Infratemporal fossa 360°
364
Infratemporal fossa 360° 10-12-2015 8.34pm
-
Upload
murali-chand-nallamothu -
Category
Health & Medicine
-
view
3.067 -
download
21
Transcript of Infratemporal fossa 360°

Infratemporal fossa 360°10-12-2015
8.34pm

Great teachers – All this is their work . I am just the reader of their books .
Prof. Paolo castelnuovo
Prof. Aldo Stamm Prof. Mario Sanna
Prof. Magnan

For Other powerpoint presentatioinsof
“ Skull base 360° ”I will update continuosly with date tag at the end as I am
getting more & more information
click
www.skullbase360.in- you have to login to slideshare.net with Facebook
account for downloading.

Infratemporal fossa anatomy video – Prof. Carrau – click
https://www.youtube.com/watch?v=gnGcxC7pSy4

HTTPS://WWW.YOUTUBE.COM/WATCH?V=2FXF0Z5DDB8
&
HTTP://WWW.YOUTUBE.COM/WATCH?V=X-6YKLY84T4&SNS=FB
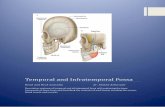
Pterygopalatine Fossa - Gross Anatomy

Do we approach infratemporal fossa through ear ????
Answer : YES – by infratemporal fossa approaches A,B,C ,D [ ITFA-A,B,C ,D ]

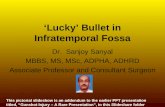
Infratemporal fossa anatomy line diagram in both anterior & lateral skull base ( Infratemporal fossa approach A, B, C , D )

Pterygo-palatine fossa

Posterior wall of maxilla & pterygoidprocess is curved anteriorly

PPF is at supero-medial area of posterior wall of maxilla

PPF & palatine bone relation

Lateral to infraorbital nerve & V2 is Infratemporal fossa , Medial to ION & V2 is Pterygopalatine fossa

Pterygopalatine ganglion in PPF

Tracking of infraorbital nerve leads to V2 & tracking of V2 leads to Trigeminal ganglion/ Middle cranial fossa [ one of the best way to track middle crannial fossa is to track V 2 ]


Medial wall of PPF is perpendicular plate of palatine bone –foramen in it is sphenopalatine foramen

foramen rotandum is 5 mm to middle cranial fossa durawhere as vidian nerve from vidial canal to laceral carotid is 2 cm
– listen 4.00 time in this video https://www.youtube.com/watch?v=Uk57MEgkde8

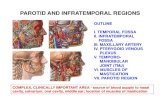
PPF extended into orbital apex

The PPF extended to superior orbital fissure ( SOF ) / Orbital apex , inferior to the cavernous sinus and
Muller’s muscle. – anterior skull base view

The PPF extended to superior orbital fissure ( SOF ) / Orbital apex , inferior to the cavernous sinus and
Muller’s muscle. – Lateral skull base view

The PPF extended to superior orbital fissure ( SOF ) / Orbital apex , inferior to the cavernous sinus and Muller’s muscle.
Anterior skull base Lateral skull base

Infratemporal fossa

Infratemporal fossa anatomy line diagram in both anterior & lateral skull base ( Infratemporal fossa approach A, B, C , D )

1. One line along Vidian nerve & another line along V22. Lateral to LPP & infra-orbital nerve [ or V2 ] is Infratemporal fossa
3. One transverse line from Vidian nerve connecting vertical line of V 2 & another transverse line from V2
4. The space above transverse line of Vidian nerve is Pterygoid Recess of sphenoid 5. The space above transverse line of V2 is Middle cranial fossa ( Meckel’s cave )

1. Pterygoid recess [= sphenoid recess ] is pneumatisation of pterygoidtrigone – spac between V2 & VN [ Vidian nerve ]
2. The space above transverse line of Vidian nerve is Pterygoid Recess of sphenoid

Pvc, vc, FR are in a 45 degree angle

SOF also comes in the 45 degree angle – my observation

MPP[ medial pterygoid plate ] present at lateral surface of posterior choana – which is in line with paraclival carotid

Vidian canal is funnel shaped

1. V1,V2,V3 of 5th nerve – V3 is 90° to V1 & V2 and anterior to petrous carotid like horse rider leg [ V3 ] [ mneumonic ] on saddle
of horse [ petrous carotid & paraclival carotid junction ]
2. Vidian nerve is continuation of GSPN crosses laterally the laceralcarotid

V1,V2,V3 of 5th nerve – V3 is 90° to V1 & V2 and anterior to petrous carotid like horse rider leg [ V3 ] [ mneumonic ] on
saddle of horse [ petrous carotid & paraclival carotid junction ]

LPP if you look anteriorly (radiologically ) is in line with FR (V2) , if you look laterally posterior border of LPP leads to V3 . So when you are removing recurrent nasopharyngeal carcinoma
transnasally you can observe LPP leads to V3 . This V3 seperates pre & post styloidcompartments.

Posterior boarder of lateral pterygoidplate leads to foramen ovale

GSPN bisects V3 & petrous carotid

In the floor of sphenoid sinus you will get Vidiannerve when you approach by antero-lateral triangle

Hand model --
left hand = medial & lateral pterygoid
right hand = index is parapharyngealcarotid , middle is IJV , ring is styloid & stylopharyngeal muscles , thumb is horizontal carotid

IAN = inferior alveolar nerve , LN = lingual nerve , MPM = medial pterygoid muscle , LPM = lateral pterygoid muscle
Different layers of muscles & aponeurosisprotecting great vessels in infratemporal fossa –
Main protectors are medial & lateral
pterygoid mucles & temporalis muscle -
great vessels are posterior to these 3
muscles –
small contribution of protection of great vessels are done by
tensor veli palatini & styloid muscles & stylopharyngeal
aponeurosis

IAN = inferior alveolar nerve , LN = lingual nerve , MPM = medial pterygoid muscle , LPM = lateral pterygoid muscle


TVPM is triangular muscle , LVPM is cylindrical muscle


SPM attached to superior constrictor ,
SGM attached to tongue ,
SHM attached to lesser cornuof hyoid bone


After drilling LPP & MPP longissmus capitis & superior constrictor seen .

Incision anterior to anterior to anterior pillar of tonsil for “Trans - Oral
approach to infratemporal fossa”

Two planes posterior to MPM which have greater surgical importance ...... …..1. Nasopharyngeal carcinoma/JNA excision - plane between medial pterygoid muscle ( MPM ) & ET tube/TVPM ( tensor veli
palatini muscle)........ 2 . Trans-oral exposure of Infratemporal fossa (ITF) - incision anterior to anterior pillar of tonsil - leads to - plane between MPM & superior constrictor / styloid muscles............In the below
diagrams MPM reflected back for understanding purpose

Two planes posterior to MPM which have greater surgical importance ...... …..1. Nasopharyngeal carcinoma/JNA excision - plane between medial pterygoid muscle ( MPM ) & ET tube/TVPM ( tensor veli
palatini muscle)........ 2 . Trans-oral exposure of Infratemporal fossa (ITF) - incision anterior to anterior pillar of tonsil - leads to - plane between MPM & superior constrictor / styloid muscles............In the below diagrams
MPM reflected back for understanding purpose

1. Each styloid muscle accompanied by one nerve – SPM by 9th nerve , SGM by lingual nerve , SHM by 12th nerve
2. SPM & SGM protects ICA whereas SHM protects both ECA & ICA 3. ECA & ICA & CCA are like tuning fork – caricature diagram

Each styloid muscle accompanied by one nerve – SPM by 9th
nerve , SGM by lingual nerve , SHM by 12th nerve

MPM is reflected back – which shows the structures seen in trans-oral approach of ITF – incision anterior to anterior pillar of tonsil

Apex of infratemporal fossa


V3 & mma are together

Schematic diagram for infratemporal fossa approach –MMA & V3 & pterygoid plate from posterior to anterior

V3[MN] & MMA & ET in lateral & Anterior skull base – see the relationship of ET tube which is medial to V3 & MMA

V3 & mma are together 2. V3 accompanied by mma whereas IAN [ inferior alveolar nerve ] is accompanied by PSAA [ postero-
superior alveolar nerve ] Lateral skull base Anterior skull base

After drilling the tympanic bone & styloid process inbetween jugular bulb & carotid , 9th nerve is seen

Cochlear aqueduct is a pyramidal shape structure present in between round window & jugular bulb – which is an important landmark for
identification of 9th nerve in retrofacial mastoid air cells area .

