METABOLIC SYNDROME - ENCOGNITIVE.COM SYNDROME-- The Twenty-First...METABOLIC SYNDROME The...
11
Transcript of METABOLIC SYNDROME - ENCOGNITIVE.COM SYNDROME-- The Twenty-First...METABOLIC SYNDROME The...


METABOLIC SYNDROMEThe Twenty-First Century Epidemic
By Steven V Joyal, MD
Dropping dead from a heart attack, being crippled hy acatastrophic stroke, having limbs amputated as a result ofperipheral vascular disease—these are among the frighten-ing consequences of vascular disease, the number-one killerof Americans.
Metabolic syndrome and its associated condition ofinsulin resistance pose a major threat to cardiovascular healththat most health care practitioners do not evendiscuss with their patients. Remarkably, the publicknows very little about this silent but deadly condition, andmany affected individuals are not even aware that metabol-ic syndrome is inflicting severe damage to their arteries andbrain cells. > > >
July 2006 LIFE EXTENSION 55

The news media and health careproviders pay almost no attention tothe epidemic of insulin resistance,the fundamental cause of metabolicsyndrome.
To avoid the potentially disastrouscardiovascular consequences ofmetabolic syndrome, you need tounderstand:• What metabolic syndrome is and
how to determine whether youmeet its diagnostic criteria (atape measure, a blood pressurecuff, and some simple blood testsare all you need).
• How to identify the risk of insulinresistance through simple bloodtests.
• Why body weight is not veryimportant for metabolic health,but body composition is critical.
• How a simple but very effectiveprogram—and not the latest faddiet—can dramatically reduceyour risk for insulin resistanceand metabolic syndrome.
• Which nutritional supplementscan help reduce your risk ofinsulin resistance and metabolicsyndrome. (These include twopromising supplements derivedfrom water-soluble extracts ofcinnamon and coffee^—one ofwhich targets the same hormonethat multibillion-dollar pharma-ceutical companies tout as key tothe next breakthrough therapyfor metabolic disease.)
GAliGiNCi YOliR RISK FORJN RESISTANCE
Metabolic syndrome is character-ized by insulin resistance. Beforeexplaining insulin resistance, weneed to understand what insulin isand how it acts in the body.
A hormone produced in thepancreas, insulin's major function isto regulate blood sugar, or glucose,levels. Insulin helps to shuttle glu-cose molecules from the blood intothe cells of the body. When bloodsugar levels increase, insulin outputincreases.
Insulin resistance means thatinsulin does not work optimally at itstarget tissue—such as muscle, fat, orliver tissue—to drive glucose into
cells. This has numerous adverseconsequences, including glucoseand insulin levels that are muchhigher than normal. As the bodyattempts to overcompensate for poorinsulin action by pumping out moreinsulin from the pancreas, insulinlevels rise. Eventually, over time, thepancreas can "burn out" and nolonger produce enough insulin tocontrol hlood sugar. When insulinlevels are not sufficient to bringblood sugar levels down to the nor-mal range, type II diabetes mellituscan result.
The gold standard for measuringinsulin resistance is a very complexprocedure called a "hyperinsuline-mic euglycemic clamp" that isoffered at specialized academicmedical research centers. In thistwo-hour procedure, insulin isinfused intravenously at a constantrate according to body weight. At thesame time, glucose is infused intra-venously at a variable rate to balanceout the insulin infusion. The rateof glucose infusion into bloodduring the last 30 minutes of the testdetermines insulin sensitivity.
Fortunately, to help determineyour risk of insulin resistance, youdo not have to travel to an academicmedical center to have the "hyper-insulinemic euglycemic clamp"performed; instead, you need onlyundergo some simple blood tests.
Certain blood tests such as fastinginsulin can serve as surrogate mark-ers for insulin resistance. Excessinsulin (fasting hyperinsulinemia) isdefined when levels equal to orgreater than 15 pU/mL are found.These higher fasting insulin levels areassociated with insulin resistance.'Other blood tests that are very usefulin evaluating the risk of insulin resis-tance include serum triglycerides andhigh-density lipoprotein (HDL).Triglycerides equal to or greater than130 mg/dL and a triglyceride:HDLratio equal to or above 3.0 suggest ahigh risk of insulin resistance.' Infact, the Life Extension Foundationhas consistently advocated evenlower levels of triglycerides (less than100 mg/dL) as being optimal.
ARE YOU AT RISKFOR METABOLIC SYNOROME?
Having your fasting insulin,triglycerides, and HDL checked canhelp you determine whether you are
at risk for Insulin resistance.The following values indicate that
you are at risk for insulin resistanceand metabolic syndrome:'
Fasting insulin > 15Triglycerides > 130 mg/dL
Triglycerides:HDL ratio > 3,0.
56 LIFE EXTENSION July 2006

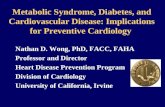
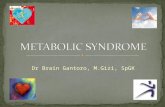
Figure 1: Age-Adjusted Prevalence of Metabolic Syndrome
. r
WhiteBlackHispanicOther
Men Women
Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults:findings from the Ttiird National Health and Nutrition Examination Survey,JAMA. 2002 ian 16; 287E3);356-9.
DOVOUK'WEMETABOLIC SI'NDROME?
