16 Woeber Graves’ Disease - UCSF · PDF filecongenital malformations (esophageal...
34
Graves Graves ’ ’ Disease Disease Kenneth A. Kenneth A. Woeber Woeber , MD, FRCPE , MD, FRCPE
Transcript of 16 Woeber Graves’ Disease - UCSF · PDF filecongenital malformations (esophageal...

GravesGraves’’ DiseaseDisease
Kenneth A. Kenneth A. WoeberWoeber, MD, FRCPE, MD, FRCPE


Causes of HyperthyroidismCauses of Hyperthyroidism
CommonCommonGravesGraves’’ hyperthyroidism, exogenous thyroid hormone hyperthyroidism, exogenous thyroid hormone excess, toxic excess, toxic multinodularmultinodular goiter, goiter, subacutesubacute thyroiditisthyroiditis
UncommonUncommontoxic adenoma, iodine excesstoxic adenoma, iodine excess
RareRaregestational transient gestational transient thyrotoxicosisthyrotoxicosis, , trophoblastictrophoblastictumors, TSH tumors, TSH hypersecretionhypersecretion, ectopic , ectopic thyoidthyoid tissue, tissue, constitutively activated TSHconstitutively activated TSH--receptor mutations, Gsreceptor mutations, Gs--alpha mutationalpha mutation

Results Results ofLaboratoryofLaboratory Investigations Investigations in Gravesin Graves’’ HyperthyroidismHyperthyroidism
Serum TSH very low or undetectableSerum TSH very low or undetectableSerum T3 and usually serum T4 elevated, Serum T3 and usually serum T4 elevated, with increased T3/T4 ratiowith increased T3/T4 ratioThyroid radioiodine uptake increased, with Thyroid radioiodine uptake increased, with diffuse pattern on diffuse pattern on scintiscanscintiscanTSH receptor antibodies present in serumTSH receptor antibodies present in serum

Epidemiology of GravesEpidemiology of Graves’’ DiseaseDisease
Cause of 50 Cause of 50 –– 80% of cases of hyperthyroidism80% of cases of hyperthyroidismPrevalence: 0.6% of populationPrevalence: 0.6% of populationIncidence: 0.5/1000/yearIncidence: 0.5/1000/yearFemale/male ratio: 5/1 Female/male ratio: 5/1 –– 10/110/1Peak incidence: 40 Peak incidence: 40 –– 60 years of age60 years of ageConcordance rate: monozygotic twins 35%; Concordance rate: monozygotic twins 35%; dizygoticdizygotictwins 3% twins 3% ((BrixBrix et al., J et al., J ClinClin EndocrinolEndocrinol MetabMetab 86: 930, 2001)86: 930, 2001)
Predisposition: 79% genetic; 21% Predisposition: 79% genetic; 21% nongeneticnongeneticFemale siblings and female children have 5 Female siblings and female children have 5 –– 8% risk8% risk

Pathogenesis of GravesPathogenesis of Graves’’ DiseaseDisease
AutoreactiveAutoreactive T cells and B cellsT cells and B cells emerge andemerge andinfiltrate the thyroid gland (as well asinfiltrate the thyroid gland (as well asextrathyroidalextrathyroidal tissues) and elaboratetissues) and elaboratevarious cytokines that ultimately lead tovarious cytokines that ultimately lead toproduction of TSH receptor antibodiesproduction of TSH receptor antibodies((TSHRAbTSHRAb) as a result of:) as a result of:
Genetic susceptibilityGenetic susceptibilityEnvironmental factorsEnvironmental factors -- infections, stress, smokinginfections, stress, smokingEndogenous factorsEndogenous factors -- female gender female gender

Susceptibility Genes in GravesSusceptibility Genes in Graves’’ DiseaseDisease
HLAHLA--DR geneDR gene -- DRB1 variant results in altered DRB1 variant results in altered peptide presentation to T cellspeptide presentation to T cellsCTLACTLA--4 gene4 gene -- several single nucleotide several single nucleotide polymorphisms (polymorphisms (SNPsSNPs) result in enhanced T cell ) result in enhanced T cell activationactivationCD40 geneCD40 gene -- ? C/T SNP results in enhanced B cell ? C/T SNP results in enhanced B cell activationactivationTSHR geneTSHR gene -- ? several ? several SNPsSNPs lead to alterations in lead to alterations in TSHR extracellular domainTSHR extracellular domain(modified from Jacobson and (modified from Jacobson and TomerTomer, Thyroid 17: 949, 2007), Thyroid 17: 949, 2007)

