Surgical anatomy of Infratemporal fossa. by Dr. Aditya Tiwari
55
“Anatomy of infratemporal fossa & various surgical approaches to it” By.. Dr. Aditya Tiwari, Junior Resident, Dept. of E.N.T. Date: 14/07/2015
-
Upload
aditya-tiwari -
Category
Health & Medicine
-
view
1.614 -
download
1
Transcript of Surgical anatomy of Infratemporal fossa. by Dr. Aditya Tiwari

“Anatomy of infratemporal fossa &
various surgical approaches to it”
By..Dr. Aditya Tiwari,Junior Resident,Dept. of E.N.T.
Date: 14/07/2015

INTRODUCTION• The infratemporal fossa is an anatomic space of
great importance to neurological surgeons specializing in skull base surgery.
• Multiple neural and vascular structures enter & exit the infratemporal fossa via foramina in the skull base.
• Knowledge of these calrelationships is extremely important to neurological surgeons, neuro-otologists, craniofacial, and head and neck surgeons.

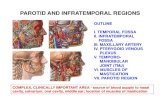
Osteology of ITF

INFRATEMPORAL FOSSA• Irregularly shaped space deep & inferior to zygomatic arch, deep to
ramus of mandible & post. To maxilla. • Communicates with temporal fossa through interval bwt (deep to)
zygomatic arch & (superficial to) cranial bones.
• Temporal fossa is superior to zygomatic arch,
• Infratemporal fossa is Inf. to zygomatic arch.

BOUNDARIES• Sup: Inf. surface of greater wing of the sphenoid• Inf: Where the medial pterygoid
muscle attaches to mandible near its angle.
• Ant: Post aspect of the maxilla• Post: Tympanic plate ,mastoid &
styloid processes of temporal bone, ant. aspect
• Med: Lateral pterygoid plate• Lat: Ramus of the mandible


OSTEOLOGY• F. ovale & spinosum open on its roof. • Alveolar canals open on its anterior wall.• At its upper & medial part are 2 fissures Form T-shaped fissure,
horizontal limb is inf. orbital, & vertical limb is pterygomaxillary.

APPROXIMATE LOCATION OF INFRATEMPORAL SPACE
A Temporalis muscleB Masseter muscleC Lateral pterygoid muscleD Medial ptaerygoid muscleE Superficial temporal spaceF Deep temporal spaceG Submasseteric space,H Pterygomandibular space,

CONTENTS & RELATED STRUCTURES• Muscle:- 1) Inferior part of temporalis muscle. 2) Lateral & medial pterygoid muscles• Ligaments:- Sphenomandibular ligament• Vessels:- 1) Maxillary artery & branches. 2) Pterygoid venous plexus• Nerves:- 1) Mandibular Nerve & branches. 2) Chorda tympani branch of facial nerve 3) Inf. alveolar, lingual, buccal nerve.• The otic parasympathetic ganglion


Temporalis muscle• Origin:-Temporal fossa & deep surface of temporal fascia• Insertion:-Medial surface, apex, ant. & post. border of coronoid
process and ant. border of ramus of the mandible• Blood supply:-Deep temporal part of maxillary artery• Nerve supply:-Deep temporal branches of ant. mandibular nerve.• Actions:- 1) Elevates & retracts mandible, 2) Side to side grinding movement.

LATERAL PTERYGOID• ORIGIN:• Upper head: Infratemporal surface of greater wing of sphenoid• Lower head: Lateral surface of lateral pterygoid plate• INSERTION: Pterygoid fovea (in front of neck of mandible) +
capsule & articular disc of TMJ• NERVE SUPPLY: Ant. division of mandibular nerve• ACTION: 1) Side-to-side movement. 2) Pulls condylar process forward to depress .

