ARTICLE IN PRESSweb.mit.edu/hst.035/ReadingSupplement/04_28_Coron/Sanduleanu C… · adenomatous...
8
In Vivo Diagnosis and Classification of Colorectal Neoplasia by Chromoendoscopy-Guided Confocal Laser Endomicroscopy SILVIA SANDULEANU,* ANN DRIESSEN, ‡ ENCARNA GOMEZ-GARCIA, § WIM HAMEETEMAN,* ADRIAAN DE BRUÏNE, ‡ and AD MASCLEE* *Department of Gastroenterology and Hepatology, ‡ Department of Pathology, and § Department of Clinical Genetics, University Hospital Maastricht, Maastricht, The Netherlands BACKGROUND & AIMS: Colorectal cancer surveillance guidelines rely on clinicohistologic features of adenomas. Un- fortunately, in common practice, recording of these features lacks precision and uniformity, which might hamper appropri- ate follow-up decisions. Confocal laser endomicroscopy (CLE) is a novel technology that allows real-time in vivo microscopy of the mucosa and provides accurate histopathology. The aims of this study were (1) to define and validate differential features of adenomatous and nonadenomatous colorectal polyps by chro- moendoscopy-guided CLE (C-CLE) and (2) to assess predictive value of this technique for diagnosis of colorectal neoplasia. METHODS: Patients at risk for colorectal cancer were pro- spectively investigated by using CLE. During extubation, fluo- rescein 10% was used in conjunction with acriflavine hydrochlo- ride 0.05% to characterize global tissue architecture as well as cytonuclear features of colorectal epithelium. Ex vivo histology was used as gold standard. Reproducibility tests were per- formed. RESULTS: In total, 116 colorectal polyps from 72 patients were examined. Ex vivo histology showed 68 adenomas, 6 invasive carcinomas, 30 hyperplastic polyps, and 12 inflam- matory polyps. C-CLE of adenomas revealed lack of epithelial surface maturation, crypt budding, altered vascular pattern, and loss of cell polarity. In contrast, C-CLE of nonadenomatous polyps revealed epithelial surface maturation, and minor abnor- malities of crypt architecture and of vascular pattern, and main- tained cell polarity. Adenoma dysplasia score reliably discrimi- nated high-grade dysplasia from low-grade dysplasia (accuracy, 96.7%). Interobserver agreement was high (K coefficients: pa- thologist, 0.92; endomicroscopist, 0.88). In vivo histology pre- dicted ex vivo data with sensitivity of 97.3%, specificity of 92.8%, and accuracy of 95.7%. CONCLUSIONS: C-CLE accurately discriminates adenomatous from nonadenomatous colo- rectal polyps and enables evaluation of degree of dysplasia during ongoing endoscopy. This technology might offer considerable potential to ultimately fine-tune surveillance programs, particularly in high-risk groups. C olorectal cancer (CRC) is a major public health issue in developed countries. 1 Early detection, accurate character- ization, and resection of the precursor lesions, adenomatous polyps, are essential for the prevention of this malignancy. 2,3 However, a large proportion of patients with adenomas also have nonadenomatous lesions such as hyperplastic and inflam- matory polyps. 4 Conventional endoscopy has limited ability to discriminate adenomatous from nonadenomatous colorectal polyps. Therefore, all identified lesions are routinely removed. This approach results in substantial increase of endoscopic workload, additional pathology costs, and possibly a higher rate of complications. Currently, decisions regarding endoscopic treatment of ade- nomas and surveillance after polypectomy rely on clinicohisto- logic features, namely size, multiplicity, grade of dysplasia, and villosity. 5,6 Unfortunately, in common practice, recording of these features frequently lacks precision and uniformity. As such, superficially taken biopsies, sampling error, and loss of polyps for histopathology are common events, making it diffi- cult to draw firm conclusions regarding follow-up. Moreover, there is well-known interobserver variation among pathologists in assessment of villosity and grading of dysplasia. 7,8 All these factors together might lead to underdiagnosis or overdiagnosis of colorectal neoplasia and, hence, suboptimal treatment and surveillance practices. Several studies addressing the outcome of CRC screening indi- cated that colonoscopy with polypectomy fails to prevent progres- sion to CRC in 10%–25% of cases. 9,10 A large population-based study has shown that colonoscopy might prevent death from left-sided but not from right-sided CRC. 11 Therefore, gastroenter- ologists and pathologists should unify their efforts to secure pre- cise diagnosis and classification of colorectal neoplasia. Recently, new enhanced imaging techniques evolved that might potentially alleviate these practical issues. It has been shown that chromoendoscopy with methylene blue or indigo carmine and targeted biopsies significantly improves the detec- tion of intraepithelial neoplasia compared with conventional colonoscopy in individuals at increased risk for CRC. 12,13 Confocal laser colonoscopy combines the classic white-light endoscopy with real-time microscopy. 14,15 Patients receive a contrast agent, fluorescein, and an endoscopically directed laser excites the targeted tissue. Confocal images are generated si- multaneously with the endoscopic images. This technique land- scapes large surface and subsurface areas, allowing generation of real-time, in vivo histologic images. Kiesslich et al 16 showed that chromoendoscopy-guided confocal laser endomicroscopy (C-CLE) enables accurate detection and classification of colo- rectal neoplasia. For this purpose, 2 histopathologic elements are mainly considered, crypt morphology and vascular pattern, Abbreviations used in this paper: ADS, adenoma dysplasia score; C-CLE, chromoendoscopy-guided confocal laser endomicroscopy; CI, confidence interval; CRC, colorectal cancer; HGD, high-grade dysplasia; HP, hyperplastic polyp; IC, invasive carcinoma; IP, inflammatory polyp; LGD, low-grade dysplasia; SA, serrated adenoma. © 2009 by the AGA Institute 1542-3565/09/$36.00 doi:10.1016/j.cgh.2009.08.006 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;xx:xxx ARTICLE IN PRESS
Transcript of ARTICLE IN PRESSweb.mit.edu/hst.035/ReadingSupplement/04_28_Coron/Sanduleanu C… · adenomatous...

