Middle Fossa Surgical Anatomy Related to the Subtemporal ... · Middle Fossa Surgical Anatomy...
6
TurkIs/i Neitrosiirgery 11: 38 - 43, 2001 Avci: Aii AIIlltomIc Stiid!! Middle Fossa Surgical Anatomy Related to the Subtemporal Preauricular Infratemporal Approach: An Anatomic Study Subtemporal Preaurikular Infratemporal Girisimde Orta Fossa Cerrahi Anatomisi: Anatomik Çalisma EMEL Avci, YALÇIN KOCAOGULLAR, DAMIREZ FOSSETT, ANTHONY CAPUTY The Harvey H. Ammerman Neurasurgical Laboratory Department of Neurosurgery George Washington University, Washington DC, (EA, DF, AC) Selçuk University School of Medicine, Department of Neurosurgery (YK) Konya, Turkey Received : 4.1.2001 ~ Accepted : 31.1.2001 Abstract: Lesions in the extradural middle and upper elival region, ineluding the posterior cavernous sinus, and those in the infratemporal and middle fossa areas can be accessed by the subtemporal preauricular infratemporal approach. This method requires drilIing of the petrous bone and elivus, and mobilization of the petrous internal carotid artery. The anatomy of the petrous apex and middle cranial fossa is complex, and thorough knowledge of the anatomic landmarks in this area is necessary in order to explore the petrous internal carotid artery with minimal risk. Key Words: Anatomy, elivus, infratemporal fossa, petrous carotid artery, trigeminal nerve INTRODUCTION it can be difficult to gain adequate surgical access to lesions anterior to the ventral brainstem involving the upper petroc1ival region, lesions of the posterior cavernous sinus, and those in the infratemporal fossa. Direct anterior and inferolateral approaches have been used to reach these areas. Fisch described and later Fisch et aL.popularized the use of infratemporal approaches to access lesions of the lateral skull base (2,3,4). The subtemporal 38 Özet: Subtemporal preaurikular infratemporal girisim orta, üst klival bölge arka kavernoz sinus, infratemporal ve orta fos sa lezyonlarina yaklasimda uygulanabilecek bir cerrahi yaklasimdir. Klivus ve petroz kemigin drilIenmesi, petroz internal karotis arterin mobilizasyonu bu cerrahi yaklasimdaki ana unsurlardandir. Petraz internal karotis arterin minimal cerrahi risk ile ortaya konmasi orta fossa ve petroz apeksin kompleks anatomik yapilarinin ayrintili olarak bilinmesini gerektirmektedir. Anahtar Kelimeler: Anatomi, infratemporal fossa, klivus, petroz karotis arter, trigeminal sinir preauricular infratemporal approach is a modification one of Fisch's classic approaches (lO,l1,12). Though it offers excellent access to the regions of interest mentioned above, the exposure is complex, requiring extensive bone removal and mobilization of the petrous internal carotid artery. Our aim in this investigation was to define of the anatomy of the floor of the middle fossa in order to safely identify, preserve and mobilize the petrous internal carotid artery.
Transcript of Middle Fossa Surgical Anatomy Related to the Subtemporal ... · Middle Fossa Surgical Anatomy...
TurkIs/i Neitrosiirgery 11: 38 - 43, 2001 Avci: Aii AIIlltomIc Stiid!!
Middle Fossa Surgical Anatomy Related to the SubtemporalPreauricular Infratemporal Approach: An Anatomic Study
Subtemporal Preaurikular Infratemporal Girisimde Orta FossaCerrahi Anatomisi: Anatomik Çalisma
EMEL Avci, YALÇIN KOCAOGULLAR,
DAMIREZ FOSSETT, ANTHONY CAPUTY
The Harvey H. Ammerman Neurasurgical Laboratory Department of Neurosurgery
George Washington University, Washington DC, (EA, DF, AC)
Selçuk University School of Medicine, Department of Neurosurgery (YK) Konya, Turkey
Received : 4.1.2001 ~ Accepted : 31.1.2001
Abstract: Lesions in the extradural middle and upper elivalregion, ineluding the posterior cavernous sinus, and thosein the infratemporal and middle fossa areas can be accessedby the subtemporal preauricular infratemporal approach.This method requires drilIing of the petrous bone andelivus, and mobilization of the petrous internal carotidartery. The anatomy of the petrous apex and middle cranialfossa is complex, and thorough knowledge of the anatomiclandmarks in this area is necessary in order to explore thepetrous internal carotid artery with minimal risk.
