
The Path of Least Resistence: Using Available Tools to Support the E-Resources Lifecycle

Stephen A. McClave, MD
Stephen A. McClave, MD
Louisville, Kentucky
Nutritional Management of the Hospitalized Patient:
Insight from the Guidelines
Timing of Nutrition TherapyFirst week
Argument to AVOID feeding
Height dz process, inflam, insulin resist, intolerance
Evidence that full feeds may be harmful
Importance of preserving autophagy
Teleologic argument disrupting fight/fright/flight response
Opposing argument to PROVIDE feeding
Window of opportunity to attenuate disease severity, SIRS
Provide non-nutritional benefits of nutrition Rx
Second week
Change in priorities, less controversial
Need for nutritional benefits, impact of increasing caloric deficit
Catabolism to anabolism
ICU
SA McClave, JK DiBaise. GE Mullin, RG Martindale (Amer J Gastroent 2016;111:315)
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 1 of 12

Stephen A. McClave, MD
Providing vs Not Providing Early EN
Early EN vs No Early EN (p=0.01)
Mortality 14.1%→8.7%, p=0.05
Early EN vs No Early EN (p=0.05)
SA McClave, BE Taylor(JPEN 2016;40:159-211)
Infection 51.7%→36.3%, p=0.03
Controls: Do nothing (STD)Intentional delay
What are the Benefits of Early EN?
• Non-Nutrition benefits – Seen in all patients (trophic feeds OK)
Gastrointestinal responsesTrophic on gut integrity Commensal bacteriaGut/lung axis of inflamm Secretory IgA, GALT tissueReduced bact virulence
Immune responsesModulate regulatory cells Promote Th-2 >Th-1 lymphocytes Maintain MALT tissue
Metabolic responsesIncretin to insulin sens Reduce hyperglycemia (AGES)
• Nutrition benefits – Seen in high risk patients (need full feeds)
Protein, calories Micronutrients, anti-oxidants
Maintain LBM Stimulate protein synthesis
• Non-Nutrition benefits – Seen in all patients (trophic feeds OK)
Gastrointestinal responsesTrophic on gut integrity Commensal bacteriaGut/lung axis of inflamm Secretory IgA, GALT tissueReduced bact virulence
Immune responsesModulate regulatory cells Promote Th-2 >Th-1 lymphocytes Maintain MALT tissue
Metabolic responsesIncretin to insulin sens Reduce hyperglycemia (AGES)
• Nutrition benefits – Seen in high risk patients (need full feeds)
Protein, calories Micronutrients, anti-oxidants
Maintain LBM Stimulate protein synthesis
S McClave, R Martindale (CCM 2014;42:2600) S McClave (Amer J Gastroent 2016;111:315)
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 2 of 12