IC
Sa
*N
BgflaittamvMsrrcwfp6msapmtn9tdadrdcp
CipHhmdpT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;xx:xxx
ARTICLE IN PRESS
n Vivo Diagnosis and Classification of Colorectal Neoplasia byhromoendoscopy-Guided Confocal Laser Endomicroscopy
ILVIA SANDULEANU,* ANN DRIESSEN,‡ ENCARNA GOMEZ-GARCIA,§ WIM HAMEETEMAN,* ADRIAAN DE BRUÏNE,‡
nd AD MASCLEE*
Department of Gastroenterology and Hepatology, ‡Department of Pathology, and §Department of Clinical Genetics, University Hospital Maastricht, Maastricht, The
etherlandswo
nlvtspctifos
cssloc
msctc
ecemsot(ra
CcHL
ACKGROUND & AIMS: Colorectal cancer surveillanceuidelines rely on clinicohistologic features of adenomas. Un-ortunately, in common practice, recording of these featuresacks precision and uniformity, which might hamper appropri-te follow-up decisions. Confocal laser endomicroscopy (CLE)s a novel technology that allows real-time in vivo microscopy ofhe mucosa and provides accurate histopathology. The aims ofhis study were (1) to define and validate differential features ofdenomatous and nonadenomatous colorectal polyps by chro-oendoscopy-guided CLE (C-CLE) and (2) to assess predictive
alue of this technique for diagnosis of colorectal neoplasia.ETHODS: Patients at risk for colorectal cancer were pro-
pectively investigated by using CLE. During extubation, fluo-escein 10% was used in conjunction with acriflavine hydrochlo-ide 0.05% to characterize global tissue architecture as well asytonuclear features of colorectal epithelium. Ex vivo histologyas used as gold standard. Reproducibility tests were per-
ormed. RESULTS: In total, 116 colorectal polyps from 72atients were examined. Ex vivo histology showed 68 adenomas,invasive carcinomas, 30 hyperplastic polyps, and 12 inflam-atory polyps. C-CLE of adenomas revealed lack of epithelial
urface maturation, crypt budding, altered vascular pattern,nd loss of cell polarity. In contrast, C-CLE of nonadenomatousolyps revealed epithelial surface maturation, and minor abnor-alities of crypt architecture and of vascular pattern, and main-
ained cell polarity. Adenoma dysplasia score reliably discrimi-ated high-grade dysplasia from low-grade dysplasia (accuracy,6.7%). Interobserver agreement was high (K coefficients: pa-hologist, 0.92; endomicroscopist, 0.88). In vivo histology pre-icted ex vivo data with sensitivity of 97.3%, specificity of 92.8%,nd accuracy of 95.7%. CONCLUSIONS: C-CLE accuratelyiscriminates adenomatous from nonadenomatous colo-ectal polyps and enables evaluation of degree of dysplasiauring ongoing endoscopy. This technology might offeronsiderable potential to ultimately fine-tune surveillancerograms, particularly in high-risk groups.
olorectal cancer (CRC) is a major public health issue indeveloped countries.1 Early detection, accurate character-
zation, and resection of the precursor lesions, adenomatousolyps, are essential for the prevention of this malignancy.2,3
owever, a large proportion of patients with adenomas alsoave nonadenomatous lesions such as hyperplastic and inflam-atory polyps.4 Conventional endoscopy has limited ability to
iscriminate adenomatous from nonadenomatous colorectalolyps. Therefore, all identified lesions are routinely removed.
his approach results in substantial increase of endoscopicorkload, additional pathology costs, and possibly a higher ratef complications.
Currently, decisions regarding endoscopic treatment of ade-omas and surveillance after polypectomy rely on clinicohisto-
ogic features, namely size, multiplicity, grade of dysplasia, andillosity.5,6 Unfortunately, in common practice, recording ofhese features frequently lacks precision and uniformity. Asuch, superficially taken biopsies, sampling error, and loss ofolyps for histopathology are common events, making it diffi-ult to draw firm conclusions regarding follow-up. Moreover,here is well-known interobserver variation among pathologistsn assessment of villosity and grading of dysplasia.7,8 All theseactors together might lead to underdiagnosis or overdiagnosisf colorectal neoplasia and, hence, suboptimal treatment andurveillance practices.
Several studies addressing the outcome of CRC screening indi-ated that colonoscopy with polypectomy fails to prevent progres-ion to CRC in 10%–25% of cases.9,10 A large population-basedtudy has shown that colonoscopy might prevent death fromeft-sided but not from right-sided CRC.11 Therefore, gastroenter-logists and pathologists should unify their efforts to secure pre-ise diagnosis and classification of colorectal neoplasia.