Key Words: Anatomy, elivus, infratemporal fossa,petrous carotid artery, trigeminal nerve
INTRODUCTION
it can be difficult to gain adequate surgicalaccess to lesions anterior to the ventral brainstem
involving the upper petroc1ival region, lesions of theposterior cavernous sinus, and those in theinfratemporal fossa. Direct anterior and inferolateralapproaches have been used to reach these areas. Fischdescribed and later Fisch et aL.popularized the useof infratemporal approaches to access lesions of thelateral skull base (2,3,4). The subtemporal
38
Özet: Subtemporal preaurikular infratemporal girisimorta, üst klival bölge arka kavernoz sinus, infratemporalve orta fos sa lezyonlarina yaklasimda uygulanabilecek bircerrahi yaklasimdir. Klivus ve petroz kemigin drilIenmesi,petroz internal karotis arterin mobilizasyonu bu cerrahiyaklasimdaki ana unsurlardandir. Petraz internal karotisarterin minimal cerrahi risk ile ortaya konmasi orta fossave petroz apeksin kompleks anatomik yapilarinin ayrintiliolarak bilinmesini gerektirmektedir.
Anahtar Kelimeler: Anatomi, infratemporal fossa, klivus,petroz karotis arter, trigeminal sinir
preauricular infratemporal approach is amodification one of Fisch's classic approaches(lO,l1,12). Though it offers excellent access to theregions of interest mentioned above, the exposure iscomplex, requiring extensive bone removal andmobilization of the petrous internal carotid artery.Our aim in this investigation was to define of theanatomy of the floor of the middle fossa in order tosafely identify, preserve and mobilize the petrousinternal carotid artery.
Tiirkish Nelll'Oslirgery 11: 38 - 43, 2001
MATERIALS AND METHOD S
This study was performed in the HarveyAmmerman Neurosurgical Laboratory at The GeorgeWashington University School of Medicine,Department of Neurosurgery. Ten adult cadaverspecimens with intracranial arteries and veinsinjected with colored silicon were used. After thevessels were injected, the subtemporal preauricularinfratemporal approach was performed. A CarI ZeissUniversal 52 operating microscope was used duringdissection of the anatomic structures on the floor ofthe middle fossa, and for drilling of the petrous boneand elivus. Drilling was done with a Midas Rex(Texas, USA) high-speed air drilL.Marathon 8-inchj200-mm Electronic Digital Calipers were used for allmeasurements.
