PEDI GU REVIEW intersex
74
Disorders of Sexual Differentiation Pediatric GU Review UCSD Pediatric Urology George Chiang MD Sara Marietti MD Outlined from The Kelalis-King-Belman Textbook of Clinical Pediatric Urology 2007 (not for reproduction, distribution, or sale without consent)
-
Upload
george-chiang -
Category
Health & Medicine
-
view
1.283 -
download
3
Transcript of PEDI GU REVIEW intersex

Disorders of Sexual DifferentiationPediatric GU Review
UCSD Pediatric UrologyGeorge Chiang MD
Sara Marietti MD
Outlined from The Kelalis-King-Belman Textbook of Clinical Pediatric Urology 2007
(not for reproduction, distribution, or sale without consent)


Outline
• Embryology• Classification• Disorders• Workup• Cases• SESAP Questions

Chromosomal sexChromosomal sex
Gonadal sexGonadal sex
Phenotypic sexPhenotypic sex
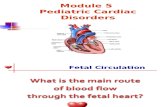
Sexual DifferentiationSexual Differentiation

Chromosomal Sex
• Genes associated with sex determination– TDF (testis-determining factor) = SRY
(sex-determining region Y gene)– WT-1 = commitment and maintenance
of gonadal tissue– SF-1 = regulator of mullerian inhibiting
substance– SOX-9– DAX-1 (X linked)

““Development”Development”
TDFTDFSRYSRY
TestTestisis
TestTestisis
TestosteroneTestosterone Müllerian Inhibiting Müllerian Inhibiting SubstanceSubstance
Penis Penis Vas DefernsVas DefernsProstateProstate
UterusUterusFallopian TubesFallopian TubesUpper VaginaUpper Vagina

Testicle Testicle DifferentiationDifferentiation
• Testicle- Sertoli and Leydig cellsTesticle- Sertoli and Leydig cells– Leydig cellsLeydig cells- testosterone- testosterone
8-12 weeks8-12 weeks
Virilization external genitaliaVirilization external genitalia
Wolfian ductsWolfian ducts Vas deferens Vas deferens
– Sertoli cells- MISSertoli cells- MIS
Müllerian Inhibiting Müllerian Inhibiting SubstanceSubstance
8-10 weeks8-10 weeks
Regression of Müllerian Regression of Müllerian structuresstructures

Ovarian Ovarian DifferentiationDifferentiation
• Absence of SRYAbsence of SRY• No testosterone or MISNo testosterone or MIS• Maintenance of Müllerian Maintenance of Müllerian
structuresstructures– Fallopian tubesFallopian tubes– UterusUterus– Upper 2/3 vaginaUpper 2/3 vagina
• ““Feminization” of Feminization” of external genitaliaexternal genitalia

Board Questions:
• Paramesonephric (Mullerian) duct
• Mesonephric (Wolffian) duct
Gartner’s Duct
Prostatic Utricle
Appendix Testes
Appendix Epididymis
Epoophoron




Male Phenotypic Sexual Differentiation
• Masculinization of the male fetus starts between 7-8 weeks gestation and is complete by 12-13 weeks
• MIS in males acts locally and unilaterally to suppress mullerian ducts(Fallopian tubes, Uterus, Upper 2/3 of the
Vagina)• Testosterone in males permits local
development of the wolffian ducts(Epididymis, Vas deferens, Seminal vesicles,
Prostate)

Female Phenotypic Sexual Differentiation
• The absence of circulating testosterone in the female fetus maintains the appearance of the external genitalia at the 6-week gestational stage


Tanner Stages

Classification
• Intersex (or DSD) vs. Ambiguous genitalia
• Workup and classification are not straightforward
• Only testicular tissue descends• Gonad causes ipsilateral mullerian
duct development/regression