Afflicting one of every five Ameri-cans (with even higher rates in cer-tain ethnic populations), metabolicsyndrome has ominous implicationsfor cardiovascuiar disease risk.'
More than 20 years ago, scientistsidentified the constellation of con-ditions that characterizes metabolicsyndrome in a group of patientswith a drastically elevated risk ofheart disease and stroke. Initiaiiycalled "Syndrome X" by scientists,it is now known as metabolic syn-drome. This dangerous condition ischaracterized by insulin resistance,which leads to abnormally highserum lipids and cholesterol, highblood pressure, abnormally highblood sugar, and increased blood-clotting tendencies.'
Metabohc syndrome dramatical-ly increases cardiovascular diseaserisk/ Recent trial results in morethan 1,200 men followed for 11 yearsfound that those with metabolicsyndrome were up to 360% morelikely to die from coronary heartdisease.'
The diagnostic criteria formetabolic syndrome can differslightly depending on the medicalexperts consulted. A standard,accepted definition was establishedby the Third Report of the NationalCholesterol Education Program(NCEP) Expert Panel on Detection,Evaluation, and Treatment of HighBlood Cholesterol in Adults (Adult
Treatment Panel 111)." According toits definition, you have metabolicsyndrome if you bave three or moreof the following criteria:" Central obesity as measured
by waist circumference:Men: > 40 inches.Women: > 35 inches.
• Fasting blood triglycerides:> 150 mg/dL.
• Blood HDL:Men: < 40 mg/dL.Women: < 50 mg/dL.
' Blood pressure: > 130/85 mmHg.• Fasting glucose: > 100 mg/dL
(recently changed from> 110 mg/dL to reflect the revisedAmerican Diabetes Associationcriterion for impaired fastingglucose).
A PRO(iR\M FOR AWRTINGMETABOLIC S T\ DROME
Tbe following step-by-stepprogram can help you avert tbepotentially deadly consequencesof metabolic syndrome. Takingthese simple steps can help youlead a long, healthy life and avoidsuccumbing to a multitude of life-threatening diseases.
Step 1: Assess YourBody Composition.
The first step involves knowingand understanding your body com-position and its importance in help-ing to prevent metabolic syndrome.Surprisingly, stepping on a scale and
seeing what you weigh does not tellvery much about your risk of devel-oping metabolic disease.
Body mass index (BMI) is a stan-dard measure of overweight and obe-sity. BMI is obtained by dividing yourbody weigbt in kilograms by yourheight in meters squared (kg/m').However, BMI fails to account forbody composition. Your body compo-sition is a measure of how much leanbody mass (muscle) and adiposetissue (body fat) you have.
Compare two 40-year-old men,both of whom stand six feet tall andweigh 200 pounds. One man is verymuscular (about 7% body fat) andhas a waist circumference of 32 inch-es. By contrast, the other man is outof shape (about 30% body fat) andhas a waist circumference of 40 inch-es. The key point is, both men havethe same BMI.
Does this mean that both menbave the same risk of developinginsulin resistance and metabolicsyndrome? No!
The man who has poor body com-position (low level of lean body mass,high level of fat mass) and carrieshis body fat around his waist {centralobesity) is at risk of developing
DETECTING METABOLIC SYNDROME
To determine whether you havemetabolic syndrome, ask your doctor
to measure your waist circumference,blood pressure, fasting glucose, serum
triglycerides, and HDL By AdultTreatment Panel III criteria, you havemetabolic syndrome if you have three
or more 0^ the following criteria:
• Central obesity as measuredby waist circumference:Men: > 40 inches.Women: > 35 inches.
• Fasting blood triglycerides:> 150 mg/dL
• Blood HOL:Men: < 40 mg/dLWomen: < 50 mg/dL
• Blood pressure:> 130/85 mmHg.
• Fasting glucose:> 100 mg/dL
July 2006 LIFE EXTENSION 57

insulin resistance and metabolicsyndrome. The physically fit manwith a low amount of body fat and aslim waist is at very, very low risk ofinsulin resistance and metabolicsyndrome.
Unfortunately, many individualspay more attention to body weightthan to body composition. Scientists,however, know better.
The easiest surrogate assessmentof body composition is central obesi-ty, and the easiest way to determinecentral obesity is to measure waistcircumference—if you have a bigwaist, your risk of metabolic diseaseis increased.
Step 2: Maintain GoodBody Composition.
How do you obtain and maintaingood body composition? Maintain-ing lean body mass and decreasingbody fat is easier than you think.
First, do not fail for the latest faddiet. Maintaining a stable bodyweight is not magic. Ignore any diet"guru" who promises "magical"weight loss, vilifies "forbiddenfoods," and promotes excluding cer-tain food "types" based on the latestround of misunderstood and misin-terpreted science. Do nof buy into it!
Instead, simply eat more wholefoods and fewer processed foods.Prioritize eating high-qualityfoods like salmon, vegetables.
wild rice, berries, and citrus fruits.De-emphasize eating foods that arehighly processed or of low nutri-tional value, such as cakes, cookies,bagels, fried chicken, and Americancheese. In fact, studies show thatdiets that emphasize whole foods,such as the Mediterranean diet,help maintain lean body mass whilealso improving metabolic markerslike insuhn, cholesterol, fibrinogen.and uric acid.' Other studies of peo-ple eating Mediterranean-type dietsshow a strong reduction in choles-terol levels, increased psychologicaland physical well-being, and atrend towards weight loss euenwithout trying to diet."