Each dissection was done with the cadaver head
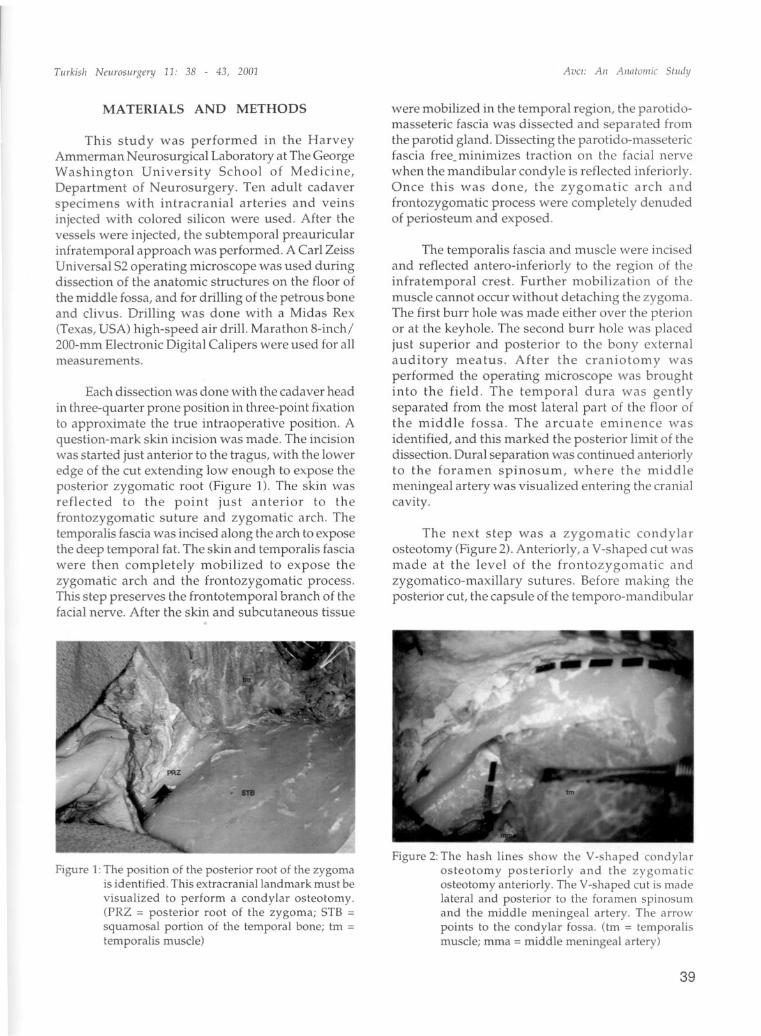
in three-quarter prone position in three-point fixationto approximate the true intraoperative position. Aquestion-mark skin incision was made. The incisionwas started just anterior to the tragus, with the loweredge of the cut extending low enough to expose theposterior zygomatic root (Figure 1). The skin wasreflected to the point just anterior to thefrontozygomatic suture and zygomatic arch. Thetemporalis fascia was incised along the arch to exposethe deep temporal fat. The skin and temporalis fasciawere the n completely mobilized to expose thezygomatic arch and the frontozygomatic process.This step preserves the frontotemporal branch of thefacial nerve. After the skin and subcutaneous tissue
Figure 1:The position of the posterior root of the zygomais identified. This extracraniallandmark must be
visualized to perform a condylar osteotomy.(PRZ = posterior root of the zygoma; STB =squamosal portion of the temporal bone; tm =temporalis muscle)
Avci: Aii Aiia/oll/ic S/iidy
were mobilized in the temporal region, the parotidomasseteric fascia was dissected and separated fromthe parotid gland. Dissecting the parotido-massetericfascia free_minimizes traction on the facial nervewhen the mandibular condyle is reflected inferiorly.Once this was done, the zygomatic arch andfrontozygomatic process were completely denudedof periosteum and exposed.
The temporalis fascia and muscle were incisedand reflected antero-inferiorly to the region of theinfratemporal crest. Further mobilization of themusele cannot occur without detaching the zygoma.The first burr hole was made either over the pterionor at the keyhole. The second burr hole was placedjust superior and posterior to the bony externalauditory meatus. After the craniotomy wasperformed the operating microscope was broughtinto the field. The temporal dura was gentlyseparated from the most lateral part of the floor ofthe middle fossa. The arcuate eminence was
identified, and this marked the posterior limit of thedissection. Dural separation was continued anteriorlyto the foramen spinosum, where the middlemeningeal artery was visualized entering the cranialcavity.
