Endometrial Ablation: Where Have We Been? Where … ablation.pdfEndometrial Ablation: Where Have We...
31
Endometrial Ablation: Where Have We Been? Where Are We Going? MALCOLM G. MUNRO, MD, FRCS(C), FACOG Department of Obstetrics and Gynecology, David Geffen School of Medicine at UCLA, Kaiser Foundation Hospitals, Los Angeles Medical Center, Los Angeles, California Abstract: Endometrial ablation (EA) is targeted destruction of the endothelial surface of the uterine cavity. The procedure was originally designed as a less invasive alternative to hysterectomy for the symptom of heavy menstrual bleeding unrelated to structural pathology of the uterus, that was not responsive to medical therapy. More recently it has become apparent that the procedure can be per- formed in the presence of submucous leiomyomas, providing they meet a number of size and location criteria. The first EA serie as published in Germany in the 1930s, but the procedure did not attract much attention until the latter part of the 20th century. Currently, EA can be performed under endoscopic direction with the neodymium:yttrium alumnum garnet laser, with a radiofrequency resectoscope, or with an expanding array of nonresectoscopic EA systems. It is apparent that most but not all of the complications associated with resectoscopic endome- trial ablation are eliminated with nonresectoscopic endometrial ablation, but serious morbidity has been reported with all of the newer systems to date. Success and patient satisfaction seem to be enduring in the majority of well-selected patients treated in clinical trials, but repeat surgery, usually hysterect- omy, is performed in 25% to 40% by 5 years after surgery. Increased efficiencies should be realized if the procedure could be moved to an office setting. Key words: endometrial ablation, heavy menstrual bleeding, menorrhagia Introduction The concept of surgical destruction of the endometrial lining for the treatment of abnormal uterine bleeding (AUB) is not new. A monopolar radiofrequency electrosurgical probe inserted blindly into the uterus was the subject of a series published by Bardenheuer, 1 from Germany, in 1936. However, the world seemed to forget about this approach to the clinical problem of heavy menstrual bleeding (HMB) for more than 30 years when cryotherapy of the endometrium for AUB was first introduced 2 and then subjected to clinical evaluation. 3,4 It was more than a decade until the introduc- tion of endoscopically guided techniques for endometrial ablation (EA), first using 736 Correspondence: Malcolm G. Munro, MD, FRCS(c), FACOG, Department of Obstetrics and Gynecology, Permanente Los Angeles Medical Center, 4900 Sunset Boulevard, Station 3-B, Los Angeles, CA 90027. E-mail: [email protected] CLINICAL OBSTETRICS AND GYNECOLOGY / VOLUME 49 / NUMBER 4 / DECEMBER 2006 CLINICAL OBSTETRICS AND GYNECOLOGY Volume 49, Number 4, 736–766 r 2006, Lippincott Williams & Wilkins
-
Upload
duongtuong -
Category
Documents
-
view
223 -
download
2
Transcript of Endometrial Ablation: Where Have We Been? Where … ablation.pdfEndometrial Ablation: Where Have We...

EndometrialAblation: WhereHave We Been?Where Are We Going?
MALCOLM G. MUNRO, MD, FRCS(C), FACOG
Department of Obstetrics and Gynecology, David Geffen School ofMedicine at UCLA, Kaiser Foundation Hospitals, Los AngelesMedical Center, Los Angeles, California
Abstract: Endometrial ablation (EA) is targeteddestruction of the endothelial surface of the uterinecavity. The procedure was originally designed as aless invasive alternative to hysterectomy for thesymptom of heavy menstrual bleeding unrelated tostructural pathology of the uterus, that was notresponsive to medical therapy. More recently it hasbecome apparent that the procedure can be per-formed in the presence of submucous leiomyomas,providing they meet a number of size and locationcriteria. The first EA serie as published in Germanyin the 1930s, but the procedure did not attract muchattention until the latter part of the 20th century.Currently, EA can be performed under endoscopicdirection with the neodymium:yttrium alumnumgarnet laser, with a radiofrequency resectoscope, orwith an expanding array of nonresectoscopic EAsystems. It is apparent that most but not all of thecomplications associated with resectoscopic endome-trial ablation are eliminated with nonresectoscopicendometrial ablation, but serious morbidity has beenreported with all of the newer systems to date.Success and patient satisfaction seem to be enduringin the majority of well-selected patients treated inclinical trials, but repeat surgery, usually hysterect-
omy, is performed in 25% to 40% by 5 years aftersurgery. Increased efficiencies should be realized ifthe procedure could be moved to an office setting.Key words: endometrial ablation, heavy menstrualbleeding, menorrhagia
IntroductionThe concept of surgical destruction ofthe endometrial lining for the treatmentof abnormal uterine bleeding (AUB) isnot new. A monopolar radiofrequencyelectrosurgical probe inserted blindlyinto the uterus was the subject of aseries published by Bardenheuer,1 fromGermany, in 1936. However, the worldseemed to forget about this approach tothe clinical problem of heavy menstrualbleeding (HMB) for more than 30 yearswhen cryotherapy of the endometriumfor AUB was first introduced2 and thensubjected to clinical evaluation.3,4 It wasmore than a decade until the introduc-tion of endoscopically guided techniquesfor endometrial ablation (EA), first using
736
Correspondence: Malcolm G. Munro, MD, FRCS(c),FACOG, Department of Obstetrics and Gynecology,Permanente Los Angeles Medical Center, 4900 SunsetBoulevard, Station 3-B, Los Angeles, CA 90027.E-mail: [email protected]
CLINICAL OBSTETRICS AND GYNECOLOGY / VOLUME 49 / NUMBER 4 / DECEMBER 2006
CLINICAL OBSTETRICS AND GYNECOLOGYVolume 49, Number 4, 736–766r 2006, Lippincott Williams & Wilkins

a hysteroscope to directed neodymium:yttrium alumnum garnet (Nd:YAG)laser energy to coagulate and vaporizethe endometrium5 and then the urologicresectoscope to remove endometrial tis-sue with a radiofrequency (RF) electro-surgical loop electrode.6 For 15 yearsresectoscopically directed EA was theprincipal method used for performingtargeted removal and/or or destructionof the endometrium, but, beginning inthe late 1990s, a number of nonresecto-scopic techniques, conceptually similarto those first introduced in the 1930s,began to appear. Today, a virtualplethora of nonresectoscopic systemsare available to the gynecologist for thetreatment of AUB by targeted destruc-tion of the endometrium. This manu-script is designed to review thesetechniques including their relative meritsand vulnerabilities as well as the resultsof clinical trials that have been publishedto date. However, a discussion of theclinical problem of AUB is necessary tohelp frame the discussion of the appro-priate role of EA in contemporarygynecology.
THE CLINICAL PROBLEM: WHAT AREWE TRYING TO SOLVE?
In the endometrium of normal ovulatorywomen, in the absence of conception andembryonic implantation, the systemicwithdrawal of corpus luteum-derivedestradiol and progesterone triggers men-strual bleeding or menstruation. Themechamism is initiated in part by theinduction of spiral artery vasoconstric-tion modulated by locally producedagents such as prostaglandin (PG)F2a7–9 and endothelin-1 (ET-1), knownto exist in abundance in the premenstrualendometrium.10–12 The resulting endo-metrial ischemia, probably aided by localproteolytic activity from matrix metallo-proteinases13–15 and other local factorssuch as nitric oxide,16,17 results insloughing of the functional layer of the
endometrium. Endometrial hemostasis islargely reliant upon local vasoconstric-tion, which, in turn is dependent uponthe local concentrations of the samevasoactive agents that initiate endome-trial ischemia. It is apparent that PGssuch as PGE218 and PGI2,19 with vaso-dilating activity, are also measurable inthe endometrial stroma, production thatis likely independent of progesterone andprobably related to estradiol and otherlocal factors.19 Consequently, an appro-priate balance of such vasoconstrictingand vasodilating agents and/or theirreceptors must be maintained to faci-litate normal endometrial hemostasis.Indeed increased local levels ofPGI2,20,21 the ratio of PGI2 to throm-boxane,22 and elevated levels of PGE2,23
PGE2 receptors,24 and the ratio of PGE2to PGF2a20 have been demonstrated inwomen with ovulatory HMB.
Heavy bleeding that occurs during thereproductive years and unassociated withpregnancy, structural pathology of theuterus, systemic disorders of hemostasis,or iatrogenic causes, has been assigneda variety of different names—HMB,menorrhagia, hypermenorrhea, anddysfunctional uterine bleeding (DUB)—a somewhat bewildering array of nomen-clature that is the root cause of bothconfusion in the interpretation of clinicaltrials and the application of their resultsto patient populations. Some use one ormore of these terms to describe asymptom, whereas others may use thesame descriptor to define a diagnosis.
Heavy bleeding in the context ofpredictable, cyclical (every 22 to 35 d)and, presumably, ovulatory cycles, isoften called menorrhagia, but as asymptom it may reflect a variety ofsystemic and local disorders that mayrequire substantial differences in investi-gation, treatment, and patient counsel-ing. Such heavy bleeding may besecondary to submucosal leiomyomasor adenomyosis, and is associated with
Endometrial Ablation: Where Have We Been? Where are We Going? 737

a surprisingly high incidence of systemicdisorders of coagulation; 13% of womenwith ‘‘menorrhagia’’ have hematologicevidence of von Willebrand disease.25,26
When cyclical HMB occurs unrelatedeither to such abnormalities, or tomedical therapy (including intrauterineprogestins) it is often called ovulatoryDUB. The endometrium of such womenlooks macroscopically and histologicallynormal, but, as previously described,tends to contain excessive vasodilatingPGs (E2 and I2) and other factors thatdistinguish the endometrial milieu ofnormally menstruating women fromthose with cyclical HMB. For example,enhanced fibrinolysis may impede theattainment of local hemostasis and hasbeen demonstrated in women with ovu-latory DUB,27,28 who generally respondfavorably when antifibrinolytic agentssuch as tranexamic acid are em-ployed.29,30 Nitric oxide, another potentvasodilator is also found in excessiveconcentrations in the endometrium ofovulatory women with HMB 31 andET-1, a vasoconstrictor important forendometrial hemostasis, is found inlower concentrations in the endome-trium of women with heavy uterinebleeding.32
AUB in women who are frequently orusually anovulatory is related to theabsence of the cyclical production ofprogesterone, and, as such, is a systemicdisorder involving or impacting thehypothalamic-pituitary-ovarian axis.Such bleeding varies in frequency, tim-ing, and flow but may be heavy, in partbecause of the lack of progesterone-mediated vasoconstricting agents suchas PGF2a33 and, in all likelihood, ET-1.
There is very little information regard-ing the pathogenesis of AUB in womenwith submucosal leiomyomas. Althoughit seems likely that myomas wouldgenerally contribute to the genesis ofAUB only if involving the endometrialsurface, there is currently no clear under-
standing of the mechanisms involved inmyoma-related bleeding.
THE CLINICAL PROBLEM: WHATINTERVENTIONS ARE AVAILABLE?
For women with chronic HMB, part ofthe therapeutic decision-making processis based on desires regarding fertility,either immediately, or for the foreseeablefuture. For those who wish to becomepregnant immediately, or who sufferfrom infertility in addition to the HMB,approaches that temporarily or perma-nently remove the ability to conceive andsupport a pregnancy are not acceptable.For those who are uncertain, or whowish to maintain the ability to bearchildren, interventions that impact ferti-lity are acceptable and are frequentlyeven desirable, but they must be rever-sible. The woman who has no desire forfertility, either now or in the future, has,at her disposal, all options, not onlythose medical approaches that allow forfuture fertility, but, as well, surgicalinterventions that inherently destroy orremove the endometrium and a variableamount of the rest of the uterus, therebyeffectively preventing the woman fromimplanting and carrying a pregnancy.
For all women with HMB, eitherovulatory or anovulatory, there exist anumber of frequently effective medicalinterventions. For women with ovulatoryDUB (HMB), options include nonster-oidal anti-inflammatory agents, anti-fibrinolytics, cyclical or continuous oralcontraceptives, and continuous, singleagent progestins, especially when admi-nistered locally via an intrauterine sys-tem (IUS) such as the levonorgesterolreleasing intrauterine system (LNG-IUS). Women with chronic anovulatoryHMB may respond to combination oralcontraceptives or the cyclic administra-tion of oral progestins alone.
When medical therapy is not tole-rated, or is ineffective, surgical interven-tions may be considered, especially if the
738 Munro

