
Ameloblastoma of the Maxilla: CT and MR Appearance · an ameloblastoma that involved the maxilla,...
4
Ameloblastoma of the Maxilla: CT and MR Appearance JaneL. Weissman, 1 ' 2 .4 Carl H. Snyderman , 2 Samuel A. Yousem, 3 and Hugh D. Curtin 1 ' 2 Summary: This paper describes the CT and MR appearance of an ameloblastoma that involved the maxilla, infratemporal fossa, and adjacent structures. Although not pathognomonic, the multicystic appearance of an ameloblastoma may suggest the correct diagnosis. Index terms: Paranasal sinuses, neoplasms; Maxilla, magnetic resonance; Maxilla, computed tomography; Maxilla , neoplasms Ameloblastoma of the jaw is an odontogenic tumor comprising epithelial elements (1). Most ameloblastomas are benign. The plain film ap- pearance of a multilocular "bubble-like" lucency (2) with no calcification in the matrix (3) has been described. However, the appearance of amelo - blastoma on computed tomography (CT) and magnetic resonance (MR) imaging has received relatively little attention (4-6) . Case Report A 70-year-old man presented with 1 year of progressive diplopia and proptosis, plus mild left otalgia. Twelve years earlier he had undergone partial maxillectom y for a left max illary amelob lastoma . Physical examination revealed a firm submucosal mass involving the left half of th e hard palate, the anterior tonsillar pillar, and the retromolar tri- gone. The left nasal cavity was obstructed by a firm submucosal mass, and th e posterior choana was obstructed by a submucosal nasopharyngeal mass. There was mild prominence of the left cheek , and proptosis of th e left eye. A CT scan (GE 9800, Milwaukee , WI) was obtained after i ntravenous administration of iodinat ed nonioni c c ontras t (lsovue (iopamidol), Squibb , Princ ton , NJ) . Co ntiguou s axial and coronal images 3 mm thick were obtained throu gh th e facial bones and skull base. An inhomogeneous ma ss with a multilocular , whorled appearance filled the left maxillar y sinus (Figs. 1 A-1 C) . Areas of low attenuation were sepa- rated by curvilinear areas of int er mediate to high attenua- tion . There was one dense calc if icati on (Fig. 1A) . Th e ma ss eroded through th e posterolateral wall of th e sinu s i nto the mast icator space and pter yg opalatin e fossa (Fig. 1B), through th e medial wall of th e sinus into the nasal cavi ty (Figs. 1B and 1 C) , and through th e roof of the sinus in to the f loor of the orbit and ethmoid sinus (Fig. 1 C). The maxillary tub eros it y (Fig. 1A), posteri or hard palate, the superior alveolar ridge, and th e pter ygo id plat es were eroded (Fig. 1A ). Th e pter ygo id mu scles on the left co uld not be identifi ed (Figs. 1A and 1B). Th e left fossa of Rosenmull er w as defo rmed by the mass, and the mastoid and middl e ea r were opacified (Fig. 1B). Th e mandible was int act. An MR scan (GE Max, 0.5 T) was o bt ained (Figs. 1 D- 1 G) . Axial and coronal T1- weig ht ed images 3 m m th ick w ith a 1-mm int ersection gap were ac qui red before and aft er th e intr avenous admini str ati on of gadopentetate di- meglumin e (Magnevist, Berlex, Cedar K noll s, NJ ). Ax ial T2-weighted images were also ac quir ed. Th ese were 5 mm thi ck, with a 2-mm inter section gap. Th e pr econtrast T 1- weighted images demon str ated a slightl y inhomogenous tumor , largely isointense with muscl e, with a few areas of lower signal intensity (Fig. 1D). Th ere were two foc i of high signal that could have re prese nt ed hemorrhage or high protein (Fig. 1E). (On th e co rr es ponding CT images, no discrete areas of high density co uld be identifi ed in these locations, but all CT images were o bt ained after contrast, which m ay have obscured subtl e areas of high density.) Th e les ion enhanced i ntense ly , but inhomogeneously, with a multilocular patt ern cr ea ted by many small ro unded foci of low to intermediat e si gnal intensit y that did not enhance, separated by enhancing tumor tissue (Fig. 1F). On T2- weighted images, the areas of low signal brightened con- siderably, while the se ptae between them remained of intermediate signal intensit y (Fig. 1 G) . Th ere was a discrete signal void (Figs. 1 D, 1F and 1 G) th at co rr esponded to the calcifica tion seen on CT. Becau se of th e patient's visual sym pt oms and the lack of other effec tiv e th erapy, he underwent a left radical m ax illectomy and a transfacial app roach to the sku ll base. Gro ssl y, all of th e tum or was resected. Th e or bit was preserved. Th e surgical defect was reconstructed wit h temporalis muscle and skin graft. Histologically, th e tumor co ntained plexiform and fo llic- ular patt erns, and m any f oc i of cystic change (Fig. 1H). Th e large calcificat ion seen on the CT and MR was co m- posed of a poorly organ ized ma ss resembling cement um. Dentin and toot h enamel were not seen . Received November 12, 1991 ; revision req uested March 19, 1992; re vision received Ap ril 7 and accepted Jul y 8. Depar tments of 1 Radiology , 2 Otolaryngology , and 3 Pathology, Uni ve rsi ty of Pittsburgh, School of Medic ine, Pittsburgh, PA. 4 Address repr in t requests to Jane L. Weissman, MD, Department of Radiology , D-1 32 PUH, DeSoto at O' Hara Streets, Pittsburgh, PA 1521 3. AJNR 14:223- 226, Jan/ Feb 1993 0195-6108/93/1 401-0223 © America n Society of Neuroradiology 223
Transcript of Ameloblastoma of the Maxilla: CT and MR Appearance · an ameloblastoma that involved the maxilla,...