Sympathetic trunk is posterior to vagus– below photo right side

SCG anastamosed with all the lower cranial nerves – below photo right side

Superior cervical ganglion is posterior to inferior ganglion of vagus – SCG lies over prevertebral facia over longus capitis
– below photo left side

11th nerve present inbetweenvertebral artery & IJV

11th nerve is postero-medial & antero-lateral to IJV
Postero-medial to IJV Antero-lateral to IJV

1. Anterior to IPS - 9th nerve seen , posterior IPS - 10th & 11th seen 2. 12th nerve crosses 10th nerve laterally

1. Anterior to IPS - 9th nerve seen , posterior IPS - 10th & 11th seen 2. 12th nerve crosses 10th nerve laterally

1. 9th & 12th nerves crosses parapharyngeal carotid above & below2. supracondylar groove leads to Hypoglossal canal

12th nerve seen in infra-petrous approach in anterior skull base

9th & 12th nerves
Anterior skull base Lateral skull base

9th nerve is the most lateral nerve & 12th nerve is most medial nerve in skull base

ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle ;Transtubercular is through Jugular tubercle &
lateral pharyngeal tubercle

Endoscopic endonasal view of a cadaveric dissection showing transection of the right eustachian tube (ET) attachment to foramen lacerum (FL). The hypoglossal nerve (XII) enters the hypoglossal canal just deep to
the ET and separates the occipital condyle (OC) and the jugular tubercle (JT). (BA, basilar artery; ICA, internal carotid artery [paraclival segment]; IPS, inferior petrosal sinus; VN, vidian nerve.) B. Endoscopic
endonasal view of cadaveric dissection showing the parapharyngeal internal carotid artery (ICA) and jugular foramen (JF) following transection and removal of the eustachian tube. (BA, basilar artery; IPS, inferior petrosal sinus; FL, foramen lacerum; JT, jugular tubercle; OC, occipital condyle; XII, hypoglossal
nerve.)

Note 12th nerve in between JT ( Jugular tubercle ) & OC ( Occipital condyle ) in both lateral & anterior skull base
Lateral skull base Anterior skull base

1. Laceral carotid & jugular tubercle & lower cranial nerves 9th ,10th ,11th are in the same line .
2. hypoglossal canal present between occipital condyle/foramen magnum & jugular tubercle

1. 9th & 12th nerves crosses parapharyngeal carotid above & below 2. 12th nerves originates medial to apex of parapharyngeal carotid
3. 11th nerve hinges the transverse process of C 1 4. 11 th nerve between vertebral artery & IJV
5. 9th nerve anterior to origin of IPS whereas 10th & 11th nerve posterior to origin of IPS 6. superior ganglion of vagus [ SGV ] is inside the jugular foramen where as inferior ganglion of
vagus [ IGV ] is outside skull base

1. 9th & 12th nerves crosses parapharyngealcarotid above & below 2. 12th nerves originates medial to apex of parapharyngeal carotid 3. 11th nerve hinges the transverse process of C 1 4. 11 th nerve between vertebral artery & IJV 5. 9th nerve anterior to origin of IPS whereas 10th
& 11th nerve posterior to origin of IPS 6. superior ganglion of vagus [ SGV ] is inside the jugular foramen where as inferior ganglion of vagus[ IGV ] is outside skull base

Incision anterior to anterior pillar of tonsil for “Trans - Oral approach of
infratemporal fossa”

Incision of trans-oral approach of ITF is – anterior to anterior pillar of tonsil – pathway is between MPM & superior constrictor

1. Each styloid muscle accompanied by one nerve – SPM by 9th nerve , SGM by lingual nerve , SHM by 12th nerve
2. SPM & SGM protects ICA whereas SHM protects both ECA & ICA 3. ECA & ICA & CCA are like tuning fork – caricature diagram

Each styloid muscle accompanied by one nerve – SPM by 9th
nerve , SGM by lingual nerve , SHM by 12th nerve

MPM is reflected back – which shows the structures seen in trans-oral approach of ITF – incision anterior to anterior pillar of tonsil

Transoral approach to SUPERO-MEDIAL Parapharyngealtumors – incision anterior to anterior pillar of tonsil

Infratemporal fossa approach A
ITFA-A

The skin incision is made as shown.
A cadaveric dissection, showing the facial nerve trunk (FNT) asit exits the stylomastoid foramen and the start of the pes anserinus (PA).IJV Internal jugular vein, MT Mastoid tip

In a right temporal bone, the intraparotid segment of the facial
nerve (FNp) has been identified. An extended mastoidectomyhas been
carried out, removing the bony covering of the sigmoid sinus (SS) and revealing
the posterior fossa and middle fossa dura (MFD). Skeletonization
of the mastoid and tympanic segments of the facial nerve (FN) has been
carried out. C Basal turn of the cochlea (promontory), DR Digastric
ridge, LSC Lateral semicircular canal
The superstructure of the stapes (S) is being cut using straight
scissors. FN Facial nerve, LSC Lateral semicircular canal

Decompression of the nerve is being carried out. C Basal turnof the cochlea (promontory), FN(m) Mastoid segment of the facialnerve, FN(t) Tympanic segment of the facial nerve, G Facial nerve genu,LSC Lateral semicircular canal, SS Sigmoid sinus
The mastoid tip (MT) is being removed by avulsing it posteriorlyaway from the stylomastoid foramen (SMF), to avoid injuring thenerve at this level. FN(m) Mastoid segment of the facial nerve, SS Sigmoidsinus, T Tympanic bone

The last shell of bone covering the mastoid (FNm) and tympanic(FNt) segments of the facial nerve is now ready to be removed. Thenew fallopian canal (NC) drilled into the root of the zygoma can be seen.LSC Lateral semicircular canal, PD Posterior belly of the digastric muscle,SMF Stylomastoid foramen, TB Tympanic bone
The last shell of bone covering the mastoid segment of the facialnerve (FNm) is being removed. ET Eustachian tube, FN(p) Intraparotidfacial nerve, G Genu, SM Stylomastoidforamen, SS Sigmoidsinus

