Pheochromocytoma Dr. Atallah Al-Ruhaily. Pheochromocytoma 1. Catecholamine...
48
Pheochromocytoma Dr. Atallah Al- Ruhaily
-
date post
19-Dec-2015 -
Category
Documents
-
view
242 -
download
2
Transcript of Pheochromocytoma Dr. Atallah Al-Ruhaily. Pheochromocytoma 1. Catecholamine...
Pheochromocytoma
Dr. Atallah Al-Ruhaily
Pheochromocytoma
1. Catecholamine Physiology/Pathophysiology2. Clinical Presentation
1. Epidemiology2. Signs & Symptoms
3. Diagnosis1. Biochemical2. Localization
4. Management1. Preoperative2. Operative3. Postoperative4. Pregnancy
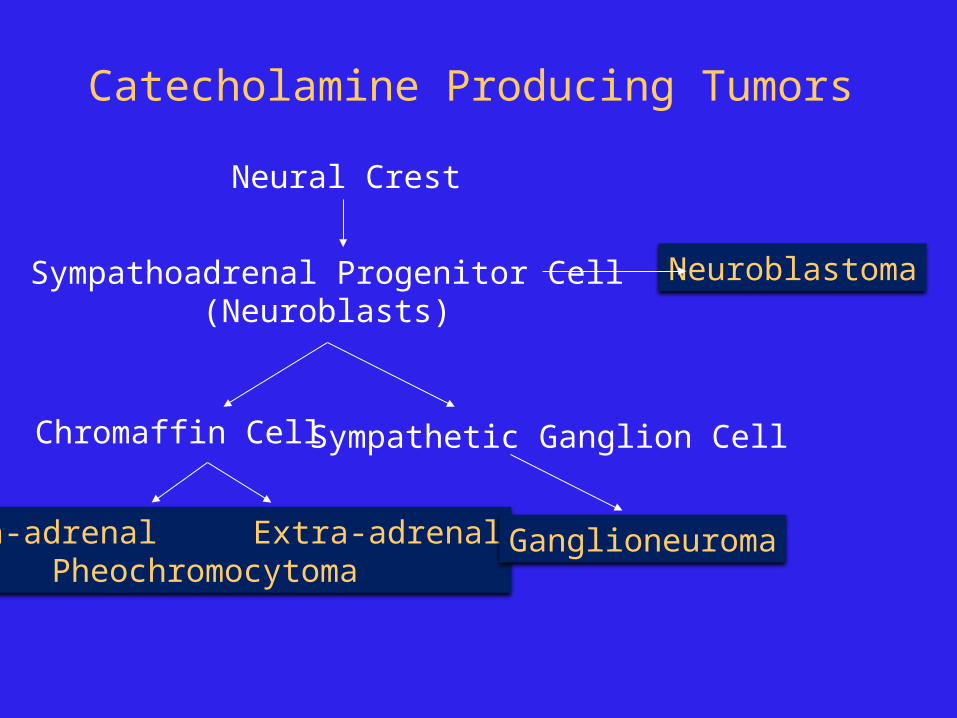
Catecholamine Producing Tumors
Neural Crest
Sympathoadrenal Progenitor Cell(Neuroblasts)
Chromaffin Cell Sympathetic Ganglion Cell
Intra-adrenal Extra-adrenalPheochromocytoma
Ganglioneuroma
Neuroblastoma
Pheochromocytoma
Paraganglioma (extra-adrenal pheo) Originate in extra-adrenal sympathetic chain/chromaffin tissue
Ganglioneuroma Behave like paraganglioma biochemically
Catecholamine Producing Tumors
Neuroblastoma Common malignancy in children, adrenal or sympathetic chain Catecholamine humoral effects usually minor Rapid growth & widespread metastasis Some differentiate and spontaneously regress Rx complex (surgery, XRT, chemotherapy)
Cheodectoma Carotid body, behave like paraganglioma biochemically
Glomus jugulare tumor Intracranial branch of CN IX and X Behave like paragangliomoa biochemically
Catecholamine Producing Tumors