Ameloblastoma of the Maxilla: CT and MR Appearance
JaneL. Weissman, 1'2
.4 Carl H. Snyderman ,2 Samuel A . Yousem ,3 and Hugh D. Curtin 1'2
Summary: This paper describes the CT and MR appearance of
an ameloblastoma that involved the maxilla, infratemporal fossa, and adjacent structures. Although not pathognomonic, the multicystic appearance of an ameloblastoma may suggest the correct diagnosis.
Index terms: Paranasal sinuses, neoplasms; Maxilla, magnetic resonance; Maxilla, computed tomography; Maxilla , neoplasms
Ameloblastoma of the jaw is an odontogenic tumor comprising epithelial elements (1). Most ameloblastomas are benign. The plain film appearance of a multilocular "bubble-like" lucency (2) with no calcification in the matrix (3) has been described. However, the appearance of ameloblastoma on computed tomography (CT) and magnetic resonance (MR) imaging has received relatively little attention (4-6).
Case Report
A 70-year-old man presented with 1 year of progressive diplopia and proptosis, plus mild left otalgia. Twelve years earlier he had undergone partial maxillectomy for a left max illary ameloblastoma. Physical examination revealed a firm submucosal mass involving the left half of the hard palate, the anterior tonsillar pillar, and the retromolar trigone. The left nasal cavity was obstructed by a firm submucosal mass, and the posterior choana was obstructed by a submucosal nasopharyngeal mass. There was mild prominence of the left cheek , and proptosis of the left eye.
A CT scan (GE 9800, Milwaukee, WI) was obtained after intravenous administration of iodinated nonionic contrast (lsovue (iopamidol), Squibb, Princton , NJ). Contiguous axial and coronal images 3 mm thick were obtained through the facial bones and skull base. An inhomogeneous mass with a multilocular, whorled appearance filled the left m axillary sinus (Figs. 1 A-1 C). Areas of low attenuation were separated by curvilinear areas of intermediate to high attenuation. There was one dense calcification (Fig. 1A). The mass eroded through the posterolateral wall of the sinus into the mast icator space and pterygopalatine fossa (Fig. 1 B), through the medial wall of the sinus into the nasal cavi ty (Figs. 1 B and 1 C) , and through the roof of the sinus into
the floor of the orbit and ethmoid sinus (Fig. 1 C). The maxillary tuberosity (Fig. 1 A), posterior hard palate, the superior alveolar ridge, and the pterygoid plates were eroded (Fig. 1 A ). The pterygoid muscles on the left could not be identified (Figs. 1 A and 1 B). The left fossa of Rosenmuller was deformed by the mass, and the mastoid and middle ear were opacified (Fig. 1 B). The mandible was intact.