The bony covering of the tympanic segment of the facial
nerve is being removed. FN(m) Mastoid segment of the facial nerve,
G Genu, LSC Lateral semicircular canal, NC New fallopian canal
The bone overlying the proximal part of the tympanic segment(FNt) and the geniculate ganglion is being removed, although thenerve is not to be rerouted at this level. The reason for removing bonehere is to prevent it from injuring the rerouted part of the nerve.ET Eustachian tube, LSC Lateral semicircular canal, MFD Middle fossadura, NC New fallopian canal

A tunnel is being created in the soft tissues of the parotidgland (PT) to accommodate the distal part of the rerouted nerve.FN(m) Mastoid segment of the facial nerve, NC New canal, PD Posteriorbelly of the digastric muscle, SM Stylomastoid foramen
A nontoothed forceps is used to hold the soft tissues (ST) surroundingthe nerve at the level of the stylomastoid foramen (SMF), andsharp scissors are used to dissect the soft tissues from the bone at thatlevel. C Cochlea, FN(m) Mastoid segment of the facial nerve, LSC Lateralsemicircular canal, NC New canal, SS Sigmoid sinus

The fibrovascular attachments (<) between the mastoid segment
of the facial nerve (FNm) and the fallopian canal (FC) should be
sharply cut.
The attachments shown in Fig. 9.14 are being sharply cut to
avoid injuring the mastoid segment (FNm) of the nerve. FC Fallopian
canal

The required length of the facial nerve has been dissected
away from the fallopian canal; the arrows (> <) show the limit. Keeping
this proximal part of the tympanic segment of the nerve (FNt) and the
geniculate ganglion attached to the canal medially will help preserve
part of the blood supply, resulting in better facial nerve function.
FN(m) Mastoid segment of the facial nerve, LSC Lateral semicircular
canal, NC New canal
In preparation for rerouting, the soft tissues (ST) surroundingthe facial nerve at the stylomastoid foramen are being held by a nontoothedforceps. FN(m) Mastoid segment of the facial nerve, FN(p) Intraparotidfacial nerve, FN(t) Tympanic segment of the facial nerve,NC New canal

Rerouting of the facial nerve. FN(m) Mastoid segment of thefacial nerve, FN(p) Intraparotid facial nerve, SM Facial nerve at the stylomastoidlevel, ST Soft tissues
The facial nerve has been rerouted into the new canal (*).FC Fallopian canal, FN(p) Rerouted part of the intratemporal facial nerve,FN(t) Rerouted part of the tympanic segment of the facial nerve, ST Softtissues

After the attached muscles have been dissected away, thestyloid process (SP) is fractured using a rongeur. FC Fallopian canal,FN Facial nerve, FN(p) Rerouted part of the intraparotid facial nerve,TB Temporal bone
To obtain control over the vascular structures as they enterthe temporal bone, the tympanic bone (TB), the fallopian canal remnants(FC), and the infralabyrinthine air cells are all to be removed.C Basal turn of the cochlea (promontory), IJV Internal jugular vein,JB Jugular bulb, SS Sigmoid sinus

The view after completely uncovering the lateral surfaces ofthe vascular structures. C Basal turn of the cochlea (promontory), ICA Internalcarotid artery, IJV Internal jugular vein, JB Jugular bulb, SS Sigmoidsinus
If further anterior exposure of the internal carotid artery (ICA)is required, a retractor is used to keep the mandibular condyle displacedanteriorly. C Basal turn of the cochlea (promontory), FN Rerouted facialnerve, IJV Internal jugular vein, JB Jugular bulb, LSC Lateral semicircularcanal, RW Round window, SS Sigmoid sinus

The proximal end of the sigmoid sinus is closed by extraluminalpacking of connective tissue (CT). FN Rerouted facial nerve, ICA Internalcarotid artery, JB Jugular bulb, MFD Middle fossa dura, SS Sigmoidsinus
The lateral wall of the sigmoid sinus (SS) has been opened.
CT Connective tissue, IJV Internal jugular vein, L Lumen of the sigmoid
sinus

The distal portion of the opened sigmoid sinus is packed withconnective tissue (CT). ICA Internal carotid artery, IJV Internal jugularvein, JB Jugular bulb, L Lumen of the sigmoid sinus
The internal jugular vein (IJV) is being dissected away. ICA Internal
carotid artery, JB Jugular bulb

The view after removal of the internal jugular vein and jugularbulb. Note that in live surgery, the opening of the inferior petrosal sinus(IPS) will start bleeding, requiring it to be packed. IX Hypoglossal nerve,X Vagus nerve, C Basal turn of the cochlea (promontory), ICA Internalcarotid artery
The plane of dissection between the internal carotid artery(ICA) and the overlying periosteum(P) is best developed at the entranceof the artery into its canal. C Basal turn of the cochlea (promontory)

A suction tube is used to displace the internal carotid artery(ICA) laterally while the medially lying bone is being drilled. C Basal turnof the cochlea (promontory), IPS Inferior petrosal sinus
The suction tube is used here both to displace the artery andto protect it during drilling of the anteriorly lying bone. ICA(h) horizontalsegment of the internal carotid artery, ICA(v) vertical segment of the internalcarotid artery

Infratemporal fossa approach B
ITFA-B

Posterolateral (Glasscock's) Triangle approach in Trans-temporal skull base approaches is called “ Infra-
temporal fossa B approach “ by Prof. Mario sanna
The petrous apex as viewed through the infratemporal fossa type B approach.
Structures lying lateral to the internal carotid artery (ICA). The mandibular nerve (V3) and the middle meningeal artery have been cut. The instrument points to the position of the already drilled bonyeustachian tube (ET).

Iatrogenic chances of injury of cochlea in infratemporal fossa transpetrous
approach

The skin incision.The external auditory canal (arrow) is closed as cul-de-sac.

The temporalis muscle is detached anteriorly.
The zygomatic arch is transected. Arrows point to the transection sites.

Subtotal petrosectomy. The facial nerve (FN) is skeletonized and the vertical internal carotid artery (ICA) is identified.

A minicraniotomy helps positioning the infratemporal fossa retractor.
Identification of the middle meningeal artery (MMA) crossing lateral to the eustachian tube (ET).

Coagulation of the middle meningeal artery (MMA).
Cutting the middle meningeal artery (MMA).

Identification of the mandibular nerve (V3). The mandibular nerve (V3) is cut.

Suturing the eustachian tube (ET) at the end of the procedure. Closure and drain insertion.

Infratemporal fossa approach B in cadaver

The temporalis muscle (TM ) of a left temporal bone has beenreflected anteriorly after it has been dissected from the squamous bone(S). TL Temporalis line, ZR Root of the zygomaticprocess

The periosteum (P) overlying the zygomatic arch (ZA) isbeing dissected away. This step helps avoid the laterally lying frontalbranch of the facial nerve. SB Squamous bone
The view after dissection of the periosteum (P) from the zygomaticarch (ZA). SB Squamous bone, TM Temporalis muscle

The zygomatic arch has been transected. EAC External auditorycanal, SB Squamous bone, TM Temporalis muscle, ZR Zygomaticroot
The skin of the external auditory canal (S) is being dissected
away under the microscope. TM Tympanic membrane

After complete removal of the external auditory canal skinand tympanic membrane, the incudostapedial joint is disarticulated inorder to remove the ossicular chain. C Chorda tympani, I Incus, M Malleus,S Stapes
The mastoid cavity and the posterior and superior walls of theexternal auditory canal have been partially drilled. FB Facial bridge,FR Facial ridge, MFP Middle fossa plate, SS Sigmoid sinus