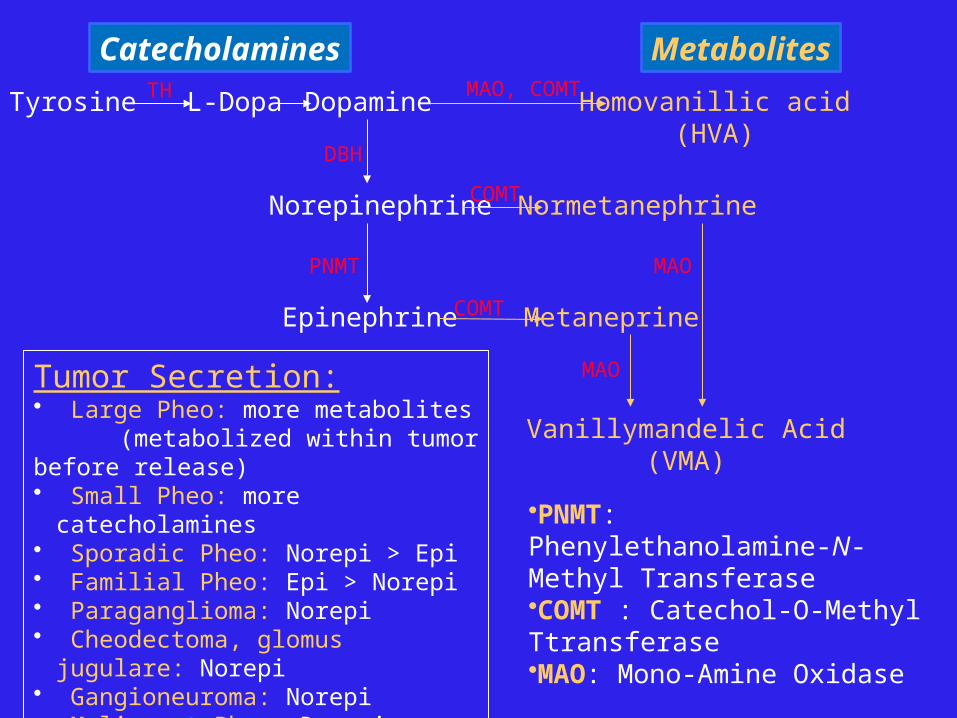
Tyrosine L-Dopa Dopamine
Norepinephrine
Epinephrine
Catecholamines
Normetanephrine
Metaneprine
PNMT
DBH
COMT
COMT
Metabolites
Homovanillic acid(HVA)
MAO, COMT
Vanillymandelic Acid(VMA)
MAO
MAOTumor Secretion:• Large Pheo: more metabolites (metabolized within tumor before release)• Small Pheo: more catecholamines• Sporadic Pheo: Norepi > Epi• Familial Pheo: Epi > Norepi• Paraganglioma: Norepi• Cheodectoma, glomus jugulare: Norepi• Gangioneuroma: Norepi • Malignant Pheo: Dopamine, HVA • Neuroblastoma: Dopamine, HVA
TH
•PNMT: Phenylethanolamine-N-Methyl Transferase•COMT : Catechol-O-Methyl Ttransferase•MAO: Mono-Amine Oxidase
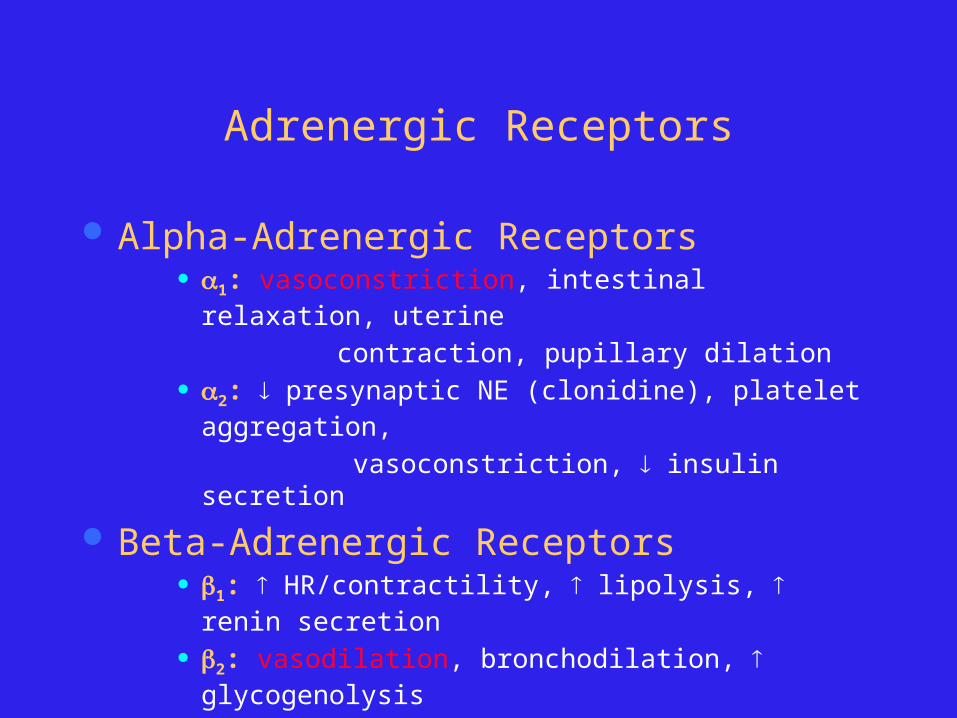
Adrenergic Receptors
Alpha-Adrenergic Receptors 1: vasoconstriction, intestinal relaxation, uterine
contraction, pupillary dilation 2: presynaptic NE (clonidine), platelet aggregation,
vasoconstriction, insulin secretion
Beta-Adrenergic Receptors 1: HR/contractility, lipolysis, renin secretion
2: vasodilation, bronchodilation, glycogenolysis
3: lipolysis, brown fat thermogenesis
Pheochromocytoma
1. Catecholamine Physiology/Pathophysiology2. Clinical Presentation
1. Epidemiology2. Signs & Symptoms
3. Diagnosis1. Biochemical2. Localization
4. Management1. Preoperative2. Operative3. Postoperative4. Pregnancy
Pheochromocytoma
0.01-0.1% of HTN population Found in 0.5% of those screened
