Genetic Testing and Management of the Hereditary...
16
Carol A. Burke, MD, FACG Genetic Testing and Management of the Hereditary Gastrointestinal Cancer Syndromes Carol A. Burke, MD, FACG Sanford R. Weiss MD Center for Hereditary Colorectal Neoplasia Department of Gastroenterology and Hepatology Cleveland Clinic, Ohio Objectives • Identify phenotype of hereditary CRC syndromes • Utilize tumor testing in Lynch Syndrome (LS) • Recognize criteria for germline genetic testing 2 ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology Page 1 of 16
Transcript of Genetic Testing and Management of the Hereditary...

Carol A. Burke, MD, FACG
Genetic Testing and Management of the Hereditary Gastrointestinal
Cancer SyndromesCarol A. Burke, MD, FACG
Sanford R. Weiss MD Center for Hereditary Colorectal NeoplasiaDepartment of Gastroenterology and Hepatology
Cleveland Clinic, Ohio
Objectives
• Identify phenotype of hereditary CRC syndromes• Utilize tumor testing in Lynch Syndrome (LS)• Recognize criteria for germline genetic testing
2
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 1 of 16

Carol A. Burke, MD, FACG
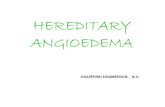
Pathways to CRC
Adenoma Serrated Neoplasm
FAP MYH
Lynch Syndrome
Sporadic CRC
CIN-MSS CIMP-MSS/MSI
MSI
MLH1 promotor methylationBRAF mutation
MSI
Lynch Syndrome• Present in 1:350 individuals, causes 5% of CRC• Caused by germline mutation in a MMR gene
– MLH1, MSH2, EPCAM MSH6, PMS2• Causes tumor signature called microsatellite instability, MSI• MSI detected through pathology lab
4
MLH1 MSH2
ImmunohistochemistryBAT25
Tumor Tissue
Normal Tissue
MSI
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 2 of 16

Carol A. Burke, MD, FACG
Hereditary Colon Cancer SyndromesSyndrome Features
Lynch Syndrome Colorectal, endometrial, ovarian, gastric, urothelial, small bowel, skin and brain Ca
Li Fraumeni Syndrome Childhood cancers, sarcoma, leukemia, brain tumors, breast cancer, CRC
Familial Adenomatous Polyposis Adenomas, CRC, duodenal, gastric, thyroid cancer, osteomas, sebaceous cysts, CHRPE, adrenal and desmoid tumors
MYH-Associated Polyposis Adenomas, CRC, duodenal cancer, thyroid cancer
NTHL1- associated Polyposis Adenomas, CRC, endometrial cancer
Polymerase proofreading associated polyposis Adenomas, endometrial cancer, brain cancer
Peutz-Jeghers Syndrome Mucocutaneous melanin, hamartomas, breast, CRC, SB, GI, lung, pancreatic, and gonadal tumor/cancers
PTEN Tumor Hamartoma Syndrome Hamartomas, dermatologic lesions, macrocephaly, breast, thyroid, endometrial, renal, colorectal cancers
Juvenile Polyposis Syndrome Hamartomas, colon, gastric cancer, HHT in patients with SMAD4 mutations5
Recognizing Hereditary CRC Personal History• Age of onset of intestinal and
extra-intestinal tumors• Pathology of tumors• Number of polyps• Head circumference (CS)• Extra-intestinal features
(epistaxis or GIB : JPS-SMAD4)
Family History • Gather in 3 generations• Occurrence and age of
cancer diagnosis• Age and cause of death• Presence of features within
spectrum of HCRC
6
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 3 of 16

Carol A. Burke, MD, FACG
Risk Assessment Tool
1. Do you have FDR with any of the following < age 50?1. CRC2. Uterus, ovary, stomach, small intestine, urinary tract, bile ducts,
pancreas or brain cancer
2. Have you had any of the following diagnosed < age 50?1. CRC2. Colorectal polyps
3. Do you have 3 or more relatives with CRC?Kastrinos et al. Am J Gastro 2009;104:
Risk Assessment Tool
1. Do you have FDR with any of the following < age 50?1. CRC2. Uterus, ovary, stomach, small intestine, urinary tract, bile ducts,
pancreas or brain cancer
2. Have you had any of the following diagnosed < age 50?1. CRC2. Colorectal polyps
3. Do you have 3 or more relatives with CRC?Kastrinos et al. Am J Gastro 2009;104:
Yes identifies up to 95% of LS patients
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 4 of 16

