Comparison Bacterial Floras Two Groups Healthy Subjects ...the nasal flora has also been of interest...
8
Vol. 27, No. 12 JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1989, p. 2736-2743 0095-1137/89/122736-08$02.00/0 Copyright © 1989, American Society for Microbiology Comparison of the Nasal Bacterial Floras in Two Groups of Healthy Subjects and in Patients with Acute Maxillary Sinusitis HANNELE R. JOUSIMIES SOMER,l* SEPPO SAVOLAINEN,2 AND JUKKA S. YLIKOSKI2 Anaerobe Reference Unit, National Public Health Institute,' and Department of Otolaryngology, Central Military Hospital/2 SF-00300 Helsinki, Finland Received 22 May 1989/Accepted 21 August 1989 The nasal bacterial flora was studied in 183 healthy men entering military service (entry group), 103 healthy recruits in service (service group), and 185 recruits with acute maxillary sinusitis. The 267 nasal and ipsilateral sinus aspirate findings in the same patients with acute maxillary sinusitis were compared pairwise. In the entry group presumed sinus pathogens were only rarely isolated from the nasal cavities: Haemophilus influenzae in 4%, Streptococcus pneumoniae in 1%, Branhamella catarrhalis in 3%, and Streptococcus pyogenes in 0%. The corresponding isolation frequencies in the service group were 19, 13, 3, and <1 %, respectively, and those in the group with acute maxillary sinusitis were 61, 25, 7, and 6%, respectively. Suppression of the major components of the normal nasal fora, Corynebacterium sp., coagulase-negative staphylococci, Propionibacte- rium acnes, and Staphylococcus aureus, was seen in the group with acute maxillary sinusitis and also occasionally in the service group. When a sinus aspirate culture yielded a presumed sinus pathogen, the same pathogen was found in the nasal samples in 91% of the cases. The predictive value of a pathogen-positive nasal finding was highest (93.8%) for S. pyogenes, followed by 77.7% for H. influenzae and 68.7% for S. pneumoniae, and lowest (20%) for B. catarrhalis. The bacterial flora of the nasal cavity has been extensively studied to define the composition of the normal flora at this site and also to identify nasal carriers of certain bacterial species, such as Staphylococcus aureus or Streptococcus pyogenes, for epidemiological purposes. Because of the communication of the nasal cavity and the maxillary sinuses, the nasal flora has also been of interest to investigators studying the bacteriology of maxillary sinusitis. The main components of the normal flora of the nasal cavity are coagulase-negative staphylococci (reported to be present in widely varied percentages, ranging from 12 to 81%), aerobic diphtheroids (6 to 68%), and S. aureus (6 to 34%) (1, 3, 7, 18, 29, 34). Other aerobic species, such as streptococci of the viridans group, meningococci, enteric bacteria, and Moraxella sp., have been isolated occasionally (1, 3, 4, 7, 11, 29, 34). Potential sinus pathogens have been relatively rarely recovered from healthy nasal cavities: Streptococcus pneumoniae in 0.5 to 15%, Haemophilus influenza in 0 to 6%, S. pyogenes in 0 to 1%, and Bran- hamella catarrhalis in 0 to 4% (1, 3, 7, 11, 18, 29, 34). In one study, higher percentages of S. pneumoniae (37%) and H. influenza (14%) were found in nasal cultures from healthy children (5). Anaerobic bacteria have been studied in the nasal flora by only a few investigators, whose main interest has been the occurrence of Propionibacterium sp., found in 8 to 100% (12, 18, 33). We have recently shown that also other anaerobes, such as Peptostreptococcus sp. and Bac- teroides sp., can occasionally inhabit the healthy nasal cavity (29, 35). The nasal bacterial flora in patients with verified sinusitis has been shown to be substantially different from that of the healthy nose. The isolation frequency of coagulase-negative staphylococci and aerobic diphtheroids are reduced (1, 3, 7), whereas those of potential sinus pathogens are significantly elevated to 36% for S. pneumoniae, over 50% for H. * Corresponding author. influenza, 6% for S. pyogenes, and 4% for B. catarrhalis (1, 3, 7, 16, 19, 25). In many studies of the nasal bacterial flora in sinusitis, a simultaneous sinus aspirate culture from the same patient has been lacking (7, 19, 25). The few studies comparing nasal and sinus findings in the same patients with acute maxillary sinusitis (AMS) (1, 9, 10) or with chronic sinusitis (7, 16) have concluded that their correlation is poor. However, in preliminary analysis among military recruits (30) we found a much better correlation for potential sinus pathogens in AMS. The purpose of the present study was to characterize the aerobic and anaerobic nasal flora, paying special attention to the occurrence of presumed sinus pathogens. Two groups of healthy young men, recruits entering military service and those in service, were compared with recruits hospitalized for AMS. The bacteriological findings in the sinus aspirates of these patients have been published (15), and this data base made it possible to compare the nasal and sinus aspirate findings in the same patients. We specifically wanted to examine in detail the predictive value for etiology of AMS of finding a presumed sinus pathogen in the nasal cavity. MATERIALS AND METHODS Healthy subjects. The study included two groups of healthy subjects. The first group (entry group) consisted of 183 young men (ages, 17 to 26 years; mean, 20 years), of whom 97 were applicants for pilot education in the Finnish Air Force in May 1984 and 86 were recruits at the entry of their military service in October 1984. Ail subjects in the entry group entered the military service from civilian living conditions and thus represented a civilian population. Nasal samples were obtained at the time of application and entry to service. Bacteriological findings of the nasal cavities in these subjects have been partially described (29, 35). All of the subjects considered themselves completely healthy. In an examination performed by an ear, nose, and throat specialist (S.S.), including anterior rhinoscopy in all subjects, none of 2736 on December 5, 2020 by guest http://jcm.asm.org/ Downloaded from
Transcript of Comparison Bacterial Floras Two Groups Healthy Subjects ...the nasal flora has also been of interest...