Hughes IA, Houk C, Ahmed SF, Lee PA. Hughes IA, Houk C, Ahmed SF, Lee PA. Consensus statement on the management of intersex Consensus statement on the management of intersex
disorders. Archives of Disease in Childhood 2006disorders. Archives of Disease in Childhood 2006
Consensus panel, organized by the Consensus panel, organized by the Lawson Wilkins Pediatric Endocrine Lawson Wilkins Pediatric Endocrine Society (LWPES) and the European Society (LWPES) and the European Society for Pediatric Endocrinology Society for Pediatric Endocrinology (ESPE): (ESPE):
• advocated that the term “Disorders of advocated that the term “Disorders of Sexual Development” (DSD), now be Sexual Development” (DSD), now be used for congenital conditions with used for congenital conditions with discordance of genotypic, gonadal, discordance of genotypic, gonadal, and/or phenotypic sexand/or phenotypic sex

HWA Protests Intersex Genital MutilationHWA Protests Intersex Genital Mutilation
[Washington, DC: 21 Apr 98] A dozen members of Hermaphrodites With Attitude and Transexual Menace picketed outside the George Washington University Hospital, protesting GWU's cutting of intersexed infants' genitals protesting GWU's cutting of intersexed infants' genitals to make them resemble 'normal' male and female genitalsto make them resemble 'normal' male and female genitals. Hermactivists call this medical intervention Intersex Genital Mutilation (IGM).
"Not only are American doctors cutting into 7 intersexed infants every working day, but people like GWU's Dr. Barry Belman are telling parents they but people like GWU's Dr. Barry Belman are telling parents they have to do it for the good of the infanthave to do it for the good of the infant," said Cheryl Chase, founder of HWA. "Mutilating my genitals wasn't for my good; it was to make the doctors and my parents more comfortable with my body."
After the demo, several protestors visited GWU Hospital departments that take part in IGM--OB/GYN, Endocrinology, Pediatrics and Plastic Surgery--to discuss their concerns with caregivers and, as one hermactivist put it, to speak for the infants who cannot speak for themselves.
From In Your Face on-line news, April 1998

First and foremost, we recommend avoidance of First and foremost, we recommend avoidance of harmful or unnecessary genital surgery on infants harmful or unnecessary genital surgery on infants and children. No surgery should be performed and children. No surgery should be performed unless unless it is absolutely necessary for the physical health and it is absolutely necessary for the physical health and comfort of the intersexual childcomfort of the intersexual child. We believe any . We believe any surgery that does not meet these criteria to be surgery that does not meet these criteria to be essentially elective cosmetic surgery which should essentially elective cosmetic surgery which should be deferred until the intersexual child is able to be deferred until the intersexual child is able to understand the risks and benefits of the proposed understand the risks and benefits of the proposed surgery and is able to provide appropriately informed surgery and is able to provide appropriately informed consent.consent.

Disorders of Sex Development
• Female Pseudohermaphrodite– 46 XY DSD
• XX Male or XX sex reversal– 46 XX testicular DSD
• XY sex reversal– 46, XY complete gonadal dysgenesis
• True hermaphrodite– Ovotesticular DSD
• Male pseudohermaphrodite– 46 XY DSD

Intersex
• Disorders of gonadal differentiation• True Hermaphrodite• Female Pseudohermaphrodite
– Masculinized female– Ovaries present but external genitalia virilized
• Male Pseudohermaphrodite– Testes present but genital ducts or external
genitalia not completely virilized

Wide range of phenotypesWide range of phenotypes

Disorders of Gonadal Differentiation
• Klinefelter• Turner’s Syndrome• Mixed gonadal dysgenesis• Pure gonadal dysgenesis• Bilateral vanishing testis/testicular
regression

Klinefelter’s
• 1 in 1000 males• Gynecomastia, increased GnRH,
small testes• 47 XXY• Azospermia with low normal
Testosterone• Not ambiguous