RELATIONS OF LATERAL PTERYGOID• Superficial: temporalis, masseter, ramus of mandible, maxillary artery,
buccal nerve• Deep: medial pterygoid, mandibular nerve, middle meningeal artery,
otic ganglion• Emerging through its upper border: deep temporal & masseteric
nerves• Emerging through its lower border: lingual & inferior alveolar nerves
+ maxillary artery• Emerging between its 2 heads: buccal nerve, maxillary artery

MEDIAL PTERYGOID• ORIGIN: Superficial head: Tuberosity of maxilla Deep head: Medial surface of lateral pterygoid plate • INSERTION: Medial surface of ramus & angle of mandible• NERVE SUPPLY: From trunk of mandibular nerve• ACTION: 1) Elevation of mandible 2) Protrusion of mandible (when muscles on both sides act together) 3)Side-to-side movement (when muscles on both sides act alternatively)

LIGAMENTS• Stylomandibular ligament:- Joins styloid process to angle of the
mandible & is a thickened part of parotid sheath.• Sphenomandibular ligament:- Suspends mandible & descends from
spine of sphenoid bone to lingula of mandible. • Pterygospinous ligament:- Join spine of sphenoid bone to post. border
of lat. pterygoid plate.

Neurovasculature of Infratemporal fossa• The maxillary artery is larger of 2 terminal branches of ECA. • Arises post. to neck of mandible & is divided into 3 parts based on its
relation to lat. pterygoid muscle. • 1st (Mandibular) part: Deep to condyle of mandible.• 2nd (Pterygoid) part: Neighbourhood of lat. pterygoid muscle.• 3rd (Pterygopalatine) part: Into pterygopalatine fossa.

Branches of the 1st part: 1) Deep auricular To ext. acoustic meatus. 2) Anterior tympanic artery To tympanic membrane. 3) Middle meningeal artery To dura mater & calvaria. 4) Accessory meningeal artery To cranial cavity. 5) Inf. alveolar artery To mandibular gingiva & teeth.
In first & third parts, five branches all enter foramina in bones.From second part, none of branches go through bony foramina.

Branches of the 2nd part: 1) Deep temporal art (to temporal muscle) 2) Pterygoid artery(to pterygoid muscles) 3) Masseteric artery (to masseter muscle) 4) Buccal artery (to buccinator muscle)Branches of the 3rd part: 1) Deep auricular (da), 2) Ant. tympanic (at) 3) Middle meningeal (mm) 4) Acc. middle meningeal (amm) 5) Inf. alveolar (ia), buccal (b) 6) Deep temporal (dt) 7) Post. Sup. alveolar (psa) 8) Desc. palatine (dp) 9) Infraorbital (io), sphenopalatine (sp)

Variation of Maxillary Artery
As superficial (a) & deep (b) A/C to lat. pterygoid (LP) (referenced
from Putz & Pabst, 2001). ST, sup. temporal artery; EC, ext. carotid
artery.
A/C to part of pterygopalatine (ref. from Morton & Khan, 1991). SP, sphenopalatine artery; DP,
descending palatine artery

PTERYGOID VENOUS PLEXUS• Lies around & within lat. pterygoid muscle.• Tributaries correspond to branches of maxillary artery.• Plexus drained by maxillary vein which begins at post. end of plexus
& unites with sup. temporal vein Form retromandibular vein.• Maxillary vein accompanies only 1ST part of maxillary artery.• It communicates with a) Inf. ophthalmic vein via inf. orbital fissure b) Cavernous sinus via emissary veins & c) Facial vein through deep
facial vein.

Clinical notes of venous drainage• Anastomoses of pterygoid venous plexus with facial
vein & cavernous sinus is important potential pathway for spread of infection.
• Normally, blood from medial angle of eye, nose & lips drains down via facial vein.
• Veins in head, including of pterygoid venous plexus, do not have valves.
• Infections reverse the flow of blood into cavernous sinus, results in meningeal infections.

Mandibular Nerve • Represents the mandibular division (v3) of trigeminal nerve (CN V)
Passes through F. ovale & descends into ITF.• Origin: Gasserian ganglion of CN V.• Located in lat. wall of cavernous sinus MIXED NERVE• Lies superficial to medial pterygoid & deep to lat. pterygoid muscle.