Carol A. Burke, MD, FACG
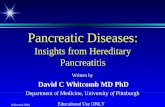
Amsterdam Criteria I for HNPCC
= unaffected
= affected CRC
• >3 relatives with CRC• >2 successive generations• 1 FDR to other 2• 1 CRC diagnosed <50 yrs• FAP excluded
Vasen HF et al, Dis Colon Rectum 1991
Your patient age 38
Dx 72
Dx 63
9
Amsterdam Criteria I for HNPCC
= unaffected
= affected CRC
• >3 relatives with CRC• >2 successive generations• 1 FDR to other 2• 1 CRC diagnosed <50 yrs• FAP excluded
Vasen HF et al, Dis Colon Rectum 1991
Your patient age 38
Only 50% of patients who meet AC I have LS
Dx 72
Dx 63
10
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 5 of 16

Carol A. Burke, MD, FACG
Other Criteria for HNPCC
Amsterdam Criteria II • >3 relatives with HNPCC-
associated Ca (CRC, SB endometrial, urothelial)
• ≥2 successive generations• 1 FDR to other two• 1 Ca dx <50 yrs• FAP excluded
Revised Bethesda Criteria• CRC diagnosed <50 years• Synchronous or metachronous
CRC or LS-associated tumor • CRC with MSI-high pathology
features diagnosed <60 years• Patient with CRC and >1 FDR with
LS-associated tumor diagnosed <50 years or 2 FDR or SDR at any age
11Vasen H, Gastroenterology 1999;116:1453–8 Umar A. et al. J Natl Cancer Inst. 2004;18;96(4):261-8
Accuracy of Methods to Diagnose LSCriteria Sensitivity Specificity
Clinical CriteriaAC II 0.22 0.98Revised Bethesda Guidelines 0.82 0.77
Prediction ModelsMMRpredict 0.69 0.90MMRPro 0.89 0.85PREMM1,2,6 0.90 0.67
Tumor TestingMSI 0.85 0.90IHC 0.83 0.89
12Giardiello FM, MSTF; Am J Gastro 2014
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 6 of 16

Carol A. Burke, MD, FACG
Importance of Universal Testing for LS• 1066 unselected CRCs
– 19.5% MSI; 21 patients diagnosed with LS– 43% diagnosed >50 yrs– 22% didn’t meet AC II or Bethesda guidelines
Hampel H et al. NEJM 2005;352;18
Germline Testing Results In 21 Relatives
Relationship Tested Positive Negative
First degree 54 25 29
Second degree 22 10 12
> Third degree 41 17 24
Total 117 52 65
13
Test all CRCs for MSI: “Universal Testing”
• Evaluation of Genomic Applications in Practice and Prevention
• US Multi-Society Task Force on Colorectal Cancer
• American College of Gastroenterology
14
Genet Med 2009:11(1):35–41
Giardiello FM , Am J Gastro 2014;109:1159
Syngal S, Am J Gastroenterol 2015; 110:223–262
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 7 of 16