Recently, new enhanced imaging techniques evolved thatight potentially alleviate these practical issues. It has been
hown that chromoendoscopy with methylene blue or indigoarmine and targeted biopsies significantly improves the detec-ion of intraepithelial neoplasia compared with conventionalolonoscopy in individuals at increased risk for CRC.12,13
Confocal laser colonoscopy combines the classic white-lightndoscopy with real-time microscopy.14,15 Patients receive aontrast agent, fluorescein, and an endoscopically directed laserxcites the targeted tissue. Confocal images are generated si-ultaneously with the endoscopic images. This technique land-
capes large surface and subsurface areas, allowing generationf real-time, in vivo histologic images. Kiesslich et al16 showedhat chromoendoscopy-guided confocal laser endomicroscopyC-CLE) enables accurate detection and classification of colo-ectal neoplasia. For this purpose, 2 histopathologic elementsre mainly considered, crypt morphology and vascular pattern,
Abbreviations used in this paper: ADS, adenoma dysplasia score;-CLE, chromoendoscopy-guided confocal laser endomicroscopy; CI,onfidence interval; CRC, colorectal cancer; HGD, high-grade dysplasia;P, hyperplastic polyp; IC, invasive carcinoma; IP, inflammatory polyp;GD, low-grade dysplasia; SA, serrated adenoma.
© 2009 by the AGA Institute1542-3565/09/$36.00
doi:10.1016/j.cgh.2009.08.006

wanphgca
dctati
tspptThastltt
aOmbaCpbc
pCsosints(a�5
w
ciwg1itaZadetAfnsp
cslepsi
2 SANDULEANU ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. xx, No. x
ARTICLE IN PRESS
hich permit differentiation between normal mucosa, regener-tive changes, and neoplasia. Nevertheless, additional aspectseed to be clarified before embedding this technique in clinicalractice. Differentiation of low-grade dysplasia (LGD) andigh-grade dysplasia (HGD) might be of relevance in this re-ard. Acriflavine hydrochloride is a contrast agent that specifi-ally labels the nuclei and hence pinpoints cytonuclear alter-tions during confocal endomicroscopy.17,18
We performed a prospective study to systematically evaluateifferential features of adenomatous and nonadenomatousolorectal polyps by C-CLE. Fluorescein was used in conjunc-ion with acriflavine to characterize global tissue architecturend cytonuclear features of colorectal epithelium. Special atten-ion was paid to define objective criteria for grading of dysplasian adenomatous lesions during endomicroscopy examination.
Subjects and MethodsSubjectsBetween December 2007 and February 2009, consecu-
ive subjects attending our outpatient clinic for counseling andurveillance of individuals at risk for CRC were recruited in thisrospective study. The following subgroups were included: (1)atients with history of advanced adenomas or CRC, (2) pa-ients with Lynch syndrome, and (3) patients with familial CRC.he latter subgroup consisted of subjects with a dominant CRCistory, but without known mutation.19 Exclusion criteria werege �18 years, suboptimal bowel preparation, known polyposisyndromes, pregnancy, lactation, previous documented allergyo intravenously administered sodium fluorescein, and coagu-opathy that precludes biopsy sampling or polypectomy. Writ-en informed consent was obtained from all participants, andhe study was approved by the local Medical Ethics Committee.
Study ProcedureBowel preparation consisted of 3-day low residue diet
nd 4 L hypertonic polyethylene glycol solution (Klean-Prep).nly patients with adequate bowel preparation (visualization ofore than 90% of colonic mucosa) were included. Cecal intu-
ation was documented. All CLE procedures were performed bysingle experienced endoscopist (S.S.), who had completed theLE training program in Mainz and performed 25 completerocedures before commencing the study. The endoscopist waslinded to histologic data and remained blinded during dataollection until data analysis.
Figure 1 outlines the study methodology. Endoscopies wereerformed by using the Pentax EC3870CIFK (Pentax Medicalo, Montvale, NJ) colonoscope and ISC-1000 CLE system. In
hort, the principle of this technique relies on use of a singleptical fiber to deliver a pinpointed argon laser light into apecimen. Light emerging from this focused point after admin-stration of an exogenous fluorophore (eg, fluorescein intrave-ously or acriflavine hydrochloride topically) is recaptured intohe same optical system. Confocal images were collected at acan rate of 0.8 frames/s (1024 � 1024 pixels) or 1.6 frames/s1024 � 512 pixels). The optical plane thickness was 7 �m, with
lateral resolution of 0.7 �m. The range of z-axis was 0 –250m below the surface layer, and the field of view was 500 �00 �m.
After ileocecal intubation, butylscopolamine (20 mg bolus)
as administered intravenously to reduce colonic peristalsis. In wase of suspect lesions, selective chromoscopy with 5–10 mLndigo carmine 0.4% (SERB S.A.S.; Lab Pharm, Paris, France)as applied via a spraying catheter. Sequential CLE images wereenerated after intravenous administration of 5 mL fluorescein0% (SA Alcon-Couvreur NV, Puurs, Belgium). Subsequently,
ndigo carmine was washed out by using tap water appliedhrough the cleansing channel of the endoscope. Then 5–10 mLcriflavine hydrochloride 0.05% (Sigma-Aldrich Chemie BV,wijndrecht, The Netherlands) was topically applied and wasllowed to stain the mucosa for about 1 minute. Experimentalata suggest that this fluorophore, displaying antiseptic prop-rties, might carry the risk for mutagenicity.18 Nevertheless,hese observations were not substantiated in human studies.fter topical application of acriflavine, washing out was per-
ormed again. At this point, targeted biopsies were taken fromormal-appearing mucosa and from focal lesions. Finally, le-ions were endoscopically removed by cold biopsy, snareolypectomy, or by endoscopic mucosal resection.