The next step was a zygomatic condylarosteotomy (Figure 2). Anteriorly, a V-shaped cut wasmade at the level of the frontozygomatic andzygomatico-maxillary sutures. Before making theposterior cut, the capsule of the temporo-mandibular
Figure 2: The hash lines show the V-shaped condylarosteotomy posteriorly and the zygomaticosteotomy anteriorly. The V-shaped cut is madelateral and posterior to the foramen spinosumand the middle meningeal artery. The arrowpoints to the condylar fossa. (tm = temporalismuscle; mma = middle meningeal artery)
39

Tiirkish Neiirosiirgery 11: 38 - 43, 2001
joint was exposed, cut sharply and the meniscus ofthe joint was separated from the condylar fossa. Theposterior cut was the n ma de and the zygomatic archwas removed (Figure 3). In performing thisosteotomy, care must be taken not to enter the middleear cavity (Figure 4). Once the arch was removed,the floor of the middle fossa was dissected to exposethe mandibular (V3) and maxillary divisions (V2) ofthe trigeminal nerve. Dissection between the arcuateeminence and the middle meningeal artery exposedthe lesser superficial petrosal nerve extendingtowards the foramen ovale. Once this nerve was cut,medial separation of the dura continued. The middle
Figure 3:A large frontotemporal craniotomy and acondylar orbitozygomatic osteotomy have beenperformed. The arrow indicates the condylarfossa. (ftd = frontotemporal dura; o = orbit; tm =temporalis muscle)
Figure 4: A dry skull specimen showing the proximity ofthe temporomandibular joint to the externalauditory meatus. When performing the condylarosteotomy, care must be taken to avoid enteringthe external auditory canal. (eam = externalauditory meatus; tmj = temporomandibular joint)
40
Avci: Aii Allnloiliic Sliidy
meningeal artery was alsa transected to permitfurther medial dissection and to expose thegreater supedicial petrosal nerve emerging fromthe faeial hiatus. A venous plexus, an extensionof the cavernous sinus, was observed surroundingthe branches of the fifth cranial nerve. There was
alsa a venous plexus in the region of Meckel'scave.
The greater supedicial petrosal nerve wassectioned and further medial elevatian of the dura
exposed part of the horizontal segment of the petrousinternal carotid artery. The horizontal part of thepetrous internal carotid artery was covered witheither thin bone, fibrous layer or no bone. The portianof the middle fossa lateral to the greater superfieialpetrosal nerve, V3, and V2 was drilled to expose thelateral part of the root of the pterygoid process.Drilling the bone of the middle fossa between V2 andV3 may expose the sphenoid sinus (Figures 5 and 6).The internal carotid artery was usually surroundedbya venous plexus. While drilling the bone laterally,the tensor tympani muscle and eustachian tube wereidentified and transected. Once these structures were
cut, drilling was continued to expose the superior,lateral, and inferior walls of the horizontal part ofthe petrous internal carotid artery. This vessel wasthen completely free to be retracted anteriorly. Whiledrilling posteriorly, care should be taken not toencounter the cochlea. The petrous pyrainid wasdrilled completely to expose the dura of the posteriorfossa, which was bounded by the superior petrosalsinus above and the inferior petrosal sinus below.The dura was opened in the region of Meckel's cave(Figure 7).
The following distance measurements weremade: foramen spinosum to foramen ovale; foramenovale to foramen rotundum; foramen rotundum tosuperior orbital fissure; foramen spinosum to lateralwall of the internal carotid artery; foi amen ovale tolateral wall of the internal carotid artery; geniculateganglion to intersection between the lateral marginof V3 and the greater superficial petrosal nerve; andgeniculate ganglion to foramen spinosum. Diametermeasurements were recorded for the foraminaspinosum, ovale, rotundum, and lacerum, as well asthe superior orbital fissure. Alsa noted were thelocation of the greater superficial petrosal nerve inrelation to the internal carotid artery, and thepresence or absence of bone between the greatersuperfieial petrosal nerve and the internal carotidartery.