An MR scan (GE Max, 0.5 T ) was obtained (Figs. 1 D-1 G). Axial and coronal T1-weighted images 3 m m thick with a 1-mm intersection gap were acquired before and after the intravenous administration of gadopentetate dimeglumine (Magnevist , Berlex, Cedar Knolls, NJ). Ax ial T2-weighted images were also acquired. These were 5 m m thick , with a 2-mm intersection gap. The precontrast T 1-weighted images demonstrated a slightly inhomogenous tumor , largely isointense with muscle, with a few areas of lower signal intensity (Fig. 1 D). There were two foc i of high signal that could have represented hemorrhage or high protein (Fig. 1 E). (On the corresponding CT images, no discrete areas of high density could be identified in these locat ions, but all CT images were obtained after contrast, which may have obscured subtle areas of high density.) The lesion enhanced intensely , but inhomogeneously , with a multilocular pattern created by many small rounded foci of low to intermediate signal intensity that did not enhance, separated by enhancing tumor tissue (Fig. 1 F) . On T2-weighted images, the areas of low signal brightened considerably, while the septae between them remained of intermediate signal intensity (Fig. 1 G) . There was a discrete signal void (Figs. 1 D, 1 F and 1 G) that corresponded to the calcification seen on CT.
Because of the pat ient's visual symptom s and the lack of other effective therapy , he underwent a left radical maxillectom y and a transfacial approach to the skull base. Grossly , all of the tumor was resected. The orbi t was preserved. The surgical defect was reconstructed with temporalis m uscle and sk in graft.
Histologically , the tumor contained plex iform and fo ll icular patterns, and many foci of cystic change (Fig. 1 H). The large ca lcification seen on the CT and MR was composed of a poorl y organized mass resembling cementum . Dentin and tooth enamel were not seen .
Received November 12, 1991 ; rev ision requested March 19, 1992; revision received April 7 and accepted July 8.
Departments of 1 Radiology , 2 Otolaryngology, and 3 Pathology, University of Pittsburgh, School of Medicine, Pittsburgh, PA. 4 Address reprin t requests to Jane L. Weissman, MD, Department of Radiology , D-1 32 PUH, DeSoto at O'Hara Streets , Pittsburgh, PA 152 13.
AJNR 14:223- 226, Jan/ Feb 1993 0195-6108/ 93/1 401-0223 © American Society of Neuroradiology
223

224 WEISSMAN AJNR: 14, January / February 1993
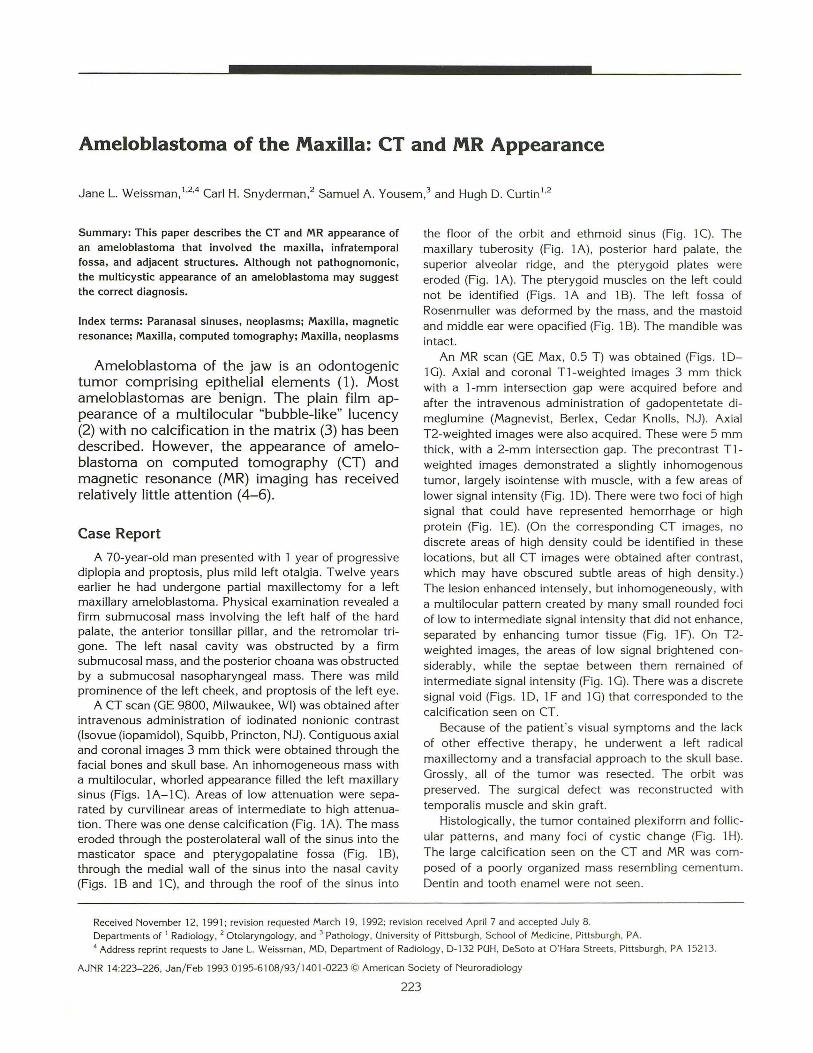
A
Fig. 1. A-C, Contrast-enhanced CT scan. A, Axia l image through the superior alveolus. An inhomogeneous mass with one focus of dense calcification (unlabeled arrow) erodes
the left maxillary tuberosity, superior alveolar ridge (arrowheads) , and hamulus, and extends posteriorly as far as the internal carotid artery (c) and styloid process (s). The mass has many foci of low density interspersed with more dense septations. The pterygoid muscles cannot be identified. Normal right maxillary tuberosity (t), hamulus (h), and medial pterygoid muscle (m).