Vol. 27, No. 12JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1989, p. 2736-27430095-1137/89/122736-08$02.00/0Copyright © 1989, American Society for Microbiology
Comparison of the Nasal Bacterial Floras in Two Groups of HealthySubjects and in Patients with Acute Maxillary SinusitisHANNELE R. JOUSIMIES SOMER,l* SEPPO SAVOLAINEN,2 AND JUKKA S. YLIKOSKI2
Anaerobe Reference Unit, National Public Health Institute,' and Department of Otolaryngology,Central Military Hospital/2 SF-00300 Helsinki, Finland
Received 22 May 1989/Accepted 21 August 1989
The nasal bacterial flora was studied in 183 healthy men entering military service (entry group), 103 healthyrecruits in service (service group), and 185 recruits with acute maxillary sinusitis. The 267 nasal and ipsilateralsinus aspirate findings in the same patients with acute maxillary sinusitis were compared pairwise. In the entrygroup presumed sinus pathogens were only rarely isolated from the nasal cavities: Haemophilus influenzae in4%, Streptococcus pneumoniae in 1%, Branhamella catarrhalis in 3%, and Streptococcus pyogenes in 0%. Thecorresponding isolation frequencies in the service group were 19, 13, 3, and <1%, respectively, and those inthe group with acute maxillary sinusitis were 61, 25, 7, and 6%, respectively. Suppression of the majorcomponents of the normal nasal fora, Corynebacterium sp., coagulase-negative staphylococci, Propionibacte-rium acnes, and Staphylococcus aureus, was seen in the group with acute maxillary sinusitis and alsooccasionally in the service group. When a sinus aspirate culture yielded a presumed sinus pathogen, the samepathogen was found in the nasal samples in 91% of the cases. The predictive value of a pathogen-positive nasalfinding was highest (93.8%) for S. pyogenes, followed by 77.7% for H. influenzae and 68.7% for S.pneumoniae, and lowest (20%) for B. catarrhalis.
The bacterial flora of the nasal cavity has been extensivelystudied to define the composition of the normal flora at thissite and also to identify nasal carriers of certain bacterialspecies, such as Staphylococcus aureus or Streptococcuspyogenes, for epidemiological purposes. Because of thecommunication of the nasal cavity and the maxillary sinuses,the nasal flora has also been of interest to investigatorsstudying the bacteriology of maxillary sinusitis.The main components of the normal flora of the nasal
cavity are coagulase-negative staphylococci (reported to bepresent in widely varied percentages, ranging from 12 to81%), aerobic diphtheroids (6 to 68%), and S. aureus (6 to34%) (1, 3, 7, 18, 29, 34). Other aerobic species, such asstreptococci of the viridans group, meningococci, entericbacteria, and Moraxella sp., have been isolated occasionally(1, 3, 4, 7, 11, 29, 34). Potential sinus pathogens have beenrelatively rarely recovered from healthy nasal cavities:Streptococcus pneumoniae in 0.5 to 15%, Haemophilusinfluenza in 0 to 6%, S. pyogenes in 0 to 1%, and Bran-hamella catarrhalis in 0 to 4% (1, 3, 7, 11, 18, 29, 34). In onestudy, higher percentages of S. pneumoniae (37%) and H.influenza (14%) were found in nasal cultures from healthychildren (5). Anaerobic bacteria have been studied in thenasal flora by only a few investigators, whose main interesthas been the occurrence of Propionibacterium sp., found in8 to 100% (12, 18, 33). We have recently shown that alsoother anaerobes, such as Peptostreptococcus sp. and Bac-teroides sp., can occasionally inhabit the healthy nasalcavity (29, 35).The nasal bacterial flora in patients with verified sinusitis
has been shown to be substantially different from that of thehealthy nose. The isolation frequency of coagulase-negativestaphylococci and aerobic diphtheroids are reduced (1, 3, 7),whereas those of potential sinus pathogens are significantlyelevated to 36% for S. pneumoniae, over 50% for H.
* Corresponding author.
influenza, 6% for S. pyogenes, and 4% for B. catarrhalis (1,3, 7, 16, 19, 25).
In many studies of the nasal bacterial flora in sinusitis, asimultaneous sinus aspirate culture from the same patienthas been lacking (7, 19, 25). The few studies comparing nasaland sinus findings in the same patients with acute maxillarysinusitis (AMS) (1, 9, 10) or with chronic sinusitis (7, 16)have concluded that their correlation is poor. However, inpreliminary analysis among military recruits (30) we found amuch better correlation for potential sinus pathogens inAMS.The purpose of the present study was to characterize the
aerobic and anaerobic nasal flora, paying special attention tothe occurrence of presumed sinus pathogens. Two groups ofhealthy young men, recruits entering military service andthose in service, were compared with recruits hospitalizedfor AMS. The bacteriological findings in the sinus aspiratesof these patients have been published (15), and this data basemade it possible to compare the nasal and sinus aspiratefindings in the same patients. We specifically wanted toexamine in detail the predictive value for etiology of AMS offinding a presumed sinus pathogen in the nasal cavity.
MATERIALS AND METHODSHealthy subjects. The study included two groups of
healthy subjects. The first group (entry group) consisted of183 young men (ages, 17 to 26 years; mean, 20 years), ofwhom 97 were applicants for pilot education in the FinnishAir Force in May 1984 and 86 were recruits at the entry oftheir military service in October 1984. Ail subjects in theentry group entered the military service from civilian livingconditions and thus represented a civilian population. Nasalsamples were obtained at the time of application and entry toservice. Bacteriological findings of the nasal cavities in thesesubjects have been partially described (29, 35). All of thesubjects considered themselves completely healthy. In anexamination performed by an ear, nose, and throat specialist(S.S.), including anterior rhinoscopy in all subjects, none of
2736
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NASAL BACTERIA IN HEALTH AND SINUSITIS 2737
the study subjects had significant infectious symptoms orsigns from the nasal cavity or the paranasal sinuses.The second group (service group) consisted of 103 recruits
(ages, 17 to 28 years; mean, 20 years) in military service andhospitalized for acute acoustic trauma at the Ear, Nose, andThroat Department of The Central Military Hospital, Hel-sinki, between March 1987 and November 1988. The acous-tic trauma was diagnosed between 4 and 318 days (mean 151days) in service, and the samples were taken between 2 hand 6 days (mean, 2 days) after the trauma and always beforethe possible hyperbaric oxygen therapy. In the service group27% of the subjects were recruits during their first 2 monthsof service, 28% were sergeant or officer trainees (2 to 11months of service), and 45% were conscripts who had beenin service for 2 to 8 months. All participated in outdooractivities and combat-firing training exercises and lived inopen barracks of 8 to 16 beds per room. Ail of the subjects inthis group underwent an ear, nose, and throat examinationconducted by the same specialist as subjects in the firstgroup. All also had sinus radiographs taken to excludecontraindications for possible hyperbaric oxygen therapy ina pressure chamber. No nasal or sinus symptoms suggestiveof respiratory tract infection were discovered at the time ofexamination.
