LPCA - HIE Handouts - Adele - LPCA :: Louisiana Primary ... Value of... · An eHealth Exchange...
13
10/5/2015 1 The Value of Interoperability Adele Allison, Director of Provider Innovation Strategies October 7, 2015 The enclosed materials are highly sensitive, proprietary and confidential. Please use every effort to safeguard the confidentiality of these materials. Please do not copy, distribute, use, share or otherwise provide access to these materials to any person inside or outside DST Systems, Inc. without prior written approval. This proprietary, confidential presentation is for general informational purposes only and does not constitute an agreement. By making this presentation available to you, we are not granting any express or implied rights or licenses under any intellectual property right. If we permit your printing, copying or transmitting of content in this presentation, it is under a non‐exclusive, non‐transferable, limited license, and you must include or refer to the copyright notice contained in this document. You may not create derivative works of this presentation or its content without our prior written permission. Any reference in this presentation to another entity or its products or services is provided for convenience only and does not constitute an offer to sell, or the solicitation of an offer to buy, any products or services offered by such entity, nor does such reference constitute our endorsement, referral, or recommendation. Our trademarks and service marks and those of third parties used in this presentation are the property of their respective owners. 2 Disclaimer The Value of Interoperability • Activity • Building Blocks • Use Cases • New Developments • Questions
Transcript of LPCA - HIE Handouts - Adele - LPCA :: Louisiana Primary ... Value of... · An eHealth Exchange...

10/5/2015
1
The Value of InteroperabilityAdele Allison, Director of Provider Innovation Strategies
October 7, 2015
The enclosed materials are highly sensitive, proprietary and confidential. Please use every effort to safeguard theconfidentiality of these materials. Please do not copy, distribute, use, share or otherwise provide access to these materials toany person inside or outside DST Systems, Inc. without prior written approval.
This proprietary, confidential presentation is for general informational purposes only and does not constitute an agreement. Bymaking this presentation available to you, we are not granting any express or implied rights or licenses under any intellectualproperty right.