woman is willing to forego future ferti-lity. For women with heavy uterinebleeding, EA represents a surgical optionto hysterectomy with the advantages ofshort hospital stay, absence of surgicalincisions, and subsequent rapid return tonormal activity. However, EA does notat present guarantee amenorrhea or therelief of other HMB-related symptoms, afact that leads many women undergoingEA to resort to hysterectomy because ofunsatisfactory outcomes.
Resectoscopic EndometrialAblation (REA)
TECHNIQUES
Destruction of the endometrial liningunder endoscopic guidance was origin-ally described using the Nd:YAG laserthrough the instrument channel of anoperating hysteroscope.5 However, themodified urologic resectoscope and RFalternating current later became the mostcommonly used instrument, first employ-ing a resection technique with a loopelectrode6 and then using electrosurgicaldesiccation/coagulation with a ball orbarrel-shaped electrode.34 Subsequently,another modification was introducedusing grooved or spiked electrodes andhigher wattage that allowed the surgeonto electrosurgically vaporize the endome-trium.35,36 This technique results in anendomyometrial furrow similar to thatcreated by a loop electrode, without thedevelopment of tissue ‘‘chips,’’ but aslightly greater degree of coagulation inthe adjacent tissue, a feature that hasbeen shown in the context of a compara-tive trial to be associated with markedlyreduced systematic absorption of disten-sion media.37 Patients treated with va-porization had a mean distending mediadeficit of 109mL (±126) versus 367mL(±257) for those who underwent loopresection. Furthermore, only 1 of 47
patients undergoing vaporization had afluid deficit over 500mL whereas thosewho were treated with resection had sucha deficit in 14 of 44 cases. Clinicaloutcomes including patient satisfactionwith therapy as well as bleeding patternsand duration of flow were similarbetween the groups.
MEDICAL PREPARATION OF THEENDOMETRIUM BEFORE EA
Thinning the endometrium by directsuppression and/or inhibition of ovariansteroidogenesis has been seen as a pre-surgical adjuvant that has the potentialto improve clinical outcomes. Thereexists high-quality evidence described ina Cochrane review (class I evidence) thatdemonstrates that either preoperativedanazol or GnRH agonists result inshorter procedures, greater ease of sur-gery, a lower rate of postoperativedysmenorrhea, and a higher rate ofpostsurgical amenorrhea.38 Whether theshort-term doubling in amenorrhea ratesassociated with adjuvant medical sup-pression is sustained for multiple years isnot known. A cost effectiveness analysisof endometrial suppression with danazolcompared with GnRH agonists hassuggested that total healthcare costsmay be greater with GnRH agonists.39
However, the study also concluded thatamenorrhea rates were slightly higher inthe GnRH-treated group, and that studywithdrawals were greater in the danazolgroup, a factor that may have skewed theresults of the analysis. At this time, thereare no high-quality data that allow forobjective evaluation of similar outcomesassociated with other preoperativeapproaches such as system progestinsor mechanical preparation of the endo-metrium with currettege. Evidence tobe discussed subsequently suggeststhat systemic media absorption may beless with preoperative GnRH agonists.
Endometrial Ablation: Where Have We Been? Where are We Going? 739

CLINICAL TRIALS COMPARING REATO HYSTERECTOMY
The highest quality evidence evaluatinghysteroscopic and resectoscopic EAcomes from randomized clinical trials(RCTs) and systemic reviews. At thistime there exist 6 randomized studiescomparing EA to hysterectomy; 4 fromthe United Kingdom,40–43 1 from Italy,44
and 1 from North America.45 Each ofthese trials have, in addition, resulted ina number of important additional pub-lications comparing hysterectomy to EAand the first 5 comprise the core of theCochrane systematic review.46,47 Hyster-ectomy is, of course, superior in attainingamenorrhea, and, although satisfactionwith REA is high, there are usuallysomewhat greater patient satisfactionrates when the uterus is removed. Itshould be noted that women probablyvary with respect to their desires withrespect to amenorrhea—some see it as aprimary goal whereas others wouldprefer to continue to menstruate, albeitwith normal flow.48 Women who re-ceived REA had shorter hospital stays,fewer postoperative complications, andresumed activities earlier than those withhysterectomy. For women assigned toEA, reoperation rates, either with repeatablation or hysterectomy, increased stea-dily over time; up to about 30% to 40%at 4 years of follow-up in the 2 studieswith such a long follow-up interval.45,49
Both hysterectomy and EA (either laseror resectoscopic) were associated withpositive outcomes with respect tomental health, depressive symptoms,and, importantly, there were no apparentdifferences in postprocedural sexualfunction.
A potential advantage of EA is areduction in the utilization of resources,both for healthcare systems and forpatients. In some of these trials therehas been an opportunity to compare thedirect and indirect resources that wereused to accomplish the 2 types of
procedures. In the Aberdeen randomizedtrial the direct costs of EA were abouthalf that of hysterectomy within monthsof the procedure.49 However, as thefrequency of visits and reoperation in-creased, the two approaches becamevirtually equivalent at 4 years. Never-theless, although indirect costs varywidely with the patient’s economic situa-tion, the Aberdeen trial suggests that it islikely that those associated with EAlikely remain substantially lower thanfor hysterectomy.
Application of these conclusions tothe North American population ofwomen should be done with caution.Besides cultural and socioeconomic dif-ferences related to dissimilarities inhealthcare systems, the dominant proce-dure performed in all but the Italianstudy was (Abdominal Hysterectomy).In North America, many, if not mostsuch women are treated with vaginalhysterectomy, an approach that couldhave a significant impact on a number ofthese outcome variables. Furthermore, itis not clear that North Americans andEuropeans are consistently similar intheir definitions of HMB and, conse-quently, the women selected for surgicaltherapy. A federally funded randomizedtrial has now completed recruitment (theSurgical Treatments Outcomes Projectfor Dysfunctional Uterine Bleeding orSTOP-DUB) with initial, 2 to 4-yearresults expected to be published in2006.45,50
There is a paucity of randomized trialscomparing the different techniques ofREA. In the randomized trial conductedby the Aberdeen group, patients assignedto EA were subsequently randomized toeither laser ablation or endometrialresection.51 Although both procedureswere associated with similar patientsatisfaction and clinical outcomes at 12months, laser ablation was significantlymore expensive, largely due to the longerprocedure time.
740 Munro

COMPLICATIONS OF REA
A measure of the safety of any procedureis found in the incidence of complica-tions discovered either intraoperativelyor later, in the postoperative time frame.For EA, the most serious complicationsare distension media overload and uter-ine perforation with subsequent damageto surrounding structures. Other compli-cations include those related to anesthe-sia, failed access, and hemorrhage. Aprospectively performed Dutch evalua-tion of 87 hospitals reported that com-plications occur rather infrequently withone-half either cervical trauma or uterineperforation, both related to entry intothe endometrial cavity.52 The largestpublished evaluation of resectoscopiccomplications reflects the experience ofthe United Kingdom and suggests thattechniques involving endometrial resec-tion are most often associated withserious complications secondary tohemorrhage or perforation.53 This studyalso documents that experience is animportant variable as these complica-tions were most commonly encounteredin the first 100 cases of a given surgeon.As a result, the low incidence of compli-cations found in the literature from seriesand trials may not reflect the risk inthe population at large because ofthe expertise and experience of mostpublished investigators.
Distension media are required ofhysteroscopic and resectoscopic surgery,and, on occasion, substantial volumes ofsuch media can be absorbed into thesystemic circulation. Standard electro-surgical operative hysteroscopy requiresthat electrolyte-free, low viscosity solu-tions be used such as 3% sorbitol, 1.5%glycine, 5% mannitol, and combinedsolutions of sorbitol and mannitol,each of which, if sufficiently absorbedinto the systemic circulation, willresult in dilutional hyponatremia and,with the possible exception of mannitol,hypo-osmolality.54,55 These electrolyte-
free fluids can result in hyponatremia,hyposmolality, and subsequent brainedema and, in some instances, perma-nent neurologic damage or death. Suchoutcomes may be more common inpremenopausal women because of theinhibitory impact of estrogen and pro-gesterone on the brain’s sodium pump,making such women more vulnerable tocerebral edema.56 As a result, appropri-ate fluid management is critical to thesafety of resectoscopic and operativehysteroscopic surgery. The developmentof hysteroscopic electrosurgical systemsthat can operate in electrolyte-rich mediasuch as normal saline has provided anopportunity to eliminate the risk ofhyponatremia,57,58 but risks of fluidoverload remain.
The volume of systemically absorbeddistension media may be reducedwith the preoperative use of GnRHanalogs56,59 and/or with the immediatepreoperative administration of diluteintracervical vasopressin.60 There exist anumber of other measures that shouldreduce the extent of systemic intravasa-tion that include operating at the lowesteffective intrauterine pressure and avoid-ance of preoperative overhydration.Early detection of intravasation isenhanced by adherence to a strict fluidmeasurement and management protocolthat preferably includes an automatedsystem that measures fluid inflow andcaptures fluid from 3 sources: the resec-toscope, the perineal collection drape,and the floor. Such systems allow forreal-time measurement of systemic intra-vasation of distension media. The man-agement of intraoperatively recognizedexcessive intravasation varies accordingto the patient’s baseline medical condi-tion, her intraoperative assessment, thestatus of the procedure, and the amountof measured fluid intravasation. If thedeficit reaches a predetermined limit,which, depending on the patient’s base-line status could range from 750 to
Endometrial Ablation: Where Have We Been? Where are We Going? 741

1500mL, serum electrolytes are mea-sured and furosemide is given intra-venously, 10 to 40mg. Should the serumsodium fall below 125mEQ/L, or shouldthe deficit reach 1500 to 2000mL, theprocedure is expeditiously terminated.
Shortly after the introduction of REA,postablation tubal ligation syndromewas first described as a complication ofEA performed in women with previoustubal occlusion for purposes of contra-ception.61 Patients experience cyclicalpelvic pain presumably related to resi-dual and trapped endometrium in one orboth cornua. The incidence of thissyndrome is unclear but has been re-ported to be as high as 10%.62 Hystero-scopic decompression and laparoscopicsalpingectomy are frequently not effec-tive and hysterectomy has been describedas the most effective treatment.62
FACTORS AFFECTING OUTCOME OFREA
As is the case with most surgicalprocedures, clinical outcomes of REAseem to be related to a number ofpatient-specific and surgeon-specific fac-tors. Women 45 and older seem to be lesslikely to have subsequent hysterectomyand more likely than those under 45 tobe amenorrheic and satisfied with theiroutcome.63,64 Surgeon experience and/orability also seem to be important. In onestudy, the subsequent hysterectomy ratewas 12.6% when endometrial resectionwas performed exclusively by theconsultant surgeon compared with 38%if all or part of the procedure was doneby a trainee.63
The presence of adenomyosis has alsobeen associated with an increased risk ofREA failure65 and has been found in upto 75% of post-EA hysterectomy speci-mens.66 There is some evidence that withincreasing depth of resection and abla-tion, the failure rate with deep hystero-scopic resection drops to as low as 5%, aresult that may reflect more complete
removal of adenomyosis.67 Althoughfailures may be higher in women withlarger uteri and correspondingly largerendometrial cavities at least in experi-enced and able hands, success rates inuteri greater than 12 gestational weekssize may be equivalent to that of womenwith smaller sized uteri.68
An early concern about EA was thepotential for delaying the diagnosis of asubsequent endometrial carcinoma.However, it seems clear that thosewomen who have been reported todevelop endometrial malignancy afterEA are those who have the usual riskfactors for endometrial hyperplasia.69
Consequently, women who are at en-hanced risk for endometrial hyperplasiabecause of chronic anovulation may becounseled that they will remain at greaterrisk than ovulatory women for develop-ing such a disorder after EA. In suchinstances, it may be wise to consider theuse of an intermittent progestationalagent.
Nonresectoscopic EndometrialAblationA number of factors contributed to thedevelopment of alternative methodsfor destruction of the endometrium.Achievement of optimal clinical out-comes with REA, including low compli-cation rates, requires substantial skilland experience on the part of thesurgeon. The requirement for anesthesiaand relatively sophisticated equipmentboth for performing the procedure andmonitoring fluid balance contribute to aneed to perform these procedures in aresource-intense setting, usually a hospi-tal or surgical center operating room.Nonresectoscopic endometrial ablation(NREA) refers to destruction of theendometrium using any of a number oftechniques or devices placed within theendometrial cavity that do not require a
742 Munro

