ENDONASAL TRANSPTERYGOID APPROACH TO THE INFRATEMPORAL ... · PDF fileoriginal article...
8
ORIGINAL ARTICLE ENDONASAL TRANSPTERYGOID APPROACH TO THE INFRATEMPORAL FOSSA: CORRELATION OF ENDOSCOPIC AND MULTIPLANAR CT ANATOMY Seid Mousa Sadr Hosseini, MD, 1 Ali Razfar, MD, 2 Ricardo L. Carrau, MD, 3 Daniel M. Prevedello, MD, 4 Juan Fernandez–Miranda, MD, 5 Adam Zanation, MD, 6 Amin B. Kassam, MD 3 1 Department of Otolaryngology–Head & Neck Surgery, Vali-E-Asr Hospital, Tehran University of Medical Sciences, Tehran, Iran 2 Department of Surgery–Division of Head and Neck Surgery, University of California Los Angeles Medical Center, Los Angeles, California 3 Neuroscience Institute, John Wayne Cancer Institute at Saint John’s Health Center, Santa Monica, California. E-mail: [email protected] 4 Department of Neurosurgery, Ohio State University Medical Center, Columbus, Ohio 5 Department of Neurological Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania 6 Department of Otolaryngology–Head & Neck Surgery, University of North Carolina. Chapel Hill, North Carolina Accepted 14 December 2010 Published online 16 May 2011 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/hed.21725 Abstract: Background. The infratemporal fossa anatomy, from an endoscopic standpoint, is poorly understood. Our pur- pose was to design an anatomic model that illustrates the anatomy of the infratemporal fossa from the endoscopic stand- point and serves as a training model for surgeons interested in pursuing this endeavor. Methods. Red and blue silicone dyes were respectively injected into the great vessels of the neck. Digital data acquired from a high resolution CT scan was imported to a navigational system. An endoscopic endonasal dissection of the infratemporal fossa was completed under conditions that mimicked our operating suite. Results. A detailed anatomic dissection of the infratempo- ral fossa was correlated to the image guidance (navigation) system. This provided a surgical map highlighting critical neu- rovascular structures and illustrating the potential surgical corridors. Conclusion. A thorough understanding of the anatomy of infratemporal fossa from the endoscopic perspective allows the surgeon to plan an adequate corridor. V V C 2011 Wiley Peri- odicals, Inc. Head Neck 34: 313–320, 2012 Keywords: endoscopy; training model; anatomy; infratemporal fossa; pterygopalatine fossa Surgical access to the infratemporal fossa is difficult, as this area is deeply seated. Briefly, the infratempo- ral fossa is situated beneath the floor of the middle cranial fossa, posterior to the maxillary sinus, medial to the ramus of the mandible, and lateral to the naso- pharynx. The greater wing of the sphenoid bone and the subtemporal surface of the temporal bone form the roof of the infratemporal fossa. The lateral ptery- goid plate along with the eustachian tube forms its medial wall. The deep aspect of temporalis muscle inserting to the mandibular ramus and the temporo- mandibular joint bounds the infratemporal fossa in its lateral aspect (Figure 1). The infratemporal fossa houses the lateral and medial pterygoid muscles, and important neurovascu- lar structures, such as the third branch of the trigem- inal nerve (V3), the internal maxillary artery, and the carotid sheath and its contents. The lateral pterygoid muscle (LPM) occupies most of the superior infratem- poral fossa. Caudally, the infratemporal fossa is pri- marily occupied by the medial pterygoid muscle, which inserts into the angle of mandible. Posterome- dially, the infratemporal fossa contains the carotid sheath (internal carotid artery [ICA], internal jugular vein, and cranial nerves IX to XII) and styloid com- plex (ie, parapharyngeal space). 1 In addition, the in- ternal maxillary artery (IMA), pterygoid venous plexus, maxillary vein, and the mandibular and chorda tympani nerves all traverse through the infra- temporal fossa (ie, masticator space). 2,3 Medially, the infratemporal fossa communicates with the pterygo- palatine fossa via the pterygomaxillary fissure, which is continuous with the inferior orbital fissure. A variety of benign and malignant neoplasms involve the infratemporal fossa. However, most neo- plasms involving the infratemporal fossa originate from adjacent structures, such as the temporal bone, parotid gland, paranasal sinuses, nasopharynx, or temporal fossa. Juvenile angiofibroma and adenoid cystic carcinoma are the most common benign and malignant tumors involving the infratemporal fossa, Correspondence to: R. L. Carrau V V C 2011 Wiley Periodicals, Inc. Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012 313
Transcript of ENDONASAL TRANSPTERYGOID APPROACH TO THE INFRATEMPORAL ... · PDF fileoriginal article...