Manifestations of GravesManifestations of Graves’’ DiseaseDisease
diffuse goiter in >90%diffuse goiter in >90%overt infiltrative overt infiltrative ophthalmopathyophthalmopathy in ~50%in ~50%overt infiltrative overt infiltrative dermopathydermopathy in <5%in <5%TSHRAbTSHRAb in >80%in >80%TPOAbTPOAb in ~75%in ~75%overlap with other autoimmune diseasesoverlap with other autoimmune diseases
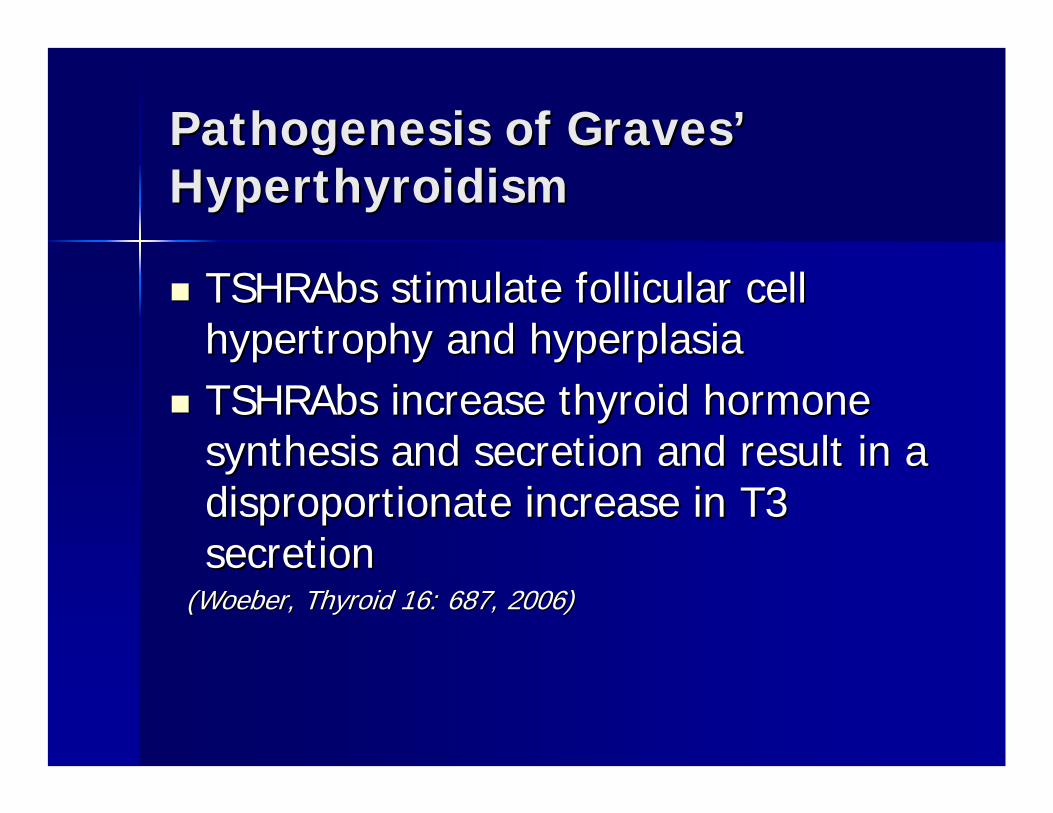
Pathogenesis of GravesPathogenesis of Graves’’HyperthyroidismHyperthyroidism
TSHRAbsTSHRAbs stimulate follicular cell stimulate follicular cell hypertrophy and hyperplasiahypertrophy and hyperplasiaTSHRAbsTSHRAbs increase thyroid hormone increase thyroid hormone synthesis and secretion and result in a synthesis and secretion and result in a disproportionate increase in T3 disproportionate increase in T3 secretionsecretion
((WoeberWoeber, Thyroid 16: 687, 2006), Thyroid 16: 687, 2006)