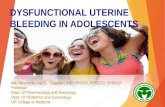
uterine resectoscope (Fig. 1). Thesesystems require less training, skill, andexperience than REA, and, as will beseen below, result in clinical outcomessimilar to those achieved by expertsurgeons. Such nonresectoscopic techni-ques are additionally attractive becausethey are relatively rapidly performed,there is a low risk of uterine perforation,a reduced or eliminated risk of systemicfluid absorption, and a potential foroffice or clinic use thereby reducingresource utilization. Nonetheless, as is
the case for any surgical device, compli-cations can occur with NREA techni-ques. A review of the Food and DrugAdministration’s (FDA) Manufacturerand User Facility Device Experiencedatabase, found reports of uterine per-foration in all of the NREA devices onthe market at that time including at leastone bowel injury in 3 of the 4.70
Although these devices are associatedwith a high degree of success, each hasintrinsic advantages and disadvantagesthat include a variable ability to destroy
FIGURE 1. NREA devices counter clockwise from top left: Microprocessor-controlled balloon thermal ablation devices including Thermachoice, Cava-term, showing the original balloon, left, and the 2 currently available balloons,right; Themablate; the Her option, a single use cryotherapeutic technique thatis performed under ultrasound direction by the surgeon; MEA, a reusablemicrowave device that uses temperature as an endpoint but which is surgeoncontrolled (the original reusable probe top and the disposable Femwave probe,bottom); HydroThermablator, a single use free fluid thermal technique that ishysteroscopically directed with the therapeutic endpoint microprocessor-controlled; NovaSure, a single use, microprocessor-controlled bipolar RFprobe that vaporizes and desiccates the endometrium.
Endometrial Ablation: Where Have We Been? Where are We Going? 743

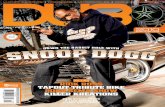
TABLE 1. Comparison of Nonresectoscopic Endometrial Ablation Devices
Energy/
Delivery
System
Trade
Name
DeviceOutside
Diameter
(mm)
SingleUse (S)/
Reusable
(R) Pretreatment
Maximum
UterineSounded
Length
(cm)
Submucus
Myomas
Allowed?
Myoma
Size/Typez
EndpointDetermination
Device (D)
Surgeon (S)
Typical
Treatment
Time (min)
Heated fluid(balloon)
Cavaterm 8.5/6.0w S Medical 10 No N/A D 15/10w
Thermablate 6.0 S Medical 9.5 ? NA D 2.1Thermachoice 5.5 S Mechanical or medical 10 Yes++ r3 cm/type II D 8.0
Cryogenic Her Option 4.5 S Medical 10 No N/A S 10Heated fluid(free)
HTA 7.8 S Medical 11 Yes+ Not known D 14
Microwave MEA 8.0 R/S Medical 14 Yes r3 cm/type II;selected type I
S 2.5
RF* (bipolar) NovaSure 7.2 S None 10 Yes++ r2 cm D 1.5
*RF=radiofrequency alternating current.
wCavaterm outside diameter (OD) is 8.5mm; Cavaterm plus OD is 6.0mm.
zType O myomas are entirely intracavitary, on a stalk; type I are sessile but have 50% of more of their maximum circumference within the endometrial cavity; type II myomas have lessthan 50% of their maximum circumference within the endometrial cavity.
+There is insufficient data to determine the type and dimension of myomas treatable with HTA.
++myomas 2 cm or less allowed, but no data available regarding clinical outcomes at this time.
744
Munro

the endometrium in endometrialcavities that are distorted by leiomyomas(Table 1).
BALLOON THERMAL ABLATION
The first system that received FDAapproval was based on the principal ofpositioning a balloon in the endometrialcavity, distending it with fluid, and thenheating that same fluid to a temperaturethat results in destruction of the endo-metrium. The first experience with theThermachoice (TC) system was pub-lished in 199471,72 and the device wasapproved for use in the United States inDecember 1997. There are now 3 otherballoon ablation systems available in atleast some regions worldwide (Table 1).
CavatermThe Cavaterm balloon ablation device(Wallsten Medical SA, Morges Switzer-land) has been in use for more than adecade in Europe and a number of othercountries, but it is, at this time, still notavailable in the United States. Theoriginal single use catheter had an out-side diameter (OD) of 8.5mm and acylindrical silicone balloon that wasadjustable according to the length ofthe endometrial cavity. The newer,modified version is called Cavaterm Plusand has a reduced OD (6mm) and apreshaped adjustable balloon, designedto facilitate intimate contact with theendometrial surface. The Cavaterm sys-tem uses an oscillating pump located inthe central control unit to vigorouslycirculate the fluid inside the balloonthereby delivering consistent tempera-ture throughout the endometrial cavity.With Caviterm Plus, the target balloontemperature was increased to 781C from751C and the pressure in the balloon wasincreased from 200 to 220mm Hg to 230to 240mm Hg, thereby allowing areduction in the treatment time from 15to 10 minutes. Power to the Cavatermcontroller is provided by a rechargeable
battery. Instructions for use limit treat-ment to normal endometrial cavities thatmeasure from 4 to 10 cm, from theinternal os to the fundus, rather than thesounded length from the external os tothe fundus, which is used as the para-meter for the TC and Menotreat devices.The manufacturer also contraindicatesuse of the device when the cervical canalis more than 6 cm in length.
There exist a number of publishedseries evaluating the Cavaterm devicebut most have rather small cohorts.A number of the reports emanate from1 group, with the most recent updatedescribing 106 of the 117 originallytreated women 10 to 49 months aftertreatment.73,74 The hysterectomy rateduring the follow-up period was 8.6%(10/116) with 7 cases associated withsubmucosal leiomyomas. The amenor-rhea rate was 29.4% but 7 of thesepatients were postmenopausal at thetime of follow-up. Satisfaction withtherapy was reported as excellent by91.5% of the study subjects. The largeststudy to date reported on 220 patientstreated with the Cavaterm Plus device,with follow-up for an average of 19months.75 The satisfaction rate at theend of the follow-up interval was 83%.Another study of 50 patients followedfor an average of 14 months (range, 6 to24mo) reported a short-term success rateof 96%, with 68% of patients developingamenorrhea, 24% with spotting, 4%eumenorrhea, and 4% failures.76 TheCavaterm study with the longest follow-up interval reported on 60 women withDUB at least 48 months after balloonablation with the Cavaterm plus sys-tem.77 In this cohort 58% were reportedto be amenorrheic, 33% hypomenor-rheic, and 9% with eumenorrhea.
MenotreatThe MenoTreat device is another bal-loon ablation device that has limiteddistribution. It is not available in the
Endometrial Ablation: Where Have We Been? Where are We Going? 745

United States. Like Cavaterm and TC,the device comprises a disposable cathe-ter, a dedicated controller unit, and aconnecting cable. The OD of the Meno-Treat is such that the cervix has to bedilated to 8mm for insertion of theballoon catheter; the duration of treat-ment 11 minutes, treatment temperatureis 851C, and the balloon pressure is set at200mm Hg. Currently unique to balloonablation systems is the ability to tailorthe therapy to cavity dimensions as thereare catheters of 2 different sizes. Thedevice also differs from the Cavatermand the TC in that the fluid is heatedwithin the controller, not the ballooncatheter. At present there are only 2published prospective evaluations. Inone, a cohort study, 84.3% of thepatients had at least a 50% reduction inbleeding [based on pictoral blood lossassessment charts (PBAC)] at 6 monthsafter the procedure.78 The other is aRCT comparing Menotreat with Cava-term, but again with 6-month results.79
Patient satisfaction and bleeding out-comes were similar for the 2 devices.
ThermablateThe EA system most recently introducedand available in a number of countries iscalled Thermablate (MDMI, Richmond,BC, Canada) and comprises a disposa-ble, prefilled catheter-balloon cartridgeand a reusable hand-held treatmentcontrol unit. The unit runs on directcurrent via a transformer that convertsalternating current from a standard walloutlet. The controller heats the glycerine-containing fluid in the cartridge that isthen forced through the catheter into theballoon by a pump that drives air intothe heating chamber. Treatment time,pressure, and temperature as well assafety checks are microprocessor con-trolled via the heating, pumping, andpressure monitoring systems. The cervixis dilated to 6 to 7mm to allow access ofthe catheter. Treatment temperature is
much higher than the other units(1731C), the pressure is similar (180mmHg), and resulting treatment time isshorter (128 s). Elevated temperature ispossible because the glycerine solutionhas a much higher boiling point. Thelimited testing has involved soundeduterine lengths of 7.0 to 9.5 cm. Thereis only one available cohort study with asmall sample size of 16 patients withresults reported at 6 months.80 Amenor-hea was experienced by half the patientsand 15 of 16 were satisfied with theresults. There have been a number ofother presentations of data related to thisdevice but most still have not beenpublished.
TCTC (Ethicon Women’s Health and Uro-logy, Sommerville, NJ) is the balloonablation system available in the UnitedStates and a number of other countriesthroughout the world. The 3 approvedversions of the device are called TC, TCII, and TC III, with the latter device theone that is currently marketed, at least inthe United States. Despite this, theavailable clinical data, particularly thosethat reflect long-term outcomes are fromstudies using the original device. Eachsystem comprises a single use ballooncatheter, a connecting cable, and adedicated controller unit that is poweredfrom a standard alternating current walloutlet. The OD of the catheter for eachsystem is 5.5mm and the heating elementis contained within the balloon itself. Thededicated controller unit activates thiselement thereby heating the fluid (5%dextrose and water) after it is injectedinto the balloon by the surgeon, and usesmicrocircuitry to monitor the parametersof balloon pressure and fluid tempera-ture and to automate treatment dura-tion. The TC II and III devices weremodified by the insertion of an impellerat the end of the catheter that serves tocirculate the heated fluid within the
746 Munro

balloon’s cavity. For each of the 3systems the target balloon temperature(871C) and pressure (160 to 180mm Hg)and the duration of treatment are thesame (8min). The data generated in allbut one published clinical trial werebased on uteri that had an endometrialcavity plus cervical canal length less than10 cm (sounded fundus to external cervi-cal os), and one that was symmetricalwithout congenital anomalies, polyps, orsubmucosal myomas. Because clinicaloutcomes are likely improved if theendometrial thickness is minimized, themanufacturer recommends that patientsshould either be mechanically treatedwith intraoperative curettage or undergopreprocedural medical suppression withgonadal steroids or GnRH analogs. Inthe clinical trials, the patient is generallygiven some sort of general or regionalanesthesia, but local and/or neurelepticanalgesia may be all that is neces-sary.81,82
There have been a number of rando-mized trials comparing TC EA toresectoscopic techniques. For FDA ap-proval in the United States, the originalTC system underwent a rigorous multi-center RCT in comparing it to REA withrollerball electrosurgical desiccation(performed by ‘‘expert’’ hysteroscopists)with follow-up at 1 year.83 Subsequentreports have described a number of out-comes at 2, 3, and 5 years, including pati-ent satisfaction and impact on bleedingvolume with the validated PBAC.84–86
The design was a 1:1 randomizationscheme involving 275 subjects withHMB, no intracavitary lesions, and asounded uterine length of 4 to 10 cm.Only a few minor complications werereported in the TC group whereas therollerball ablation patients experienced1 uterine perforation and 2 instances ofdistending media overload. Patient satis-faction with the therapeutic results wasequal at 1 year (TC 95.9%; REA 99.1%)and the FDA-defined ‘‘success’’ rates
(PBAC <75) were equivalent. The ame-norrhea rates were higher for REA(27.2%) than for TC (15.2%) and therewere 3 hysterectomies in the REA groupversus 2 in the TC group. At 5 years,there were 61 of the original 131 patientstreated with the TC system that wereavailable for evaluation, the same num-ber available from the resectoscopiccomparison group. By this time, 21 ofthe evaluable women in each of the TCand resectoscopically treated groups hadundergone hysterectomy; 3 and 2,respectively, underwent repeat ablation.
Another single-institutional RCT fromthe Netherlands also compared TC withrollerball ablation in 137 patients.87,88
Perioperatively there were a number ofcomplications with REA that includeduterine rupture and electrolyte imbalancerelated to excess absorption of distentionmedia; no such complications were seenin the balloon ablation group. At 24months the reduction in bleeding (asmeasured by the same PBAC system usedin the US trial) was greater with balloonablation but success rates (PBAC <185)and satisfaction rates (REA 75%; TC80%) were equivalent.
Although it was not randomized, alarge multicenter, multinational cohortstudy described results of TC balloonablation for 260 women with DUB.89
Results have been published describingthe experience of 188 of the original 260(72%) patients at 5 years after theirprocedure.90 Of these 75% had avoidedsubsequent surgery altogether, whereas21 had repeat ablation and 25 hadundergone hysterectomy.
For any study with high attrition (lossto follow-up) and that is reported basedon the evaluable patients, there exists thepossibility that there is selection bias andthat repeat surgery rates could be higherin the subset of women not available forevaluation, in this instance up to 5 yearsafter the original surgery. Nonetheless, itseems that a substantial proportion of
Endometrial Ablation: Where Have We Been? Where are We Going? 747