ORIGINAL ARTICLE
ENDONASAL TRANSPTERYGOID APPROACH TO THEINFRATEMPORAL FOSSA: CORRELATION OF ENDOSCOPICAND MULTIPLANAR CT ANATOMY
Seid Mousa Sadr Hosseini, MD,1 Ali Razfar, MD,2 Ricardo L. Carrau, MD,3 Daniel M. Prevedello, MD,4
Juan Fernandez–Miranda, MD,5 Adam Zanation, MD,6 Amin B. Kassam, MD3
1Department of Otolaryngology–Head & Neck Surgery, Vali-E-Asr Hospital, Tehran University of Medical Sciences,Tehran, Iran
2Department of Surgery–Division of Head and Neck Surgery, University of California Los Angeles Medical Center,Los Angeles, California
3Neuroscience Institute, John Wayne Cancer Institute at Saint John’s Health Center, Santa Monica, California.E-mail: [email protected]
4Department of Neurosurgery, Ohio State University Medical Center, Columbus, Ohio5Department of Neurological Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania6Department of Otolaryngology–Head & Neck Surgery, University of North Carolina. Chapel Hill, North Carolina
Accepted 14 December 2010Published online 16 May 2011 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/hed.21725
Abstract: Background. The infratemporal fossa anatomy,
from an endoscopic standpoint, is poorly understood. Our pur-
pose was to design an anatomic model that illustrates the
anatomy of the infratemporal fossa from the endoscopic stand-
point and serves as a training model for surgeons interested in
pursuing this endeavor.
Methods. Red and blue silicone dyes were respectively
injected into the great vessels of the neck. Digital data
acquired from a high resolution CT scan was imported to a
navigational system. An endoscopic endonasal dissection of
the infratemporal fossa was completed under conditions that
mimicked our operating suite.
Results. A detailed anatomic dissection of the infratempo-
ral fossa was correlated to the image guidance (navigation)
system. This provided a surgical map highlighting critical neu-
rovascular structures and illustrating the potential surgical
corridors.
Conclusion. A thorough understanding of the anatomy of
infratemporal fossa from the endoscopic perspective allows
the surgeon to plan an adequate corridor. VVC 2011 Wiley Peri-
odicals, Inc. Head Neck 34: 313–320, 2012
Keywords: endoscopy; training model; anatomy; infratemporal
fossa; pterygopalatine fossa
Surgical access to the infratemporal fossa is difficult,as this area is deeply seated. Briefly, the infratempo-ral fossa is situated beneath the floor of the middlecranial fossa, posterior to the maxillary sinus, medialto the ramus of the mandible, and lateral to the naso-pharynx. The greater wing of the sphenoid bone andthe subtemporal surface of the temporal bone form
the roof of the infratemporal fossa. The lateral ptery-goid plate along with the eustachian tube forms itsmedial wall. The deep aspect of temporalis muscleinserting to the mandibular ramus and the temporo-mandibular joint bounds the infratemporal fossa inits lateral aspect (Figure 1).
The infratemporal fossa houses the lateral and
medial pterygoid muscles, and important neurovascu-
lar structures, such as the third branch of the trigem-
inal nerve (V3), the internal maxillary artery, and the
carotid sheath and its contents. The lateral pterygoid
muscle (LPM) occupies most of the superior infratem-
poral fossa. Caudally, the infratemporal fossa is pri-
marily occupied by the medial pterygoid muscle,
which inserts into the angle of mandible. Posterome-
dially, the infratemporal fossa contains the carotid
sheath (internal carotid artery [ICA], internal jugular
vein, and cranial nerves IX to XII) and styloid com-
plex (ie, parapharyngeal space).1 In addition, the in-
ternal maxillary artery (IMA), pterygoid venous
plexus, maxillary vein, and the mandibular and
chorda tympani nerves all traverse through the infra-
temporal fossa (ie, masticator space).2,3 Medially, the
infratemporal fossa communicates with the pterygo-
palatine fossa via the pterygomaxillary fissure, which
is continuous with the inferior orbital fissure.A variety of benign and malignant neoplasms
involve the infratemporal fossa. However, most neo-plasms involving the infratemporal fossa originatefrom adjacent structures, such as the temporal bone,parotid gland, paranasal sinuses, nasopharynx, ortemporal fossa. Juvenile angiofibroma and adenoidcystic carcinoma are the most common benign andmalignant tumors involving the infratemporal fossa,
Correspondence to: R. L. Carrau
VVC 2011 Wiley Periodicals, Inc.
Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012 313

respectively. Other various tumors may arise withinthe infratemporal fossa including sarcomas, lympho-mas, schwannomas, and meningiomas.4
Multiple surgical approaches to the infratemporalfossa have been proposed including lateral preauricu-lar and postauricular approaches, anterior trans-max-illary or trans-nasal approaches, and inferior trans-mandibular approaches.3 Among others, traditionalanterior approaches to the infratemporal fossainclude the extended maxillary sinusotomy, Le Fort Iand/or II osteotomies, maxillary swing, and facialtranslocation.4 Recently, endoscopic endonasal trans-pterygoid approaches have provided new corridors toaccess a variety of pathologies in the paramedian andlateral skull base.
Endoscopic endonasal transpterygoid approacheswere first described to access the lateral recess of thesphenoid sinus5–7 and was subsequently modified andexpanded to manage lesions of the petrous apex, mid-dle cranial fossa, and infratemporal fossa.8 Under-standing the complex anatomic relationships of theinfratemporal fossa from the endoscopic perspective ismandatory before attempting an endoscopic endo-nasal transpterygoid approache.9–12 Familiarity withmicrosurgical anatomy of infratemporal fossa and dis-section techniques via anterior and lateral approachesis helpful but may not be sufficient to dominate thisarea.2,3,13–16
The purpose of this study was to provide adetailed endoscopic anatomic description of the infra-temporal fossa correlated to CT multiplanar imaging.We describe the endoscopic transpterygoid approachand discuss the benefits and limitations of thiscorridor.
