4 Bronchial Asthma
9
1 INTERNAL MEDICINE LEC . #4 PART #2, 04-03-2013 P.S. DOCTOR SAID THAT HE WOULD SPEAK QUICKLY TO LET US UNDERSTAND AND ANSWER THE QUESTIONS IN THE EXAM, SO THINGS HE DIDN'T MENTION YOU CAN GO BACK TO THE SLIDE TO READ THEM! BRONCHIAL ASTHMA Definition and Characteristi cs It is a chronic in flammatory disorder of the airways , its phenotypes or Causing recurrent/intermitte nt episodes (attacks) of: ❍ Wheezing ❍ Breathlessness ❍ Chest tightness ❍ Cough particularly more at night Those Symptoms are worse at night and/or in the early morning. when we test their lung function the Variable airflow limitation that is at least partly reversible either spontaneously or with treatment, in another words when we give them bronchodilator drug they usually go back to normal. Airway hyper-responsiveness to a variety of stimuli; for example when they smoke they show symptoms Wheezing, Chest tightness & Cough. The Scope of the Problem -USA There is no good studies about asthma in Jordan but it's very common, in USA it Affects 14 -15 million people, 6% of children under 18 years of age and adults having wide range of age , Inner city children have
-
Upload
shanfiza92 -
Category
Documents
-
view
219 -
download
0
Transcript of 4 Bronchial Asthma

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 1/9
1
INTERNAL MEDICINE LEC. #4 PART #2, 04-03-2013
P.S. DOCTOR SAID THAT HE WOULD SPEAK QUICKLY TO LET US UNDERSTAND AND ANSWER THE QUESTIONS IN THE EXAM , SO
THINGS HE DIDN'T MENTION YOU CAN GO BACK TO THE SLIDE TO READ THEM!
BRONCHIAL ASTHMA
Definition and Characteristics
It is a chronic inflammatory disorder of the
airways , its phenotypes or Causing
recurrent/intermittent episodes (attacks) of:
❍Wheezing
❍ Breathlessness
❍ Chest tightness
❍ Cough particularly more at night
Those Symptoms are worse at night and/or
in the early morning.
when we test their lung function the
Variable airflow limitation that is at least
partly reversible either spontaneously or with
treatment, in another words when we give
them bronchodilator drug they usually go back to normal.
Airway hyper-responsiveness to a variety of stimuli; for example when they smoke they
show symptoms Wheezing, Chest tightness & Cough.
The Scope of the Problem -USA
There is no good studies about asthma inJordan but it's very common, in USA it
Affects 14 -15 million people, 6% of children
under 18 years of age and adults having wide
range of age , Inner city children have

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 2/9
2
highest rates bcz of pollution, Rates higher among females, Rates higher among blacks.
This study has been made to know what is population's experience with asthma for
example 35.1% of population have family member of asthma and almost 6% themselves
have asthma, So asthma is a common disease, it's unusual that there is some body don't
know anything about asthma almost 25% or less.
causative factors of asthma are:
Genetic : those who are born with atopy, and
others bcz of Environmental factors : allergy,
viruses, diet, antibiotics and smoking.
Pathophysiology of asthma
It's complicated multiple cells, multiple pathways
and multiple cytokines are involved in the end all of
these lead to :
❍Inflammation of airway
❍Airway hyper responsiveness❍Airflow obstruction
❍Bronchial injury
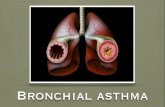
in this picture we can notice the difference
between the normal and asthmatic airways; where
the asthmatic one is narrowed, there is mucus
hyper secretion, smooth muscles hyperplasia, so it'snarrowed but not a mechanical narrow it's due to
thickening of the walls because of a disease so the
bronchodilators alone will not solve the problem.

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 3/9
3
Consequences of events of Asthma:
in the figure beside, there is a stimulus like
allergies to flowers or grass in spring season which
lead to acute airway inflammation which with timebecome chronic inflammation and injury to the
airway and with frequent inflammation lungs will
try to protect themselves by remodeling of the
airways, so it's not a benign disease.
in the figure beside, the lungs function was measured
by FEV1, the curve above is determining the lung
function of normal person it drops with age , but in
the lower curve for the asthmatic one which drops
worse with age , indicating that it's not a benign
reversible disease.
We can notice that the curve is a step wise manner ,
the steps usually indicate acute exacerbation of the
asthma; whenever there is worsening of the disease
or acute exacerbation they use more function of thelungs.
Asthma is an inflammatory airway disease, has it's won stimulus, cause airway hyper responsiveness, has
symptoms, not benign in all patients some of them progress and lose their lung function with time.
popularly asthma is known as chronic lifelong
disease, if asthma onset occurs at younger ages
5 years for example the majority of them will
be remission and some of them will persist, but
if it occurs at late stages the majority will
persist and some of them will resolve or
remission. So the Onset of the disease will
detect what will happen at the end.

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 4/9
4
Risk Factors for Asthma
Perinatal exposure to tobacco smoke, parents when they
smoke near their children they increase their risk of
asthma.so take this advice from Dr. "It's not a benign thing to
somebody to smoke in a KIA car with his wife and 5
children!!"
Atopy is associated with inherited elevation of total IgE
mediated to specific things like olive, house dust mite, ... ect.
Indoor Air Triggers, inside the house the most common is the
house dust mite ; which live on the dust we could see when sun
shine go through the window, we can inhale it to inter ourairways and other parts of our body, a lot of people are allergic
to this but it's very difficult to get rid of it bcz it's everywhere!
There are people allergic to Cockroaches, Animal dander (cats
and dogs), Environmental tobacco smoke
outdoor Air Triggers, olive is a common tree in Jordan bcz it's
easy to deal with so it presents everywhere and there are
somebody allergic to it.
Additional Triggers:
❍ Viral upper respiratory infections
❍ GERD (Gastroesophageal reflux disease)
❍ Sinusitis and rhinitis
❍ Diet, allergic to food
❍ Cold air
❍ Drugs, regarding the dentists almost the NSAIDs are
used, some patients of asthma die from one tablet or one injection of NSIAD, Beta
blockers for those with heart failure.