Patients with AMS. The study group consisted of 185patients diagnosed with AMS (AMS group), based on clini-cal and radiographic findings, enrolled in a recent bacterio-logical survey (15). Of the 238 patients described in thereport (15), 53 were omitted from the present study becausenasal specimens were not available. Of the 185 patients 5were women and 180 were men (ages, 17 to 46 years; mean,21 years). The military occupational specialties, activities, orliving conditions of the patients and the service group werecomparable. None of the patients had experienced symp-toms for more than 3 weeks. Patients with a concomitantdental root canal infection suggesting dentogenic sinusitiswere excluded (15). Informed consent was obtained from thepatients before the invasive procedures were performed.None of the healthy subjects or the patients with AMS had
received antimicrobial agents during the 2 weeks before theexamination or earlier for the present infection (AMSgroup).Specimen collection. Altogether 366 nasal samples from the
183 healthy subjects of the entry group and 206 samples fromthe 103 healthy subjects of the service group were collectedthrough a nasal speculum, by a sterile cotton swab soaked inactivated charcoal, from the posterior parts of both nasalcavities (care being taken to avoid contamination from thevestibule). The samples were transported to the AnaerobeReference Unit, National Public Health Institute, Helsinki,in modified Stuart transport medium (Transpocult; OrionDiagnostica, Helsinki, Finland) and processed within 30 minof collection.From the 185 patients with AMS, 334 samples of visible
secretion were collected with a swab in the nasal cavity or,when no secretion was present, from the middle meatusclose to the ostium before the nasal cavity was prepared forantral puncture. The samples were transported as describedabove. After the puncture site was anesthetized, 267 sinussecretions from the same patients were collected by antralaspiration, immediately transported in syringes, and quanti-tatively cultured for aerobic and anaerobic bacteria as de-scribed previously (15).
Culture and identification. In the laboratory the nasalsamples were inoculated onto the following media: bloodand chocolate agar for the isolation of aerobes; crystal
violet-nalidixic acid-gentamicin agar (24) for the selectiveisolation of pneumococci; vitamin Kl- and hemin-supple-mented, nonselective brucella blood agar for all anaerobes;and kanamycin-vancomycin-laked blood agar for Bacteroi-des sp. (31). The swab was soaked in supplemented thio-glycollate broth and firmly pressed against the wall of thetube to elute material from it into the medium for enrichment(31).The sinus aspirates were quantitatively inoculated to the
media described above and also onto several other media forthe selective isolation of anaerobic bacteria as described(15).Aerobic cultures were incubated at 36°C in an atmosphere
containing 5% C02 and examined after 24 and 48 h; anaer-obic cultures were incubated in jars filled by the evacuationreplacement method with mixed gas (10% H2, 10% C02, and80% N2) for up to 7 days, with examination every 48 h. Thethioglycolate broth was subcultured aerobically and anaero-bically when growth appeared or at the latest after 5 days.The numbers of bacterial colonies were semiquantitated as
follows: heavy growth (>100 colonies), moderate growth (20to 99 colonies), and light growth (<20 colonies). "Enrich-ment only" describes isolations that were negative afterdirect plating on agar media but positive after subculturingthe thioglycolate broth. The isolated aerobic and anaerobicbacteria were identified and typed by standard methods (13,17, 31).
Statistical methods. The data were analyzed by the chi-square test or the Fisher exact test (when individual datapoints were less than 5). The predictive values were deter-mined as described by Vecchio (32).
RESULTS
Altogether, 366 samples from the nasal cavities of the 183healthy subjects in the entry group and 206 samples from the103 healthy subjects in the service group were analyzed. In103 (56%) of the patients with AMS, secretion was obtainedfrom one sinus only (unilateral sinusitis cases). In theremaining 82 patients (44%), secretion was obtained fromboth sinuses (bilateral sinusitis cases). A sample was ob-tained from 334 nasal cavities; from both sides in all 82patients with bilateral sinusitis (164 ipsilateral and contralat-eral samples) and from the diseased side in all of theunilateral cases (103 ipsilateral samples) but only 67 samplesfrom the opposite (contralateral) side (Table 1).
Aerobic bacterial findings. All of the samples from thenasal cavities of both the healthy subjects and the patientswith AMS yielded aerobic bacteria by culture. The maxi-mum number of aerobic isolates from one nasal cavity was 6.The culture findings in the ipsilateral and the contralateralnasal cavities of the patients with AMS are presentedseparately in Table 1. There were, however, no significantdifferences between the two sides in the isolation frequencyof any bacterial group. For statistical comparisons, thefindings from the ipsilateral side only were used.Major components of normal nasal flora (coagulase-nega-
tive staphylococci, S. aureus, Corynebacterium sp., andstreptococci of the viridans group) were frequently recov-ered from the nasal samples of both the healthy subjects andthe patients with AMS. There were, however, differencesbetween the groups of study subjects in the isolation fre-quency of these bacteria. Coagulase-negative staphylococciwere most often recovered from the nasal samples of healthysubjects in the entry group (76%), less often from the servicegroup (62%, P < 0.01), and least often from the AMS group
VOL. 27, 1989
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

