Kuliah Rangkaian Digital Kuliah 6: Blok Pembangun Logika Kombinasional

of 94
Upload
natallia-batuwaelCategory
view
216download
07/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
1/94
GI Tract
Dr.Yanto Budiman. Sp.Rad, M.Kes
Bagian Radiologi FK/RS. Atma Jaya
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
2/94
MODALITIES FOR GI TRACT IMAGING
Plain abdominal film
Intraluminal contrast studies
Ultrasound
CT scan
MRI
ERCP
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
3/94
Plain Abdominal Film
Often the first preliminary test
INDICATIONS
Bowel obstruction Viscus perforation Foreign body ingestion
ADVANTAGES
Easy availability
Low cost
LIMITATIONS Screening modality; usually need another imaging test to confirm d
iagnosis Lack of anatomic detail
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
4/94
4
Plain Abdominal Film
The supine abdominal film
The erect chest film
The horizontal-ray abdominal film:- Left lateral decubitus
- Cross Table
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
5/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
6/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
7/94
7
Plain Abdominal Film
Supine positionAsses:
- The preperitoneal fat line
- The psoas outlines- Distribution of gas
- The calibre of bowel :
N: Calibre of small bowel is 2.5 cm & colon is 5 cm.
- The thickened of bowel wall- Displacement of bowel by soft-tissue masses.
- Calculus
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
8/94Supine
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
9/94
Plain Abdominal Film
NORMAL GAS PATTERN
Stomach
Always
Small Bowel Two or three loops of non-distended bowel
Normal diameter = 2.5 cm
Large Bowel
In rectum or sigmoid almost always
Normal diameter = 5 cm
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
10/94
Gas in
stomach
Gas in a few
loops of
small bowel
Gas in
rectum or
sigmoid
Normal Gas Pattern
Gas in large
bowel
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
11/94
Large vs. Small Bowel
Large Bowel
Peripheral
Haustral markings don't extend
from wall to wall
Small Bowel
Central
Valvulae extend across lumen
Plain Abdominal Film
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
12/94
Small bowel obstruction
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
13/94
13
The erect chest film
Erect
To asses:
- free gas beneath the diaphragm
(pneumo-peritonium)
- air fluid levels
- chest abnormality e.g effusion pleura
Plain Abdominal Film
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
14/94
Plain Abdominal Film
Normal Fluid Level
Stomach
Always (except supine film) Small Bowel
Two or three levels possible
Large Bowel
None normally
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
15/94
Erect Abdomen (normal)
Always
air/fluid level
in stomach
A fewair/fluid
levels in
small bowel
Plain Abdominal Film
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
16/94
Air fluid levels (step ladder sign)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
17/94
The horizontal-ray abdominal film
Erect & left lateral decubitus.
The patients should be in position for
10 min before the film is taken.
To asses :
fluid levels & free gas
Plain Abdominal Film
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
18/94
-Supine - Erect - LLD
Pneumoperitonium
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
19/94
Intraluminal Contrast Examinations
CONTRAST MEDIA
Positive : Barium and iodine containing water soluble contrastmedium (iodograffin).
Negative : air and CO2
Barium Swallow
INDICATION
Esophageal pathologies
Single- or Double-Contrast Upper GI Series / Barium meal
INDICATIONS
Imaging of pharynx, esophagus, stomach, and duodenum
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
20/94
Intraluminal Contrast Examinations
Small Bowel Follow-Through Examination and
Enteroclysis
INDICATIONS
Imaging of small intestinal and ileocecal pathologies
Single- or Double-Contrast Enemas
INDICATIONS
Imaging of the large intestine
Fistulograms and Sinograms
INDICATIONS
for assessment of fistulae and sinus tracts
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
21/94
21
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
22/94
Barium
Esophagogram
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
23/94
Upper GI Series
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
24/94
Small Bowel Follow- Through Examination
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
25/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
26/94
Barium EnemaStudy (Double
Contrast Study) ofLarge Intestine
Descending Colon
Transverse Colon
AscendingColon
Hepatic
Flexure ofColon
Splenic Flexure ofColon
Sigmoid Colon
Rectum
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
27/94
Fistulogram
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
28/94
Abdominal Ultrasound
APPROACHES Superficial
Endoscopic: Assisting probes are used in upper GI, pancreaticobiliary, and colorectal pathologies for staging malignancies
INDICATIONS Gallbladder and hepatic pathology
Delineation and differentiation of intra-abdominal cystic structures
Trauma; FAST (focused abdominal sonography in trauma) is a veryuseful tool in assessment of trauma patients
Emerging role of endoscopic ultrasound in biliary and pancreatic pathologies
Guiding procedures
Dopplerstudies for evaluation of vascular structures
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
29/94
Abdominal Ultrasound
ADVANTAGES
Inexpensive, noninvasive, no contrast
LIMITATIONS
Operator dependent Inferior for assessment of bowel pathology due to artifact
from air
Lack of mucosal detail
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
30/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
31/94
Abdominal CT
INDICATIONS Assessment ofacute abdomen and to rule out conditions such
as acute appendicitis, acute pancreatitis, small bowel obstruction, colitis.