MATERIALS AND METHODS
We performed our Committee for Oversight ofResearch Involving the Dead-approved anatomic stud-ies at the Minimally Invasive Neurosurgery Centeranatomy laboratory at the University of PittsburghMedical Center. Major vessels of the neck, includingthe common carotid and vertebral arteries and the in-ternal jugular veins were identified and respectivelyinjected with red and blue silicone dyes. A high reso-lution CT scan was performed and the data wasimported to a Stryker navigational system (Kalama-zoo, MI). Five cranial screws, spaced around thehead, served as fixed landmarks for the registration.
We used a 0� endoscope coupled to a high defini-tion camera and monitor (Karl Storz Endoscopy, Tut-tlingen, Germany) to provide visualization duringmost of the dissections; thus, emulating the environ-ment of our operating room. An AIDA system (KarlStorz Endoscopy, Tuttlingen, Germany) was used torecord and save images (JPG format) and videos ofthe dissections (MPEG-2 format). Still photographswere obtained to define and document the anatomicrelationships of the endoscopic anatomy and to be cor-related with the multiplanar CT views provided bythe image guidance system. A high-speed electric drilland endoscopic dissecting instruments (Karl StorzEndoscopy, Tuttlingen, Germany) were used asneeded. We used a ‘‘Total Performance System’’ drill(Stryker Co., Kalamazoo, MI) with an angled hand-pi-ece and 3 to 4 mm rough diamond (hybrid) short andlong burrs.
RESULTS
We began our approach with the preparation andexpansion of the sinonasal corridor followed by theharvesting of the Hadad–Bassagastaguy nasoseptalflap.17 We removed the inferior half of the middle tur-binate and then completed anterior and posterior eth-moidectomies, ipsilateral to the infratemporal fossadissection. A large middle meatus nasoantral window,extending from the nasolacrimal duct anteriorly tothe sphenopalatine foramen posteriorly and from thelamina papyracea superiorly to the inferior turbinateinferiorly, allows the exposure of the posterior wall ofthe antrum (superior half), and the sphenopalatineforamen with its sphenopalatine and posterior nasalarteries. This window allows the exposure of the ce-phalic half of the pterygopalatine fossa and superome-dial infratemporal fossa. An endoscopic medialmaxillectomy, however, is most commonly needed toexpose the entire height of the posterior wall of max-illary sinus; therefore, allowing an extended dissec-tion of the pterygopalatine fossa and infratemporalfossa exposing and controlling their caudal area. Re-moval of the posterior wall of the antrum is com-pleted with 1 to 2 mm Kerrison Rongeurs,osteotomes, curved ethmoid forceps and curettes, orhigh-speed drill (Figure 2A and 2B).
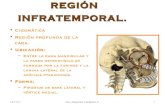
FIGURE 1. Basal skull view. The boundaries of the infratempo-
ral fossa are delineated by the dotted line. Note that the lateral
pterygoid plate and eustachian tube constitute the medial wall
of infratemporal fossa and temporomandibular joint (TMJ) and
temporalis muscle form its lateral wall. The carotid and jugular
foramens are located in posterior part of infratemporal fossa.
314 Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012

The lateral exposure provided by a medial maxil-lectomy, however, is limited by the surgeon’s inabilityto displace the nasolacrimal duct with the rod lensendoscope or dissection instruments. Bringing theinstruments from the contralateral side of the nose,which in turn requires a posterior septectomy, mayenhance this angle of approach. To dissect the mostlateral aspect of the infratemporal fossa, however, itis best to extend the medial maxillectomy anteriorly;thus, achieving the necessary line of sight. This modi-fication includes the removal of the remaining inferiorturbinate and anterior aspect of the inferior meatuswith backbiting rongeurs, osteotomes, or high-speed
drill. In select cases, the removal may be confined tothe area inferior to the nasolacrimal opening. For afull exposure, however, we remove the piriform aper-ture and ascending process of the maxilla, dissectingthe lacrimal duct and transecting it sharply (endo-scopic Denker’s approach). Exposure of the piriformaperture requires a vertical incision just anterior tothe head of the inferior turbinate, right over the edgeof the aperture. This edge can be palpated with ablunt dissector to optimize the placement of the inci-sion, which is then carried through the periosteumdown to the bone. Extension of the dissection later-ally, after a subperiosteal plane, exposes the entireanterior maxilla including the infraorbital foramen,its corresponding nerve, and the inferior orbital rim.The medial maxillectomy is then extended anteriorlyto remove the piriform aperture and laterally toremove the anterior maxillary wall until the entirelateral wall of the antrum is in direct and full view.This modification allows the placement of the endo-scope and dissecting instruments in such a way thatthe line of sight extends to encompass the most lat-eral aspect of the infratemporal fossa.
In the contralateral side, a Hadad–Bassagastaguynasoseptal flap is harvested and transposed into theipsilateral antrum. This requires a large maxillaryantrostomy similar to that described as part of theinfratemporal fossa dissection. It is critical to harvestthe Hadad–Bassagastaguy nasoseptal flap from thecontralateral side, as its pedicle and proximal bloodsupply would be sacrificed ipsilateral to the infratem-poral fossa dissection.
