Gliosarcoma with extension to infratemporal fossa and ventricle · 2016-12-07 · CASE REPORT...
6
CASE REPORT Gliosarcoma with extension to infratemporal fossa and ventricle Sang-Jek Liew a,b , Wen-Jui Liao a,b , Jung-Tung Liu a,b , Wei-Chean Tan a,b, * a Department of Neurosurgery, School of Medicine, Chung Shan Medical University, Taichung 402, Taiwan b Department of Neurosurgery, Chung Shan Medical University Hospital, Taichung 402, Taiwan Received 2 September 2011; received in revised form 3 April 2013; accepted 1 October 2013 Available online 27 December 2013 KEYWORDS gliosarcomas; infratemporal fossa; ventricle Summary Gliosarcomas are bimorphic intra-axial tumors. They rarely involve both the skull base and ventricles simultaneously. A case of temporal lobe gliosarcoma with significant infra- temporal fossa and lateral ventricle extension is reported. The patient, an 82-year-old man, had gradual general weakness and a poor response to speech for 3 weeks. Neurological exam- ination was unremarkable except for poor awareness and myoclonic jerks. Magnetic resonance imaging revealed a 72-cm 3 right temporal mass with extension into the infratemporal fossa and the wall of the temporal horn of the lateral ventricle, and consisted of intra-axial and extra- cranial components with extension to the cavernous sinus, dura, temporal bone, and sphenoid ridge. The patient underwent a right-sided craniotomy through the orbitozygomatic approach. Gross total resection was achieved. The histopathological diagnosis was gliosarcoma. Frac- tional whole-brain radiation and chemotherapy with temozolomide were administered subse- quently. However, the tumor recurred 1.5 months after his initial treatment, and the survival time was 9.2 months. In the case of a mass lesion with both intra-axial and extracranial involvement, the simultaneous involvement of both the skull base and ventricles is highly un- expected, and gliosarcoma should be included in the differential diagnoses of brain tumors. The overall treatment and outcome will be difficult to determine if the skull base and ventri- cles are both involved. An extensive multimodality treatment might be effective in patients with gliosarcomas according to a review of the literature. The recurrence-free time of gliosar- coma with skull base extension ranges from 2 months to 12 months, and for gliosarcoma with ventricular extension, it ranges from 1.5 months to 2 months. The survival time of gliosarcoma with skull base extension ranges from 7 months to 22 months, and with ventricular extension, it Conflicts of interest: The authors have no conflicts of interest relevant to this article. * Corresponding author. Department of Neurosurgery, Chung Shan Medical University Hospital, and School of Medicine, Chung Shan Medical University, 110, Section 1, Chien-Kuo North Road, Taichung 402, Taiwan. E-mail addresses: [email protected] (S.-J. Liew), [email protected] (W.-C. Tan). 1682-606X/$ - see front matter Copyright ª 2013, Taiwan Surgical Association. Published by Elsevier Taiwan LLC. All rights reserved. http://dx.doi.org/10.1016/j.fjs.2013.10.002 Available online at www.sciencedirect.com ScienceDirect journal homepage: www.e-fjs.com Formosan Journal of Surgery (2013) 46, 211e216
Transcript of Gliosarcoma with extension to infratemporal fossa and ventricle · 2016-12-07 · CASE REPORT...

Formosan Journal of Surgery (2013) 46, 211e216
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.e-f js .com
CASE REPORT
Gliosarcoma with extension to infratemporalfossa and ventricle
Sang-Jek Liew a,b, Wen-Jui Liao a,b, Jung-Tung Liu a,b,Wei-Chean Tan a,b,*
aDepartment of Neurosurgery, School of Medicine, Chung Shan Medical University, Taichung 402,TaiwanbDepartment of Neurosurgery, Chung Shan Medical University Hospital, Taichung 402, Taiwan
Received 2 September 2011; received in revised form 3 April 2013; accepted 1 October 2013Available online 27 December 2013
KEYWORDSgliosarcomas;infratemporal fossa;ventricle
Conflicts of interest: The authors h* Corresponding author. Department
University, 110, Section 1, Chien-KuoE-mail addresses: [email protected]
1682-606X/$ - see front matter Copyrhttp://dx.doi.org/10.1016/j.fjs.2013.