Stephen A. McClave, MD
What is the OptimumDose for Feeding in ICU?
• Proposed strategies:
Starvation (Van den Berghe, Marik) - Autophagy
Trophic feeding (Rice) – ARDSNet Trial, Surviving Sepsis
Permissive underfeeding – Charles, Arabi, Petros
Full dose aggressive feeding (Heyland) - Pep Up
• Best option: High protein hypocaloric feeding (first week)
Advance by slower ramp-up
• Proposed strategies:
Starvation (Van den Berghe, Marik) - Autophagy
Trophic feeding (Rice) – ARDSNet Trial, Surviving Sepsis
Permissive underfeeding – Charles, Arabi, Petros
Full dose aggressive feeding (Heyland) - Pep Up
• Best option: High protein hypocaloric feeding (first week)
Advance by slower ramp-up
Trophic Feeds
Full Feeds
1CCM 2011;39:967 2JAMA 2012;307:795 3JPEN 2016;40:242 4Am J Clin Nutr 2014;100:1337 5NEJM 2015;372:2398
80% Goal calories
25% Goal calories
• Trophic feeds vs full feeds (ARDS pts)Rice Single center (n=200) 1
Outcomes same (Full Rx to home)ARDSNet Multicenter (n=1000) 2
Outcomes no different (12 mos) • Permissive underfeeding
Half vs full calories/protein - Petros Med ICU pts (n=100) 3
Infections less in full feeds (11.1 vs 26.1%, p=0.04)Half vs full calories, full protein both
Charles Trauma pts (n=83) 4 Outcomes no differentArabi Mix ICU pts (n=1350) 5 Outcomes no different (3 mos)
Is Trophic Feeding OK to Start?
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 3 of 12
Stephen A. McClave, MD
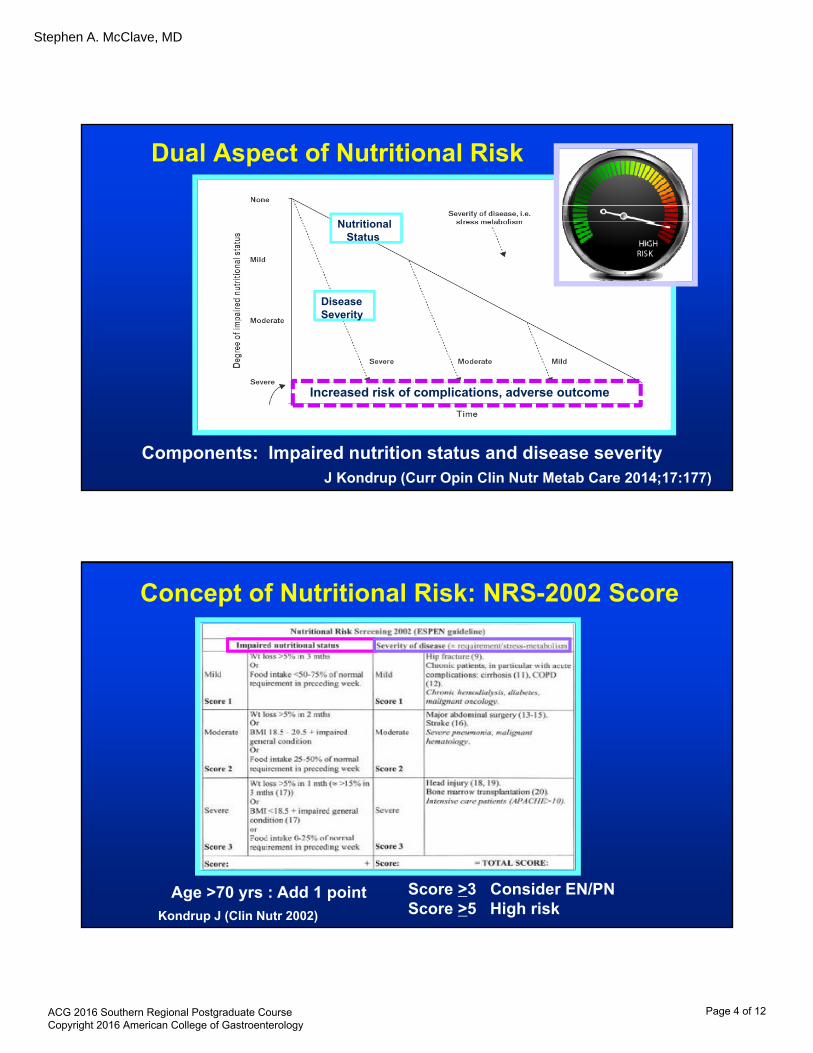
Dual Aspect of Nutritional Risk
Components: Impaired nutrition status and disease severityJ Kondrup (Curr Opin Clin Nutr Metab Care 2014;17:177)
NutritionalStatus
Disease Severity
Increased risk of complications, adverse outcome
Kondrup J (Clin Nutr 2002)
Age >70 yrs : Add 1 point Score >3 Consider EN/PNScore >5 High risk
Concept of Nutritional Risk: NRS-2002 Score
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 4 of 12

Stephen A. McClave, MD
Concept of Nutritional Risk: Nutric Score
Heyland DK (Crit Care 2011;6:1)
Six factors for Nutric Score: Disease severity:
AgeInitial APACHE II scoreInitial SOFA scoreInterleukin-6Comorbidities
Poor nutritional status:Hosp LOS prior to ICU
Nutritional Risk May Predict Benefit from Rx
1 ClinNutr 2012 2 Clin Nutr 2015 Jan 3 Amer J Resp Crit Care 2016
• Jie Study NRS-2002 1 - High Risk patients (n=120)with NRS Score >5Insufficient (n=77) Sufficient Nutr Rx (n=43)
Overall complications 51% 26% *Nosocomial infection 34% 16% *
No benefit (sufficient vs insufficient ) Low Risk pts (n=965) NRS <5
• Heyland Study Nutric Score 2
Observational Trial (n=1199)
• Arabi Trial Post Hoc Analysis 3
Nutric score did not predictbetter response to Rx
(both full protein, 46 vs 71% kcal)
EN Rx Effect onHigh Risk Pts (p<0.0001)
Low Risk (p=NS)
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 5 of 12