M = F 3rd to 5th decades of life Rare, investigate only if clinically suspicion:
Signs or Symptoms Severe HTN, HTN crisis Refractory HTN (> 3 drugs) HTN present @ age < 20 or > 50 ? Adrenal lesion found on imaging (ex. Incidentaloma)
Pheo: Signs & Symptoms
The five P’s: Pressure (HTN) 90% Pain (Headache) 80% Perspiration 71% Palpitation 64% Pallor 42% Paroxysms
The Classical Triad: Pain (Headache), Perspiration, Palpitations Lack of all 3 virtually excluded diagnosis of pheo in a series of
> 21,0000 patients
Pheo: Paroxysms, ‘Spells’
10-60 min duration Frequency: daily to monthly Spontaneous Precipitated:
Diagnostic procedures, I.A. Contrast (I.V. is OK) Drugs (opiods, unopposed -blockade, anesthesia induction,
histamine, ACTH, glucagon, metoclopramide) Strenuous exercise, movement that increases intra-abdo
pressure (lifting, straining) Micturition (bladder paraganlgioma)
Pheo: Hypotension!
Hypotension (orthostatic/paroxysmal) occurs in many patients
Mechanisms: ECFv contraction Loss of postural reflexes due to prolonged
catecholamine stimulation Tumor release of adrenomedullin (vasodilatory
neuropeptide)

Pheo: Signs & Symptoms
N/V, abdo pain, severe constipation (megacolon) Chest-pains
Anxiety Angina/MI with normal coronaries:
– Catecholamine induced: myocardial oxygen consumption or coronary vasospasm
CHF HTN hypertrophic cardiomyopathy diastolic dysfn. Catechols induce dilated cardiomyopathy systolic dysfn.