A generous posterior septectomy allows a bima-nual technique traversing both sides of the nasal
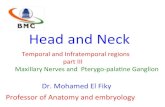
FIGURE 2. (A) Photograph of an endoscopic endonasal ptery-
gopalatine fossa dissection with exposure of the medial infra-
temporal fossa (ITF). Multiplanar images on the left represent
point A which corresponds to the infratemporal crest (origin of
deep temporalis muscle). Multiplanar images on the right repre-
sent point B that corresponds to the inferior edge of the fora-
men rotundum. Note that infraorbital nerve separates the
infraorbital fissure (IOF) from the infratemporal fossa and that
the temporalis muscle defines the lateral border of infratemporal
fossa. ION, infraorbital nerve; TM, temporalis muscle; DPA, de-
scending palatine artery; SPA, sphenopalatine artery; PNA,
posterior nasal artery; IT, inferior turbinate. (B) Photograph
obtained after an endoscopic endonasal medial maxillectomy.
Multiplanar images on the left represent point A which is at the
medial and caudal aspect of the temporalis muscle. Multiplanar
images in the right represent point B which indicates the fusion
between the pterygoid plates and the posterior wall of maxillary
sinus. ION, infraorbital nerve; TM, temporalis muscle; LPM, lat-
eral pterygoid muscle; IMA, internal maxillary artery; VN, vidian
nerve. (C) Photograph obtained during an endoscopic endo-
nasal dissection demonstrating a pterygopalatine fossa and
medial infratemporal fossa dissection. 1 ¼ infraorbital nerve, 2
¼ pterygopalatine ganglion, 3 ¼ vidian nerve, 4 ¼ sphenopala-
tine artery, 5 ¼ greater palatine nerve, 6 ¼ infraorbital artery.
Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012 315

cavity. In general, the posterior septectomy needs tobe extended to a level that is anterior to the posteriorwall of the antrum. This extensive posterior septec-tomy allows the visualization of the entire posteriorwall of the maxillary sinus using a 0� endoscope thatcrosses over from the contralateral side of the nose.As the removal of the posterior and lateral walls ofthe antrum expose the pterygopalatine and infratem-poral fossae, the dissection could be performedthrough the contralateral side without the need touse angled endoscopes.
A wide sphenoidotomy is completed after identify-ing key anatomic landmarks. In a coronal plane, onemay visualize the letter H with its vertical limbs com-posed by the lateral walls of the sphenoid sinus andthe medial pterygoid plates (lateral wall of the poste-rior choana) and the floor of the sinus forming its hor-izontal limb. Trifurcation of the medial pterygoidplate with the lateral wall and floor of the sphenoidsinus forms a wedge-shaped area (‘‘pterygoid wedge’’)that contains the vidian canal. It also contains thepalatovaginal canal with the pharyngeal arterythat can be identified as they travel toward the naso-pharynx. Just lateral to the palatovaginal canal, liesthe vidian (pterygoid) canal with the vidian arteryand nerve. Before removing the inferolateral aspect ofthe rostrum of the sphenoid, its mucoperiosteum isdissected laterally and the area is carefully inspectedfor these landmarks. Subsequently, the bony trifurca-tion of vomer, sphenoid sinus floor, and inter-sinusseptum is removed and the sphenoidotomy isextended in all directions. Ultimately, the sphenoidot-omy should yield a sphenoid sinus roof that is inplane with the roof of the nose and lateral walls thatare in plane with the laminae papyracea bilaterally.Intersinus and intrasinus septations frequentlyinserted in the ICA and optic nerve canals; thus, theirremoval should be completed using cutting instru-ments and/or the high-speed drill.18 Stripping of thesphenoid sinus mucosa facilitates the identification ofcritical landmarks including the sella turcica, theICA, and the optic nerve canals. In the live patient,however, this step should be weighed against the pro-longed healing and possible crusting formation associ-ated with denuded bone.
Pterygopalatine Fossa Dissection. After dissectingand removing the fat of the pterygopalatine fossa, themain terminal branches of the IMA were identifiedincluding the infraorbital, descending palatine,vidian, sphenopalatine, and posterior nasal arteries(Figure 2C). All branches, except the infraorbital ar-tery, were transected to expose the underlying neuralstructures including the infraorbital, descending pala-tine, vidian, and pharyngeal nerves. The pterygomax-illary fissure, which represents the boundary betweenthe pterygopalatine fossa and the infratemporal fossa,is continuous with the infraorbital fissure (IOF). A
short course of the infraorbital nerve (ION) traversesthe infraorbital fissure, just after arising from themaxillary nerve near the foramen rotundum, andbefore entering the infraorbital canal. This portion ofthe ION accurately delineates the border betweeninfratemporal fossa and IOF, after the ION mediallyand posteriorly leads to the foramen rotundum.
Transpterygoid Dissection. For the transpterygoidinfratemporal fossa dissection, we exposed the base ofthe pterygoid plates and transected the vidian nerve.Using a high-speed drill, the maxillary nerve (V2)was followed into Meckel’s cave, identifying the man-dibular nerve (V3) and the dura of middle fossa. Thesulcus tubae, which houses the cartilaginous part ofthe eustachian tube, is situated posterior and medialto the foramen ovale.
Infratemporal Fossa Dissection. The lateral ptery-goid plate is the anterior and medial boundary of theinfratemporal fossa, whereas, the temporalis muscleconstitutes its lateral boundary. The junction of theinfraorbital canal and the posterior maxillarysinus wall is just medial to the vertical fibers of thetemporalis muscle. This point can be used as aproxy landmark to divide the infratemporal fossaand the pterygopalatine fossa from the endoscopicperspective.