Carol A. Burke, MD, FACG
Cancer Risk in AC I FamiliesImpact of MSI vs MSS
* P<.001 Compared to SEER Lindor N, JAMA. 2005;293:1979-1985
15
Site of Cancer SIR
161 families MSI(N=1855)
CRC 6.1*
Uterus 4.1*
Stomach 4.6*
Kidney 2.6*
Ovary 2.0*
Small Intestine 7.6*
Ureter 9.0*
Site of Cancer SIR
No MSI(N=1567)
CRC 2.3*
Uterus 0.8
Stomach 1.4
Kidney 0.9
Ovary 1.5
Small Intestine 1.6
Ureter 2.9
Site of Cancer SIR
MSI(N=1855)
No MSI(N=1567)
P value
CRC 6.1* 2.3* <0.001
Uterus 4.1* 0.8 <0.001
Stomach 4.6* 1.4 0.008
Kidney 2.6* 0.9 0.04
Ovary 2.0* 1.5 0.60
Small Intestine 7.6* 1.6 0.10
Ureter 9.0* 2.9 0.29
Cancer Risk in AC I FamiliesImpact of MSI vs MSS
* P<.001 Compared to SEER Lindor N, JAMA. 2005;293:1979-1985
16
Site of Cancer SIR
161 families MSI(N=1855)
CRC 6.1*
Uterus 4.1*
Stomach 4.6*
Kidney 2.6*
Ovary 2.0*
Small Intestine 7.6*
Ureter 9.0*
Site of Cancer SIR
No MSI(N=1567)
CRC 2.3*
Uterus 0.8
Stomach 1.4
Kidney 0.9
Ovary 1.5
Small Intestine 1.6
Ureter 2.9
Site of Cancer SIR
MSI(N=1855)
No MSI(N=1567)
P value
CRC 6.1* 2.3* <0.001
Uterus 4.1* 0.8 <0.001
Stomach 4.6* 1.4 0.008
Kidney 2.6* 0.9 0.04
Ovary 2.0* 1.5 0.60
Small Intestine 7.6* 1.6 0.10
Ureter 9.0* 2.9 0.29
Familial CRC Type X
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 8 of 16

Carol A. Burke, MD, FACG
Yield of Biopsy of Adenomas in LS
• Maximize preoperative diagnosis of LS• Biopsy all CRCs• Consider biopsy of adenomas for IHC if:
• Proximal, large, in patient <40 years old• Patient with adenoma and family history HNPCC or LS
Detection of MMR in Adenomas in Lynch Syndrome
Adenoma Size MSI-H IHC<5 mm (N=22) 32% 38%5-9 mm (N=7) 29% 57%>10 mm (N=6) 100% 100%
Yurgelun MB, Cancer Prev Res 2012:5;574
Extended Colectomy Decreases CRC recurrence in LS
• Comparison: Extended vs segmental colectomy• Recurrence: 0% in extended colectomy cohort
CRC Risk In Segmental Colectomy Cohort
Parry S, et al Gut 2011;60:950-95718
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 9 of 16

Carol A. Burke, MD, FACG
MSI/IHC
Loss MLH1
BRAF mutation (+) and/or MLH1promoter methylation (+)
Sporadic Cancer
BRAF mutation (–) and/or MLH1 promoter methylation (-)
Genetic assessment and germline testing for MLH1 mutation
Loss MSH2, MSH6, PMS2
Germline testing directed by IHC
Tumor Testing based Patient Care
Giardiello, MSTF, Am J Gastro 2014:109
Manage patient and family according to genetic test results
19Follow sporadic CRC Guidelines
Tumor Testing based Patient CareCRC
MSI/Abnormal IHC
Germline MMR
Mutation
Lynch Syndrome
No MSI
Familial Colorectal
Cancer Type X
20Follow LS guidelines
Colonoscopy every 3-5 years
Sporadic
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 10 of 16

Carol A. Burke, MD, FACG
Tumor Testing based Patient CareCRC
MSI/Abnormal IHC
No Germline Mutation Detected
Lynch Like Syndrome
*Bi-allelic Somatic MMR
mutations
Germline MMR
Mutation
Lynch Syndrome
No MSI
Familial Colorectal Type X
or Sporadic
*Mensenkamp, Gastro 2014;146:643
21Follow LS guidelines
Follow Sporadic CRC guidelines
Cancer Surveillance in LSOrgan Age to Begin Method Interval
Colon 20-25 yrs* Colonoscopy 1-2 yrs
Uterus/Ovary 30-35 yrs TVUS, Endometrial Bx 1-2 yrs
After childbearing or age 40
TAH-BSO
Stomach/SB 30-35 yrs EGD-bx H pylori 2-3 yrs
Urothelium 30-35 yrs Urinalysis 1 yr
*Or 10 years younger than the youngest age of the affected relative (2-5 yrs if relative <25 yrs)
22
Giardiello F, Gastro 2014;147:502Syngal S, Am J Gastroenterol 2015; 110:222
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 11 of 16