Turner’s Syndrome– 45,X female phenotype – One normal functioning X chromosome, can have mosaicism; – Presence of Y increases masculinization and gonadoblastoma– 1/2500 live births– No secondary sexual characteristics– Multiple cardiac and renal anomalies– Search for Y chromosome and prophylactic
gonadectomy if Y found– Streak gonad (oocytes undergo rapid apoptosis in fetal
period- 2-3 cm in broad ligament)– FSH/LH elevated– Ultrasound for renal and cardiac anomalies– Growth hormone to improve stature and exogenous estrogen
at 12-15 years to induce puberty– Not ambiguous

• 2nd most common DSD
• XO/XY Mosaic Karyotype
(45X0/46XY)
• Testis and a Streak
• Wolffian structures with testis
• Mullerian structures with streak
Mixed Gonadal Dysgenesis

Hypospadias plus
Unilateral undescended testis
“Bilateral” undescended testis (If neither testis is palpable, could be female CAH)
-Can be ambiguous genitalia or normal male
genitalia
Mixed Gonadal Dysgenesis

• Treat according to genital potential ???
– 2/3 raised as female
• Higher risk of Wilms’ tumor
• What about the testis if raised male ?
– - Bring it down or Remove it
– - Annual testis ultrasounds after puberty
Mixed Gonadal Dysgenesis

Pure Gonadal Dysgenesis
• 46 XY [46XX is straightforward]• Abnormality of SRY gene that eliminates SRY
function• Bilateral streak gonad with similar Turner’s histology• 30% risk of gonadoblastoma by 30• Normal female genitalia, well developed Mullerian
structures• Delayed puberty, elevated FSH/LH, amenorrhea• Treat with removal of streak gonads, cyclic hormonal
replacement• Not Ambiguous

Embryonic Testicular Regression and Bilateral
Vanishing Testes• Genetic mutation vs teratogen vs bilateral torsion• 3 phenotypes
• Early before 60-70 days gestation with female phenotype and no inner ductal or Wolfian structures
• Intermediate: ambiguous genitalia, absent gonads, no internal Mullerian structures, some elongation of phallus
• Late: microphallus, absent testes, fully developed Wolfian structues (bilateral vanishing testes)
• Diagnosis: Elevated FSH/LH and castrate testosterone levels; 46 XY
• Management– Phenotypic femalesestrogen supplementation and
dilation of vagina vs. reconstruction– Phenotypic MalesAndrogen replacement can
succesfully result in normal penis, secondary sexual characteristics

True Hermaphrodite
• Ambiguous genitalia• 1 ovary or 1 testes or ovotestis
– Ovary usually on left and testis or ovotestis on right
• Hidden mosaicism with a Y cell ine• 60% 46 XX, 33% mosaicism• 75% raised as males• Gender assignment based on functional potential• Potential for fertility as female unlike males• Monitor for tumors

Female Pseudohermaphrodite
• Etiologies include CAH and maternal virilizing hormone– Defect in one of 5 enzymes
• 21 hydroxylase (95%) – CYP21 gene on 6p21.3– Autosomal recessive– Salt-wasters (75%)shock within 1-2 weeks after birth, simple
virilizers (25%)males Diagnosis with elevated plasma levels of progesterone and 17 OH progesterone (pelvic u/s demonstrates mullerian tissues; adrenal u/s demonstrates enlargement)
• 11B-hydroxylase (5%)– HTN common from increased levels of deoxycorticosterone– Increased plasma 11-DOC and 11-deoxycortisol; urinary levels of 17-
ketosteroids and 17-hydroxysteroids increased • 3 B-hydroxysteroid dehydrogenase
– Impaired synthesis of aldosterone, cortisol, and sex steroids– Elevated serum 17-hydroxpregnenalone and DHEA– Autosomal recessive– Females have clitoral enlargement and labial fusion (mullerian
structures by pelvic u/s)– Males have hypospadias and masculinize later

