwere challenged?
Figure 1 shows a sample patient recordcard which would be regarded by the AOPlegal department as being an above averageexample. We can see the patient attendedbecause of a floater but had no lightflashes. He is a driver, is not diabetic, hasno previous ocular history and no familyhistory. Pupils were dilated with 1.0%tropicamide and an information card wasgiven explaining the rare side effects ofmydriatics. There are minor lens opacitiesin the right eye and none in the left. Theposterior pole was examined with a VolkSuper 66 and the maculae were flat. Theperiphery was examined with a Volk SuperVitreo Fundus lens and there were no signsof holes or tears. Pupil reactions werenormal; the AV ratio was 2/3 with nonipping; CD ratio is noted and the cupswere round and central. Fundus photoswere taken and the record number isnoted. Slit lamp examination of theanterior vitreous showed no sign ofpigment cells (tobacco dust). Visual fieldswere normal with a 26pt single stimulussupra threshold test and the thresholds arenoted. This field plot is filed electronicallyand the reference number is given. IOPs arenoted with the time, although a criticismmight be the lack of any indication ofmultiple readings.
The conclusion is that the patient hashad a posterior vitreous detachment. Hehas been warned of further symptoms ofretinal detachment and given a flashes andfloaters leaflet that explains this. Hisdriving licence has been seen as evidenceof age for the Point of Service check and isnoted for the future. His spectacles do notrequire change.
Negative findings can be just asimportant as positive ones. Consider the
situation above of examining theperipheral retina. A note of the mydriaticdrop used will establish that you dilated ifyou felt this necessary. The type ofophthalmoscope will demonstrate howgood the view was likely to be. Even thetype of fundus lens used, since a Volk‘Super Vitreo Fundus’ lens will give a muchbetter view of the periphery than, say, a78D lens. The statement, “Peripheral retinaappears healthy, no sign of holes, tears orbreaks”, establishes not only that you foundnothing abnormal, but also that you knewwhat you were looking for, as does, “slitlamp – no sign of pigment cells in the anteriorvitreous”. Not writing this down, or notusing these techniques, does not of itselfmean you are not taking reasonable care,but keeping a definite record does make itmuch more likely that any complaint willnever progress to further action.
Some aspects of record keeping can bereduced to circling the appropriate option,providing it is clear what this means. So“Media 3”, means absolutely nothing, butthe statement “Media clear?” followed by“Y/N” options, which can be circled, makethe meaning clear. Again, this allows forrecording both positive and negativefindings, although findings such as “Medianot clear” should have an accompanyingexplanation.
Not all patients will require as manyinvestigations as this one and, if the test isNHS, you can charge if you feel thatinvestigations are outside the remit ofGeneral Ophthalmic Services (GOS), solong as you have completed your GOSobligations.
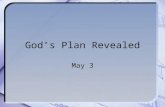
In addition to recording your findingsduring the consultation, make notes ofother interactions with the patient – even ifthese were on other occasions and notassociated with a sight test or eyeexamination. If you give advice, either inthe waiting room, or by phone, write it onthe record and date it. Where appropriate,it is useful to give advice to patients inwriting, making the usual note on therecord. Pre-prepared information sheets ona variety of conditions leave no doubt as tothe advice given to the patient (Figure 2).You should document all dispensing andrepairs. For example, never submit repairvouchers for children without a supportingentry on the record.
Sometimes, when a patient has somesymptoms, you may choose not to pursueadditional investigations. This could bebecause the investigations involveadditional cost and the patient does notwish to pay, or because your feel theinvestigations are inappropriate for somereason. In this case, you should ensure thatyour records document all the reasons foryour decision. If there is any risk that thesymptoms could relate to an immediatelysight-threatening condition, you shouldrefer the patient to A&E.
Always remember that you have a legal
obligation to supply a prescriptionfollowing a sight test, as well as a lensspecification for contact lens wearers. If youhave to re-check a patient shortly after atest, and find a refractive change, youshould remember to issue an amendedprescription.