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 5/9
5
Asthma Diagnosis
usually it is clinical diagnosis just doing :
❍History and patterns of symptoms.
❍Physical examination, office spirometry.
❍Measurements of lung function.
❍Measurements of allergic status to identify risk factors to a certain patient.
Symptoms and Signs
❍Variety of symptoms
*wheeze*shortness of breath
*chest tightness that
*cough
worse during night or early in the morning and also there is something called provoked by
triggers
❍Asthma symptoms tend to be:
*Variable and intermittent, go up and down
*Worse at night and early morning , and there is seasonal variation to those with seasonalallergy
*Provoked by triggers, because of their airway hyper responsiveness to factors like
smoke, perfume ,.. ect.
❍Additional Elements in History
Personal or family history of:
Asthma, Atopic condition: eczema, allergic rhinitis
Worsening of symptoms after:
*Exposure to recognized triggers
*Taking aspirin, NSAID, b-blockers. it's important as a dentist to ask the patient is he has
allergy to one of them.
*Exercise, they are ok but when they run they start coughing especially in children.

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 6/9
6
In examination some patients look normal don't have any signs that doesn't mean they
don't have asthma, they may be normal during the day but get worse at night! but you
should hear wheezes.
Differential Diagnoses
what looks like asthma? those who have the same signs
and symptoms of asthma:
❍ COPD; this is a similar disease but in heavy smokers
with 50 or more years of age, who have more than 20
years back of smoking.
❍ Gastro-esophageal reflux disease (GERD); they have
cough during night.
❍ Cystic fibrosis; sputum production❍ Vocal cord dysfunction;
Diagnostic Tools
❍Peak flow monitoring by patients, a small instrument
measures the speed of the air exhalation of the patient,
for example measure the peak flow at morning it's 300
then at night it becomes 600 which is the variability that is
typical to asthma.❍Pulmonary function testing (spirometry)
1- Obstructive pattern
↓ Forced Vital Capacity (FVC)
↓ Forced Expiratory Volume in 1 second (FEV1)
FEV1/FVC < 70% to say that this patient is asthmatic.
2- Reversible airflow limitation
FEV1 increases by ≥ 15% after inhalation of a rapid-acting beta-2-agonistthat means the patient who has obstruction or he can't exhale all air from his lungs is
given a bronchodilator then measure the obstruction again , if he gets better by more
than 15% then he is asthmatic.

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 7/9
7
Clinical Control of Asthma
Asthma at the past was a difficult disease to treat but now with discovery of newer
medications especially inhaled corticosteroids we can control asthma, in a large number
of patients they are completely normal they have:
✔ No (or minimal)* daytime
symptoms
✔ No limitations of activity
✔ No nocturnal symptoms
✔ No (or minimal) need for rescue
medication
✔ Normal lung function
✔ No exacerbations
_________
Minimal = twice or less per week
So it can be controlled , diagnosed
and treated appropriately.
# Usually we classify asthma according to the characteristics mentioned in the table
above; Controlled, partly controlled or Uncontrolled. then we can make adjustment to
the medication accordingly. But the main goal of us to get the patient to the left sided
column (controlled).
Asthma Management
Although there is no cure for asthma Appropriate management most often results in
the achievement of control, if it cured it will cure spontaneously.
Controller Medications1- Inhaled glucocorticosteroids , which is the most important one. 2- Leukotriene modifiers, it's name is montelukast in the market it can be effective
especially children
3- Anti-IgE , they are expensive can be very effective with some patients. 4- Theophylline

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 8/9
8
5- Systemic glucocorticosteroids , used in severe cases. Long-acting inhaled β2-agonists
Reliever Medications
those medication are given to the patient in emergencies when we want a rapidresponse:
1- Rapid-acting inhaled β2-agonists : available in the hospital which is Salbutamol ,
available as tablet, syrup or inhaler.
2- Systemic glucocorticosteroids ,
used in acute exacerbation.
**a picture of inhalers we use :
** the table below just to knowthat there is step up step down
approach for the pulmonologist
to help them decide to increase
or decrease the dose of a drug.
Asthma Exacerbations
It's the same asthma but sometimes it get acute to
worse those have :
Episodes of progressive increase in shortness of
breath, cough, wheezing, or chest tightness
Characterized by decreases in expiratory airflow
Potentially life-threatening and treatment requires close supervision
there were patients who were dead because of asthma in the hospital! So Asthma is nota completely benign disease like many people think!
Manage Asthma Exacerbations
we use the same medication used to manage the chronic asthma but more intensively,
for example instead of giving inhaler we give metaboliser or IV.

7/29/2019 4 Bronchial Asthma
http://slidepdf.com/reader/full/4-bronchial-asthma 9/9
9
ORAL HEALTH CHANGES IN PATIENTS WITH ASTHMA
Increased rate of caries development
Reduced salivary flow
Oral mucosal changes
Gingivitis
Orofacial abnormalities (adenoid face)
Increased upper anterior and
total anterior facial height
Higher palatal vaults
Greater overjets
Higher prevalence of posterior crossbites
_____________________________________
☀☁【THE HAPPY END】☀☁ Done by :
Baraa'h Al-Salamat