Endoscopic and Histopathologic Classificationof Colorectal LesionsAfter chromoendoscopy, the morphology of lesions was
haracterized according to Paris classification.20,21 Size of le-ions was classified as diminutive (�5 mm), small (6 –9 mm), orarge (�10 mm). All specimens were examined by an experi-nced gastrointestinal pathologist (A.D.), who was unaware ofatient information, endoscopic data, and CLE findings. Tissuepecimens were sectioned at 4-�m intervals, immediately fixedn 10% buffered formalin solution, and subsequently stained
Figure 1. Study methodology.
ith hematoxlyin-eosin. Intraepithelial neoplasia was classi-

fiaH
swmw(a1wiww
fciuaa
wOt
nttifn2eLstsio
t(00IwTs
2ngwHnmoAt(ni
dC(paeiww0
w
pw4otyw2c
cmwvdc
Month 2009 DIAGNOSIS OF COLORECTAL NEOPLASIA BY C–CLE 3
ARTICLE IN PRESS
ed according to the modified Vienna classification.22 Advanceddenomas were defined as adenomas �10 mm, or containingGD, or any villous component.6
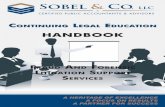
Confocal Endomicroscopy: Image Acquisitionand Characterization of LesionsFigure 2 depicts the sequence of events for the acqui-
ition of confocal images during endoscopy. Confocal imagesere collected in a 4-quadrant clockwise fashion from nor-al colonic mucosa (within 10 cm away from the lesion), asell as from focal lesions. For each colorectal lesion, normal
control) data were available. In case of diminutive, small,nd large polyps, images were obtained from at least 6, 8, and2 separate endomicroscopic fields, respectively. Biopsiesere taken 1 mm below the mucosal erythematous landmark
nduced by the suction port stabilization, as described else-here.16 In case of adenomatous polyps, grading of dysplasiaas based on “worst area” approach.23
During the procedure, the endoscopist classified all con-ocal images obtained. General architecture of normal mu-osa and of focal lesions was initially characterized afterntravenous administration of sodium fluorescein 10% bysing the Mainz classification.16 Cytonuclear features werenalyzed in detail after topical administration of 10 –20 mLcriflavine hydrochloride 0.05%.
The complete digital video recording of confocal imagesas also obtained, allowing further review when necessary.nly good quality images, defined as clear pattern recogni-
ion, were considered.
Study Design and Statistical CalculationsThis study consisted of 2 consecutive parts: (1) defi-
ition and standardization of data, in which diagnostic cri-eria were described, on an explorative basis; and (2) valida-ion study, in which consecutive patients were prospectivelynvestigated during 1 year. A total of 60 adenomas wereound in 72 patients. In our experience, prevalence of ade-omas with HGD in patients with Lynch syndrome is about0% (unpublished data). On the basis of this assumption, wexpected that 12 (20%) adenomas would harbor HGD and 48GD. The power to detect a difference in adenoma dysplasiacore (ADS) of a minimum 3 points, with a standard devia-ion of 2 points (on the basis of data from the explorativetudy) and with a significance level (�) of 5% by using a t test,s 0.995. As previously shown,24 it is expected that the power
Figure 2. Algorithm of confocal imaging acquisition during the study.
f Mann–Whitney U test in this case is �0.95. r
Interobserver agreement was tested by using the propor-ion of agreement (Pa) and weighted Cohen K coefficientwK). The strength of agreement was considered as slight,.01– 0.20; fair, 0.21– 0.4; moderate, 0.41– 0.60; substantial,.61– 0.80; and high (excellent), 0.81–1.0 (SPSS 16.0; SPSSnc, Chicago, IL).25 Nonparametric tests (Mann–Whitney U)ere used to assess differences between continuous variables.wo-sided P values �.05 were assumed to indicate statistical
ignificance.
ResultsClassification of Colorectal Neoplasia byConfocal Laser EndomicroscopyDefinition and standardization of data. A total of
860 CLE images from 20 subjects with histologically provenormal mucosa (subgroup I, n � 5), nonadenomatous (sub-roup II, n � 7), or adenomatous (subgroup III, n � 8, ofhich 4 with LGD and 4 with HGD) lesions were examined.erewith, we propose a classification of adenomatous andonadenomatous colorectal lesions by using CLE, as sum-arized in Table 1. In addition, in an attempt to provide
bjective criteria to differentiate LGD from HGD by CLE, theDS was calculated by adding up scores corresponding to
he following parameters: (1) epithelial surface maturation,2) crypt morphology, (3) vascular pattern, and (4) cyto-uclear atypia. Each parameter was scored from 0 –2, accord-
ng to severity of changes (Table 2).Reproducibility estimates for confocal laser en-
omicroscopy image interpretation. This initial set ofLE images was also examined by a second endomicroscopist
W.H.) and a pathologist (A.D.), who were blinded to theatient’s records and endoscopy data. The interobservergreement for classification into the 3 subgroups betweenndoscopist and pathologist was Pa, 0.94 (95% confidencenterval [CI], 0.88 –1.00) and wK, 0.92 (95% CI, 0.87–1.00),hereas the interobserver agreement between endoscopistsas Pa, 0.91 (95% CI, 0.84 – 0.99) and wK, 0.88 (95% CI,.82– 0.98), respectively.