Turkish Neurosiirgenj 11: 38 - 43, 2001
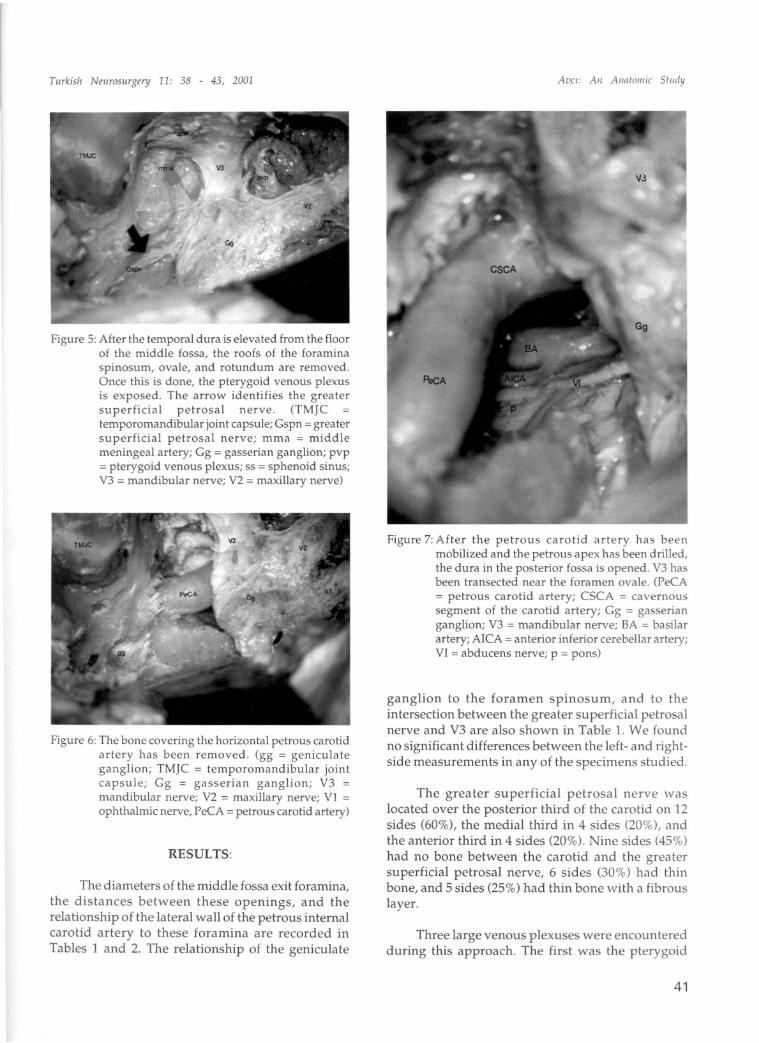
Figure 5: After the temporal dura is elevated from the floorof the middle fossa, the roofs of the foraminaspinosum, ovale, and rotundum are removed.Once this is done, the pterygoid venous plexusis exposed. The arrow identifies the greatersupedicial petrosal nerve. (TMJCtemporomandibular joint capsule; Gspn = greatersuperHcial petrosal nerve; mma = middlemeningeal artery; Gg = gasserian ganglion; pvp= pterygoid venous plexus; ss = sphenoid sinus;V3 = mandibular nerve; vi = maxillary nerve)
Figure 6: The bone covering the horizontal petrous carotidartery has been removed. (gg = geniculateganglion; TMJC = temporomandibular jointcapsule; Gg = gasserian ganglion; V3 =mandibular nerve; vi = maxillary nerve; VI =ophthalmic nerve, PeCA = petrous carotid artery)
RESULTS:
The diameters of the middle fossa exit foramina,
the distances between these openings, and therelatianship of the lateral wall of the petrous internalcarotid artery to these foramina are recorded inTables 1 and 2. The relatianship of the geniculate
Avci: Aii AJlntolii;c Study
Figure 7: After the petrous carotid artery has beenmobilized and the petrous apex has been drilled,the dura in the posterior fossa is opened. V3 hasbeen transected near the foramen ovale. (PeCA= petrous carotid artery; CSCA = cavernoussegment of the carotid artery; Gg = gasserianganglion; V3 = mandibular nerve; SA = basilarartery; AICA = anterior inferior cerebellar ar tery;VI = abducens nerve; p = pons)
ganglion to the foramen spinosum, and to theintersection between the greater superficial petrosalnerve and V3 are alsa shown in Table i. We found
no significant differences between the left- and rightside measurements in any of the specimens studied.
The greater superhcial petrosal nerve waslocated over the posterior third of the carotid on 12sides (60%), the medial third in 4 sides (20%), andthe anterior third in 4 sides (20%). Nine sides (45%)
had no bone between the carotid and the greatersuperficial petrosal nerve, 6 sides (30%) had thinbone, and 5 sides (25%) had thin bone with a fibrous
layer.