The time factorIt can be many years after the event that apotential claim or disciplinary casebecomes apparent. Potential claimants havethree years after they first become aware ofthe right to claim in order to do so. In thecase of children, the three-year period doesnot start to run until they are 18.
Picture a case of missed potentiallysight-threatening retinopathy. It may beanother year or two before visual symptomsdrive the patient to seek help. There maythen follow a period of two or three yearsof treatment in the hope and belief that thesituation is retrievable. Furtherdeterioration may follow to eventualregistration of blindness. Someone nowsuggests to the patient that it is surprisingthat the condition was missed all thoseyears ago, so the patient starts to look intoit. Another year goes by and you arenotified of a claim against you for a patientyou last saw eight years ago. GOSregulations only require you to keeprecords for seven years. If you don’t havethe record you have no defence and thecourts will probably side with the patient.
So how long should you keep a record?The AOP recommends that for the purposeof defending negligence claims, the recordsof adult patients should be kept for 12years, and children’s records should beretained until they are both 25 years oldand it is 12 years since they were last seen.Records of the deceased should be kept for10 years. This advice is based in part onDepartment of Health recommendationsfor the minimum period clinical recordsshould be kept after the conclusion oftreatment. The College of Optometristsagrees with this. The Data Protection Actstipulates that data should not be keptlonger than is necessary. This is a balancingact, and is open to interpretation. Somepractices have a policy of destroying recordsafter as little as five years. You shouldremember it is the practitioner who willsuffer if they have no record to defendthemselves.
When a practice changes hands, orcloses, the records still require safe keeping.Just because the practice is closed does notmean a claim cannot arise some yearsdown the line. When a practice is sold itwould be wise to insert a clause requiringthe new owner (and any future owner) tomaintain the records safely, and to allowyou access in the event of any claim.
What should you do if you are anemployed or locum practitioner and youremployer holds the records? It would beworth asking for a written statement of the
Figure 2
Example of a patient information sheet

Communication
23 | August 20 | 2004 OT
policy regarding records and discussingthe matter if you are unhappy with theanswer. You need to ensure that you willbe able to obtain access to the records ifyou are called on to defend a claim, as itwill be your problem rather that youremployer’s (especially if a lay employer) ifthe records are not available in the eventof a claim or disciplinary action. Whilstaccess to the records should ultimately beavailable under section 35 of the DataProtection Act 1998, this is of no help ifthe records have been destroyed.
It is always worth regarding theappointment book as a record andtreating it the same way. Patientssometimes get confused about whichpractice they visited and when. Ifallegations are made against you, and youcannot find a record, you have a problem.If the appointment book shows that thepatient did not attend when they say theydid – indeed, shows that others attendedon that day and you do have their records– then you are in a much strongerposition.
ConclusionGenerally, in the event of a claim ordisciplinary case, you will be judgedagainst the standard of the averagereasonably competent practitioner. This isa moving feast, as standards change overtime. Thirty years ago, it was unusual tocheck IOPs; now it is the norm (althoughthe practitioner should only be judged bythe standards of a reasonable optometristthat were ‘in force’ at the time of theincident). The exception to this rule iswhere a practitioner claims a particularexpertise. So someone describingthemselves as a specialist paediatricoptometrist will be judged against theaverage, reasonably competent specialistpaediatric optometrist. How can you knowwhat is average? Attending peer reviewgroups is one excellent way of seeing howother practitioners practise, especially forthose practitioners who work alone.
Write down every event in every patientinteraction, whatever it is, at the time.Audit your own records from time to time,as if you were about to present them tothe GOC Disciplinary Committee. Bebrave enough to ask a colleague tocomment critically on how you areperforming in this vital area.
All of this may seem a pain when youare busy; it can seem much easier just towrite “NAD” (not actually done) butremember, the spare tyre in your car bootis a waste of space most of the time - untilyou need it!
About the authorTrevor Warburton is an AOP Director,Chairman of the AOP ProfessionalServices Committee and an independentpractitioner in Stockport.

20 | December 1 | 2006 OT
CLINICAL
Short clinical case record - a classic insight
Remember to carry out yourwork properly, or not at all
are called for than just a simple pressurecheck.