• Branches within infratemporal fossa is divided into 3 groups:Branches from trunk:- 1) Spinous nerve 2) Medial pterygoid nerve Anterior branches:- 1) Buccal nerve 2) Masseteric nerve 3) Deep temporal nerves 4) Lateral pterygoid nervePosterior branches:- 1) Auriculotemporal nerve 2) Lingual nerve 3) Inferior alveolar nerve

• Spinous nerve Pass via spinous foramen & enters cranium Sensory nerve innervating the dura mater.
• Medial pterygoid nerve Innervates med. pterygoid, tensor veli palatini & tensor tympani muscle.
• Buccal , masseteric, deep temporal, lat. pterygoid nerve Innervate muscles with the same name except buccal nerve.
• Buccal nerve is sensory and innervates the inner surface of the cheek.

Auriculotemporal nerve • Supplies sensory fibers to auricle, temporal region & TMJ. • Conveys postsynaptic parasympa. secretomotor fibers from otic
ganglion to parotid gland.• Frey syndrome also c/a Auriculotemporal syndrome, Baillarger
syndrome, Dupuy syndrome, Salivosudoriparous syndrome, Gustatory sweating syndrome.

• Its U/L hyperhidrosis, flushing of malar region & pinna on eating or drinking that stimulates the parotid gland to produce saliva.
• Occurs 2-13 mnths after surgery, open trauma, or infection of parotid gland.
• Caused by improper regeneration of sympathetic & parasympathetic nerves subserving parotid gland & affected anatomic areas.
• Diagnostic test:- Minor Iodine-Starch Test.• T/t:- 1) Symptomatic T/t. 2) Inj. Botulinum A toxin. 3) Med. T/t:- Anticholinergics, Antihydrotics 4) Surg.T/t:- Excision & muscle flap interposition.

• Inf. alveolar nerve Mandibular foramen Mandibular canal, forming inf. dental plexus Sends branches to all mandibular teeth on its side.
• Terminal branch of inf. alveolar nerve is Mental nerve Mental foramen.

Lingual nerve • Sensory to ant. 2/3RD of tongue, floor of the mouth,
& lingual gingivae.

Chorda tympani nerve• A branch of CN VII carrying taste fibers from ant. 2/3rd of tongue.• CT nerve Int. acoustic canal Middle ear Petrotympanic fissure
Joins lingual nerve in ITF. • Carries secretomotor fibers for submandibular & sublingual salivary
glands.

Otic ganglion (Parasympathetic)• Located in ITF inferior to F.ovale.• Presynaptic parasympathetic fibers, derived mainly from via lesser
petrosal nerve synapse in otic ganglion. • Postsynaptic parasympathetic fibers, secretory to parotid gland, pass
from otic ganglion to this gland through the auriculotemporal nerve.

COMMUNICATIONSThe infratemporal fossa communicates with……….. 1) Temporal fossa Via space below zygomatic arch. 1) The orbit Via inferior orbital fissure. 2) The middle cranial fossa Via foramen spinosum, ovale, lacerum 3) The pterygopalatine fossa Via pterygomaxillary fissure

ITF & NERVE BLOCKInf. alveolar N. block:2 intraoral & 1 extraoral approach. Mandibular N. block:1 internal ‘high condyle’ (Gow-Gates)& 1 extraoral approach.
Inferior alveolar nerve block:- 1) Open-mouth direct tecq.2) Closed mouth tecq.3) External tecq.Mandibular nerve block using 1) Int. ‘high condyle’ (Gow-Gates) tecq.

• The post. Sup. alveolar artery runs with nerve(s), but is no more likely to be damaged than arteries in other neurovascular bundles.
• The pterygoid venous plexus should not be damaged unless the needle is inserted too deeply or laterally.
• If a positive (venous) aspiration is observed during this procedure, withdrawal will disengage the needle with minimal bleeding resulting—injecting into the friable plexus causes disruption which can lead to haematoma formation and postoperative trismus.