2738 JOUSIMIES-SOMER ET AL.
TABLE 1. Aerobic bacteria in the nasal cavities of patients with AMS and two groups of healthy subjects (both nasal cavities sampled)
% of patients with the indicated isolate P for difference between groups
Bacterium or parameter Patients with AMS Healthy subjects Entry versus AMSÛ versus AMSI versus
Ipsilateral Contralateral Entry group Service group service entry service
Major components of normal nasal floralCoagulase-negative staphylococci 59 57 76 62 <0.01 <0.001 NSCStaphylococcus aureus 18 19 36 34 NS <0.001 <0.001Corynebacterium sp. 19 17 43 70 <0.001 <0.001 <0.001Viridans group streptococci 10 il il 20 <0.01 NS <0.01
Common sinus pathogensHaemophilus influenza 61 59 4 19 <0.001 <0.001 <0.001Streptococcus pneumoniae 25 26 1 13 <0.001 <0.001 <0.01Branhamella catarrhalis 7 9 3 3 NS <0.01 <0.05Streptococcus pyogenes 6 5 0 <1 NS <0.001 <0.01
Other bacteriaNeisseria meningitidis 8 10 1 3 NS <0.001 <0.05Moraxella sp. 1 2 3 5 NS NS <0.05Streptococcid 2 2 2 1 NS NS NSEnterobacteriaceaee 10 9 6 12 <0.05 NS NSOthers 2 1 <1 1 NS NS NS
No. of patients 185 185 183 103No. of nasal cavities sampled 267 2319 366 206No. of isolates 609 526 680 503Mean no. of isolates per cavity 2.3 2.3 1.9 2.4 <0.001 <0.001 NS
a The ipsilateral side was used for all comparisons.b Individual bacterial species present in -10% of the nasal cavities of healthy subjects.C NS, Not significant.d Includes Streptococcus anginosus, Streptococcus agalactiae, Streptococcusfaecalis, beta-hemolytic streptococci or groups C and G, each present in 0 to
2% of the nasal cavities.e Includes Citrobacter diversus, Citrobacterfreundii, Enterobacter aerogenes, Enterobacter agglomerans, Enterobacter cloacae, Escherichia coli, Hafnia
alvei, Klebsiella oxytoca, Klebsiella pneumoniae, Morganella morganfi, and Proteus mirabilis, each present in 0 to 3% of the nasal cavities.f Includes Neisseria spp. other than Neisseria gonorrhoeae or N. meningitidis, Acinetobacter calcoaceticus, and Alcaligenesfaecalis, each present in 0 to 2%
of the nasal cavities.8 Nasal culture not available from the contralateral side in 36 patients with unilateral sinusitis.
(59%, P < 0.001 between the AMS and entry groups). Theisolation frequency of S. aureus was lowest in the AMSgroup (18%) compared with both groups of healthy subjects(entry group, 36%; service group, 34%; P < 0.001 in bothcases). Corynebacterium sp. were isolated most often in theservice group (70%), less often in the entry group (43%), andleast often in the AMS group (19%). The differences ofisolation frequencies between each group were highly signif-icant (P < 0.001). Streptococci of the viridans group weremore often found in the service group (20%) than in the entrygroup (11%) or the AMS group (10%) (P < 0.01 for the entryand AMS groups).Presumed sinus pathogens were each significantly (P <
0.05) more often isolated from the patients with AMS thanfrom either group of healthy subjects. H. influenza was thepredominant organism recovered in the AMS group (61%),outnumbering even the isolation rate of coagulase-negativestaphylococci within the group. However, the isolation rateof H. influenza was also higher in the service group (19%)than in the entry group (4%) (P < 0.001 in each case). Thedistribution of the isolation rates of S. pneumoniae amongthe study groups resembled that of H. influenza (AMSgroup, 25%; service group, 13%; entry group, 1%). B.catarrhalis was found much less often, in 3% of the healthysubjects and in 7% of the patients with AMS (P < 0.05between these groups). The same trend was seen for theisolation rates of S. pyogenes. None of the healthy subjectsin the entry group harbored S. pyogenes, and it was recov-ered from only one nasal cavity in the service group. In
contrast, 16 patients (16 ipsilateral nasal cavities) in the AMSgroup had a positive culture for S. pyogenes (P < 0.01).
Differences of isolation rates were also found betweenhealthy subjects and patients with AMS among other bacte-ria, including Neisseria meningitidis, Moraxella sp., andspecies of the family Enterobacteriaceae (P < 0.05 for eachof these).The mean number of aerobic bacterial isolates per nasal
cavity was 1.9 in the entry group, 2.4 in the service group,and 2.3 in the AMS group. The majority (93%) of thepathogen-positive nasal cultures from patients with AMSwere also positive for other bacterial species (Table 1), andtwo to three other bacterial species (maximum number, five)were recovered in more than one half of these cultures.
Anaerobic bacterial findings. Anaerobic bacteria were lessoften recovered in the nasal cultures. The highest isolationrate for anaerobes (Table 2), 74%, was encountered amongthe healthy subjects of the entry group, followed by rates of55% in the AMS group and 51% in the service group. Themaximum number of anaerobic isolates from one nasalcavity was five. Propionibacterium acnes was the mostcommonly isolated anaerobe in all groups of subjects. It wasalso clearly more common in the entry group (73%) than ineither the patients with AMS (46%) or the service group(47%, P < 0.001 in both cases). Peptostreptococcus magnuswas the second most commonly isolated anaerobic speciesamong all the subjects studied. There were no significantdifferences between the three study groups in the isolationrates of P. magnus or other anaerobic species.