Trauma
CT angiograms for suspected vascular leaks, aneurysm, bowelinfarctions
CT enterography is being used for inflammatory bowel diseases (Crohns disease).
Virtual CT colonoscopy: Not yet a very widely used tool
ADVANTAGES
Excellent cross-sectional imaging modality that provides functional information as well
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
32/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
33/94
Abdominal CT
LIMITATIONS
Availability
Radiation exposure
Expensive
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
34/94
MRI
ADVANTAGES Superior soft tissue detail
Excellent cross-sectional imaging tool for evaluation and
staging of malignancies, especially rectal and esophage
al, inflammatory and obstructive pathologies
DISADVANTAGES
Higher cost
Contraindicated in patients with metallic hardware
Long imaging time/ Claustrophobia
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
35/94
ERCP
Endoscopic, Retrograde Cholangio Pancreatography
Involves introduction of an endoscope into the duodenum
followed by cannulation of the biliary tree.
It is often performed along with papillotomy, which serves
as a therapeutic intervention for biliary calculi and drainage
procedures of obstructed bile ducts.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
36/94
ERCP
INDICATIONS in jaundice of unclear origin and suspected pancreatic e.g chronic
pancreatitis and pseudocysts.
Primary approach for drainage and stenting of benign and malignant
biliary obstruction, the main advantage being that the liver need not be
punctured. If the papilla cannot be cannulated or the obstruction cannot be passe
d with a guidewire, a percutaneous transhepatic approach may be trie
d. However, in difficult and postoperative cases, noninvasive methods
such as magnetic resonance cholangiopancreatography (MRCP) are i
ncreasingly being used for evaluation.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
37/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
38/94
GI Tract
Oesophagus Stomach
Duodenum
Small Bowel
Large Bowel
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
39/94
Oesophagus
Achalasia Motilitas disorder
Neuronal degeneration within the
Auerbachs plexus in the region
of the gastro-oesophageal junction The characteristic barium swallow
findings are of a dilated oesophag
us with a smoothly tapered,conical
narrowing of the distal oesophagus
beak signorrat tail
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
40/94
Oesophagus
Hiatus Hernia The stomach has herniate
d through the oesophageal
hiatus (above diaphragma)
Most hernias (80%) are sliding in nature and hernia
te directly while 20% are
paraoesophageal and are
pushed up alongside the
oesophagus
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
41/94
Oesophagus
Oesophageal carcinoma Dysphagia ,age > 40,.Weight lo
ss and anorexia
Irregular circumferential lesion
with mucosal destruction, oesop
hageal narrowing with shoulderi
ng and abrupt transition to adja
cent normal tissue
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
42/94
Stomach
Gastric ulcer Discontinuity in the mucous membrane of
the stomach with inflammatoory base.
Roentgen signs of a benign ulcer:
1. Location: lesser curvature & adjacent part of the
posterior wall
2. Multiple3. 4% of benign ulcers greater in diameter than 4 cm
4. Ulcer niche/fleck/spot
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
43/94
43
5. Cartwheel configuration
= folds radiate from the ulcer like the spokes
on a wheel
6. An incicura on the greater curvature opposite
a gastric ulcer.