Validation StudyFor this purpose, a second series of consecutive subjects
ere prospectively investigated.Characteristics of study population. Seventy-eight
atients were invited to participate in the study. Six patientsere excluded as a result of suboptimal bowel preparation (n �), incomplete colonoscopy related to severe diverticular diseasef the sigmoid (n � 1), and lack of histopathology (n � 1). Aotal of 72 patients (40 men and 32 women; median age, 56ears [range, 32–71 years] were included. Twenty-four (33.3%)ere patients with history of advanced adenomas and/or CRC;0 (27.8%) patients had Lynch syndrome, whereas 28 (38.9%)ases were patients with familial (non-Lynch) CRC.
The median duration of ileocecal intubation and total pro-edure time were 15 minutes (range, 8 –35 minutes) and 62inutes (range, 30 –96 minutes), respectively. The procedureas safe and generally well-tolerated, without any serious ad-
erse events. All patients experienced transient mild yellowiscoloration of urine caused by excretion of sodium fluores-ein. One patient had a mild allergic reaction, possibly as a
esult of fluorescein.
cf
dcwciit
tTncsort
Hwswnw
cntwawliwa
fclwLn
T
N
N
A
T
E
C
V
C
A
4 SANDULEANU ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. xx, No. x
ARTICLE IN PRESS
Classification of colorectal lesions by selectivehromoscopic colonoscopy. In total, 116 colorectal polypsrom 72 patients were examined and classified (Table 3).
Characterization of lesions by confocal laser en-omicroscopy, with focus on general architecture andytonuclear features. In total, 928 endomicroscopy fieldsere scanned. Seventy-eight percent of all CLE images were
onsidered of good quality. Interpretation of the rest ofmages was precluded as a result of movement artifacts (8%),nsufficient resolution (6%), or a combination of these fac-ors (8%).
able 1. Systematic Classification of Colorectal Lesions by U
General architecture
ormal mucosa ● Regular (uniform) architecture of surface and glepithelium
● Regular “honey-comb” appearance of vascular p
onadenomatouspolyps
● Slightly disturbed architecture: enlarged, branchcrypts (HP, IP)
● Increased number of cells in the crypts (mucos“stellar” aspect) (HP)
● Mild alterations of vascular pattern: faint aspecslightly dilated, irregular vessels (IP)
● Inflammatory infiltrate of lamina propria, decreacrypt/stroma ratio (IP)
denomatouspolyps
● Disturbed architecture: mild irregularity of the ceventual villous transformation, simple to comp(HGD), causing increased crypt/stroma ratio toaltered morphology, crypt destruction (IC)
● Mild to moderate alterations of vascular patternvessels, irregular aspect (LGD, HGD); neoangiocapillary leakage (IC)
able 2. ADS to Discriminate HGD From LGD DuringEndomicroscopy Examination
LGD HGD
pithelial surface maturation 0–1 1–20: normal1: incomplete maturation2: lack of epithelial surface maturation
rypt architecture 0–1 1–20: normal1: enlarged, slightly crowded crypts2: crowding, distorted crypts
ascular pattern 0–1 1–20: normal1: slightly increased vascular pattern, preserved
hexagonal pattern2: increased, distorted vessels
ytonuclear atypia 1 20: basal, regular nuclei1: pseudostratification of regular, pencillate
nuclei2: pseudostratification of irregular, large, round,
more apically localized nuclei
Hdemona dysplasia score 1–4 5–8
Classification of colorectal lesions was performed in realime during ongoing confocal endomicroscopy, as described inable 1. Special attention was paid to general architecture,amely crypt architecture and vascular pattern, as well as toytonuclear features, in particular alterations of cell polarity,ize, and morphology of nuclei. Figure 3 illustrates examplesf normal mucosa, adenomatous and nonadenomatous colo-ectal polyps by C-CLE, and corresponding targeted his-opathologic specimens.
Histopathologic classification of focal lesions.istopathology showed 68 adenomatous lesions, of which 44ere adenomas with LGD, 16 adenomas with HGD, and 8 were
errated adenomas. There were also 6 invasive carcinomas, 4ell-differentiated and 2 poorly differentiated. In addition, 42onadenomatous (30 hyperplastic and 12 inflammatory) polypsere analyzed.
Correspondence between histopathology andonfocal laser endomicroscopy images. Intraepithelialeoplasia and/or cancer could be predicted in vivo by usinghe proposed classification of colorectal lesions (Table 1),ith sensitivity of 97.3% (72/74), specificity of 92.8% (39/42),nd accuracy of 95.7% (111/116). Two serrated adenomasere misclassified as hyperplastic polyps by C-CLE. Both
esions were diminutive. Conversely, 1 hyperplastic and 2nflammatory (pseudo)polyps were misclassified as adenomasith LGD by C-CLE. Two of these lesions were diminutive,nd 1 was small.
Characterization of advanced adenomas by con-ocal laser endomicroscopy. In this study, 32 advancedolorectal lesions were examined. Of them, 12 were large tubu-ar adenomas (�10 mm), 16 were adenomas with HGD with/ithout a villous component, and 4 were villous adenomas withGD. CLE showed villous features in 6 lesions that were diag-osed as tubular adenomas by ex vivo histopathology. Also,
C-CLE
Cytonuclear features
lar
n
● Epithelial cells are uniformly lined up along thebasement membrane
● Normal cell polarity of surface and glandularepithelium, normal aspect of mucin-producing gobletcells (epithelial cell maturation)
elongated
ing,
) or
● Epithelial cells are morphologically normal; preservedcell polarity
● Depletion of goblet cells
(LGD, SA),rowdingletely
tedsis, with
● Incomplete to lack of epithelial surface maturation(LGD, HGD, IC)
● Slight cytonuclear atypia: basally localized,“pencillate” nuclei, loss of cell polarity withpseudostratification (LGD, SA) to severe cytonuclearatypia: more apically localized, enlarged, roundishnuclei, depletion of goblet cells (HGD)
● Islands of malignant cells (IC)
sing
andu
atter
-like,
al fold
t (HP
sed
ryptslex ccomp
: dilagene
GD was found by CLE examination in a large flat adenoma

(c
ddp1eth[dsp
eyoo
pfpltglptgnamrp
testadfrp
abH
bgTHcacACpmi
crrvtpdvwr
oOrs
ccmaocrrdtio
T
H
FL
a
Month 2009 DIAGNOSIS OF COLORECTAL NEOPLASIA BY C–CLE 5
ARTICLE IN PRESS
II-a), whereas ex vivo histology showed LGD only. This indi-ates potential sampling error at biopsy.