A great-tasting, healthy diet isabundant in whole foods, much likethe traditional diets of Africa, Asia,and the Mediterranean. This styleof eating is rich in whole grains,whole fruits, and green vegetables,incorporates low to modest amountsof protein, and is high in "good fats"from sources such as sesame seeds,walnuts, almonds, and olives.Moderate amounts of high-fibercarbohydrates and "good fats" pre-dominate in traditional diets of theMediterranean, Asia, and Africa.
Randomized clinical trials haveshown that this type of diet may bebest for people at risk for metabolicdisease. For example, a trial inpatients with type II diabetes melli-tus showed better blood sugar
control and cholesterol levels inpeople consuming a diet comprising40% carbohydrates, 45% fat. and15% protein compared to those whoconsumed a diet consisting of 55%carbohydrates, 30% fat, and 15%protein.''
In other studies, a diet moderatein carbohydrates and relatively highin monounsaturated fat from oliveoil and polyunsaturated fat fromfish—such as the Mediterraneandiet—actually decreased insulinresistance and inflammation.'" Fur-thermore, this diet is better thanthe step I National CholesterolEducation Program (NCEP) diet inpreventingheart disease and stroke."
Second, if you are not physicallyactive, start moving your body! Sim-ply walking at a brisk pace three tofive days each week for at least 20minutes will help. If and when youget more ambitious, you can engagein more demanding physical activi-ties at a higher level of exertion. Inaddition, consider weight training tobuild more muscle mass and to stim-ulate your metabolism.
Step 3: Improve Metabolic Functionwith Nutritional Supplements.
Smart supplementation can havea significant impact on metabolichealth. A number of nutritionalsupplements hold great promise fornormalizing blood sugar andmetabolic control.
Chromium, Chromium is a criti-cally essential cofactor for glucosecontrol. Chromium helps insulinshuttle blood sugar (glucose) intocells. In fact, without chromium,insulin cannot work properly.Unfortunately, most Americans aredeficient in this critical nutrient.Some experts believe that Americansingest less than half the recom-mended daily amount of chromi-um.'- This may be partly due to thenation's over-reliance on processedfoods, which are generally rich incalories but poor in nutrients.
Another factor contributing towidespread chromium deficiency isfood grown in soil containing a lowcontent of minerals such as chromi-um. In fact, the 1992 Earth Summit
58 LIFE EXTENSION July 2006

report showed that North Americansoils have been depleted of 85% oftbeir mineral content in tbe past 100years—the highest rate of mineraldepletion in the world.'' Thus, itshould come as no surprise that thefoods we consume are deficient intrace minerals such as chromium.Some scientists have postulated thatrising rates of metabolic syndromeand diabetes in the US may result inpart from declining levels of chromi-um in American soil and diets.
Many clinical studies of patientswith and without metabolic diseasehave shown metabolic benefits-including improved blood sugarcontrol, cholesterol, and insuhn—with supplemental chromium dosesfrom 200 to 1000 meg daily.'' '•
Recently, a bioavailable andbiologically safe form of chromiumcalled chromium 454'" has attract-ed the attention of nutritionalscientists seeking ways to promotemetabolic health. Derived fromplant and biological extracts, thisdistinct form of chromium is watersoluble, allowing for outstandingabsorption. Insulin-deficient dia-betic rats tbat received chromium454" for three weeks demonstratedan impressive 38% reduction inblood glucose levels. These find-ings led scientists to suggest thatchromium may provide metabolicsupport for individuals seekingto optimize their blood glucoselevels.'"
DHEA. In both middle-aged andolder men and women, suboptimalhormone profiles are not unusual.Dehydroepiandrosterone (DHEA) isa critical hormone that is involved inmany metabolic processes, bothdirectly and indirectly (through itsconversion to testosterone andestrogen).
Low levels of DHEA are associatedwith an increased risk of developingmetabolic syndrome. For example,a cross-sectional study of 400 men,aged 40-80, showed that the lowerthe DHEA level, the greater the riskof insulin resistance and metabolicsyndrome.'''
DHEA dosing should be individ-ualized based on blood testing.A simple blood test known asDHEA-sulfate (DHEA-S) will pro-vide important information aboutyour DHEA levels. However, evenrelatively low doses can providebenefit. A study of elderly men andwomen sbowed that a daily doseof as httle as 50 mg of DHEA forsix montbs was associated with sig-nificant fat loss and improvementsin insulin sensitivity.-"
DHA/EPA.The long-chain omega-3 fatty acids docosahexaenoic acid(DHA) and eicosapentaenoic acid(EPA) have a multitude of healthbenefits, including increased fatburning and improved glucosemetabolism." In addition, EPA andDHA decrease the expression ofgenes involved in fat storage,-- down-
regulate genes involved in inflamma-tion/' and lower levels of C-reactiveprotein, a marker of inflammation.^'
Be careful, however, if you con-sume large amounts of fish, as youmay be unwittingly ingesting largeamounts of mercury, a kidney toxinthat is found in high amounts in fishsuch as swordfish, shark, and eventuna.-^^" Supplementing with ahigh-quality omega-3 fatty acidproduct that has been tested andfound to be free of contaminants andpollutants is a smart alternative toeating mercury-contaminated fisb.