the treated women were able to avoidfuture trips to the operating room in thefollow-up interval.
There is a relative paucity of informa-tion regarding the performance of theTC device in women with abnormalendometrial cavities, particularly thosedistorted by leiomyomas. However, arandomized trial involving 93 subjectscompared treatment results of balloonablation (under local anesthesia withconscious sedation) with REA ablationin patients with type II myomas (<50%of diameter within the endometrialcavity) that were up to 3 cm in diameter.At 1 year, bleeding outcomes weresignificantly and equally reduced in the2 treatment groups.91
CRYOTHERAPY
The first clinical series describing intrau-terine cryotherapy for AUB appearedalmost 40 years ago.3,4 Subsequently,Pittrof and investigators92 from theUnited Kingdom published a cohort of67 women, 63% of whom experiencedimprovement in symptoms at follow-upintervals that ranged from 3 to 18months. The Yale group reported a75.5% amenorrhea rate at 6 monthswhich dropped to 50.3% at 22 monthsin a group of 15 patients.93 Collectively,this work allowed for the development ofa NREA system based on cryotherapeu-tic principles modified for use within theendometrial cavity.
As a result, the FDA-approved device(Her Option, American MedicalSystems, Minnetonka, MN) comprisesa disposable 4.5mm OD probe attachedto a dedicated controller unit. The probeis passed transcervically into the endo-metrial cavity, usually with little orminimal requirement for dilation. Whenactivated, the device creates an ellipticalfreeze zone about 1.5mm deep by redu-cing the local endomyometrial tempera-ture to less than – 901C. Although thereexists appropriate concern about the
potential for such a freeze depth toinvolve adjacent structures such as bo-wel, the surgeon can monitor the depthof the freeze using transabdominal ultra-sound. The required number of freezecycles depends in part on the size andshape of the endometrial cavity, butusually numbers 2 or 3 contributing toa treatment time of about 10 minutes.Published data regarding the device hasbeen limited to endometrial cavities thatare without submucosal myomas andwhich sound to 10 cm or less. Conse-quently, preprocedural assessment withone or a combination of transvaginalultrasound, saline infusion sonographyand/or hysteroscopy is necessary toidentify appropriate patients for cryo-ablation.
The clinical outcomes from the pivotaltrial designed for the FDA approvalprocess have been published at 1294
and 24 months.95 Patients enrolled intothese trials had entry criteria that weresimilar to those for most of the otherrandomized trials performed in the Uni-ted States. To be eligible, subjects wererequired to have objectively documentedheavy uterine bleeding without regard toovulatory status, but with careful exclu-sion of intracavitary abnormalities suchas polyps or leiomyomas. The totalenrollment was 279 subjects with a 2:1randomization scheme that resulted in193 patients assigned to cryoablationand 86 to resectoscopic endometrialelectrodesiccation. At 12 months, 156of the cryoablation patients were evalu-able whereas 94 took part in the24-month follow-up. The number ofevaluable patients for the resectoscopicablation group at 12 and 24 months were72 and 43, respectively. Success rateswere defined by reduction of the PBACscores to less than 75 and were equiva-lent in the 2 groups at 12 months(cryotherapy 84.6%; REA 88.9%). Eva-luation of the 2-year outcomes is a littledifficult as amenorrhea rates are not
748 Munro

reported. However, the investigatorsreport that 7.0% of the cryoablationgroup and 8.1% of the resectoscopicgroup underwent hysterectomy inthe follow-up period whereas repeatablations were performed on 8.1% and1.2%, respectively.95
FREE-HEATED FLUID
The rationale for developing balloons tocontain heated fluid was the concern thatfree fluid would pass from the endome-trial cavity either into the vaginal orthrough the fallopian tubes and into theperitoneal cavity. However, designing aballoon that can develop and maintainintimate contact with a spectrum ofcavity configurations is a challengingtask. As a result, there has been sus-tained interest in developing systemsbased around the concept of heated freefluid because of potential advantageswith respect to treatment of distortedendometrial cavities, including thosewith submucosal leiomyomas.
The HydroThermablator (HTA)(Boston Scientific Corp, Natick, MA)is a system based upon the instillation offree fluid into the peritoneal cavity underhysteroscopic monitoring. It has beenapproved by the FDA in the UnitedStates and is available in a number ofcountries worldwide. The device com-prises a single use sheath that adapts toany of a number of 2.7 to 3mm ODstandard hysteroscopes, and which isconnected to a proprietary controllerunit that uses a saline bag mounted onan attached modified IV pole. Thesystem uses low-pressure inflation ofthe endometrial cavity (<40 cm H2O)thereby dramatically reducing the inci-dence of fluid loss through the fallopiantubes. Furthermore, by creating anelectronically monitored closed system,egress of fluid via either the cervix orfallopian tubes can be detected byreduction in circulating volume, therebyallowing automatic alarms and shut-off
systems to act as safeguards. Afterdilation of the cervix and priming ofthe circuit, the telescope and sheath areplaced transcervically into the endome-trial cavity, when, after confirmation ofintracavitary positioning, the micropro-cessor-controlled automated system isstarted. The process takes approximately3 minutes to heat the fluid to 901C, 10minutes to ablate the endometrium, andabout 1 minute for the fluid to cool downat which time the device is removed.
All of the currently published seriesand the single clinical trial were per-formed on women who underwent med-ical pretreatment with leuprolide acetate;usually the 3.75mg intramuscular dose.The only published clinical trial was therandomized comparison of 276 patientswith DUB (no intracavitary or submu-cosal leiomyomas or endometrial polyps)treated with either HTA or with resecto-scopic rollerball ablation in a 2:1 rando-mization scheme.96 A report describingthe 3-year results has also been pub-lished.97 Of the 177 patients treated withHTA according to protocol, 167 wereevaluable at 12 months and 135 wereavailable for data collection at 3 years.At a year, bleeding was reduced tonormal or less in 127 of these patients(94%) with 72 (53%) experiencing ame-norrhea. Each of these results wassimilar to those for resectoscopic electro-desiccation; 91% and 46%, respectively.At 3 years, patient satisfaction was highfor the patients in both groups (98% forHTA; 97% resectoscopic endometrialelectrodesiccation) and hysterectomywas performed in 16 (9%) of the HTAgroup and 5 (6%) of the REA patients.There were 3 repeat ablations in eachgroup—2% of the HTA patients and 4%of the resectoscopic group.
The device has been evaluated in uterithat sound from 4 to 10.5 cm, but despitethe potential for treating abnormalendometrial cavities, the randomizedtrial included only patients without
Endometrial Ablation: Where Have We Been? Where are We Going? 749

intracavitary polyps or myomas. Tworetrospective studies have indicated thatwomen with intracavitary myomas mayhave outcomes similar to that womenwith normal cavities,98,99 but prospectivetrials will be necessary to confirm suchan impression. Regardless, because ofthese limitations, selection of appropri-ate patients requires preoperative assess-ment with one or a combination oftransvaginal ultrasound, saline infusionsonography, and/or hysteroscopy.
MICROWAVE
The use of microwave energy for per-forming NREA was initially published in1995.100 Microwaves occupy the part ofthe electromagnetic spectrum betweenradio and infrared waves and exert theireffect first by direct heating of tissue, andthen, in adjacent deeper layers, bythermal propagation. There are currently2 versions of the microwave endometrialablation (MEA) device, one reusable andone disposable (FemWave MicrosulisAmericas, Waltham, MA), each of whichcomprises a 8mm OD probe, calibratedto 15 cm, attached to a dedicated controlmodule by a reusable cable. The micro-wave frequency is 9.2GHz, the poweroutput 30W, and the local tissue isheated to about 901C, achieving anaggregate depth of tissue necrosis ofabout 5 to 6mm (direct plus indirect).The probe also contains an integratedthermal coupling device that transmitsinformation about adjacent tissuetemperature back to the control modulefor display on a screen. Activation andcontrol of the device is entirely in thehands of the surgeon. The device has thecapacity to treat uteri with a soundedcavity length of up to 14 cm, but, at thistime, there are limited data available forcavities that exceed 10 cm, a length thatis similar to that of other devices.Consequently, as is the case with othersystems, it is necessary to performultrasound, saline infusion sonography,
and or hysteroscopy to identify appro-priate patients for microwave ablation.
Patients may be treated with localanesthesia, conscious sedation, or usingregional or general anesthetics.101 Oncethe cervix is dilated and imaging (cur-rently with hysteroscopy) confirms thatthe hysteroscope is within the endome-trial cavity, and that the canal and cavityare intact (no partial or completeperforations), the microwave probe isinserted to the uterine fundus. When themeasured temperature of the tissuearound the probe reaches 301C, themachine is activated and the surgeonuses sweeping movements in the hori-zontal plane until a treatment tempera-ture threshold is reached (801C). Thenthe operator ‘‘covers’’ the entire endo-metrial surface in a preordained mannerfrom the fundus down, gradually with-drawing the device while maintaining thelocal tissue temperature within atreatment band centered around 801C.When the tip of the probe reaches anarea that approximates the location ofthe internal os, the device is deactivatedand the probe removed. Treatment timeis usually about 2 to 4 minutes.
The technique has been the subject anumber of high-quality randomized trials.The first RCT involved 263 women, wasperformed in Scotland, and comparedMEA to endometrial resection by expertsurgeons with outcomes published at 1,102
2,103 and 5 years.104 Surgical time wasshorter for those treated with microwaveablation and there were 2 intraoperativeperforations, one in each group, includingone emergency hysterectomy in a patientundergoing resection. In addition, bleed-ing requiring intraoperative tamponadeoccurred in 6 of the resection patients, oneof whom ultimately required readmissionand hysterectomy. No such complicationsoccurred in the microwave group. At 1year of follow-up, 116 of the 129 assignedto microwave ablation and 124 of the 134on whom endometrial resection was
750 Munro

performed were evaluable, with 3-quartersof each group satisfied with their outcomeat 12 months after treatment. At 5 years,236 of the original 263 women wereavailable for follow-up. Bleeding and painscores both were significantly reducedand amenorrhea rates were similar(MEA 65%; REA 69%), but thoseassigned MEA more likely to be satisfiedwith therapy than those who underwentREA (86% vs. 74%).
Another high-quality RCT was per-formed in North America comparedmicrowave ablation to REA by expertsurgeons using rollerball ablation.105 Inthis trial, 322 subjects were randomizedto either MEA or REA in a 2:1 alloca-tion scheme. Of the 215 patients allo-cated to MEA, 209 were treated withMEA with 194 evaluable at 1 year; of the107 designated for REA, 106 weretreated with 96 available for evaluationat 12 months. MEA treatment time was3.45 minutes whereas that for rollerballelectrodesiccation was 20.22 minutes.Unlike the Scottish randomized trial,there were no serious perioperativecomplications in either group of patients.At 12 months, and using intention totreat analysis, 87.0% and 83.2% of theMEA and REA groups had ‘‘successful’’outcomes (PBAC scores <75). If onlyevaluable cases were considered (ie, onlythose treated according to assignmentand evaluable at 12mo) the rate rose to96.4% and 92.7%, respectively. The rateof amenorrhea in evaluable patients was61.3% for MEA and 51.0% for theresectoscopic group. At 1 year, 98.5%of the women undergoing MEA and99.0% of those having REA were eithersatisfied or highly satisfied with theirtreatment.
This trial was unique in that it allowedsubjects with submucus myomas of up to3 cm diameter provided that they did notinterfere with the positioning of theprobe; such patients were available forsubgroup evaluation. This is a similar
diameter and configuration as thosereported in the Soysal et al106 study onTC balloon ablation. In the subgroupanalysis of these patients treated byMEA, success, amenorrhea and patientsatisfaction rates did not differ fromthose experienced by women withnormally configured endometrial cavitieswithout submucosal leiomyomas.
The previously described MEA trials,like those evaluating cryotherapy, bal-loon ablation, and free-heated fluid, allrequired that preoperative endometrialthinning be performed, either with suc-tion curettage (TC) or with GnRHagonists (microwave, free fluid, cryother-apy). The MEA device has also been thesubject of RCT comparing patientspretreated medically with those havingthe procedure performed without suchmedication, early in the proliferativephase of the cycle, when the endome-trium is very thin.101 In this trial of 210patients, the 12-month amenorrhea rateswere 55.9% in the early follicular phasegroup and 61.9% in the pretreatedgroup, and satisfaction was similar inthe 2 groups (92.5% early follicular;88.4% pretreatment). Utilization ofhealthcare resources was less in thepatients treated in the early follicularphase.
RF
The Novasure system (Cytyc Corpora-tion, Palo Alto, CA) is a NREA devicethat uses RF electricity to performautomated EA. The system is basedaround a single use 7.2mm OD probethat delivers a bipolar gold mesh elec-trode array attached to an expandableframe located at the distal end of thedevice. The electrode assembly alsocontains a cavity integrity testingsystem that is based on injection of afixed volume of CO2 after intrauterineplacement of the probe. The probe isattached to a dedicated microprocessor-based controller unit. The Novasure
Endometrial Ablation: Where Have We Been? Where are We Going? 751