NOSPECS Classification of Ocular NOSPECS Classification of Ocular Manifestations of GravesManifestations of Graves’’ OphthalmopathyOphthalmopathy
0 0 -- No changesNo changes1 1 -- Only lid retractionOnly lid retraction2 2 -- Soft tissue involvementSoft tissue involvement3 3 -- ProptosisProptosis4 4 -- ExtraocularExtraocular muscle involvementmuscle involvement5 5 -- Corneal involvementCorneal involvement6 6 -- Sight loss due to optic nerve involvementSight loss due to optic nerve involvement

Pathogenesis of Pathogenesis of GravesGraves’’ophthalmopathyophthalmopathy
Characterized by increased orbital fat and increased Characterized by increased orbital fat and increased extraocularextraocular muscle volumemuscle volumeOrbital Orbital preadipocytepreadipocyte fibroblasts express TSHR and expression fibroblasts express TSHR and expression correlates with eye disease activitycorrelates with eye disease activityTSHRAbsTSHRAbs are potent stimulators of are potent stimulators of adipogenesisadipogenesis in cultures of in cultures of orbital orbital preadipocytepreadipocyte fibroblastsfibroblastsInfiltration of Infiltration of autoreactiveautoreactive T cells targeted through T cells targeted through recognition of TSHRrecognition of TSHR-- expressing fibroblasts results in expressing fibroblasts results in cytokinecytokine--mediated mediated adipogenesisadipogenesis and hydrophilic and hydrophilic glycosaminoglycanglycosaminoglycan productionproduction
(modified from (modified from KhooKhoo and and BahnBahn, Thyroid 17: 1013, 2007), Thyroid 17: 1013, 2007)


Pathogenesis of Infiltrative Pathogenesis of Infiltrative DermopathyDermopathy
Infiltration of Infiltration of autoreactiveautoreactive T cells in T cells in cutaneouscutaneous tissues targeted by TSHRtissues targeted by TSHR--expressing fibroblasts results in expressing fibroblasts results in cytokinecytokine--mediated hydrophilic mediated hydrophilic glycosaminoglycanglycosaminoglycan production, causing production, causing edema and ultimately fibrosisedema and ultimately fibrosis


PREVALENCE OF ATRIAL FIBRILLATION INENDOGENOUS OVERT AND SUBCLINICAL
HYPERTHYROIDISM
22,300 513 ( 2.3%)
725 100 (13.8%)*
613 78 (12.7%)*
Control (>45 years)(TSH 0.4 - 4.0 mU/ L)
Overt Hyperthyroidism(TSH < 0.03 mU/ L)
Subclinical Hyperthyroidism(TSH < 0.4 mU/ L)
Group Number With AtrialFibrillation
*p < 0.01 vs Control Group.Adapted from Auer et al., Am Heart J 148:838, 2001