A radical mastoidectomy has been carried out, and the facialnerve has been skeletonized. AR Anterior attic recess, C Basal turn of thecochlea (promontory), DR Digastric ridge, FN(m) Mastoid segment ofthe facial nerve, FN(t) Tympanic segment of the facial nerve, LSC Lateralsemicircular canal, MFP Middle fossa plate, PSC Posterior semicircularcanal, RW Round window, S Stapes, SS Sigmoid sinus, SSC Superiorsemicircular canal, TT Tensor tympani
The retrofacial and infralabyrinthine air cells are being drilledusing an appropriately sized diamond drill. Attention must be paidduring this step to avoid injuring the laterally lying facial nerve with theburr or the shaft. ELS Endolymphatic sac, FN(m) Mastoid segment of thefacial nerve, ICA Internal carotid artery, SS Sigmoid sinus

The anterior wall of the external auditory canal has been partiallydrilled, and the vertical segment of the internal carotid artery (ICA)has been identified. FN(m) Mastoid segment of the facial nerve,FN(t) Tympanic segment of the facial nerve, JB Jugular bulb, LSC Lateralsemicircular canal, S Stapes, SS Sigmoid sinus, TT Tensor tympani
Dissecting the articular disk (AD) of the temporomandibular
joint. ACWAnterior canal wall, SB Squamous bone, ZR Zygomaticroot

A small craniotomy (CT) has been created in the squamous
bone. ACWAnterior canal wall, AD Articular disk
A self-retaining retractor is used to keep the mandible retractedinferiorly. ACWAnterior canal wall, AZT Anterior zygomatictubercle, GF Glenoid fossa

The rest of the anterior canal wall has been drilled away, andthe internal carotid artery is better skeletonized. C Basal turn of thecochlea (promontory), ET Eustachian tube, FN(m) Mastoid segment ofthe facial nerve. G Genu of the internal carotid artery, ICA(v) Verticalsegment of the internal carotid artery
To obtain control of the horizontal segment of the internalcarotid artery, the eustachian tube (ET), glenoid fossa bone (GF), and theanterior zygomatic tubercle (AZT) have to be carefully drilled away.ICA Vertical segment of the internal carotid artery

In live surgery, the middle meningeal artery (MMA) should becoagulated to prevent bleeding. ICA Internal carotid artery, MFP Middlefossa plate
The middle meningeal artery (MMA) is being sharply cut.
ET Eustachian tube, ICA Internal carotid artery, MFP Middle fossa plate

Further anterior drilling uncovers the mandibular nerve (MN).This nerve also has to be coagulated in live surgery before it is cut.ET Eustachian tube, ICA Internal carotid artery, MFP Middle fossa plate
Sharply cutting the mandibular nerve (MN). ET Eustachian
tube, ICA Internal carotid artery, MFP Middle fossa plate

The stumps of the mandibular nerve (*). ET Eustachian tube,
ICA Internal carotid artery, MFP Middle fossa plate
The eustachian tube (ET) and tensor tympani muscles (TT)are the last structures lying lateral to the horizontal segment of the facialnerve and should be removed. ICA Internal carotid artery, JB Jugularbulb, MN The cut end of the mandibular nerve

The lateral, thin part of the eustachian tube (ET) that remainscan be removed with forceps. C Basal turn of the cochlea (promontory),ICA Internal carotid artery, MFP Middle fossa plate
The tensor tympani muscle has been dissected away from itscanal (TTC). ET Medial wall of the eustachian tube, ICA Internal carotidartery, MFP Middle fossa plate

A large diamond burr is used to remove the remaining boneoverlying the horizontal segment of the internal carotid artery. C Basalturn of the cochlea (promontory), ICA Vertical segment of the internalcarotid artery, MFP Middle fossa plate, MMA Stump of the middlemeningeal artery, MN Stump of the mandibular nerve
The horizontal segment of the internal carotid artery (ICAh)has been skeletonized. Note that the greater petrosalnerve (GPN) is adherentto the dura, and that retracting the dura will lead to stress on thefacial nerve at the geniculate ganglion (GG) level. Thus, if dural retractionis needed, cutting the petrosal nerve will prevent this injury. C Basal turnof the cochlea (promontory), CL Clivus bone, G Genu, ICA(v) Verticalsegment of the internal carotid artery

The tip of the suction is used to displace the internal carotidartery (ICA) laterally while the medially lying bone is being drilled.C Basal turn of the cochlea (promontory), FN(m) Mastoid segment ofthe facial nerve, FN(t) Tympanic segment of the facial nerve,GPN Greater petrosal nerve, MFP Middle fossa plate, MMA middlemeningeal artery stump
Drilling of the clivus has been completed. C Basal turn of thecochlea (promontory), FN(m) Mastoid segment of the facial nerve,FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion,GPN Greater petrosal nerve, ICA Internal carotid artery, RW Round window

The full course of the intratemporal internal carotid artery hasbeen freed. AFL Anterior foramen lacerum, CF Carotid foramen, CL Duraoverlying the clivus area, ICA(h) Horizontal segment of the internalcarotid artery, ICA(v) Vertical segment of the internal carotid artery,MN Stump of the mandibular nerve
The view after completion of the approach.

The relationship of the internal carotid artery (ICA) to thetympanic membrane (TM) and middle ear in a right temporal bone.
A Annulus, FN(m) Mastoid segment of the facial nerve, I Incus, JB Jugularbulb, LSC Lateral semicircular canal, M Malleus, MFD Middle fossa
dura, PSC Posterior semicircular canal, SSC Superior semicircular canal

Infratemporal fossa approach C
ITFA-CThis is an anterior extension of the type B approach, in which
the pterygoid process is drilled, providing control of the nasopharynx,the pterygopalatine fossa, and the sphenoid sinus
(Fig. 9.18). The approach is designed to give lateral access forthe extirpation of extradural lesions involving the infratemporal
fossa, the nasopharynx, the pterygopalatine fossa, thesphenoid sinus, and minimal extension into the cavernous
sinus.

The sphenoid (SphS) sinus lies superomedial to the base of the pterygoid.
The bony anatomy of the base of the skull. The hatched line
represents the pharyngobasilar fascia.

Cutting the fibrous attachments of the eustachian tube (ET).
The petro-occipital synchondrosis (arrow) separating theclivus from the petrous apex.

Exposure of the base and lateral process (PtP) of the pterygoid. Opening the nasopharynx (NP).

Locating the sphenoid sinus (SphS). The maxillary nerve (V2)runs roughly at the level of the sinus roof.
Retracting the middle fossa duraallows complete control ofthe horizontal internal carotid artery (ICA) to the foramen lacerum. AFL,anterior foramen lacerum.

Opening the sphenoid sinus (SphS).
Cutting the maxillary nerve to gain access to the lateral wall
of the cavernous sinus.

The abducent nerve (VI) crosses from the medial to thelateral aspect of the internal carotid artery (ICA) before entering thecavernous sinus.