Mrs A accepted the argument and madean appointment to return for an eyeexamination.
At the examination it transpired that shehad been waking during the night withsevere pains in one or both eyes, morecommonly the left, for a couple of months.She was hypermetropic, with a smallprescription change producing acuities of R6/6 and L 6/6pt.
Intra ocular pressures were well withnormal range at R12 and L14 mmHg andher central visual fields showed no defects.Examination and photographs of the fundishowed moderately large disc cupping, butthese were round and central, with a healthneuro-retinal rim.
With the standard triad of tests all
Trevor Warburton BSc FCOptom, uses his experience ofdisciplinary cases and record keeping to remindpractitioners of an important message - that byanswering the necessary question in full, you helpyourself and your patient. You have a duty of care to thepatient which can be discharged either by seeing them, orby advising them to see someone else who is in a positionto make appropriate and timely investigations. If you dosee them yourself, you need to do a proper job. To doless can leave you vulnerable
Everyone will have had the patient whopresents telling you that their GP has askedfor a “quick pressure check”. Tempting as itmay be to simply perform tonometry, writedown the numbers and give them to thepatient to take back, this is not actually inanyone’s best interest, especially yours ifthings are not straightforward.
This was precisely the scenario when MrsA walked into the practice. She had neverbeen to us before, but clearly expected theprocess to take no more than a minute ortwo. As ever, we patiently explained thatthe question that the doctor was reallyasking was “does this patient haveglaucoma?”, and that they only asked forpressures because they don’t know whatelse to ask. We explained that manypatients with glaucoma have normalpressures and so rather more investigations
looking fairly normal, attention turned toslit lamp examination which revealed, apartfrom mild Blepharitis, stunningly narrowangles when judged by Van Herick –between grade 0 and grade 1. A series ofsub-acute or pro-dromal attacks of angleclosure seemed a possible explanation. Aletter was written to the GP advisingreferral to the eye clinic soon for assess-ment and possible provocative tests. Thepatient was advised that if an attackbecame severe they should attend theAccident and Emergency departmentimmediately.
The patient was seen in the eye clinicwithin two months and the diagnosisconfirmed. She was started on pilocarpineas a temporary measure and was listed forbilateral laser iridotomies “soon”.Interestingly, further questioning by theconsultant revealed the information that ifshe switched on the light during one of herattacks at night, the pain eased off.
This case demonstrates the generaladvice that you should either do thingsproperly, or not at all. The pressures wouldhave provided no useful information ontheir own. Indeed, they may haveerroneously led the GP to believe all waswell. Patients don’t ask about the serviceyou provide with contact lenses, they askabout the price because they don’t knowwhat other questions to ask. It is the samewith the GP, so when asked for pressures(or anything else), you need to readbetween the lines and decide what the realquestion is. Then either answer it in full, ornot at all.
• Trevor Warburton practises in Stockport,and is chairman of the AOP
Patient record card: It is vital to keep good records
Slit lamp examination: Revealedstunningly narrow angles when judged byVan Herick

40
28
/11/
08
RE
CO
RD
KE
EP
ING
By Trevor Warburton BSc FCOptom
Staying out of trouble – Will your record keeping help or hinder?
PRACTICE ADVICE
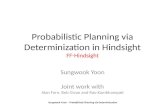
Sample record: This sample record uses the quick selection of Y/N for items with a definitive answer (e.g. driver?). It alsoallows for quick recording of routine advice and of any information given to the patient. Cataract is recorded on an arbitrarynumeric scale where 0 is clear and 5 is opaque. Ophthalmoscopy has written notes; there can be no doubt in this case thatthe retina was viewed and the macula was seen for both eyes and they were OK. The visual field result is recorded, but theplot has also been stored as an image in imaging software. Non-standard advice is clearly recorded.
There are all manner of circumstances which leadpatients to make complaints about a practitioner orpractice. Some have a genuine grievance, somemistakenly believe they have a genuine grievance and
a minority are simply vexatious complaints, with little realmerit.