Cardiac dysrhythmia & conduction defects
Pheo: Signs (metabolic)
Hypercalcemia Associated MEN2 HPT PTHrP secretion by pheo
Mild glucose intoleranceLipolysis
Weight-loss Ketosis > VLDL synthesis (TG)
Pheo: ‘Rule of 10’
10% extra-adrenal (closer to 15%)10% occur in children10% familial (closer to 20%)10% bilateral or multiple (more if familial)10% recur (more if extra-adrenal)10% malignant10% discovered incidentally
Familial Pheo MEN 2a
50% Pheo (usually bilateral), MTC, HPT MEN 2b
50% Pheo (usually bilatl), MTC, mucosal neuroma, marfanoid habitus
Von Hippel-Landau 50% Pheo (usually bilat), retinoblastoma, cerebellar
hemangioma, nephroma, renal/pancreas cysts NF1 (Von Recklinghausen's)
2% Pheo (50% if NF-1 and HTN) Café-au-lait spots, neurofibroma, optic glioma
Familial paraganglioma Familial pheo & islet cell tumor Other: Tuberous sclerosis, Sturge-Weber, ataxia-telangectgasia,
Carney’s Triad (Pheo, Gastric Leiomyoma, Pulm chondroma)
Pheochromocytoma
1. Catecholamine Physiology/Pathophysiology2. Clinical Presentation
1. Epidemiology2. Signs & Symptoms
3. Diagnosis1. Biochemical2. Localization
4. Management1. Preoperative2. Operative3. Postoperative4. Pregnancy
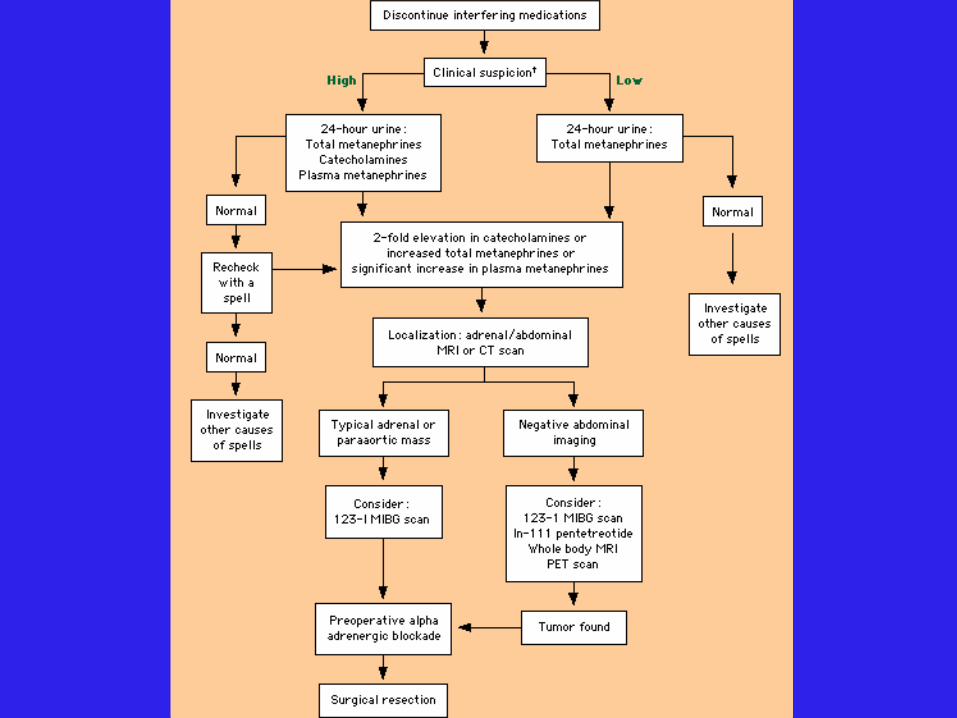
24h Urine Collection
24h urine collection: Creatinine, catecholamines, metanephrines,
vanillymandelic acid (VMA), +/-dopamine HPLC with electrochemical detection or mass spect