Summary Gliosarcomas are bimorphic intra-axial tumors. They rarely involve both the skullbase and ventricles simultaneously. A case of temporal lobe gliosarcoma with significant infra-temporal fossa and lateral ventricle extension is reported. The patient, an 82-year-old man,had gradual general weakness and a poor response to speech for 3 weeks. Neurological exam-ination was unremarkable except for poor awareness and myoclonic jerks. Magnetic resonanceimaging revealed a 72-cm3 right temporal mass with extension into the infratemporal fossa andthe wall of the temporal horn of the lateral ventricle, and consisted of intra-axial and extra-cranial components with extension to the cavernous sinus, dura, temporal bone, and sphenoidridge. The patient underwent a right-sided craniotomy through the orbitozygomatic approach.Gross total resection was achieved. The histopathological diagnosis was gliosarcoma. Frac-tional whole-brain radiation and chemotherapy with temozolomide were administered subse-quently. However, the tumor recurred 1.5 months after his initial treatment, and the survivaltime was 9.2 months. In the case of a mass lesion with both intra-axial and extracranialinvolvement, the simultaneous involvement of both the skull base and ventricles is highly un-expected, and gliosarcoma should be included in the differential diagnoses of brain tumors.The overall treatment and outcome will be difficult to determine if the skull base and ventri-cles are both involved. An extensive multimodality treatment might be effective in patientswith gliosarcomas according to a review of the literature. The recurrence-free time of gliosar-coma with skull base extension ranges from 2 months to 12 months, and for gliosarcoma withventricular extension, it ranges from 1.5 months to 2 months. The survival time of gliosarcomawith skull base extension ranges from 7 months to 22 months, and with ventricular extension, it
ave no conflicts of interest relevant to this article.of Neurosurgery, Chung Shan Medical University Hospital, and School of Medicine, Chung Shan MedicalNorth Road, Taichung 402, Taiwan.om (S.-J. Liew), [email protected] (W.-C. Tan).
ight ª 2013, Taiwan Surgical Association. Published by Elsevier Taiwan LLC. All rights reserved.10.002

212 S.-J. Liew et al.
ranges from 0.33 months to 9.2 months. Gliosarcoma with ventricular involvement might be apoor prognostic factor, and may help in the prediction of recurrence-free and survival time.Copyright ª 2013, Taiwan Surgical Association. Published by Elsevier Taiwan LLC. All rightsreserved.
1. Introduction
Gliosarcomas account for 2e8% of all cases of glioblastomamultiforme (GBM), depending on the definitions used. Theyare primary brain tumors with mixed glial and mesenchymalcomponents and were first described in 1895 by HeinrichStroebe.1 The most common location has been reported tobe the temporal lobe, accounting for 37.5e44% of cases.2e4
However, skull base or ventricular involvement is highlyunexpected. Only five cases of skull base involvement 4e8
and only four cases of ventricular involvement 9e12 havebeen reported in the English literature. Moreover, to thebest of our knowledge, the simultaneous involvement ofthe skull base and ventricles has not been previously re-ported in the English literature. In this report, we describea case of temporal lobe gliosarcoma with significant infra-temporal fossa and lateral ventricle extension.
2. Case report
2.1. History and examination
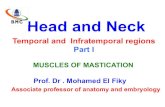
An 82-year-old man presented with a history of old cere-brovascular accident with left hemiparesis and epilepsyunder Dilantin control for 2 years. He experienced a gradualgeneral weakness and had a poor response to speech for 3weeks. His neurological examination showed unremarkableresults except for poor awareness and myoclonic jerks. Theinitial Karnofsky performance status score was 50% beforethe operation. Magnetic resonance imaging revealed a 72-cm3 right temporal mass spreading into the infratemporalfossa (Fig. 1A) via the foramen ovale (Fig. 1D). The tumorextended to the wall of the temporal horn of the lateralventricle (Fig. 1B), cavernous sinus (Fig. 1C), temporal bone(Fig. 1A), and sphenoid ridge. The lesion’s overall appear-ance suggested a possible extra-axial origin, with differ-ential diagnoses including GBM, sarcoma, abscess,hemangiopericytoma, and metastatic carcinoma.