Three large venous plexuses were encounteredduring this approach. The first was the pterygoid
41
Tiirkish Neiirosiirgery 11: 38 - 43, 2001
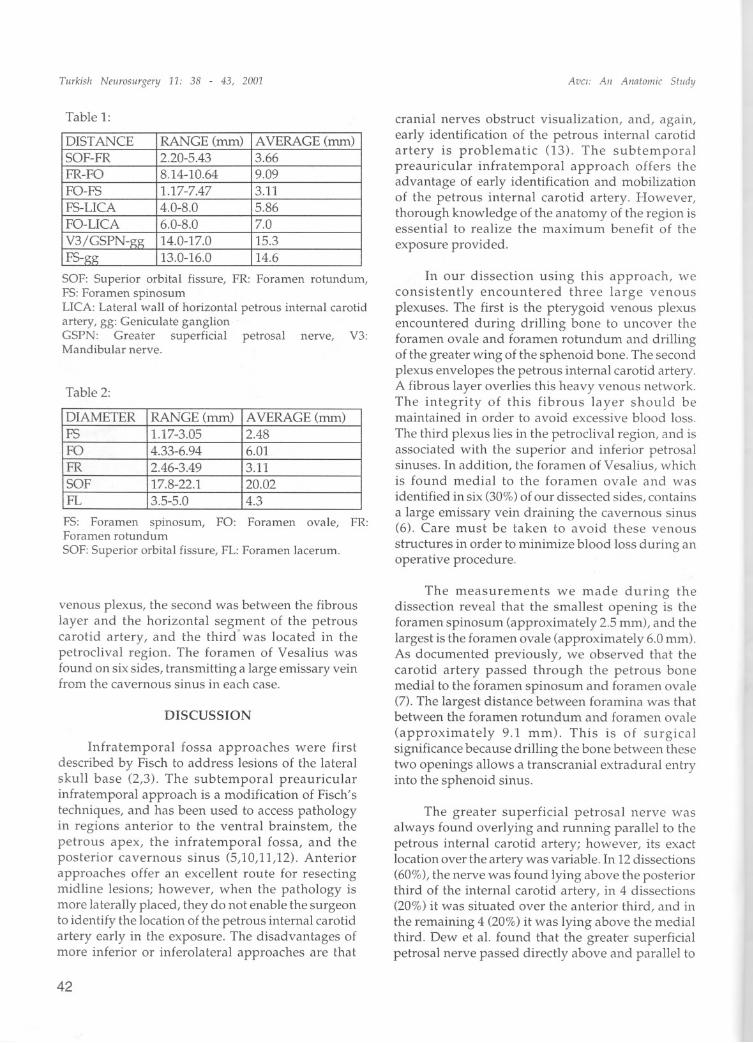
Table 1:
DISTANCE RANGE(mm)AVERAGE (mm)SOF-FR
2.20-5.433.66FR-FO
8.14-10.649.09FO-FS
1.17-7.473.11FS-LICA
4.0-8.05.86FO-LICA
6.0-8.07.0V3/GSPN-gg
14.0-17.015.3FS-gg
13.0-16.014.6
SAF: Superior orbital fissure, FR: Foramen ratundum,FS:Foramen spinosumLICA:Lateral wall of horizontal petrous internal carotidartery, gg: Geniculate ganglionGSPN: Greater superficial petrosal nerve, V3:Mandibular nerve.
Table 2:
DIAMETER RANGE(mm)AVERAGE (mm)FS
1.17-3.052.48FO
4.33-6.946.01FR
2.46-3.493.11SOF
17.8-22.120.02FL
3.5-5.04.3
FS: Foramen spinosum, FO: Foramen ovale, FR:Foramen rotundumSAF:Superior orbital fissure, FL: Foramen lacerum.
venous plexus, the second was between the fibrouslayer and the horizontal segment of the petrouscarotid artery, and the third· was located in thepetroclival region. The foramen of Vesalius wasfound on six sides, transmitting a large emissary veinfrom the cavernous sinus in each case.