device is restricted to cavities that arebetween 6 and 10 cm in length asmeasured from the external os to thefundus. An important feature of theNovaSure device is the fact that thetechnique allows performance of EAwithout mechanical or medical endo-metrial preparation.
Although most procedures are likelyperformed in operating theaters, EAwith the Novasure device has beenreported under local anesthesia withconscious sedation.107–109 After cervicaldilation to an appropriate diameter, andsounding of the length of the canal andendometrial cavity, the electrode assem-bly is inserted transcervically and themesh electrode deployed by retraction ofthe outer sleeve. This action results in theelectrodes assuming a triangular shapethat conforms to the surface of a normalendometrial cavity. The surgeon thenmeasures the intercornual distance usingan output device on the probe and entersthis value into the controller unit allow-ing the system to calculate the amount ofpower required for the specific uterus.Upon activation, the dedicated control-ler unit performs the uterine integritytest, and then, if successful, the unit isused to apply RF energy to the bipolarmesh simultaneously applying suction,thereby evacuating steam and carbonizeddebris. This process allows for electro-surgical vaporization and underlyingdesiccation in a relatively rapidfashion (approximately 80 to 90 s). Thedepth of this vaporization and desicca-tion varies—less in the cornual areas andmore in the fundus and body—and iscontrolled by the increasing tissueimpedance of the adjacent desiccatedtissue, shutting the system off when itexceeds 50O.
In the US trial, patients with leiomyo-mas or polyps less than 2 cm in diameterwere allowed, but there was no subgroupanalysis of patients with such lesions.108
Consequently, the efficacy of the
NovaSure device in the presence ofsubmucosal myomas, even under 2 cmin diameter, remains unknown. As aresult, patients with chronic HMB whoare potential candidates for the Nova-sure device require pretreatment imagingof the endometrial cavity with sonohys-terography or hysteroscopy.
The NovaSure device has beensubjected to prospective observationalstudies107,110 and a RCT, comparing thedevice with REA108 and other NREAtechniques.109,111 In the randomizedtrial, 265 subjects were enrolled at 9clinical centers in a 2:1 randomizationscheme. The REA procedure was differ-ent from all of the other US NREA trialsto date, as resection was used withsubsequent electrosurgical desiccationwith a rollerball electrode. Intraopera-tively, and despite the fact that REA wasperformed by expert surgeons, there were3 uterine perforations (3.3% of the totaltreated) versus none in the Novasuregroup. At 1 year, success, as defined bythe study (PBAC scores r75) wasexperienced by 88.3% of the Novasuretreated patients and 81.7% of thosein whom endometrial resection wasperformed. The amenorrhea rates at1 year were 41% for Novasure and35% for endometrial resection. In thefirst year there were 3 hysterectomiesin the Novasure group (1.3%) and 2 inthe REA cohort (2.2%). The 1-yearpatient satisfaction rates were alsosimilar with 92.8% of the Novasurepatients and 93.9% of the REA patientsreporting that they were satisfied orvery satisfied with the outcome. Trialscomparing Novasure to other NREAmethods are discussed later.
OTHER NREA TECHNIQUES
Diode LasersLow-power Nd:YAG lasers are underdevelopment for use in NREA systems.A Belgian study has reported initial and
752 Munro

1-year follow-up results using this tech-nique with outcomes similar to otherNREA technologies.112 The laser energy(wavelength 830 nm) was delivered to theendometrial cavity via a 6-mm OD probewith an expanded tripolar structure thatin appearance is similar to an intrauter-ine contraceptive device. Each of the 3poles delivers 5 to 7W of power forapproximately 7 minutes. The lasergenerator is very small in size, and, isconsidered to be less costly than previouslaser devices. However, at this time, dueto developmental difficulties with thedevice, it is not yet available.
Photodynamic TherapyThe potential application of photody-namic therapy for the treatment of HMBis being evaluated by a number ofinvestigators. Successful destruction ofendometrium with photosensitive agentshas been reported in rat, rabbit, andmonkey models.113–115 The systemic orlocal pretreatment of target tissues suchas endometrium with agents activated bymonochromatic light can produce a localcytotoxic effect. For each photosynthe-sizer molecule, a specific wavelength(usually laser light), accurately matchedto the absorption peak, must be usedto produce local tissue necrosis. Theactivated photosensitizer molecule isthought to react with tissue oxygenproducing singlet oxygen which is cyto-toxic. A preliminary pilot study of 16patients resulted in reduced uterinebleeding for 3 months that recurred overthe subsequent months.116 These systemsclearly need refinement before largerscale trials are justified.
Chemoablation of the EndometriumTopically administered caustic agentshave been used to destroy epitheliallesions such as those secondary tohuman papillomaviral infection. Suchan approach has been evaluated for theperformance of EA in patients with
HMB using 95% tricholoracetic acid,the same substance used for the topicaltreatment of exophytic human papillo-maviral infection.93,117 In these trials, thevolume of tricholoracetic acid was pre-determined based upon anticipated cav-ity volume, and the material was insertedinto the endometrial cavity via a 3mmdiameter catheter. The authors alsoreport on their laparotomy studies per-formed before the clinical trial thathelped confirm that intraperitoneal spillwas unlikely. In the randomized trial93
the objective was to determine the impactof pretreatment with GnRH agonist onoutcome. All patients enrolled weretreated in a procedure room, withoutanesthesia, and all went home the sameday. There were no reported proceduralcomplications. The 1-year amenorrhearates were 31.1% in the GnRH pretreat-ment group and 26.7% in the groupwithout pretreatment. Bleeding wasreduced or normal in 68.9% of thosewithout pretreatment and 66.7% ofthose with pretreatment. The authorsreport patient satisfaction at 93.3% and95.6% in the nonpretreated and pre-treated groups, respectively. If confirmedin other centers, this type of therapycould be somewhat revolutionary asoutcomes are similar to those of someof the NREA devices.
COMPARISONS OF ONE NREADEVICE TO ANOTHER
Although there are abundant trials com-paring REA to NREA techniques, therehas been a relative paucity of compara-tive studies involving 2 or more NREAdevices. In a review of the literature viaMEDLINE and the Cochrane Database,no comparative trials were found invol-ving the HTA device or the cryotherapysystem called ‘‘Her Option.’’ However,there were trials involving MEA,Novasure, and 2 of the balloonablation systems, TC and Cavaterm.
Endometrial Ablation: Where Have We Been? Where are We Going? 753

Two double blinded, RCTs have beenpublished comparing the RF bipolardevice, Novasure, to balloon ablationtechniques, one using Cavaterm90 andthe other with TC.111 The Cavaterm trialenrolled 57 women and randomized thanin a 2:1 schema favoring Novasure.Those assigned to the Novasure grouphad no preoperative preparation of theendometrium whereas those treated withthe Cavaterm balloon had preoperativemechanical preparation of the endome-trium with suction currettage. The resultsat 1 year confirmed that both interven-tions were effective but showed thatalthough amenorrhea was more likelywith Novasure (43% to 11%) the chanceof failing with Novasure was higher thanfor Cavaterm (13% to 0%). The authorsnote that there were problems with thegenerator unit in 3 of the 5 womenundergoing Novasure ablation who wenton to have hysterectomy. There were nohysterectomies in the follow-up period inthe Cavaterm group.
The RCT comparing Novasure andthe original TC device also followed a 2:1randomization scheme with 83 of the 126subjects assigned to Novasure and 43 tothe thermal balloon. Similar to theCavaterm versus Novasure trial des-cribed above, the TC patients underwentpreprocedural mechanical thinning ofthe endometrium with suction curret-tage. There was also a generator problemencountered with the Novasure control-ler unit that was not discovered until 44subjects had been treated. The generatorwas replaced and enrollment into thetrial continued with clinical outcomesreported considering both the entiretreatment cohort (intent to treat analy-sis) and by including only the patientswho were randomized after replacementof the generator. The patients werefollowed to 12 months postprocedureusing PBAC as the primary outcome.The rate of amenorrhea in the entirecohort in the Novasure group was 43%
(34/83) and for those assigned to TC 3%(3/43). When the patients treated beforechanging the generator were excluded,56% of those treated with Novasureexperienced amenorrhea, a proportionthat is consistent with the results ob-tained in other RCTs. For both treat-ment groups, therapy was generallysuccessful as the mean PBAC scoresreduced to the normal range, butthe magnitude of the decrease wassignificantly greater for the Novasuregroup. There were 4 hysterectomies ineach group in the 12-month follow-upinterval.
As previously mentioned, the Meno-treat device has been compared withCavaterm in a relatively small RCT withonly short-term follow-up with similarclinical outcomes.79 Balloon ablation hasalso been compared with MEA with theMEA device in a cost modeling exercisebased upon existing data.118 The conclu-sions of this group were that thermalballoon ablation and MEA were similarwith respect to overall resource utiliza-tion and that both were much lessexpensive than hysterectomy.
USE OF NREA DEVICES IN AN OFFICESETTING UNDER LOCAL ANESTHESIA
As noted above, in RCTs, clinical out-comes associated with NREA systemsare similar to those achieved by expertsurgeons performing REA by one or acombination of rollerball electrodesicca-tion and transcervical resection. How-ever, the per case device costs of NREAdevices are substantial (approximately$1000 US in 2006), an amount that ismuch greater than the combination ofdisposable and amortized per case costsof REA. Although optimal clinical out-comes and minimal complications withREA are achieved with expert surgeons,a wider spectrum of endometrial cavitiescan be treated because of the limitationsinherent in the design of NREA systems.Consequently, maximal value of NREA
754 Munro

devices will only be achieved when theirsafety and simplicity is applied in envi-ronments that are less resource intensethan standard operating rooms as evi-dence already exists demonstrating thatlocal anesthesia in standard operatingrooms is unlikely to reduce costs.119
Ideally, to minimize risk and the needfor the personnel and equipmentrequired for conscious sedation, NREAwould be performed in an office proce-dure room setting without the need forparenteral systemic analgesics or anxio-lytics. However, provided such resourcesare available, office-based conscioussedation would likely be less resourceintense and therefore, less expensivethan a traditional operating room or‘‘surgicenter.’’
The only clinical trial of ‘‘localanesthesia’’ has compared Novasure toTC in a prospective, multicenter, non-randomized evaluation of intraoperativepain in 67 patients who also receivedstandardized intravenous sedation withfentanyl citrate.109 Thirty-seven of thepatients self selected the Novasure devicewhereas the other 30 chose to be treatedwith TC. The primary outcomes werenumeric and visual analog scales thatpurport to show both higher proceduralpain scores for TC patients and a longerduration of procedural pain consistentwith procedure time—approximately 1.5minutes for Novasure versus 8 minutesfor TC. Notably absent from this studydesign was a description of the locationof the procedures which may have beenperformed in standard operating rooms.There was also no specific evaluation ofthe pain experienced by the patientsduring dilation of the cervix which couldimpact the overall results. Finally, only asingle pain score was obtained for theprocedure and the investigators took theliberty to multiply that pain score timesthe duration of the procedure, plottingthe imputed results on a graph that couldbe interpreted as being created from
serial data points, in stead of one.Consequently, and unfortunately, theresults of this study may not reflect thetotal picture of pain associated withthese 2 modalities and, consequently,notwithstanding the use of fentanyl, itis difficult to use these results toevaluate applicability to the officeenvironment.
There are a number of published seriesthat have reported the use of singleNREA systems using local anesthesia.Hydrothermablation has been investi-gated in 2 published series using theoffice without requirement for parenteralanxiolytics or analgesics.120,121 In onestudy, performed in the NorthernCalifornia Kaiser system, 54 patients weretreated using preoperative oral agentsincluding hydrocodone-acetominophenand intramuscular ketorolac and atro-pine. The procedure was then performedusing intracervical mepivicaine. All pa-tients were apparently treated successfullyin the office environment but no pain orsatisfaction scores were provided. In theother series, from the United Kingdom,the only preoperative medication wasmefenamic acid and the only proceduralanesthesia was provided with a 1%lidocaine adrenaline solution injected in-tracervically and paracervically. Thesepatients were selected based on preferenceand were usually parous, but all proce-dures were completed with maximummedian pain scores of 6.4 (Range 4.0 to8.9).
MEA has been evaluated in thecontext of a RCT comparing patientstreated under ‘‘local’’ anesthesia withgeneral anesthetic.122 Although localanesthesia was generally well accepted,procedures were performed in the formaloperating ‘‘theater’’ regardless of thetype of anesthesia assigned/performed.In this trial there were no cost savingswhen MEA was performed under localanesthesia, but, in a cost modelingexercise published subsequent to the
Endometrial Ablation: Where Have We Been? Where are We Going? 755