The Group of PreauricularTranszygomatic Approaches
1. Type D Infratemporal Fossa Approach
2. Preauricular Infratemporal TranszygomaticApproach
3. Preauricular FTOZ = FrontotemporalOrbitozygomatic Approach

Type D Infratemporal Fossa Approach
RationaleThe type D approach is like the type C but is performed through a preauricular incision. Mastoidectomy is not performed and the middle ear is left intact. The eustachian tube is not sacrificed. The approach is designed for infratemporal fossa lesions with or without extension to the pterygopalatine fossa, sphenoid sinus, and/or minimal cavernous sinus extension; for example, trigeminal neurinomas with predominant infratemporalfossa component and minimal middle fossa extension. The approach will be discussed together with the more extensive preauricular approaches, namely, the preauricular infratemporal fossa

Preauricular InfratemporalTranszygomatic Approach
Rationale The preauricular infratemporal approach is a variant of theinfratemporal approach in which a large frontotemporal craniotomy is performed. This approach is suitable for infratemporal fossa lesions with or without extension to the petrous apex, sphenoid sinus, or upper clivus or minimal cavernous sinus extension. It is suitable for both intradural and extradural lesions affecting the upper clivus and parasellar regions. The craniotomy allows tumor removal with minimal brain retraction.

Skin incision.A semilunar incision (arrows) is made in the superficial layer of the deep temporal fascia.

The temporalis muscle, zygomaticarch, and orbital rim are
fully exposed. The temporalis muscle (TeM) is incised in a line about 1 cm along its attachment.
Drawing showing the zygomatic cuts for the pure transzygomatic approach.

Orbitozygomatic osteotomy performed.
Drawing showing the partial orbitozygomatic osteotomy.

Zygomatic and Orbitozygomatic OsteotomyThe zygomatic osteotomy is performed according to the extension of
the lesions as follows:a) In limited cases, only the zygomatic arch is displaced inferiorly.
The zygomatic bone and the lateral orbital rim are left intact .b) For the majority of lesions only an “extended” zygomatic
osteotomy is performed in which the zygomatic arch and part of the zygomatic bone are included in the zygomatic osteotomy . The orbitozygomatic osteotomy in more advanced cases in which the tumor extends into the orbital apex through the inferior or superior orbital fissures: The frontal and temporal dura are detached from the periorbita exposing the bony orbit.

Standard orbitozygomatic osteotomy.
Standard orbitozygomatic osteotomy.

Drawing outlining the lines of the standard orbitozygomaticosteotomy.

The removed orbitozygomatic bone to be placed in saline.

The bone is drilled to the base of the middle fossa (MFD).
The temporal lobe is retracted for further bone removal. The hatched lines represent the bone that needs to be removed for the
standard orbitozygomaticosteotomy.

With temporal lobe retraction, the three branches of thetrigeminal nerve (V1, V2, V3) are exposed. More exposure can be gained
by further performing the standard orbitozygomatic osteotomy.

Approach of infratemporal fossa by anterior skull base

1. External corridor doesn’t matter except cosmesis , only internal corridor matters – so in Open approaches of skull
base also use endoscope to get best results – see this video how the Dr. Dugani Suresh ; Neurosurgeon is using
endoscope in Weber Fergusson incision https://www.youtube.com/watch?v=Y95Jf3u8S8o&feature=y
outu.be2. Most of the times “Don’t cross the NERVES”

Only to lesion lateral to meridian of pupil in frontal sinus we have to do osteoplastic flap
The landmarks for canine fossapuncture/trephine are the intersection between a vertical line through the pupil and a horizontal line drawn through the floor of the nose.

Enhanced T1-weighted magnetic resonance imaging (MRI),coronal section demonstrates a right nasoethmoidal lesion (adenocarcinoma)
with an “hourglass” intradural extension through the ethmoidalroof. Diffuse enhancement of the dural layer (arrowheads) over
the orbital roof is suspicious for neoplastic spread. The vertical lines limitthe area of the dura safely resectable by a pure endoscopic approach.

“Up & below” approach to frontal sinus

Illustration of the septal incisions necessary to achieve good access to the entire anterior wall of the maxillary sinus for
tumors either originating from this region or with a significant anterior wall attachment. (B) Cadaveric image demonstrating the access to
the anterior wall (AW) of the maxillary sinus with a 70-degree diamond drill (D).


(A) The microdebrider blade has been passed through an inferior meatal antrostomy. Note the anterior fulcrum (nasalvestibule, broken white arrow) and the posterior fulcrum (inferior meatal antrostomy, white arrow). The region of the maxillary
sinusthat can be cleared through this access is shaded. This shaded region is smaller with a middle meatal antrostomy. The single
fulcrum ofthe canine fossa puncture is indicated (white arrow) (B,C,D), illustrating how the entire maxillary sinus can be accessed as the
bladeonly has a single fulcrum.Medial , posterior & Lateral walls approached through Caldwel-luc

The red arrows demonstratethe endonasal approach, and the green arrows represents the transmaxillary
approach. The blue rectangle shows the parasellar structures.A more perpendicular angle of attack is achieved in the transmaxillaryapproach, and the distance to the target from this route is equal to or
smaller than that in the endonasal approach. Temp.: temporal.

Note that in the transmaxillary approach thestructures in the lateral wall of the sphenoid sinus are seen in a
more perpendicular way, facilitating dissection of this region.

Close-up view of the cavernous sinus through the transmaxillary
approach. Gasser.: gasserian.

The pink and orange linesdemonstrate the possible angles of maneuver in transmaxillary
approach.In green is emphasized the possibilities of resection through
transmaxillary approach.

General view of the radial endoscopic accesses to the skullbase --- The green arrows represent the endonasal approaches,
the red arrows represent the transmaxillaryapproaches, and the purple arrows represent the
subtemporal approaches. Note the multiple possibilitiesof combination of these approaches.

Modified denkers approach - Blue dotted line showsthe medial maxillary wall. (B) Panoramic view after removing the medial
maxillary wall. Yellow dotted line shows the connected nasal cavity with maxillary sinusthe maxillary sinus.

Schematic demonstrating how the removal of the lateralaspect of the piriform overture (in the red circle) enables a wider approach
(the green cone compared with the yellow cone) to the lateralregions (pterygopalatine and infratemporal fossa).

Use combination of approaches when ever it is necessary -Combined Transmastoid Middle Cranial
Fossa Approach

Rt lower cranial nerve shwannoma, which approach will be better ,which approach will be better considering this side is
dominant sinus.

Answer
• Amit Keshri says - eight nerve was normal,so was 7th,removed tumor completely with retrolab approach and to get space,the sigmoid plate was decompressed and sinus retracted posteriorly after RMSO [ Retro mastoid sub-occipital ] craniotomy without opening dura posteriorioly.
• Murali Chand Nallamothu For lower cranial nerve schawnnoma POTS approach is the best - but here you are saying it is dominent sinus , no need to sacrifice sigmoid sinus -- so in this case we can use extended translabyrinthine approach for the AFB area part & at carotid canal area part of the tumor can be removed by externally which is included in the lower C - shaped incision
• Murali Chand Nallamothu if the 8 th nerve is good we can try retrolabyrinthinne & retrosigmoid approach & take the help of endoscope.
• Post-op :

Approaches to Infratemporalfossa

B, approach to infratemporal fossa. A, approach to MCF through greater
wing of sphenoid bone.


MPP/VNLPP/V2

Anteriorly MPP & LPP are fused & posterioly only they are divided .

Anteriorly MPP & LPP are fused & posterioly only they are divided .



Erosion of right greater wing of sphenoid in a case of maxillary carcinoma


Medial pterygoid is in line with lateral wall of Sphenoid -- The superior vertical limb represents the paraclival ascending carotid and the
descending vertical limb is represents the medial pterygoid plate. The horizontal bar of the ‘H’ is represented by the sphenoid sinus floor.