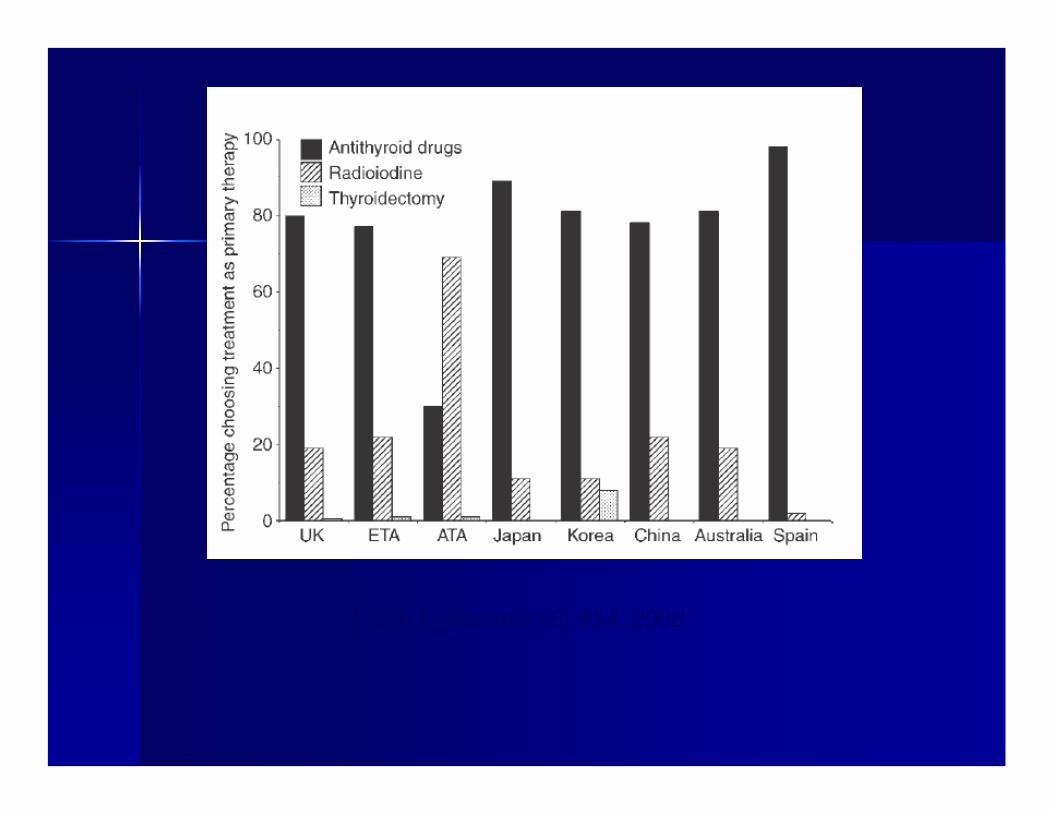
From Vaidya et al. Clin Endocrinol 68: 814, 2008

MethimazoleMethimazole (MMI) or (MMI) or CarbimazoleCarbimazole (CMI) vs. (CMI) vs.
PropylthiouracilPropylthiouracil (PTU)(PTU)
MMI 15 mg once daily as effective as PTU 100 mg three times dailMMI 15 mg once daily as effective as PTU 100 mg three times daily y with lower incidence of minor adverse effects (14 % vs. 52 %)with lower incidence of minor adverse effects (14 % vs. 52 %)MMI 15 mg twice daily is more effective than 15 mg once daily wiMMI 15 mg twice daily is more effective than 15 mg once daily with th higher incidence of minor adverse effects (30 % vs. 14 %)higher incidence of minor adverse effects (30 % vs. 14 %)(Nakamura et al., J (Nakamura et al., J ClinClin EndocrinolEndocrinol MetabMetab 92: 2157, 2007)92: 2157, 2007)
Serious adverse effects are rare with both drugsSerious adverse effects are rare with both drugs–– agranulocytosisagranulocytosis (baseline WBC) (baseline WBC) –– MPOMPO--ANCA, ANCA, vasculitisvasculitis, and lupus, and lupus--like syndromelike syndrome–– hepatitis (hepatitis (cholestaticcholestatic with MMI or CMI and with MMI or CMI and necroinflammatorynecroinflammatory
with PTU) (baseline with PTU) (baseline alkalk. . phosphos. and ALT). and ALT)

MMI or CMI vs. PTU (cont.)MMI or CMI vs. PTU (cont.)
MMI, CMI,MMI, CMI, and PTU reduce efficacy of 131I treatment, and PTU reduce efficacy of 131I treatment, with larger effect of PTU with larger effect of PTU (Walter et al., BMJ 334: 514, 2007) (Walter et al., BMJ 334: 514, 2007)
MMI during gestation may be rarely associated with MMI during gestation may be rarely associated with congenital malformations (esophageal congenital malformations (esophageal atresiaatresia, , choanalchoanalatresiaatresia, , aplasiaaplasia cutis) cutis) ((DiGiantonioDiGiantonio et al., Teratology 64:et al., Teratology 64: 262,.262,.2001).2001). No associations with PTU have been reported; No associations with PTU have been reported; therefore preferred drug during gestation.therefore preferred drug during gestation.