Bioflavonoids. Inflammation isan important factor in the develop-ment of insulin resistance andmetabolic syndrome.--" Bioflavo-noids like quercetin, resveratrol, andolive polypbenols bave natural anti-inflammatory properties and mayoffer protection against metabolicsyndrome.
Quercetin, a potent bioflavonoidfound in vegetables, inhibits pro-inflammatory cytokines (proteinsinvolved in immunity and inflamma-tion).'"' Resveratrol, found in the skinof red fruits like grapes, has beenshown to inhibit the expression ofgenes involved in inflammationbetter than the potent prescriptioncorticosteroid dexamethasone.'"
In addition to having potentanti-inflammatory effects," olivepolyphenols have beneficial benefitson the cardiovascular system. Stud-ies show that olive polyphenols dra-matically increase the resistance of
July 2006 LIFE EXTENSION 59

GREEN TEA'S REMARKABLEMETABOLIC BENEFITS
Green tea is a super-nutrient. LifeExtension members have long knownabout the anti-cancer benefits of greenfea rich in epigallocafechin gallate(EGCG). Green tea also has valuablemefabolic advantages.
Green tea promotes healthy bloodsugar (glucose) mefabolism in humansand obese, diabetic mice withoutincreasing insulin levels.^' Life Extensionhas long warned abouf the dangers ofexcess insulin levels. Green tea rich inEGCG enhances insulin acfion instead ofpromoting insulin release." Furthermore,green tea and EGCG reduce fat cellcreation and growth, as well as bloodlevels of triglycerides and cholesterol.^"
As an added bonus, green tea protectsagainst protein oxidation and glycafion(fhe process by which tissues becomedamaged by high levels of circulatingblood glucose).^^
cholesterol to oxidation. ^ This is veryimportant, as oxidized cholesterolserves as a trigger for atherosclerosis(hardening of the arteries)." Olivepolyphenols also benefit the vascularendothehum, the hning of bloodvessel walls. Hydroxytyrosol, a prin-cipal polyphenol in olives, reducesthe "stickiness" of cells in the vascu-lar endothelium/" Cell "stickiness"may increase the tendency to formblood clots in the arteries.
Carotenoids and retinuids.Carotenoids (found in foods likecarrots, squash, and tomatoes) andretinoids, which are beneficial to eyehealth, also play an important rolein preventing metabolic disease.
Interestingly, experiments in earlygrowth and development show thatlow vitamin A intake decreasesinsulin-producing cells,'' pointingto the importance of adequate vita-min A intake for development ofthe insulin-producing cells of thepancreas.
The National Health and NutritionExamination Survey found that evenafter adjusting for confoundingfactors like age, sex, ethnicity, educa-tion, smoking status, and physical
activity, people with metabolicsyndrome had significantly lowerconcentrations of carotenoids andretinyl esters (a type of vitamin A). "
Evidence suggests that there maybe a threshold for vitamin Aconsumption in terms of metabolicbenefit. In one study, daily vitaminA intake of more than 10,000 IU sig-nificantly lowered blood sugar andinsulin levels in healthy humanvolunteers, while daily intake ofless than 8000 IU was associatedwith higher blood sugar levels."
Water-soluble cinnamonextracts. Exciting data show that aspecial extract from cinnamon holdstremendous promise for normaliz-ing blood sugar levels naturally.
A 2003 study of patients withtype II diabetes examined theeffects of cinnamon on blood sugar.Participants received one, three, orsix grams per day of cinnamon orplacebo. After 40 days, the threegroups receiving cinnamon demon-strated significant reductions inblood sugar of up to 29%, in triglyc-erides of up to 30%. and in choles-terol of up to 26%/*
So, all you need to do to preventmetabolic disease is consumelarge amounts of cinnamon, right?Wrong!
Whole cinnamon containsvolatile oils, which are well-knownirritants that may trigger allergicreactions. Even more worrisome isthat toxicology studies in mice showthat consuming raw cinnamon rich
in these oils can cause tumors,including squamous cell papillo-mas." Therefore, the best strategy isto avoid the danger of cinnamon'svolatile oils while still obtaining theremarkable benefits of cinnamon.
Fortunately, these oils are notresponsible for cinnamon's impres-sive effects in stabilizing blood sug-ar. Instead, cinnamon's water-soluble polyphenol polymers are thekey components responsible for itsbeneficial metabolic effects."
The polyphenol type-A polymersfrom cinnamon up-regulate genesinvolved in blood sugar control.''Other cinnamon polyphenol poly-mers such as methylhydroxychal-cone have additional beneficialeffects on blood sugar control.'"Recent studies consistently showthe anti-diabetic effects of cin-namon extracts in validated animalmodels of metabolic disease.''""
Cinnamon extract not onlysupports healthy blood sugar levels,but also has excellent antioxidantproperties. The natural water-soluble cinnamon extract inhibitsoxidation even better than thepowerful synthetic antioxidantbutylated hydroxytoluene, or BHT"
Coffee polyphenois. Who wouldhave ever thought that a water-soluble extract of coffee acts toboost the key target hormone thatmulti-billion-dollar pharmaceuticalcompanies are targeting as the nextbreakthrough treatment for meta-bolic disease?