J. CLIN. MICROBIOL.
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NASAL BACTERIA IN HEALTH AND SINUSITIS 2739
TABLE 2. Anaerobic bacteria in the nasal cavities of patients with AMS and two groups of healthy subjects (both sides sampled)
% of patients with the indicated isolate P for difference between groups
Bacterium or parameter Patients with AMS Healthy subjects Entry versus AMS' versus AMS' versus
Ipsilateral Contralateral Entry group Service group service entry service
Propionibacterium acnes 46 46 73 47 <0.001 <0.001 NSbPropîonibacterium sp. <1 <1 0 0 NS NS NSPeptostreptococcus asaccharolyticus <1 0 0 0 NS NS NSPeptostreptococcus magnus 6 6 4 9 NS NS NSPeptostreptococcus productus O O O <1 NS NS NSPeptostreptococcus sp. 0 0 1 0 NS NS NSBacteroides capillosus O O O <1 NS NS NSBacteroides corporis <1 0 0 0 NS NS NSBacteroides intermedius 2 2 1 1 NS NS NSBacteroides melaninogenicus <1 0 0 <1 NS NS NSBacteroides oralis <1 <1 0 0 NS NS NSBacteroides oris O O O <1 NS NS NSBacteroides ovatus O O O <1 NS NS NSBacteroides ureolyticus 1 1 <1 0 NS NS NSEikenella corrodensc O <1 <1 0 NS NS NSEubacterium sp. 1 <1 0 0 NS NS NSFusobacterium nucleatum 1 <1 0 0 NS NS NSVeillonella parvula <1 0 0 <1 NS NS NS
No. of patients 185 185 183 103No. of nasal cavities sampled 267 23ld 366 206No. of isolates 159 134 295 124Mean no. of isolates per cavity 0.6 0.6 0.8 0.6 <0.01 <0.001 NS
a See footnote a to Table 1.b NS, Not significant.C Microaerophilic.d See footnote g to Table 1.
Quantity of growth. To assess the quantity of bacterialgrowth in the nasal samples, semiquantitative culture resultsof the entry group were estimated and compared with thoseof the AMS group (Table 3). Enrichment was necessary topick up 10.5% of all the isolates in the AMS group and 5.8%in the entry group. Of the major components of normal nasalflora, coagulase-negative staphylococci, P. acnes, and strep-tococci of the viridans group were usually present in rela-
tively low numbers only (<20 colonies per plate). S. aureuswas equally often present as heavy (>100 colonies perplate), moderate (20 to 99 colonies per plate), or light (<20colonies per plate) growth in the patients with AMS butshowed a tendency to heavy or moderate growth in healthysubjects. Also, Corynebacterium sp. isolates were mostoften present as heavy or moderate growth in both studygroups.
TABLE 3. Semiquantitative nasal culture results of the common sinus pathogens and the major components of normal nasal flora inpatients with AMS (ipsilateral side) and healthy subjects (entry group, both sides sampled)a
No. of samples containing the indicated isolate
Patients with AMS Healthy subjectsIsolate
Heavy Moderate Light By Heavy Moderate Light Bygrowth growth growth en ychment n eeowthgrowth growth only
Major components of normal nasalflora
Coagulase-negative staphylococci 157 5 24 87 41 279 12 78 183 6P. acnes 124 3 31 89 1 269 3 40 226 0Corynebacterium sp. 50 20 20 8 2 156 48 72 35 1S. aureus 49 10 13 14 12 132 47 31 36 18Viridans group streptococci 24 1 7 10 6 39 1 il 15 12All 39 95 208 62 111 232 495 37
Common sinus pathogensH. influenzae 163 109 29 19 6 16 13 3 0 0S. pneumoniae 67 35 25 7 0 5 2 3 0 0B. catarrhalis 20 4 12 4 0 10 2 3 5 0S. pyogenes 16 16 0 0 0 0 0 0 0 0AUl 164 66 30 6 17 9 5 0
a Heavy, moderate, and light growth are defined as >100, 20 to 99, and <20 colonies per plate, respectively.
VOL. 27, 1989
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

2740 JOUSIMIES-SOMER ET AL.
lthy 80- Healthy 80-e nosery) (service)
60- 60-
40- 40-
20-_ __o20-
i7 8 9 1 2 3 4 5 6 7 8 9
Normal flora1= Coagulase negative staphylococci2= Propionibacterium acnes3= Corynebacterium sp.
4= Staphylococcus aureus5= Viridans group streptococci
AMS 80- AMSnose sinus
60-
44'1~~~401 2 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 9
Sinus pathogens6= Haemophilus influenza7= Streptococcus pneumoniae8= Branhamella catarrhalis9= Streptococcus pyogenes
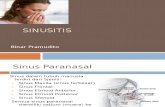
FIG. 1. Major components of normal nasal flora and common sinus pathogens in nasal cultures of two groups of healthy subjects andpatients with AMS compared with cultures from the sinus. Patterns from left to right are from healthy subjects entering military service,healthy subjects in military service, patients with AMS (nose), and the same patients with AMS (sinus secretion).
The presumed sinus pathogens were usually present asheavy or moderate growth in either group of subjects. Anexception was B. catarrhalis, which was more often found aslight growth in the healthy subjects. Thus, when presumedsinus pathogens were recovered from the nasal cultures ofeither the patients with AMS or healthy subjects, theirnumbers were usually higher than those of the major com-ponents of the normal nasal flora.