Randomized Prospective Studies on Effect of Randomized Prospective Studies on Effect of CarbimazoleCarbimazole Treatment DurationTreatment Duration
Relapse rate at 2 years was 58% after 6 months compared Relapse rate at 2 years was 58% after 6 months compared to 38% after 18 months to 38% after 18 months ((AllanicAllanic et al., J et al., J ClinClin EndocrinolEndocrinol MetabMetab70:675, 1990)70:675, 1990)
Relapse rate at 2 years was 46% after 12 months compared Relapse rate at 2 years was 46% after 12 months compared to 54% after 24 months and at 5 years was 86% and 83%, to 54% after 24 months and at 5 years was 86% and 83%, respectively respectively (Garcia(Garcia--Mayor et al., J Mayor et al., J EndocrinolEndocrinol Invest 15: 815, Invest 15: 815, 1992). 1992).
Relapse rate at 1 year was 59% after 6 months compared to Relapse rate at 1 year was 59% after 6 months compared to 65% after 12 months 65% after 12 months ((WeetmanWeetman et al., Q J Med 87: 337, 1994).et al., Q J Med 87: 337, 1994).
Relapse rate at 2 years was 36% after 18 months compared Relapse rate at 2 years was 36% after 18 months compared to 29% afterto 29% after 42 months 42 months ((MaugendreMaugendre et al., et al., ClinClin EndocrinolEndocrinol 50:127, 50:127, 1999)1999)

Comparison of Block Comparison of Block –– Replace Replace regimen with Titration regimenregimen with Titration regimen
12 12 randomisedrandomised controlled trials revealed no controlled trials revealed no significant difference between the regimens significant difference between the regimens with respect to relapse of Graveswith respect to relapse of Graves’’hyperthyroidism (RR 0.93; 95%CI 0.84 hyperthyroidism (RR 0.93; 95%CI 0.84 ––1.03)1.03)(Abraham et al., (Abraham et al., EurEur J J EndocrinolEndocrinol 153: 489, 2005)153: 489, 2005)

Predictors of RelapsePredictors of Relapse
young patientyoung patientmale gendermale gendercigarette smokingcigarette smokinglarge goiterlarge goitersevere severe ophthalmopathyophthalmopathyundetectable TSHundetectable TSHhigh high TSHRAbTSHRAb

Indications for Indications for 131131I treatmentI treatment
severe severe thyrocardiacthyrocardiac diseasediseasetoxic nodular goitertoxic nodular goiteradverse reaction to adverse reaction to antithyroidantithyroid drugdrugrelapse after 12 to 18 months of relapse after 12 to 18 months of antithyroidantithyroiddrug treatmentdrug treatment

131131I Treatment of HyperthyroidismI Treatment of Hyperthyroidism(Alexander and Larsen, J (Alexander and Larsen, J ClinClin EndocrinolEndocrinol MetabMetab 87: 1073, 2002)87: 1073, 2002)
261 patients treated with 261 patients treated with 131131I providing an average retained I providing an average retained dose of 173 dose of 173 uCi/guCi/g at 24 hat 24 h225 patients (86 %) became hypothyroid or 225 patients (86 %) became hypothyroid or euthyroideuthyroid at 1 yr, at 1 yr, of whom 79 % were on PTU or MMI before of whom 79 % were on PTU or MMI before 131131I; 36 patients I; 36 patients (14 %) remained hyperthyroid of whom all had been on PTU (14 %) remained hyperthyroid of whom all had been on PTU or MMI before or MMI before 131131IIinverse, asymptotic relationship between retained inverse, asymptotic relationship between retained 131131I at 24 h I at 24 h and persistent hyperthyroidism with success rate of ~90 % and persistent hyperthyroidism with success rate of ~90 % with doses >138 with doses >138 uCi/guCi/g; failure rate of ~10 % did not decline ; failure rate of ~10 % did not decline with doses up to 400 with doses up to 400 uCi/guCi/g
Calculation of Calculation of 131131I DoseI Dose
Target dose = ~150 Target dose = ~150 uCi/guCi/g as efficacy not as efficacy not increased with higher dose increased with higher dose 131131I dose (I dose (mCimCi) = 0.15 multiplied by estimated ) = 0.15 multiplied by estimated gland weight (g) divided by fractional uptake gland weight (g) divided by fractional uptake of of 131131I at 24 h I at 24 h