8 , Axial image through the maxillary sinus. The left maxillary sinus is completely filled by the inhomogeneous mass, which has partially destroyed the sinus walls (small black arrows). The mass extends medially up to the nasal septum (open arrow), and through the pterygopalatine fossa into the maxticator space (m) . The pterygoid processes are destroyed. The left nasopharynx is deformed (small white arrows). There is fluid in the left mastoid air cells (f) .
C, Coronal image through the maxillary sinus and orbit. The mass in the maxillary sinus has extended through the sinus roof (small arrows) into the orbit. The mass abuts the inferior rectus muscle (black arrowhead). Medially , the superior extent of the mass is the ethmoid sinus (wavy arrow), and, below this, the nasal septum (open arrows). Inferiorly , the maxilla is eroded (black arrows).
Discussion
Ameloblastoma is an odontogenic tumor comprising epithelial elements ( 1 ). The tumor may arise from the enamel organ (odontogenic apparatus) (1), follicle, periodontal membrane (2), lining of an odontogenic (dentigerous) cyst (1, 2), or marrow of the jaw (2). The name "adamantinoma" is sometimes used interchangeably with ameloblastoma. However, ameloblastomas never differentiate to form enamel, and may not even contain ameloblasts (7) . Adamantinoma, suggesting the presence of hard material (3), is therefore a misnomer (1).
Ameloblastomas represent 1 % of all jaw tumors (1, 8). Most present in the third and fourth decades of life as a painless swelling. Most series have found an equal sex distribution or slight male predominance ( 1 ). Eighty percent of ameloblastomas arise in the mandible, most in the molar region and ramus. The remaining 20% arise in the maxilla . The maxillary tuberosity is the most common location for ameloblastomas of the upper jaw (1 ). The tumor described in this report appears to have arisen from the maxillary tuberosity.
Ameloblastomas are nonencapsulated and locally invasive. There are two histologic patterns,
and both patterns are usually present in the same lesion, as in the case presented here. The more common follicular pattern consists of islands of epithelial elements in a stroma of mature fibrous connective tissue (1). The plexiform pattern contains cords of epithelial elements in the same mature fibrous stroma. Areas of cystic transformation are often seen.
The histology does not predict the biologic behavior. Recurrence after excision is seen in 33% of reported cases (8). Metastasis, indicative of malignancy, is rare (8), and tends to occur after many resections and recurrences (1). The metastases are histologically benign (3). The presence of metastases, rather than their histology, determines the tumor's classification as malignant.
An ameloblastoma may cause resorption of the roots of an adjacent tooth, which is most often a molar. The maxilla of the patient described here was edentulous.
Most of what little has been written about the CT or MR appearance of ameloblastomas deals with mandibular lesions. Hertzanu et at (4) described the CT appearance of mandibular ameloblastoma as a multiseptated soft-tissue mass. Heffez et at (5) compared CT with MR in assessing

AJNR: 14, January/ February 1993 AMELOBLASTOMA OF THE MAXILLA 225
Fig. 1. -Continued. D-F, Axial MR images. 0 , Unenhanced Tl-weighted 480/ 25/ 4 (TR/ TE excitations) image through the alveolus. The mass (arrows) is isointense with muscle,
with foci of lower signal. One focus of signal void (arrowhead) corresponds to the dense calcification seen on CT (Fig . 1 A). £ , Unenhanced Tl-weighted image through the maxillary sinus. There is a focus of high signal (black arrow) within the tumor which
could represent methemoglobin on this unenhanced scan. A left mastoid effusion is present (white arrow). F, Gadolinium-enhanced T1-weighted (480/ 25/ 4) image through the floor of the maxillary sinus. The tumor (solid black arrows)
enhances intensely but inhomogeneously. Nonenhancing low-signal foci (open arrows) persist throughout the mass. The material in the mastoid (white arrow) does not enhance, indicating that this is fluid and not tumor.