original study, predicted per case savingswould be significant.119
Studies evaluating the use of balloonNREA (TC) have showed that theprocedure may be accomplished success-fully in the office setting. A series of 20women were treated in an office settinghaving received a diclofenac suppository1 hour preoperatively and a paracervicalblock with 10mL of 1% bupivicaine.One patient was nulliparous, all weresuccessfully treated with a median visualanalog scale (0 to 10) score of 4.0 (0.1 to9.9), and all left the clinic within 65minutes of the procedure.123 In anotherstudy of 27 women, 14 were treated,under an institutional review board-approved protocol, without any prepro-cedural anesthesia, then, the subsequentcohort of 13 women underwent TCNREA after taking 3 600-mg ibupro-phen tablets at predetermined intervalsbefore the procedure. In each of these 2groups of patients, 1 case was abandonedbecause of inability to dilate the cervicalcanal, and 1 woman in the nonpremedi-cated group terminated the proceduremidway through. Dilation and treatmentscores were similar but those withoutibuprofen pretreatment requested ‘‘rescueanalgesia,’’ usually with nitrous oxide, in4 instances, features that confound thepain scores recorded. Nausea and vomit-ing after the procedure seemed to be lessfrequently encountered in the pretreatedgroup.
There have been no published studiesexpressly oriented to the evaluation ofcryoablation with the Her Option device.However, in the RCT performed for thepurposes FDA approval the patientsundergoing EA were stratified accordingto the method of anesthesia/analgesisused for the index procedure.124
Although the method of reporting makesit difficult to determine which patientscould be treated in an office situation,about 10% of the cohort had only localanesthesia whereas about 40% had a
combination of local anesthesia andconscious sedation.
From the studies discussed in thepreceding paragraphs, it is apparent thatperformance of NREA in the officesetting is feasible, at least for themajority of the systems in selectedpatients. However, it seems that at leastsome anesthesia is optimal and that thefull potential of local anesthetics, con-sidering the differences in innervation ofthe corpus and cervix, has not been fullyexploited; the design of future studiesshould be undertaken with this inmind.122 The use of conscious sedationis problematic for many practitionersconsidering use of NREA in an officesetting, because of the prerequisites forappropriately trained staff and monitor-ing equipment. Nevertheless, changes inUS reimbursement policy allowing sur-geons to bill for technical fees associatedwith NREA may stimulate a greaterdegree of development and criticalanalysis in this area.
COMPARISONS OF NREA DEVICETO INTRAUTERINE PROGESTINRELEASING SYSTEMS
Early high-quality trials involving theLNG-IUS demonstrated that hypo-menorrhea and even amenorrhea werecommon events.125 A subsequent rando-mized trial of women on a waiting list forHMB resulted in 64.3% of those as-signed to the progestin IUD cancelingsurgery compared with 14.3% of thosewho remained on oral medical ther-apy.126 These and other studies suggesteda place for the LNG-IUS in the manage-ment of HMB.
There have been 2 RCTs comparingthe LNG-IUS to REA performed byexpert surgeons, each with somewhatsimilar results.127,128 In the Italian trialwith a total of 70 patients, 12-monthresults were similar with objectivelymeasured blood loss being reduced by79% in the LNG-IUS group and 89%
756 Munro

for those assigned to endometrial resec-tion; there were also high-satisfactionscores and similar rates of amenorrhea/hypomenorrhea in the 2 groups.127 Inthe Norwegian trial comparing 30women assigned the LNG-IUS and 29treated by REA, both groups experi-enced significant blood loss, althoughmore patients in the REA group than theLNG-IUS group attained treatment suc-cess (90% for REA; 69% for LNG-IUS).The 3-year results of this trial suggestthat, if anything, the outcomes remaingenerally successful and become moresimilar with time.129 Given that the REAprocedures in these trials were performedby surgeons with extensive experience,one could infer that in general use, theLNG-IUS results would more likely besimilar to, if not better than thoseachieved by resectoscopic technique.
There now exist a number ofwell-designed studies comparing theLNG-IUS with various NREA devices.TC balloon ablation has been comparedwith the LNG-IUS system called Mirena(Berlex, Montville, NJ).130 In this rando-mized trial, 36 patients received thelevonorgestrel device whereas 36 wereallocated to receive balloon ablationafter undergoing medical pretreatmentwith the gonadotropin releasing hor-mone agonist goserelin (Zoladex). At 12months, both interventions were success-ful, with pretreatment and 12-monthPBAC scores of 417 (±81.4) and 21.8(±14.0) for balloon ablation and 408(±101.0) and 55.0 (±1.5) for thelevonorgestrel device. Quality of lifescores were not quite as high in thelevonorgestrel group in some sections ofthe assessment but similar in most. Inanother RCT from New Zealand, 79women were randomized to the LNG-IUS or TC balloon ablation and fol-lowed periodically for at least 2 years.131
In this trial the PBAC scores were lowerin the IUS group, and the amenorrhearates were higher, but there were no
differences in patient satisfaction andhealth-related quality of life scales. Abla-tion with the MEA device was comparedwith the LNG-IUS in a retrospectivestudy of 62 patients published in 2002.132
Both interventions were effective with anaverage follow-up of 14 months andthere were no differences in effectiveness,acceptability, or quality of life outcomes.A recent modified Cochrane systematicreview has compared the randomizedtrials involving oral medical therapy, theLNG-IUS, REA, and hysterectomy.133
Aside from noting that oral therapy suitsonly a minority of women long term, theLNG-IUS, REA, and hysterectomy wereall equivalent with respect to satisfactionand quality of life outcomes.
It is evident that the progestin releas-ing IUS is a compelling competitor forEA, whether it is performed by resecto-scopic technique or using one ofthe nonresectoscopic systems discussedabove. Convenience and cost are 2important factors. The device can almostalways be inserted in a relatively briefoffice visit rather than in the context ofan operating room, such as is the case forresectoscopic ablation. It is less expen-sive than a NREA device at least atpresent, although a single LNG-IUSdevice has a limited period of efficacythat will be no longer than 5 years.Repeated insertions would erode costadvantages associated with LNG-IUSuse.
SummaryEA was originally developed for patientssuffering from disabling HMB with nodesire for future fertility, and who werepoor surgical candidates for hysterec-tomy. However, provided fertility is notan issue, EA is now an option forotherwise healthy women who havefailed or refused medical intervention orin whom medical treatments are not welltolerated. High-quality evidence suggests
Endometrial Ablation: Where Have We Been? Where are We Going? 757

that for appropriately selected patientsthese ablative procedures typically re-duce menstrual blood flow significantly,and may decrease the severity of otherassociated symptoms. In expert hands,both REA and NREA techniques seemto result in similar degrees of patientsatisfaction and failure rates. However, itis clear from longer-term trials, thatalthough most women are initially satis-fied, many subsequently choose or re-quire either repeat EA or hysterectomy.The reasons for these treatment failuresare still not clear and deserve furtherstudy. For example, it is possible thatthose with anovulatory HMB might beless likely to find satisfaction with EAthan those women with ovulatory bleed-ing. Alternatively, given the apparentprevalence of otherwise occult vonWillebrand disease, it is possible thatsome if not many of the ‘‘failures’’ maybe related to undiscovered cases ofcoagulopathy.
The training, required operative en-vironment, and complications associatedwith REA were collective stimuli for thedevelopment of the plethora of nonre-sectoscopic techniques now available fortreating HMB. Clearly, with normal ornear normal endometrial cavities, thesetechniques have similar outcomes bothto each other and to the resectoscopictechniques. In addition, in each com-parative trial, there seem to be fewerserious or potentially serious complica-tions such as uterine perforation or fluidoverload when NREA techniques areused as compared with resectoscopictechniques. It should also be appreciatedthat in the clinical trials, expert resec-tionists are performing the procedures—available evidence suggests that REA—associated complications may occurmore frequently when the procedure isperformed by the general population ofgynecologists. Nevertheless, it is appar-ent from the FDA’s Manufacturer andUser Facility Device Experience data-
base, the NREA techniques are notexempt from serious complications asuterine perforation and bowel injury hasbeen reported in association with each ofthe approved devices.
There are other limitations to currentNREA technology. To a greater or lesserextent, each NREA system has limita-tions related to one or a combination ofthe size and configuration of the endo-metrial cavity that prevents generalapplication of any device to the HMBpopulation. From the available data, it isapparent that the MEA device has beensubjected to rigorous analysis in thelargest spectrum of endometrial cavitysize and myoma-related cavity distor-tion. However, both the HydroTherma-blator and at least the TC balloon havepublished data demonstrating efficacy inthe presence of type II myomas 3 cm orless in diameter, and it is possible thatthe Novasure and Her Option devicesare effective in a larger spectrum ofendometrial cavity configurations thanwere included in the available clinicaltrials. However, despite these consi-derations, there exist a number ofwomen who wish EA who will not becandidates for any of the devices andwho may be better served with resecto-scopic techniques. Consequently, havingindividuals with expertise in these tech-niques is still important for healthcaresystems.
There seems to be a clear need formore rigorous evaluation of the resourceutilization associated with EA in generalcompared with hysterectomy, and forREA compared with NREA. TheAberdeen experience suggests that directcosts of EA may be greater thanhysterectomy if patients are followedlong enough after their index procedure.However, despite this, for many women,indirect costs of EA may still be muchless than for hysterectomy, and thereforemay be a significant factor to be con-sidered as they make their choice. For
758 Munro

example, the self-employed lawyer withHMB will be back earning money soonerif she has an EA instead of a hyster-ectomy, and that even if an additionalEA is required in a few years, the neteconomic impact to her will be less thanhysterectomy. Such indirect economicadvantages may not be so significantfor women of lower socioeconomicstatus.
From available data, it could besurmised that most patients undergoingNREA are still being treated in resource-intensive surgical environments liketraditional operating theaters. Wherethis is the case, the single use costsassociated with NREA could actuallyincrease the cost of providing the proce-dure, because per-use costs of resecto-scopes are relatively low. It seemsincumbent on investigators and health-care delivery systems to collaborate in afashion that would shed more light onthis issue.
The addition of the levonorgestrelreleasing IUS to the list of medicalinterventions has added a new dimensionto the therapeutic armamentarium. Notonly does the device seem to offer similarsuccess rates for the treatment of heavyuterine bleeding (at least in the absence ifintrauterine lesions) but it preserves theoption of future fertility and is aprocedure that can virtually always beaccomplished in an office setting withrelatively little surgeon training.
Ultimate judgment of the value of EAawaits the results of more of carefullycrafted long-term longitudinal studiesthat compare the economic, social, andmedical benefits of hysterectomy to EAfor the treatment of AUB.
References1. Bardenheuer FH. Elektrokoagulation
der Uterusschleimhaut zur Behandlungklimakterischer Blutungen. Zentralblattfur Gynakol. 1937;4:209–211.
2. Cahan WG, Brockunier A Jr. Cryosur-gery of the uterine cavity. Am J ObstetGynecol. 1967;99:138–153.
3. Droegemueller W, Greer BE, Makows-ki EL. Preliminary observations ofcryocoagulation of the endometrium.Am J Obstet Gynecol. 1970;107:958–961.
4. Droegemueller W, Greer B,Makowski E. Cryosurgery in patientswith dysfunctional uterine bleeding.Obstet Gynecol. 1971;38:256–258.
5. Goldrath MH, Fuller TA, Segal S.Laser photovaporization of endome-trium for the treatment of menorrhagia.Am J Obstet Gynecol. 1981;140:14–19.
6. DeCherney A, Polan ML. Hystero-scopic management of intrauterinelesions and intractable uterine bleeding.Obstet Gynecol. 1983;61:392–397.
7. Abel MH, Baird DT. The effect of 17beta-estradiol and progesterone onprostaglandin production by humanendometrium maintained in organculture. Endocrinology. 1980;106:1599–1606.
8. Lumsden MA, Brown A, Baird DT.Prostaglandin production from homo-genates of separated glandular epithe-lium and stroma from humanendometrium. Prostaglandins. 1984;28:485–496.
9. Sugino N, Karube-Harada A, TaketaniT, et al. Withdrawal of ovarian steroidsstimulates prostaglandin F2alpha pro-duction through nuclear factor-kappaBactivation via oxygen radicals in humanendometrial stromal cells: potentialrelevance to menstruation. J ReprodDev. 2004;50:215–225.
10. Rees MC, Parry DM, Anderson AB,et al. Immunohistochemical locali-sation of cyclooxygenase in thehuman uterus. Prostaglandins. 1982;23:207–214.
11. Word RA, Kamm KE, Casey ML.Contractile effects of prostaglandins,oxytocin, and endothelin-1 in humanmyometrium in vitro: refractorinessof myometrial tissue of pregnantwomen to prostaglandins E2 and F2alpha. J Clin Endocrinol Metab. 1992;75:1027–1032.
Endometrial Ablation: Where Have We Been? Where are We Going? 759