60 LIFE EXTENSION July 2006

BANABA LEAF OFFERSBLOOD SUGAR SUPPORT
A traditional folk remedy trom South-east Asia, banaba leaf extract may offerpowerful support for people seeking tomaintain healthy blood sugar levels.Banaba {Lagerstroemia speciosa L)contains an active ingredient calledcorosolic acid. Laboratory, animal, andhuman studies show that corosolic acideffectively helps to support optimalglucose metabohsm.^'
Adults with diabetes or impairedglucose metabolism who received coroso-lic acid prior to an oral glucose tolerancetest demonstrated significantly lowerpost-challenge glucose levels than peoplewho did not take corosolic acid.''
A randomized clinical trial showedthat banaba leaf extract rich in corosolicacid benefited adults with type II diabetes.When the diabetic individuals took astandardized corosolic acid supplementeach day for two weeks, their bloodglucose levels decreased by 20-30%,^^
These findings suggest that banabaleaf extract standardized for corosolic acidcontent may benefit the millions ofAmericans who seek support for optimalblood sugar levels.
A very large study (14,629 men andwomen) published in the Journal ofthe American Medical Association in2004 showed that the greater yourcoffee consumption, the lower yourrisk of metabolic disease, includingtype II diabetes mellitus.™ Anothervery large study that followed 41,934men showed a similarly powerfulassociation between increased cof-fee intake and decreased risk oftype II diabetes, even after adjustingfor age, body mass index, and otherrisk factors.^'
Before you decide to drink a potof coffee a day or open your ownStarbucks, be advised tbat drinkinglarge amounts of coffee is not thebest strategy for preventing meta-bolic disease.
Coffee can cause insomnia andmay induce bigb blood pressure insome people, largely due to its caf-feine content. Morever, results of the2004 ATTICA study showed thatcoffee consumption dramatically
increases markers of inflammationlike C-reactive protein, interleukin-6,and tumor necrosis factor-alpha.'^
A smart strategy is to identify andisolate the components of coffee thatare responsible for its beneficialeffects on metabolism, includingblood sugar control. Scientists havefound that water extracts of roastedcoffee residues, including the prima-ry coffee polypbenols caffeic acidand chlorogenic acid, are key compo-nents responsible for coffee's benefi-cial metabolic effects.
Preclinical studies show thatchlorogenic acid improves bloodsugar control and decreases choles-terol and triglycerides.^^
In human studies, chlorogenicacid, a major polyphenol in waterextracts of coffee, has improved therelease of hormones critical to bloodsugar control. For example, inbealthy human volunteers, consum-ing coffee polyphenols like chloro-genic acid dramatically increasedglucagon-like peptide 1 (GLP-1)secretion.^" This finding is remark-able because several GLP-1-relatedpharmaceutical agents are targetingthis hormone as a treatment formetabolic disease, including therecently FDA-approved GLP-1 ana-log BYETTA" (exenatide). Chloro-genic acid acts to increase GLP-1. ^
Coffee extracts offer other benefitsas well. Water-soluble coffeepolyphenols hke chlorogenic acidscavenge free radicals and providepowerful protection against lipidperoxidation and oxidative damageby proteins."
CONCLUSION
With so much focus on choles-terol, little attention has been paid tothe critical role of insulin resistancein the development of cardiovasculardisease. Insulin resistance is the rootcause of metabolic syndrome, a seri-ous risk factor for heart disease andstroke that has received little atten-tion until recently.
Identifying your risk for metabol-ic syndrome involves only a series ofvery simple tests. If you are found tobe at risk, decreasing your body fat—particularly around your waist^is
critically important. Avoid fad diets,eat a wbole-food diet like those con-sumed by Mediterranean cultures,and get some physical exercise—your body will thank you for it!
Nutritional supplements can helpimprove blood sugar control andmetabolic healtb naturally, withoutdanger or stress to your body. Partic-ularly compelling are polyphenol-rich, water-soluble extracts ofcinnamon and coffee, along withgreen tea extract, chromium, andbanaba leaf-derived corosolic acid.Documented evidence demon-strates the ability of these agents tobelp normalize blood sugar levels.
Avoiding tbe perils of metabohcsyndrome is simple. First, get testedto see whether you are at risk. If lab-oratory testing and a physicalexamination reveal that you are atrisk, immediately take the neces-sary steps—including exercise, ahealthy diet, and targeted nutri-tional strategies—to prevent thedire cardiovascular consequencesof insulin resistance and metabolicsyndrome. •
SEVERAL SUPPLEMENTSFOR SUPPORTING OPTIMAL
BLOOD SUGAR (GLUCOSE) LEVELS
DHEA:10-50 mg daily to start (men);10-30 mg daily to start (women).Assess the effects of supplementa-tion via repeat blood tests,EPA:1400 mg daily;DHA: 1,000 mg daily.Take with meals. Double these dosesto combat high triglyceride levels.Mixed bioflavonoids:1400 mg twice daily.Vitamin A:4000 lU daily; mixed carotenoids(for example, lutein: 15-20 mg daily;lycopene: 3-30 mg daily;zeaxanthin: 3-10 mg daily)Water-solubte cinnamon extract:125 mg three times daily,30 minutes before meals.Chromium:400-800 meg daily.