Predictive value of nasal cultures. The bacterial findings insinus secretions of the patients with AMS have been pre-sented in detail (15). In the 185 patients included in thepresent study, the frequencies of isolation of the commonsinus pathogens were as follows: H. influenza in 53%, S.pneumoniae in 18%, S. pyogenes in 6%, and B. catarrhalis in2% (Fig. 1).To assess the predictive value of the nasal culture findings
for etiology of AMS, a pairwise comparison of the commonsinus pathogens recovered from the nasal cavity and fromthe ipsilateral maxillary sinus was performed (Table 4).When the sinus aspirate was positive for a common sinuspathogen (208 times), the same pathogen was also isolatedfrom the ipsilateral nasal sample in 91% (sensitivity of thenasal culture). When the sinus aspirate was negative for acommon sinus pathogen (860 times), the nasal culture wasalso negative for that pathogen in 91% (specificity of thenasal culture). However, the nasal culture alone was positive76 times (28.5%), when the corresponding pathogen was not
isolated from the ipsilateral sinus aspirate (false-positivenasal culture). On the other hand, the sinus aspirate alonewas positive 18 times (8.6%), when the corresponding patho-gen was not isolated from the nasal sample (false-negativenasal culture).When we were evaluating the likelihood of a nasal culture
positive for a sinus pathogen in a patient with AMS topredict finding the same organism from the sinus aspirate(positive predictive value) and, on the other hand, thelikelihood of a nasal culture negative for a common sinuspathogen to predict a negative sinus culture for that patho-gen (negative predictive value), differences were seen amongthe bacterial species. The predictive value of a positive nasalculture was highest (93.8%) for S. pyogenes, 77.7% for H.influenza, 68.7% for S. pneumoniae, and lowest (20%) forB. catarrhalis. On the other hand, the predictive value of anasal culture negative for one of the common sinus patho-gens was high (>99.5%) for all other pathogens except for H.influenza (84.8%).Because of the relatively low predictive values of nasal
cultures positive for S. pneumoniae (68.7%) or H. influenza(77.7%), we analyzed in more detail the nasal and sinuscultures that were positive for these organisms (Table 5). H.influenza alone was isolated 120 times from the nasalsamples and was recovered from 93 (77.5%) of the sinusaspirates of the same patients. Similarly, S. pneumoniae wasthe only isolate in 31 nasal samples and was recovered in 24
TABLE 4. Pairwise comparison of the common sinus pathogens in the maxillary sinus and the ipsilateral nasal cavityof patients with AMS
isolates from: No. of samples isolated as follows Predictive value (%) of:Bacterium
Nose Sinus Nose+, Nose-, Nose+, Nose-, Positive Negativesinus sinus+ sinus+ sinus- culture culture
H. influenzae 163 141 38 16 125 88 77.7 84.6S. pneumoniae 67 47 21 1 46 199 68.7 99.5B. catarrhalis 20 5 16 1 4 246 20.0 99.6S. pyogenes 16 15 1 0 15 251 93.8 100.0
a A plus superscript indicates that the bacterium was isolated from that site. A minus superscript indicates that the bacterium was not isolated from that site.
J. CLIN. MICROBIOL.
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NASAL BACTERIA IN HEALTH AND SINUSITIS 2741
TABLE 5. H. influenza and S. pneumoniae isolated from the nose and maxillary sinus in patients with AMS
No. of maxillary sinus samples positive for:Growth in the ipsilateral
nasal cavity (n) H. influenzae s. pneumoniae H. influenza plus Different NeitherS. pneumoniae pathogen
H. influenza (120) 92 0 1 1 26S. pneumoniae (31) 1 23 1 1 5H. influenza plus S. pneumoniae (33) 9 7 15 0 2
(77.4%) of the corresponding sinus aspirates. However,when H. influenza and S. pneumoniae were found togetherin the nasal samples (33 times), the same combination wasisolated in only 45.5% of the sinus aspirates, whereas 16 ofthe 18 remaining aspirates were positive for either one ofthese organisms.
Other combinations of presumed sinus pathogens werealso found in the nasal cultures. These included H. influ-enzae and B. catarrhalis (seven samples), H. influenza andS. pyogenes (one sample), H. influenza and a mixture ofanaerobes (two samples), S. pneumoniae and B. catarrhalis(three samples), and S. pyogenes and B. catarrhalis (onesample).
In summary, when the nasal sample was positive for acombination of presumed sinus pathogens (47 times), bothcomponents of the combination were recovered in 16 (34%)of the ipsilateral sinus aspirates, and one or the other ofthemwas recovered alone in 51% (24 aspirates). Of the presumedsinus pathogens present in these combinations, B. catarrh-alis was least often (one of eight) isolated from the corre-sponding sinus aspirate. Altogether, one-third of all false-positive nasal cultures (26 of 76) were derived from culturespositive for a combination of presumed sinus pathogens.Another major group (13 of 76) of the false-positive nasal
cultures was derived from patients with bilateral sinusitis, inwhom the pathogen was, in fact, cultured from the contra-lateral sinus. Thus, these nasal cultures reflected the correctetiology of AMS in the patients. Of these 13, 9 were H.influenza, 3 were S. pneumoniae, and 1 was B. catarrhalis.Similarly, four false-negative nasal cultures for H. influenzaand the only one false-negative nasal culture for S. pneumo-niae were from bilateral sinusitis patients in whom thecontralateral nasal cavity was, in fact, positive for thisorganism.
DISCUSSIONIn this study the bacterial flora of the nasal cavities in
healthy young men entering military service (from civilianliving conditions) was found to differ substantially from thatof recruits in service with no respiratory infection and ofrecruits in service with AMS (Fig. 1). To ensure the healthstatus of the healthy subjects in both groups, only individu-als free of infectious symptoms or signs from the respiratorytract at the time of examination were included. This wasaccomplished by taking histories and by an examinationincluding anterior rhinoscopy performed by an ear, nose,and throat specialist. The diagnosis of AMS was based onclinical and radiographic findings and was accomplished bybacteriological cultures of sinus aspirates (15). The livingconditions of patients with AMS were similar to those ofmen in the service group; both lived in open militarybarracks occupied by 8 to 16 men, whereas the men enteringservice represented a civilian population.
Nasal bacterial fora in healthy subjects. In the entry groupthe common sinus pathogens H. influenza, S. pneumoniae,
S. pyogenes, and B. catarrhalis were isolated only rarelyfrom the nasal samples. This isolation rate of potential sinuspathogens differs from the definitely higher rates observed inchildren (5). Bacterial species considered as components ofthe normal nasal flora were found in frequencies comparableto previous reports in adults (1, 3, 7, 11, 18, 34). In thosestudies 8 to 50% of cultures were negative (1, 18, 34),whereas all nasal cultures in the present study were positivefor bacteria. The higher isolation rates may be explained byprompt (<30 min) processing of the specimens and the use ofenrichment, which yielded 6 to 11% of the isolates in eachstudy group.