2.2. Treatment
The patient underwent a right craniotomy through theorbitozygomatic approach. The tumor consisted of intra-axial and extracranial components with extension to thecavernous sinus, dura, temporal bone, and sphenoid ridge.The tumor had a yellow and reddish-brown color withan irregular, hard consistency and a relatively well-circumscribed margin. The frozen-section analysis sug-gested a spindle-cell malignancy. Extracapsular dissectionwas performed after internal debulking of the tumor. Grosstotal resection was achieved. The exposed sphenoid sinusfloor and temporal dural defect were repaired with surgisis
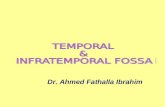
dural graft (Co. COOK, Cook Biotech Incorporated, WestLafayette, USA). The patient was subsequently treatedwith fractionated whole-brain radiation with a total dose of50 Gy, followed by 5 days of temozolomide; however, thetumor recurred 1.5 months after his initial treatment(Fig. 2). The patient died of pneumonia, and the survivaltime was 9.2 months.
2.3. Histological examination
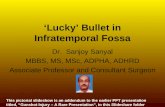
The histopathological diagnosis was consistent with glio-sarcoma. A gliomatous area of the tumor had the featuresof GBM and positive immunoreactivity for GFAP (Fig. 3A),S100 (Fig. 3B), and vimentin (Fig. 3C). In the sarcomatousarea, there was a spindle-cell proliferation. The geneticanalysis revealed P53 focal positive (Fig. 3D) and MGMT (O6-methylguanince-DNA methyltransferase) negative (Fig. 3E).
3. Discussion
Gliosarcoma is a variant of GBM and diagnosed as a Grade IVneoplasm (World Health Organization in 2007) that consistsof glial and sarcomatous cell populationsdthe glialcomponent being that of GBM and the sarcomatous elementhaving the features of any sarcoma type, but most oftenthose of the malignant fibrous histiocytoma.2,13 It has beeninitially suggested that gliosarcomas should be regarded asGBM with proliferating endothelium having sarcomatousfeatures. Vascular smooth muscle and multipotent stemcells 13 have also been proposed in the context of histo-genesis. However, data from recent studies have showncommon genetic features for both cell populations,2 andsarcomatous areas are believed to represent a phenotypicchange in GBM cells instead of a separate malignancy.1 Theincidence of gliosarcoma in published series varies between2% and 8% of all malignant gliomas.1e3 The most commonlocation has been reported to be the temporal lobe (in37.5e44% of the patients).2e4 However, skull base andventricular involvement has rarely been reported.
We performed a Medline database search. The keywords“gliosarcoma”, “skull base”, and “ventricle” were queriedindividually and also in association. The included limits were“English” for the language category. The date of the latestsearch was March 2013. There were only five cases of skullbase involvement 4e8 and only four cases of ventricularinvolvement 9e12 in the English literature. Moreover, thesimultaneous involvement of the skull base and the ventri-cles has not been previously reported in the English litera-ture. We reviewed age, sex, race, location, treatment,recurrence-free and survival time, and immunohistochem-ical studies in these cases (Table 1). In the six cases of skullbase involvement group (including our patient), the patients

Figure 1 (A) Postcontrast coronal T1-weighted magnetic resonance imaging (MRI) showing a 72-cm3 right temporal mass withextension into the infratemporal fossa (arrow) and invading the temporal bone (arrowhead). (B) Postcontrast axial T1-weighted MRIshowing tumor extending to the wall of the temporal horn of the lateral ventricle (arrowheads). (C) Noncontrast axial T2-weightedMRI showing cavernous sinus invasion (arrow). (D) Postcontrast coronal T1-weighted MRI showing temporal mass spreading into theinfratemporal fossa via the foramen ovale (arrow).
Gliosarcoma with infratemporal fossa extension 213
comprised four men and two women with a median age of61.8 years (range 51e82 years). The locations were all in theright temporal region. Themedian recurrence-free time was6.6 months (range 1.5e12 months) after the initial treat-ment, and the survival time ranged from 7 months to 22months after the initial treatment. In the ventricularinvolvement group (including our patient; Table 1), therewere five patients consisting of four men and one womanwith a median age of 51.2 years (range 25e82 years). Thetumor(s) were all located in the lateral ventricles: three onthe right side, one on the left side, and one on both sides.After the initial treatment, the recurrence-free time rangedfrom 1.5 months to 2 months, and the survival time rangedfrom 0.33 months to 9.2 months.