I have written previously about the need for good recordkeeping (OT August 20 2004) and the article is still available inthe OT archives, and has recently been reproduced in theOptometry Red Book. If you receive a complaint, it is too late atthat point to think “I wish I had written down x, y or z”. Thisarticle will look at a few of the issues that cause patients tocomplain and consider what is required within the records toadequately defend the actions of the practitioner.
To begin with, it is worth understanding the potentiallyescalating pathway for patient complaints.
Generally they will complain first to the practice. If thiscomplaint is in any way about clinical performance you shouldimmediately consult your professional indemnity insurers.
They may also complain to the NHS locally. In some cases the
NHS will investigate and in others they will pass it on elsewhere(eg, the GOC). The patient may also complain to the OpticalConsumer Complaints Service (OCCS) or to the GOC directly. Ifthe complaint is about product, then the GOC will pass it toOCCS. If it appears to be about a clinical matter or professionalconduct, then the GOC Investigation Committee (IC) will look atthe case.
You should be aware that there is no such thing as a brief lookand dismissal of a case by the IC.
They will require copies of all paperwork and records relatingto the case from both sides. It will all take some time, creating anextended anxious period for the practitioner. The result mayultimately be the dismissal of the case, or referral to a Fitness toPractise (FTP) panel or, in some cases, the IC may ask for aperformance assessment, which is a relatively new addition.Some cases have gone to an FTP hearing where the charges bearno real relationship to the original patient complaint. Forinstance, the original complaint may have had no merit, but thecase brings to light poor record keeping, which then becomes thesubject of a hearing.

28
/11/
08
RE
CO
RD
KE
EP
ING
41
On the non-clinical side, problems of some sort withspectacles are the most common complaint and, thankfully,these are mostly dealt with effectively by the practice to thepatient’s satisfaction. Sometimes it simply needs adjustments tothe frame, or the prescription. On other occasions the patient justloses confidence and, rightly or wrongly, wants their moneyback. It is always worth remembering that if you leave a patientdissatisfied, then a few of them will find other ways to complain.If their complaint is dismissed by OCCS, a few savvy ones realisethat changing their complaint slightly to cast doubt on theclinical side means that the GOC will also look at it. Don’t leavea patient dissatisfied if you can possibly avoid it; refusing arefund can sometimes turn out be a very bad decision, so makethem early and amicably!
CataractStill a major cause of complaint clinically is a patient not beinginformed about some aspect of the condition of their eyes, withthe most common being cataract. It happens easily; the patientappears to have no symptoms or complaints; the vision isslightly down in one eye, say 6/6 down to 6/9+, and a smallamount of cataract is observed in the affected eye. It may seem areasonable decision to avoid worrying the patient by not tellingthem about the cataract. Suppose it later turns out that thepatient was concerned about the reduced vision but they simplydidn’t like to say so – they were waiting for you to raise thematter. So they go somewhere else a few months later and aretold “well, you have a bit of cataract in that eye”. Next thing youknow, you are on the receiving end of a letter of complaint. Thismay seem to be about a trivial matter, but it won’t seem trivial ifit ends up at the GOC.
How do you protect yourself against this situation? The firstpoint, obviously, is to always tell patients about conditions likecataract. The problem is; when is an ageing change in thecrystalline lens a cataract? Many would argue that, with dilation,you can find some degree of lens opacity in everyone over theage of 60. So when is an ageing change a cataract? A good guidefor this purpose is to call it a cataract when it is producing somenoticeable or measureable effect on the vision or is easily visibleto you. Earlier than that you may choose to refer to it as an ageingchange, but nevertheless it is good safe practice to record it andto tell the patient about it.
It may even be that the practitioner did explain it away as an“ageing change” without mentioning cataract, so the nextimportant point is to ensure that you document any explanationgiven to the patient on your record card, and that you have alsodocumented the cataract itself. So when the complaint is that “Iwasn’t told” or “that practitioner is incompetent because theydon’t know how to identify cataract”, your records will showotherwise. If you provide any written information to the patient,document that also.
Macular DegenerationAs far as civil claims go, it might be fair to say that wet maculardegeneration shows signs of being the new flashes and floaters.