DISCUSSION
Infratemporal fossa approaches were firstdescribed by Fisch to address lesions of the lateralskuII base (2,3). The subtemporal preauricularinfratemporal approach is a modification of Fisch'stechniques, and has been used to access pathologyin regions anterior to the ventral brainstem, thepetrous apex, the infratemporal fossa, and theposterior cavernous sinus (5,10,11,12). Anteriorapproaches offer an excellent route for resectingmidline lesions; however, when the pathology ismore lateraIly placed, they do not enable the surgeonto identify the location of the petrous internal carotidartery early in the exposure. The disadvantages ofmore inferior or inferolateral approaches are that
42
Avci: Aii Aiiatomic Stiidy
cranial nerves obstruct visualization, and, again,early identification of the petrous internal carotidartery is problematic (13). The subtemporalpreauricular infratemporal approach offers theadvantage of early identification and mobilizationof the petrous internal carotid artery. However,thorough knowledge of the anatomy of the region isessential to realize the maximum benefit of the
exposure provided.
In our dissection using this approach, weconsistently encountered three large venousplexuses. The first is the pterygoid venous plexusencountered during driIIing bone to uncover theforamen ovale and foramen rotundum and driIIingof the greater wing of the sphenoid bone. The secondplexus envelopes the petrous internal carotid artery.A fibrous layer overlies this heavy venous network.The integrity of this fibrous layer should bemaintained in order to avoid excessive blood loss.The third plexus lies in the petroclival region, and isassociated with the superior and inferior petrosalsinuses. In addition, the foramen of Vesalius, whichis found medial to the foramen ovale and wasidentified in six (30%)of our dissected sides, containsa large emissary vein draining the cavernous sinus(6). Care must be taken to avoid these venous
structures in order to minimize blood loss during anoperatiye procedure.
The measurements we made during thedissection reveal that the smallest opening is theforamen spinosum (approximately 2.5 mm), and thelargest is the foramen ovale (approximately 6.0 mm).As documented previously, we observed that thecarotid artery passed through the petrous bonemedial to the foramen spinosum and foramen ovale(7). The largest distance between foramina was thatbetween the foramen rotundum and foramen ovale
(approximately 9.1 mm). This is of surgicalsignificance because driIIing the bone between thesetwo openings allows a transcranial extradural entryinto the sphenoid sinus.
The greater supedicial petrosal nerve wasalways found overiying and running parallel to thepetrous internal carotid artery; however, its exactlocation over the artery was variable. In 12 dissections(60%), the nerve was found lying above the posteriorthird of the internal carotid artery, in 4 dissections(20%) it was situated over the anterior third, and inthe remaining 4 (20%) it was lying above the medialthird. Dew et aL.found that the greater supedicialpetrosal nerve passed directly above and paraIlel to

Turkish Neiirosurgery 11: 38 - 43, 2001
the internal carotid artery in 21% of their specimens.In 7%, the nerve was either medial to lying over themedial aspect of the artery, and in 64% it ran medialto lateralover the artery and continued its anteriorroute lateral to the artery (1).Naquib et aL.alsa founda variable but parallel course of the greater superficialpetrosal nerve in relation to the carotid artery (8).They found that the intersection of V3 with thegreater superficial petrosal nerve was always foundto overlying the petrous internal carotid artery.
In our cadavers, we found that the petrousinternal carotid ar tery was not always covered bybone. In 9 (45%) of the dissections, there was no boneseparating the greater superficial petrosal nerve fromthe petrous carotid artery. Similarly, Paullus et aL.found that approximately half of their 50 carotidarteries were not covered by bone (9). Injury to thepetrous carotid artery can occur if the greatersuperficial petrosal nerve is not dissected carefully.
For the subtemporal preauricular infratemporalapproach, the geniculate ganglion and the cochlearapparatus mark the lateralmost limit of thedissection. In our dissections, on average, the distancebetween geniculate ganglion and the intersection ofthe greater superficial nerve with V3 was 15.3 mm,and the distance from the geniculate ganglion to theforamen spinosum was 14.6 mm.