Differentiation between high-grade and low-gradeysplasia by confocal laser endomicroscopy (adenomaysplasia score). Endomicroscopy images of adenomatousolyps with histologically proven LGD (n � 44) and HGD (n �6) were examined. ADS was calculated by summing scores forpithelial surface maturation, crypt morphology, vascular pat-ern, and cytonuclear atypia. Median ADS was significantlyigher in adenomas with HGD versus those with LGD (7
range, 4 – 8] vs 2 [range, 1–5]; P � .0001) (Figure 4.). ADS �5iscriminated HGD from LGD with 93.7% sensitivity, 97.7%pecificity, and accuracy of 96.7%. Clinical examples are de-icted in Figure 5.
DiscussionThis study showed that C-CLE allows accurate differ-
ntiation of adenomatous and nonadenomatous colorectal pol-ps during ongoing endoscopy. C-CLE predicted histopathol-gy with sensitivity of 97.3%, specificity of 92.8%, and accuracyf 95.7%.
In line with histopathology principles, special attention wasaid to describe general architectural as well as cytonucleareatures of colorectal mucosa during CLE examination. Weropose a systematic, reproducible classification of colorectal
esions by means of CLE. The following features were charac-eristic for adenomatous polyps: simple to complex crowding oflands (crypt budding), altered vascular pattern, lack of epithe-ial surface maturation, depletion of goblet cells, loss of cellolarity, and pseudostratification of irregular nuclei. In addi-ion, cancerous tissue showed crypt destruction and neoangio-enesis with interstitial leakage of fluorescein. In contrast,onadenomatous polyps were characterized by only minorbnormalities of crypt architecture (star-shaped, branch-like),inor alterations of vascular pattern, epithelial surface matu-
ation, preserved appearance of goblet cells, and maintained cellolarity.
Our results are in agreement with literature data indicatinghat CLE, either endoscopy-based or probed-based techniques,nables accurate in vivo characterization of colorectal neopla-ia.16,26 –28 This study also showed that C-CLE is a reproducibleool for classification of colorectal neoplasia when performed in
different center from the one where the basic concept waseveloped. The Mainz classification provides basic guidelinesor pattern recognition to distinguish among normal mucosa,egenerative changes, and neoplasia. However, a systematic ap-
able 3. Characteristics of the Study Population
Patients No. of polyps Sizea (mm)
istory of advanced adenoma and/orCRC (n � 24)
46 6 (2–18)
amily history of CRC (n � 28) 42 8 (3–32)ynch syndrome (n � 20) 28 8 (4–24)
Values are median (ranges).
roach with focus on architectural changes and cytonuclear d
typia is needed when presence and grading of dysplasia are toe evaluated. We defined the ADS, which reliably discriminatesGD from LGD during CLE.In the present study, 32 advanced neoplasias were examined
y C-CLE. In 7 (21.8%) of them, histologic diagnosis was up-raded by C-CLE from nonadvanced to advanced adenomas.his was due to detection of either a villous component or ofGD. It is conceivable that systematic scanning of large mu-
osal areas during C-CLE minimizes the risk of sampling errornd thereby might improve diagnostic accuracy. Of note, aonsiderable proportion of adenomas in this study was small.lthough most of these lesions were correctly classified duringLE, 5 (4.3%) small lesions were misclassified. Because smallolyps are more difficult to target, small-scale correlations re-ain difficult for both routine histopathology and CLE exam-
nation.Colonoscopic screening and surveillance have steadily in-
reased worldwide. Surprisingly, the protection against CRCemains far from perfect, among other factors, also as aesult of inherent limitations of endoscopic techniques. Sur-eillance policies are usually based on clinicopathologic fea-ures of adenomas. Recording of these features in routineractice frequently lacks precision and uniformity, making itifficult to draw firm conclusions regarding follow-up inter-als. Biopsy specimens do not represent histology of thehole polyp, leading to underestimation of advanced colo-
ectal neoplasia in up to 60% of cases.29
Quality improvement of colonoscopic examination in termsf detection and classification of lesions is therefore mandatory.ur data indicate that C-CLE offers considerable potential to
efine the diagnosis of colorectal lesions and, hence, to delineateubgroups of patients at high risk for CRC.
We believe the strength of this study is that patients wereonsecutively included via our multidisciplinary outpatientlinic, providing a survey of current practice. During endo-icroscopy, systematic examination was performed in an
ttempt to minimize the risk of sampling error. In addition,ptical biopsies of normal-appearing mucosa were taken asontrol data. The study results reinforce the need to adopteliable features and terminology for classification of colo-ectal neoplasia. However, such classification might remainifficult, because most histopathologic features are not pa-hognomonic and might not clearly distinguish among clin-cally relevant entities.30 It is also plausible that progressionf adenomas to CRC is merely a continuous process in which
LocationMorphology (Paris
classification)
ight colon Left colon Rectum 0-Ip 0-Is 0-IIa 0-IIb/c
15 21 10 20 20 6 0
26 10 6 10 22 8 212 8 8 18 6 4 0
R
ifferent stages coexist rather than a sequential process.