Now that there are treatments available for wet AMD, there isalso the possibility of a claim if the patient believes it was notidentified early enough. The performance of Photo DynamicTherapy (PDT) as a treatment was always suspect. Even NICEsaid that, on average at 24 months, patients treated with PDThave just one line of vision more than those who received notreatment1.
Time marches on, and PDT has been replaced by anti-VEGfinjections which are proving to be more effective. This makes itever more important that wet AMD is identified and referred
effectively, and ever more likely that claims will arise where apatient believes it was not. This does present a challenge since,although wet AMD is a fairly sudden onset condition, a patientwho begins to notice effects a couple of weeks after a sight testmight start to wonder if it should have been spotted. Your recordneeds to show VA and, if this is worse than your previouslyrecorded findings, then there should be a reason (cataract is anobvious one). Ophthalmoscopy should have some indication thatthe macular area, or posterior pole, was normal.
If a patient, especially an elderly one, returns complaining ofdistortion with new spectacles, at least consider the possibilitythat it may not be the spectacles. Check the VA and show theman Amsler chart. Look at the fovea. Make a note of all these tests.Then change the varifocal type!
Dry macular degeneration is more difficult, but the risk of the“I wasn’t told” complaint is still there. Where vision is affected,some explanation to the patient is obviously required, but it ismore difficult in those patients who have a mass of soft confluentdrusen and some pigmentary changes, but no apparentdeterioration in vision. Unlike cataract, there is no consolation ofa potential treatment. It is reasonable to explain such signs asageing changes and it might be considered best practice toexplain that these changes carry a risk of affecting the vision,along with giving advice not to smoke and to protect the eyesfrom bright light. Opinions vary on the value of nutritionalsupplements, but the AREDS study2 suggests that their vitaminmix can potentially give a 25% reduction in progression fromintermediate to advanced AMD. If you do not feel comfortablediscussing nutritional supplements, consider giving the patientwritten information that points them or their family to theAREDS study on the internet.
A useful tip3 arising out of the AREDS study is a four- pointscale for assessing the risk of AMD progression. Count one pointfor large drusen of 125 microns or larger (about the size of a veinat the disc margin) and one point for any pigmentary change.Score each eye separately and then add them together for a scoreout of four. A full score of four points means a 50% chance ofprogressing to advanced AMD in the next five years. Three pointsgives a 25% chance, 20 points a 12% chance and with one pointthe risk is just 0.5%.
Never forget that patients with dry AMD can still develop wetAMD. Providing a home Amsler chart and instructions on its useis a good safeguard for both the patient and yourself(www.stockportloc.co.uk/pub/amsler_a5.pdf).
Retinal DetachmentFlashes and floaters are still out there and there has been plentyof information about good practice in dealing with them,including journal articles, College advice and an audiodiscussion in an issue of Optometric Quarterly. It is becomingvery difficult to defend actions that do not conform to goodpractice. With stable floaters over two months old you will needto make a judgement but, for more recent onset floaters or flashes,your record will need to show in addition to the normal findings:• Dilation• Examination of the vitreous with a slit lamp• Negative or positive findings of tobacco dust• Examination of the peripheral fundus with indirectophthalmoscopy• Advice and warnings given to the patient, preferably in writingDo not refer recent onset flashes or floaters, or suspect retinaltears, via the GP unless you have established that the GP will beable to make an immediate (within 24hours) referral to an eyedepartment. If you are unable to examine a patient with recentfloaters, remember that flashes and floaters should be treated as a
PRACTICE ADVICE

28
/11/
08
RE
CO
RD
KE
EP
ING
42
PRACTICE ADVICE
others to draw conclusions. Then if any questions are later raisedabout the referral, it is entirely clear why you were referring thepatient.
GOSPrimary care organisations monitor sight tests, vouchers and repairs looking for outliers. Who does more repairs thanaverage? Who does more early sight tests? There is nothing wrongwith being an outlier if your claims are valid. So long as all yourrepairs for children are documented there is nothing to worryabout. You may also be able to point out an obvious explanationsuch as being very close to the largest primary school in the area.Likewise, you may have acquired a reputation for problem solvingand dealing with difficult cases, so you tend to have more than theaverage number of patients presenting with symptoms orconcerns. This is fine; the important thing is that your recordclearly documents the reason or justification for the early sighttest, or for that tint or prism. It is wise to note early retest codes onthe record as well as on the GOS1 form so that you are quite clearabout your reasons.