Potential sinus pathogens, especially H. influenza and S.pneumoniae, were 5 to 10 times more common in the servicegroup than in the entry group. The high isolation rate of H.influenza (19%) in the service group resembles that re-ported in children (5). These higher isolation rates of poten-tial pathogens may reflect a high rate of transmission ofmicrobes in military barracks, resembling the high rate ofcross-infection among children in day-care centers (14). Thenasopharyngeal carrier rate of meningococci and pneumo-cocci has been shown to increase during military service (2,6, 21, 22). Likewise, viral infections are known to spreadrapidly in the military (26, 27), and we have previouslyshown elevated antiviral (mainly to adenoviruses and influ-enza viruses) antibody titers in 7% of a comparable in-service group with acoustic trauma (28). Virus-inducedimpairment of the local host defenses may facilitate coloni-zation of the upper respiratory tract by potentially patho-genic bacteria (8, 23).The isolation rates of Corynebacterium sp. and strepto-
cocci of the viridans group were higher in the service groupthan in the entry group, but that of coagulase-negativestaphylococci was lower. These changes in the normal floramay reflect incompletely understood facets of bacterialinterference in maintaining a balance between componentsof the resident flora and the transient invaders (20).Thus, our results suggest that military service increases
nasal colonization with pathogenic bacteria accompanied bychanges in the balance of the major components of thenormal flora. The nasal carriage of presumed pathogens mayalso predispose the recruits to AMS; however, this was notassessed in the present study.
Nasal bacterial flora in patients with AMS. In the AMSgroup the isolation frequencies of all the common sinuspathogens were significantly higher (P < 0.05) than those inthe healthy subjects and closely resembled the isolationfrequencies in the corresponding sinus aspirates of the samepatients (Fig. 1). On the other hand, the isolation frequenciesof normal flora components (Corynebacterium sp., coagu-lase-negative staphylococci, P. acnes, and S. aureus) weredecreased compared with those in both the entry and servicegroups. Similar findings have been described earlier forCorynebacterium sp. (3, 7), coagulase-negative staphylo-cocci (1, 7), and S. aureus (1).
VOL. 27, 1989
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

2742 JOUSIMIES-SOMER ET AL.
Correlation of nasal and sinus culture findings. When asinus aspirate grew a presumed sinus pathogen, the samepathogen was found in the nasal samples in 91% of the cases,thus giving a fairly high sensitivity for a pathogen-positivenasal culture. However, there were clear differences be-tween the bacterial species in the predictive value of apositive finding.Thus, when a nasal sample in a patient with AMS was
positive for S. pyogenes, there was a high (93.8%) likelihoodthat the same pathogen had invaded the sinus. Moreover,when the nasal culture was negative for this pathogen it wasnever isolated from the sinus either. Although the predictivevalues of positive nasal cultures for H. influenza (77.7%) orS. pneumoniae (68.7%) were lower, the sensitivity of thesefindings was definitely higher than described in most otherstudies (1, 9, 10). The true predictive value of culturespositive for these two organisms could, in fact, be consid-ered better on the patient level, taking into account patientswith bilateral sinusitis, in whom the pathogen was isolatedfrom the contralateral sinus, and patients in whom the nasalcultures were positive for two pathogens, only one of whichwas recovered in the sinus. By contrast, a positive nasalculture for B. catarrhalis was of no predictive value (20%).This is consistent with the relatively low pathogenic poten-tial of this organism in sinusitis of adults.Axelsson and Brorson (1) compared bacterial findings in
51 samples from the middle meatus and the ipsilateral sinusand found the same bacteria from both in 50% and adifference of one bacterial species in 28%. These data cannotbe compared with ours, since these authors did not specifythe bacterial species (which probably included componentsof the normal flora). In the present study 93% of thepathogen-positive nasal cultures contained, in addition to thepathogen, one or more bacteria of the normal nasal flora,which was irrelevant to the etiology of sinusitis in thepatient. Evans et al. reported a very high rate of false-negative nasal cultures, but the material was small (only 24patients) (9). Also Gwaltney et al. (10), who studied AMS,and Kessler (16), who studied chronic sinusitis, consideredthe correlation of nasal and sinus cultures to be poor,whereas Bjorkwall (3) found a high overall sensitivity (95%)of a positive nasal culture in 95 patients with AMS.
ACKNOWLEDGMENTS
We thank Inga Laukkonen, Marja Piekkola, Arja Kanervo, andPaula Summanen for excellent technical assistance; the staff of theEar, Nose, and Throat Department, Central Military Hospital, forskillful assistance; and Kaija Helisjoki for typing the manuscript.Our thanks are given to P. H. Makela, chief of the BacteriologicalDepartment, National Public Health Institute, Helsinki, for con-structive criticism and valuable help with preparing the manuscript.
LITERATURE CITED
1. Axelsson, A., and J. E. Brorson. 1973. The correlation betweenbacteriological findings in the nose and maxillary sinus in acutemaxillary sinusitis. Laryngoscope 83:2003-2011.
2. Aycock, W. L., and J. H. Mueller. 1950. Meningococcus carrierrates and meningitis incidence. Bacteriol. Rev. 14:115-160.
3. Bjorkwall, T. 1950. Bacteriological examination in maxillarysinusitis: bacterial flora of the nasal meatus. Acta Otolaryngol.Suppl. 83:1-32.
4. Bovre, K. 1970. Oxidase positive bacteria in the human nose
incidence and species distribution, as indicated by genetictransformation. Acta Pathol. Microbiol. Scand. Sect. B 78:780-784.
5. Box, Q. T., R. T. Cleveland, and C. Y. Wiliard. 1961. Bacterial
flora of the upper respiratory tract. Am. J. Dis. Child. 102:293-301.
6. Brundage, J. F., and W. D. Zollinger. 1987. Evolution ofmeningococcal disease epidemiology in the U.S. army, p. 5-25.In N. A. Vedros (ed.), Evolution of meningococcal disease.CRC Press, Inc., Boca Raton, Fla.
7. Catlin, F. I., L. E. Cluff, and R. C. Reynolds. 1965. Thebacteriology of acute and chronic sinusitis. South. Med. J.58:1497-1502.