Lateral part of Posterior choanae is MPP

ET is just posterior to MPP

Lateral part of Posterior choanae is MPP

Medial pterygoid is in line with Paraclival carotid

Tracking of infraorbital nerve leads to V2 & tracking of V2 leads to Trigeminal ganglion/ Middle cranial fossa [ one of the best way to track middle crannial fossa is to track V 2 ]

Zygomatic nerve [ ZN ]

Infraorbital groove near inferior orbital fissure – If we drill supero-lateral to infraorbital nerve it is nothing but Inferior orbital fissure .

Infraorbital groove near inferior orbital fissure – If we drill supero-lateral to infraorbital nerve it is nothing but Inferior
orbital fissure .

Red ring = V2

Inferior orbital foramen continues as pterygomaxillary fissure .


One line along Vidian nerve & another line along V2



Lateral to LPP & infra-orbital nerve [ or V2 ] is Infratemporal fossa

One transverse line from Vidian nerve connecting vertical line of V 2 & another transverse line from V2

The space above transverse line of Vidian nerve is Pterygoid Recess of sphenoid – Read the CT – scan/ Plane the surgery by using these lines


The space above transverse line of V2 is Middle cranial fossa ( Meckel’s cave ) –
Read the CT – scan/ Plane the surgery by using these lines

Pterygo-palatine fossa


Pterygopalatine fossa. A, V2 (blue dotted line) coming outfrom the foramen rotundum; B, green-yellow dotted line shows the
pterygopalatine ganglion; C, yellow dotted line shows the vidiannerve; D, red dotted line shows the sphenopalatine artery; E, light bluedotted line shows the great palatine nerve; F, white dotted line showing
the infraorbital artery.

EC – Ethmoidal crest – left nose

Vidian canal is funnel shapped

PVC , VC & FR are in 45 degree angle line



Endoscopic view of PPG

Tracking of infraorbital nerve leads to V2 & tracking of V2 leads to Trigeminal ganglion/ Middle cranial fossa [ one of the best way to track middle crannial fossa is to track V 2 ]

Zygomatic nerve [ ZN ]


Endoscopic view of foramen rotundumarea

Infratemporal fossa



Lateral pterygoid muscle devides internal maxillary artery into 3 parts -1 . Mandibular part 2. lateral pterygoid [ infratemporal fossa ] part
3. pteygo-palatine fossa part

Dissection done by Dr.Janakiram , india

1. The maxillary artery & Buccal nerve enters the infratemporal fossa between the superior and inferior head of the
lateral pterygoid muscles. 2. Lingual nerve & Inferior alveolar nerve comes between medial pterygoid & lateral
pterygoid mucles .

.

Anteriorly lingual nerve & posteriorly Inferior Alveolar nerve coming lateral to medial pterygoid muscle – Lingual nerve is
just submucous & palpable just posterior to 3rd molar

Forceps behind IAN Forceps behind LN

IAN = Inferior alveolar nerve

Triangle formed by temporalis muscle , MPM & LPM
Mandibulotomy approach Endospic view

Post-maxillectomy “Fat pad” over temporalis muscle – which is seen as Fat Pad [ FP ] in the triangle formed by temporalis
mucle , MTM & LPM endoscopically

Internal carotid artery going medial & posterior to medial pterygoid muscle into Parapharyngeal space &
becoming Parapharyngeal carotid

Internal carotid artery going medial & posterior to medial pterygoid muscle into Parapharyngeal
space & becoming Parapharyngeal carotid

After removing the LPM you will see Tensor veli palatini muscle (TVPM) coming vertically downwards from anterior surface of ET , protecting parapharyngeal carotid
& after TVPM , thick Stylopharyngeal apneurosis (SPHA ) present ANTERIOR to Parapharyngeal carotid [ So 2 structures ( TVPM & SPHA ) protecting parapharyngeal
carotid ]

After removing the LPM you will see Tensor veli palatini muscle (TVPM) coming vertically downwards from anterior surface of ET , protecting parapharyngeal carotid & after TVPM thick Stylopharyngeal apneurosis present ANTERIOR to Parapharyngeal
carotid -- Attached to this ET cartilage [ TP/ET attachment ] is the tensor palatini(TP) fibrous aponeurosis (solid white line) with its muscle fibers seen below (broken
white line).

Hand model --
left hand = medial & lateral pterygoid
right hand = index is parapharyngealcarotid , middle is IJV , ring is styloid & stylopharyngeal muscles , thumb is horizontal carotid

Hypoglossal is just behind the upper end of parapharyngel carotid – very easy way to
identify 12th nerve in paraphayrngeal space – Dr.Satish jain


Parapharyngeal space

Devided into
• Pre-styloid compartment – no vital structures
• Post-styloid compartment = carotid space –contains last 4 cranial nerves & great vessels & sympathetic chain

prestyloid mass originating from parotid deep lobe







Note : Glossopharygeal nerve & styloglossus in the bed of tonsil





Internal carotid artery going medial & posterior to medial pterygoid muscle into Parapharyngeal space &
becoming Parapharyngeal carotid

Internal carotid with aberrant loop lying in thesagittal plane of the neck.
The normal internal carotid artery runs in a straightcourse to the skull base. The pharynx lies anteromedialand is normally at least 1.5 cm away with fatty areolartissue and pharyngeal veins in between. In the embryo, the internal carotid artery, derived from the third aortic arch and dorsal aortic root, is normally coiled. Straightening occurs when the foetal heart and great vessels descend into the mediastinum. Failure of or incomplete uncoiling can result in the vessel assuming a wide loop in the coronal, saggital or, rarely, transverse plane of the neck .Such an anomalyis rare but well recognized. This emphasizes the importance of palpating for pulsating vessels while undertaking an adenoidectomy. A medialized internal carotid artery is a well-described entity associated with velocardiofacial syndrome. In this syndrome, where pharyngoplasty may be undertaken for velopharyngealinsufficiency, this internal carotid anomaly is particularly relevant.

Internal carotid with aberrant loop lying in thecoronal plane of the neck. – add pulsating internal carotid
artery video link here

Post-styloid compartment = carotid space – contains last 4 cranial nerves & great vessels & sympathetic
chain




PVC – is occupied by Ascending palatine artery (APA)

Transoral approach to SUPERO-MEDIAL Parapharyngealtumors – incision anterior to anterior pillar of tonsil

Paraphayrngeal JNA removal by Endoscopic trans-oral approach by
Dr.Janakiram



The jugular bulb lies beneath the fl oor of the middle ear cavity (Roche et al. 2008 ) . It can be of variable shape and size. All the lower cranial nerves ( LCNs ) exit the foramen anteromedially to the jugular bulb, separated from it by connective
tissue. The superior ganglion of the vagus nerve is within the jugular foramen ( JF ). At the level of the intraforaminalcourse, there is a strict connection between the LCNs. The vagus nerve exits the JF vertically, behind IXcn and ICAp
(Roche et al. 2008 ) and gives its inferior ganglion on the outer skull base surface. The accessory nerve lies immediately lateral to the vagus nerve.
CR carotid ridge, DM digastric muscle (posterior belly), ICAp parapharyngeal portion of theinternal carotid artery, IJV internal jugular vein, JB jugular bulb, MMA middle meningeal
artery, VIIcn facial nerve, IX glossopharyngeal nerve, X vagus nerve, XI accessory nerve, XIIhypoglossal nerve, black arrow inferior ganglion of vagus nerve

Internal Jugular foramen External jugular foramen

Right side. The acousticofacial nerve bundle, posteriorinferior cerebellar artery, and lower cranial nerves are seenin the lower part. The inferior cerebellar vein (not constant)enters the jugular bulb. As the posterior fossa is approachedfrom behind the sigmoid sinus, the jugular dural fold appearsas a white linear structure overlying the lower cranial nerves.
Right side. The acousticofacial nerve bundle, posteriorinferior cerebellar artery, and lower cranial nerves are seenin the lower part. The inferior cerebellar vein (not constant)enters the jugular bulb. As the posterior fossa is approachedfrom behind the sigmoid sinus, the jugular dural fold appearsas a white linear structure overlying the lower cranial nerves.