12. Ohbuchi H, Nagai K, Yamaguchi M,et al. Endothelin-1 and big endothelin-1increase in human endometrium duringmenstruation. Am J Obstet Gynecol.1995;173:1483–1490.
13. Lockwood CJ, Krikun G, HausknechtVA, et al. Matrix metalloproteinaseand matrix metalloproteinase inhibitorexpression in endometrial stromal cellsduring progestin-initiated decidualiza-tion and menstruation-related proges-tin withdrawal. Endocrinology. 1998;139:4607–4613.
14. Marbaix E, Kokorine I, Moulin P,et al. Menstrual breakdown of humanendometrium can be mimicked in vitroand is selectively and reversibly blockedby inhibitors of matrix metalloprotei-nases. Proc Natl Acad Sci USA.1996;93:9120–9125.
15. Dong JC, Dong H, Campana A, et al.Matrix metalloproteinases and theirspecific tissue inhibitors in menstrua-tion. Reproduction. 2002;123:621–631.
16. Cameron IT, Campbell S. Nitric oxidein the endometrium. Hum ReprodUpdate. 1998;4:565–569.
17. Tschugguel W, Schneeberger C,Unfried G, et al. Elevation of induciblenitric oxide synthase activity in humanendometrium during menstruation.Biol Reprod. 1999;60:297–304.
18. Hofmann GE, Rao CV, De Leon FD,et al. Human endometrial prostaglan-din E2 binding sites and their profilesduring the menstrual cycle and inpathologic states. Am J Obstet Gynecol.1985;151:369–375.
19. Levin JH, Stanczyk FZ, Lobo RA.Estradiol stimulates the secretion ofprostacyclin and thromboxane fromendometrial stromal cells in culture.Fertil Steril. 1992;58:530–536.
20. Smith SK, Abel MH, Kelly RW, et al.Prostaglandin synthesis in the endome-trium of women with ovular dysfunc-tional uterine bleeding. Br J ObstetGynaecol. 1981;88:434–442.
21. Cameron IT, Leask R, Kelly RW, et al.Endometrial prostaglandins in womenwith abnormal menstrual bleeding.Prostaglandins Leukot Med. 1987;29:249–257.
22. Makarainen L, Ylikorkala O. Primaryand myoma-associated menorrhagia:role of prostaglandins and effects ofibuprofen. Br J Obstet Gynaecol.1986;93:974–978.
23. Willman EA, Collins WP, Clayton SG.Studies in the involvement of prosta-glandins in uterine symptomatologyand pathology. Br J Obstet Gynaecol.1976;83:337–341.
24. Adelantado JM, Rees MC, LopezBernal A, et al. Increased uterineprostaglandin E receptors in menor-rhagic women. Br J Obstet Gynaecol.1988;95:162–165.
25. Kadir RA, Economides DL, Sabin CA,et al. Frequency of inherited bleedingdisorders in women with menorrhagia.Lancet. 1998;351:485–489.
26. Shankar M, Lee CA, Sabin CA, et al.von Willebrand disease in women withmenorrhagia: a systematic review.BJOG. 2004;111:734–740.
27. Rybo G. Plasminogen activators in theendometrium. II. Clinical aspects. Var-iation in the concentration of plasmi-nogen activators during the menstrualcycle and its relation to menstrualblood loss. Acta Obstet Gynecol Scand.1966;45:429–450.
28. Gleeson N, Devitt M, Sheppard BL,et al. Endometrial fibrinolytic enzymesin women with normal menstruationand dysfunctional uterine bleeding. BrJ Obstet Gynaecol. 1993;100:768–771.
29. Gleeson NC, Buggy F, Sheppard BL,et al. The effect of tranexamic acidon measured menstrual loss andendometrial fibrinolytic enzymes in dys-functional uterine bleeding. Acta ObstetGynecol Scand. 1994;73:274–277.
30. Lethaby A, Farquhar C, Cooke I.Antifibrinolytics for heavy menstrualbleeding. Cochrane Database Syst Rev.2000;CD000249.
31. Zervou S, Klentzeris LD, Old RW.Nitric oxide synthase expression andsteroid regulation in the uterus ofwomen with menorrhagia. Mol HumReprod. 1999;5:1048–1054.
32. Marsh MM, Malakooti N, Taylor NH,et al. Endothelin and neutral endopep-tidase in the endometrium of women
760 Munro

with menorrhagia. Hum Reprod. 1997;12:2036–2040.
33. Smith SK, Abel MH, Kelly RW, et al.The synthesis of prostaglandins frompersistent proliferative endometrium. JClin Endocrinol Metab. 1982;55:284–289.
34. Vancaillie TG. Electrocoagulation ofthe endometrium with the ball-endresectoscope. Obstet Gynecol. 1989;74:425–427.
35. Vercellini P, Oldani S, DeGiorgi O,et al. Endometrial ablation with avaporizing electrode in women withregular uterine cavity or submucousleiomyomas. J Am Assoc GynecolLaparosc. 1996;3:S52.
36. Glasser MH. Endometrial ablation andhysteroscopic myomectomy by electro-surgical vaporization. J Am AssocGynecol Laparosc. 1997;4:369–374.
37. Vercellini P, Oldani S, Yaylayan L,et al. Randomized comparison ofvaporizing electrode and cuttingloop for endometrial ablation. ObstetGynecol. 1999;94:521–527.
38. Sowter MC, Singla AA, Lethaby A.Pre-operative endometrial thinningagents before hysteroscopic surgeryfor heavy menstrual bleeding. CochraneDatabase Syst Rev. 2000;CD001124.
39. Sculpher M, Thompson E, Brown J,et al. A cost effectiveness analysis ofgoserelin compared with danazol asendometrial thinning agents. BJOG.2000;107:340–346.
40. Gannon MJ, Holt EM, Fairbank J,et al. A randomised trial comparingendometrial resection and abdominalhysterectomy for the treatmentof menorrhagia. BMJ. 1991;303:1362–1364.
41. Dwyer N, Hutton J, Stirrat GM.Randomised controlled trial comparingendometrial resection with abdominalhysterectomy for the surgical treatmentof menorrhagia. Br J Obstet Gynaecol.1993;100:237–243.
42. Pinion SB, Parkin DE, AbramovichDR, et al. Randomised trial of hyster-ectomy, endometrial laser ablation, andtranscervical endometrial resection fordysfunctional uterine bleeding. BMJ.1994;309:979–983.
43. O’Connor H, Broadbent JA, MagosAL, et al. Medical Research Councilrandomised trial of endometrial resec-tion versus hysterectomy in manage-ment of menorrhagia. Lancet. 1997;349:897–901.
44. Crosignani PG, Vercellini P, ApoloneG, et al. Endometrial resection versusvaginal hysterectomy for menorrhagia:long-term clinical and quality-of-lifeoutcomes. Am J Obstet Gynecol. 1997;177:95–101.
45. Dickersin K, Munro MG, LangenbergPftS-DWG. Surgical TreatmentsOutcomes Project for DysfunctionalUterine Bleeding (STOP-DUB): Designand methods. Control Clin Trials.2003;24:591–609.
46. Lethaby A, Shepperd S, Cooke I, et al.Endometrial resection and ablationversus hysterectomy for heavy menstru-al bleeding. Cochrane Database SystRev. 2000;CD000329.
47. Lethaby A, Hickey M. Endometrialdestruction techniques for heavy mens-trual bleeding: a Cochrane review. HumReprod. 2002;17:2795–2806.
48. Sculpher M. The cost-effectiveness ofpreference-based treatment allocation:the case of hysterectomy versusendometrial resection in the treatmentof menorrhagia. Health Econ. 1998;7:129–142.
49. Anonymous. A randomised trial ofendometrial ablation versus hysterect-omy for the treatment of dysfunctionaluterine bleeding: outcome at four years.Aberdeen Endometrial Ablation TrialsGroup. Br J Obstet Gynaecol. 1999;106:360–366.
50. Weber AM, Munro MG. Endometrialablation versus hysterectomy: STOP-DUB. Medscape Womens Health. 1998;3:3.
51. Bhattacharya S, Cameron IM, ParkinDE, et al. A pragmatic randomisedcomparison of transcervical resectionof the endometrium with endometriallaser ablation for the treatment ofmenorrhagia. Br J Obstet Gynaecol.1997;104:601–607.
52. Jansen FW, Vredevoogd CB, vanUlzen K, et al. Complications of
Endometrial Ablation: Where Have We Been? Where are We Going? 761

hysteroscopy: a prospective, multicen-ter study. Obstet Gynecol. 2000;96:266–270.
53. Overton C, Hargreaves J, Maresh M. Anational survey of the complications ofendometrial destruction for menstrualdisorders: the MISTLETOE study.Minimally Invasive Surgical Techni-ques—Laser, EndoThermal or Endor-escetion. Br J Obstet Gynaecol. 1997;104:1351–1359.
54. Istre O, Skajaa K, Schjoensby AP, et al.Changes in serum electrolytes aftertranscervical resection of endometriumand submucous fibroids with use ofglycine 1.5% for uterine irrigation.Obstet Gynecol. 1992;80:218–222.
55. Kim AH, Keltz MD, Arici A, et al.Dilutional hyponatremia during hystero-scopic myomectomy with sorbitol-mannitol distention medium. J AmAssoc Gynecol Laparosc. 1995;2:237–242.
56. Taskin O, Buhur A, Birincioglu M,et al. Endometrial Na+ , K+-ATPasepump function and vasopressin levelsduring hysteroscopic surgery in patientspretreated with GnRH agonist. J AmAssoc Gynecol Laparosc. 1998;5:119–124.
57. Isaacson K, Nardella P. Developmentand use of a bipolar resectoscope inendometrial electrosurgery. J Am AssocGynecol Laparosc. 1997;4:385–391.
58. Vilos GA. Intrauterine surgery using anew coaxial bipolar electrode in normalsaline solution (Versapoint): a pilotstudy. Fertil Steril. 1999;72:740–743.
59. Donnez J, Vilos G, Gannon MJ, et al.Goserelin acetate (Zoladex) plusendometrial ablation for dysfunctionaluterine bleeding: a large randomized,double-blind study. Fertil Steril.1997;68:29–36.
60. Goldenberg M, Zolti M, Bider D, et al.The effect of intracervical vasopressinon the systemic absorption of glycineduring hysteroscopic endometrialablation. Obstet Gynecol. 1996;87:1025–1029.
61. Townsend DE, McCausland V,McCausland A, et al. Post-ablation-tubal sterilization syndrome. ObstetGynecol. 1993;82:422–424.
62. McCausland AM, McCausland VM.Frequency of symptomatic cornualhematometra and postablation tubalsterilization syndrome after total roller-ball endometrial ablation: a 10-yearfollow-up. Am J Obstet Gynecol. 2002;186:1274–1280; discussion 1280–1283.
63. Pooley AS, Ewen SP, Sutton CJ. Doestranscervical resection of the endome-trium for menorrhagia really avoidhysterectomy? Life table analysis of alarge series. J Am Assoc GynecolLaparosc. 1998;5:229–235.
64. Seidman DS, Bitman G, Mashiach S,et al. The effect of increasing age on theoutcome of hysteroscopic endometrialresection for management of dysfunc-tional uterine bleeding. J Am AssocGynecol Laparosc. 2000;7:115–119.
65. McCausland V, McCausland A. Theresponse of adenomyosis to endome-trial ablation/resection. Hum ReprodUpdate. 1998;4:350–359.
66. Bae IH, Pagedas AC, Barr CA, et al.Retrospective analysis of 305 consecu-tive cases of endometrial ablationand partial endomyometrial resection.J Am Assoc Gynecol Laparosc. 1996;3:549–554.
67. Browne DS. Endometrial resection—acomparison of techniques. Aust N Z JObstet Gynaecol. 1996;36:448–452.
68. Eskandar MA, Vilos GA, Aletebi FA,et al. Hysteroscopic endometrial abla-tion is an effective alternative to hyster-ectomy in women with menorrhagiaand large uteri. J Am Assoc GynecolLaparosc. 2000;7:339–345.
69. Valle RF, Baggish MS. Endometrialcarcinoma after endometrial ablation:high-risk factors predicting its occur-rence. Am J Obstet Gynecol. 1998;179:569–572.
70. Gurtcheff SE, Sharp HT. Complica-tions associated with global endo-metrial ablation: the utility of theMAUDE database. Obstet Gynecol.2003;102:1278–1282.
71. Singer A, Almanza R, Gutierrez A,et al. Preliminary clinical experiencewith a thermal balloon endometrialablation method to treat menorrhagia.Obstet Gynecol. 1994;83:732–734.
762 Munro