If we permit your printing, copying or transmitting of content in this presentation, it is under a non‐exclusive, non‐transferable,limited license, and you must include or refer to the copyright notice contained in this document. You may not create derivativeworks of this presentation or its content without our prior written permission. Any reference in this presentation to anotherentity or its products or services is provided for convenience only and does not constitute an offer to sell, or the solicitation ofan offer to buy, any products or services offered by such entity, nor does such reference constitute our endorsement, referral,or recommendation.
Our trademarks and service marks and those of third parties used in this presentation are the property of their respectiveowners.
2
Disclaimer
The Value of Interoperability
• Activity
• Building Blocks
• Use Cases
• New Developments
• Questions
10/5/2015
2
Interop and Workflow Redesign
4
Use Technology as a Change
Agent!
The Value of Interoperability
• Activity
• Building Blocks
• Use Cases
• New Developments
• Questions
• Narrative Text− Examples: Cut/Paste Dictation, Voice Recognition, Typing
− Pro: Personalizes patient encounter information, “Say it the way you want”
− Con: Not machine readable, no conducive to research and reporting
• Structured, User‐Defined Fields− Examples: Customizable Drop‐down Lists
− Pro: Customizable, reportable within organization
− Con: Not conducive to aggregated research and reporting
• Codified, Object‐Oriented Data− Examples: ICD, CPT, SNOMED, LOINC
− Pro: Machine readable, consistent across country or world, very
researchable and reportable
− Con: Rigid structure, hard to personalize to individual patient
3 Essential Types Of Data Capture
10/5/2015
3
Machines Read in Code
7
• Definition:− Standardized, machine‐readable
terms
− Describes clinical problems,
procedures and other information
− Coded for easy comprehension
and consistency
Meaningful Use Defined
Vocabularies/Code Sets
Best Practice: Use codified
data capture for reporting
Block 1: Vocabulary and Code Sets
8Adapted from HHS Interoperability Basics at
http://www.healthit.gov/public‐course/interoperability‐basics‐training/HITRC_lsn1069/wrap_menupage.htm
Code Sets Used to Define …
OMB Standards
Race, Ethnicity
ISO 639‐2 Alpha‐3
Preferred Language
SNOMED CT Smoking Status
ICD or SNOMED CT
Problems
HCPCS and CPT
Procedures
RxNormMedications and Medication Allergies
LOINC Lab tests, values and results
CVX Immunizations
Block 2: Content Structure
9
• Definition:− Message format/architecture specific to the digital environment
− Delineates the information contained in the message
− Defines the structure of the information to be exchanged
− Allows disparate machines to communicate
• Used in interop and interfaces
• Examples:− HL7 2.5.1 format for Lab Results
− Clinical Document Architecture (CDA) for Care Summaries, Care Plans
− Admission, Discharge and Transfer (ADT) for Demographics
• 2014 Edition EHR Testing and Certification helps insure
capabilities, compliance

10/5/2015
4
CCDA
MU2 Consolidated CDA Template
• MU2 sets forth “Clinical Concepts”