We can define 5 planes of dissection in the infra-temporal fossa, as we move from an anterior (superfi-cial) and medial to posterior (deep) and lateral planes(Figure 3). The first plane of dissection is between theLPM medially and the deep part of the temporalismuscle and mandibular ramus laterally. The IMA,which enters the infratemporal fossa posteriorly and
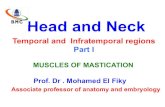
FIGURE 3. Planes of dissection of the infratemporal fossa. First
plane is between lateral pterygoid muscle (LPM) and temporalis
muscle. Second plane includes the LPM. Third plane lies
medial to V3 and its branches. Fourth plane is between medial
pterygoid muscle (MPM) and tensor veli palatini muscles. Fifth
plane contains the internal carotid artery (post-styloid paraphar-
yngeal space).
316 Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012

inferiorly, passing between the neck of mandible andsphenomandibular ligament, is the dominant struc-ture in this plane. It travels anteriorly and superiorlytoward the pterygopalatine fossa. The deep temporalartery, vein, and nerve are in the deepest aspect ofthis plane (deep surface of the temporalis muscle).The maxillary vein runs with the IMA and has multi-ple branches that pass through the LPM. There is anextensive network of venous channels lateral to theLPM, forming the superficial pterygoid venous plexus.A large venous plexus in the deep aspect of the infra-temporal fossa, near the mandibular condyle, repre-sents the confluence of the superficial and deepvenous plexuses. One or 2 branches of the anterior di-vision of mandibular nerve pass between 2 heads ofthe lateral pterygoid muscle and cross the infratem-poral fossa. A consistent branch is the buccal nervethat passes inferiorly to supply sensation to thecheek.
The second plane of dissection (Figure 3) encom-passes the LPM. The LPM comprises 2 heads thatoccupy most of the infratemporal fossa. The superiorhead attaches to the infratemporal surface of thegreater wing of the sphenoid bone and the lower headoriginates from the lateral pterygoid plate. Afterdetaching the lower head from the lateral pterygoidplate and displacing it laterally, the deep pterygoidvenous plexus comes into view (Figure 4). The epicen-ter of this plexus encompasses the area of the fora-men ovale and foramen spinosum. Sensory branchesof the posterior division of the mandibular nerve, exit-ing the foramen ovale, and the middle meningeal ar-tery, entering the foramen spinosum, appear withinthe deep part of the pterygoid venous plexus just pos-
terior to the lateral pterygoid plates. Removal of theLPM provides access to the lateral, medial, and poste-rior walls of the infratemporal fossa and opens a cor-ridor to adjacent structures (Figure 5A and 5B).
The third plane of dissection (Figure 3) is poste-rior to the lateral pterygoid plate, medial to the mid-dle meningeal artery and V3, and extends laterally tothe temporomandibular joint (TMJ). The medial pter-ygoid muscle (MPM), originating from the medial
FIGURE 4. Photograph obtained during an endoscopic endo-
nasal dissection of the medial infratemporal fossa. A dissection
plane medial to the lateral pterygoid muscle (LPM) has been
elevated to illustrate the pterygoid venous plexus. LPMU, upper
head of LPM; LPML, lower head of LPM; TM, temporalis mus-
cle; IMA, internal maxillary artery; DTN, deep temporal nerve;
BN, buccal nerve; PVP, deep part of pterygoid venous plexus;
LPP, lateral pterygoid plate; FO, foramen ovale.
FIGURE 5. (A) Photograph obtained during an endoscopic
endonasal dissection illustrating the infratemporal fossa after re-
moval of lateral pterygoid muscle (LPM). Note the position of
mandibular condyle in the posterior and lateral aspect of the
infratemporal fossa. Multiplanar images on the left represent
point A which indicates the lateral border of infratemporal fossa
(infratemporal crest). Multiplanar images in the right represent
point B which indicates the most medial point of mandibular
condyle. DTN, deep temporal nerve; MN, masseteric nerve;
BN, buccal nerve; ATN, auriculotemporal nerve; MMA, middle
meningeal artery; IAN, inferior alveolar nerve; LN, lingual nerve;
DTA, deep temporal artery; MC, transected insertion of lateral
pterygoid muscle (to the mandibular condyle); IMA, divided end
of internal maxillary artery. (B) Photograph obtained during an
endoscopic endonasal dissection illustrating a transpterygoid
dissection. Multiplanar images in the left represent point (A)
which indicates foramen ovale. Multiplanar images in the right
represent point B which indicates the dura of the middle fossa.
FR, foramen rotundum; TG, trigeminal ganglion; ICA, internal
carotid artery; FO, foramen ovale; V3, mandibular nerve; VN,
vidian nerve; ET, eustachian tube.
Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012 317

aspect of the medial pterygoid plate in the pterygoidfossa, occupies the inferior part of this plane. The eu-stachian tube and its associated muscles occupy thesuperior aspect. A significant amount of fat separatesthe eustachian tube and its accompanying musclesfrom neurovascular structures superiorly and MPMinferiorly. Posteriorly we identify the deep lobe of theparotid, styloid process, and stylopharyngeus muscle(Figure 6).