APPROACHES TO INFRATEMPORAL FOSSA• There are several surgical approaches to the ITF.• They are grouped as……A) Anterior = Transoral, Transantral, Transpalatal,
Transmaxillary, Exteded transmaxillary, Maxillary swing, Transfacial.
B) Inferior = Transmandibular, Transcervical.C) Lateral = Transzygomatic, Lateral infratemporal.D) Other = Fisch types A, B, C, and D, Facial
translocation, Transcranial, Combined

TRANSORAL APPROACH• Sup. gingivolabial sulcus posteriorly is close to
tuberosity of the maxilla & provides access to lower part of the ITF.
• Does not provide enough exposure for removal of tumours,
• View obstructed by fatty tissue & there is no vascular control. • Access for biopsy purposes
if lesion low in ITF.• Benign tumour may be
removed via this.

TRANSANTRAL APPROACH• Antral cavity entered via sublabial incision, from canine to 1st molar.• Mucoperiosteal flap elevated till infraorbital foramen To preserve
infraorbital vessels. • Window on anterolateral wall of antrum For exposure of complete
post. wall of maxillary sinus. • Roots of canine & premolars are preserved. • Antral mucosa of post. wall incised at its junction with med, lat & sup
walls mucoperiosteal flap reflected down

1.infraorbital nerve; 2.posterior wall maxilla3.maxillary artery4.lat. pterygoid plate5.lat pterygoid muscle6.lat. pterygoid muscle 7.nasal cavity; 8.eyeball & optic nerve.
• At the end, bony posterior wall & mucoperiosteal flap are replaced.• It is not suitable for tumour excision by itself, but may be combined
with other approaches. • Used for the purpose of obtaining a biopsy.

TRANSPALATAL APPROACH• Kornfehl et al. described transpharyngeal approach via palate. • Nasopharynx reached via ‘S'-shaped incision vertically on soft
palate & on to ant. pharyngeal arch towards side of lesion. • Mucosa of lat. nasopharynx incised vertically, sup. constrictor
muscle of pharynx split to enter medial part of ITF.

Limitations:-• Not a safe approach for tumour excision. • Internal carotid artery is close to pharyngeal wall &
inot possible to obtain any control on vessel.• Limited exposure of tumor.

TRANSMAXILLARY APPROACH• By Langenbeek in 1859 Osteoplastic technique for tumours of
pterygopalatine fossa.• An incision placed in buccal sulcus above attached gingivae bwt
maxillary second premolars. • Incision placed half cm. above apices of tooth to ensure viability of
teeth. • Mucoperiosteal flap raised. Nasal septum separated from ant. nasal
spine & maxillary crest. Facial soft tissue retracted cranially.

• Osteotomy incision from one maxillary tuberosity to other. • The incision passes just under zygomatic buttress & divides ant
nasal aperture. • Medial maxilla wall osteotomy done via inf. meatus to palatine
canal. At this stage the palate & inf. portion of maxilla remain attached by the pterygomaxillary suture, thin post. wall of maxillary sinus & bone forming canal of palatine vessels.
• Using a curved osteotome, maxilla separated & disimpacted downwards.
• The buttress of bone anterolaterally & at piriform nasal aperture are preserved so that they can be approximated at closure.

EXTENDED MAXILLOTOMY APPROACH• Transantral approach with extended sublabial incision, from
midline to maxillary tuberosity & carried down to periosteum.
• Post. wall of maxillary sinus widely excised Access to pterygomaxillary portion of the tumour.

• The medial wall of the maxillary sinus and the nasopharynx is removed.
• Lateral extension of tumour exposed by removing the lateral wall of antrum.
• Combined with a transpalatal approach.• Krause & Baker 1ST used for surgical treatment of
nasopharyngeal angiofibroma.