Positive results (> 2-3 fold elevation): 24h Ucatechols > 2-fold elevation
• ULN for total catechols 591-890 nmol/d 24h Utotal metanephrines > 1.2 ug/d (6.5 umol/d) 24h UVMA > 3-fold elevation
• ULN 35 umol/d for most assays
24h Urine Collection
Test Characteristics: 24h Ucatechols Sen 83% Spec 88%
24h Utotal metanephrines Sen 76% Spec 94%
24h Ucatechols + Utotal metanephrines Sen 90% Spec 98%
24h UVMA Sen 63% Spec 94%
Sensitivity increased if 24h urine collection begun at onset of a paroxysm
24h Urine: False Positive
Drugs: TCAs, MAO-i, levodopa, methyldopa, labetalol, propanolol, clonidine (withdrawal), ilicit drugs (opiods, amphetamines, cocaine), ethanol, sympathomimetics (cold remedies)
Hold these medications for 2 weeks! Major physical stress (hypoglycemia, stroke,
raised ICP, etc.) OSA
Plasma Catecholamines
Drawn with patient fasting, supine, with an indwelling catheter in place > 30 min
Plasma total catechols > 11.8 nM (2000 pg/mL) SEN 85% SPEC 80%
False positives: same as for 24h urine testing, also with diuretics, smoking
CRF & ESRD: Oliguric to Anuric 24h Urines inaccurate Plasma epinephrine best test for pheo in ESRD Plasma norepi and metanephrines falsely elevated in ESRD
Plasma Metanephrines
Not postural dependent: can draw normallySecreted continuously by pheoSEN 99% SPEC 89%False Positive: acetaminophen
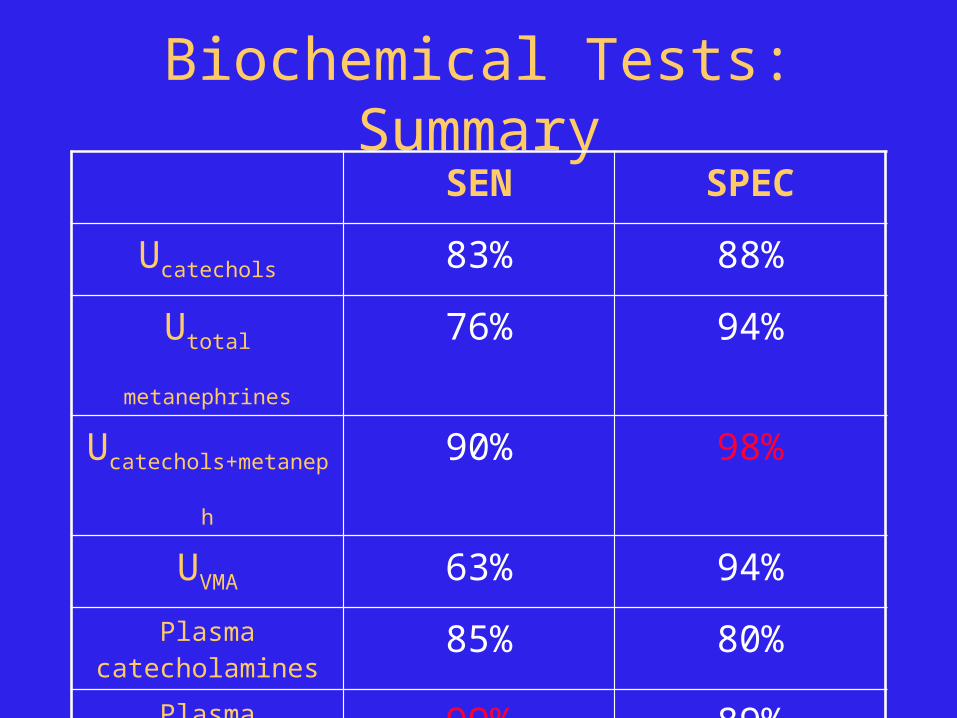
Biochemical Tests: SummarySEN SPEC