8. Couch, R. B. 1981. The effects of influenza on host defences. J.Infect. Dis. 144:284-291.
9. Evans, F. O., Jr., J. B. Sydnor, W. E. C. Moore, G. R. Moore,J. L. Manwaring, A. H. Brill, R. T. Jackson, S. Hanna, J. S.Skaar, L. V. Holdeman, G. S. Fitz-Hugh, M. A. Sande, andJ. M. Gwaltney, Jr. 1975. Sinusitis of the maxillary antrum. N.Engl. J. Med. 293:735-739.
10. Gwaltney, J. M., Jr., A. Sydnor, Jr., and M. A. Sande. 1981.Etiology and antimicrobial treatment of acute sinusitis. Ann.Otol. Rhinol. Laryngol. 90(Suppl. 84):68-71.
11. Hays, G. C., and J. E. Mullard. 1972. Can nasal bacterial florabe predicted from clinical findings? Pediatrics 49:596-599.
12. Heczko, P. B., U. Hôffler, A. Kasprowicz, and G. Pulverer. 1981.Quantitative studies of the flora of the nasal vestibule in relationto nasal carriage of Staphylococcus aureus. J. Med. Microbiol.14:233-241.
13. Holdeman, L. V., E. P. Cato, and W. E. C. Moore (ed.). 1977.Anaerobe laboratory manual, 4th ed. Virginia Polytechnic In-stitute and State University, Blacksburg.
14. Istre, G. R., J. S. Conner, C. V. Broome, A. Hightower, andR. S. Hopkins. 1985. Risk factors for primary invasive Hae-mophilus influenza disease: increased risk from day careattendance and school-aged household members. J. Pediatr.106:190-195.
15. Jousimies-Somer, H. R., S. Savolainen, and J. S. Ylikoski. 1988.Bacteriological findings of acute maxillary sinusitis in youngadults. J. Clin. Microbiol. 26:1919-1925.
16. Kessler, L. 1968. Die Bakterienflora der Nasenhaupt- undNasennebenhohlen bei chronischen Sinuitiden und ihre Bezie-hung zueinander. Hals-Nasen-Ohrenartz 16:35-39.
17. Lennette, E. H., A. Balows, W. J. Hausler, Jr., and J. P. Truant(ed.). 1980. Manual of clinical microbiology, 3rd ed. AmericanSociety for Microbiology, Washington, D.C.
18. Linoli, O., S. Marconi, and M. Garaffa. 1981. Ecologia batteriaquantitative della mucosa nasale normale. Ann. Sclavo 23:151-161.
19. Lystad, A., P. Berdal, and L. Lund-Iversen. 1964. The bacterialflora of sinusitis with an in vitro study of the bacterial resistanceto antibiotics. Acta Otolaryngol. Supply. 188:390-400.
20. Mackowiak, P. H. 1982. The normal microbial flora. N. Engl. J.Med. 307:83-93.
21. MacLeod, G. M., R. G. Hodges, M. Heidelberger, and W. B.Bernhard. 1945. Prevention of pneumococcal pneumonia byimmunization with specific capsular polysaccharides. N. Engl.J. Med. 82:445-465.
22. Makela, P. H., H. Kayhty, P. Weckstrom, A. Sivonen, and O.-V.Renkonen. 1975. Effect of group-A meningococcal vaccine inarmy recruits in Finland. Lancet ii:883-886.
23. Mattie, H., and R. van Furth. 1981. Mechanisms of viral andbacterial infection of the respiratory mucosa. Rhinologyl(Suppl.):13-18.
24. Nichols, T., and R. Freeman. 1980. A new selective medium forStreptococcus pneumoniae. J. Clin. Pathol. 33:770-773.
25. Nylén, O., P.-H. Jeppsson, and P. Branefors-Helander. 1972.Acute sinusitis. A clinical, bacteriological and serological studywith special reference to Haemophilus influenza. Scand. J.Infect. Dis. 4:43-48.
26. Penttinen, K., K. Cantell, P. Somer, and A. Poikolainen. 1968.Mumps vaccination in the finnish defence forces. Am. J. Epi-demiol. 88:234-244.
27. Pyhala, R., K. Aho, and R. Visakorpi. 1979. Seroepidemiologyof HlNi influenza: striking differences in the attack rate amongyoung people. Acta Pathol. Microbiol. Scand. Sect. B 87:161-164.
J. CLIN. MICROBIOL.
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NASAL BACTERIA IN HEALTH AND SINUSITIS 2743
28. Savolainen, S., H. Jousimies-Somer, M. Kleemola, and J. Yli-koski. 1989. Serological evidence of viral or Mycoplasma pneu-
moniae infection in acute maxillary sinusitis. Eur. J. Clin.Microbiol. Infect. Dis. 8:131-135.
29. Savolainen, S., J. Ylikoski, and H. Jousimies-Somer. 1986. Thebacterial flora of the nasal cavity in healthy young men. Rhinol-ogy 24:249-255.
30. Savolainen, S., J. Ylikoski, and H. Jousimies-Somer. 1987.Predictive value of nasal bacterial culture for etiological agentsin acute maxillary sinusitis. Rhinology 25:49-55.
31. Sutter, V. L., D. M. Citron, and S. M. Finegold. 1980. Wads-worth anaerobic bacteriology manual, 3rd ed. The C. V. MosbyCo., St. Louis.
32. Vecchio, T. J. 1966. Predictive values of a single test inunselected populations. N. Engl. J. Med. 274:1171-1173.
33. Watson, E. D., N. J. Hoffman, R. W. Simmers, and T. Rosebury.1962. Aerobic and anaerobic bacterial counts of nasal washings:presence of organisms resembling Corynebacterium acnes. J.Bacteriol. 83:144-148.
34. Winther, B., S. Brofeldt, H. Gronborg, N. Mygind, M. Pedersen,and R. Vejlsgaard. 1984. Study of bacteria in the nasal cavityand nasopharynx during naturally acquired common colds. ActaOtolaryngol. 98:315-320.
35. Ylikoski, J., S. Savolainen, and H. Jousimies-Somer. 1989.Bacterial flora in the nasopharynx and nasal cavity of healthyyoung men. ORL 51:50-55.
VOL. 27, 1989
on Decem
ber 5, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from