July 2006 LIFE EXTENSION 61

PHARMACEUTICAL OPTIONS FOR METABOLIC SYNOROME
Drug companies are keenly interested in developing new drug treatments for peoplewith metabolic syndrome. Unfortunately, due to the overwhelming drive by multibillion-dollarpharmaceutical companies to continually make profits, one of the very best drugs to helpincrease insulin sensitivity and improve blood sugar control (without promoting weight gain)is rarely mentioned. This drug, metformin, is currently off patent and very cost-effective.
Metformin. which belongs to a class of drugs called biguanides, works in several differentways to improve insulin's ability to work at the cellular level in tissues such as muscle andthe liver. Metformin is not associated with weight gain—a major advantage over all otherdrugs used to treat diabetes. Of additional interest is that gene-chip research funded byLife Extension showed that metformin influences gene expression in ways similar to those ofcaloric restriction. This suggests that metformin may have potential anti-aging benefits inaddition to its documented effects on blood sugar control.
Other currently available drugs that may be useful in treating metabolic syndromeinclude the thiazolidinediones. a class of drugs approved for the treatment of diabetes.Thiazolidinediones include GlaxoSmithKline's rosiglitazone (Avandia®) and Takeda/Eli Lilly'spioglitazone (Actos®). Thiazolidinediones work by targeting PPARs (peroxisome proliferator-activated receptors), which are attractive drug targets for treating metabolic disease.PPARs help regulate the expression of genes involved in the storage and use of dietary fats.Two subtypes, PPAR alpha and PPAR gamma, have insulin-sensitizing effects.
Among the new drugs in development for metabolic syndrome are AstraZeneca'stesaglitazar, and Bristol-Myers Squibb's muraglitazar.
Individuals with kidney disease should not use metformin. Rosiglitazone (Avandia®) andpioglitazone (Actos®) should not be used by people with a history of congestive heart failureor liver disease. Please consult your doctor before using any pharmaceutical drug to treatmetabolic syndrome.
McLaiighlin T, Abbasi H Cheat K, ei ill. Use ofmetabolic markers to identity' overweightindividuals who are insulin resistant. AnnIntern Med. 2003 Nov 18;13i)(101:R02-9.Ford ES, Giles WH, Dietz WH. Prevalence ofthe metabolic syndrome among US adults:findings from tbe third National I lealth andNutrition Examination Survey. lAMA. 2002Ian 16;287(3):35(i-9.
Reaven GM. Syndrome X: 6 years later. /Intern Med Siippl. 1994;736:13-22,Eckel RI I. Grundy SM, Ziminet PZ. Themetabolic syndrome. Lancet. 2005 Apr16;36n[9468):1415-28.l-akka HM. Laaksonen DE. Lakka TA, el al.The metabolic syndrome and total and car-diovascular disease mortality in tniddle-agedmen./,4MA2002Dec4;288(21):2709-16.Anon. Third Report of the National Choles-terol Education Program (NGEP) Expert Pan-el on Detection, Evaluation, and Treatmentof High Blood Cholesterol in Adults (AdultTreatment Panel 111) final report. CircnUirlon.2002 Dec 17;IO(){25):3143-42I.De LA, Petrnni ML, De Luca PR et al. Use ofquality control indices iti moderatelyhypocaloric Mediterranean diet for treat-ment or obesity. Diabeies Nutr Metab. 2001Aug;14(4):181-8.
Castagnetta L, Granata OM. Cusimano R, etal. Tbe Mediet Project. Ann NYAcad.Sci.2002 Iun;9fi3:282-9.
9. Cben YD, Coiilston AM, Zhou MY, Hollen-
beck CB, Reaven GM, Wby do low-fat bigh-
carbobydrate dieis accentuate postprandial
lipemia in patients vvitb NIDDM? Diabetes
Care. 1995 Jan;IR(]l:10-6.
10. Esposito K, Marfella R, Ciotola M, et al.
Effect of a mediterranean-siyle diet on
endotbelial dysfunction and markers of vas-
cular inflammation in the tiietaboiic syn-
drome: a randomized trial. JAMA. 2004 Sep
22;292(12):]440-6.
11. Singb RB, Dubnov G, Niaz MA, et al. Effect of
an Indo-Mediterranean diet on progression
of coronary artery disease in bigb risk
patients [Indo-Mediterranean Diet Heart
Study): a randomized single-blind trial.
Lancet. 2002 Nov 9;.160[9344):1455-61.
12. Anderson RA. Essentiality of chromium in
bumans. Sci Total Ent'iron. 1989 Oct 1:
86(l-2):75-8l,
13. Available at: bttp://www,eartbsummit.info.
Ac-cessed Marcb 9, 2006.
14. Andfrson RA, Cbeng N, Bryden NA, et al.
Hlevated intakes of supplemental chromium
improve glucose and insulin variables in
individuals with lype 2 diabetes. Diabetes.
1997Nov;46[il):1786-91.
\5. Babijri SM, Mufti AM. Beneficial effects of
cbromium in people with ty|ie 2 diabetes,
and urinary cbromium response to glucose
load as a possible indicator of status. Biol
Trace Elem Res. 2002 Feb;85(2);97-109.