Stephen A. McClave, MD
Should We Push to Goal Quickly?Endogenous Glucose Production
• Endogenous glucose production
Greater early in ICU
Cannot be suppressed
• Energy requirements not same as
energy needs
• Hypocaloric feeding
Avoids overfeeding
Better tolerance
Better outcome
More appropriateV Fraipont, JC Prieser (JPEN 2016;37:705-13)
Endogenous
Exogenous
GS Doig (Lancet Respir Med 2015; 3: 943–52) Heymsfield (Amer J Cardiol 1987;60:75G)
• Patient candidatesNPO x 7-10d, low BMI, wght lossCHF, mech vent, hypercapnea
• Spectrum of changes with feedingCHF, underlying cardiomyopathy Electrolyte, fluids, gas exchange abnsInsulin resistence, poor WBC fxn, infection, respir failure
• RCT ICU Multicenter (n=339) phos <0.65 mmol/LSlow ramp-up over 4 days vs standard (STD)
Results: Mortality worse in STDInfection: Slow 8% vs STD 16% (p=0.01)
No different: MOF, Durat MVOther signs: ↓K+ (27%) ↑gluc (52%)
Resp fail (91%) Diuretic need (30%)
Calories Phosphate
Survival
Should We Push to Goal Quickly?Refeeding Syndrome
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 6 of 12

Stephen A. McClave, MD
Monitor Tolerance and Adequacy• GRVs should not be used as part of routine care1
Montejo Multicenter RCT 2 GI Complic %Goal 500cc GRV (n=160) 47.8% * 89% *200cc GRV (n=169) 63.6% 83%
Reignier Multicenter RCT 3 VAP Infect Mortality DeficitNo GRV used (n=227) 16.7% 26.4% 27.8% 319 kcalRoutine GRV (n=222) 15.8% 27.0% 27.5% 509 kcal
• Implementation plan – Announce new policy of No GRVs in 1 year
Use GRVs on initiating EN x 3days only, d/c EN for 2nd 500 cc
No GRVs: Awake/alert pts, tube in SB
• Focus instead on:
Phys exam Passing stool, gas Tracking I&Os
Aspirat risk Access site Protein calorie goals1McClave (JPEN 2016;40:159) 2Montejo (ICM 2010;36:1386) 3Reignier (JAMA 2013;309:249)
Which Formula Should Be Used?
• Most patients - Start with standard polymeric formula • Elective Surgery, SICU – Use arg/fish oil formula 1
Infection ↓ 41% (OR=0.59)Hosp LOS ↓2.38 days
• Crit Care MICU – Don’t recommend arg/FO formulaNo difference mortality, infection, LOS
• ALI/ARDS – No recommendation anti-inflammatory lipid profile formula 2-8
Gadek, Singer, Pontes-Arruda, Grau-CarmonaAll benefit
Rice ARDSNet, Stapleton, MetaPlusHarm or no benefit
Elective Surg
Critical ICU
ARDS or ALI
1 JW Drover (JACS 2011;212(3);385) 2 JE Gadek (CCM 1999;27:1409) 3 P Singer (CCM 2006;34:1033) 4 A Pontes-Arruda (CCM 2006;34:2325)5 T Grau-Carmona (Clin Nutr 2011;30:578) 6 T Rice (JAMA 2012;307:795)7 R Stapleton (CCM 2011;39:1655) 8 A Van Zanten (JAMA 2014;312:514)
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 7 of 12