oun
scu(adhppesa
Fvnsemsvtsnocbccri
Ftps.
6 SANDULEANU ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. xx, No. x
ARTICLE IN PRESS
A few comments have to be made concerning method-logic aspects. Additional use of acriflavine enabled individ-al cell characterization and highlighted mucosal cyto-uclear features. Although some nuclear features, namely
t
ize, intracellular location, morphology, and pseudostratifi-ation, could be more precisely characterized by combinedse of fluorescein and acriflavine, other important aspects
eg, nuclear hyperchromasia, aspect of nucleoli) could not beddressed. This information is particularly important forifferentiation of HGD from LGD and for differentiation ofyperplastic polyps from serrated adenomas. The last areutative precursors of CRC via the newly described serratedathway.31 In this regard, new contrast agents should bexplored to accurately detect and characterize dysplastic tis-ue. A promising development was reported by Hsiung etl.32 These authors applied a fluorescein-bound heptapeptide
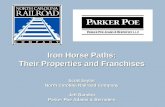
igure 3. (A) Normal colonic mucosa. (A-1) Endomicroscopy (acrifla-ine) shows regular crypt architecture. Crypt detail showing normaluclei (white dots) within the epithelial cells (arrow). (A-2) The corre-ponding histologic specimens of normal colonic mucosa (hematoxylin-osin staining, �30 original magnification; crypt detail, �50 originalagnification). (B) Hyperplastic polyp. The luminal openings of crypts
how stellar appearance (arrows) by CLE (acriflavine) (B-1) and by con-entional histology (B-2, hematoxylin-eosin, �20 original magnifica-ion). (C) Serrated adenoma. (C-1) CLE (acriflavine) shows epithelialurface maturation (arrow), regular crypts, and pseudostratification ofuclei (arrowhead). (C-2) Corresponding histologic specimens (�20riginal magnification). (D) Adenomatous polyp. Slight irregularity of therypts in a tubular adenoma by endomicroscopy (fluorescein) (D-1) andy conventional histology (D-2, �15 original magnification). (E) Invasivearcinoma. (E-1) Endomicroscopy of a poorly differentiated adenocar-inoma shows cryptal destruction, distorted vessels, leakage of fluo-escein into the surrounding tissue (neoangiogenesis, arrow), andslands of malignant (dark) cells (arrowhead). (E-2) Corresponding his-
igure 4. ADS was calculated by adding up scores correspondingo the following parameters: epithelial surface maturation, crypt mor-hology, vascular pattern, and cytonuclear atypia. Median ADS wasignificantly higher in adenomas with HGD vs those with LGD (P �0001).
ologic specimens (�20 original magnification).

te
jtdcagpu
1
1
1
1
1
1
1
1
1
1
FfsAcb
Month 2009 DIAGNOSIS OF COLORECTAL NEOPLASIA BY C–CLE 7
ARTICLE IN PRESS
opically to detect colonic dysplasia during endomicroscopyxamination.
In summary, we have shown that chromoendoscopy in con-unction with confocal endomicroscopy allows in vivo differen-iation of adenomatous and nonadenomatous colorectal polypsuring ongoing colonoscopy. We propose a systematic classifi-ation of colorectal lesions by CLE, yielding high interobservergreement. The ADS represents a step toward more objectiverading of dysplasia. This technology might offer considerableotential to ultimately fine-tune surveillance programs, partic-larly in high-risk groups.
References
1. International Agency for Research on Cancer. Globocan 2002:cancer incidence, prevalence, and mortality worldwide. Availableat: http://www-dep.iarc.fr/. Accessed February 26, 2009.
2. Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic alterationsduring colorectal tumor development. N Engl J Med 1988;319:525–532.
3. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectalcancer by colonoscopic polypectomy: the National Polyp StudyWorkgroup. N Engl J Med 1993;329:1977–1981.
4. Ansher AF, Lewis JH, Fleischer DE, et al. Hyperplastic colonicpolyps as a marker for adenomatous colonic polyps. Am J Gas-troenterol 1989;84:113–117.
5. Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screen-ing and surveillance: clinical guidelines and rationale—updatebased on new evidence. Gastroenterology 2003;124:544–560.
6. Winawer SJ, Zauber AG, Fletcher RH, et al. Guidelines for colonos-copy surveillance after polypectomy: a consensus update by theUS Multi-Society Task Force on Colorectal Cancer and the Amer-ican Cancer Society. Gastroenterology 2006;130:1872–1885.
7. Chandler I, Houlston RS. Interobserver agreement in grading ofcolorectal cancers—findings from a nationwide web-based survey
igure 5. Grading of dysplasia in adenomatous polyps. (A) Adenoma wamilial CRC (A-1). CLE (acriflavine) shows enlarged, slightly irregular crurface epithelium (A-3, arrowhead). Conventional histology of targedenoma with HGD. Endoscopic appearance of adenoma (Paris IIa�Iomplex crowding of crypts (B-2, arrow), reaching the surface epitheliuy conventional histology (B-4, �12 original magnification).
of histopathologists. Histopathology 2008;52:494–499. 2
8. Terry MB, Neugut AI, Bostick RM, et al. Reliability in the classifi-cation of advanced colorectal adenomas. Cancer Epidemiol Bi-omarkers Prev 2002;11:660–663.