Outcomes of 10Outcomes of 10--year MMI versus year MMI versus 131131IITreatmentsTreatments ((AziziAzizi et al., et al., EurEur J J EndocrinolEndocrinol152:695,2005)152:695,2005)
MMI group (n=26) 100% MMI group (n=26) 100% euthyroideuthyroid, 50% , 50% had goiterhad goiter131131I group (n=41) 61% hypothyroid, 25% I group (n=41) 61% hypothyroid, 25% had goiterhad goiterQoLQoL score, DXA, & Echocardiogram score, DXA, & Echocardiogram similarsimilarTotal and LDL cholesterol higher in Total and LDL cholesterol higher in 131131I I groupgroup

Indications for Indications for ThyroidectomyThyroidectomy
large goiter with compressive large goiter with compressive manifestationsmanifestationspregnant patient with adverse reaction to pregnant patient with adverse reaction to antithyroidantithyroid drugdrugsevere infiltrative eye disease severe infiltrative eye disease ((MoletiMoleti et al., et al., Thyroid 13: 653, 2003; Thyroid 13: 653, 2003; UsulaUsula et al., Asian J et al., Asian J SurgSurg 31: 115, 31: 115, 2008)2008)

Pharmacological Utility of Iodine Pharmacological Utility of Iodine ((LugolLugol’’ss iodine 3 drops iodine 3 drops t.i.dt.i.d. or SSKI 1 drop . or SSKI 1 drop t.i.dt.i.d.).)
Abrupt decrease in thyroid hormone secretion dueAbrupt decrease in thyroid hormone secretion dueto transient (~10 days) inhibition of to transient (~10 days) inhibition of thyroglobulinthyroglobulinproteolysis proteolysis ((WartofskyWartofsky et al., J et al., J ClinClin InvestInvest 49: 78, 1970)49: 78, 1970) --indicated in thyroid stormindicated in thyroid stormTransient reduction of thyroid Transient reduction of thyroid vascularityvascularity ininGravesGraves’’ hyperthyroidism hyperthyroidism (Erbil et al., J (Erbil et al., J ClinClin EndocrinolEndocrinol
MetabMetab 92: 2182, 2007)92: 2182, 2007) -- indicated for 10 days beforeindicated for 10 days beforethyroidectomythyroidectomyInhibition of thyroid hormone synthesis after Inhibition of thyroid hormone synthesis after 131131IItreatment due to failure of escape from Wolfftreatment due to failure of escape from Wolff--ChaikoffChaikoff effect effect ((BravermanBraverman et al., N et al., N EnglEngl J MedJ Med 281: 816, 1969)281: 816, 1969)

Management of GravesManagement of Graves’’ OphthalmopathyOphthalmopathy
Acute Active PhaseAcute Active Phasedark lensesdark lenseselevate head of bedelevate head of bedartificial tears & ointmentsartificial tears & ointmentsdiureticsdiureticsprisms for prisms for diplopiadiplopiaglucocorticoidsglucocorticoids &/or orbital radiotherapy for severe disease &/or orbital radiotherapy for severe disease
((BartelenaBartelena J J ClinClin EndocrinolEndocrinol MetabMetab 90: 5497, 2005)90: 5497, 2005)
surgical followed by surgical followed by 131131I ablation for severe diseaseI ablation for severe disease((MoletiMoleti et al. Thyroid 13: 653, 2003; et al. Thyroid 13: 653, 2003; UsluUslu et al. Asian J et al. Asian J SurgSurg 31: 115, 2008)31: 115, 2008)
Chronic Inactive PhaseChronic Inactive Phaseorbital decompressionorbital decompressioneye muscle surgeryeye muscle surgeryeyelid surgeryeyelid surgery