Stephen A. McClave, MD
Multicenter Trial in EnglandEN vs PN in 2400 ICU pts
High risk (mortality 34%)Each provided 80% goal feedsNo difference in outcomes
Impact: Under controlled conditions, high risk patients, PN can = ENEN still preferred over PN, but should lower threshold to use PN
SE Harvey CALORIES Trial Group [NEJM 2014; 371(18):1673]
What is the Role of Parenteral Nutrition?
Use of Parenteral Nutrition
• Exclusive PN (EN not feasible)
Low Risk - Withhold exclusive PN
(NRS 2002 ≤3, Nutric Score ≤5)
High Risk - Initiate exclusive PN ASAP (esp malnourished)
(NRS 2002 ≥5, Nutric Score ≥6)
• Supplemental PN (on EN) - Add at 7-10d if <60% goal high or low risk 1
• Maximize efficacy of PN
Use Multidisciplinary Nutrition Team, protocols in place
Moderate glucose control (140-180 mg/dL)
High protein hypocaloric (80%) dosing first week 2
Transition off PN when EN provides >60% goal
1Heiddeger (Lancet 2012 Dec 3) 2 Jiang (Clin Nutrit 2011;30:730)
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 8 of 12
Stephen A. McClave, MD
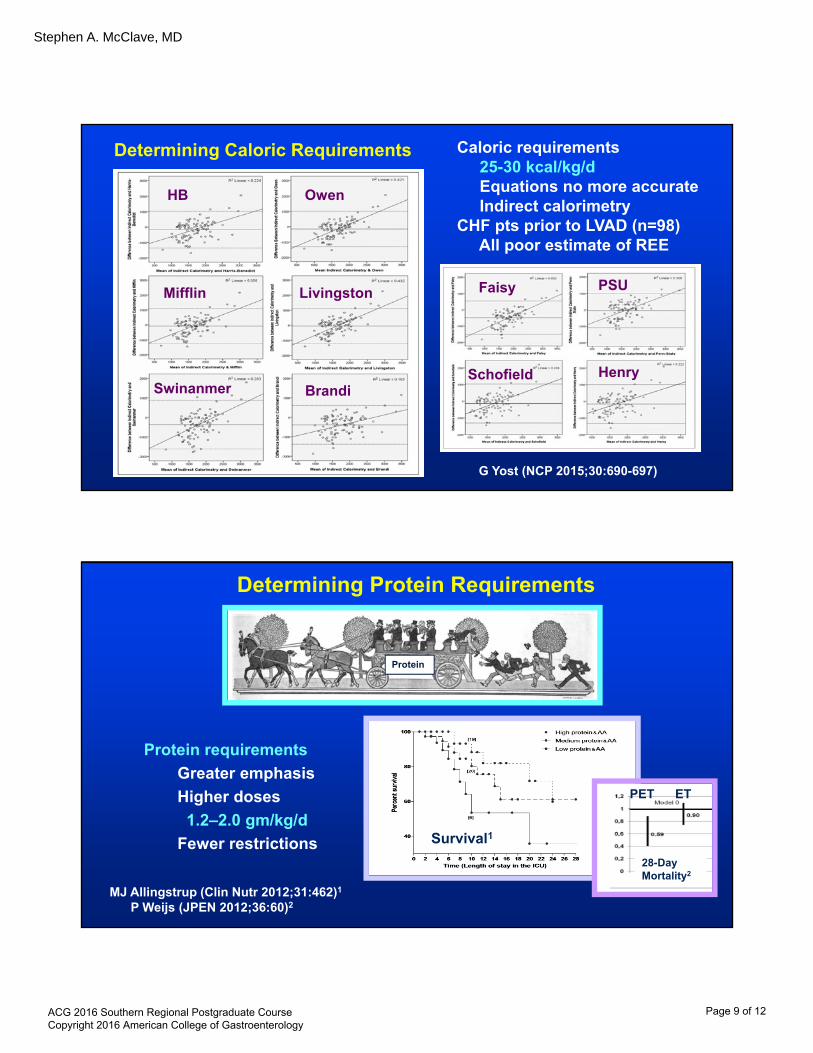
Determining Caloric Requirements
G Yost (NCP 2015;30:690-697)
Caloric requirements25-30 kcal/kg/dEquations no more accurateIndirect calorimetry
CHF pts prior to LVAD (n=98)All poor estimate of REE
HB Owen
Mifflin Livingston
BrandiSwinanmer
Faisy PSU
Schofield Henry
Determining Protein Requirements
Protein requirements
Greater emphasis
Higher doses
1.2–2.0 gm/kg/d
Fewer restrictions
MJ Allingstrup (Clin Nutr 2012;31:462)1
P Weijs (JPEN 2012;36:60)2
28-Day Mortality2
Survival1
PET ET
Protein
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 9 of 12