RecordsIf you use any non-standard abbreviations in your records then you should keep a list of those abbreviations explaining theirmeaning. There is a useful list of standard abbreviations in theCollege Guidelines. If you have a number of optometrists in thepractice, or regularly use locums, then it is a good idea to makethat list available in each consulting room for every optometrist tosee.
So your records need to be a complete account of yourinteraction with the patient and they need to be capable ofjustifying the tests that you did or did not perform – and do keepthem legible! They are supposed to assist with continuity of care,so do ensure that those who see the patient after you can read therecord easily.
Finally; do unto others as you would have them do unto you.
Don’t criticise a colleague’s previous encounter with a patient without a full knowledge of the history. In fact, don’tdo it even then. You wouldn’t want them to do it to you. It is a factthat many civil claims and complaints to the GOC only startbecause a second or subsequent practitioner makes a passingremark that criticises the actions of the first practitioner. This israrely done vindictively, although it is frequently done to make thesecond practitioner appear more knowledgeable or experienced inthe eyes of the patient. These idle remarks can create a quiteunjustifiable cascade of events that cause an enormous amount ofstress and anxiety. We can’t stop other professions from doing it tous, but we can at least not do it to each other.
About the authorTrevor Warburton is an AOP director and clinical advisor to the AOP
Legal Services Department. He is an independent practitioner with his
own practice in Stockport.
References1. NICE Press Release 2002/ 0051 Issued: October 14 2002
2. Age-Related Eye Disease Study Research Group. A Randomized,
Placebo-Controlled, Clinical Trial of High-Dose Supplementation with
Vitamins C and E, Beta Carotene, and Zinc for Age-Related Macular
Degeneration and Vision Loss: AREDS Report No. 8
Arch Ophthalmol. 2001 October ; 119(10): 1417–1436.
3. FL Ferris et al. Four-point scale developed to simplify AMD risk
assessment Ocular Surgery News January 22 2007
retinal tear until examination shows otherwise. This means that,for safety, recent onset flashes and floaters that you do notexamine require referral to an eye unit within 24 hours (Collegeadvice), via A&E if necessary. In any situation where you have dilated the patient’s pupils, it isgood practice to provide some form of written advice regardingthe effects of dilation.
GlaucomaIt goes without saying that it is important to be certain, at theconclusion of any sight test, that the patient does not haveglaucoma or, indeed, any other sight threatening condition.Practitioners make that decision many times every day.Sometimes the decision is easy and sometimes it is not. In a fewcases, that patient will go on to develop glaucoma in the future.Usually this is a slow process, but occasionally it progressesmuch faster. Patients who suffer from an aggressive form of thecondition, yet who are told it is normally slow to progress, canstart to wonder if it should have been detected sooner. You needto be sure that your records demonstrate that you did not missan early manifestation of glaucoma.
This does not mean that you have to do every test on everypatient to feel safe. Indeed, it is by no means certain that thiswould help as there becomes the danger of not seeing the woodfor the trees. It does mean that you need to document intra-ocular pressures and C:D ratios for adults at the very least. If thepatient has a family history of glaucoma, ensure that fact is notedon the record. At all times you need to stay alert to the need forfurther tests. The pressures may be 15mmHg R&L at the momentand, whilst the C:D ratio is 0.6 R&L, you have observed that thedisc is large, the cup is round and central and the neuro-retinalrim looks healthy. Therefore you have decided, as the patient isonly 42, you don’t need to do a visual field. If you have writtendown all that information, then the decision should be seen as areasonable one, even if the patient later develops glaucoma. If allyour record shows is IOP and a C:D of 0.6, then you invite laterquestions that you cannot defend.
If you make a referral, whether for glaucoma or anything else,it is as well to be explicit about your suspicions. If you suspectglaucoma, then say so, don’t simply list your findings and leave