Ucatechols 83% 88%
Utotal metanephrines 76% 94%
Ucatechols+metaneph 90% 98%
UVMA 63% 94%
Plasma catecholamines 85% 80%
Plasma metanephrines 99% 89%
Suppression/Stimulation Testing
Clonidine suppression May precipitate hypotensive shock! Unlike normals, pheo patients won’t suppress their
plasma norepi with clonidine
Glucagon stimulation May precipitate hypertensive crisis! Pheo patients, but not normals, will have a > 3x
increase in plasma norepi with glucagon
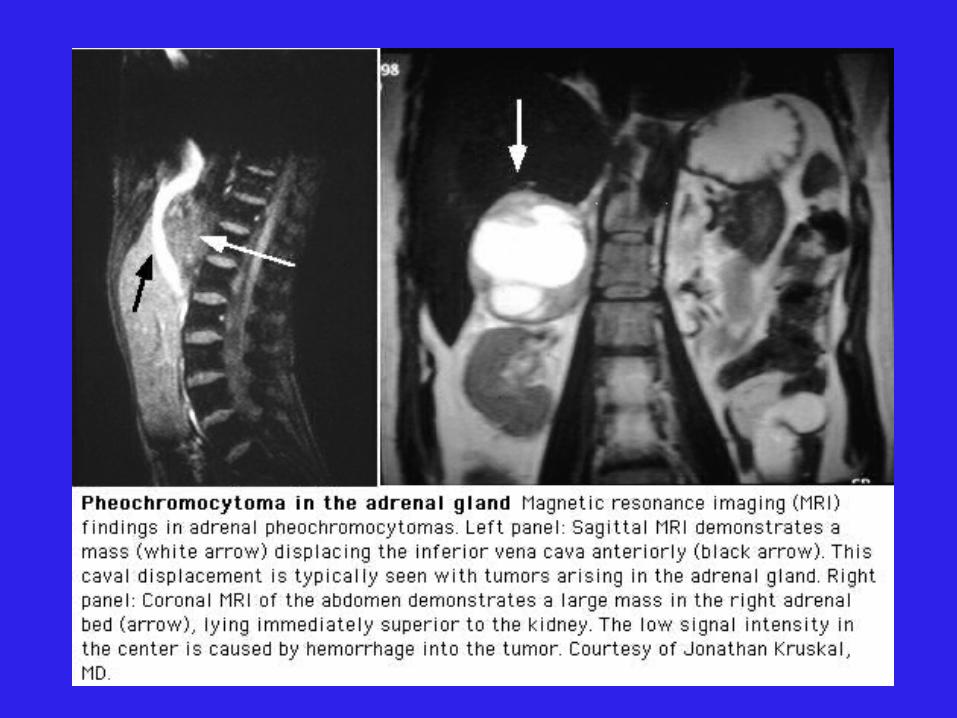
Localization: Imaging
CT abdomen Adrenal pheo SEN 93-100% Extra-adrenal pheo SEN 90%
MRI > SEN than CT for extra-adrenal pheo
Localization: Imaging
CT abdomen Adrenal pheo SEN 93-100% Extra-adrenal pheo SEN 90%
MRI > SEN than CT for extra-adrenal pheo
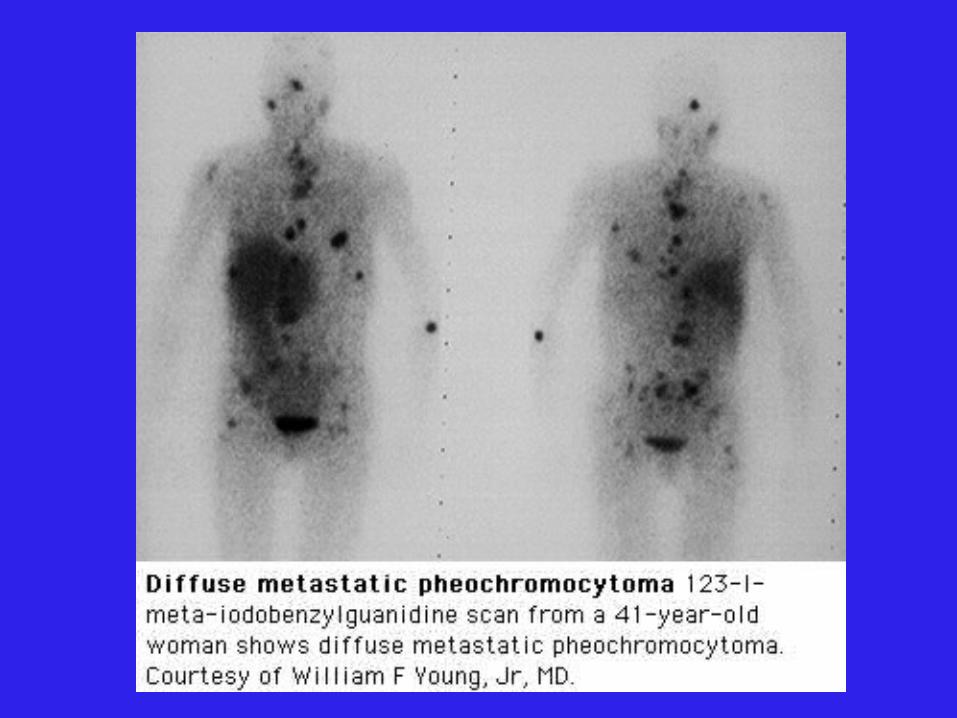
MIBG Scan SEN 77-90% SPEC 95-100%

MIBG Scan
123I or 131I labelled metaiodobenzylguanidine MIBG catecholamine precurosr taken up by the
tumor Inject MIBG, scan @ 24h, 48h, 72h Lugol’s 1 gtt tid x 9d (from 2d prior until 7d after
MIBG injection to protect thyroid) False negative scan:
Drugs: Labetalol, reserpine, TCAs, phenothiazines Must hold these medications for 4-6 wk prior to scan
Localization: Nuclear medicine
MIBG111Indium-pentreotide
Some pheo have somatostatin receptors
PET 18F-fluorodeoxyglucose (FDG) 6-[18F]-fluorodopamine
Pheochromocytoma
1. Catecholamine Physiology/Pathophysiology2. Clinical Presentation