9. Loeve F, van Ballegooijen M, Boer R, et al. Colorectal cancer riskin adenoma patients: a nation-wide study. Int J Cancer 2004;111:147–151.
0. Bressler B, Paszat LF, Vinden C, et al. Colonoscopic miss ratesfor right-sided colon cancer: a population based analysis. Gas-troenterology 2004;127:452–456.
1. Baxter NN, Goldwaser MA, Paszat LF, et al. Association ofcolonoscopy and death from colorectal cancer. Ann Intern Med2009;150:1–8.
2. Kiesslich R, Neurath MF. Chromoendoscopy and other novelimaging techniques. Gastroenterol Clin North Am 2006;35:605–619.
3. Bernstein CN. The color of dysplasia in ulcerative colitis. Gastro-enterology 2003;124:1135–1138.
4. Sakashita M, Inoue H, Kashida H, et al. Virtual histology ofcolorectal lesions using laser-scanning confocal microscopy. En-doscopy 2003;35:1033–1038.
5. Polglase AL, McLaren WJ, Skinner SA, et al. A fluorescenceendomicroscope for in vivo microscopy of the upper- and thelower GI tract. Gastrointest Endosc 2005;62:686–695.
6. Kiesslich R, Burg J, Vieth M, et al. Confocal laser endomicros-copy for diagnosing intraepithelial neoplasias and colorectal can-cer in vivo. Gastroenterology 2004;127:707–713.
7. Kiesslich R, Goetz M, Angus EM, et al. Identification of epithelialgaps in human small and large intestine by confocal endomicros-copy. Gastroenterology 2007;133:1769–1778.
8. Wainwright M. Dyes in the development of drugs and pharmaceu-tical. Dyes Pigments 2008;76:582–589.
9. Dove-Edwin J, de Jong AE, Adams J, et al. Prospective results ofsurveillance colonoscopy in dominant familial colorectal cancerwith and without Lynch syndrome. Gastroenterology 2006;130:1995–2000.
D. Endoscopic appearance of flat adenoma (Paris IIa) in a patient withnd pseudostratification of nuclei within the crypt (A-2, arrow), and theiopsies shows similar findings (A-4, �15 original magnification). (B)a patient with familial CRC (B-1). Endomicroscopy (acriflavine) showsat clearly lacks normal differentiation (B-3, arrowhead). Similar findings
ith LGypts ated bIc) inm, th
0. Participants in the Paris Workshop. The Paris endoscopic classi-

22
2
2
2
2
2
2
2
3
3
3
R
moM4
A
s
C
io
8 SANDULEANU ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. xx, No. x
ARTICLE IN PRESS
fication of superficial neoplastic lesions: oesophagus, stomach,and colon. Gastrointest Endosc 2003;58:S3–S43.
1. Kudo S. Early colorectal cancer. Tokyo, Japan: Igaku-Shoin, 1996.2. Schlemper RJ, Riddell RH, Kato Y, et al. The Vienna classification
of gastrointestinal neoplasia. Gut 2000;47:251–255.3. Hamilton S. Tumours of the digestive systen. Lyon: IARC Press,
2000.4. Zimmerman DW, Zumbo BD. The relative power of the Wilcoxon-
Mann Whitney test and Student t test under simple boundedtransformations. J Gen Psychology 1990;117:425–436.
5. Bland JM, Altman DG. Statistical methods for assessing agree-ment between two methods of clinical measurement. Lancet2009;1:307–310.
6. Kiesslich R, Goetz M, Rafoud K, et al. Staging of colorectalneoplasia with confocal laser endomicroscopy using two con-trast agents simultaneously. Gastrointest Endoscopy 2008;67:AB123.
7. Wallace MB, Fockens P. Probe-based confocal laser endomicros-copy. Gastroenterology 2009;136:1509–1513.
8. Sanduleanu S, Driessen A, Hameeteman W, et al. Inflammatorycloacogenic polyp: diagnostic features by confocal endomicros-copy. Gastrointest Endosc 2009;69:595–598.
9. Gondal G, Grotmol T, Hofstad B, et al. Biopsy of colorectal polypsis not adequate for grading of neoplasia. Endoscopy 2005;37:1193–1197.
0. Montgomery EA. Biopsy interpretation of gastrointestinal tract mu-
cosa. Philadelphia: Lippincott Williams & Wilkins, 2006:269–316. m1. East JE, Saunders BP, Jass JR. Sporadic and syndromatic hyper-plastic polyps and serrated adenomas of the colon: classifica-tion, molecular genetics, natural history, and clinical manage-ment. Gastroenterol Clin N Am 2008;37:25–46.
2. Hsiung P-L, Hardy J, Friedland S, et al. Detection of colonicdysplasia in vivo using a targeted heptapeptide and confocalmicroendoscopy. Nat Med 2009;14:454–458.
eprint requestsAddress requests for reprints to: S. Sanduleanu, MD, PhD, Depart-ent of Internal Medicine, Division of Gastroenterology and Hepatol-
gy, Maastricht University Medical Center, Postbox 5800, 6202 AZaastricht, The Netherlands. e-mail: [email protected]; fax: (31)3-3875006.
cknowledgmentsThe authors thank M. Frusch-Brouwer and Ton Mestrom for out-
tanding technical assistance.
onflicts of interestThese authors disclose the following: This study was investigator-
nitiated. Dr S. Sanduleanu and Prof Dr A. Masclee were the recipientsf an educational grant from Pentax B.V., The Netherlands. The re-
aining authors disclose no conflicts.