A closer view of the pars nervosa of the jugular foramen. The glossopharyngeal nerve has its own dural porus, which is situated 0-3 mm upwards from the duralporus of the tenth cranial nerve. The vagus and the accessorynerve exit the posterior fossa together in a sleeve of durathrough the jugular foramen.
Closer view of the inferior area of the left CPA, with
the tip of the endoscope just over the flocculus. The vagus nerve
(X) and spinal accessory nerve (XI) arise as a widely separatedseries of rootlets that originate from the lower medulla and from theupper cervical cord. The rootlets of the hypoglossal nerve (XII) runhorizontally and are displaced and stretched by the curved vertebral
artery (VA). The posterior-inferior cerebellar artery (PICA) arisesfrom the vertebral artery and forms a vascular loop inferior to the
root exit /entry zone of the acoustic-facial nerve bundle (VII/ VIII).

When they exit from the skull base, the glossopharyngeal nerve is the most lateral, while the hypoglossal nerve is the most medial. The glossopharyngeal nerve crosses the internal carotid artery shortly after exiting the skull base.Thehypoglossal nerve
turns inferiorly to run together with the vagus nerve for a short distance in the upper neck (Fig. 8.4).

The glossopharyngeal nerve is seen crossing the internal carotid artery. More inferiorly, the hypoglossal nerve crosses the artery and passes anteriorly. The vagus nerve is seen coursing
between the internal jugular vein and the internal carotid artery. The accessory nerve crosses anterolateral to the internal jugular vein and travels posteriorly (Fig. 8.5).

In about half the cases, the accessory nerve crosses posteromedial to the internal jugular vein.
In all cases, it passes anterolateral to the transverse process of the atlas. Note the close relation between the vertebral artery and the internal jugular vein. In
extensive cases of posteriorly located glomus tumors, the vertebral artery may be involved .




In infrapetrous approach there are chances of injury to 6th nerve [ in dorello’scanal medial to paraclival carotid ] & 12th nerve


V3 & MMA

V 3 falls like niagara falls from middle cranial fossa to infratemporalfossa 90 degrees away from V1 & V2 – it is anterior to all the 3
structures , Petrous carotid & ET tube & Parapharyngeal carotid

ATN = Auriculotemporal nerve



MMA


IAN = Inferior alveolar nerve


My forceps touched the lingual nerve , posterior to this LN is Inferior alveolar nerve – These two nerves present in triangle formed by
medial pterygoid , lateral pterygoid & temporalis muscle


Chorda[CT] attached to LN

Chorda[CT] attached to LN

Schematic diagram for infratemporalfossa approach

Sometimes V3 can be seen in the sphenoid sinus – in “pneumosinus dilatans multiplex”

The greater wing of sphenoidal is almost completely pnematised. So is the temporal bone on the left.the Left carotid can be traced from the middle ear to the sphenoid - in “pneumosinus dilatans
multiplex”

V3 & MMA

V3 & MMA

V3[MN] & MMA & ET in lateral & Anterior skull base – see the relationship of ET tube which is medial to V3 & MMA


Posterior boarder of Lateral pterygoid bone leads to Foramen Ovale [ FO ] – Dr.Kuriakose

Posterior boarder of Lateral Pterygoid bone leads to Foramen Ovale [ FO ] – Dr.Kuriakose

Endoscopically [ Anterior skull base ] if we follow upper end of LPT posteriorly we can reach V3 [ Posterior boarder of Lateral Pterygoid bone leads to Foramen Ovale –
Dr.Kuriakose ]
View in nasopharyngectomy of recurrent nasopharyngeal carcinoma

In Infratemporal fossa approach- Posterior boarder of Lateral pterygoid bone leads to Foramen Ovale [ FO ] – Dr.Kuriakose

V3 is anterior (infront) to Horizontal carotid (= Petrous carotid ) & ET – It cause indentation on the
ET also .

In open approaches in maxillary swing approach as long as you stay lateral to ET you will not injure the
horizontal part of carotid

Petrous carotid & paraclival carotid is SADDLE shape – LEG of the rider is V3

V 3 is anteriror to all the 3 structures - Petrous carotid & ET & Parapharyngeal carotid [ very imp ]

Cochlea in anterior skull base
b is cochlea in middle cranial fossa – cochlear angle between GSPN & IAC

1. V3 is an important landmark to locate the post-styloid compartment, as it is anterior to this space (Falcon et al. 2011 ) .
2. styloid process & tensor veli palatini seperates pre-styloid & post-styloidcompartments .

TP & LP




See the relationship of MPP & TP which is just posterior



Sinus of Morgagni - In nasopharyngeal carcinoma, the tumor may
extend laterally and involve this sinus involving the Mandibular nerve. This produces a triad of symptoms known as Trotter's triad [ 1) Conductive deafness ( due to
eustachian tube involvement) 2) Ipsilateral immobility of soft palate 3) Neuralgic pain in the distribution of V3 ]
Add fossa of rosenmullardiagram photo present in
scott brown text book


See the relationship between LPP & V3 which is just posterior


Eustachian tube

ET is just posterior to MPP [ Lateral part of Posterior choanae is MPP ]

ET is just posterior to MPP

ET is pointing like an ARROW the posterior genuof internal carotid [ ICAp & CF is parapharyngeal
carotid ]

Sinus of Morgagni - In nasopharyngeal carcinoma, the tumor may
extend laterally and involve this sinus involving the Mandibular nerve. This produces a triad of symptoms known as Trotter's triad [ 1) Conductive deafness ( due to
eustachian tube involvement) 2) Ipsilateral immobility of soft palate 3) Neuralgic pain in the distribution of V3 ]



black asterisks medial corridor to ICAp – TVPM attached to anterior surface of ET – so if we go inbetween MPM & TVPM
we reach to ICAp


Bony-cartilagenous junction of ET tube is at posterior genu of carotid - ET is pointing like an ARROW the
posterior genu of internal carotid

Yellow arrow - Bony-cartilagenous junction of ET tube is at posterior genu of carotid - ET is pointing like an
ARROW the posterior genu of internal carotid

V 3 is anteriror to all the 3 structures - Petrous carotid & ET & Parapharyngeal carotid [ very imp ]


ET tube in SPF [Spheno-petrosal fissure]

At bony-cartilagenous junction of ET tube – Horizonalcarotid & Parapharyngeal carotid is above & below ET -
My understanding

In open approaches in maxillary swing approach as long as you stay lateral to ET you will not injure the
horizontal part of carotid

Fossa of Rossenmuller apex is laceral carotid [ Foramen Lacerum ] pharyngeal recess (fossa of Rosenmüller), which projects laterally from the
posterolateral corner of the nasopharynx with its lateral apex facing the internal carotid artery laterally and the foramen lacerum above;

endonasal approaches to expose thearea between the ICAs belong to the sagittal plane, and the
approachesaround the ICA define the coronal plane modules.