A fourth plane of dissection (Figure 3) existsbetween the medial pterygoid and the tensor veli pal-atine muscles. A venous plexus lies between these 2muscles and extends posterior to the tensor veli pala-tini muscle. The origin of the medial pterygoid musclemay be transected and its upper half resected to ex-pose the styloid diaphragm. The styloid diaphragm isa thick fascia that covers the styloid complex andICA. It separates the post-styloid compartment (ca-rotid sheath) from the pre-styloid compartment (deeplobe of parotid) and attaches to the skull base.
The ICA lies immediately medial to the styloidcomplex in the fifth and last plane of dissection (Fig-ure 3). The MPM covers a major portion of the para-pharyngeal ICA in the inferior infratemporal fossa;thus, its identification needs removal of the MPM.The styloid diaphragm must also be dissected to ex-pose the parapharyngeal ICA. Exposure of the verti-cal bony carotid canal requires resection of thecartilaginous and eustachian tube (Figure 7).
DISCUSSION
Various lateral and anterior approaches have beendescribed to access the infratemporal fossa.3,19–21 Lat-eral approaches include a combination of preauricularor postauricular incisions, parotidectomy with facialnerve dissection and preservation, displacement or
resection of the mandibular condyle, orbito-zygomaticosteotomies, displacement of the temporalis musclewith or without coronoid transection, identificationand/or transposition of the petrous ICA, and a tempo-ral or pterional craniotomy. In addition to exposingthe infratemporal fossa, these approaches can beextended to expose the sphenoid sinus, nasopharynx,sella, clivus, jugular fossa, cranial nerves, cervicalICA, and petrous apex. Possible sequelae or risksinclude postoperative TMJ pain, dysfunction and tris-mus, facial paralysis, and hearing loss.22 Anteriorapproaches to the infratemporal fossa use the airspace of the maxillary sinus as part of the corridor.Anterior approaches can be divided into traditionaltransmaxillary and endoscopic transmaxillaryapproaches. A variety of modifications of the tradi-tional transmaxillary approaches have been proposedincluding the use of facial, sublabial and palatal inci-sions, Le Fort I and II osteotomies, maxillary sinusot-omy, and partial or total maxillectomy.2,15,23 Theextent of exposure obtained with the anteriorapproaches is comparable to that obtained with lat-eral approaches. However, the anterior approachesprovide a more direct access to the median cranialbase than the lateral approaches. Their morbidityincludes facial deformity, infraorbital nerve injury,epiphora, dental injury, frontalis nerve deficit, ptery-goid plexus venous bleeding, medial canthus mis-alignment, dental malocclusion, eustachian tubedysfunction, masticatory problems, and trismus.
An endoscopic sublabial transmaxillary approachhas been previously described.24,25 It was originallyintroduced to approach the pterygopalatine fossa, lat-eral sphenoid sinus, and retrobulbar lesions with orwithout endonasal access. In this approach, entry to
FIGURE 6. Photograph obtained during an endoscopic endo-
nasal dissection illustrating the third plane of dissection. Multipla-
nar images in the left represent point A that indicates the base
of the styloid process. Multiplanar images in the right represent
point B that indicates the tip of the styloid process. Styloid dia-
phragm (SD) has opened to show the stylopharyngeus (SPM)
muscle. Note the relationship of internal carotid artery to the sty-
loid process. PG, parotid gland; MPM, medial pterygoid muscle.
FIGURE 7. Photograph obtained during an endoscopic endo-
nasal dissection illustrating the fifth plane of the infratemporal
fossa dissection. Multiplanar images on the left represent point
A that indicate the edge of carotid canal. Multiplanar images on
the right represent point B that indicates sulcus tubae and eu-
stachian tube. ION, infraorbital nerve; ICA, internal carotid ar-
tery; VN, vidian nerve; TVP, tensor veli palatini muscle; MPM,
divided part of medial pterygoid muscle; TM, temporalis muscle;
SPM, stylopharyngeus muscle; GPN, glossopharyngeal nerve.
318 Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012

the infratemporal fossa follows a corridor thatinvolves anterior and posterior maxillary sinusoto-mies. It requires that the origin of the LPM be dis-sected and displaced laterally so that a subtemporalcraniotomy can be opened. One drawback is the lim-ited extent of the craniotomy, which in turn may limitthe management of some pathologies arising in thiscomplex area. Its clinical applications remainundefined.
Clinical applications of endoscopic endonasalapproaches for the management of lesions of the ante-rior skull base including cribiform, planum sphenoi-dale, tuberculum sellae, sella, middle and lowerclivus, craniovertebral junction, and C1 have beenpreviously documented.26–29 A transpterygoid dissec-tion expands the lateral exposure; thus, gainingaccess to Meckel’s cave, infratemporal fossa, middlecranial fossa, and petrous apex.30–33
Compared to lateral approaches to the infratempo-ral fossa, the endonasal endoscopic transpterygoidapproach provides better visualization and moredirect exposure of midline structures such as the par-anasal sinuses, nasopharynx, eustachian tube, sella,and clivus. Bleeding from the pterygoid venous plexusis expected, therefore, hemostatic agents (eg, throm-bin/gelatin, oxidized methylcellulose paste, and micro-fibrillar collagen), bipolar cautery and warm salineirrigation need to be available.33 In this approach, thepalatine nerve and dental branches of V2 are oftensacrificed; therefore, the patient will lose sensation tothe hard palate and ipsilateral upper dentition.