On magnetic resonance images, gliosarcomas appear asan extra-axial lesion despite the intra-axial origin of thetumor, as in the present case. The lesions extend to theinfratemporal fossa and the wall of the temporal horn of
the lateral ventricle, and also involved the cavernous sinus,temporal bone, and sphenoid ridge. In this case, involve-ment of the infratemporal fossa and the lateral ventriclewas apparent at the time of initial presentation. The pa-tient underwent a right craniotomy through the orbitozy-gomatic approach, which enabled the surgeons to gain wideaccess to the high lesion, temporal floor, and cavernoussinus, and to avoid the temporal muscle, in a shortdistance.
The median actuarial survival is 11.5 months for glio-sarcoma patients, 11.0 months for the control group ofGBM, and 8.1 months for the entire GBM group.1 The me-dian survival for the gliosarcoma group does not differsignificantly from that of the control GBM group (p Z 0.36)or of the entire GBM group (p Z 0.16).1 Median survival forgliosarcoma patients ranges from 6.25 months13 to 8.75months2 with radiation therapy. Sade et al4 reported apatient with gliosarcoma with infratemporal fossa

Figure 2 Postcontrast (A) axial and (B) coronal T1-weighted magnetic resonance imaging showing tumor recurrence in thetemporal area (arrowhead) and infratemporal fossa (arrow).
214 S.-J. Liew et al.
extension, having completed radiotherapy and chemo-therapy, who was recurrence-free at the 12-month follow-up evaluation. Schuss et al 8 reported an unusual case ofgliosarcoma that involved the temporal skull base and thedura, having extensive multimodality treatment (partialresection, radiotherapy and chemotherapy with temozo-lomide, imatinib, hydroxycarbamide, bevacizumab, irino-tecan). Their report demonstrated that extensivemultimodality treatment might be effective in patientswith gliosarcomas who have poor prognostic factors, forexample, unmethylated MGMT status 8 (12 months ofrecurrence-free and 22 months of survival time; Table 2).However, in our case, the patient was subsequentlytreated with fractionated whole-brain radiation, followed
Figure 3 Microscopic examination by histochemical stains revevimentin. Genetic analysis reveals (D) P53 focal positive amethyltransferase.
by 5 days of temozolomide. The tumor recurred 1.5months after his initial treatment, and his survival timewas 9.2 months. An analysis of the predominant compo-nents of the tumor and whether there is ventricular in-vasion might be helpful to us for prediction of theprognosis. Gliosarcoma with ventricular involvementmight be a poor prognostic factor. However, because ofthe small number of cases in the literature, this needs tobe determined in the future.
In the reviewed six cases of the skull base involvementgroup (including our patient), the tumor was all in the righttemporal region. Whether the anatomic structure, anypathophysiological factor, or other reasons led to thisphenomenon should likewise be explored in the future.
als positive immunoreactivity for (A) GFAP, (B) S100, and (C)nd (E) MGMT negative. MGMT Z O6-methylguanine-DNA

Table 1 Clinical data on gliosarcoma with skull base and/or ventricular extension reported in the literature.
Study, year, ref no Age(y)
Sex Race Location Surgical resection Radiation, totaldose (Gy)
Chemotherapy Recurrence-free (mo)
Survival(mo)
Murphy, 19857 70 Female Caucasian Right temporal base Right anteriortemporal lobectomy
Local radiation(100)
NM 6 NM
BoRota, 20065 59 Male NM Right fronto-temporalwith infratemporal fossaextension
Gross-total resection Radiotherapy (NM) NM 6 NM
Sade, 20064 55 Male NM Right temporal base withinfratemporal fossaextension
Gross-total resection Whole-brainradiation (NM)
temozolomide (NM) 12 NM
Maeda, 20106 51 Female NM Right temporal base Gross-total resection Local radiation (60) ACNUtemozolomide,imatinib,
2 7
Schuss, 20118 54 Male Caucasian Right temporal base withinfratemporal fossaextension
Partial resection Radiotherapy (NM) hydroxycarbamidebevacizumab,irinotecan
12 22
Higashino, 200110 29 Male NM Right lateral ventricle Partial resection Whole-brainradiation (60)
ACNU, carboplatin NM 2.6
Walker, 200612 25 Male NM Left frontal withintraventricular extension
NM NM NM NM NM
Govindan, 20099 55 Female NM Bilateral lateral ventricle Gross-total resection Non Non NM 0.33Moiyadi, 201011 65 Male NM Right lateral ventricle Surgical resection Radiotherapy (NM) temozolomide 2 NMLiew (our patient) 82 Male Asian Right temporal base with
infratemporal fossa andlateral ventricle extension
Gross-total resection Whole-brainradiation (50)
temozolomide 1.5 9.2
ACNU Z nimustine; NM Z not mentioned.