16. Babijiri SM, Mira SA, Mufti AM, AjabnoorMA. Tbe effects of inorganic cbromitim andbrewer's yeast supplementation on glucosetolerance, serum lipids and drug dosage inindividuals with type 2 diabetes. Saudi Medy.2000Sep;21(9):831-7.
17. Wilson BE, Gondy A. Effects of chromiumsupplementation on fasting insulin levelsand lipid parameters in healthy, non-oheseyoung subjects. Diabetes Res Clin Praci. 1995Jun;28(3): 179-84.
18. Machalinski B, Walczak M, Syrenicz A, et al.Hypoglycetiiic potency of novel trivalentcbromium in byperglycemic insulin-defi-cieni rats. / Trace Elem Med Biol.2006;20(l):33-9,
19. Muiler M, Grobbee DE, den T, I, LamhertsSW, van der Schouw Y"f. Endogenous sexhormones and metabolic syndrome in agingtnen. / Clin Endocrinol Metab. 2005May;90(5):26ia-23,
20. Villareal DT, Holloszy )0. Effect of DHHA onabdominal fat and insulin action in elderlywomen and men: a randomized controlledtrial.MMA 2004 Nov 10;292(18):2243-8.
21. Eerre ?. Tbe biology of peroxisome prolifera-tor-activated receptors: relationship vvitblipid metabolism and insulin sensitivity.Diabeles. 2004 Eeb;53 SuppI 1S43-S50,
22. Delarue I, LeFoll C, Corporeau C, Lucas D,N-3 long cbain polyunsaturated fatty acids:a nutritional tool to prevent insulin resis-tance associated to t>'pe 2 diabetes and obe-sity? Reprod Niiir Dev. 2004 May;44(3):289-99,
23. Li H, Ruan XZ, Powis SH, et al. EPA and DHAreduce LPS-induced inflammation respons-es in HK-2 cells: evidence for a PPAR-gam-ma-dependent mechanism. Kidney Int. 2005Mar;67(3):Rfi7-74.
24. Madsen T, Skou HA, Hansen VE, et al. C-reactive protein, dietary n-3 fatty acids, andthe extent of coronary artery disease.
Am ; CardioL 200\ Nov ]r);88(10):ll39-42,25. Foran SE, Flood JG, Lewandrowski KB. Mea-
surement of mercury levels in concentratedover-tbe-counter fisb oil preparations: is fishoil bealthier tban fisb? Arch Parhol Lab Med.2003Dec;127fl2):]603-5.
26. Burger I. Stern AH, Gocbfeld M, Mercury incommercial fish: optitnizing individualcboices to reduce risk. Environ HealthPerspect. 2005 Mar:l 1313):2(i6-71.
27. Savage DB, Petersen KF, Sbulman Gl. Mecb-anisnis of insulin resistance in bumans andpossible links with inflammation.Hypertension. 2005 May:4515):828-33.
28. Perseghin G. Petersen K, Shulman GL Gellu-lar mechanism of insulin resistance: poten-tial links vvitb inflammation. //;/ / Obes RelatMetab Disord. 2003 Dec;27 Suppl 3S6-11.
29. Comalada M, Camuesco D, Sierra S, et al. Invivo quercitrin anti-inflammatory effectinvolves release of quercetin, vvbicb inhibitsinflammation tbrougb douni-regulation oftbe NF-kappaB pathway. Bur / Immunol.2005 Feb:35f2):584-92.
30. Donnelly LE, Newton R, Kennedy GE, et al.Anti-inflammatory effects of resveratrot inlung epitbelial cells: tnolecular mechanisms.Am 1 Physiol Lung Cell Mol Physiol. 2004Oct;287(4):L774-83.
62 LIFE EXTENSION July 2006

:i 1. Martinez-Dominguez I-, de la PR, Ruiz-Gutierrez V. Protective effects upon experi-mental inflammation models of apolyphenol-supplemented virgin olive oildiet. Inflamm Res. 2001 Feb:50(2): 102-6.
32. Tsuneki H, Ishizuka M, Terasawa M, Wu |B,Sasaoka T, Kimura 1. Effect of green tea onblood glucose levels and serum proteomicpatterns in diabetic (db/db) mice and onglucose metabolism in healthy humans.BMC Pharmacol. 2004 Aug 26;4:18.
33. Anderson RA, Polansky MM. Tea enhancesinsulin activity. / Agric Food Chem. 2002 Nov20;50(24):7182-6.
34. Wolfram S, Wang Y, Thielecke F Anti-obesityeffects of green tea: from bedside to bencb.Mol Nurr Food Res. 2006 Feb;50(2):176-87.
35. NakagawaT, YokozawaT, Terasawa K, Sbu S,luneja LR. Protective activity of green teaagainst free radical- and glucose-mediatedprotein damage, / Agric Food Chem. 2002Apr 10;50(8):2418-22.