Endoscopic endonasal transpterygoid approachesto the infratemporal fossa compares favorably withthe exposure provided by traditional anteriorapproaches except for lesions that extend below thelevel of the hard palate. Its exposure is more exten-sive than that of an endoscopic or microscopic subla-bial transmaxillary approach, therefore, allowing forthe management of lesions of greater extent. Fur-thermore, endoscopic endonasal transpterygoidapproaches avoids morbidities that are inherent tolateral and non-endoscopic anterior approaches suchas cosmetic issues related to skin incision, need forbony osteotomies, or temporalis muscle manipula-tion, TMJ pain and dysfunction, paralysis of facialnerve branches, craniotomy, and brain retraction.Trismus can result from scarring of the pterygoidmuscles.
A drawback of the endoscopic endonasal trans-pterygoid approaches is the limited exposure of theparapharyngeal ICA. The medial pterygoid muscle,eustachian tube, and styloid diaphragm have to bemobilized to identify the ICA in the medial wall ofinfratemporal fossa. Proximal control of the ICA isbest achieved transcervically, if necessary. This con-sideration is of utmost importance as it limits the in-dication of the endoscopic endonasal transpterygoidapproaches to lesions that displace rather thaninvade the soft tissues of the infratemporal fossa. Be-
nign tumors such as neurilemmomas and juvenileangiofibromas are ideal lesions. However, select low-grade adenocarcinomas and adenoid cystic carcino-mas, presenting with a ‘‘displacing’’ rather than aninvasive growth pattern, can also be removed throughthis approach. Invasive tumors most often mandate atraditional approach that enables proximal ICA con-trol and exenteration of the soft tissues of the infra-temporal fossa. Regardless of the approach, theanatomy of the infratemporal fossa is complex and itscontrol requires significant surgical expertise. Sur-gery in this area should only be attempted by a teamthat is well versed in its anatomic and surgical intri-cacies. This is especially relevant for any minimalaccess technique where the margin for error is small.
Postoperative cerebrospinal fluid leak and ascend-ing infection are a concern. However, the introductionof the nasoseptal flap has dramatically lowered theincidence of postoperative cerebrospinal fluid leakand the incidence of meningitis or other intracranialinfection is very low.17,34 These flaps can also coverthe ICA and prevent its exposure to nasopharyngealsecretions. Healing of the surgical defect is fasterusing a vascularized flap than with free tissue grafts.
Nasal morbidity and function after endoscopicendonasal transpterygoid approaches have raisedsome of valid concerns regarding bleeding, crustingand local infection. These are related to the extent ofdissection and resection; therefore, the approachshould be modified according to the needs of the case,taking this issue into consideration. In a prospectivestudy, however, we found that nasal function recoversto preoperative levels around 6 months after thesurgery.35
CONCLUSION
Endonasal endoscopic transpterygoid approacheshave opened new corridors for the treatment oflesions affecting the infratemporal fossa. Potentialmorbidity associated with endoscopic transpterygoidapproaches seems less than that of open approaches.A detailed understanding of the anatomy of infratem-poral fossa from the endoscopic perspective allows thesurgeon to plan an adequate corridor, and completethe resection in a safe manner.
REFERENCES
1. Berkovitz B. Infratemporal region and temporomandibular joint.In: Standring S, editor. Gray’s Anatomy. 39th ed. Philadelphia,PA: Elsevier Churchill Livingstone; 2005. pp519–525.
2. Hitotsumatsu T, Rhoton AL Jr. Unilateral upper and lower sub-total maxillectomy approaches to the cranial base: microsurgicalanatomy. Neurosurgery 2000;46:1416–1452; discussion 1452–1453.
3. Isolan GR, Rowe R, Al–Mefty O. Microanatomy and surgicalapproaches to the infratemporal fossa: an anaglyphic three-dimensional stereoscopic printing study. Skull Base 2007;17:285–302.
4. Tiwari R, Quak J, Egeler S, et al. Tumors of the infratemporalfossa. Skull Base Surg 2000;10:1–9.
Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012 319

5. Bolger WE. Endoscopic transpterygoid approach to the lateralsphenoid recess: surgical approach and clinical experience. Oto-laryngol Head Neck Surg 2005;133:20–26.
6. DelGaudio JM. Endoscopic transnasal approach to the pterygo-palatine fossa. Arch Otolaryngol Head Neck Surg 2003;129:441–446.
7. Fortes FS, Sennes LU, Carrau RL, et al. Endoscopic anatomy ofthe pterygopalatine fossa and the transpterygoid approach: de-velopment of a surgical instruction model. Laryngoscope2008;118:44–49.
8. Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau RL.Expanded endonasal approach: fully endoscopic, completelytransnasal approach to the middle third of the clivus, petrousbone, middle cranial fossa, and infratemporal fossa. NeurosurgFocus 2005;19:E6.
9. Herzallah IR, Germani R, Casiano RR. Endoscopic transnasalstudy of the infratemporal fossa: a new orientation. OtolaryngolHead Neck Surg 2009;140:861–865.
10. Dallan I, Bignami M, Battaglia P, Castelnuovo P, TschabitscherM. Fully endoscopic transnasal approach to the jugular foramen:anatomic study and clinical considerations. Neurosurgery2010;67(3 Suppl Operative):ons1–7; discussion ons7–8.
11. Theodosopoulos PV, Guthikonda B, Brescia A, Keller JT, ZimmerLA. Endoscopic approach to the infratemporal fossa: anatomicstudy. Neurosurgery 2010;66:196–202; discussion 202–203.