Glio
sarco
mawith
infra
temporalfossa
exte
nsio
n215

Table 2 Immunohistochemical analysis on gliosarcomawith skull base and/or ventricular extension reported in theliterature
Study MGMT EGER p53 1p/19qloss
Murphy,19857
NM NM NM NM
BoRota,20065
NM Negative Negative Negative
Sade, 20064 NM Negative Negative NegativeMaeda,20106
NM NM NM NM
Schuss,20118
Unmethylated NM Positive NM
Higashino,200110
NM NM NM NM
Walker,200612
NM NM NM NM
Govindan,20099
NM Positive Positive NM
Moiyadi,201011
NM NM Positive NM
Liew (ourpatient)
Unmethylated NM Positive NM
EGFR Z epidermal growth factor receptor; MGMT Z O6-meth-ylguanine-DNA methyltransferase.
216 S.-J. Liew et al.
Thus, we conclude that, with regard to a mass lesionwith both intra-axial and extracranial involvement, thesimultaneous involvement of the skull base and ventriclesmust be extremely rare, and gliosarcoma should beincluded in the differential diagnosis of brain tumors. Theoverall treatment and outcome would be difficult todetermine if the skull base and ventricles are bothinvolved. However, radical resection combined withextensive multimodality treatment might be effective inpatients with gliosarcomas and might promise a betteroutcome. Ventricular involvement might be a poor prog-nostic factor, but this should be proved in the future.Whether ventricular invasion might help in prediction of
recurrence-free and survival time also needs to beinvestigated.
References
1. Lutterbach J, Guttenberger R, Pagenstecher A. Gliosarcoma: aclinical study. Radiother Oncol. 2001;61:57e64.
2. Galanis E, Buckner JC, Dinapoli RP, et al. Clinical outcome ofgliosarcoma compared with glioblastoma multiforme: NorthCentral Cancer Treatment Group results. J Neurosurg. 1998;89:425e430.
3. Morantz RA, Feigin I, Ransohoff 3rd J. Clinical and pathologicalstudy of 24 cases of gliosarcoma. J Neurosurg. 1976;45:398e408.
4. Sade B, Prayson RA, Lee JH. Gliosarcoma with infratemporalfossa extension: case report. J Neurosurg. 2006;105:904e907.
5. Borota OC, Scheie D, Bjerkhagen B, Jacobsen EA, Skullerud K.Gliosarcoma with liposarcomatous component, bone infiltra-tion and extracranial growth. Clin Neuropathol. 2006;25:200e203.
6. Maeda D, Miyazawa T, Toyooka T, Shima K. Temporal glio-sarcoma with extraneural metastasis: case report. Neurol MedChir. 2010;50:343e345.
7. Murphy MN, Korkis JA, Robson FC, Sima AA. Gliosarcoma withcranial penetration and extension to the maxillary sinus.J Otolaryngol. 1985;14:313e316.
8. Schuss P, Ulrich CT, Harter PN, Tews DS, Seifert V, Franz K.Gliosarcoma with bone infiltration and extracranial growth:case report and review of literature. J Neurooncol. 2011;103:765e770.
9. Govindan A, Bhat DI, Mahadevan A, et al. An unusual case ofintraventricular gliosarcoma. Clin Neuropathol. 2009;28:379e383.
10. Higashino T, Inamura T, Kawashima M, et al. A lateral ven-tricular gliosarcoma arising in an ependymoma. Clin Neuro-pathol. 2001;20:219e223.
11. Moiyadi A, Sridhar E, Jalali R. Intraventricular gliosarcoma:unusual location of an uncommon tumor. J Neurooncol. 2010;96:291e294.
12. Walker M, Gabikian P. Benign and malignant pathology inneurofibromatosis type 1. Neurology. 2006;67:E13.
13. Perry JR, Ang LC, Bilbao JM, Muller PJ. Clinicopathologic fea-tures of primary and postirradiation cerebral gliosarcoma.Cancer. 1995;75:2910e2918.