The subtemporal preauricular infratemporalapproach offers the aforementioned benefits of earlyidentification and mobilization of the petrous internalcarotid artery, direct unimpeded access to the regionof the petrous apex, minimal brain retraction,preservation of the hearing apparatus, preservationof the facial nerve, avoidance of traversing nasalsinuses, and ease of reconstruction. However, onedisadvantage is the need to disarticulate themandibular condyle for condylar resection, whichmay lead to trismus or malocclusion if realignmentis not done properly. Another drawback is the needto mobilize the petrous internal carotid artery inorder to gain access to the region of the petrous apex.Failure to mobilize the carotid artery greatlyminimizes the exposure gained with this approach.A further issue is that the eustachian tube must besacrificed in this approach, and this may lead todelayed middle ear pathology.
The advantages of the subtemporal preauricularinfratemporal approach for anterolateral skull baselesionsfar outweigh the disadvantages; however, thistechnique requires extensive exposure, and demands
Avci: Aii Aiiatoiiiic Study
patience and diligence. A thorough knowledge of thesurraunding anatamy is crucial to the successfulperformance of this approach.
Correspondence: Emel Avci, MDDepartment of NeurosurgeryGeorge Washington University2150 Pennsylvania Ave NW, Suite 7-420Washington DC, 20037Fax: 001-202-994-9944E-mail: [email protected]
REFERENCES
1. Dew LA, Shelton C, Harnsberger R, Thompson, Jr. G:Surgieal exposure of the petrous internal carotid ;irtery:Praetical application for skull base surgery.Laryngoscope 107:967-976, 1997
2. Fisch U: The infratemporal fossa approach to tumomsof the temporal bone and base of skull. J. Liryngol Otol92: 949-967, 1978
3. Fiseh U: Infratemporal fossa approach for glomustumors of the temporal bone. Ann Otol Rhino Larnygol91:474-479, 1982
4. Fiseh U, Fagan P, Valavanis A: The infratemporal fossaapproaeh for the lateral skull base. Otolaryngol C1inNorth Am 17(3):513-442, 1984
5. Inoue T, Rhoton Jr AL, Theele D, Barry M: Surgicalapproaches to the cavernous sinus: A mierosurgicalstudy. Nemosmgery 26:903-932, 1990
6. Lang J: Clinical anatomy of the head, nemoeranium,orbit and craniocervieal regions. New York: SpringerVerlag, New York, 1983
7. Leonetti JP, Smith PG, Linthicum FH: The petrouscarotid artery: Anatomic relationships in skull basesurgery. Otolaryngol Head Neek Surg 102:1, 1990
8. Naguib MB, Aristegui M, Saleh E, et al : Surgiealanatomy of the petrous apex as it relates to the enlargedmiddle cranial fossa approaches. Otolaryngol HeadNeck Surg 111: 488-493, 1994
9. Paullus W, Pait G, Rhoton,Jr A: Microsurgical exposureof the petrous portion of the carotid artery. J Neurosurg47:713-726, 1977
10. Sanna M, Saleh E, Russo A, Taibah A: Atlas ofTemporal Bone and Lateral Skull Base Surger)'.Stuttgard, New York: George Thieme, 1995
11. Sekhar LN, Raso JL: Orbitozygomatic FrontotemporalApproach. Cranial Microsurgery: Approaches andTechniques. Eds. Sekhar LN, De Olivera New York,NY,1997
12. Sekhar L, Schramm V, Jones N: Subtemporalpreauricular infratemporal fossa approaeh to largelateral and posterior cranial base neoplasms. JNeurosurg 67:488-499, 1987
13. Sen C, Sekhar L: The subtemporal and preauricularinfratemporal approach to intradural structmes ventra!to the brainstem. J Neurosurg 73:345-354, 1990
14. Tedeschi H, Rhoton Jr. A: Lateral approaehes to thepetroclival region. Surg NeuroI41:180-216, 199.i
43