12. Zimmer LA, Hart C, Theodosopoulos PV. Endoscopic anatomy ofthe petrous segment of the internal carotid artery. Am J RhinolAllergy 2009;23:192–196.
13. Vrionis F, Cano WG, Heilman CB. Microsurgical anatomy of theinfratemporal fossa as viewed laterally and superiorly. Neuro-surgery 1996;39:777–785; discussion 785–786.
14. Couldwell WT, Sabit I, Weiss MH, Giannotta SL, Rice D. Trans-maxillary approach to the anterior cavernous sinus: a microana-tomic study. Neurosurgery 1997;40:1307–1311.
15. Sabit I, Schaefer S, Couldwell WT. Modified infratemporal fossaapproach via lateral transantral maxillotomy: a microsurgicalmodel. Surg Neurol 2002;58:21–31; discussion 31.
16. Bejjani GK, Sullivan B, Salas–Lopez E, et al. Surgical anatomyof the infratemporal fossa: the styloid diaphragm revisited. Neu-rosurgery 1998;43:842–852; discussion 852–853.
17. Hadad G, Bassagasteguy L, Carrau R, et al. A novel reconstruc-tive technique after endoscopic expanded endonasal approaches:vascular pedicle nasoseptal flap. Laryngoscope 2006;116:1882–1886.
18. Fernandez–Miranda J, Prevedello D, Madhok R, et al. Sphenoidseptations and their relationship with internal carotid arteries:anatomical and radiological study. Laryngoscope 2009;119:1893–1896.
19. Vilela MD, Rostomily RC. Temporomandibular joint-preservingpreauricular subtemporal-infratemporal fossa approach: surgicaltechnique and clinical application. Neurosurgery 2004;55:143–153; discussion 153–154.
20. Mansour OI, Carrau RL, Snyderman CH, Kassam AB. Preauric-ular infratemporal fossa surgical approach: modifications of the
technique and surgical indications. Skull Base 2004;14:143–151;discussion 151.
21. Carrau R, Kassam A, Snyderman C. Skull base infratemporalfossa approach. Otolaryngology and Facial Plastic Surgery.eMedicine. 2009. http://emedicine.medscope.com/article/851375-overview.
22. Leonetti JP, Anderson DE, Marzo SJ, Origitano TC, Schuman R.The preauricular subtemporal approach for transcranial petrousapex tumors. Otol neurotol 2008;29:380–383.
23. Moreira–Gonzalez A, Pieper DR, Cambra JB, Simman R, Jack-son IT. Skull base tumors: a comprehensive review of transfacialswing osteotomy approaches. Plast Reconstr Surg 2005;115:711–720.
24. Har–El G. Combined endoscopic transmaxillary-transnasalapproach to the pterygoid region, lateral sphenoid sinus, andretrobulbar orbit. Ann Otol Rhinol Laryngol 2005;114:439–442.
25. Ong BC, Gore PA, Donnellan MB, Kertesz T, Teo C. Endoscopicsublabial transmaxillary approach to the rostral middle fossa.Neurosurgery 2008;62(3 Suppl 1):30–36; discussion 37.
26. Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL.Expanded endonasal approach: the rostrocaudal axis. Part I.Crista galli to the sella turcica. Neurosurg Focus 2005;19:E3.
27. Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL.Expanded endonasal approach: the rostrocaudal axis. Part II.Posterior clinoids to the foramen magnum. Neurosurg Focus2005;19:E4.
28. Kassam A, Snyderman C, Gardner P, Carrau R, Spiro R. Theexpanded endonasal approach: a fully endoscopic transnasalapproach and resection of the odontoid process: technical casereport. Neurosurgery 2005;57(1 Suppl):E213; discussion E213.
29. Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R.Expanded endonasal approach: fully endoscopic, completelytransnasal approach to the middle third of the clivus, petrousbone, middle cranial fossa, and infratemporal fossa. NeurosurgFocus 2005;19:E6.
30. Fortes FS, Sennes LU, Carrau RL, et al. Endoscopic anatomy ofthe pterygopalatine fossa and the transpterygoid approach: de-velopment of a surgical instruction model. Laryngoscope2008;118:44–49.
31. Kassam AB, Prevedello DM, Carrau RL, et al. The front door toMeckel’s cave: an anteromedial corridor via expanded endoscopicendonasal approach- technical considerations and clinical series.Neurosurgery 2009;64(3 Suppl):71–82; discussion 82–83.
32. Zanation AM, Snyderman CH, Carrau RL, Gardner PA, Preve-dello DM, Kassam AB. Endoscopic endonasal surgery for petrousapex lesions. Laryngoscope 2009;119:19–25.
33. Kassam A, Snyderman CH, Carrau RL, Gardner P, Mintz A.Endoneurosurgical hemostasis techniques: lessons learned from400 cases. Neurosurg Focus 2005;19:E7.
34. Kassam AB, Thomas A, Carrau RL, et al. Endoscopic reconstruc-tion of the cranial base using a pedicled nasoseptal flap. Neurosur-gery 2008;63(1 Suppl 1):ONS44–52; discussion ONS52–53.
35. Pant H, Bhatki AM, Snyderman CH, et al. Quality of life follow-ing endonasal skull base surgery. Skull Base 2010;20:35–40.
320 Correlation of Endoscopic and Multiplanar CT Anatomy HEAD & NECK—DOI 10.1002/hed March 2012