7. The ulcer protrudes beyond the line of the lumen.
Stomach (Benign Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
44/94
Stomach (Benign Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
45/94
45
8. Edematous ridge leads to the ulcer & surrounds
it at its base:
- Hamptons line
- Ulcer collar
- Ulcer mound
9. The association of a gastric ulcer with a duodenal ulcer
10. 80% heal within 4 weeks (rapid healing)
Stomach (Benign Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
46/94
Stomach (Benign Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
47/94
Stomach (Benign Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
48/94
48
Roentgen signs of a malignant ulcer:
1. Location: upper part of the greater curvature
2. Ulcer edges irregular3. Doesnt protrude beyond the line of the lumen
4. Ulcer within a polypoid mass
5. Shallow ulcer surrounded by thick rigid fold
Stomach (Malignant Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
49/94
49
6. The Carman-Kirklin meniscus sign:
Large ulcer niche ( 3 to 8 cm) with an elevated
rolled margin:- In antrum: crater is crescentic toward lumen of
stomach
- In body: crater is crescentic & curves away
from lumen of stomach
Stomach (Malignant Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
50/94
Stomach (Malignant Ulcer)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
51/94
Stomach (Malignant Ulcer)
Gastric carcinoma as a large
Irregular filling-defect (arrow
heads) in the stomach. An area ofulceration has filled with
barium (arrow). The normal
mucosal and rugal fold pattern is
destroyed.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
52/94
Duodenum
Duodenal Ulcer On double-contrast barium examination, duodenal ulcer
craters are shown as sharply defined, constant collections
of barium, sometimes with a surrounding zone of oedema
or radiating folds.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
53/94
Atresia Duodeni
Supine posisition : two bubble app. Erect posisiton : Two air fuid level
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
54/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
55/94
55
Crohns disease
Contrast studies remain the mainstay for diagnosis
The radiological changes:
* Early:
- Mucosal granularity (filling defects) (villous oedema)- Fold thickening
- Aphthous ulceration (small, shallow, circular, discret
e ulcers surrounded by an oedematous halo)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
56/94
56
Crohns disease
*Advanced:
- Cobblestoneappearance, discontinuous &
asymmetrical along the bowel circumference
- Pseudodiverticulae (ballooning of the contralateralwall)
* Complicated:
Strictures, fistulation, abscess formation, tumour
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
57/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
58/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
59/94
K,,,,,,,,,,,,,,,,,,,,,,,,,
Crohn disease
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
60/94
Crohn disease
Crohn's disease. (A) Coronal reconstruction image of CT enterography
shows thickened distal ileal loops and mural stratification resulting in a target
appearance (arrows). Prestenotic dilatation is also seen. (B) A coronal, three-
dimensional projection of the same patient showing the vascular engorgement
(arrows) of an involved ileal loop (comb sign).
A. B.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
61/94
61
Benign tumours and malignant tumours
Benign tumours:
- Adenoma
- Leiomyoma (the commonest)
Malignant tumours:
- Lymphoma (the commonest)
- Leiomyosarcoma- Carcinoid
- Metastases (malignant melanoma & bronchial ca)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
62/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
63/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
64/94
64
Large-bowel disorders:
- Colorectal tumours
- Diverticular disease- Colitis
- Miscellaneous conditions (appendicitis,
volvulus)
LARGE BOWEL
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
65/94
65
Colorectal tumours
Polyps:- A mucosal elevation
- Radiographic appearance:
* Bowler-hat sign
* En face: target sign
Colorectal cancer:
- The commonest cancers in western Europe & US
- Men = women
- Tumours tend to be right-sided- May be associated urinary tract & gynaecological
malignancy
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
66/94
POLYPS
Familial Adenomatous Polyposis
Syndrome. innumerable small polyps,
seen as tiny filling defects (arrow) Bowler-hat sign
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
67/94
67
Colorectal cancer
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
68/94
68
Colorectal cancer
Fungating type:- Medullary carcinoma
- Sites: caecum, ascending colon, rectum
- Complication: bleeding, fistula
Polypoid type:
- Sites: ascending colon usually
- Complication: Intussusception
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
69/94
69
Annular type:
- Mucoid adenocarcinoma, scirrhousfibrocarcinoma
- Sites: sigmoid, descending colon, flexures
- Complication: fistula, obstruction
Radiological appearances:
- Filling defect
- Obstruction
Colorectal cancer
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
70/94
Colorectal cancer
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
71/94
71
Colorectal cancer
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
72/94
72
Colorectal cancer
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
73/94
73
Diverticular disease
Protrusions of the mucosa & submucosa through
a defect in the wall of the bowel.
30% over the age of 60 years & 60% overthe age of 80 years
The sigmoid colon is typically affected.