72. Neuwirth RS, Duran AA, Singer A,et al. The endometrial ablator: a newinstrument. Obstet Gynecol. 1994;83:792–796.
73. Friberg B, Ahlgren M. Balloon catheterendometrial thermotherapy in menor-rhagia. New simple and safe alternativeto hysterectomy. Lakartidningen. 1999;96:4179–4181.
74. Friberg B, Ahlgren M. Thermalballoon endometrial destruction: theoutcome of treatment of 117 womenfollowed up for a maximum period of4 years. Gynecol Endosc. 2000;9:389–395.Abstract.
75. El-Toukhy T, Chandakas S, Grigoria-dis T, et al. Outcome of the first 220cases of endometrial balloon ablationusing Cavaterm plus. J ObstetGynaecol. 2004;24:680–683.
76. Hawe JA, Phillips AG, Chien PF, et al.Cavaterm thermal balloon ablation forthe treatment of menorrhagia. Br JObstet Gynaecol. 1999;106:1143–1148.
77. Mettler L. Long-term results in thetreatment of menorrhagia and hyper-menorrhea with a thermal balloonendometrial ablation technique. JSLS.2002;6:305–309.
78. Ulmsten U, Carstensen H, Falconer C,et al. The safety and efficacy of Meno-Treat, a new balloon device for thermalendometrial ablation. Acta ObstetGynecol Scand. 2001;80:52–57.
79. Vihko KK, Raitala R, Taina E.Endometrial thermoablation for treat-ment of menorrhagia: comparison oftwo methods in outpatient setting.Acta Obstet Gynecol Scand. 2003;82:269–274.
80. Mangeshikar PS, Kapur A, Yackel DB.Endometrial ablation with a newthermal balloon system. J Am AssocGynecol Laparosc. 2003;10:27–32.
81. McAllister KF, Bigrigg A. Uterineballoon therapy for menorrhagia: afeasibility study of its use in thecommunity setting. J Fam PlannReprod Health Care. 2002;28:133–134.
82. Marsh F, Thewlis J, Duffy S. Therma-choice endometrial ablation in the out-patient setting, without local anesthesiaor intravenous sedation: a prospective
cohort study. Fertil Steril. 2005;83:715–720.
83. Meyer WR, Walsh BW, Grainger DA,et al. Thermal balloon and rollerballablation to treat menorrhagia: a multi-center comparison. Obstet Gynecol.1998;92:98–103.
84. Grainger DA, Tjaden BL, Rowland C,et al. Thermal balloon and rollerballablation to treat menorrhagia: two-yearresults of a multicenter, prospective,randomized, clinical trial. J Am AssocGynecol Laparosc. 2000;7:175–179.
85. Loffer FD. Three-year comparison ofthermal balloon and rollerball ablationin treatment of menorrhagia. J AmAssoc Gynecol Laparosc. 2001;8:48–54.
86. Loffer FD, Grainger D. Five-yearfollow-up of patients participating in arandomized trial of uterine balloontherapy versus rollerball ablation fortreatment of menorrhagia. J Am AssocGynecol Laparosc. 2002;9:429–435.
87. van Zon-Rabelink IA, Vleugels MP,Merkus HM, et al. Endometrial abla-tion by rollerball electrocoagulationcompared to uterine balloon thermalablation. Technical and safety aspects.Eur J Obstet Gynecol Reprod Biol.2003;110:220–223.
88. van Zon-Rabelink IA, Vleugels MP,Merkus HM, et al. Efficacy and satis-faction rate comparing endometrialablation by rollerball electrocoagula-tion to uterine balloon thermal ablationin a randomised controlled trial.Eur J Obstet Gynecol Reprod Biol. 2004;114:97–103.
89. Amso NN, Stabinsky SA, McFaul P,et al. Uterine thermal balloon therapyfor the treatment of menorrhagia: thefirst 300 patients from a multi-centrestudy. International CollaborativeUterine Thermal Balloon WorkingGroup. Br J Obstet Gynaecol. 1998;105:517–523.
90. Abbott J, Hawe J, Hunter D, et al. Adouble-blind randomized trial compar-ing the Cavaterm and the NovaSureendometrial ablation systems for thetreatment of dysfunctional uterinebleeding. Fertil Steril. 2003;80:203–208.
Endometrial Ablation: Where Have We Been? Where are We Going? 763

91. Soysal ME, Soysal SK, Vicdan K.Thermal balloon ablation in myoma-induced menorrhagia under localanesthesia. Gynecol Obstet Invest.2001;51:128–133.
92. Pittrof R, Majid S, Murray A. Trans-cervical endometrial cryoablation(ECA) for menorrhagia. Int J GynaecolObstet. 1994;47:135–140.
93. Kucuk M, Okman TK. Intrauterineinstillation of trichloroacetic acid iseffective for the treatment of dysfunc-tional uterine bleeding. Fertil Steril.2005;83:189–194.
94. Duleba AJ, Heppard MC, SoderstromRM, et al. Randomized study compar-ing endometrial croyoablation and roll-erball electroablation for treatmentof dysfunctional uterine bleeding.J Am Assoc Gynecol Laparosc.2003;10:17–26. Abstract.
95. Townsend DE, Duleba AJ, WilkesMM. Durability of treatment effectsafter endometrial cryoablation versusrollerball electroablation for abnormaluterine bleeding: two-year results of amulticenter randomized trial. Am JObstet Gynecol. 2003;188:699–701.
96. Corson SL. A multicenter evaluationof endometrial ablation by HydroThermAblator and rollerball for treat-ment of menorrhagia. J Am AssocGynecol Laparosc. 2001;8:359–367.
97. Goldrath MH. Evaluation of Hydro-ThermAblator and rollerball endome-trial ablation for menorrhagia 3 yearsafter treatment. J Am Assoc GynecolLaparosc. 2003;10:505–511.
98. Glasser MH, Zimmerman JD. TheHydroThermAblator system for man-agement of menorrhagia in women withsubmucous myomas: 12- to 20-monthfollow-up. J Am Assoc GynecolLaparosc. 2003;10:521–527.
99. Rosenbaum SP, Fried M, Munro MG.Endometrial hydrothermablation: acomparison of short-term clinicaleffectiveness in patients with normalendometrial cavities and those withintracavitary pathology. J MinimInvasive Gynecol. 2005;12:144–149.
100. Sharp NC, Cronin N, Feldberg I, et al.Microwaves for menorrhagia: a new
fast technique for endometrial ablation.Lancet. 1995;346:1003–1004.
101. Jack SA, Cooper KG, Seymour J, et al.A randomised controlled trial of micro-wave endometrial ablation without en-dometrial preparation in the outpatientsetting: patient acceptability, treatmentoutcome and costs. BJOG. 2005;112:1109–1116.
102. Cooper KG, Bain C, Parkin DE.Comparison of microwave endometrialablation and transcervical resection ofthe endometrium for treatment ofheavy menstrual loss: a randomisedtrial. Lancet. 1999;354:1859–1863.
103. Bain C, Cooper KG, Parkin DE.Microwave endometrial ablation versusendometrial resection: a randomizedcontrolled trial. Obstet Gynecol. 2002;99:983–987.
104. Cooper KG, Bain C, Lawrie L, et al. Arandomised comparison of microwaveendometrial ablation with transcervicalresection of the endometrium; followup at a minimum of five years. BJOG.2005;112:470–475.
105. Cooper JM, Anderson TA, Fortin CA,et al. Microwave endometrial ablationvs. rollerball electroablation for menor-rhagia: a multicenter randomized trial.J Amer Assoc Gynecol Laparosc. 2004;11:394-403. Abstract.
106. Soysal ME, Soysal SK, Vicdan K.Thermal balloon ablation in myoma-induced menorrhagia under localanesthesia. Gynecol Obstet Invest.2001;51:128–133.
107. Gallinat A, Nugent W. NovaSureimpedance-controlled system for endo-metrial ablation. J Am Assoc GynecolLaparosc. 2002;9:283–289.
108. Cooper J, Gimpelson R, Laberge P,et al. A randomized, multicenter trialof safety and efficacy of the NovaSuresystem in the treatment of menorrha-gia. J Am Assoc Gynecol Laparosc.2002;9:418–428.
109. Laberge PY, Sabbah R, Fortin C, et al.Assessment and comparison of intra-operative and postoperative pain asso-ciated with NovaSure and Thermachoiceendometrial ablation systems. J AmAssocGynecol Laparosc. 2003;10:223–232.
764 Munro

110. Baskett TF, Clough H, Scott TA.NovaSure bipolar radiofrequencyendometrial ablation: report of 200cases. J Obstet Gynaecol Can. 2005;27:473–476.
111. Bongers MY, Bourdrez P, Mol BW,et al. Randomised controlled trialof bipolar radio-frequency endometrialablation and balloon endometrialablation. BJOG. 2004;111:1095–1102.
112. Donnez J, Polet R, Rabinovitz R, et al.Endometrial laser intrauterine thermo-therapy: the first series of 100 patientsobserved for 1 year. Fertil Steril.2000;74:791–796.
113. Bhatta N, Anderson RR, Flotte T,et al. Endometrial ablation by meansof photodynamic therapy with photo-frin II. Am J Obstet Gynecol. 1992;167:1856–1863.
114. Mhawech P, Renaud A, Sene C, et al.High efficacy of photodynamic therapyon rat endometrium after systemicadministration of benzoporphyrinderivative monoacid ring A. HumReprod. 2003;18:1707–1711.
115. Van Vugt DA, Krzemien A, Roy BN,et al. Photodynamic endometrialablation in the nonhuman primate.J Soc Gynecol Investig. 2000;7:125–130.
116. Degen AF, Gabrecht T, Mosimann L,et al. Photodynamic endometrial abla-tion for the treatment of dysfunctionaluterine bleeding: a preliminary report.Lasers Surg Med. 2004;34:1–4.
117. Kucukozkan T, Kadioglu BG, UygurD, et al. Chemical ablation of endome-trium with trichloroacetic acid. Int JGynaecol Obstet. 2004;84:41–46.
118. Garside R, Stein K, Wyatt K, et al. Acost-utility analysis of microwave andthermal balloon endometrial ablationtechniques for the treatment of heavymenstrual bleeding. BJOG. 2004;111:1103–1114.
119. Seymour J, Wallage S, Graham W,et al. The cost of microwave endome-trial ablation under different anaes-thetic and clinical settings. BJOG.2003;110:92292–92296.
120. Glasser MH, Zimmerman JD. TheHydroThermAblator system for man-agement of menorrhagia in women with
submucous myomas: 12- to 20-monthfollow-up. J Am Assoc GynecolLaparosc. 2003;10:521–527.
121. Farrugia M, Hussain SY. Hystero-scopic endometrial ablation using theHydro ThermAblator in an outpatienthysteroscopy clinic: feasibility andacceptability. J Minim Invasive Gynecol.2006;13:178–182.
122. Hassan L, Gannon MJ. Anaesthesiaand analgesia for ambulatory hystero-scopic surgery. Best Pract Res ClinObstet Gynaecol. 2005;19:681–691.
123. McAllister KF, Bigrigg A. Uterineballoon therapy for menorrhagia: afeasibility study of its use in thecommunity setting. J Fam PlannReprod Health Care. 2002;28:133–134.
124. Duleba AJ, Heppard MC, SoderstromRM, et al. A randomized study com-paring endometrial cryoablation androllerball electroablation for treatmentof dysfunctional uterine bleeding. J AmAssoc Gynecol Laparosc. 2003;10:17–26.
125. Sivin I, Stern J, Diaz J, et al. Two yearsof intrauterine contraception withlevonorgestrel and with copper: arandomized comparison of the TCu380Ag and levonorgestrel 20mcg/daydevices. Contraception. 1987;35:245–255.
126. Lahteenmaki P, Haukkamaa M,Puolakka J, et al. Open randomisedstudy of use of levonorgestrel releasingintrauterine system as alternativeto hysterectomy. BMJ. 1998;316:1122–1126.
127. Crosignani PG, Vercellini P, MosconiP, et al. Levonorgestrel-releasing in-trauterine device versus hysteroscopicendometrial resection in the treatmentof dysfunctional uterine bleeding.Obstet Gynecol. 1997;90:257–263.
128. Istre O, Trolle B. Treatment ofmenorrhagia with the levonorgestrelintrauterine system versus endo-metrial resection. Fertil Steril. 2001;76:30430–30439.
129. Rauramo I, Elo I, Istre O. Long-termtreatment of menorrhagia with levo-norgestrel intrauterine system versusendometrial resection. Obstet Gynecol.2004;104:1314–1321.
Endometrial Ablation: Where Have We Been? Where are We Going? 765

130. Soysal M, Soysal S, Ozer S. A rando-mized controlled trial of levonorgestrelreleasing IUD and thermal balloon abla-tion in the treatment of menorrhagia.Zentralbl Gynakol. 2002;124:213–219.
131. Busfield RA, Farquhar CM, SowterMC, et al. A randomised trial compar-ing the levonorgestrel intrauterinesystem and thermal balloon ablationfor heavy menstrual bleeding. BJOG.2006;113:257–263.
132. Henshaw R, Coyle C, Low S, et al. Aretrospective cohort study comparingmicrowave endometrial ablation withlevonorgestrel-releasing intrauterinedevice in the management of heavymenstrual bleeding. Aust N Z J ObstetGynaecol. 2002;42:205–209.
133. Marjoribanks J, Lethaby A, FarquharC. Surgery versus medical therapy forheavy menstrual bleeding. CochraneDatabase Syst Rev. 2006;CD003855.
766 Munro