Carol A. Burke, MD, FACG
Adenomatous Polyposis SyndromesFAP• Due to APC mutation• Autosomal dominant• Affects 1:10,000 individuals
– 30% cases de novo• 60-100% risk of CRC
MAP• Due to bi allelic MYH mutations• Autosomal recessive • Usually <100 adenomas
– (lymphoid aggregates)
• 2-3% population carriers• 60% risk of CRC
Colorectal Phenotype and Genotype
Grover S, et al. JAMA. 2012;308(5):485-492
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 12 of 16

Carol A. Burke, MD, FACG
Prevalence of extra-intestinal features of FAP/MAP
Desmoid tumors (15%) Thyroid carcinoma (2-17%) Adrenal adenoma (7-13% ) Osteomas (50-90%) Supernumerary teeth (11-27%) CHRPE (70-80%) Soft tissue tumors (50%)
Lipoma, fibroma, sebaceous cysts Hepatoblastoma (<2%)
Gastric features of FAP/MAP• Fundic gland polyposis
– Prevalence: 88%– Histology
• LGD: 38%• HGD: 3%:
• Gastric adenomas– Prevalence: 10%– Usually antrum
• Gastric Cancer: IncreasingCHRPE
Bianchi L, Burke CA, et al. Clin Gastro Hep 2007;6:180
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 13 of 16

Carol A. Burke, MD, FACG
Duodenal features of FAP• Duodenal adenomas
– Prevalence: 100%• Adenomatous papilla1
– 54% if papilla appears normal – 89% if papilla appears abnormal– TIP: EGD with papilla bx to help establish diagnosis
• Periampullary/Duodenal cancer– Risk based upon duodenal polyposis stage
2Groves C Gut 2002;50:6361Burke C, GIE 1999;49:358
Staging of Duodenal Polyposis1 point 2 points 3 points
No. of polyps 1-4 5-20 >20
Polyp size (mm) 1-4 5-10 >10
Histology Tubular TVA Villous
Dysplasia Mild Moderate Severe
Spigelman AD. Lancet 1989;2: 783
Stage Points Cancer Risk1 EGD Interval*
0 0 0% 4 yrs
I 1-4 0% 2-3 y
II 5-6 2.3% 1-3 y
III 7-8 2.4% 6 -12 m
IV 9-12 36% Duodenectomy vs
3 - 6 m
Groves C Gut 2002;50:636*Syngal S, Am J Gastroenterol 2015; 110:223; 1Groves C Gut 2002;50:636
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 14 of 16

Carol A. Burke, MD, FACG
Surveillance of FAP/MAPPhenotype Procedure Age (yrs) Interval (yrs)
Classic FAP FS or colonoscopy 10-15 1
aFAP/MAP Colonoscopy 18-20/
25-30
1-2
Surgical Consult When polyps detected
Post operative FS or pouchoscopy NA 1
Thyroid Thyroid Ultrasound Late teens 1
Duodenum EGD- duodenoscopy 20-25 Based on stage
NCCN guidelines Genetic/Familial High Risk Assessment Colorectal. version 1.2015
Genetic Testing IndicationsLynch Syndrome testing• AC I or II• Revised Bethesda Criteria• Family History of LS• Endometrial Cancer <50• >5% risk of LS based on
predictive models
APC and MYH* testing• Personal history of >20 adenomas or
>10 adenomas with other features• Family hx of APC or MYH mutation• Desmoid, hepatoblastoma, papillary
thyroid cancer, CHRPE (multi focal, bilateral)
• *Serrated Polyposis Syndrome (criteria 1 and 3 with some adenomas)
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 15 of 16

Carol A. Burke, MD, FACG
Serrated Polyposis Syndrome WHO Criteria
1. >5 SP above sigmoid, >2 are >10 mm 2. >1 SP above sigmoid and FDR with SPS3. >20 SP distributed throughout the colon
1Snover, et al. WHO Classification of tumours of the digestive system. Berlin: Springer-Verlag; 2010
Conclusions
• HCRC phenotype includes CRC and extra-colonic manifestations
• Utilize tumor testing in Lynch Syndrome (LS)• Germline genetic testing used for diagnosis of
hereditary polyposis syndromes
32
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 16 of 16