Content Structure (Block 1)
• CCDA is the document “Template”
that must be used (Block 2)o Standardizes how “Clinical Concepts”
(Words) are used / re‐used
o Templates put it into a “Package”
o Packages are arranged to create a
clinical “Document” that is purpose‐
oriented
DemographicsMedications
AllergiesProblems
Lab ResultsVitals
Smoking Status
Procedures
2014 Edition CEHRT
EHR Data Captured
• Humans read in document format → CCD
• Machines read in code → CDA
Human vs. Machine Readable Data
EHR ‐ A EHR ‐ B
Problems
Problems
Meds
Meds
Smoking
Smoking
Human vs. Machine Readable Data
EHR ‐ A EHR ‐ B
Problems
Problems
Meds
Meds
Smoking
Smoking
10/5/2015
5
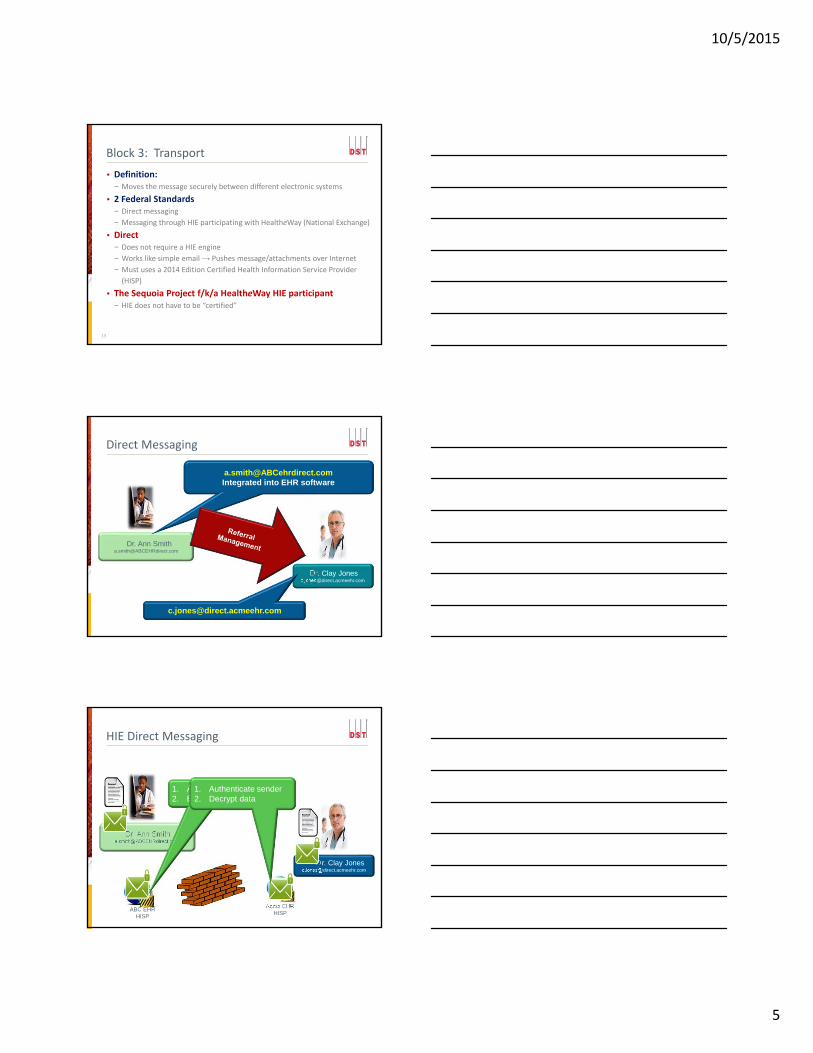
Block 3: Transport
13
• Definition:− Moves the message securely between different electronic systems
• 2 Federal Standards− Direct messaging
− Messaging through HIE participating with HealtheWay (National Exchange)
• Direct− Does not require a HIE engine
− Works like simple email → Pushes message/attachments over Internet
− Must uses a 2014 Edition Certified Health Information Service Provider
(HISP)
• The Sequoia Project f/k/a HealtheWay HIE participant− HIE does not have to be “certified”
Direct Messaging
Dr. Clay [email protected]
Dr. Ann [email protected]
[email protected] into EHR software
HIE Direct Messaging
Dr. Clay [email protected]
Dr. Ann [email protected]
ABC EHRHISP
Acme EHRHISP
1. Authenticate recipient2. Encrypt data
1. Authenticate sender2. Decrypt data

10/5/2015
6
HealtheWay Alternative
HealtheWayExample
1.EHR generates CCDA2.EHR sends CCDA to eHealth Exchange Participant3.eHealthExchangeParticipant sends to Provider B
Provider AProvider B
CEHRT
eHealth Exchange Participant(formerly NwHIN Exchange)
An eHealth Exchange Participant does not have to be certified in order for Provider A’s transmissions to count for MU.
However, Provider A must still use CEHRT to generate a standard summary record in accordance with the CCDA.
• Ensures that health information is safe, secure and private
• Facilitates trusted exchange over something insecure →Internet− Locates health information exchange participants
− Uses registration and certificate authorities
− Managed by the HISP
Block 4: Security Services
17
The Value of Interoperability
• Activity
• Building Blocks
• Use Cases
• New Developments
• Questions
10/5/2015
7
=
User Satisfaction with Technology…
=
20
Done right, interoperability should bevery underwhelming!
Moving Data Between Systems
• 3 Ways to Move Data
• Point‐to‐Point→Interface / Direct
− When does it add complexity?
− When does it make sense?
PCP

10/5/2015
8
• 2 Ways to Move Data
• Point‐to‐Point→Interface / Direct
− When does it add complexity?
− When does it make sense?
PCP• Health Information
Exchange (HIE)
− “Normalizes” Data
− All HIE Participants can communicate