Note that the eustachian tube indicates the carotid canal only approximately. In other words, it lies ona different CORONAL plane in respect of the vessel, and from an anterior viewpoint, it covers the vessel for all its
length. -- Medially the space between these two CORONAL planes is nothing but Fossa of Rosenmuller [ My understanding ]

Note that the eustachian tube indicates the carotid canal only approximately. In other words, it lies on
a different CORONAL plane in respect of the vessel, and from an anterior viewpoint, it covers the vessel for all its
length. -- Medially the space between these two CORONAL planes is nothing but Fossa of Rosenmuller [ My understanding ]

Surgeons should have in mind that the external orifi ce of the carotid canal is not on the same
coronal plane of the foramen lacerum (anterior genu). It is by far more posteriorlylocated.


GSPN-VIDIAN NERVE

Vidian canal is 2 cm to foramen lacerum – Amin kassam – refer paolo castelnuovo book , Foramen rotundum is 5mm to dura –
listen 4.00 time in this video https://www.youtube.com/watch?v=Uk57MEgkde8

Gasserian ganglion is intradural – it is not extradural or intradural – listen 4.00 time in this video
https://www.youtube.com/watch?v=Uk57MEgkde8

GSPN passes above Horizontal [=petrous] carotid & passes underneath V3 & crosses petro-paraclival carotid junction at
foramen lacerum before becoming vidian nerve

The bone overlying the internal auditory canal has been removedand the dura of the canal has been removed near the fundus. The
facial nerve (FN) can be seen entering its labyrinthine segment to form thegeniculate ganglion (GG) more laterally. V Trigeminal nerve, < Acousticofacial
bundle, C Cochlea, ET Eustachian tube, GPN Greater petrosalnerve, I Incus, IAC Internal auditory canal, ICA Internal carotid artery,
M Malleus, SSC Superior semicircular canal, SV Superior vestibular nerve
Observe the relationship between GSPN & horizontal carotid

Fig. 2.62 The course of the horizontal segment of the internal carotidartery (ICAh), as seen from the middle cranial fossa of a left temporalbone. VI Abducent nerve, C Cochlea, GPN Greater petrosal nerve, IAC
Internal auditory canal, ICA(ic) Intracranial internal carotid, M Mandibularnerve, MMA Middle meningeal artery, MX Maxillary nerve

Fig. 5.47 The view after completion of the middle crannial fossa approach. AE Arcuate eminence,BB Bill’s bar, C Cochlea, FN(iac) Internal auditory canal segmentof the facial nerve, FN(t) Tympanic segment of the facial nerve,
G Geniculate ganglion, GPN Greater petrosal nerve, I Body of the incus,L Labyrinthine segment of the facial nerve, M Head of the malleus,
MFD Middle fossa dura, SVN Superior vestibular nerve

In Infratemporal fossa - Note that the greater petrosal nerve (GPN) is adherent
to the dura, and that retracting the durawill lead to stress on the
facial nerve at the geniculate ganglion (GG) level. Thus, if dural retraction
is needed, cutting the petrosal nerve will prevent this injury.
In middle cranial fossa – same point

Foramen lacerumAFL = Anterior foramen lacerum
* [ black asterisk ] = foramen lacerum
Petrolingual area = foramen lacerum

After elevating V3 anterior[infront] to ET & petrous carotid observe -- GSPN continues as VN [ VN is lateral to paraclival
carotid ]

GSPN & GSPN groove in Surpra petrous windowET eustachian tube, GPN greater petrosal nerve, MCFd dura of the middle cranial fossa, MMA
middle meningeal artery, SPS superior petrosal surface, TI trigeminal impression, V3 thirdbranch of the trigeminal nerve, yellow arrow accessory middle meningeal artery, white
asterisks greater petrosal nerve groove

Vidian nerve is formed by GSPN & Deep petrosal nerve – so GSPN (passes underneath V3) crosses laterally the Horizontal carotid and paraclival carotid
junction (Prof.Kassam) & continues as Vidian nerve
Blue arrow – LPN & Yellow arrow – GPN

Trans-pterygoid approch-- Vidian Artery present in 60% & enters at the junction of Horizontal carotid & paraclival carotid – it is present above the Vidian nerve so while drilling vidian canal in
JNA first we have to drill inferior half and then upper half [the bone around the vidiancanal is drilled along its inferior half (from 3 o’clock to 9 o’clock) until the carotid
artery is identified at the lacerum segment ]

Vidian nerve - lateral to paraclival carotid & medial to FO [ Foramen Ovale ]- actually it is
GSPN

Vidian canal & Spheno-palatine foramen are in 90 degrees


Vidian nerve - lateral to paraclivalcarotid

Vidian nerve - lateral to paraclival carotid

Vidian nerve - lateral to paraclivalcarotid

Vidian nerve - lateral to paraclival carotid
Close vision of the middle cranialfossa. The gasserian ganglion has been removed

Vidian nerve - lateral to paraclivalcarotid

Axial T2-weighted magnetic resonance imaging (MRI) sequence at the level of the vidian canal: 1, clivus; 2, pterygoid; 3,
horizontal tractof the internal carotid artery (ICA); 4, vidian canal.

The space between V1 & V 2 and V2 & V3 is sphenoid sinus
Middle cranial fossa approach –the nerve between V2 & V3 is VN
Anterior skull base

Infratemporal fossa approach type C
Middle cranial fossa approach –the nerve between V2 & V3 is VN

Foramen lacerumAFL = Anterior foramen lacerum
* [ black asterisk ] = foramen lacerum
Petrolingual area = foramen lacerum

Vidian artery – origin from Laceralsegment

Lateral Recess is the space between V2 & Vidian nerve .

Courtesy – Dr. Satish Jain , Jaipur

Lateral Recess is the space between V2 & Vidian nerve .

Here TI [ trigeminal impression ] is V2

LRSS = Lateral recess of the sphenoid sinus



Floor of Lateral recess is by ET ----BS basisphenoid, ET eustachian tube, LRSS lateral recess of the sphenoid sinus, OPPB orbital
process of the palatine bone, PVA(s) palatovaginal artery(ies), RPm rhinopharyngeal mucosa,SPAib inferior branch of the sphenopalatine artery, SPPB sphenoidal process of the palatine bone,
SS sphenoid sinus, RS rostrum sphenoidale, VN vidian nerve


Surpra petrous windowET eustachian tube, GPN greater petrosal nerve, MCFd dura of the middle cranial fossa, MMA
middle meningeal artery, SPS superior petrosal surface, TI trigeminal impression, V3 thirdbranch of the trigeminal nerve, yellow arrow accessory middle meningeal artery, white
asterisksgreater petrosal nerve groove


Carotid nerve

Transmaxillary infratemporal fossa approach –Endoscopic assisted microscopic approach –mainly useful for stage 4 JNAs & cavernous
extensions
• Click video : https://www.youtube.com/watch?v=Uk57MEgkde8

For Other powerpoint presentatioinsof
“ Skull base 360° ”I will update continuosly with date tag at the end as I am
getting more & more information
click
www.skullbase360.in- you have to login to slideshare.net with Facebook
account for downloading.