Female Pseudohermaphrodite
• Maternal androgen exposure:– <12 weeks Progestational agents or maternal tumor
(luteoma, arrhenoblastoma, adrenal CA)– Medications:2% of female infants if tx with progestins in-
utero (Danazol)• Prenatal treatment
– Dexamethasone at 5-6 weeks GA– Can assay for 17-OH progesterone at 16-17 weeks– 3 of 4 children do not need the treatment
• Postnatal treatment– Supply deficient hormone to suppress ACTH– Mineralocorticoid replacement for salt wasters– Feminizing genitoplasty at 3-6 months– Prophylactic adrenalectomy for salt losers and severely
masculinized females

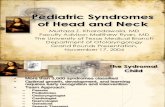
21-Hydroxylase deficiency21-Hydroxylase deficiency
TestosteroneTestosterone

FEMALE CAHFEMALE CAH

Female CAH

Female CAH


• Inadequate production of testosterone
• Inadequate metabolism of testosterone
• End-organ sensitivity to testosterone
• Inadequate production of MIS
Male Pseudohermaphrodite

Male Pseudohermaphrodite
• Inadequate production– Defect in 5 enzymes can cause
incomplete or absent virlization– StAR, 3 B-hydroxysteroid, 17alpha-
hydroxylase, 17,20 lyase, 17 B-hydroxysteroid oxidoreductase

Male Pseudohermaphrodite
• Inadequate metabolism– 5 alpha reductase deficiency– 46 XY karyotype varying from penoscrotal
hypospadias to markedly ambiguous genitalia– Partial masculinization at puberty “guevedoces”– Elevated mean plasma testosterone/DHT ratios
• hCG stim can increase from 3-25 to 75-160
– Diagnose with genital skin fibroblasts cultures– Tx: male sex rearing; if female, early
gonadectomy

Male Pseudohermaphrodite
• End organ sensitivity• CAIS
– Phenotypic unambiguous female– Evaluation of inguinal hernia (50%) with testis or
primary amenorrhea, lack of pubic/axillary hair– Absence of Mullerian derivatives– Fetal testes secrete MIS and have absent
spermatogenesis with normal or hyperplastic Leydig cells
– At puberty gonadotropin levels rise with increased estradiol and breast development
– Timing of gonadectomy controversial (if early, no estradiol; if late, risk of malignancy)

Male Pseudohermaphrodite
• PAIS– Variable ambiguity– Repair of hypospadias and/or
cryptorchidism– Diagnosis
• 46 XY ambiguous genitalia and absent Mullerian structures on pelvic u/s
– Management depends on degree of ambiguity

Male Pseudohermaphrodite
• Inadequate production of MIS • Persistent Mullerian Duct
– 46 XY– Normal male external genitalia with internal
mullerian duct structures– Unilateral or bilateral undescended testes, fallopian
tubes, uterus, and upper vagina draining a prostatic utricle
– PMDS defect in MIS on Chromosome 19p13 or receptor on chromosome 12q13
– Tx with orchiopexy; risk of malignancy in retained mullerian structures

• Classic ambiguous genitalia
• Female with palpable gonads
• Male with nonpalpable gonads
• Hypospadias and cryptorchidism
• “Normal” Female or Male
Common Nenonatal Presentations



•History– Born to a 32 yo G5P4 female at ~34 weeks
gestation– Prenatal care begun at ~1 month– Triple screen showed low estriol– Amniocentesis negative– No family history of intersex disorders– No known prenatal exposures
Case #1Case #1

Case #1Case #1

Physical ExamPhysical Exam
• Physical Exam– General exam WNL– Genitalia
• Fused labia majora with slight hyperpigmentation
• Single perineal opening• Slightly enlarged clitoris • No palpable gonads

Workup?
• Labs– Electrolytes all WNL x 12 days in NICU– Karyotype – 46, XX– Androstenediol – WNL– Deoxycortisone – elevated– DHEA – elevated– Testosterone – insufficient initially, sl elevated
at 1 month– 17-Hydroxyprogesterone - elevated

Workup?