1. Epidemiology2. Signs & Symptoms
3. Diagnosis1. Biochemical2. Localization
4. Management1. Preoperative2. Operative3. Postoperative4. Pregnancy
Pheo Management
Prior to 1951, reported mortality for excision of pheochromoyctoma 24 - 50 %
HTN crisis, arrhythmia, MI, stroke Hypotensive shock
Currently, mortality: 0 - 2.7 % Preoperative preperation, -blockade? New anesthetic techniques?
• Anesthetic agents• Intraoperative monitoring: arterial line, EKG monitor, CVP
line, Swan-Ganz
Experienced & Coordinated team: Endocrinologist, Anesthesiologist and Surgeon
Preop W/up
CBC, lytes, creatinine, INR/PTTCXREKGEcho (r/o dilated CMY 2º catechols)
Preop Preperation Regimens
Combined + blockade Phenoxybenzamine Selective 1-blocker (ex. Prazosin) Propanolol
Metyrosine Calcium Channel Blocker (CCB)
Nicardipine
Preop: + blockade
Start at least 10-14d preop Allow sufficient time for ECFv re-expansion
Phenoxybenzamine Special pharmacy access only (no DIN) Drug of choice Covalently binds -receptors (1 > 2) Start 10 mg po bid increase q2d by 10-20 mg/d Increase until BP cntrl and no more paroxysms Maintenance 40-80 mg/d (some need > 200 mg/d) Salt load: NaCl 600 mg od-tid as tolerated
Preop: + blockade
Phenoxybenzamine (cont’d) Side-effect: orthostasis with dosage required to normalized
seated BP, reflex tachycardia Drawback: periop hypotension/shock unlikely to respond to
pressor agent.