36. Wiseman SA, Matbot IN, de Fouw N|,Tijburg LB, Dietary non-tocopherol antioxi-dants present in extra virgin olive oilincrease the resistance of low densitylipoproteins to oxidation in rabbits.Atherosclerosis. 1996 Keb;120(l-2):15-23,
37. Sies H, StabI W, Sevanian A. Nutritional,dietary and postprandial oxidative stress,JNutr. 2005 May:135(5):969-72,
38. Garluccio MA, Siculella L, Ancora MA, et al.Olive oil and red wine antioxidant polypbe-nols inhibit endothelial activation:antiatberogenic properties of Mediterraneandiet phytocbemicals. Arterioscler ThrombVflirB/o/. 2003 Apr l;23(4):622-9.
39. Mattbews KA, Rboten WB, Driscoll HK,Cbertow BS, Vitamin A deficiency impairsfetal islet development and causes subse-quent glucose intolerance in adult rats.JNutr. 2004 Aug;134(8):1958-63.
40. Ford ES, Mokdad AH, Giles WH, Brown DW.The metabolic syndrome and antioxidantconcentrations: findings from the IbirdNational Healtb and Nutrition ExaminationSurvey Diabetes. 2003 Sep;52(9):2346-52.
41. Faccbini FCoulstonAM, Reaven GM,Relation between dietary vitamin intake andresistance to insulin-mediated glucose dis-posal in healtby volunteers. Am J Clin Niiir.l99K)un;63{6):946-9.
42. Kban A, Safdar M, Ali Khan MM, KhattakKN, Andersoti RA, Cinnamon improvesglucose and lipids of people witbtype 2 diabetes. Diabetes Care. 2003Dec;26(12):3215-8,
43. Balacbandran B, Sivaramkrisbnan VM.Induction of tumours by Indian dietaryconstituents. Indian J Cancer. 1995Sep;32(3):104-9.
44. Anderson RA, Broadburst CL, Polansk>' MMet al. Isolation and cbaracterization ofpolypbenol type-A polymers from cinnamonwitb insulin-like biological activity. J AgricFood Chem. 2004 |an 14;52(l):65-70.
45. Imparl-Radosevich I, Deas S, Polansky MM,et al. Regulation of PTP-1 and insulin recep-tor kinase by fractions from cintiamon:implications for cinnamon regulation ofInsulin signalling, Horni Res. 1998Sep;50(3):17?-82,
46. Jarvill-Taylor K], Anderson RA, Graves D|. Ahydrox\'cbalcone derived from cinnamonfunctions as a mimetic for insulin in 3T3-L1adipocytes. JAm Colt Nuir. 2001Aug;20[4):327-36.
47. Qin B, Nagasaki M, Ren M, et al. Cinnamonextract prevents tbe insulin resistanceinduced by a high-fructose diet. HormMetab Res. 2004 Feb:36[2):l 19-25.
48. Kim SH, Hyun SH, Cboung SY. Anti-diabeticeffect of cinnamon extract on blood glucosein db/db mice, / F.thnopharmacol. 2006 Mar8;104ll-2):tl9-23.
49. Mancini-FilboJ.Van-Koiij A, Mancini DA,Cozzolino FF Torres RP Antioxidatit activityof cinnamon (Cinnamomum Zeytanicum,Breyne) extracts. Boll Chim Farm. 1998Dec;137[ll):443-7.
50. Tuomilehto ], Hu G, Bidel S, Lindstrom J,Jousilabti H Coffee consumption and risk oftype 2 diabetes mellitus among middle-agedI-innisb men and women. JAAIA. 2004 Mar10;291(10):1213-9,
51, Fukushima M, Matstiyama F, Ueda N, et al.Effect of corosolic acid on postchallenge glu-cose levels. Diabetes Res Clin Pract. 2006 Mar18; [Epub ahead of printi
52, ludyWV, HariSP, StogsdillWW, ludylS,NaguibYM, Passwater R. Antidiabetic activi-ty of a standardized extract (Glucosol) fromLagerstroemia speciosa leaves in Type I! dia-betics. A dose-dependence study. /Ethriopharmacol. 2003 iuhi^7i]]:l\5-7.
53, Salazar-Martinez E, Willett WC, Ascberio A,et al. Coffee consumption and risk for tyjie 2diabetes mellitus. Ann Intern Med. 2004 [an
54. Zampelas A, Panagiotakos DB, Pitsavos G,Ghrysoboou C, Stefanadis G. Associationsbetween coffee consumption and inflamma-tory markers in healthy persons: the ATTICAstudy Am I Clin Nutr. 2004 Oct;80(4):862-7,
55. Rodriguez de Sotillo DV Hadley M. Cbloro-genic acid modifies plasma and liver con-centrations of: cholesterol, triacylglycerol,and minerals in (fa/fa) Zucker rats. / NuirBiochem. 2002 Dec;U{l2):7n-2ti.
56. lohnston KL, Clifford MN, Morgan LM.Coffee acutely modifies gastrointestinalhormone secretion and glucose tolerancein bumans: glycetnic effects of chlorogenicacid and caffeine. Am J Clin Nutr. 2003Oct;78(4):728-33.
57. McCarty MF. A chlorogenic acid-inducedincrease in GLP-1 production may mediatetbe impact of beavy coffee consumption ondiabetes risk, Med Hypotheses.2005;6414):848-53.
58. Yen W|, Wang BS, Cbatig LW, Dub PD.Antioxidant properties of roasted coffeeresidues. J Agric Food Chem. 2005 Apr6;53(7):2658-63,
July 2006 LIFE EXTENSION 63