TRANSMANDIBULAR APPROACH• 1st done by Conley & Barbosa. ITF communicates inf. with neck.• If mandible lat. retracted & med. pterygoid muscle detached from its
mandibular attachment, ITF reached. • Good control of vessels & nerves & en bloc resection of nasopharynx,
post. maxilla, ITF , mandibular ramus & parotid gland.• Modified by Attia et al To obtain wide exposure without sacrifice of
mandibular function & sensory supply of face & oral cavity.

• Mandibular osteotomies To spare inf. alveolar nerve & vessels & positioned under intercondylar notch, above the opening of mandibular canal & medial to mental foramen.
• Detachment of med. & lat. pterygoid muscles & sphenomandibular ligament allows mandibular segment to reflect sup.
• Provides direct access to ITF Intermaxillary fixation performed.• Preserves function, exposure is good & cosmetically acceptable.

MAXILLARY SWING• Incision – Weber Ferguson incision without gingivolabial component• B/L tarsorraphy should be performed• Inverted “U” shaped incision marked on hard palate• After deepening facial incision, lacrimal sac skeletonized & sectioned
at its lower end.• Infra orbital nerve sectioned as it comes out of infraorbital foramen.• Periosteum of inf. orbital wall elevated.

• Osteotomy on frontal process of maxilla & maxillo zygomatic suture.• Maxillo-ethmoidal junction separated.• Hard palate mucoperiosteum elevated based on C/L greater palatine
vessels & I/L greater palatine vessels cauterized & sectioned. • Straight osteotome placed bwt arms of v shaped notch on ant. nasal
spine & hammered To separate maxilla down middle. • Whole maxilla with its attached cheek tissue swung like a door
laterally exposing whole of nasopharynx.

• Mass in nasopharynx can now be removed under direct vision.
• Maxilla can be repositioned after surgery and secured in position by using miniplate & screws.

Transzygomatic approach1) Preauricular incision & ant. displacement of the flap. 2) Section of the zygomatic arch.3) Masseter & zygomatic arch displaced inferiorly.4) Coronoid process sectioned, displaced upward with temporal muscle.
1. masseter muscle; 2.deep temporal fascia; 3.coronoid process; 4.maxillary artery; 5.Lateral pterygoid muscle (upper head

Fisch(1984) infratemporal fossa approach• Type A= Access to temporal bone right up to petrous apex
Glomus jugulare tumours• Type B= Cross petrous apex to basiocciput & clivus Chordoma, petrous apex cholesteatoma. • Type C= Upto nasopharynx, parasellar , retromaxillary & paratubal regions.• Type D= Upto lat. orbital wall, infratemporal & PPF.

Le Fort I osteotomy approachA) Proposed osteotomy site just above the level of nasal floor.B&C) Incisions & bone cuts along anterolateral maxillary surface.
D) Separation of the nasal septum with an osteotome.
E) Separation of maxilla from the pterygoid plate with curved osteotome F) Down-fracture of maxilla to allow access to maxillary sinuses, nasopharynx, and adjacent skull base.

COMBINATION OF APPROACHES• Radical excision of tumours & relatively limited access
obtained by any single approach have made combined approaches necessary.
• It offers the patients the maximum benefit of the technical ‘know-how’ of the surgical team & the best opportunity for surgical excision.
• They are as follow………………..

• Combined infratemporal & PCF approach• Subtemporal preauricular infratemporal fossa
approach• Mid facial degloving approach.• In 1969, Terez et al Craniofacial approach for
tumors invading pterygoid fossa.• In 1976, House & Hitselberger Transcochlear
approach for tumors medial to the IAC or from the clivus.

References• Grays anatomy, Last anatomy.• Atlas of human body- Netters.• B.D. Chaurasia- Text book of anatomy.• John d Langdon- Surgical anatomy of infratemporal fossa.• Jatin shah- Head and Neck cancer.• Scott Brown 6th edition.• Cumming’s 6th edition.• Original study ‘Microanatomy & Surgical Approaches to
the Infratemporal Fossa: An Anaglyphic Three-Dimensional Stereoscopic Printing Study’- Gustavo Rassier Isolan et al.
• Various journals.