Radiological findings:
- Small, flasklike or rounded outpouchings
0.5-2.0 cm, having narrow neck
- En face, ring shadows
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
74/94
74
Complication:
- diverticulitis results in pericolic abscess
& localised peritonitis
(Barium enema is contraindicated, water-soluble contrast is preferred)
Diverticular disease
Diverticular disease
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
75/94
75
Diverticular disease
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
76/94
Crohn Disease
Idiopathic characterized by the development of multiple GI tract ulcer
s from mouth to anus
Common sites : terminal ileum and/or cecum (45%), ileo-c
olonic (13%), or colorectal region (30%)
Sign on barium meal/ enema :
Segmental intestinal wall thickening with thickened mucosal
folds
Apthous ulcer; cobble stone app.
Multiple skip lesions String sign
In the colon, CD mainly aff ects the ascending color with rela
tive sparing of the rectum (50%)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
77/94
a.
b.c.
Crohn Disease
a. demonstrating the barium sign of cobble-stone
appearance
b. aphthus ulcer
c. Strictura in CD affecting ascending colon,
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
78/94
Thickened Folds, Irregular: Crohn Disease. Crohn disease of the ileum causes
thickened folds (straight arrow) that are irregular and distorted. A more proximal
segment of jejunum (open arrow) is effaced and narrowed. The transverse colon
(curved arrow) is narrowed and stiffened and has multiple inflammatory polyps
producing filling defects. This is skip lesions that are characteristic of Crohn
disease.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
79/94
79
Colitis
Colitis can subdivided into idiopathic ulcerative,ischaemic and infection aetiologies.
The hallmarks of colitis are mucosal inflammati
on & ulceration.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
80/94
80
Idiopathic ulcerative colitis
Barium examination is absolutely contraindicatedif there is evidence of toxic dilatation.
Begins in the rectosigmoid region & eventually
involves the entire colon & long stretches of the ileum
Plain Radiograph finding
Toxic mega colon.
Gasless abdomen: due to chronic diarrhea.
Absence of fecal materials
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
81/94
Idiopathic ulcerative colitis
Ba-enema findings: Collar button ulcer
Pipe stem colon: this refers to rigidity and narrowing of the
colon due to longitudinal muscle spasm and hypertrophy
Back-wash ileitis (ileocaecal valve becomes fixed & incompetent, re
sulting in terminal ileal granularity)
Stricture
Toxic megacolon
Pneumatosis coli
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
82/94
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
83/94
83
Ischaemic colitis
Primary site: splenic flexure.
Radiological appearances:
- ulceration
- splenic flexure thumb-printing
I h i liti
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
84/94
84
Ischaemic colitis
Classical splenic flexure thumb-
printing
Thumbprinting pattern involving the proximal
portion of a redundant transverse colon and
hepatic flexure
Volvulus
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
85/94
85
Volvulus
The colon may twist on its mesentery, resulting in intermi-ttent obstruction.
Sigmoid volvulus (60-70%), caecal & transverse volvulus.
Radiological examination:- Plain films
- Water-soluble contrast enema
Radiological findings:
- Inverted U without haustra (sigmoid volvulus)
- the caecum is often in the left upper quadrant
(caecal volvulus)
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
86/94
86
volvulus
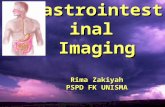
Appendicitis
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
87/94
R Signs of acute appendicitis:-Appendix calculus (0.5-6cm)
- Localised paralytic ileus in RLQ
- Sentinel loop-dilated atonic ileum containinga fluid level
- Widening of the preperitoneal fat line
- Blurring of the preperitoneal fat line- Blurring of the right psoas outline-unreliable
cont
87
Appendicitis
A di iti
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
88/94
- Scoliosis concave to the right
- Dilated caecum
- Right lower quadrant (RLQ) mass identing
the caecum on its medial border (abscessformation)
- RLQ haze due to fluid & oedema
- Gas in the appendix-rare, unreliable.
88
Appendicitis
A di iti
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
89/94
89
Ultrasound signs of acute appendicitis :
- Blind-ending tubular structure at the point oftenderness:
- Non-compressible- Diameter 6 mm
- No peristalsis
- Appendicolith casting acoustic shadow
- Surroundingfluid/abscess
Appendicitis
USG APPENDICITIS
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
90/94
90
USG APPENDICITIS
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
91/94
91
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
92/94
Acute appendicitis
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
93/94
93
Acute appendicitis
Acute appendicitis with appendicolith. Abscess formation & appendicolith.
7/27/2019 Kuliah Blok GI Tract_Ro Abd_September 2010
94/94
THANK YOU