Stephen A. McClave, MD
Initiation of EN: Adjustments for Obesity• Adjustment for obesity – high protein hypocaloric feeds
Push protein to 2.0 (Class I, II) to 2.5 (Class III) gm prot/kg IBW/day
Reduce calories to 65-70% of requirements (IC)
• Beware of paradox of obesity 1
Effect of central adiposity - ICU mortality 25%→44% 2
Effect of sarcopenia - Mortality 14→32% 3
• Adjustment for obesity – high protein hypocaloric feeds
Push protein to 2.0 (Class I, II) to 2.5 (Class III) gm prot/kg IBW/day
Reduce calories to 65-70% of requirements (IC)
• Beware of paradox of obesity 1
Effect of central adiposity - ICU mortality 25%→44% 2
Effect of sarcopenia - Mortality 14→32% 3
1 NCP 2008;23:16-34 2 CCM 2010;38:1308 3 Crit Care 2013;17:R206
Avoid common mistakes:Don’t need to feed (reserves)Feed to maintain fat mass
Drag Tube Drag Wire Untethered EndoscopyTube
NJ
PEGJ
Prioritizing Techniques for Enteral Access
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 10 of 12
Stephen A. McClave, MD
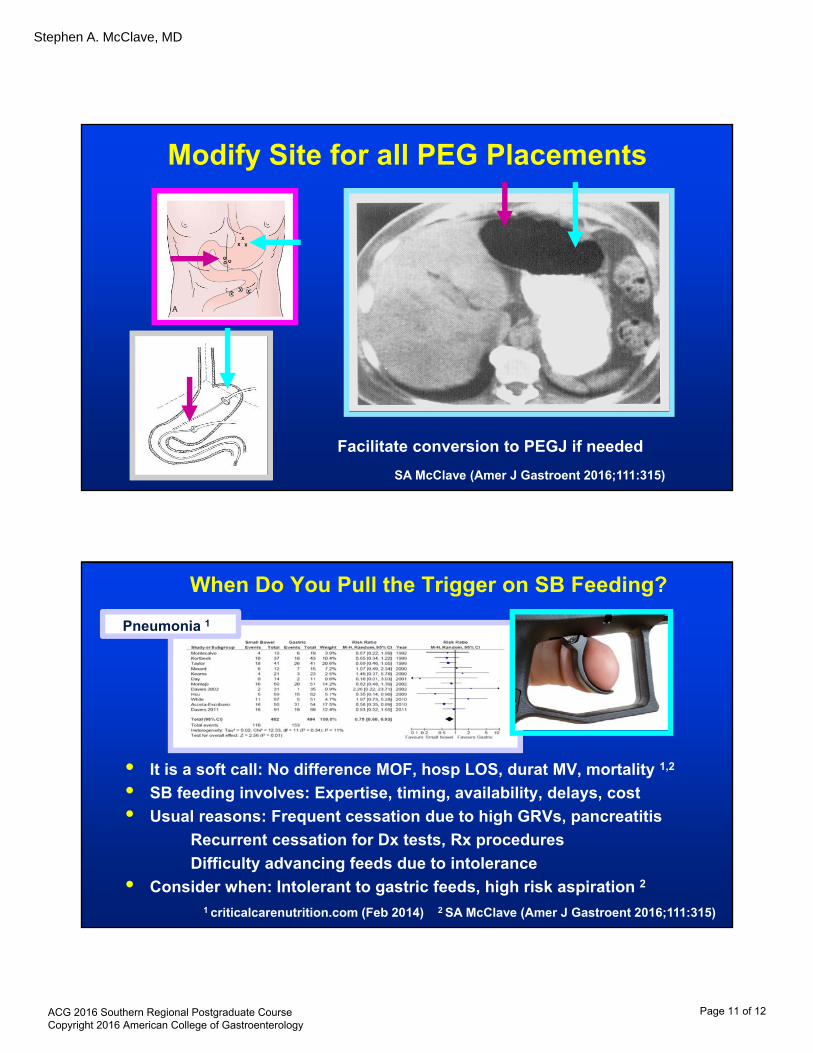
Modify Site for all PEG Placements
Facilitate conversion to PEGJ if needed
SA McClave (Amer J Gastroent 2016;111:315)
When Do You Pull the Trigger on SB Feeding?
• It is a soft call: No difference MOF, hosp LOS, durat MV, mortality 1,2
• SB feeding involves: Expertise, timing, availability, delays, cost
• Usual reasons: Frequent cessation due to high GRVs, pancreatitis
Recurrent cessation for Dx tests, Rx procedures
Difficulty advancing feeds due to intolerance
• Consider when: Intolerant to gastric feeds, high risk aspiration 2
1 criticalcarenutrition.com (Feb 2014) 2 SA McClave (Amer J Gastroent 2016;111:315)
Pneumonia 1
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 11 of 12

Stephen A. McClave, MD
Take Time to Secure Enteral Access Device
Hollister (Vertical) Clamp
Magnetic Nasal BridleSA McClave (Amer J Gastroent 2016;111:315)
Conclusions
• The benefit of early nutrition Rx is due primarily to EN• The risk/benefit ratio of PN is narrower, use in high risk
patients when EN insufficient
• Manner of delivery shifting
Trophic feeding initially with slower ramp up
High protein hypocaloric feeding may be best option first week
• Assess risk, monitor tolerance - Important, prognostic, directs Rx
ACG 2016 Southern Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
Page 12 of 12


