Selective 1-blockers Prazosin, Terazosin, Doxazosin Some experience with Prazosin for Pheo preop prep Not routinely used as incomplete -blockade Less orthostasis & reflex tachycardia then phenoxybenzamine Used more for long-term Rx (inoperable or malignant pheo)
Preop: + blockade
-blockade Used to control reflex tachycardia and prophylaxis
against arrhythmia during surgery Start only after effective -blockade (may ppt HTN) If suspect CHF/dilated CMY start low dose Propanolol most studied in pheo prep
• Start 10 mg po bid increase to cntrl HR
Preop: + blockade
If BP still not cntrl despite + blockade Add Prazosin to Phenoxybenzamine Add CCB, ACE-I Avoid diuretics as already ECFv contracted Metyrosine
Preop: + blockade
Meds given on AM of surgery Periop HTN:
IV phentolamine– Short acting non-selective -blocker– Test dose 1 mg, then 2-5 mg IV q1-2h PRN or as continuous
infusion (100 mg in 500cc D5W, titrate to BP) IV Nitroprusside (NTP)
Periop arrhythmia: IV esmolol Periop Hypothension: IV crystalloid +/- colloid
Pheo: Rx of HTN Crisis
IV phentolamineIV NTPIV esmololIV labetalol – combined + blocker
Preop: Metyrosine
Synthetic inhibitor of Tyrosine Hydroxylase (TH) Special pharm access, no DIN Start 250 mg qid max 1 gm qid Severe S/E’s: sedation, extrapyramidal, diarrhea,
nausea/vomit, anxiety, renal/chole stones, galactorrhea Alone may insufficiently cntrl BP and reported HTN crises
during pheo operation Restrict use to inoperable/malignant pheo or as adjunct to
+ blockade or other preop prep
Tyrosine L-Dopa Dopamine
Norepinephrine
Epinephrine
PNMT
DBH
TH
Preop: CCB CCB
Block norepi mediated Ca transport into vascular smooth muscle
Nicardipine: most commonly used agent Nicardipine (France Study)
Started po 24h to few weeks preop to cntrl BP and allow ECFv restoration
After intubation IV Nicardipine gtt (start 2.5 ug/kg/min) IV Nicardipine adjusted to SBP Stopped prior to ligation of tumor venous drainage Tachycardia Rx with concurrent IV esmolol
Advantage: periop hypotension may still respond to pressor agents as opposed to those patients who are completely -blocked
O.R.Admit night before for overnight IV salineArterial line, EKG monitor, CVP lineKnown CHF: consider Swan-GanzRegardless of preop medications:
Have ready: IV phentolamine, IV NTP, IV esmolol Rx hypotension with crystalloid +/- colloid 1st
Aim for CVP 12 or Wedge 15 Inotropes may not work!
O.R.
Anesthetic choice: Enflurane or isoflurane: don’t sensitized
myocardium to catecholamines Halothane: may sensitize heart arrhythmia
Laprascopic adrenalectomy if tumor < 8cm
Postop
Most cases can stop all BP meds postop Postop hypotension: IV crystalloid HTN free: 5 years 74% 10 years 45%
24h urine collection 2 wk postopSurveillance:
24h urine collections q1y for at least 10y Lifelong f/up
Pheo: Unresectable, Malignant
-blockade Selective 1-blockers (Prazosin, Terazosin, Doxazosin) 1st line
as less side-effects Phenoxybenzamine: more complete -blockade
-blocker CCB, ACE-I, etc. Nuclear Medicine Rx:
Hi dose 131I-MIBG or 111indium-octreotide depending on MIBG scan or octreoscan pick-up
Sensitize tumor with Carboplatin + 5-FU
Pheo & Pregnancy
Diagnosis with 24h urine collections and MRI No stimulation tests, no MIBG if pregnant 1st & 2nd trimester (< 24 weeks):
Phenoxybenzamine + blocker prep Resect tumor ASAP laprascopically
3rd trimester: Phenoxybenzamine + blocker prep When fetus large enough: cesarian section followed by tumor
resection