G H
Fig. 1. -Continued. G, Axial MR T2-weighted (2500/ 80/ 1) image through the alveolus. The tumor is hyperintense, though septa tions of lower signal intensity are still seen (open arrows). The signal void of the calcification (solid black arrow) seen on the CT and T1 -weighted images is again apparent. The mastoid effusion is hyperintense (white arrow).
H, Pathology specimen. Both follicu lar and plexiform growth patterns are present, with foci of cystic transformation (solid arrow). At the center of the epithelial islands, there is a loose network of cells resembling stellate reticulum and showing squamous metaplasia (open arrow). Hematoxilyneosin X 40 at left; hematoxilyneosin X350 at right.
conspicuity, artifact degradation , and edge definition in three cases of ameloblastoma, one of which had inhomogeneous signal representing solid and cystic areas, confirmed histologically. Schultz et al (6) described a multiseptated, expansile ameloblastoma of the mandibular ramus in a patient with basal cell nevus (Gorlin) syndrome.
Although the appearance of this tumor on CT or MR is not pathognomonic, there are features that may suggest the diagnosis , or help exclude other more common sinus tumors . The importance in differentiating ameloblastoma from the more common malignant neoplasms of the sinonasal region lies in the different prognosis each

226 WEISSMAN
tumor carries, and therefore the different therapeutic implications. Squamous cell carcinomas of the paranasal sinuses are generally homogeneous, without the many cystic foci seen here. The degree of contrast enhancement of this ameloblastoma, as well as the marked hyperintensity on T2-weighted sequences, would be unusual for a squamous cell tumor (3). Minor salivary gland malignancies such as adenoid cystic carcinoma and the more rare colonic-type adenocarcinoma may be inhomogeneous. Adenoid cystic carcinoma may demonstrate perineural spread, which was not seen here. Most colonic-type adenocarcinomas arise in the ethmoids (3). The calcification in this tumor would also be unusual for squamous cell and adenoid cystic carcinomas.
In summary, ameloblastoma is an invasive tumor of the jaws that most frequently arises from the mandible. The less common maxillary ameloblastoma, as in the case presented here, usually originates around the maxillary tuberosity. This location, and the extensive local invasion, may suggest a more common malignancy, such as squamous cell or adenoid cystic carcinoma of the paranasal sinuses or oral mucosa.
With the development of sophisticated techniques facilitating resection of skull base tumors, even invasive maxillary ameloblastomas may be amenable to surgery. As with other tumors of the
AJNR : 14, January /February 1993
skull base, CT and MR contribute to preoperative planning by delineating the anatomic extent of the tumor. The CT and MR appearance of a multicystic, enhancing mass with aggressive local invasion but no evidence of perineural spread is unusual for the more common malignancies of the sinonasal cavity and skull base. Therefore, this appearance could raise the diagnostic possibility of an ameloblastoma.
References
I. Appel BN, Verbin RS. Odontogenic tumors. In: Barnes EL, ed. Surgical
pathology of the head and neck. New York: Marcel Dekker, 1985: 1331-1409
2. Stafne EC, Gibilisco JA. Oral roentgenographic diagnosis. Philadel
phia: Saunders, 1975:169-187
3. Som PM. The sinonasal cavity. In: Som PM, Bergeron RT, eds. Head
and neck imaging. 2nd ed. St. Louis: Mosby, 1991:51-276
4. Hertzanu Y, Mendelsohn DB, Cohen M . Computed tomography of
mandibular ameloblastoma. J Comput Assist Tomogr1984 ;8:
220-223
5. Heffez L, Mafee MF, Vaiana J. The role of magnetic resonance
imaging in the diagnosis and management of ameloblastoma. Oral
Surg Oral Med Oral Patho/ 1988;65:2-12
6. Schultz SM, Twicker DM, Wheeler DE, Hogan TD. Ameloblastoma
associated with basal cell nevus (Gorlin) syndrome: CT findings . J Comput Assist Tomogr 1987;11:901-904
7. Tsaknis PJ , Nelson JF. The maxillary ameloblastoma: an analysis of
24 cases. J Oral Surg 1980;38:336-342
8. Wood NK, Goaz PW, Goldman S. Solitary cystlike radiolucencies not
necessarily contacting teeth. In: Wood NK, Goaz PW, eds. Differential
diagnosis of ora/lesions. St. Louis: Mosby , 1985:379-415


