Plan?
• Multidisciplinary approach• Stabilize electrolytes if necessary• Plan for surgical management

Voiding Cystourethrogram

Case #2
• 6 month old presents with undescended testicle
• Past Sur Hx: None• Past Med Hx: No prenatal care• Meds: None



Workup/Plan?
• Karyotype 45X/46XY

Case 3
• 12 year old female presents with bilateral inguinal hernias

Case 3

QUESTIONS

The earliest clinically detectable pubertal change in a boy is:
a) Enlargement of the testes
b) Appearance of pubic hair
c) Deepening of the voice
d) Scrotal rugation
e) Increase in phallic length

Inhibin is a substance derived from the testicle which mediates secretion of:
a) Testosterone
b) FSH
c) LH
d) GnRH
e) Mullllerian inhibiting factor

During the first three years of life, hymenal morphology demonstrates progression of its:
a) Redundancy
b) External ridging
c) Notching
d) Annular configuration
e) Crescentic configuration

The diagnosis of testicular agenesis is confirmed by:
a) Absence of an ipsilateral kidney
b) Absence of an ipsilateral vas deferens
c) Blind-ending testicular vessels
d) Ipsilateral scrotal hypoplasia
e) Ipsilateral mullerian structures

5-alpha-reductase deficiency is associated with:
a) Poorly differentiated Wolffian structures
b) Poorly differentiated Mullerian structures
c) Gynecomastia
d) Elevated concentration of testosterone at puberty
e) Elevated dihydrotestosterone-testosterone ratio

Unilateral renal agenesis is associated with an increased incidence of:
a) Ipsilateral anorchia
b) 2 vessel umbilical cord
c) Ipsilateral adrenal agenesis
d) Mullerian duct abnormalities
e) Urethral anomalies

A 3 year old phenotypic girl undergoes an abdominal and pelvic ultrasound for intermittent abdominal pain. No uterus is seen on the ultrasounds. Right and left gonads are identified in their respective inguinal canals. Karyotype is 46 XY. The next step is:
a) Genetic sequencing of the patient’s androgen receptor gene
b) Serum for LH, FSH and serum testosterone
c) Serum for mullerian inhibitory factor
d) Serum for 17-OH
e) Gonadal biopsy

A 22 year old man with CAH has bilateral testicular masses. The next step is:
a) Serum ACTH and cortisol
b) Serum LH and testosterone
c) Pituitary MRI scan
d) Percutaneous testis biopsy
e) Bilateral excisional biopsies

A 3 year old girl has normal external genitalia and an absent vagina. Her chromosomes are 46 XY. The most common associated finding is:
a) Unilateral gonadal agenesis
b) Tethered spinal cord
c) Unilateral renal agenesis
d) Inguinal hernia
e) VUR

A 38 year old woman undergoes amniocentesis at 24 weeks gestation. The fetal karytotype is 45X/46XY. The gonads will most likely be:
a) Bilateral streak gonads
b) Streak gonad and testis
c) Streak gonad and ovary
d) Streak gonad and dysgenetic testis
e) Bilateral testes

A phenotypically normal 3 year old girl has bilateral inguinal hernias. During a hernia repair, the gonad is discovered within the hernia sac. Frozen section biopsy documents that it is a testis. These findings suggest:
a) Persistent mullerian duct syndrome
b) True hermaphroditism
c) Complete androgen insensitivity
d) Mixed gonadal dysgenesis
e) Adrenogenital syndrome

A 17 year old-boy undergoes evaluation for delayed puberty. He is above average height, has bilateral small testes, and gynecomastia. Serum FSH and LH are elevated and testosterone is low. The patient is at increased risk for:
a) Breast cancer
b) Gonadoblastoma
c) Testicular cancer
d) Prostate cancer
e) TCC