− Requires Participation by stakeholders for “value”
− Emerging Technology
− Typically, Data Repository
HIE
Moving Data Between Systems
• To do what? → Use Case• Provides a Business Model Framework− Step 1 – Identify the Problem (Problem Statement)
− Step 2 – What are the needs? (E.g., Care Coordination, Data
Capture)
− Step 3 – Who has the need? (Actors)
− Step 4 – Map the Solution (To meet needs for each Actor)
− Step 5 – What technology is needed? (E.g., Interface, Direct, HIE)
− Step 6 – Determine Financial and Operational Impact (E.g., Initial
and Ongoing costs, Workflows, etc.)
“I want to connect!”
2. Improve Patient Care Safety
3 Interoperability Guiding Principles
1. Improve Patient Quality of Care
3. Increase Operational Efficiency to
lower clinic costs
Use Case
Guiding
Principles
10/5/2015
9
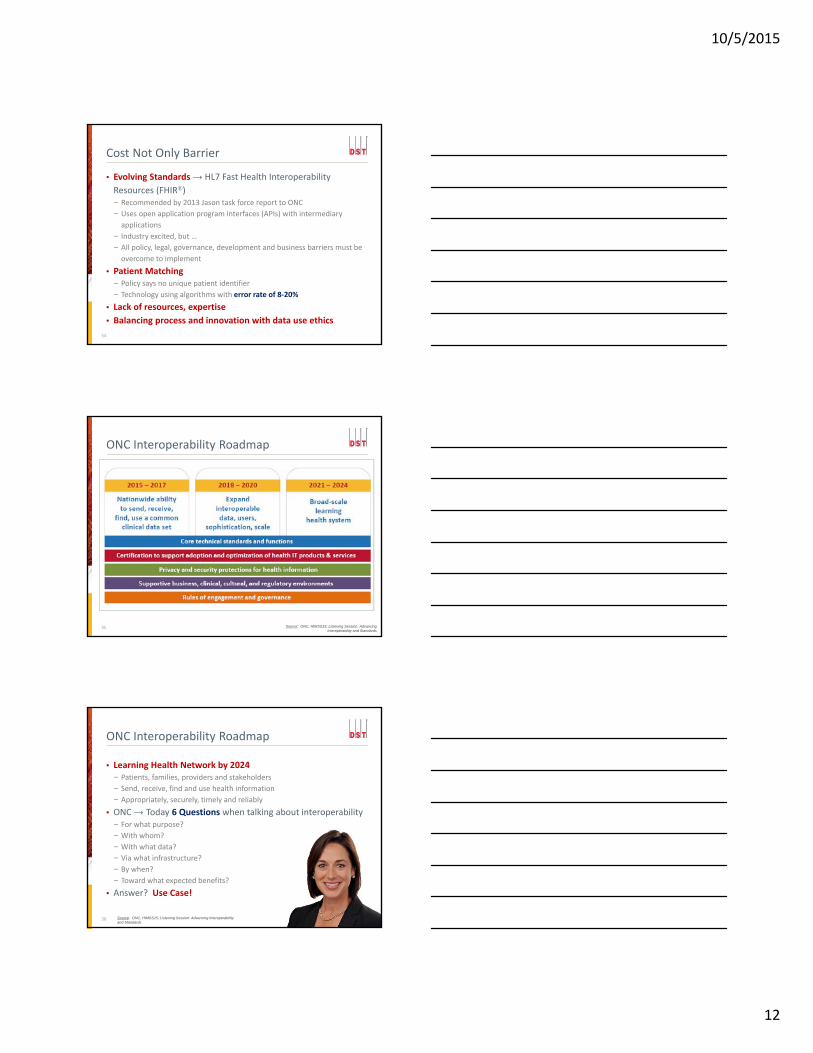
• Referral Management → PCP sends Care Summary to SCP
• Clearly Specify Workflow
• Consider Various Technical Requirements− 2014 Edition CEHRT
− Mechanisms for patient identification / matching
− Multiple Direct addresses?
• Guiding Principles− Quality: Improves privacy/security
− Safety: Timely, reliable and precise communication
− Efficiency: Reduced phone call referrals, awaiting faxes, easily uploaded
PCP Direct Use Case
Use Case Scenarios
Patient Gets Injured PCP Physician
• Cleaning Yard• Pain in calf and knee• Over evening leg swelled• Next day → Fever• Health Home
• Performs I&D• Collects specimen • 48 hours on cultures• Determine sensitivity• Interim Antibiotic• Suspected Spider Bite• Follow‐up in 48 hours• Sooner if problems• Discharged
EHR / HIE
• Antibiotics cross‐referenced in EHR Rx database
• Appropriate Antibiotic• EHR confirms last date of tetanus‐diphtheria
• Avoids unnecessary immunization
Source: ONC Interoperability Basics – www.healthit.gov/providers-professionals/interoperability-training-courses
Quality, Safety,Efficiency
Use Case ScenariosPatient Spikes Fever
• No Follow‐up• Travels with friends• Fever peaks at 104• Ends up in ED• Gets admitted
Hospital Physician
• IV Antibiotics• Fever continues• Unknown etiology• Deep leg pain develops• New culture → +48 hrs• Results needed NOW, or• Surgical excision of infected tissue
EHR / HIE
• HIE used by Hospital• Obtains culture results quickly from PCP
• Susceptibility identified
Quality, Safety,Efficiency
Source: ONC Interoperability Basics – www.healthit.gov/providers-professionals/interoperability-training-courses

10/5/2015
10
Use Case ScenariosPhysician
• Culture shows MRSA• Sensitive to different Antibiotic than using
• Doctor immediately switches
• Rapid improvement • Discharge home
Patient RTW
• What’s MRSA?• Didn’t know it could getso bad!
• Glad my MD got a culture and results
• Need to RTW asap!
EHR / HIE
• MRSA “Notifiable” Dz.• HIE send notice to State Health Dept.
Quality, Safety, Efficiency
Source: ONC Interoperability Basics – www.healthit.gov/providers-professionals/interoperability-training-courses
The Value of Interoperability
• Activity
• Building Blocks
• Use Cases
• New Developments
• Questions
• $30 Billion in federal HITECH funding
• 2014 ONC received 60 unsolicited reports of “Information
Blocking”− Dominant complaint was cost
− Examples:
EHR vendor charging > $2.00/patient/year + transactional fee for Direct
EHR vendor charging $30,000 to interface to HIE in CT
• 113th Congress → Consolidated and Further Continuing
Appropriations Act (enacted Dec. 2014)− Authorizes ONC to de‐certify any EHR vendor found practicing
“information blocking”
• HIMSS15 Conference – Vendor Announcements− athenahealth and Epic to eliminate fees
Warning Against “Information Blocking”
30
10/5/2015
11
• Fast Healthcare Interoperability Resources (FHIR®)• HL7 Interoperability Standard− Leverages “Resources” a/k/a “Models” → E.g., Patient, Condition, Procedure,
Medication, Appointment, etc.
− Resource = Properties → E.g., DOB, Gender, Name under the Patient Resource
− Resources are bundled with related resources
• Resources can be:− Created (HTTP POST)
− Retrieved (HTTP GET)
− Updated (HTTP PUT)
− Removed (HTTP DELETE)
FHIR®
31 Source: Orion Health, White Paper, FHIR ignites healthcare sharing, Dr. David Hay, Mar. 31, 2015, http://ehidc.org/resource-center/white-papers/2015-03-31-FHIR-Ignites-Healthcare-Sharing.pdf
• FHIR uses Application Programming Interfaces (APIs) → Tells
computers how to locate and exchange Resources
• Some Key Benefits− Removes some cost barriers
− Speedy to Implement
− Adaptable to changing requirements
− No vendor “lock‐in” due to no proprietary interfaces
− Support mobile, device and Internet technologies
• Only a draft interop standard today, even though broadly supported− Strong industry enthusiasm
− No regulatory requirement
− Not prominent in tech vendor’s near‐term product roadmaps
− 2‐5 year ramp‐up for industry use and availability
FHIR®
32
Sources: Orion Health, White Paper, FHIR ignites healthcare sharing, Dr. David Hay, Mar. 31, 2015, http://ehidc.org/resource-center/white-papers/2015-03-31-FHIR-Ignites-Healthcare-Sharing.pdf;
Chilmark Research, https://www.chilmarkresearch.com/2015/07/23/new-insight-report-on-moving-to-open-platforms-now-available/
FHIR®
33
Condition
Patient
Encounter
Procedure
Practitioner
Diagnostics
Medications
Resources
FHIR
10/5/2015
12
• Evolving Standards → HL7 Fast Health Interoperability
Resources (FHIR®)− Recommended by 2013 Jason task force report to ONC
− Uses open application program interfaces (APIs) with intermediary
applications
− Industry excited, but …
− All policy, legal, governance, development and business barriers must be
overcome to implement
• Patient Matching − Policy says no unique patient identifier
− Technology using algorithms with error rate of 8‐20%
• Lack of resources, expertise
• Balancing process and innovation with data use ethics
Cost Not Only Barrier
34
ONC Interoperability Roadmap
35 Source: ONC, HIMSS15, Listening Session: Advancing Interoperability and Standards
• Learning Health Network by 2024− Patients, families, providers and stakeholders
− Send, receive, find and use health information
− Appropriately, securely, timely and reliably
• ONC → Today 6 Questions when talking about interoperability− For what purpose?
− With whom?
− With what data?
− Via what infrastructure?
− By when?
− Toward what expected benefits?
• Answer? Use Case!
ONC Interoperability Roadmap
36 Source: ONC, HIMSS15, Listening Session: Advancing Interoperability and Standards
10/5/2015
13
• CommonWell Health Alliance – Industry‐driven Initiative for
“best practices” in Interoperability− Members include: Allscripts, athenahealth, Cerner, Greenway,
McKesson, Aprima, CVS Caremark, Meditech and others
− Exploring FHIR
• Carequality – Convener and Consensus point for Technical
Specifications− Public‐private, multi‐stakeholder collabration
− Members include: AMA, eClinicalWorks, Cerner, Epic, Greenway, Kaiser
Permanente, Surescripts, Walgreens and others
− Focused in 3 elements
Common rules
Technical Specs Participant Directory
Industry Collaborations
37
Questions?
Thank You!
Adele [email protected]
Follow me on Twitter:www.twitter.com/Adele_Allison